
ABSTRACT
It is essential to understand the strategies and processes which are deployed currently across the Assistive Technology (AT) space toward measuring innovation. The main aim of this paper is to identify functional innovation strategies and processes which are being or can be deployed in the AT space to increase access to AT globally. We conducted a scoping review of innovation strategies and processes in peer-reviewed literature databases and complemented this by identifying case studies demonstrating innovation strategies. The review includes WHO world region, publication year, AT type and a sector analysis against the Systems-Market for Assistive and Related Technologies Framework. We analyzed the case studies and interviews using thematic analysis. We included 91 papers out of 3,127 after review along with 72 case studies. Our results showed that product innovations were more prevalent than provision or supply innovations across papers and case studies. Case studies yielded two themes: open innovation (OI); radical and disruptive innovation. Financial instruments which encourage OI are needed and we recommend pursuing OI for AT innovation. Embedding AT within larger societal missions will be key to success governments and investors need to understand what AT is and their translational socioeconomic value.
Introduction
Assistive technology (AT) is the umbrella term for the combination of assistive products (APs) and the services needed to ensure safe assessment, distribution and use of APs. An AP is any physical or digital device which is external to the human body, whose primary purpose is to maintain or improve an individual’s functioning and independence and thereby promote their well-being (WHO, Citation2016). Of the one billion people globally who are in need of AP, it is estimated that nine in ten people do not have access, due to barriers such as cost and availability, broken supply systems, and societies that socially exclude persons with disabilities (WHO, Citation2021). Access to AT is a requisite for inclusion in other domains and the realization of other rights such as access to education, civic life, healthcare, and the labor market (MacLachlan, Banes et al., Citation2018; WHO, Citation2018), and States therefore have an ex-ante duty to ensure accessibility (CRPD, Citation2014).
Despite the cross-cutting nature of APs, they are predominantly understood (both in academic and policy discussions) from health and social perspectives. From these perspectives, APs form a coherent group of products, however as has been demonstrated through the recent product narratives for wheelchairs (AT2030 & ATscale, Citation2019), Prosthetics (AT2030 & ATscale, Citation2020), Digital (AT2030 & ATscale, Citation2020), eyeglasses (AT2030 & ATscale, Citation2020) and hearing aids (AT2030 & ATscale, Citation2019) market dynamics can be different across different categories of products, and individual markets might feature unique barriers and opportunities that affect their ability to thrive. It is also the case that market sectors might transcend product definitions. An example could be digital manufacturing systems which could transform eyeglasses, prosthetics and wheelchairs production. A recently trialed example is the InnovATe wheelchair by Motivation, which leverages digital manufacturing technology to enable local providers to produce bespoke wheelchairs of consistent quality locally, using available materials and components (Barbareschi et al., Citation2020). The core of this technology uses parametric computer assisted design (CAD) model that can be modified according to the measurements, the user’s environment and their preferences (Barbareschi et al., Citation2020). Such fundamental technology can be applied to other technologies for example, walking frames. A second example is the introduction of novel payment schemes such as pay-as-you-go models of mobile money payments. Such payment models have been used in low resource settings to make utilities such as solar energy or water more accessible to people on low incomes, and is currently being trialed in Kenya through the Assistive Technology Impact Fund by HearX to trial making hearing aids affordable and accessible (HearX, Citation2021).
The word innovation is sometimes used quite freely, too widely and without defined limits. However, the Oslo Manual (OECD, Citation2018) has precisely defined innovation for over 25 years. This precise definition has allowed for detailed business sector surveys to be developed and deployed, which then allow for analysis of policy effectiveness and development of new policy to aid sector growth (Gault, Citation2018). Gault (Citation2018) has built on the Oslo Manual definitions to develop a more general definition of innovation which goes beyond the business sector and includes Government, nonprofit and household. This broader definition defines innovation as “the implementation of a new or significantly changed product or process.”
Healthcare systems are complex, adaptive systems, which are socially constructed (Sturmberg, Citation2018). When interventions are implemented to change the system, such complexity means that health systems do not react in a predictable way, but rather “the total of the negotiations, trade-offs, and positioning of stakeholders pulls strongly towards inertia” (Braithwaite, Citation2018). Indeed, systems may be unyielding to change and become “policy resistant” (WHO, Citation2009). Despite such challenges, innovations can operate at multiple levels within this system. This also means that systems can be entered into and changed from different places, in different ways and by different stakeholders. This therefore provides many more possibilities for leveraging change, even in complex systems, including by those who are not centrally situated in the system. Systems thinking is therefore central to innovation.
When applied to healthcare technology, innovations are seen as new services or ways of delivering practice as well as new technologies (Länsisalmi et al., Citation2006). Ultimately, innovations benefit the patient by improving health or reducing suffering or illness (Faulkner & Kent, Citation2001). Innovation for healthcare cuts across the interactions with patients (e.g., how people are seen and heard) as well as how services are provided safely, efficiently, and affordably (Omachonu & Einspruch, Citation2010). Provision is a system that enables the production of products from the assessment of needs to supply of the devices. It also includes the processes of research and development, testing, manufacture, marketing, and distribution. Supply is the process by which APs and parts are delivered from manufacturers to service providers, either through sale or donation (Danemayer et al., Citation2021).
The latest Oslo Manual provides a common, inclusive framework for measuring innovation across the economy from government to nonprofit organizations and households. The manual highlights that an innovation must go beyond the imaginary (beyond the formation of an idea), instead, innovation must materialize and be implemented, though it need not be successful. The resulting social and economic impacts of the innovation depend on its diffusion into society (ibid.). Diffusion of a technology happens through communication across various networks (e.g., within production chains, or among users) and is often analyzed using Roger’s Technology Diffusion Theory (Rogers, Citation1962). When used to analyze AT, the theory found the relative advantage offered by AT and user involvement were key to predicting if a device would be used or discontinued (Riemer-Reiss, Citation1999).
Within this paper we begin the journey toward a method for mapping the innovation ecosystem of AT and investigate whether different types of APs follow different innovation strategies. We answer this question by first analyzing the status of innovation across AT as a whole, using the Systems-Market for Assistive and Related Technologies (SMART) Thinking Matrix which has been developed specifically to show the intersections between the systems level and market characteristics for AT (MacLachlan, McVeigh et al., Citation2018). Through this process we identify innovation strategies and processes which are being adopted in different sectors, different market operation level and across systems level. We conclude with a discussion on the gaps and opportunities followed by recommendations.
Objectives
The overarching aim of this paper is to identify useful and usable innovation strategies and processes which are being or can be deployed in the AT space to increase access to AT globally. In doing this we address the following objectives:
Characterize the landscape of AT innovation
Identify useful and usable innovation strategies and processes which are being or can be deployed in the AT Innovation space
Map characteristics of the innovation strategies to AT types and provide recommendations for how to deploy the innovation strategy most effectively.
Identify gaps in knowledge and practice in the existing literature on AT innovation strategies and processes
Present recommendations for governments and other funders and AT providers to help establish successful innovation strategies for different sectors; and inform the World Report on AT
We will start by exploring key concepts for the AT sector in the Background section. Secondly, we will explain the motivation of this paper. Then we explain the rationale we have used (methodology) to approach the aims. This is followed by a scoping review that was designed with the aim of identifying and reviewing innovation strategies and processes in the AT space to inform future innovation policy, practice, and investment. The literature review complements the analysis presented in our motivation. Then, case studies were identified as demonstrating exemplar innovation strategies through a global call and complemented by those already identified within the AT2030 programme. The data is triangulated into a sector analysis of AT which uses the existing SMART framework for AT.
Methodology
It is essential to understand the strategies and processes which are deployed currently across the AT space toward measuring innovation (OECD, Citation2018). Therefore, we have adapted the general definitions given by the Organization for Economic Co-operation and Development (OECD) to better fit the AT domain (OECD, Citation2015). We have focussed on innovation factors which affect product, supply and provision and have adapted the OECD definitions accordingly. Both the original OECD definitions of Innovation and our adapted definitions of AT innovation are provided in . These new definitions of AT innovation guide our methods.
In our methodological approach, AT is not one single organic sector, but it encompasses multiple sectors. Across these, different innovation strategies are implemented by different actors. Actors can also have multiple roles within the AT systems. Governments can both be large procurers of APs and fund the staff and services which provide the APs to people; however, this function can also be taken on by large non-governmental organizations (NGOs) or multilateral organizations (e.g., UNICEF). Governments also set the policies which dictate not only the health services of a country, but the education, social welfare, transport, and ICT services – and all of these will impact AT diffusion. Furthermore, Governments have the power to set both the direction and velocity of innovation within a country (Mazzucato, Citation2016). Alongside governments are a plethora of other actors from charities to social enterprises, private businesses, and accelerator networks. Given the many actors and many markets which all intersect, it is essential to apply systems thinking to the problem of AT provision (MacLachlan, McVeigh et al., Citation2018).
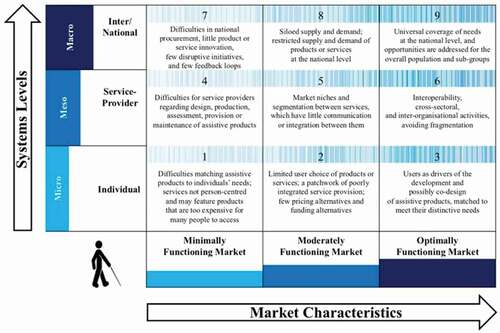
The SMART Thinking Matrix () shows how systems levels and market characteristics interact and contribute toward successful outcomes within the AT sector (MacLachlan, McVeigh et al., Citation2018). At the micro level is the individual. In poorly functioning markets the user experiences a poor fit between their AT and their needs. This is due to a lack of range in affordable product and product feature options, which are provided with a lack of person-centered thinking. In well-functioning markets, the user experiences a wide range of affordable options and both products and service, provisions are user-centered. At the meso level are service-providers and within this level are the following services: manufacturing, distribution, repair and provision. In poorly functioning markets, service providers of AT are unable to reliably gain access to well-designed and manufactured products or to ensure repair when broken. In well-functioning markets, not only are these things present but there is also a level of interoperability across products, and different sectors of the market are working together avoiding fragmentation in services or experience to either the people providing AT or the end users. Finally, at the macro level are the national and international organizations which set the policy and financing infrastructures for AT services. It is important to note that within this matrix, system levels build on each other; the foundational level of this matrix is the individual (micro) level, where the actual needs and contexts of the individuals who will use or benefit from any innovation are defined; without fulfilling those needs within the correct context, service providers and international organizations cannot accomplish a meaningful outcome for individuals. For instance, it is easy to envision a service provider (meso) level creating an AT product that does not fulfil the needs of any individual with a disability, yet still is supported by the international (macro) level and is widely distributed. It is clear that such a situation would represent a failure in the matrix. When this level is functioning well there is universal coverage of AT at a national level and AT users gain impact from having their AT in the form of employment and job opportunities which are inclusive. When not functioning well, there are few feedback loops between the micro, meso and macro levels leading to limited products, no national provision systems and few innovations in products or services.
Figure 1. SMART thinking matrix, source: MacLachlan et al., Citation2018
Research design
There are two distinct studies presented in this paper (see ), each with their own methods. Study 1 is a literature review and case studies. The literature review corpus was identified through two search strings that are relevant to AT and adjacent innovation strategies and processes. The case studies were identified through the AT2030 programme and an open global call.
Table 1. Studies, type of data, topics of data and analysis methods used for each study
Study 2 consists of a reexamination of interviews collected for the product narratives on prosthetics, eyeglasses and digital that were reexamined to unravel the barriers and enablers to innovation in each product area.
Study 1
Study 1 consisted of a standard systematic literature with additional case studies. Additional case studies were added as it was anticipated there would be relatively few published peer-reviewed papers on the topic of innovation strategies and processes pertaining to AT.
Methods
We performed a systematic literature review and identified and collected case studies through the AT2030 programme and an open global call. We utilized familiarization and exploratory data analysis, categorization, higher level categorization, description of corpus through histograms and inductive analysis.
One of the aims of this paper is to understand the strategies and processes which are deployed currently across the AT space and the identification of strategies and processes which could be useful to AT to incorporate to accelerate levels of innovation. As clarity of definition is essential for the measurement of innovation (OECD, Citation2018), we have adapted the general definitions given by the OECD to better fit the AT domain. For the purposes of this review, we have focussed on innovation factors which affect product, supply and provision and have adapted the OECD definitions accordingly. Both the original OECD definitions of Innovation and our adapted definitions of AT innovation are provided in .
Figure 2. Innovation definitions by OECD (product innovation, process innovation, marketing innovation and organizational innovation) and the AT innovation definitions that we have adapted from OECD (innovation, product, supply and provision)
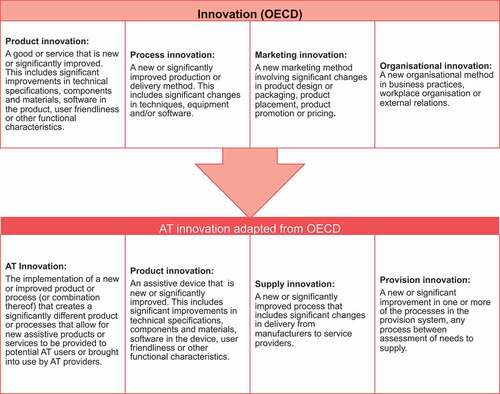
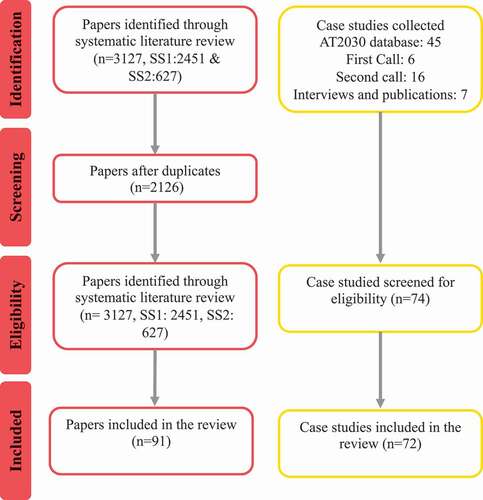
Figure 3. Prisma flow diagram showing the flow of information through the identification, screening, eligibility and inclusion of papers and case studies (Moher et al., Citation2009)
A systematic search was conducted for this paper in June 2020. The search strategy was designed to identify studies reporting innovation strategies and processes being used in an AT sector as well as innovation strategies which had potential for being deployed within the AT sector. The search spanned ten databases: AMED, MEDLINE, EMBASE, Global Health Archive, CINAHL Plus, Cochrane Library, Web of Science, ACM, IEEE and Taylor and Francis (see ).
Our search strings were iteratively developed and informed by preliminary test-searches across the ten databases. Our iterations resulted in 2 distinct search strings: the first one which focussed on current AT innovation strategies and the second one which looked to broaden the scope to include adjacent innovation strategies with the potential to be adopted into the AT sector. Search string 1 (SS1) captured papers with reference to innovation strategy and a synonym for assistive technology or business process domain (). Search string 2 captured papers that explored ethos-led innovation strategies that were adjacent but relevant to AT, across frugal innovation, open innovation (OI), philanthropic innovation, inclusive innovation, humanitarian innovation, and social innovation (). The terms for this both the AT innovation and adjacent innovation search strings were developed via consensus over several weeks across the authorship group.
Table 2. Search string 1 used to create a corpus relevant to AT innovation and 2 used to create a corpus relevant to adjacent innovation strategies with potential for adoption in the AT sector
Case studies which had already been collected as part of the AT2030 programme (between Aug 2018 and June 2020) were added to the corpus of literature. These focussed on wheelchairs, prosthetics, eyeglasses, hearing aids and digital. The digital product narrative focusses specifically on three assistive products: mobile phones, screen reading software and augmentative and alternative communication devices. To ensure we had innovations which fall outside of these specific products, we ran a global call for case studies between March and June 2020. The call was distributed through the World Health Organization (WHO) Global Corporation on Assistive technology (GATE) network in a first call (in March) and a second call (in May). The inclusion and exclusion criteria applied to all papers and case studies can be seen in .
Table 3. Inclusion and exclusion criteria used for literature review and case studies
Following deduplication from the literature and case study searches, all included papers underwent a title/abstract screening to identify records relevant to the inclusion criteria. These were then screened by second reviewers and conflicts resolved by a third. Each case study was reviewed by two reviewers and conflicts resolved by a third. Where possible the following characteristics were extracted from full paper reviews and case study reviews: market function level, systems level of innovation operation, WHO world region, publication year, AT domains (e.g., education, health, employment), AT Type (e.g., digital, prosthetics), success definition, evidence of success (yes, partial, not yet), actors (e.g., Government, University), lead actor, innovation strategy, innovation processes, innovation outputs. Case study reviews took the form of reviewing form submissions, along with additional material submitted or held by the AT2030 programme on the case study.
Results
Corpus Characteristics
A total of 3127 unique records were captured in the systematic search. After a broad title/abstract review, 2126 records were identified for a second review. Following a second review of title and abstract only, 91 studies were included in our corpus. A total of 61 conflicts were settled by a third reviewer, demonstrating inter-rater agreement of 95%.
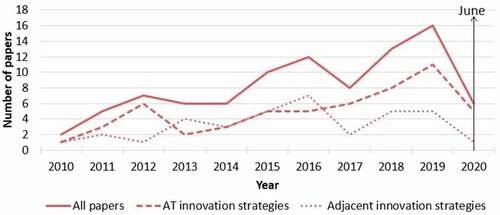
The total number of papers relevant to AT innovation strategies has been increasing over time (See ) rising from 2 in 2010 to 16 in 2019. However, this number is low as an absolute – and reveals a lack of data more generally on the strategies used.
Figure 4. Number of papers in AT innovation strategies, adjacent innovation strategies and a combination of these are presented across time, from 2010 to June 2020
Characteristics from the 91 papers and 73 case studies were then extracted. Given that the sample size of the corpus for case studies (n = 73), adjacent innovation strategies papers (n = 36) and AT innovation strategy papers (n = 55) were different, the percentage relative to the sample size was calculated. In the percentage of case studies, adjacent innovation papers and AT innovation strategy papers are given. Over half the papers from both search strings came from the European region (EURO), followed by the Americas (AMRO) and then the region of the Western Pacific (WPRO). The case studies were differently and more evenly spread with the largest number coming from the African (AFRO) and South East Asia (SEARO) regions followed by the EURO and AMRO regions.
Figure 5. WHO region (EMRO, WPRO, EURO, SEARO, AMRO or AFRO) for AT innovation strategies, adjacent innovation strategies and case studies
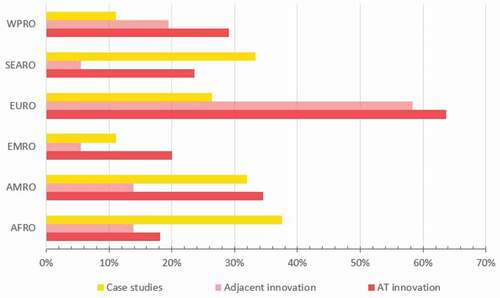
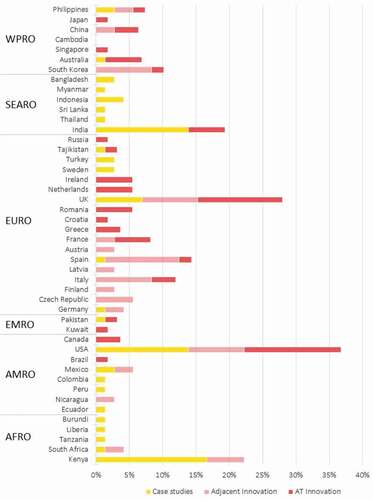
The full break down of percentages of papers and case studies across countries is given in . Case studies of innovation clustered around single countries – in the AFRO region case studies were dominated by Kenya (32%), in the SEARO region India (22%), in the EURO region the UK and in the AMRO sector the USA (). In we also see the papers are dominated by the USA, then UK, Spain, Italy, South Korea.
Figure 6. Countries relevant to AT innovation strategies, adjacent innovation strategies and case studies. Presented also by WHO regions
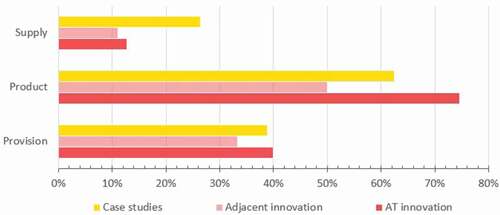
shows the spread of papers and case studies across supply product and provision. The case study data most strongly gave evidence of supply innovations (36%) when compared with papers. AT innovation papers relating to products represented 75% of the corpus. This points to evidence that product innovations do not consider the supply issues during their research, which might in turn lead to products which are unable to reach users as they lack supply routes. It also demonstrates that innovation within supply innovation is ongoing, however, it appears disconnected from academic/published product related research.
Figure 7. Percentage of supply, product and provision for AT innovation strategies, adjacent innovation strategies and case studies
During the abstract and case study review there were repeated discussions on the boundaries of the definitions between procurement, product, supply, and provision. Many innovations overlap, however for the purposes of this paper we chose a core category which is reported in . A second discussion point revolved around the need for a definition of innovation which specifically addresses procurement. We therefore propose the following definitions:
Figure 8. Diagram to visualize the relationships between people, provision, utilization, policy and AT workforce. Examples of processes within provision and utilization are given. R&D: research and development. These processes are just examples, there may be additional processes not included in the diagram

Procurement is a system for the incorporation of technology and includes the following processes: planning, forecasting, identifying needs, sourcing, solicitation of offers, evaluation of offers, review and award of contracts, financing, administration of delivery or installation or commissioning and administration until the end of contracts and until the useful life of the technology.
Provision is a system that enables the production of products from the assessment of needs to supply of the products. It also includes the processes of research and development, testing, manufacture, marketing, and distribution.
Supply is the process by which APs and essential parts are delivered from manufacturers to AP/essential service providers, either through sale or donation.
In the health technology life cycle there are three main components: provision, utilization and acquisition (WHO, Citation2011). However, the GATE initiative has suggested that provision refers to the AT service provision and that people are at the center of policy, provision, products and personnel (WHO, Citation2021). A standard assistive technology life-cycle does not exist’. Yet, taking inspiration from the health technology life cycle, and the 5Ps diagram by the WHO GATE, we think of provision, procurement, supply, utilization, policy and people as shown in . Assessment of need, research and development (R&D), manufacture, marketing, procurement, and supply are processes within the system of Provision. Training, personnel, maintenance, and refurbishment are processes within the system of Utilization. Provision and utilization are systems that make a Product feasible. Yet, AT workforce and Policy are essential factors that affect or benefit products and are also essentially related to People, that sits above products. Assessment of people with disabilities’ needs and R&D are essential processes within provision and considering them as separate processes from rovision is what we think has led to the manufacture of inappropriate and non-essential AT products in the past. Here we aim to highlight the importance of assessment of needs and R&D toward more effective provision and utilization of AT.
The SMART thinking matrix
We have used this matrix to map the innovation corpus findings in which maps paper number e.g., P01, and case study numbers e.g., C01. A paper or case study is cited within a market functionality-systems square or helps to move from one square to another. There were very few examples of innovation within optimally functioning markets at a national or international (macro) level. However, encouragingly innovation examples entering the top right square tended to cross at least one square. For example, four case studies moved from minimally functioning market to optimally (C02, C10, C12, C19) and a paper 89 (P89) covered innovation across the spectrum of levels and market functionality.
Figure 9. SMART thinking matrix depicting micro, meso and macro system
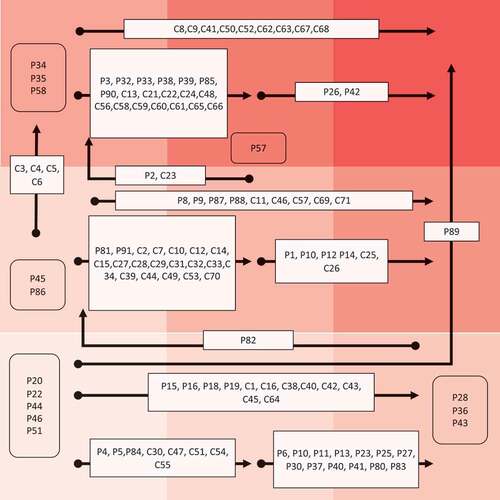
When reading the SMART thinking matrix, a published paper or case study which resides within a square would boost innovation within that level of systems level and market. For example, P57 is the application of a framework to bolster innovation within a moderately functioning market at a macro level. Whereas case studies C33–C36 were digital interventions which had the potential to move from a meso level to macro and from a minimally functioning market to an optimal one. This does not mean that this transformation had occurred, but the innovation strategy and process had the potential to enable this level of progress.
The micro level innovations consisted of papers which reported for example, undergraduate projects (P22). Meso levels included case studies C15–C18 representing accelerators, and C28 a multinational trade body’s disability organization. Macro level contained a number of hearing case studies (C64–C72) were more likely to be implemented at the macro level (C64–C69) or meso level (C70–C72). Eyeglasses (C50–C63) were more likely to be at a meso level (C51-55, C57-C60). Prosthetics were more mixed (C38–C46). The full table along with details of innovation case studies described under lead actor clusters is given in the supplementary material.
The overall picture is one where there is plenty of case study and published evidence of best practice in enabling the acceleration of innovation. However, very little makes it to the optionally functioning market at a macro level. This speaks both to the lack of optimally functioning markets. However, there are good examples e.g., digital C33 – C36 and mobility option P89 which demonstrate the ability to jump levels and enable markets to operate optimally whilst providing a systematic solution.
Innovation strategies and processes
An innovation strategy is a plan of action designed to achieve an agreed innovation aim. An innovation process is a series of actions or steps that take place to achieve innovation. The different innovation strategies found in the corpus are given in and the innovation process are shown in . The literature on AT innovation was dominated by product innovation as a strategy (61%) and social innovation (58%). This contrasted with papers from the adjacent AT space (8% product, 16% social) and case studies (28% product, 16% social). Case studies tended to be focussed on service (80%) and process innovations (59%). Only 2% of AT innovation papers (search string 1) were on business models, compared to 42% of adjacent innovation publications (search string 2) and 33% of case studies.
Figure 10. Innovation strategies identified in AT innovation, adjacent innovation, and case studies
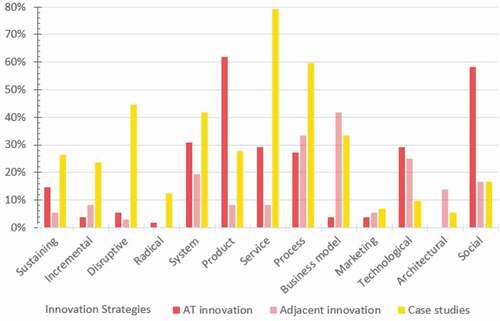
Figure 11. Innovation processes identified in AT innovation, adjacent innovation, and case studies
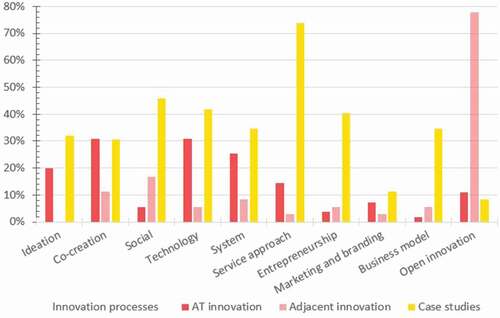
The innovation process (in ) shows 78% of adjacent to AT papers focussed on open innovation. This was to some extent expected given the definition of search string 2. However, what was noteworthy was the small number of AT innovation papers which mentioned open innovation (11%) or the number of case studies which identified open innovation as a strategy (7%). A general theme identified throughout each case study was the process of user centered design, the value of stakeholder networks and how knowledge is created and disseminated at all levels of the innovation process within all contexts and settings, leading to positive outcomes. This was infused into different strategies: co-creation, social, technology, system and service approaches.
Domains and actors
For AT type, the AT innovation literature focused on multiple types at once (35%), then mobility (22%) and followed by enabling digital technology with 20%. Within mobility, wheelchairs (11%),: prosthetics (6%); orthotics (4%), walking aids (2%) were included. Digital and AAC devices (14%), robotics (4%) and AI (2%) are some examples of what we included within enabling digital technology. AT innovation papers focused on AT types relevant to communication (7%) and environment (5%) also but much less on cognition (2%). There were no published papers on hearing and vision innovation processes and strategies. Case study data was differently spread with vision representing 19% of cases and hearing 12%. Mobility devices together accounted for 30% of the remaining case studies: from wheelchairs (12%), prosthetics (15%), orthotics (3%). The remaining case studies were based on digital (6%) and associated products: ICT (6%), Mobile applications (10%), AAC devices (3%); which were then grouped as enabling digital technology and together representing 20% (see ) No case study focused on Cognition.
Figure 12. AT domain and type for AT innovation papers and case studies. ADLs: activities of daily living
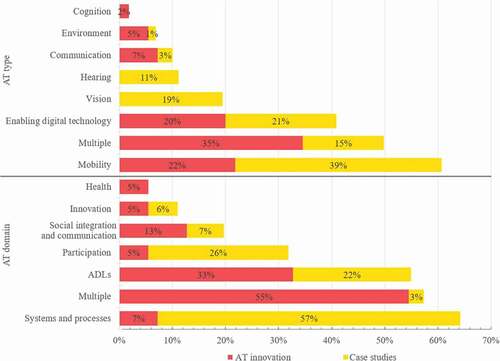
For AT domain the most frequent papers related to multiple domains (54%), followed by activities of daily living (ADLs) (32%), then social integration and communication (13%) followed by innovation and participation both at 5%. Several case studies also reported on ADLs (22%). However, the most frequent domain was related to systems and processes(57%) followed by participation (26%). Innovation and multiple domains were also represented in the case studies with 5% and 3% respectively. No case study focused on Health.
In the various actors and lead actors for the papers and case studies reviewed are shown. When the case studies and papers are taken together, the university sector is the lead actor (62%), followed by NGOs (38%), then Government (32%) and in some instances specific country (30%) interventions through a consortium of lead partners. The evidence for University led came from across AT innovation papers and case studies, whereas case studies only supported lead actor status of NGOs and specific country initiatives came from the adjacent to AT field.
Figure 13. Actors (left) and lead actors (right) found in AT innovation and adjacent innovation strategies papers and case studies
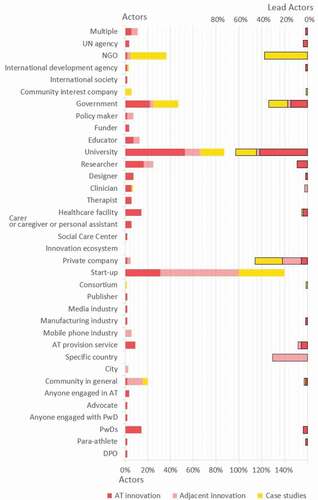
The Start-up community were never a lead actor but were present in many initiatives and were a part of 40% of case studies, 68% of adjacent to AT papers and 30% of AT innovation papers. The University sector was also well represented within case studies (22%) and AT innovation papers (50%), though fewer adjacent to AT innovation papers noted an active role of the universities (10%) within the innovation activity reported.
The case studies were further investigated to identify the innovation strategies observed alongside the definitions of success used by each lead actor. These are given in .
Table 4. Lead actors, innovation strategies and definitions of success observed from the selected case studies
Study 2
Study 2 set out to answer the following question: What are the innovation strategies which best overcome (common) barriers and enhance enablers to innovation across the product areas – digital, eyewear and prosthetics in low- and middle-income countries (LMICs)?
Methods
Product specific interviews with manufacturers, entrepreneurs, NGOs, DPOs for three APs: prosthetics, eyeglasses, and digital products were conducted between 2019 and 2020. These product specific interviews were led by the Clinton Health Access Initiative to develop the product narratives for Prosthetics (AT2030 & ATscale, Citation2020) Digital Products (AT2030 & ATscale, Citation2020) . For the purposes of this paper and future peer-reviewed publications these interviews were recorded, transcribed and pseudo-anonymized. Each set of data has been analyzed using thematic analysis (Braun & Clarke, Citation2006). We treated the data sets in a critical realist way to give us a sense of how the case has managed to successfully provide people with disabilities with the required AT solutions in a given context and the nature of barriers they have faced in doing so. During this analysis, we used a flexible and open coding system, allowing us to engage iteratively with the data, which led to the identification of latent patterns or themes. The results were then triangulated across the different AP areas to identify common themes of innovation strategy and processes.
Results
The full analyses of these interviews are being submitted in separate publications. Here we report the themes from each study. Themes go beyond the area of innovation; however, two high-level innovation themes have emerged and are reported here with evidence from across the data sets. These are: 1) Open innovation and 2) Disruptive and radical innovation.
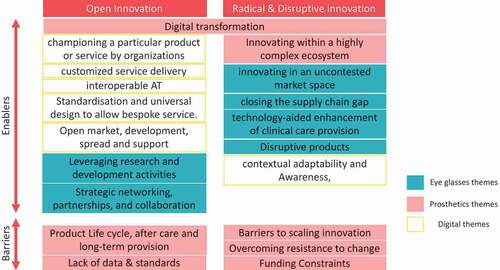
The analysis of the eyeglasses data resulted in seven themes: disruptive products; supply: technology-aided enhancement of clinical care provision; innovating in an uncontested market space; closing the supply chain gap; sustainable, adaptive business models; leveraging research and development activities; strategic networking, partnerships, and collaboration. The analysis of the prosthetic data resulted in five themes: Digital transformation; Innovating within a highly complex ecosystem, Lack of data and standards; Product Life cycle, after care and long-term provision; and barriers to scaling innovation. The last theme had three key subthemes: Lack of perceived value and awareness of potential solutions; Overcoming resistance to change; and Funding Constraints. The analysis of the digital data resulted in three overarching themes: accessing accessible solutions and assistive technology; provision strategies for LMICs and criteria for design. The first theme had four sub-themes: knowing that the solution exists; overcoming the high cost of ownership; becoming digitally literate; accessible content and services. The second theme had three sub-themes: open market, development, spread and support; championing a particular product or service by organizations; customized service delivery. The third theme had three sub themes: universal design first; interoperable assistive technology; contextual adaptability and awareness, standardization and universal design to allow bespoke service.
The following overarching themes were conceptualized: Open innovation, Radical or Disruptive innovation. How these overarching themes relate to the original product themes is shown in .
Figure 14. Themes feeding into overarching themes of open innovation and radical and disruptive innovation for the themes of eyeglasses, prosthetics and digital. Barriers and enablers are presented
Open innovation
Frequently innovation of APs was described as a difficult process due to the highly complex nature of the ecosystem within which prosthetics were delivered. This meant that whilst people might see a user-product fit, they were struggling to prove a product-market fit. P10 states:
“We see a market for it in Africa, but we’ve got to get all those bits right, you’ve got to get the product right. Then you’ve got to get the price point right, then you’ve got to get the supply and distribution right, you’ve got to get the people who use it trained and familiar with it and then you’ve got to convince the service providers, those that have money, and the prosthetists on the ground to fit it, service it, maintain it.” P10
Even when products are innovated well, gaining enough trusted exposure to them as options is a very slow process, during which a small company must stay afloat long enough for revenue to begin to come in.
“The other barrier that we face is just a significantly, painfully long lead time between the invention of something meaningful and the wide scale understanding that it exists.” P05
Open innovation is a process that sees information or knowledge from internal and external sources being used to advance innovation (Chesbrough et al., Citation2014) Such knowledge then is capable of altering business models. Open innovation is not internal, centralized, behind doors research and development. Through open innovation, outside ideas advance businesses. Driven by partnership approaches, we found that strategic networking had enabled innovators in the eye care industry to find “the right” partnership by which to navigate through existing business networks. These partnerships may be with key stakeholders, public/private or internal/external partnerships.
“We’re still testing some other models, but right now we have a few partnerships in place which are already showing signs of big success, where we work very closely with the country representative who then develops the market themselves.” (E2)
At the meso level organizations spoke of acting as champions for a specific service or product. Their experience was steeped in user-frustrations about gaining access to reliable and repairable APs. Charities gathered evidence of the needs and benefits of APs, whilst also actively working to develop a provision system. This involved building the service infrastructure around the device including financing models for users, partnerships with private organizations, requesting government offices to develop content and asking developers to improve the APs.
“All of these (organizations) have to be linked together […]. A lot of work and effort goes in managing the relationship with government institutions. We work with the hope that as we include them, they see the benefits, as they see how things change.” (D4)
Championing was also found at the macro level. We saw examples of how Ministries with remits outside AT provision were empowered to enable change for people with disabilities. For example, in an LMIC, the ICT Ministry under the mandate from the President’s office partnered with big companies to develop e-learning and job matching platforms for people with disabilities, to employ people with disabilities in the booming IT sector of the country. The ministry championed the idea of employment of people with disabilities in ICT and developed all the necessary resources and training modules to accomplish the mission.
Learning: open innovation fosters the entrance and expansion of innovations in the market and partnerships can facilitate start-up or scale-up.
Disruptive and radical innovation
We observed that business model innovation strategies increased access to eyeglasses and disruptive innovation strategies facilitated the delivery of clinical care and dispensation of spectacles. Product innovation of refraction devices facilitated flexible delivery of refraction services. These innovation strategies provide a solution to poor spectacle access, particularly in rural areas and non-clinical settings. For example, one innovator mentioned: “So, what we decided to do was to try to imagine an autorefractor and reimagine it from the ground up” (E3).
In prosthetics, companies were trying to enter nonfunctional markets with radical innovation strategies. However, there was often a resistance to change, this was summed up by a prosthetics interviewee: “the prosthetics community is […] resistant to change of practice and there are sort of received wisdom issues that come up when you try and challenge some of these things. That doesn’t mean they’re set in stone, but you can spend some time having debates about things that may seem less important from an engineering perspective” (P12).
Introducing new technologies and approaches brought regulatory challenges. For example, the ISO standards for prosthetic components only apply to the engineered components not the socket which traditionally is crafted by clinicians: “The ISO standards, actually only officially are applied to the components. The socket was never in the equation until 3-D printing came along.” (P09). A key challenge for introducing new approaches was the “painfully long lead time between the invention of something meaningful and the wide scale understanding that it exists.” (P05). This was in part due to a lack of population data to enable an effective case for investment: “So we need data. We need to collect data. “We’ve been in Cambodia for 26 years and we have no idea how many amputees there are in Cambodia, because nobody will pay for the survey.” (P10). A lack of data could also lead to barriers in changing attitudes of key decision makers, for example, Government or funders who can continue to believe poor quality APs are appropriate when they are in fact not being used: “until you’ve got real world data on whether they’re actually used or not, I think there’s an in-built bias I guess on both parts for the receiver to not upset the donor, and the donor not to want to feel good about themselves.“ (P12).
Within the digital space, automation of sign language captioning brought accessible solutions in local languages and in regions with poor connectivity: “good assistive applications in (country) are in other languages, like English or French and not in our local language and many don’t understand those languages. Other applications are not suitable for the environment, for example, those that use GPS. They don’t work for people in rural areas.” (P15).
Learnings: Disruptive APs are appearing and are often accelerated by digital advances in assessment and manufacture. However, a lack of standards and data are preventing demand creation.
Discussion
As highlighted in this paper, innovation systems themselves are complex systems, involving a collaborative process between several stakeholders including research institutions, companies and universities (Katz, Citation2016). A systems approach is therefore key to understanding and strengthening AT provision and innovation. A systems approach is also needed for AT to be equitably allocated across the population and life course (MacLachlan & Scherer, Citation2018).
It is also important to recognize that a complex system, such as AT provision, “clearly does not change merely because someone devises and then mandates a purpose designed solution … Instead, the system alters over time and to its own rhythm (idiosyncratically and locally)” (Braithwaite, Citation2018). Indeed, due to their complexity, systems may be resistant to change (WHO, Citation2009), and such resistance to change was identified in our findings. For example, path dependence (David, Citation2007) – a prevalent concept in the innovation literature (Kingston, Citation1977) – may be used to explain resistance to change within a system. As noted by (Uusitalo & Lavikka, Citation2020, p. 1), past decisions have “been found to lock organisations onto pathways that constrain future choices and limit their ability to respond to changes.” For instance, path dependency has been used to explain inadequate healthcare policies (Bevan & Robinson, Citation2005).
With this in mind, we look discuss the gaps in innovation strategy and process evidence before looking toward opportunities to strengthen systems for AT innovation.
Gaps in innovation strategy and processes evidence
As identified in Error! Reference source not found. most innovations are occurring within products, with provision and supply being less well documented. Despite high levels of innovation within the product space there are still frustrations of APs making it to the marketplace as is evidenced by the interview data. This tendency for innovations in products to get stuck and fail to make it to the marketplace was also demonstrated by the recent World Intellectual Property Organization’s review of patents across the AT space. WIPO found only 17% of patents are commercialized. This alongside our data points to a sort of Technology Readiness Level (TRL)-level 5 challenge, where ideas get stuck at the proof-of-concept stage. One possible explanation for this is that supply and provision systems are not incorporated into product development, this can lead to incompatibility of the AP to be used within health care settings. Previous work has found for example, that exoskeletons are often not compatible with rehabilitation practices within the UK’s National Health Service (Hill et al., Citation2017). A second explanation is aided by the analysis of the actors who are driving the innovating. In Universities are central to much of the AT innovation presented. Models such as the Grants-Research-Industry-Dissemination (GRID) framework demonstrate the powerful role Universities can play in creating and developing new product innovations to market. The GRID model demonstrates the need for a commercial partner to be on board from the early stages and also for flexibility in funding to ensure an easy pathway from product to market (Sujatha et al., Citation2019). What appears to be clear is that not all product innovations are being created with the GRID principles and are therefore contributing to the poor commercialization rate of APs. Interestingly in the role of universities in adjacent to AT is much diminished and replaced with country-led and start-up initiatives. This demonstrates a lack of a fully connected network of innovation actors to ensure effective innovation activities.
Opportunities for AT innovation
Open innovation
Open Innovation is frequently used as a strategy by adjacent to AT initiatives, however, it appeared lacking from the AT sector as a whole. Open innovation can often be confused with open-source innovation. Open innovation does not mean cost-free; open innovation typically means incentives, such as license fees, would be paid between actors (De Backer & OECD, Citation2008). Open innovation was defined as the use of “purposeful inflows and outflows of knowledge to accelerate internal innovation and expand the markets or external use of innovation respectively“ (Chesbrough et al., Citation2014, p. 1). It has been described as a paradigm shift which assumes internal and external ideas should be used to create innovations within products, supply and provision.
Historically, a well-resourced R&D department provided a required strategic competitive advantage. However, only the largest companies could expedite innovation to market at pace and at scale using this closed innovation approach (Chesbrough, Citation2003). Small- and Medium-Sized Enterprises (SMEs) often lack the speculative R&D capacity, capability and appetite of larger companies (Verbano et al., Citation2013). This is particularly relevant to strategic alliances, favoring universities as a low-risk exposure strategy, rather than venture, IP licensing and partnerships with other firms. SMEs often lack the internal resources to manufacture, market and distribute innovations, and especially during the scale-up required to meet increasing demand and need in the AT sector.
The influence of OI has diversified sectors and allowed smaller companies, and collaborative innovation networks, to gain traction and provide alternatives to larger corporate offerings. In the Assistive Technology sector, this could provide much-needed resilience in a turbulent global industry and a complementary, rather than alternative strategy, to traditional R&D (Lazzarotti & Manzini, Citation2009; Paik & Chang, Citation2015).
Open Innovation can be adopted in many ways and at various parts of an innovation lifecycle, and the collaborative nature of an OI strategy has produced shorter and more meaningful technology development lifecycles (Su et al., Citation2015). This is strategically beneficial for all industry stakeholders. Flor et al. (Citation2019) describe a holistic OI strategy, capitalizing on internal non- and pecuniary outbound resources. They highlight the importance of identifying redundant or stagnant internal innovation that, once made available to external (and/or cross-sector) organizations, can provide value creation within (through partnerships) and beyond (through collaboration) the host organization. The juxtaposition, well presented by Flor et al, is the balance between revealing non-pecuniary innovation to an external environment where competitors may be better placed to exploit. In certain sectors, like AT, the benefits are notable to the recipients of the AT and could form the basis of a OI collaborative strategy that has translational social impact. However, by adopting a pecuniary strategy, this risk is at least minimized by the host organization and the sector at large will benefit.
From an organizational perspective, smaller enterprises, and those with low R&D intensity, are less able to pivot to competition, evolving markets and stakeholder needs (Paik & Chang, Citation2015). Verbano et al. (Citation2013) empirically reported that innovation strategies for SMEs, like the larger organizations reported by Flor et al. (Citation2019), are dependent on their competitive strategy, internal competencies and intensions to grow these competencies with external contributions. This strategy, as with larger organizations, is inextricably linked to the implementation of mechanisms to support OI; where optimal firm performance is linked to strategic integration of external resources and internal competencies. Verbano et al. (Citation2013), importantly, reported that an OI approach was preferred by larger SMEs. This supports the perspective that smaller SMEs are more cautious in their innovation and collaboration strategies, having fewer core competencies and exploitable innovations. However, the evidence of both Flor et al. (Citation2019) and Verbano et al. (Citation2013) indicate that a well-positioned OI strategy, capitalizing on innovation networks and ecosystems (specific to the AT sector and cross-sector), provide a competitive advantage and reflect positively on firm performance. In addition, Paik and Chang (Citation2015) report that both outbound and inbound OI strategies have a positive effect on an organization (specifically, in this case, its technological capabilities). Notably, this study found that coupled OI strategies (embodying both outbound and inbound OI strategies) do not prove to exhibit the same benefits in that industry.
Sectors and missions
We have seen that AT is not a single sector. Instead, it appears as a complex mix of sectors, operating at different systems levels as seen in the SMART matrix (). These sectors are further complicated by different market dynamics. There is an opportunity for cross-sectoral learning to take place. Transitioning to digital methods for refraction index detection could have faced similar issues of needing new standards or overcoming stickiness to evolve culture and clinical practice, which could now be shared with other sectors e.g., prosthetics. Best practice could be developed to better aid technology transfer. The fact that innovation dynamics are different across APs should not come as a surprise. Innovation dynamics differ in different sectors. For example, industries as diverse as vaccines (Azimi et al., Citation2017; Batson et al., Citation2006; Robertson et al., Citation2017) and green technology (Mathews, Citation2017) have managed to demonstrate the ability to shape markets. Within the green economy for example, investment and innovation in solar photovoltaics has led to a year-on-year fall in the cost of associated energy costs which “have been fallen by 28.5 per cent for every doubling of production, which has occurred every two to three years.” (Matthews, Citation2020). Such reductions then make technology affordable which is ripe for pairing with innovative financing models. For example, M-KOPAFootnote1 which leveraged the infrastructure gap in electricity provision in sub-Saharan Africa and the successful uptake of M-PESAFootnote2 (Kenya’s mobile phone-based money transfer service) to propagated solar power as an alternative to traditional energy (kerosene) (Rastogi, Citation2018).
Key to these dynamics have been public investments that “crowded in” or created the market for private investors and users (Mazzucato, Citation2013). Behind the fall of costs are various technological advances in competing solutions that in turn diffuse increasing knowledge around specific products. Yet, what is important from the policy perspective is to understand what kind of public investment (R&D investment, production subsidy, education, etc.) is needed to spur on such innovation dynamics that decrease costs, increase learning, and provide users with better products/services.
AT innovation in and by itself does not make a mission (Albala et al., Citation2021). Instead, AT is key to delivering a host of possible missions and resulting grand challenges. A recent review of a mission approach for AT (Albala et al., Citation2021) highlights how enabling AT access helps deliver against the aging society as well as artificial intelligence and mobility grand challenges of the UK’s Industrial Strategy. Enabling access to AT is also demonstrated as helping to deliver each of the SDGs (Tebbutt et al., Citation2016) and is essential to providing universal health coverage and realizing the Convention on the Rights of Persons with Disabilities, now ratified by 182 countries (UN, Citationn.d.; WHO, Citation2018). For governments and investors to understand the economic and social power of AT it will be essential for AT access to be embedded within these wider challenges (Albala et al., Citation2021). Once embedded, public funds will be needed to tilt the economic playing field to enable AT to be commercialized in a timely fashion and to ensure APs are affordable and available.
A key challenge for AT markets is for a strategic approach to be taken to scaling, not only technology innovation, but also innovation in the processes surrounding it, in the uptake of such innovation, and through service and policy development. Sánchez Rodríguez et al. (Citation2020) reviewed frameworks for scaling social innovation and synthesizing these, identified four directions for scaling. Scaling-up focuses on producing changes in laws, policies, institutions, or norms, to create a more facilitative infrastructure in which innovation can be stimulated and take root. Scaling-down addresses the need to ensure that resources – including funding and skills – are allocated to follow policy downward into the contexts where action is needed for implementation. Scaling-in focuses on the capacity within organizations to move, for instance, form prototyping to larger production. Scaling-out is perhaps how people more generally think of scaling, it is about replicating or broadening availability of a product or service, so that more people, in more places can benefit from it. Crucially, these four directions of scaling are often codependent; when attention focuses only on one direction, it is hindered by a lack of preparation in the other directions. Each direction can be addressed through five phases – identifying, planning, implementing, learning, and adapting – which also anticipates, addresses and assesses the extent to which scaling is inclusive of marginalized groups. These “coordinates of scaling” are therefore consistent with a missions-oriented approach to innovation, working across cognate sectors and interweaving related requirements for an environment of innovation in AT.
Limitations
Our research is limited by how frequently innovation processes and strategies are described by authors, but the systematic review benefitted from the addition of search string 2 which incorporated adjacent AT strategies of innovation. A broader definition of innovation strategies for example, only using “innovation” resulted in too large a corpus to be possible to analyze in time for this background paper. Previous interviews with AT innovators were reexamined and triangulated to narrow the search for innovation keywords. However, future work which investigates a larger corpus of AT-relevant innovation papers would be beneficial to the AT community.
Despite best endeavours to ensure this corpus represented the full spectrum of AT innovation, it is limited in that the reach of the call was in English, and to the AT2030 and WHO’s Global Cooperation on Assistive Technology (GATE), communities and as AT innovation expands, it is probable that AT innovators exist and are unaware of GATE or AT2030. Future work should look to build on our start.
Recommendations
We conclude by presenting recommendations which we see as prerequisites for ensuring healthy AT innovation ecosystems which drive disability inclusion.
Mission-led innovation for AT: Bold missions are proven mechanisms to increase innovation within countries. AT must be embedded into Government missions and resulting grand challenges. For example, to tackle the Aging Society grand challenge the need for AT to be delivered through Universal Health Care would be essential; moreover, policies which reduce import taxes on APs or incentivize innovation of APs would generate growth. Deliberate and strategic approaches to scaling also need to be developed and adapted to market and local circumstances.
Explaining AT: For missions to incorporate AT and for investors to invest in new APs, people need to understand what AT is. Given the heterogeneity of the sector, this requires careful messaging so that the exciting opportunities such as robotics and AI do not overshadow the equally important need for prosthetics or walking aids. Only when Governments and investors understand the sector and the value of the sector will significant change be possible.
Open innovation: Established companies should begin to better engage with start-ups, universities, and other actors in the innovation ecosystem to drive innovation and growth. Agencies and sector bodies have a role to play here in influencing companies to open up, and Governments can also incentivize these collaborations for the greater good of the sector.
Systems strengthening: The link between market characteristics and systems level of AT provision demonstrates the need for strengthening at each level. Understanding the market characteristics of a sector is key to being able to diagnose what type of support is best needed. To do this better data is needed on product availability, provision options and supply chains within each market to provide a better understanding of what would be optimal AT provision systems in a particular context. Initiatives at all levels must include active engagement of end users to be successful.
Finance and expertise: There is a need for investment to help scale viable solutions which are currently stuck at a meso level, often with multiple small-scale demonstrations of a product that fits user needs and a provision model which works. However, supply chains will often vary with scale. To address this, a combination of financial support and expertise to scale is needed. This goes beyond the remit of an accelerator and would help bridge the gap between accelerators and traditional impact or venture capital funding. Financial instruments to help fund initiatives which allow for venture building and scale is needed.
Acknowledgments
We would like to acknowledge all contributors to our global call for case studies in giving their time to share their knowledge and expertise.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Additional information
Funding
Notes
References
- Albala, S., Holloway, C., Austin, V., & Kattel, R. (2021, January 25). New economics of assistive technology: A call for a missions approach | AT2030 programme. UCL Institute for Innovation and Public Purpose. https://www.at2030.org/new-economics-of-assistive-technology:-a-call-for-a-missions-approach/
- AT2030 & ATscale, Savage, M., Afdhila, N., Seghers, F., Frost, R., Fineberg, A. E., Austin, V., & Holloway, C. (2019). Product narrative: Wheelchairs. AT2030, GDI Hub, ATscale. https://www.at2030.org/product-narrative:-wheelchairs/
- AT2030 & ATscale, Savage, M., Bhatnagar, T., Liao, C., Chaudron, M., Boyar, J., Laurentius, D., Torrens, G., Perry, K., Morjaria, P., Ramos Barajas, F., Goedde, B., & Holloway, C. (2020). Product narrative: Digital assistive technology. A market landscape and strategic approach to increasing access to digital assistive technology in low- and middle-income countries. AT2030, ATscale. https://www.at2030.org/static/at2030_core/outputs/Product_Narrative_Digital_Assistive_Technology_a11y.pdf
- AT2030 & ATscale, Chaudron, M., Savage, M., Seghers, F., End Fineberg, A., Goedde, B., Austin, V., Catherine, H., Oldfrey, B., Morjaria, P., & Perry, K. (2020). Product narrative: Eyeglasses. AT2030, ATscale. https://www.at2030.org/product-narrative:-eyeglasses/
- AT2030 & ATscale, Kejariwal, R., Kobayashi, E., Savage, M., Seghers, F., Bhosa, T., End Fineberg, A., Goedde, B., Austin, V., & Holloway, C. (2019). Product narrative: Hearing aids. A market landscape and strategic approach to increasing access to hearing aids and related services in low and middle income countries. AT2030, ATscale, Global Disability Innovaiton Hub. https://www.at2030.org/product-narrative:-hearing-aids/
- Azimi, T., Franzel, L., & Probst, N. (2017). Seizing market shaping opportunities for vaccine cold chain equipment. Vaccine, 35(17), 2260–2264. https://doi.org/https://doi.org/10.1016/j.vaccine.2016.12.073
- Barbareschi, G., Daymond, S., Honeywill, J., Singh, A., Noble, D., Mbugua, N., Harris, N., Austin, I., & Holloway, C. (2020). Value beyond function: Analyzing the perception of wheelchair innovations in Kenya. In The 22nd International ACM SIGACCESS Conference on Computers and Accessibility (pp. 1–14). Association for Computing Machinery. https://doi.org/https://doi.org/10.1145/3373625.3417017
- Batson, A., Meheus, F., & Brooke, S. (2006). Chapter 26: Innovative financing mechanisms to accelerate the introduction of HPV vaccines in developing countries. Vaccine, 24(S3), S219–S225. https://doi.org/https://doi.org/10.1016/j.vaccine.2006.05.042
- Bevan, G., & Robinson, R. (2005). The interplay between economic and political logics: Path dependency in health care in England. Journal of Health Politics, Policy and Law, 30(1–2), 53–78. https://doi.org/https://doi.org/10.1215/03616878-30-1-2-53
- Braithwaite, J. (2018). Changing how we think about healthcare improvement. BMJ, 361(k2014). https://doi.org/https://doi.org/10.1136/bmj.k2014
- Braun, V., & Clarke, V. (2006). Using thematic analysis in psychology. Qualitative Research in Psychology, 3(2), 77–101. https://doi.org/https://doi.org/10.1191/1478088706qp063oa
- Chesbrough, H. (2003). The new imperative for creating and profiting from technology. Harvard Business School Press.
- Chesbrough, H., Kim, S., & Agogino, A. (2014). Chez Panisse: Building an open innovation ecosystem. California Management Review, 56(4), 144–171. https://doi.org/https://doi.org/10.1525/cmr.2014.56.4.144
- CRPD. (2014). General Comment No. 2. Committee on the Rights of Persons with Disabilities. https://www.ohchr.org/en/hrbodies/crpd/pages/gc.aspx
- Danemayer, J., Boggs, D., Smith, E., Delgado Ramos, V. A., Battistella, L., Polack, S., & Holloway, C. (2021). Assistive technology supply and demand. In E. Smith (Ed.), Pub details: RESNA special edition 2021. Rehabilitation Engineering Society of North America (RESNA).
- David, P. A. (2007). Path dependence: A foundational concept for historical social science. Cliometrica, 1(2), 91–114. https://doi.org/https://doi.org/10.1007/s11698-006-0005-x
- De Backer, K, & OECD. Eds. (2008). Open innovation in global networks.
- Faulkner, A., & Kent, J. (2001). Innovation and regulation in human implant technologies: Developing comparative approaches. Social Science & Medicine, 53(7), 895–913. https://doi.org/https://doi.org/10.1016/S0277-9536(00)00389-0
- Flor, M. L., Oltra-Mestre, M. J., & Sanjurjo, E. L. (2019). An analysis of open innovation strategies in firms in low and medium technology industries. IEEE Transactions on Engineering Management,68(3), 853–867. https://doi.org/http://dx.doi.org/10.1109/TEM.2019.2911253
- Gault, F. (2018). Defining and measuring innovation in all sectors of the economy. Research Policy, 47(3), 617–622. https://doi.org/https://doi.org/10.1016/j.respol.2018.01.007
- HearX. (2021). HEARX® becomes the first to receive funding from the assistive technology impact fund. https://hearxgroup.com/blog/HEARX%C2%AE-BECOMES-THE-FIRST-TO-RECEIVE-FUNDING-FROM-THE-ASSISTIVE-TECHNOLOGY-IMPACT-FUND.html
- Hill, D., Holloway, C. S., Ramirez, D. Z. M., Smitham, P., & Pappas, Y. (2017). What are user perspectives of exoskeleton technology? A literature review. International Journal of Technology Assessment in Health Care, 33(2), 160–167. https://doi.org/https://doi.org/10.1017/S0266462317000460
- Katz, J. S. (2016). What is a complex innovation system? PLOS ONE, 11(6), e0156150. https://doi.org/https://doi.org/10.1371/journal.pone.0156150
- Kingston, W. (1977). Innovation: The creative impulse in human progress: Industry, art, science. Calder Publications Limited.
- Länsisalmi, H., Kivimäki, M., Aalto, P., & Ruoranen, R. (2006). Innovation in healthcare: A systematic review of recent research. Nursing Science Quarterly, 19(1), 66–72. https://doi.org/https://doi.org/10.1177/0894318405284129
- Lazzarotti, V., & Manzini, R. (2009). Different modes of open innovation: A theoretical framework and an empirical study. International Journal of Innovation Management, 13(4), 615–636. https://doi.org/https://doi.org/10.1142/S1363919609002443
- AT2030 & ATscale, Liao, C., Seghers, F., Savage, M., Fineberg, A. E., Goedde, B., Austin, V., Holloway, C., & Oldfrey, B. (2020). Product narrative: Prostheses. A market landscape and strategic approach to increasing access to prosthetic device and related services in low-and middle-income countries. AT2030, ATscale. https://www.at2030.org/product-narrative-prostheses/
- MacLachlan, M., Banes, D., Bell, D., Borg, J., Donnelly, B., Fembek, M., Ghosh, R., Gowran, R. J., Hannay, E., Hiscock, D., Hoogerwerf, E.-J., Howe, T., Kohler, F., Layton, N., Long, S., Mannan, H., Mji, G., Odera Ongolo, T., Perry, K., & Hooks, H. (2018). Assistive technology policy: A position paper from the first global research, innovation, and education on assistive technology (GREAT) summit. Disability and Rehabilitation: Assistive Technology, 13(5), 454–466. https://doi.org/https://doi.org/10.1080/17483107.2018.1468496
- MacLachlan, M., McVeigh, J., Cooke, M., Ferri, D., Holloway, C., Austin, V., & Javadi, D. (2018). Intersections between systems thinking and market shaping for assistive technology: The SMART (systems-market for assistive and related technologies) thinking matrix. International Journal of Environmental Research and Public Health, 15(12), 2627. https://doi.org/https://doi.org/10.3390/ijerph15122627
- MacLachlan, M., & Scherer, M. J. (2018). Systems thinking for assistive technology: A commentary on the GREAT summit. Disability and Rehabilitation: Assistive Technology, 13(5), 492–496. https://doi.org/https://doi.org/10.1080/17483107.2018.1472306
- Mathews, J. A. (2017). Global green shift: When ceres meets gaia. Anthem Press.
- Matthews, J. A. (2020, April 1). Greening industrial policy. Globalgreenshift. https://www.globalgreenshift.org/post/greening-industrial-policy
- Mazzucato, M. (2013). The entrepreneurial state: Debunking public Vs. private sector myths. Anthem Press.
- Mazzucato, M. (2016). From market fixing to market-creating: A new framework for innovation policy. Industry and Innovation, 23(2), 140–156. https://doi.org/https://doi.org/10.1080/13662716.2016.1146124
- Moher, D., Liberati, A., Tetzlaff, J., & Altman, D. G. (2009). Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. BMJ, 339(jul21 1), b2535. https://doi.org/https://doi.org/10.1136/bmj.b2535
- OECD. (2015). The innovation imperative: Contributing to productivity, growth and well-being. OECD. https://doi.org/https://doi.org/10.1787/9789264239814-en
- OECD. (2018). Oslo manual 2018: Guidelines for collecting, reporting and using data on innovation.
- Omachonu, V. K., & Einspruch, N. G. (2010). Innovation in healthcare delivery systems: A conceptual framework. Innovation Journal, 15(1), 1–20. https://www.innovation.cc/scholarly-style/2010_15_1_2_omachonu_healthcare-delivery.pdf
- Paik, J., & Chang, H. J. (2015). Post-catch-up strategy for medium-sized South Korean firms: Improving technological capabilities by balancing R&D intensity and open innovation. Engineering Management Journal, 27(4), 164–176. https://doi.org/https://doi.org/10.1080/10429247.2015.1100931
- Rastogi, C. (2018). M-Kopa solar: Lighting up the dark continent. South Asian Journal of Business and Management Cases, 7(2), 93–103. https://doi.org/https://doi.org/10.1177/2277977918774648
- Riemer-Reiss, M. L. (1999). Applying Rogers’ diffusion of innovations theory to assistive technology discontinuance. Journal of Applied Rehabilitation Counseling, 30(4), 16–21. https://doi.org/https://doi.org/10.1891/0047-2220.30.4.16
- Robertson, J., Franzel, L., & Maire, D. (2017). Innovations in cold chain equipment for immunization supply chains. Vaccine, 35(17), 2252–2259. https://doi.org/https://doi.org/10.1016/j.vaccine.2016.11.094
- Rogers, E. M. (1962). Diffusion of innovations. Free Press of Glencoe.
- Sánchez Rodríguez, A. M., MacLachlan, M., & Brus, A. (2020). The coordinates of scaling: Facilitating inclusive innovation. In Systems research and behavioral science, (pp. 1–18). https://doi.org/https://doi.org/10.1002/sres.2740
- Sturmberg, J. (2018, May 22). Is it time to think big – And design a “real health system”? Rapid Response to: Changing How We Think about Healthcare Improvement. BMJ. https://www.bmj.com/content/361/bmj.k2014/rr-1
- Su, C.-Y., Lin, B.-W., & Chen, C.-J. (2015). Technological knowledge co-creation strategies in the world of open innovation. Innovation, 17(4), 485–507. https://doi.org/https://doi.org/10.1080/14479338.2016.1159526
- Sujatha, S., Bapat, G. M., & Dash, S. S. (2019). GRID: A model for the development of assistive devices in developing countries. Disability and rehabilitation: Assistive technology, 16(3), 317–323. https://doi.org/https://doi.org/10.1080/17483107.2019.1673838
- Tebbutt, E., Brodmann, R., Borg, J., MacLachlan, M., Khasnabis, C., & Horvath, R. (2016). Assistive products and the Sustainable Development Goals (SDGs). Globalization and Health, 12(1), 6. https://doi.org/https://doi.org/10.1186/s12992-016-0220-6
- United Nations (UN). (n.d.). Convention on the rights of persons with disabilities (CRPD). Retrieved September 8, 2021, from https://www.un.org/development/desa/disabilities/convention-on-the-rights-of-persons-with-disabilities.html
- Uusitalo, P., & Lavikka, R. (2020). Overcoming path dependency in an industrialised house-building company through entrepreneurial orientation. Buildings, 10(3), 1–22. https://doi.org/https://doi.org/10.3390/buildings10030045
- Verbano, C., Crema, M., & Venturini, K. (2013, July 1–3). Connecting strategy, open innovation and performance in SMEs. EDULEARN13 Proceedings, 232–241, Barcelona, Spain. https://www.researchgate.net/publication/260770513_CONNECTING_STRATEGY_OPEN_INNOVATION_AND_PERFORMANCE_IN_SMES
- WHO. (2009). Systems thinking for health systems strengthening. https://www.who.int/alliance-hpsr/systemsthinking/en/
- WHO, Ed. 2011. Procurement process resource guide. World Health Organization.
- WHO. (2016). Priority assistive products list. World Health Organization. https://apps.who.int/iris/bitstream/handle/10665/207694/WHO_EMP_PHI_2016.01_eng.pdf?sequence=1
- WHO. (2018). Assistive technology. https://www.who.int/news-room/fact-sheets/detail/assistive-technology
- WHO. (2021, January 18). Policy brief: Access to assistive technology. https://www.who.int/publications-detail-redirect/978-92-4-000504-4