
Abstract
The objective of this study was to assess the biofidelity of the Global Human Body Models Consortium (GHBMC) 50th male (M50-O) v6.0 seated in an upright (25-degree recline) all-belts-to-seat (ABTS) in a 56 km/h rear-facing frontal impact. The experimental boundary conditions from the post-mortem human subjects (PMHS) tests were replicated in the computational finite element (FE) environment. The performance of the rigidized FE ABTS model obtained from the original equipment manufacturer was validated via simulations using a Hybrid III FE model and comparison with experiments. Biofidelity of the GHBMC M50-O was evaluated using the most updated NHTSA Biofidelity Ranking System (BRS) method, where a biofidelity score under 2 indicates that the GHBMC response varies from the mean PMHS response by less than two standard deviations, suggesting good biofidelity. The GHBMC M50-O received an occupant response score and a seat loading score of 1.71 and 1.44, respectively. Head (BRS = 0.93) and pelvis (BRS = 1.29) resultant accelerations, and T-spine (avg. BRS = 1.55) and pelvis (BRS = 1.66) y-angular velocities were similar to the PMHS. The T-spine resultant accelerations (avg. BRS = 1.93) and head (BRS = 2.82), T1 (BRS = 2.10) and pelvis (BRS = 2.10) Z-displacements were underestimated in the GHBMC. Peak chest deflection in the anterior-posterior deflection in the GHBMC matched with the PMHS mean, however, the relative upward motion of abdominal contents and subsequent chest expansion were not observed in the GHBMC. Updates to the GHBMC M50-O towards improved thorax kinematics and mobility of abdominal organs should be considered to replicate PMHS characteristics more closely.
Keywords:
Introduction
Vehicles equipped with advanced driver-assistance systems (ADAS) technologies such as forward collision warning, autonomous emergency braking, and lane departure warning represent Level 2 automation in vehicles and have already helped reduce injury to occupants during frontal impacts (Cicchino Citation2017; Cicchino Citation2018). The concept of automated driving systems (ADS) that represent Level 4 and 5 ‘self-driving‘ automation is also being pursued (Lutin et al. Citation2013). Eliminating traditional driving position requirements in ADS-equipped vehicles could result in a potential shift to non-traditional seating configurations for the efficient utilization of vehicle interior space. The effectiveness of restraint systems, typically designed for forward-facing and upright occupants, could potentially change for occupants seated in non-traditional seating configurations. In case the ADS-equipped vehicles are unable to perform equal to or better than human operators, there may be crashes that can prove more injurious or fatal for vehicle occupants.
A survey study identified rear-facing (RF) seats as a potential configuration for front-row occupants, where they can engage in conversations with second-row forward-facing occupants in a ‘campfire‘ arrangement during long drives (Jorlöv et al. Citation2017). When ADS-equipped vehicles are exposed to a frontal impact, RF occupants experience rear impact kinematics and interaction with the seat back and head restraint. The injury risk of RF occupants in frontal crashes is not well understood due to the lack of fatality and injury data from real world 1st row RF frontal crashes. Recently, a series of high-speed (56 km/h) RF frontal impact sled tests were conducted to investigate biomechanical responses and injuries of 50th percentile male (50 M) post-mortem human subjects (PMHS) (Kang et al. Citation2020, Kang et al. Citation2022, Kang et al. Citation2023). In these studies, two different seats, an all-belts-to-seat (ABTS) and a conventional seat, and two different seat back recline angles, 25-degree and 45-degree, were used. The ABTS has a shoulder belt retractor installed within the seat back, and buckle and lap belt portion of the belt are anchored to the seat pan (Kang et al. Citation2020). Multiple rib fractures and pelvis injuries were observed in the PMHS during their interaction with the seat back components in both the upright (25-degree) and reclined (45-degree) seat back conditions.
Safety tools such as anthropomorphic test devices (ATDs) and finite-element (FE) human body models (HBMs) are being relied on in various crash configurations, to assess injury risks to occupants. HBMs, in particular, have a detailed representation of human anatomy and material properties (Pipkorn et al. Citation2019). To use HBMs for the evaluation of seats and restraint systems, they should replicate human-like characteristics in any crash mode being studied. PMHS response corridors generated by Kang et al. (Citation2020) have been previously utilized in the biofidelity assessment of the THOR-50M ATD in the same loading conditions, using the NHTSA Biofidelity Ranking System (BRS) (Hagedorn et al. Citation2022). Although good biofidelity was found in the spine and thorax of the ATD in the upright seat back condition, occupant response characteristics such as spine straightening, ramping along the seat back, and pelvis kinematics still need to be improved. The Total Human Model for Safety (THUMS) FE model has been previously used in a high-speed RF frontal impact condition, in which the Neck Injury Criteria (Nij) and upper chest deflection values were higher compared to other seating configurations, reflecting the injury potential in the RF scenario (Kitagawa et al. Citation2017, Wu et al. Citation2020). However, the THUMS model was only validated up to 8 km/h against PMHS data (Iwamoto et al. Citation2018). The Global Human Body Models Consortium (GHBMC) 50th male occupant (M50-O) model has been previously evaluated in both low-speed (<17km/h) and moderate-speed (24 km/h) rear impacts (Katagiri et al. Citation2019). The model exhibited PMHS-like gross kinematics with good biofidelity in the head to T1 region in moderate-speed (24 km/h) rear impacts, which were consistent with the head and neck validation in low-speed (<17km/h) rear impacts (Fice et al. Citation2011). Zeng et al. (Citation2021) validated the chest deflection (Correlation and Analysis (CORA) score = 0.94) and spine extension (CORA score = 0.89) of the GHBMC v4.5 in a rear hub impact at 5.5 m/s. However, the loading of the occupant back is expected to be different between a rear hub impact and a rear sled impact involving an original equipment manufacturer (OEM) seat. In a 37 km/h rear impact study with the GHBMC M50-O in a fixed seat back condition, rib fractures, predicted by the elastoplastic material model at a failure strain of 1.8% for the cortical bone, were observed (Ramachandra et al. Citation2021). However, there were no biomechanical and injury data (e.g. PMHS data) to confirm these outcomes. The GHBMC M50-O model has not been evaluated in a high-speed RF frontal impact condition. Improving and validating the model in this impact condition is essential to better comprehend PMHS interaction with seat and restraint systems. It will also help develop and evaluate the efficacy of new seat designs, restraint systems and other counter measures towards occupant protection in ADS-equipped vehicles in the future.
As a preliminary step towards model improvement, the current study aims to evaluate the biofidelity of GHBMC M50-O seated in a RF ABTS with a 25-degree fixed seat back recline angle in a high-speed frontal-impact simulation (ΔV of 56 km/h) using the available PMHS biomechanical corridors (Kang et al. Citation2020, hereafter referred as Kang study).
Methods
A FE model of a rigidized Honda Odyssey ABTS (TS Tech Americas, Inc, OH, USA) and the GHBMC M50 v6.0 occupant model (Elemance, LLC, NC, USA) were used to simulate occupant response in a high-speed RF frontal impact condition. The seat was validated using simulations with the Hybrid III FE model against physical tests. The seat validation process is shown in Appendix A. FE simulations were performed using the general-purpose multi-physics simulation software package LS-DYNA MPP v11.0.0 (LSTC, CA, USA) on 168 processors on the Owens cluster at the Ohio Supercomputer Center (OSC, OH, USA).
Sled boundary conditions
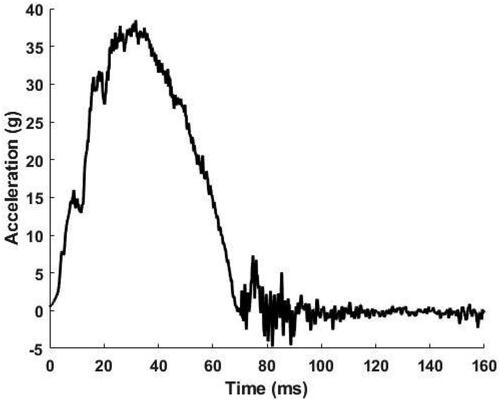
The experimental boundary conditions from the Kang study were replicated in LS-PrePost. A rigid sled floor was created using shell elements to represent its thin plate geometry and was only allowed to translate in the global X-direction (SAEJ211). Seat back rotation was restricted using a reinforcing frame. The load plates, load cells (LCs), and a rigid backplate were simplified using the geometry of the reinforcing frame, which was obtained from a three-dimensional laser scan (FARO Edge Arm, Lake Mary, FL). The frame was meshed using hexahedral solid elements to represent the simple uniform solid volume geometry of the load plates and load cells. Hexahedral elements were preferred over tetrahedral elements from an overall computational effectiveness standpoint for the current setup (Benzley et al., Citation1995; Tadepalli et al., Citation2011). Biased meshing was utilized at the interfaces to maintain nodal connectivity. An isometric view of the simplified reinforcing frame is shown in . The backplate () was constrained as a rigid body to the sled floor, and the seat anchor nodes were constrained to the sled floor as an extra node set (). The head restraint (HR) was isolated from the seat model and attached to a load plate through a tied contact. The most posterior nodes of the HR LC were tied to a reinforcing plate. The nodes of the bottom surface of the reinforcing plate were constrained as an extra node set to the sled floor (). Since the sled pulses from the PMHS tests were repeatable in nature, an unfiltered sled pulse from one of the tests (PMHS2) () was applied to the sled floor using a prescribed boundary motion.
Figure 1. Simplified reinforcing frame consisting of top plate, middle plate, back plate and LCs - A. top left B. top right C. middle left D. middle right E. bottom left F. bottom right.
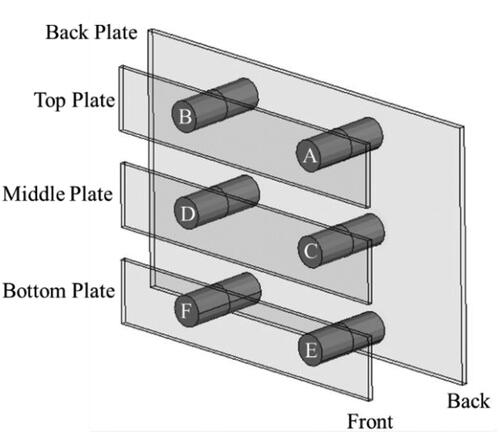
Figure 2. Sled boundary conditions. The sled floor was constrained to move in the X-direction.
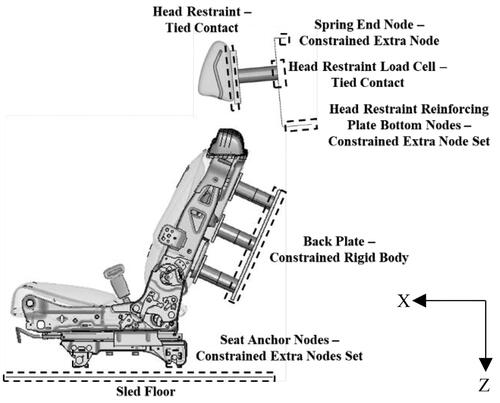
Figure 3. Sled pulse derived from experiments (Kang et al. Citation2020).
Development of spine curvatures of the PMHS and GHBMC spine curvature adjustment
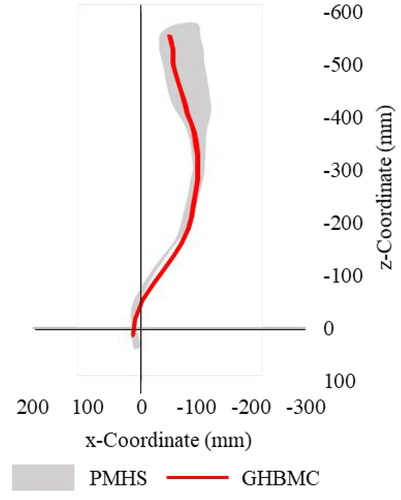
The mid-anterior points on vertebral bodies of the three male PMHS (mean ± 1 standard deviation age = 59.7 ± 51 years, mean ± 1 standard deviation weight = 76.4 ± 15.9 kg) were digitized from X-ray images in WebPlotDigitizer (Rohatgi Citation2014). Individual PMHS characteristics can be found in the Kang study. The digitized images were transformed from the X-ray domain to the FARO domain by using bony landmarks (e.g. mastoid process and anterior superior iliac spine) and instrumentation locations (e.g. a center of C4 and C6 motion blocks). The X-ray images and spinal curvatures are shown in . A corridor for the spine curvatures from the PMHS (mean ± 1 standard deviation) is shown in . The spine curvature of the GHBMC was adjusted using the boundary prescribed final geometry function to comply with the PMHS spine curvature corridor (). The origin was located at the lumbar vertebra L5 – sacrum S1 joint center.
Figure 4. Spinal curvatures determined from PMHS X-ray images.
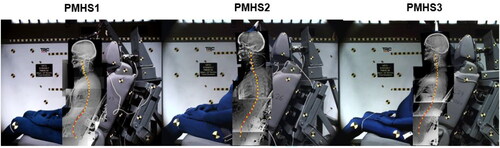
Figure 5. Corridor for spine curvature from the PMHS and adjusted GHBMC spine curvature.
Gravity settling of GHBMC and final setup
A combination of a boundary-prescribed final geometry function and a belt-pulling technique (Poulard et al. Citation2015) were used to match the positioning targets of the GHBMC (). The bones were constrained using Single Point Constraints (SPCs) in all directions except in the z-translational direction for gravity settling on the seat in a pre-simulation. Differences in anthropometry between the PMHS and GHBMC are shown in Table C1. The gravity-settled position of the GHBMC was used for seat belt routing and pretensioning. HR adjustment was done similarly to the Hybrid III simulation (Appendix A). A simulation was performed using the gravity-settled and belted GHBMC, while an input sled pulse was applied to the sled. A coefficient of friction of 0.2 (Bini Leite, Citation2021; Friedman et al., Citation2017) was used for an automatic surface-to-surface contact between the GHBMC and seat in the simulation.
Figure 6. Final GHBMC setup based on PMHS positioning information A: Thigh angle (11.3 deg) B: Leg angle (43.5 deg) C: Pelvis angle (31.9 deg) D: Backset (95 mm) E: Topset (93.90 mm) F: Greater trochanter (GT) height (48.6 mm) G: Acromion height (563.8 mm).
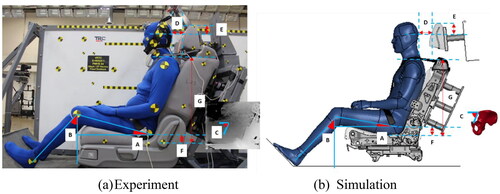
Table 1. Summary of method of alignment for dummy curves (Hagedorn et al. Citation2022), BRS score, time duration for BRS calculation, absolute value of DPS and average and maximum of absolute values of PMHS shift for occupant kinematics.
Data analysis
Head kinematics were obtained from a constrained interpolation node at the head center of gravity (ID 1990002), which was pre-defined head instrumentation in the GHBMC. Constrained interpolation nodes for the thoracic spine (T1, T4, T8 and T12), pelvis, femora, and tibiae were modeled using the whole bones for the node sets. Body-fixed coordinate systems were defined in the same way as the Kang study. Chest deflection was measured between chestband nodes on the anterior side (ID 4198170) and posterior side (ID 4198203) in the local coordinate system (ID 1994201) and normalized by half chest depth. Uncompensated seat reaction load corridors were generated from the PMHS experiments. Corresponding loads for the GHBMC were obtained using the same method as the Hybrid III simulation (Appendix A). GHBMC data were filtered in the same way as the Kang study, with the exception of lower extremities, where a CFC180 filter was used. This change was also implemented in the PMHS lower extremity data for consistent comparisons. The most updated NHTSA BRS was utilized to quantify the biofidelity scores (Hagedorn et al. Citation2022). The response curve alignment techniques and time durations used for calculations were consistent with those used for the THOR ATD in the same loading condition in the Hagedorn study ( and ). A BRS score under 2 indicates that the GHBMC response is within two standard deviations of the PMHS mean response, suggesting good biofidelity. An occupant response score was computed as an average of BRS scores of the kinematics of the relevant body regions of the GHBMC (). One of the angular rate sensors for T8 failed in one PMHS test so a biomechanical corridor could not be generated. Additionally, a seat loading score was computed as an average of BRS scores of resultant forces obtained from the LCs used in this study to investigate how closely the GHBMC matched PMHS interactions with the seat back and HR (). A dummy phase shift (DPS) value was reported along with the calculated BRS score as supplemental information (Hagedorn et al. Citation2022). In this study, the GHBMC model will be treated as the ‘dummy‘. The phase shift represents the amount of physical time shift needed to align common events, such as, an increase and/or a decrease in the magnitude of the response or peak response of the dummy time history to the mean PMHS time history. This was done to prevent phase differences between dummy and PMHS from negatively influencing BRS scores. DPS is not a part of the BRS calculation and analysis. However, DPS becomes meaningful when compared to phase variations amongst the PMHS tested in the same loading condition. Specifically, the average and maximum phase shifts (Donnelly and Moorhouse Citation2012) performed on the PMHS response curves for corridor generation can be utilized to compare and gain insights into the phase biofidelity of HBMs or ATDs. The PMHS average and maximum phase shifts are reported as supplemental information in and , similar to Hagedorn et al. (Citation2022). The current study focuses only on BRS scores, and DPS information could be utilized for future studies.
Figure 7. Evaluation of occupant response score and seat loading score. Here, Ar: Resultant acceleration, Ry: Y-rotation, Dx: X-displacement, Dz: Z-displacement, Wy: y-angular velocity, A-P: anterior-posterior and Fr: Resultant force.
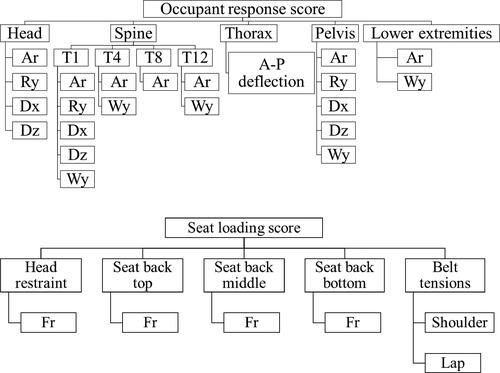
Table 2. Summary of method of alignment for dummy curves (Hagedorn et al. Citation2022), BRS score, time duration for BRS calculation, absolute value of DPS and average and maximum of absolute values of PMHS shift for seat reaction loads and belt tensions.
Results
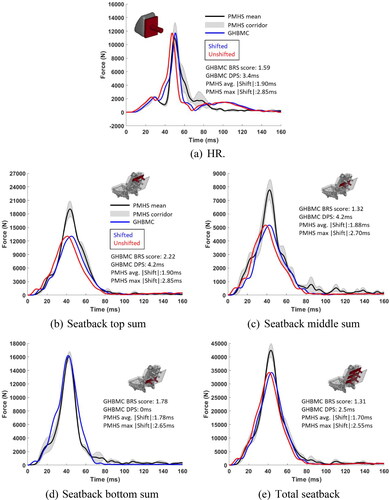
The GHBMC M50-O received an occupant response score and a seat loading score of 1.71 and 1.44, respectively. Information on DPS has been provided in and . The average BRS scores for each body region are shown in Table C2, and for each seat location and belt are shown in Table C3. The GHBMC kinematics and seat reaction loads generally trended similar to the PMHS, but some of the peak responses were underestimated. Although GHBMC head Y-rotation deviated from the corresponding PMHS corridor around 125 ms (), the BRS score for the overall response was 1.17 owing to the large variation in PMHS head Y-rotation. PMHS variation in T1 Y-rotation () was more than the variation in T1 resultant acceleration (), similar to the head rotation (). This was reflected in the corresponding BRS scores for the GHBMC, as T1 Y-rotation in the GHBMC deviated from the PMHS corridor around 70 ms. The peak T4 positive (forward) angular velocity in the GHBMC was within the PMHS corridor, whereas the peak T4 negative (rearward) angular velocity was slightly outside the PMHS corridor (Figure B1b). A sudden drop in T8 resultant acceleration after the first peak in the GHBMC occurred at the time of initiation of seat back compression at the top (Figure B2). The peak T12 resultant acceleration was about 60g lower in the GHBMC as compared to the PMHS mean (). The y-angular velocity of T12 of the GHBMC fell inside the corresponding PMHS corridor for most of the time duration (). The pelvis of the GHBMC had a large peak forward rotation of 20 degrees as compared to 4.3 degrees for the PMHS mean (). Resultant accelerations () and y-angular velocities () of lower extremities of the GHBMC generally exhibited peaks and trends similar to the PMHS. The peak HR resultant force in the simulation () fell within the experimental corridor but the response returned to zero quicker than the PMHS mean. Although the peak resultant forces at the top () and middle () of the seat back from thorax interaction with the seat back were outside the corresponding PMHS corridors, the rates of loading and unloading were similar to the experiments. The peak resultant force at the bottom of the seat back from pelvis interaction with the seat back was within the PMHS corridor (). The shape of the total seat back resultant force time history for the simulation was similar to the PMHS. However, the peak force in the simulation had a peak error of 19.3% with respect to the PMHS mean peak ().
Figure 8. Head kinematics.
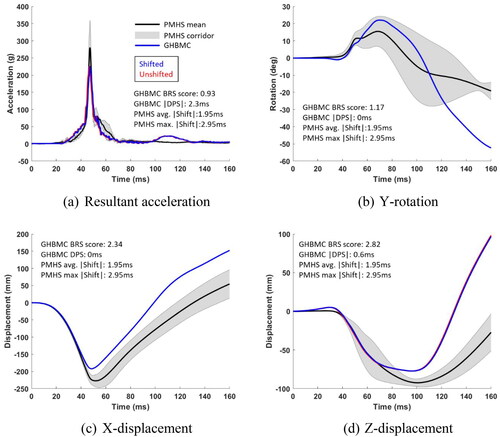
Figure 9. T1 kinematics.
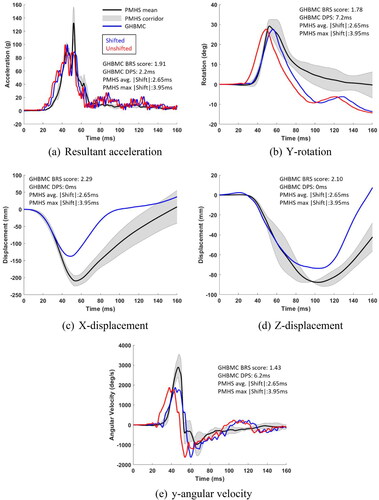
Figure 10. Pelvis kinematics.
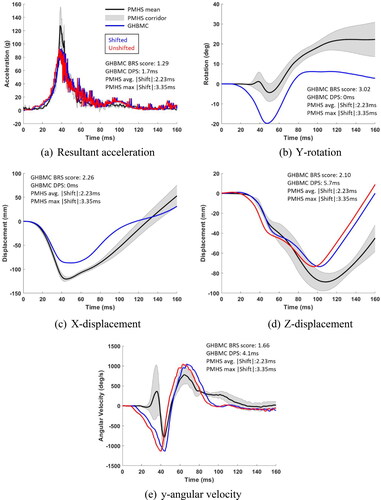
Figure 11. Seat resultant forces.
Discussion
Head-neck interaction with HR
The GHBMC exhibited good biofidelity for head resultant acceleration (BRS = 0.93) and HR resultant force (BRS = 1.59), likely due to biofidelic GHBMC head compliance during interaction with the HR. The Y-rotation of the GHBMC head demonstrated good biofidelity (BRS = 1.17), consistent with outcomes from previous studies (low-speed: Fice et al. Citation2011 and moderate-speed: Katagiri et al. Citation2019). Anisotropy, asymmetry in tension and compression loading, and a wide range of strain-rate sensitivity have been incorporated in the GHBMC neck skin, adipose tissue and passive musculature. These updated properties have been previously shown to improve agreement of GHBMC head rotation with PMHS corridors for 7 g rear impacts (Gierczycka et al. Citation2021).
Head X-displacement was biofidelic up to the peak (BRS = 1.17), however overall biofidelity was poor (BRS = 2.34). Peak head X-displacement of the GHBMC was 35.1 mm lower than the PMHS mean peak (). Of all the parts in the GHBMC head, the highest internal energy increase was predicted in the head flesh (Part ID 1400036), which could influence the head X-displacement. Overly stiff viscoelastic properties of head and neck flesh may reduce the flesh deformation and cause lower head X-displacement, as has previously been observed in the GHBMC (Gierczycka et al. Citation2021).
The overall shape and trace of T1 resultant acceleration () in the GHBMC was similar to the PMHS (BRS = 1.91). However, the second peak was underestimated. Differences in neck anthropometry between the GHBMC and PMHS could potentially affect T1 kinematics. For instance, the neck circumference of the GHBMC is 3.8 cm lower than the PMHS mean, indicating that the soft tissue distribution in the neck of the GHBMC was probably different from the PMHS, resulting in lower peak T1 resultant acceleration in the GHBMC. The peak T1 X-displacement of the GHBMC was 71.9 mm lower than the mean PMHS peak (). T1 Y-rotation () also exhibited good biofidelity (BRS = 1.78). Higher forward rotation was seen in both head and T1 in the rebound phase in the GHBMC, which is probably influenced by differences in neck muscle geometry and/or passive muscle response with respect to PMHS during flexion. Previous studies have shown geometry of the muscle-tendon complex to have a significant effect on passive muscle stretch (Best et al. Citation1994) and differences in passive muscle response between PMHS and live humans (on which the models are based) (Van Ee et al. Citation1998).
Spine straightening and ramping behaviour
Angular velocities about the y-axis are representative of spine straightening behaviour as discussed in the Kang study. T1, T4, and T8 of the GHBMC exhibited peak rearward angular velocity, while T12 exhibited peak forward angular velocity at the time of peak rearward translation into the seat back. BRS scores for these responses were less than 2, indicating a similar spine straightening behaviour as the PMHS (Figure B6). The change in spinal curvature of the GHBMC from 0 to 45 ms was very small between spinal levels T7 and L2 (Figure B7), indicating that the GHBMC might have a stiffer thoracolumbar spine as compared to the PMHS. Stiffness of the thoracolumbar spine has been shown to influence GHBMC ramping up the seat back in moderate-speed rear impacts (Katagiri et al. Citation2019).
The shoulder (Figure B8a) and lap (Figure B8b) belt forces exhibited BRS scores of 1.17 and 0.69, respectively, demonstrating similar soft tissue-seatbelt interactions between GHBMC and the PMHS. However, GHBMC peak pelvis Z-displacement was 17% lower than the PMHS mean, indicating that the GHBMC did not ramp up as much as the PMHS (). One of the potential reasons for lower ramping in the GHBMC is the large forward Y-rotation of the pelvis () due to the pelvis pocketing into the seat and interacting with the metal cross bar in the bottom of the seat back (Figure B9). Element instability was observed in the sacroiliac (SI) joints during pelvis rotation (Figure B10), indicating non-biofidelic deformation of the SI joints or pelvis. Moreover, the higher pelvis rotation in the GHBMC () could generate shear forces between the pelvis and the surrounding soft tissue that are sufficient enough to cause the soft tissue to get into the gap between the seat back and seat pan foams during the rearward translation phase (Figure B11), restricting peak ramping. A lack of biofidelity was observed in other kinematics representing ramping, such as the head () and T1 () Z-displacements, consistent with the pelvis Z-displacement (). The peak head and T1 Z-displacements in the GHBMC were lower than the corresponding mean PMHS peaks by 15.2 and 14.1 mm, respectively.
Unlike the PMHS, the relative upward motion of the abdominal organs into the thoracic cavity and subsequent expansion of the thorax (Figure B12) was not observed in the GHBMC during ramping (up to 100 ms). Although current material properties and element formulations in the abdominal region could limit a phenomenon like soft tissue expansion in the GHBMC (Perez-Rapela et al. Citation2019), differences in anthropometry between the GHBMC and PMHS may also lead to differences in abdominal responses. The GHBMC has a smaller abdomen compared to the PMHS used in the experiments (Figure B13), as indicated by a smaller waist depth (92.1 cm in GHBMC vs 94.6 cm PMHS mean). This suggested that the PMHS could have abdominal organs that weighed more than those in the GHBMC and were therefore subjected to higher inertial loading resulting in more relative upward motion. Lee and Kim (Citation2017) found that chest x-displacement in the GHBMC with a morphed abdomen has a good CORA rating with respect to PMHS in a high-speed frontal impact scenario. Therefore, morphing the abdominal region of the GHBMC to match the abdominal anthropometry of the PMHS could help improve the abdominal upward movement.
The diaphragm in the human body has ligamentous connections with the stomach, spleen, and liver (e.g. falciform ligaments connecting the diaphragm and liver). The diaphragm undergoes deformation during ramping up of abdominal organs as loads are transferred through the ligaments. Any difference in stiffness of the diaphragm (MAT181–Simplified_Rubber/Foam) or the ligaments (MAT74–Elastic_Spring_Discrete_Beam) between the GHBMC and PMHS could affect the biofidelity of upward motion of abdominal organs. Abdominal organs are connected to each other via the mesentery, which were modelled as tied contacts in the GHBMC. The tied contacts could possibly reduce the relative mobility of organs in the GHBMC.
Occupant interaction with seat back
Resultant accelerations of the spine and pelvis, as well as resultant seat reaction loads, are indicators of the interaction between the occupant and the seat back (Kang study; Kang et al. Citation2022). The peak resultant accelerations of T4 (Figure B1a), T8 (Figure B2), and T12 (Figure B3a) were lower than the corresponding mean PMHS peaks by 42, 59 and 54 g, respectively. Lower peak resultant forces were observed in the seat back top () and middle () compared to the PMHS, consistent with spinal acceleration outcomes. Lower seat back loads for the GHBMC were previously observed in moderate-speed rear impacts, as compared to the PMHS (Katagiri et al. Citation2019). The underestimation of peak accelerations in the thoracic spine of the GHBMC might be from either the foam material optimized from Hybrid III simulation or from compliance of the back and vertebral bodies. Lack of spinal biofidelity from the difference in compliance with respect to PMHS has been previously observed in the GHBMC in a side impact condition (Park et al. Citation2013). Ramachandra et al. (Citation2019) observed a softer initial response in the GHBMC from more compliant skin and musculature in the thoracic region than PMHS. Although the loading condition in the previous study was a low-severity frontal hub impact, the material properties in the muscles, skin, and adipose tissue in the GHBMC could affect the kinematics of the thoracic vertebrae and chest AP deflection in a high-severity RF frontal impact.
Although chest AP deflection was biofidelic up to the peak compression (Figure B12), only one rib (L8) on the posterior side in the GHBMC experienced the cortical bone failure threshold of 1.8% effective plastic strain, up to peak compression. On the contrary, multiple rib fractures were observed on the posterior left side in the PMHS, up to peak chest compression. The difference in the shape of the ribs or distribution of cortical thickness along the ribs may lead to differences in rib deformation between the GHBMC and the PMHS (Li et al. Citation2010). The GHBMC ribs have been represented through bilinear material curves in the piecewise linear plastic model, which takes elastic modulus, yield stress, and tangent modulus into account. A parametric study could be done by updating these material model parameters to see the effect of material properties on rib deformation patterns.
The resultant acceleration of the pelvis in the GHBMC had good biofidelity (BRS = 1.29), supporting the similarity of soft tissue and back muscle compliance with the PMHS. However, its peak was lower than the PMHS mean (), likely due to larger forward rotation of the pelvis (). Further exploration is needed to confirm this. The rotation of the pelvis is possibly linked to the position of the pelvis with respect to the seat. Since the GHBMC skin and adipose tissue were stiff during gravity settling on the seat, achieving the same GT height was impossible, resulting in a higher Z-location of the GHBMC pelvis than the PMHS. Cortical bone failures were predicted in the pelvis of the GHBMC along the left acetabular rim and inferior edges of both the SI joints as the pelvis underwent rotation and rearward translation (Figure B14). On the contrary, the PMHS did not sustain any pelvis injuries. The difference in pelvis kinematics may be playing a role in the difference in pelvis injury outcomes between the GHBMC and PMHS. Strain rate sensitivity has not been currently implemented in the piecewise linear plastic model for both cortical and cancellous bone of the pelvis in the GHBMC. With Cowper-Symonds strain rate sensitivity, the material of the pelvis could possibly sustain higher stresses for each strain level without undergoing failure. Moreover, the maximum principal strain threshold of 2.5% for cortical bone failure derived from isolated pelvis low-speed impact tests (Guillemot et al. Citation1997) and coupon tensile tests (Kemper et al. Citation2008) might be underpredicted for RF impacts, resulting in overprediction of failures. The peak resultant force on the seat back bottom in the simulation had good biofidelity (B = 1.78), consistent with pelvis resultant acceleration.
Lower extremities kinematics
The pelvis and lower extremities directly interacted with metal components in the seat back and seat pan during rearward excursion (Figure B15), resulting in excessive noise in contact forces in the simulation from the contact algorithm in LS-DYNA. The noise was more pronounced in the lower extremities than the pelvis. To reduce the effect of contact noise on biofidelity evaluation of lower extremities, and have a better comparison with biofidelity evaluations of other body regions and for consideration towards average biofidelity of the GHBMC, a CFC180 filter was used instead of CFC1000 filter for lower extremities. Linear kinematics of the lower extremities of the GHBMC had good biofidelity (BRS ≤ 2), indicating efficient modelling of the ball and socket joint in the pelvis. Although the rotational characteristics of the femora of the GHBMC had good biofidelity, a significant deviation was observed in the rotational kinematics of the tibiae in the rebound phase due to a kicking-up motion (Figure B16), which was also observed in moderate-speed rear impacts (Katagiri et al. Citation2019). This could be due to a lower y-axis rotational stiffness at the knee joints in the GHBMC compared to the PMHS. Shear failure was predicted in the femoral head and necks of the GHBMC in the preliminary simulations (Figure B14), which could subsequently affect the pelvis and lower extremity responses (Figure B17). Since no injuries were reported in the lower extremities of the PMHS, the failure criteria were turned off for the lower extremities in the GHBMC.
Limitations
The soft tissues of the GHBMC have been shown to be stiff during gravity settling (Gepner et al. Citation2022) on the seat back and seat pan, thereby not allowing the model to fully conform to the final position based on anatomical landmarks from experiments, which may affect the responses.
Small seat back rotation and seat sliding, as seen during the PMHS experiments, may affect the occupant responses and seat reaction loads. The seat back reinforcing frame and the seat anchor bolts in the simulation were rigidly constrained to the sled floor which was only allowed to translate in the x-direction, thereby not allowing any seat back rotation and seat slide. Physical joint connections with rotational stiffness could be introduced in the seat back reinforcing frame to allow seat back rotation.
The resultant peak accelerations of vertebral bodies in the GHBMC may have been underpredicted by the stiffness of the foam material, which was optimized through LSTC Hybrid III simulations and not directly obtained from material testing of the foam. Lack of foam compression or bottoming out near the retractor structure due to stiff foam material could have prevented localized rib deformations and fractures in the GHBMC. The forward rotation of the pelvis in the GHBMC may have been amplified by stiff seat back foam material interaction, which did not allow the pelvis to translate into the seat back as much as the PMHS pelvis. The LSTC Hybrid III FE model has not been previously validated in rear impacts. Foam material densification was adjusted in the current study due to the rigidity of the Hybrid III, and its ability to bottom-out seat back foam during rearward excursion on the seat. The foam material densification that aided in matching the peak seat back reaction loads in the simulation to ATD experiments, might be extreme for deformable HBMs, such as the GHBMC. shows the comparison of the total seat back resultant force and the occupant inertia force. The peak total seat back resultant force was higher than the peak occupant inertia force due to contact between the occupant and the seat back, indicating the role of the seat back in governing the peak total seat back resultant force. Material testing of the physical foam could be done at different strain rates and incorporated into the strain rate sensitive Fu Chang foam material model (MAT 83, LS-DYNA manual) in the simulation to see if better outcomes can be achieved for the GHBMC as compared to the foam optimization technique. Moreover, the foam material property utilized in this study was optimized only for the loading phase of the impact since the majority of the rib fractures sustained by the PMHS seated on the ABTS (25-degree recline) were observed up to peak seat back loading in the Kang study. Generic model parameters were used for the unloading phase in the material model, which might have resulted in a quicker rebound in the simulations than in experiments. An additional effort could be made to optimize the foam material property for the unloading phase.
Previous response comparisons of the GHBMC with PMHS in rear impact scenarios were not only in low-to-moderate speeds, but also utilized deformable HRs and seat backs (typical of real-world rear impacts). Given that the boundary conditions in PMHS experiments in the RF frontal impact scenario are more extreme in terms of the impact speed, and a supported HR and seat back, the GHBMC outcomes could be influenced by the boundary conditions utilized. It would be useful to compare GHBMC’s response in the high-speed RF frontal impact scenario for an unsupported HR/seat back condition, if PMHS data were available.
There were anthropometric and inertial differences in the abdominal region of the GHBMC and PMHS. This will affect the inertial loading up the seat back during the high-speed RF frontal impact, therefore, the relative mobility of abdominal organs into the thoracic cavity. Future studies could aim to morph the abdominal region of the GHBMC to that of the PMHS to see the effect on the relative mobility of abdominal organs.
CORA method has typically been used for biofidelity evaluation of the GHBMC. However, the current study utilized the NHTSA BRS method. This was consistent with BRS evaluations performed for the THOR (Hagedorn et al. Citation2022) and THOR-AV (Wang Citation2022) ATDs in the same high-speed RF frontal impact condition. This could be useful for comparative analysis between the ATDs and the GHBMC in this loading condition in the future. However, CORA evaluations should also be performed for the GHBMC in this loading condition in the future.
Conclusions
The present study validated an OEM ABTS seat model using a Hybrid III FE model in a high-speed RF frontal impact scenario, and utilized the validated seat for evaluating the biofidelity of GHBMC M50-O in the same loading condition using the most recent BRS method. The study used a novel approach to optimize the foam material for the seat back. A comprehensive comparison of PMHS and GHBMC outcomes was made and found that the GHBMC M50-O received an occupant response score and a seat loading score of 1.71 and 1.44, respectively. Head and lower extremities of the GHBMC M50-O exhibited a good average biofidelity. Peak resultant accelerations for T4, T8 and T12 were underestimated in the GHBMC M50-O, consistent with seat back loading at the top and middle. Spine straightening behavior was seen in the GHBMC M50-O, similar to the PMHS. Peak ramping was underestimated in the GHBMC M50-O, resulting in a poor biofidelity score. Although peak chest compression was similar to the PMHS, the GHBMC M50-O did not experience a movement of abdominal contents into the thoracic cavity causing chest expansion like in the PMHS. Only one rib fracture (L8-posterior) was predicted in the GHBMC M50-O, unlike multiple rib fractures in the PMHS. A large pelvis forward rotation in the GHBMC M50-O was experienced during the rearward excursion and may be one of the reasons for the observed pelvic injuries, unlike the PMHS.
| Abbreviations | ||
| ABTS | = | all-belts-to-seat |
| ADAS | = | advanced driver assistance systems |
| ADS | = | automated driving systems |
| ATD | = | anthropomorphic test device |
| BRS | = | biofidelity ranking system |
| CORA | = | correlation and analysis |
| DPS | = | dummy phase shift |
| FE | = | finite element |
| GHBMC | = | global human body models consortium |
| HBM | = | human body model |
| HR | = | head restraint |
| LC | = | load cell |
| Nij | = | neck injury criteria |
| OEM | = | original equipment manufacturer |
| PMHS | = | post-mortem human subject |
| RF | = | rear-facing |
| THUMS | = | total human model for safety |
Supplemental Material
Download MS Word (5.6 MB)Acknowledgements
We would like to acknowledge TS-Tech Americas, Inc for providing the FE model of the OEM seat. We would also like to thank the Ohio Supercomputer Center for providing resource units for running our simulations. Finally, we would like to thank all the faculty, staff, and students at the Injury Biomechanics Research Center for assisting with various aspects of the project and providing valuable insights on the same.
Disclosure statement
The primary author of the paper does not have anything to disclose.
Additional information
Funding
References
- Benzley SE, Perry E, Merkley K, Clark B, Sjaardama G. 4th international meshing roundtable, A comparison of all hexagonal and all tetrahedral finite element meshes for elastic and elasto-plastic analysis, Sandia National Laboratories Albuquerque, NM, 1995, 17.
- Best TM, McElhaney J, Garrett WE, Jr, Myers BS. 1994. Characterization of the passive responses of live skeletal muscle using the quasi-linear theory of viscoelasticity. J Biomech. 27(4):413–419. doi:10.1016/0021-9290(94)90017-5.
- Bini Leite, Rafael. 2021. Dynamics of and injury assessment to occupants in high-speed planing boats under pure vertical loading condition using a human body model with active muscle behaviour. Doctoral dissertation, Wichita State University.
- Cicchino JB. 2017. Effectiveness of forward collision warning and autonomous emergency braking systems in reducing front-to-rear crash rates. Accid Anal Prev. 99(Pt A):142–152. doi:10.1016/2016-11-009.
- Cicchino JB. 2018. Effects of lane departure warning on police-reported crash rates. J Saf Res. 66:61–70. doi:10.1016/2018-05-006.
- Donnelly BR, Moorhouse K. 2012. Optimized phasing of PMHS response curves for biofidelity targets. In IRCOBI Conference Proceedings (No. IRC-12-51).
- Elemance LLC. 2021. Global Human Body Models Consortium User Manual: m 50 Detailed Occupant Version 6.0 for LS-DYNA®.
- Fice JB, Cronin DS, Panzer MB. 2011. Cervical spine model to predict capsular ligament response in rear impact. Ann Biomed Eng. 39(8):2152–2162. doi:10.1007/s10439-011-0315-4.
- Friedman K, Mattos G, Bui K, Hutchinson J. 2017. Potential Effects of Friction on Injury Measures Computed in Aircraft Seat HIC Analysis Testing. SAE Technical Paper. doi: 10.4271/2017-01-2054.
- Gepner BD, Perez-Rapela D, Forman JL, Ostling M, Pipkorn B, Kerrigan JR. 2022. Evaluation of GHBMC, THUMS and SAFER human body models in frontal impacts in reclined postures. Paper presented at: international Research Council on Biomechanics of Injury (IRCOBI); Porto, Portugal; September p. 14–16.
- Gierczycka D, Rycman A, Cronin D. 2021. Importance of passive muscle, skin, and adipose tissue mechanical properties on head and neck response in rear impacts assessed with a finite element model. Traffic Inj Prev. 22(5):407–412. doi:10.1080/15389588.2021.1918685.
- Guillemot H, Besnault B, Robin S, Got C, Le Coz JY, Lavaste F, Lassau JP. 1997. Pelvic injuries in side impact collisions: a field accident analysis and dynamic tests on isolated pelvic bones. SAE Trans. 106:3624–3633.
- Hagedorn A, Stammen J, Ramachandra R, Rhule H, Thomas C, Suntay B, Kang Y-S, Kwon HJ, Moorhouse K, Bolte Iv JH. 2022. Biofidelity evaluation of THOR-50M in rear-facing seating configurations using an updated Biofidelity Ranking System. SAE Int J Trans Saf. 10(2):291–375. doi:10.4271/09-10-02-0013.
- Iwamoto M, Nakahira Y, Kato D. 2018. Finite element analysis for investigating the effects of muscle activation on head-neck injury risks of drivers rear-ended by a car after an autonomous emergency braking. IJAE. 9(3):124–129. doi:10.20485/9.3_124.
- Jorlöv S, Bohman K, Larsson A. 2017. Seating positions and activities in highly automated cars - a qualitative study of future automated driving scenarios. Paper presented at: international Research Council on Biomechanics of Injury (IRCOBI); Antwerp, Belgium; September p. 13–15.
- Kang Y, Stammen J, Ramachandra R, Agnew AM, Hagedorn A, Thomas C, Kwon HJ, Moorhouse K, Bolte JH. 2020. Biomechanical responses and injury assessment of post mortem human subjects in various rear-facing seating configurations. Stapp Car Crash J. 64:155–212. doi:10.4271/2020-22-0005.
- Kang Y, Stammen J, Bendig A, Agnew AM, Hagedorn A, Thomas C, Ramachandra R, Kwon HJ, Moorhouse K, Bolte JH. 2022. Effects of seatback recline and belt restraint type on PMHS responses and injuries in rear-facing frontal impacts. SAE Int J Trans Saf. 10(2):235–284. doi:10.4271/09-10-02-0012.
- Kang Y, Stammen J, Agnew AM, Baker GH, Pradhan V, Bendig A, Hagedorn A, Moorhouse K, Bolte JH. 2023. Thoracic responses and injuries to male postmortem human subjects (PMHS) in rear-facing seat configurations in high-speed frontal impacts. Traffic Inj Prev. 24(sup1):S47–S54. doi:10.1080/15389588.2023.2167490.
- Katagiri M, Zhao J, Lee S, Moorhouse K, Kang YS. 2019. Biofidelity evaluation of GHBMC male occupant models in rear impacts. Paper presented at: international Research Council on Biomechanics of Injury (IRCOBI); Florence, Italy; September p. 11–13.
- Kemper AR, McNally C, Duma SM. 2008. Dynamic tensile material properties of human pelvic cortical bone. Biomed Sci Instrum. 44:417–418. PMID: 19141951.
- Kitagawa Y, Hayashi S, Yamada K, Gotoh M. 2017. Occupant kinematics in simulated autonomous driving vehicle collisions: influence of seating position, direction and angle. Stapp Car Crash J. 61:101–155. 1994593908.
- Lee I, Kim H. 2017. Evaluation of biofidelity of the human body model morphed to female with abdominal obesity in frontal crashes. SAE Technical Paper. doi: 10.4271/2017-01-1429.
- Li Z, Kindig MW, Subit D, Kent RW. 2010. Influence of mesh density, cortical thickness and material properties on human rib fracture prediction. Med Eng Phys. 32(9):998–1008. doi:10.1016/2010.06.015.
- Lutin JM, Kornhauser AL, Masce ELL. 2013. The revolutionary development of self-driving vehicles and implications for the transportation engineering profession. Inst Transport Eng J. 83(7):28. 1417586906.
- Park G, Kim T, Crandall JR, Arregui Dalmases C, Luzón Narro BJ. 2013. Comparison of kinematics of GHBMC to PMHS on the side impact condition. Paper presented at: international Research Council on Biomechanics of Injury (IRCOBI); Gothenburg, Sweden; September p. 11–13.
- Perez-Rapela D, Markusic C, Whitcomb B, Pipkorn B, Forman JL, Crandall JR. 2019. Comparison of the simplified GHBMC to PMHS kinematics in far-side impact. Paper presented at: international Research Council on Biomechanics of Injury (IRCOBI); Florence, Italy; September p. 11–13.
- Pipkorn B, Iraeus J, Björklund M, Bunketorp O, Jakobsson L. 2019. Multi-scale validation of a rib fracture prediction method for human body models. Paper presented at: international Research Council on Biomechanics of Injury (IRCOBI); Florence, Italy; September p. 11–13.
- Poulard D, Subit D, Donlon JP, Kent RW. 2015. Development of a computational framework to adjust the pre-impact spine posture of a whole-body model based on cadaver tests data. J Biomech. 48(4):636–643. doi:10.1016/2014.12.050.
- Ramachandra R, Kang YS, Stammen J, Moorhouse K, Murach M, Bolte J, IV, Agnew A. 2019. Evaluation of skeletal and soft tissue contributions to thoracic response of GHBMC M50-O model in dynamic frontal loading scenarios. Paper presented at: international Research Council on Biomechanics of Injury (IRCOBI); Florence, Italy; September p. 11–13.
- Ramachandra R, Pradhan V, Kang Y, Davidson R, Humer M, Zhang J. 2021. Evaluate the effect of seat back restriction on head, neck and torso responses of front seat occupants when subjected to a moderate speed rear-impact. SAE Technical Paper Series, NSF-PAR. ID: 10224828.
- Rohatgi A. 2014. WebPlotDigitizer user manual version 3.4. URL http://arohatgi. info/WebPlotDigitizer/app., 1–18.
- Tadepalli SC, Erdemir A, Cavanagh PR. 2011. Comparison of hexahedral and tetrahedral elements in finite element analysis of the foot and footwear. J Biomech. 44(12):2337–2343. 10.1016/j.jbiomech.2011.05.006. 21742332
- Van Ee CA, Chasse AL, Myers BS. 1998. The effect of postmortem time and freezer storage on the mechanical properties of skeletal muscle. SAE Trans. 107:2811–2820. http://www.jstor.org/stable/44741238.
- Wang ZJ. 2022. Biomechanical responses of the THOR-AV ATD in rear facing test conditions. SAE Int J Adv & Curr Prac in Mobility. 4(6):2089–2105. doi:10.4271/2022-01-0836.
- Wu H, Hou H, Shen M, Yang KH, Jin X. 2020. Occupant kinematics and biomechanics during frontal collision in autonomous vehicles—can rotatable seat provides additional protection? Comput Methods Biomech Biomed Eng. 23(5):191–200. doi:10.1080/10255842.2019.1710496.
- Zeng W, Mukherjee S, Caudillo A, Forman J, Panzer MB. 2021. Evaluation and validation of thorax model responses: a hierarchical approach to achieve high biofidelity for thoracic musculoskeletal system. Front Bioeng Biotechnol. 9:712656. doi:10.3389/fbioe.2021.712656.