
ABSTRACT
Information and communications technology (ICT) has the potential to contribute to the quality of life of older adults. The aim of this study was to analyze the use of a broad array of ICT devices and services among Dutch older adults and to determine whether demographics and health outcomes are associated with this use. A questionnaire was dispensed among a group of Dutch older adults (≥65 years). A univariate analysis of covariance was used to analyse results. Two hundred ninety-one subjects filled out the questionnaire. Reported use of newer technologies was lower compared with older technologies. Increased age (p = 0.048, Confidence Interval [CI]: –0.73: –0.004), lower degree of education (p = 0.008, CI: –59.64: –5.59), birthplace outside of Europe (p = 0.024, CI: –21.99: –0.73), lower income (p = 0.005, CI: –46.44:25.38), less arthrosis of the hands (p = 0.042, CI: –1.38:21.11), and a lower physical functioning (p = 0.008, CI: 1.43:9.41) resulted in a lower ICT use score with an adjusted R2 of 0.311. Older adults are slower to adapt to newer technologies. It appears it is not the degree of physical restrictions, but rather the degree of adaptability to these restrictions that influence the use of ICT.
Introduction
Information and communications technology (ICT) has the potential to ease the performance of tasks for everyone and especially for older adults (in this article, they are defined as 65 years and older). It can enable them to accomplish activities they might otherwise not be able to do on their own, and in turn, increase their quality of life (Czaja, Charness, Fisk, et al., Citation2006; Olson, O’Brien, Rogers, & Charness, Citation2011). However, ICT use is generally higher in younger adults than in older adults (Czaja, Charness, Dijkstra, et al., Citation2006a; Heart & Kalderon, Citation2013; Hernández-Encuentra, Pousada, & Gómez-Zúniga, Citation2009; Olson et al., Citation2011; Vroman, Arthanat, & Lysack, Citation2015), and technology literacy is lower in older adults compared with younger persons (Shelley, Thrane, & Shulman, Citation2004).
Older adults encounter more difficulties in adopting new technologies. They experience physical challenges due to an age-related decline in ability, they can have sceptical attitudes towards the benefits of new technologies, and they encounter difficulties in learning how to use new technologies (Smith, Citation2014). This may be due to a generation-related lack of earlier experience with ICT-based interfaces. Experience with an interaction style during early adulthood, before the age of 25, influences interactions with software interface styles. Older adults are more likely to use technologies that have been available to them for longer periods of time (Docampo Rama, De Ridder, & Bouma, Citation2001). However, there is only limited evidence that older adults cannot or are averse to using technology (Olson et al., Citation2011).
While several U.S. and European studies have looked into the use of a broad array of ICT devices and services by older adults (Heart & Kalderon, Citation2013; Hernández-Encuentra et al., Citation2009; Olson et al., Citation2011; Vroman et al., Citation2015), for Dutch older adults, this remains restricted to the use of the Internet (Akkermans, Citation2013). Internet use in the Netherlands among older adults is high compared to other European countries (80% versus a European Union average of 40%; Akkermans, Citation2013), which might also translate to increased use in other ICT areas.
Demographics such as age and level of education have been shown to influence the use of ICT (Heart & Kalderon, Citation2013; Vroman et al., Citation2015); however, these associations are not always found (Scanlon, O’Shea, O’Caoimh, & Timmons, Citation2015). There are indications that reduced health status can be a barrier to ICT use among older adults (Heart & Kalderon, Citation2013). The associations between various health outcomes with the use of a broad array of ICT devices and services has not been studied, but can be of significance in light of technology-based assistance in health care (eHealth). This relatively new area in health care deploys various forms of ICT to assist with diagnosis, treatment, and self-management of patients. It holds the promise to address the challenges of an aging population (Layzell, Manning, & Benton, Citation2009) by enabling more informed decision making and creating more efficient (and potentially more cost-effective) delivery of care (Internet Innovation Alliance, Citation2011). A considerable amount of (future) users of eHealth are older adults with health issues. Subsequently, the associations between various health outcomes with the use of ICT are important to consider. These results can aid to successfully develop and implement eHealth interventions.
This study aims to analyze the use of a broad array of ICT devices and services among Dutch older adults and to determine whether demographics and health outcomes are associated with this use.
Methods
Questionnaire
The questionnaire used in this study consists of 68 questions and was originally constructed to predict older adults’ willingness to use a specific eHealth technology—namely remote telecare (Chan, Campo, & Esteve, Citation2005; Chan et al., Citation2005). The questionnaire is based on validated questionnaires on health and technology use and has been translated into Dutch from the original English version. A few items were adjusted to make them more suitable for Dutch respondents. The Dutch questionnaire was tested for face and content validity (Antonietti, Barakat, Van Houwelingen, & Kort, Citation2013). This questionnaire can be found in online supplement Appendix 3. In this study, part of the results of this questionnaire is used to find factors associated with ICT use among older adults in the Netherlands. Two authors (AA and SV) used the gerontechnology based literature to independently select those items from the questionnaire that had the potential to be associated with ICT use in older adults. According to the study aim, all of the chosen items refer to demographics or health status. After a comparison, the differences were discussed among the two authors and final decisions made. The final items of the questionnaire used in this study are shown in the second column of the table in online supplement Appendix 2. These items were subsequently used to form the (in)dependent variables.
Sample and recruitment
Recruitment took place in September 2012 and varied for the paper and online versions of the questionnaire. The inclusion criteria were: Dutch citizenship, an age of 65 years or older, and the ability to live independently at home. For the paper version, the subjects were recruited from two senior and/or client organizations, two social senior clubs, five health care organizations, and a senior information day in Utrecht. Older adults were recruited with an information brochure. After recruitment, the paper version of the questionnaire was sent and included a self-addressed, stamped envelope. For the online version, an existing client panel was recruited via email. This client panel consisted of a group of approximately 2,000 older adults who have monthly experience representing a senior population by filling out surveys online.
Ethics
According to the Central Committee on Research Involving Human Subjects (CCMO), filling out a questionnaire generally does not require ethics approval (CCMO, n.d.). Cliëntenbelang Utrecht (an organization that defends the interest of health care clients) approved of the study and provided access to the client panel. Participants filled out a participant slip stating they were willing to take part in the study.
Analysis
Descriptive statistics include frequencies, means, and standard deviations of the variables where appropriate.
Dependent variable: ICT use
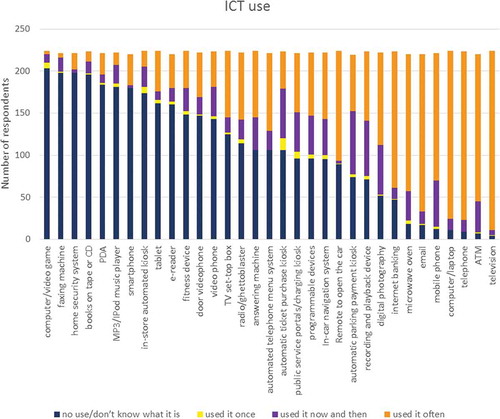
Question 41 (“Please fill out how often you have used the following electronical devices or services in the past year”) was based on the technology experience questionnaire (Czaja, Charness, Dijkstra, et al., Citation2006b) and lists 33 technological devices and services. The respondents enumerated their experience with these items. The scores are as follows: 0: no use/don’t know what it is; 1: used it once; 2: use it now and then; 3: use it often. The scores of the 33 items were summed per respondent. This resulted in a range from 0–99 points on the dependent variable ICT use. The composition of the dependent variable can be found in online supplement Appendix 1. The respondents with more than 10% of missing values in the 33 items (four items or more) were excluded from the analysis. The remaining missing values were replaced with the respondent’s average score (the total average of the 33 items minus the missing items).
Independent variables
To reduce the data and simplify the analyses, the questions that addressed similar concepts were combined into one variable. The composition of each of these independent variables (the formulation of the questions used as well as the calculation of the composite score) can be found in online supplement Appendix 2.
The resultant independent demographic variables are gender (male/female, q.2), age (years, q.3), degree of education (1: no education–4: higher education, q.4), ethnicity (born outside/within Europe, in the Netherlands, q.5a), income (1: <half of Dutch average–7: >3× average, q.8), and employed/volunteer work (yes/no, q.14).
The resultant independent health status variables are perceived general health (1: poor–5: excellent, q.17–19), physical functioning (1: poor–3: good, q.20–21), sight (1: impaired–2: not impaired, q.22–25), hearing (1: impaired–3: not impaired, q.26–29), arthrosis of the hands (1: severe problems–4: no problems, q.30), and support with activities of daily living (ADL support) (1: no support–4: maximal support, q.31,36,38).
A Cronbach’s alpha was used to determine the internal consistency of the pooled items. The variables with a Cronbach’s alpha <0.6 were excluded from analyses due to a lack of internal consistency (Bland & Altman, Citation1997).
A univariate analysis of covariance (ANCOVA) was used to find associations between ICT use and the explanatory, independent variables. The primary model incorporated the independent variables and all of the two-way interactions (e.g., between hearing and age) that had some merit in relation to the study aim. Additionally, whether subjects filled out the questionnaire online or on paper was inserted in the model as a confounder. Subsequently, the non-significant interactions were removed first, and the main factors were removed later, one by one, starting with the highest p-value. Finally, only significant main factors and interactions constitute the final model. The ANCOVA was run using a 5% α-level. To test the validity of the outcome, the residuals were checked for compliance with the normal distribution. The other assumptions of ANCOVA were also verified.
Furthermore, independent t-tests were conducted to analyze the differences between groups (e.g., <70 years old versus ≥70 years old). Analyses were carried out using SPSS (IBM®, PASW Statistics, version 20.0, Chicago, IL, USA) for Windows.
Results
Of the respondents who started the web-based questionnaire (n = 218), 166 completed this version. A total of 73 paper versions of questionnaires were received. The ICT use score for the respondents that filled out the web-based questionnaire was higher than it was for the paper questionnaire respondents (47.9 ± 13.2 versus 39.6 ± 17.8, respectively, p = 0.001). However, the variable “paper or online version” was not significantly associated with ICT use in the ANCOVA model (p = 0.772; CI: –6,4:4,8) and subsequently not seen as a confounder. A total of 14 questionnaires were excluded from the analysis due to more than 10% of missing values in the 33 items of the dependent variable. This resulted in a total number of 225 questionnaires used for analysis. Gender was equally distributed over the respondents, and over half of them still worked or performed volunteer work. A total of 47% of the respondents had completed higher education, 31% received some form of ADL support, 30% perceived their health as worse than average, and 17% scored their physical functioning as being poor. The characteristics of the respondents are summarized in . Additional insight into the distribution of these characteristics is provided in .
Table 1. Subject characteristics; data are presented as frequencies or means ± SD. For composition and clarification of the variables see online supplemental data.
The internal consistency was acceptable to excellent for the combined variables ICT use, perceived general health, physical functioning, hearing, and ADL support (Cronbach’s alphas: 0.852; 0.891; 0.959; 0.725; and 0.787, respectively), but poor for the variable sight (Cronbach’s alpha: 0.346) (Bland & Altman, Citation1997). Removing items from this latter variable increased the Cronbach’s alpha to only 0.449. Hence, instead of the variable sight, the individual items glasses/contacts, glaucoma/cataract, and poor vision were entered in the ANCOVA.
For the dependent variable ICT use, 180 subjects filled out all 33 items (80%). Of all data points (7,425), 94 were missing data (1.27%). ICT use is shown in . We see 18% of the respondents use smartphones, whereas 95% use mobile phones. Computer use is high with 95% of the respondents as well as the use of e-mail, with 92%, whereas a tablet is used by 28%. Within this group of older adults, those who are below the age median (<70 years) reported a significantly higher use of mobile phones (96% versus 93% for the upper age median (≥70 years, p = 0.007), and e-mail (96% versus 90%, p = 0.017).
Figure 1. Subject characteristics. For composition and clarification of the variables see online supplement Appendix 2. Score ranges are as follows: education level (1: no education – 4: higher education, N=223); Income (1: < half of Dutch average – 7: > 3x average, N=185); Perceived general health (1: poor – 5: excellent, N=225); Physical functioning (1: poor – 3: good, N=225); Sight (1: impaired - 2: not impaired, N=225); Hearing (1: impaired – 3: not impaired, N=225); Arthrosis in the hands (1: severe problems - 4: no problems, N=224); ADL support (1: no support – 4: maximal support, N=205).
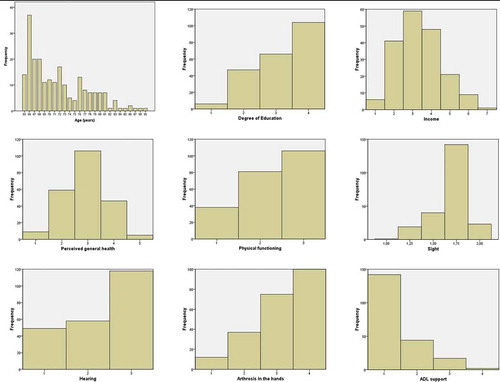
Figure 2. ICT use. Frequency distribution of the use of 33 ICT devices and services among the respondents.
The first ANCOVA did not reveal any significant two-way interactions. The interaction education and income was bordering on significance with p = 0.056. As this is a logical interaction and explained the variance to some degree, this interaction was retained in the model. The respondents with a lower level of education and with an income that was average or lower had a lower ICT use score compared with those who received higher forms of education and had higher incomes.
The final model revealed age, degree of education, income, arthrosis of the hands, physical functioning, and ethnicity were significantly associated with ICT use with an adjusted R2 of 0.311. The results are shown in . The residual plot showed a normal distribution. All remaining ANCOVA assumptions were also met.
Table 2. Factors associated with ICT use in older adults (B = regression coefficients, CI = 95% confidence interval).
For age, we saw with each additional year, the ICT use score diminishes by 0.366 points (out of a total possible score of 99 points). Generally, the respondents with a higher education also had higher ICT use scores. The overall trend with respect to income is that the higher one’s income, the higher their ICT use score turns out to be. For example, the respondents that make <half of average scored 10.53 points lower on ICT use than respondents that make >3× average. The respondents that have more severe arthrosis of the hands have a higher ICT use score than respondents with less or no arthrosis of the hands. Furthermore, a higher physical functioning is associated with a higher ICT use score. Lastly, the respondents who were born outside of Europe on average scored 11.38 points lower on ICT use than natives, whereas those who were born within Europe actually have higher scores than natives.
Discussion
This study aimed to analyze the use of a broad array of ICT devices and services among Dutch older adults and to determine whether demographics and health outcomes are associated with this use. The reported use of newer technologies, such as smartphones and tablets, was considerably lower compared with older technologies, such as computers, e-mail, and mobile phones. Compared with other studies, the use of e-mail, Internet banking, a mobile phone, a personal computer, digital photography, a PDA, and a playback device is high (Heart & Kalderon, Citation2013; Olson et al., Citation2011; Vroman et al., Citation2015). This may be attributed to a higher digital literacy of Dutch older adults compared with older adults in other European countries previously demonstrated by high Internet use in Dutch older adults (≥65 years; Akkermans, Citation2013).
Future studies into technology use should take in mind the fast developments in this field, and adjust questionnaires or other measurement instruments accordingly.
The demographic variables degree of education, income, ethnicity, and age were significantly associated with ICT use, whereas gender and employed and/or volunteer work did not. The health related variables physical functioning and arthrosis of the hands were significantly associated with ICT use in older adults, whereas perceived general health, hearing, sight items (glasses/contacts, glaucoma/cataract, and poor vision), and ADL support were not.
Demographics
We did not find an association between gender and ICT use. Previous studies, similarly, do not always show a gender association with computer use (Wagner, Hassanein, & Head, Citation2010). Generally, subjects with a higher degree of education reported more ICT use than the less educated subjects. Cognitive ability and memory may be underlying factors influencing the amount of ICT use. They have both been shown to be related to years of formal education (Albert et al., Citation1995; Bennett et al., Citation2003; Berry et al., Citation2003). Cognitive ability has been shown to be an important predictor of technology use (Umemuro, Citation2004), and memory appears to be a good predictor of age related differences in digital skills with video and mobile phone interfaces (Docampo Rama et al., Citation2001, Citation2001; Smith, Citation2014). Higher education was previously found to be associated with the use of computers and the Internet (Gell, Rosenberg, Demiris, Lacroix, & Patel, Citation2015; Ingen, De Haan, & Duimel, Citation2007; Smith, Citation2014). Here we see that a higher degree of education is also related to ICT use in the broader sense (the use of various technological devices and services, not restricted to computers and the Internet), whereas this was not found in a recent study (Scanlon et al., Citation2015). Education may be more strongly associated with the use of computers and Internet than ICT use in the broader sense.
More affluent older adults had a higher ICT use score than less affluent ones. Internet access at home has already been shown to be more prominent in older adults with higher levels of income (Smith, Citation2014). Additionally, financial reasons have been mentioned as a limitation to smartphone use in older adults (Mohadisdudis & Ali, Citation2014; Nguyen, Irizarry, Garrett, & Downing, Citation2014). ICT can be quite costly, and the fast developing rate in this area also results in a quick turnover rate of devices and software, causing less affluent persons to be at a disadvantage in this area.
Regarding ethnicity, we see those who were not born in Europe stand out for their low ICT use scores, which are significantly lower compared with those who were born in Europe and the Netherlands. In a study conducted in the Netherlands (Razvi Far, Citation2014), interviews were held with 159 Iranian and Turkish immigrants on the use of e-government services. A total of 22% of the interviewees never used the Internet. In the general Dutch population (including immigrants), this is only 3% (Centraal Bureau voor de Statistiek, Citation2014). Stronger language skills and male gender were related to higher Internet use in Razvi Far’s study (Citation2014). There seems to be quite a bit of variation among ethnic minorities with respect to digital skills. For example, Turkish and Moroccan immigrants are found to have a relatively large disadvantage, whereas Surinamese and Antilleans have skill levels near those of the indigenous Dutch (Ingen et al., Citation2007). The knowledge of the Dutch language and culture may play a role here because in Suriname and part of the Antilles, Dutch is the officially spoken language. However, these studies did not focus solely on older adults, whereas our study did. It may be easier for younger immigrants in the Netherlands to acquire ICT skills as they may have more interactions with Dutch peers and receive information technology lessons at school. Second generation immigrants did indeed have higher digital skills in the study of Ingen et al. compared with first generation immigrants; however, when correcting for age, education, sex, and employment, these differences diminished and the contrast with the indigenous Dutch increased (2007).
The older respondents within this sample of older adults reported less use of ICT. Previous studies showed a reduction in the use of e-mail, sending text messages, and Internet use with increasing age, and similarly within senior groups (Gell et al., Citation2015; Smith, Citation2014; Vroman et al., Citation2015). The results of this study show that, especially with the use of more modern technologies, such as smartphones and tablets, older adults report low use. Within this senior group, those over 70 years old report less frequent use of e-mail and mobile phones than younger respondents. These technologies are again relatively new compared to technologies such as the landline telephone or television, for which no differences within the senior group are apparent. In general, Dutch older adults possess fewer adequate digital skills than their younger counterparts, and they mention a lack of interest and the belief they are too old as reasons for their non-use (Ingen et al., Citation2007). Age-related physical limitations can also contribute to a lower level of ICT use. For example, some major barriers for learning and using the computer and the Internet include the age-related deterioration of visual, perceptual, motor, and cognitive abilities (Xie, Citation2003).
Health outcomes
The respondents with a lower physical functioning score, who are thus hindered in their ADL due to health issues, report less ICT use than those who are not hindered. Interestingly, the amount of support received for ADL was not associated with ICT use. Additionally, it is not the perception of one’s health status (perceived general health) or physical restrictions, but only functional restrictions that influence the use of ICT in this study. Previous studies showed a decreased use of the Internet and smartphones with greater physical impairment (Gell et al., Citation2015; Mohadisdudis & Ali, Citation2014). In both studies, vision impairment as a cause of difficulty in reading is mentioned as one of the barriers. This restriction could greatly restrict the use of ICT, which is mostly screen-based. However, we did not find sight items to be associated with ICT use. There were no respondents who suffered from blindness, so that item could not be used as an independent variable. The other sight problems might have been well enough compensated for in our respondents not to influence their ICT use. This may also be the reason why hearing was not found to be associated with ICT use.
We found older adults without or with less severe arthrosis of the hands had a lower ICT use score. Most ICT devices are hand-operated, which may lead one to assume this would prove problematic for these patients. However, ICT can also compensate for physical restrictions. Algar and Valdes (Citation2014) argued the use of smartphone applications that facilitate neuromuscular control may even serve as a valuable component of a hand therapy program for persons with arthrosis of the hands. Furthermore, the difficulties in using ICT devices due to arthrosis of the hands can be circumvented by devices that can also be operated without using the hands (for example with speech; Kashioka, Citation2012).
User centred design
There has been debate as to whether ICT represents an opportunity or whether it is a cause of exclusion for persons with disabilities (Toboso, Citation2011). This is an important topic in light of the increasing use of technology in health care (e.g., eHealth). There is agreement that ICT can bring such persons innumerable benefits if accessibility is provided (Landers, Citation2013). A “design for all” approach, or a universal design, can address this issue. The approach focuses on finding solutions in the design phase so that, without the need for special adaptations, as many people as possible, regardless of their age and physical functioning, can access products and services (Toboso, Citation2011). This should not be seen as developing products that offer a single solution for everybody, but rather it is a user-centered approach where products can be adjusted depending on an individual’s abilities, skills, and preferences (Emiliani, Citation2009). One example is a tool that can be used when designing new products, which takes into account the formative age of the end user when the use of technologies was first learnt, and the “technology era” in which this occurred (Lim, Citation2010). Another example is a decision tree model that can help understand why older adults with mobility impairments choose (not) to use certain smart technologies (Davenport, Mann, & Lutz, Citation2012).
From the results of this study, it appears it is not the degree of physical restrictions, but rather the degree of adaptability to these restrictions (from older adults) that influence the use of ICT. A more advanced user-centered approach might help older adults with less adaptability to increasingly benefit from the potential of ICT to ease the performance of tasks, enable them to accomplish activities they might otherwise not be able to do on their own, and in turn increase their quality of life.
Limitations
Most of the questionnaires were filled out by subjects that were part of the panel (68%). These persons might have better digital skills compared with the persons that filled out the paper questionnaire, because they have access to the Internet and a computer and complete online questionnaires more often. Their ICT use score was indeed higher, which might have increased the overall ICT use in our respondents compared with the general population. However, there were only 5% of respondents who did not use a computer and 8% that did not use e-mail, which should make this less of a confounder. Being that Internet access in the Netherlands is high among older adults (Akkermans, Citation2013), overall our pool of respondents may still fairly reflect the Dutch older adult population. The subjects of the online panel were slightly younger, higher educated, and worked/volunteered more often. The portion of indigenous Dutch was also higher in this group. However, most importantly, the variable online or paper version was not significantly associated with ICT use in the ANCOVA model and was thus not seen as a confounder.
General conclusions from this study with respect to ethnicity and arthrosis of the hands should be drawn with caution. Firstly, there were only 32 non-native respondents (14%). Secondly, peripheral arthrosis is only seen in a small fraction of the Dutch population (2%; Poos & Gommer, Citation2015), and those who are too disabled to fill out the questionnaire are clearly not represented in our sample.
The predicted variance was not high (R2 was 0.311). Finding factors that are associated with ICT use in older adults is a complex issue, where other variables in addition to demographics and health status also figure in. For example, according to the Telecare Acceptance and Use Model for older adults (Sponselee, Citation2013), perceived benefits are considered to be the key predictor for the use of telecare technologies with accessibility, facilitating conditions, and personal variables as influencing variables. Still, the demographic and health related outcomes that were (not) associated with ICT use provide new insights into which variables should be taken into account to develop successful (eHealth) technologies for older adults.
Conclusion
Older adults are slower to adapt to newer technologies, even within a sample of 65 years and older. Increased age, a lower degree of education, being born outside of Europe, lower income, less arthrosis of the hands, and a lower physical functioning were significantly associated with lower ICT use in older adults. For the development and implementation of technologies for this user group, these variables should be taken into account as influencing factors. Efforts should be made to make these factors less of a barrier to ICT use. This could help in the successful adaptation of new technologies by older adults.
Supplementary_material.zip
Download Zip (196.5 KB)Acknowledgments
A grateful acknowledgement goes to the Foundation Innovation Alliance, SIA RAAK project number: 2010-2-004 INT. Furthermore we would like to thank Dr. Walter Boot for his assistance in developing the questionnaire.
Supplemental Material
Supplemental data for this article can be accessed on the publisher’s website.
Related Research Data
References
- Akkermans, M. (2013). Internetgebruik ouderen fors toegenomen. centraal bureau voor de statistiek. Retrieved from http://www.cbs.nl/nl-NL/menu/themas/vrije-tijd-cultuur/publicaties/artikelen/archief/2013/2013-4005-wm.htm. (Archived by WebCite® at http://www.webcitation.org/6YIPpX3ZG)
- Albert, M. S., Jones, K., Savage, C. R., Berkman, L., Seeman, T., Blazer, D., & Rowe, J. W. (1995). Predictors of cognitive change in older persons: MacArthur studies of successful aging. Psychology and Aging, 10(4), 578–589. doi:10.1037/0882-7974.10.4.578
- Algar, L., & Valdes, K. (2014). Using smartphone applications as hand therapy interventions. Journal of Hand Therapy, 27(3), 254–257. doi:10.1016/j.jht.2013.12.009
- Antonietti, A., Barakat, A., Van Houwelingen, T., & Kort, H. (2013). Remote telecare in an aging Dutch sample: Critical factors predicting their intention to use. In: P. Encarnação et al. (Eds.), Assistive Technology Research Series, 33: Assistive Technology: From Research to Practice (pp. 1229-1234). Amsterdam, The Netherlands: IOS Press. doi:10.3233/978-1-61499-304-9-1229
- Bennett, D. A., Wilson, R. S., Schneider, J. A., Evans, D. A., Mendes De Leon, C. F., Arnold, S. E., … Bienias, J. L. (2003). Education modifies the relation of AD pathology to level of cognitive function in older persons. Neurology, 60(12), 1909–1915. doi:10.1212/01.WNL.0000069923.64550.9F
- Berry, M. J., Rejeski, W. J., Adair, N. E., Ettinger, Jr., W. H., Zaccaro, D. J., & Sevick, M. A. (2003). A randomized, controlled trial comparing long-term and short-term exercise in patients with chronic obstructive pulmonary disease. Journal of Cardiopulmonary Rehabilitation, 23(1), 60–68. doi:10.1097/00008483-200301000-00011
- Bland, J. M., & Altman, D. G. (1997). Cronbach’s alpha. BMJ (Clinical Research Ed.), 314(7080), 572. doi:10.1136/bmj.314.7080.572
- Centraal Bureau voor de Statistiek. (2014). ICT gebruik van personen naar persoonskenmerken. Retrieved from http://statline.cbs.nl/StatWeb/publication/?VW=T&DM=SLNL&PA=71098ned&D1=33,55-59,93-95,97-100,102-104,106-109,112-113,119,124-133&D2=0&D3=0,l&HD=130422-1124&HDR=G2,G1&STB=T. (Archived by WebCite® at http://www.webcitation.org/6Yz02GrCQ)
- Central Committee on Research Involving Human Subjects (CCMO). (n.d.). Does your study have to be reviewed? Retrieved from http://www.ccmo-online.nl/main.asp?pid=10&sid=30&ssid=51
- Chan, M., Campo, E., & Esteve, D. (2005). Assessment of activity of elderly people using a home monitoring system. International Journal of Rehabilitation Research. Internationale Zeitschrift Fur Rehabilitationsforschung. Revue Internationale De Recherches De Readaptation, 28(1), 69–76. doi:10.1097/00004356-200503000-00010
- Czaja, S. J., Charness, N., Dijkstra, K., Fisk, A. D., Rogers, W. A., & Sharit, J. (2006a). Computer and technology experience questionnaire (Technical report no. CREATE-2006-03). Atlanta, GA: Center for Research and Education on Aging and Technology Enhancement (CREATE).
- Czaja, S. J., Charness, N., Dijkstra, K., Fisk, A. D., Rogers, W. A., & Sharit, J. (2006b). CREATE common core battery of measures (Technical report no. CREATE-2006-01). Atlanta, GA: Center for Research and Education on Aging and Technology Enhancement (CREATE).
- Czaja, S. J., Charness, N., Fisk, A. D., Hertzog, C., Nair, S. N., Rogers, W. A., & Sharit, J. (2006). Factors predicting the use of technology: Findings from the center for research and education on aging and technology enhancement (CREATE). Psychology and Aging, 21(2), 333–352. doi:10.1037/0882-7974.21.2.333
- Davenport, R. D., Mann, W., & Lutz, B. (2012). How older adults make decisions regarding smart technology: An ethnographic approach. Assistive Technology, 24(3), 168–181. doi:10.1080/10400435.2012.659792
- Docampo Rama, M., De Ridder, H., & Bouma, H. (2001). Technology generation and age in using layered user interfaces. Gerontechnology, 1(1), 25–40. doi:10.4017/gt.2001.01.01.003.00
- Emiliani, P. L. (2009, January). Technology for the independent living of people with activity limitations (pp. IS9–IS12). In Proceedings of the 2nd International Conference on Biomedical Electronics and Devices, 2009, IS9-IS12. Porto, Portugal.
- Gell, N. M., Rosenberg, D. E., Demiris, G., Lacroix, A. Z., & Patel, K. V. (2015). Patterns of technology use among older adults with and without disabilities. The Gerontologist. 55(3), 412-421. doi:10.1093/geront/gnt166
- Heart, T., & Kalderon, E. (2013). Older adults: Are they ready to adopt health-related ICT? International Journal of Medical Informatics, 82(11), e209–e231. doi:10.1016/j.ijmedinf.2011.03.002
- Hernández-Encuentra, E., Pousada, M., & Gómez-Zúniga, B. (2009). ICT and older people: Beyond usability. Educational Gerontology, 35(3), 226–245. doi:10.1080/03601270802466934
- Ingen, E., De Haan, J., & Duimel, M. (2007). Achterstand en afstand. digitale vaardigheden van lager opgeleiden, ouderen, allochtonen en inactieven. Den Haag, the Netherlands: Sociaal en Cultureel Planbureau.
- Internet Innovation Alliance. (2011). 10 benefits of health IT. Retrieved from http://internetinnovation.org/files/telemed_infographic_palmcard.pdf. (Archived by WebCite® at http://www.webcitation.org/6YcJQaCsv)
- Kashioka, H. (2012). Spoken language communication technology: Overview of spoken language communication technologies. Journal of the National Institute of Information and Communications Technology, 59(3–4), 11–14.
- Landers, S. H. (2013). The case for “connected health” at home. Cleveland Clinic Journal of Medicine, 80(Electronic Suppl. 1), S27–S29. doi:10.3949/ccjm.80.e-s1.06
- Layzell, B., Manning, B., & Benton, S. (2009). The elderly demographic time bomb—sharing the load with the active ageing: Can eHealth technologies help defuse it? Studies in Health Technology and Informatics, 146, 166–170.
- Lim, C. S. C. (2010). Designing inclusive ICT products for older users: Taking into account the technology generation effect. Journal of Engineering Design, 21(2), 189–206. doi:10.1080/09544820903317001
- Mohadisdudis, H. M., & Ali, N. M. (2014, September). A study of smartphone usage and barriers among the elderly. 3rd International Conference on User Science and Engineering (i-USEr; pp. 109–114). Shah Alam, Malaysia. doi:10.1109/IUSER.2014.7002686
- Nguyen, T., Irizarry, C., Garrett, R., & Downing, A. (2014). Access to mobile communications by older people. Australasian Journal on Ageing. doi:10.1111/ajag.12149
- Olson, K. E., O’Brien, M. A., Rogers, W. A., & Charness, N. (2011). Diffusion of technology: Frequency of use for younger and older adults. Ageing International, 36(1), 123–145. doi:10.1007/s12126-010-9077-9
- Poos, M., & Gommer, A. (2015, October 6). Hoe vaak komt artrose voor en hoeveel mensen sterven eraan? Retrieved from http://www.nationaalkompas.nl/gezondheid-en-ziekte/ziekten-en-aandoeningen/bewegingsstelsel-en-bindweefsel/artrose/omvang/ (Archived by WebCite® at http://www.webcitation.org/6c4gXmLpN)
- Razvi Far, A. (2014). Access and use of e-government services: The case of Iranian and Turkish immigrants in the Netherlands. (Unpublished Eindhoven).
- Scanlon, L., O’Shea, E., O’Caoimh, R., & Timmons, S. (2015). Technology use and frequency and self-rated skills: A survey of community-dwelling older adults. Journal of the American Geriatrics Society, 63(7), 1483–1484. doi:10.1111/jgs.13507
- Shelley, M. C., Thrane, L., & Shulman, S. W. (2004). Generational differences in informational technology use & political involvement. Seattle, WA: Digital Government Society of North America.
- Smith, A. (2014). Older adults and technology use. Retrieved from http://www.pewinternet.org/2014/04/03/older-adults-and-technology-use/
- Sponselee, A. (2013). Acceptance and effectiveness of telecare services from the end-user perspective. Eindhoven: Technische Universiteit Eindhoven.
- Toboso, M. (2011). Rethinking disability in Amartya Sen’s approach: ICT and equality of opportunity. Ethics and Information Technology, 13(2), 107–118. doi:10.1007/s10676-010-9254-2
- Umemuro, H. (2004). Computer attitude, cognitive abilities, and technology use among older Japanese adults. Gerontechnology, 3, 64–76. doi:10.4017/gt.2004.03.02.002.00
- Vroman, K. G., Arthanat, S., & Lysack, C. (2015). “Who over 65 is online?” Older adults’ dispositions toward information communication technology. Computers in Human Behavior, 43, 156–166. doi:10.1016/j.chb.2014.10.018
- Wagner, N., Hassanein, K., & Head, M. (2010). Computer use by older adults: A multi-disciplinary review. Computers in Human Behavior, 26, 870–882. doi:10.1016/j.chb.2010.03.029
- Xie, B. (2003). Older adults, computers, and the Internet: Future directions. Gerontechnology, 2(4), 289-305. doi:10.4017/gt.2003.02.04.002.00