
ABSTRACT
To explore global trends in manual wheelchair service provision knowledge across geographic, professional, and socioeconomic domains. A secondary analysis of a dataset from the International Society of Wheelchair Professionals’ Wheelchair Service Provision Basic Knowledge Test was conducted. The dataset included test takers from around the world and was extracted from Test.com and International Society of Wheelchair Professionals’ Wheelchair International Network. Participants 2,467 unique test takers from 86 countries. Interventions Not applicable. International Society of Wheelchair Professionals’ Wheelchair Service Provision Basic Knowledge Test. We identified significant inverse associations between pass rate and the following variables: education (high school and some college), test taker motivation (required by academic program or employer), and country income setting (low and middle). There were significant positive associations between pass rate and the following variables: training received (offered by Mobility India or ‘other NGO’), and age group served (early childhood). Global wheelchair knowledge trends related to key variables such as training, occupation, and income setting have been preliminarily explored. Future work includes further validation of the primary outcome measure and recruitment of a larger sample size to further explore significant associations between additional test taker variables.
Introduction
Access to an appropriate wheelchair remains a global challenge where an estimated 115 million people are in need in primarily less-resourced settings (Alqahtani et al., Citation2019; Gowran, Bray et al., Citation2019; Toro-Hernández et al., Citation2019; WHO, Citation2008; World Bank, Citation2018; World Health Organization, Citation2011). When a person receives a wheelchair that is not fit for one’s needs, there is a greater risk of secondary complications related to one’s health, education, employment, community participation, and abandonment of the device (Borg et al., Citation2009; Carver et al., Citation2016; Greer et al., Citation2012; Toro et al., Citation2017; Visagie et al., Citation2016). This is a human rights issue in accordance with the United Nations Convention on the Rights of Persons with Disabilities (UNCRPD) Articles 20 and 26 which guarantee the right to personal mobility and full inclusion and participation in all aspects of life. The lack of trained and qualified personnel to provide wheelchairs is evident across income settings and contributes to this challenge (McSweeney & Gowran, Citation2019a). Several regions, especially less-resourced settings, often lack rehabilitation professionals that require lay health workers to provide assistive devices (Gupta et al., Citation2011). Even in settings where formal professional rehabilitation training programs are available, the amount of wheelchair training provided is variable and insufficient (K Fung et al., Citation2019; KH Fung et al., Citation2017; Toro-Hernández, Alvarez et al., Citation2020; Toro-Hernández, Mondragón-Barrera et al., Citation2020).
Despite the variability in formal training, higher-resourced settings may have more opportunities for continuing education and providers to be recognized. In North America, as an example, there are several organizations like the Rehabilitation Engineering and Assistive Technology Society of North America (RESNA), Clinicians Task Force, and American Occupational Therapy Association that help to bridge the gap through continuing education. Additionally, RESNA’s Assistive Technology Professional (ATP) and Seating and Mobility Specialist (SMS) certifications help to demonstrate competence in analyzing the needs of consumers with disabilities and assisting in the selection of appropriate assistive devices. These organizations also influence policy, and higher-resourced settings may also be more likely to have policies in place, like the United States Assistive Technology Act of 2004, which provides federal funding to improve the provision of assistive technology to individuals with disabilities of all ages. This abundance of resources, guidance, and standards is not the same in many areas of the world, and particularly in less-resourced settings.
To help in addressing this lack of resources and contextual variability of training and service, the World Health Organization (WHO) developed the Guidelines on the Provision of Manual Wheelchairs in Less-Resourced Settings (WHO, Citation2008) and a series of training packages at basic (World Health Organization, Citation2005), intermediate (Khasnabis et al., Citation2013), managers, and stakeholders (Organization WH., Citation2015), and trainers (Munera et al., Citation2017; Organization WH, USAID, Citation2015) levels to support appropriate wheelchair delivery (,; United Nations Convention on the Rights of Persons with Disabilities, Citation2020). Parallel work by non-governmental organizations (NGOs) and researchers resulted in open-source training resources to raise awareness and educate providers, caregivers, and users on appropriate provision and maintenance to increase users’ well-being and engagement (Coolen et al., Citation2004; MacPhee et al., Citation2004; Múnera et al., Citation2019; Rushton et al., Citation2012; Toro et al., Citation2017; Wheelchair Skills Program, Citation2008).
The International Society of Wheelchair Professionals (ISWP) was founded in 2015 through initial investment by the United States Agency for International Development (USAID) to further support and coordinate personnel and organizations involved in the advocacy, delivery, and training of wheelchairs (Goldberg et al., Citation2018). ISWP developed training and assessment materials, including the ISWP Wheelchair Service Provision Basic Knowledge Test (WSPBKT) (Gartz et al., Citation2017), and a personnel certification, aligned with the WHO Guidelines and to complement the WHO wheelchair service training packages (Ardianuari, Goldberg, Pearlman, Schmeler et al., Citation2020a; Burrola-Mendez et al., Citation2019; Burrola-Mendez, Goldberg et al., Citation2018; Burrola-Mendez, Toro-Hernández et al., Citation2018; Gartz et al., Citation2017; Rushton et al., Citation2020). A global Wheelchair Stakeholders’ Meeting in 2018 reaffirmed that competency development of personnel was critical to advancing appropriate wheelchair service (,; Gartz et al., Citation2017; CitationProfessionals IS of W).
To the best of our knowledge, the ISWP WSPBKT (Gartz et al., Citation2016) is the first test, dataset and study that explores trends in wheelchair service provision knowledge on a global scale. The test and dataset have limitations as they were not originally intended for research purposes, including a primary limitation that the test is lacking psychometric properties. However, in addition to being developed by subject-matter experts (a committee of wheelchair service providers, researchers, and trainers with several years of experience across academic and NGO sectors, in addition to one expert in test development and implementation), it is now facilitated by ISWP, and has been adopted by dozens of organizations, including both governmental and non-governmental organizations, as a standard measure of wheelchair service provision knowledge. To date, the test results have not been comprehensively analyzed or published. This data has potential to reveal gaps in knowledge across economic, geographic, and/or professional domains that could motivate additional capacity building to ensure standardized quality of wheelchair services are available to users globally. A capacity building strategy that includes advocacy to support recognition of the profession can result in policy development, refinement, and adoption to better regulate wheelchair personnel and services. This analysis also helps to address the paucity of global data and intersectional trends (e.g., by profession, region, and test domain) that can help raise awareness of the needs in the wheelchair sector and lead to full implementation of the WHO Guidelines, Training Packages, and UNCRPD.
Thus, our research objectives were to explore global trends in wheelchair service provision knowledge, based upon a dataset from the ISWP WSPBKT databases, and determine whether relationships existed between test taker pass/fail status and test taker demographic variables.
Methods
Study design
This study is an exploratory analysis of ISWP WSPBKT data from 2017–2020 to identify global trends in wheelchair service provision knowledge across different demographic variables.
Outcome measure
The ISWP WSPBKT was purposefully developed to be agnostic to context (i.e. relevant across cultures) and to mirror fundamental, basic principles that are described in the WHO Guidelines. The ISWP WSPBKT was piloted and preliminarily validated by subject-matter experts (Burrola-Mendez, Goldberg et al., Citation2018). The open-source test on ISWP’s Wheelchair International Network (WIN) website mirrors the WHO ‘8 steps’ process for providing wheelchairs, and 75 multiple-choice questions are drawn randomly across 7 domains (assessment, fitting, follow-up, prescription, process, production, user training) resulting in a unique exam for each test taker. Since the initial pilot phase and as of September 2020, the test has been translated from English to 14 languages by subject-matter experts and taken 4,785 times by 2,911 unique users in 96 countries (Gartz et al., Citation2016).
The test includes a demographics section that inquires about key variables such as the test taker’s education, profession, and country of origin. Like most tests and any survey, the demographics questions are not required. In this dataset, that resulted in a limitation of a significant amount of missing data and different sample sizes for several key inquiries (e.g., the profession and country of origin variables both have missing data but different sample sizes since not every user chose to respond to the same questions).
Inclusion criteria
Inclusion criteria for the analysis included complete exam in English, Spanish, Romanian, and French; user’s first attempt; and taken between November 1, 2016 – September 30, 2020. Queries were developed for pass/fail status by gender, country income setting, education level, occupation, training received, organization providing training, current service exposure (hours per week serving clients), work setting, age group served, employment status, experience, test taken on weekend (Friday, Saturday, Sunday), language, occurrence (to identify a user’s first attempt), source of attempt (test.com/WIN) and domain performance.
Database
ISWP maintains user and test attempts data in two distinctive databases: test.com and the ISWP Wheelchair International Network (WIN; wheelchairnetwork.org). Test.com was the initial platform used for data collection during the time period (2015–2018) until a new platform, WIN, was designed and developed to offer both training and testing to users in one location. While both test.com and WIN require a unique username and password, WIN also includes a user profile feature with additional demographic queries. For the purpose of this study, all test attempts from both platforms in English, Spanish, Romanian, and French, the most frequently taken languages out of the 15 offered, were exported.
A database was developed in Microsoft Azure (Microsoft Azure, Citation2021) to support the combination and mining of the test.com and WIN test attempts datasets. A single attempt represented a user reference, date and time, elapsed time, score, percentage (i.e., score divided by total score), result (pass/fail/incomplete), test language, and source (test.com or WIN). Moreover, the dataset included 7 test domains (assessment, fitting, follow-up, prescription, process, production, user training) to organize questions. As described above, in both platforms, the test taker randomly received questions per domain for a total of 75 multiple-choice questions out of a larger pool of either 169 (test.com) or 139 (WIN) test questions. The test.com dataset also included 26 unique demographic questions. The WIN dataset included 12 unique demographic questions and 19 demographic queries from user profile data. Eight novel variables were created to combine test.com demographic questions, WIN demographic questions or user profile data as questions or response options were different in the data sub-sets. For example, the novel variable ‘training received’ was created based upon the following question in test.com “Have you completed any wheelchair trainings sponsored by WHO or other organizations specializing in health, disability, or rehabilitation? If yes, list the organizations below.” and query in the WIN user profile “Where did you receive your wheelchair training? Check all that apply (University, NGO, Government organization, Continued-Education in my work setting and others (options to enter text)).”
Analysis
The Tableau Desktop Citation2020.2 platform (Tableau Desktop, Citation2020) and Python version 3.9.0 (Python, Citation2020) were used for descriptive statistics and data visualization, for nullity (missing data) analysis and data pre-processing and modeling, respectively. The nullity analysis aims to check distribution of missing values and the nullity correlation between variables, and was performed using Missingno (Bilogur, Citation2018) package. In the pre-processing step, we cleaned the data, encoded the variables (i.e., converted discrete values to numbers), and selected features (i.e., input variables (e.g., ‘country income setting’ and ‘training received’) that have the strongest relationship with the target variable of pass/fail status). Categorical variables were encoded using the One-Hot encoding scheme where a new binary variable (e.g., labeled as ‘yes’ or ‘no’ for ‘high,’ ‘middle,’ and ‘low’ for the ‘country income setting’ variable) was created for each enclosed category. Modeling was used to determine the relationship between the response (i.e., pass/fail status) and predictor variables. The Statsmodels (statsmodels, Citation2021) package was employed to build the statistical models.
Fisher’s Exact Test (Clarkson et al., Citation1993; Fisher, Citation1970) was utilized first to determine the existence of nonrandom associations between pass/fail status and other categorical variables and was run in R version 4.0.3. Fisher’s Exact Test was preferred for this analysis because of its capability of coping with variables with more than two categories and variables with multiple response categories (i.e., where test takers can provide more than one answer, e.g., education level, occupation, and training received) with expected frequencies of less than five, which would violate the chi-square test’s assumptions.
Logistic regression was used next, in Python version 3.9.0 (Python, Citation2020), to examine the magnitude and direction of the associations between the pass and fail test attempts and all variables’ levels. Logistic regression is appropriate for models that include a significant amount of missing data. Furthermore, logistic regression computes confidence intervals and hypothesis tests for its coefficients (i.e., the strength of the relationship between variables), which helps to determine statistically how well the fitted model represents the data. The data was split randomly into training (i.e., two-thirds of data) and testing (i.e., one-third of data) sets. The former dataset was used for building and tuning the logistic regression model, while the latter dataset was for assessing the model’s performance.
Ethical Approval: This study (STUDY19100169) was approved by the University of Pittsburgh’s Institutional Review Board.
Results
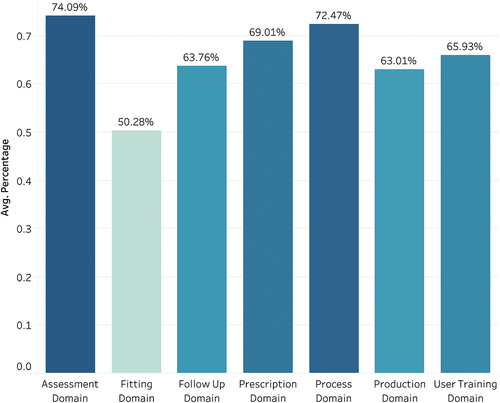
The initial exported dataset resulted in a total of N = 1,768 and N = 2,281 tests from test.com and WIN, respectively. After combining the datasets (a total of N = 4,049) and filtering the data in adherence to the inclusion criteria (i.e., complete exam in English, Spanish, Romanian, and French; user’s first attempt; and taken between November 1, 2016 – September 30, 2020) the revised dataset included test attempt data from N = 2,467 test takers from 86 countries (see frequency and proportion of test takers by WHO region in ). includes the demographic characteristics of test-takers and test results reveal that occupational therapists had a higher pass percentage rate (87%) than any other profession (physical therapy, prosthetics and orthotics, other) sampled. There were more test takers from middle income (68% of sample) than any other income setting, but those in high-income countries passed at the highest rate (78%). presents the domain score averages across all test takers; the highest average scoring domain was assessment (74% questions answered correctly), and the lowest was fitting (50% correct).
Table 1. Test taker frequency and proportion by WHO region.
Table 2. Test taker characteristics and pass/fail rates.
Figure 1. Test domain score averages across all test takers.
In order to conduct additional significance tests, we analyzed missing data. , the nullity matrix, demonstrates dispersion of missing data over variables. Each row and column represent a unique test attempt and variable (i.e. individual demographic question), respectively. Gaps in the columns indicate where a test taker did not respond to an individual demographic question. The difference between totals of the test-taker attempts and the nullity matrix appeared in is due to non-mutually exclusive events (i.e., for a particular question, a test taker may not respond or may select one or more options (e.g., for type of setting(s) the test taker received training)). As can be noticed, there is a weak association between the missing values and the observed ones for some features. For example, as displayed in , only 421 (17%) test-takers reported his or her occupation, and thus, because most of the data are missing (i.e., 2,046 test attempts do not include occupation data), we discarded this feature from the analysis. For other variables which contained missing data but the proportion of missing data was less extreme, we followed a pairwise deletion process where we dropped cases with missing values on analysis-by-analysis basis.
Figure 2. Nullity matrix displaying association between missing and observed values.
Figure 3. Nullity bar chart displaying frequency of missing data across key variables for total sample.
To evaluate associations between the categorical variables (test taker demographic characteristics) and the dichotomous test pass/fail variable, we conducted a Fisher’s Exact Test, resulting in several significant relationships (). In order to determine the magnitude and direction of the association and which levels were significant, we conducted a logistic regression. We chose a stepwise selection approach for the feature selection for the model because it was dependent on p-value and identified a pseudo R-square of .203 (appropriate fit is identified as a range between .20–40) (McFadden, Citation1977). reveals the estimation of the Logistic regression model based on the training set (i.e., 1,238 observations), which has a remarkable performance () on the test set resulting in F1-score of 74%, which is the harmonic mean of the precision (i.e. likelihood of the model predicting the pass status based on select individual demographic characteristics) and recall (i.e. reliability of the model to identify the passed test taker consistently over time). The comparison of the model performance on the training and testing datasets demonstrates that the model is robust.
Table 3. Fisher’s exact test results.
Table 4. Logistic regression results.
Table 5. Logistic regression model performance.
Our logistic regression demonstrates several key results () including significant negative associations (all P ≤ .05) between pass rate and education (high school and some college), motivation (test required by academic program or employer), and country income setting (low and middle). Additionally, were significant positive associations between training received (offered by Mobility India or ‘other NGO’), and age group served (early childhood). There was a nearly significant positive (P = .06) relationship between pass rate and if the test was taken on a Friday, Saturday, or Sunday.
Discussion
Our objective was to identify global trends in wheelchair service provision knowledge across different demographic variables. The results suggest that test-takers with certain demographic characteristics (training participation, country income setting, occupation) were more likely to pass the test than others. Additionally, test takers on average were more likely to pass the Assessment and Prescription domains than other test domains. Our discussion details our inferences from these findings, how the test can elucidate knowledge trends, and potential capacity-building strategies to improve wheelchair service provision knowledge. We also describe the study limitations.
Those who did not receive training were more likely to fail the test
An expected finding was that those who did not receive training were less likely to pass the test. This suggests that wheelchair provision training such as that promoted by the WHO and ISWP (CitationProfessionals IS of W; World Health Organization, Citation2005) is impactful and, in fact, our results suggest that those who reported being trained by an NGO or in particular, Mobility India, a training institution in south India, were more likely to pass the test than those who received training in their work setting or other venue. This is congruent with ISWP’s recommendations that training can improve knowledge related to wheelchairs. Future studies could investigate this finding through further analyses of training modality (e.g., whether online training can result in comparable knowledge gain or influence a particular domain score); whether training received in formal training programs results in similar gains to those provided by NGOs (i.e., more likely to be delivered in a concentrated ‘bootcamp’ style format rather than stretched out over several weeks); and investigate interactions between training and income settings.
We may also infer that those who received training may have been encouraged to take the test by a training organization. In this situation, the test environment may have been accommodating and allowed the test taker to focus. The test taker also may have been provided with verbal instructions and general test-taking strategies. The same holds true for students who passed at a high rate (84%). Our results suggest those with less formal education are more likely to fail, which may also be a result of less digital literacy, and overall multiple-choice test-wiseness strategies (Millman et al., Citation1965). ISWP may consider offering ‘test taking recommendations’ on its website, especially flagged to the attention of test takers with less formal education or who did not receive training.
Most test-takers were from countries designated as ‘middle-income,’ but those in high-income countries pass at the highest rate
Inverse significant relationships between low and middle-income settings and pass rates were found, despite most of the test takers residing in middle-income settings. The greater proportion of test takers from middle-income countries may be due to the users’ awareness of wheelchair sector activities aimed at low- and middle-income countries (LMICs) including those facilitated by WHO (e.g., the Guidelines and Training Packages are both targeted at LMICs) and ISWP. The assistive technology sector is generally less established in LMICs (Matter et al., Citation2017). Test takers from these countries may be less prepared for the test based on decreased access to education (see the association between training and passing the test) or less accustomed to the test format. Our prior work identified that even in higher income settings, wheelchair training is also variable (some programs provide little wheelchair training), but the proliferation of continuing education may contribute to increased knowledge (Organization WH, Citation2016). This finding is in line with literature that suggests a capacity-building infrastructure and resources related to both pre- and post-professional training are needed in LMICs (Gowran, Goldberg et al., Citation2019; McSweeney & Gowran, Citation2019b; Sugawara et al., Citation2018; Walters et al., Citation2020).
Physical therapists are the most frequent test taker type, but descriptive statistics suggest that occupational therapists may pass more than any other rehabilitation profession sampled
While we do not know whether the association between pass rate and occupation is statistically significant due to the amount of missing data, this finding corresponds with other studies in that occupational therapists (OT) are trained and expected to have knowledge in assistive technology and wheelchairs (Best et al., Citation2015; Kanny & Anson, Citation1998; Robin Jones, Citation2010; Steel et al., Citation2017). Likewise, in the early development of the rehabilitation sector in a given country, physical therapy is often the first developed profession with recognized training programs (Armstrong & Ager, Citation2006; Footer et al., Citation2017; Kay et al., Citation1994). Therefore, there are more physical therapists (PT) worldwide (Organization WH, Citation2017), suggesting a larger pool from which to sample, but if wheelchair service provision may be less commonly in the scope of practice, then it is not surprising that OT may be more likely to pass the test. This finding may warrant organizations that govern the professions to review education and service standards language relating to wheelchairs (McSweeney & Gowran, Citation2019b). This important step and any increased attention to wheelchairs in education and scope of practice may impact both curricula and services across the rehabilitation professions (e.g., PT, O&P) (Fung et al., Citation2017).
The descriptive analysis suggests that test takers scored highest on Assessment and Process Domains
Similarly, further domain performance analysis was challenging in the current dataset due to the uneven number of questions across domains in the test (e.g., test takers received four “follow-up” questions resulting in a ‘failing’ score with only 2 questions answered incorrectly; demonstrates variability). However, the descriptive analysis suggests that test takers score higher on ‘Assessment’ and ‘Process’ domains than in any other category. As both assessment and process tasks may have commonalities across rehabilitation professions (Brown & Greenwood, Citation1999) and services (Skinner & Turner-Stokes, Citation2006) (e.g., interviewing or conducting body measurements; appointment and referral), there may be some preexisting knowledge around these topics that do not require wheelchair-specific knowledge that support a higher score in these domains.
Figure 4. Box and whisker plot of 7 domain scores for total sample.
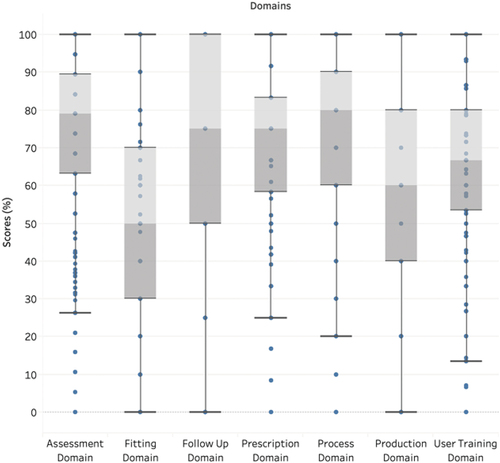
In contrast, the lowest scoring domains of ‘Fitting’ and ‘Follow up’ both require some degree of specialized knowledge including, but not limited to, posture and pressure analysis (Kirkner & Dworak, Citation2008), equipment adjustments (Brienza et al., Citation2010; Brubaker, Citation1986), and maintenance techniques (Morgan et al., Citation2017; Worobey et al., Citation2016). This finding may highlight a lesser degree of knowledge and encourage further emphasis in training as supported in the literature (Kamalakannan et al., Citation2020; McSweeney & Gowran, Citation2019b; Worobey et al., Citation2016). These results also may guide professionals’ continuing education focus.
Key learnings
Our findings can contribute to expanded and improved wheelchair service provision training. The results suggest that there is still an imminent need to make wheelchair service provision training and the ISWP WSPBKT more accessible to other disciplines and individuals with different digital literacy skills around the world. This may include marketing both the training and test in different formats (e.g., paper-based, in-person or remote basic skills tests (Ardianuari, Goldberg, Pearlman, Schmeler et al., Citation2020b)) throughout the ISWP and other professional networks, including those who represent providers who may be underrepresented in the dataset. The lower scores in fitting and follow-up may suggest that more content and time needs to be dedicated to these domains in training.
Study limitations
Our study poses some limitations. First, the test validation to date has presented face and content validity (Gartz et al., Citation2017). As the test was developed by an outside test development agency and prior funding sources, some details are unknown outside of a general consensus process by subject matter experts that determined face validity of the instrument, construct validity (resulting in test domains and the categorization of items), and their weighting. Initial item-level difficulty was determined and based on the results of pilot testing that resulted in questions that were either extremely difficult or easy being removed. However, the test has been organically accepted among many sub-sectors including academia, NGOs, and industry. Trainers and supervisors across several prominent wheelchair-sector organizations have used the test to assist in evaluating their training programs and/or knowledge of service providers in multiple occurrences. Additional validity and reliability evidence will support more confidence in the representation of the findings.
To the best of our knowledge, this study is the first of its kind that compares multi-country wheelchair service provider knowledge. The data presented in this manuscript are a depiction of 4 languages (English, Spanish, French, and Romanian) out of the 15 languages available. While the dataset is sizable and representative of 86 countries, it is still representative of less than half of the countries in the world, and the majority of the test takers were from the Americas. Further analysis of other language versions may represent differing knowledge trends. Additionally, our sample represents organic uptake of the test rather than a systematic process that could be reproduced suggesting that the sample from any one country may not be a random sample of wheelchair service providers and instead be biased toward those engaged in training or other motivating sector activities.
The combination of the two datasets and development of novel variables, though performed systematically and according to best practice, may have resulted in errors that impacted our analysis. Test.com data, unlike WIN, does not have a user profile feature. Although we generated profiles for test.com entries, matched test attempts, and selected the first test attempt manually to ensure validity, the outcomes cannot be fully guaranteed. Some test taker activities may also influence the results. For example, a test taker might fail the test and make another attempt with another account. We manually removed subsequent accounts where noted and only included the first attempt. However, as this was a manual process, a single user with two accounts may have been missed and therefore may have included multiple attempts in the analysis.
Moreover, statistical models, when integrated with qualitative predictors, are confounded with the effects of the number of response choices (i.e., levels, or a high number of answer choices; e.g., name of training organization). Due to the large number of response choices, the predictor levels are represented using ‘dummy’ numerical variables, which leads to a large number of feature variables (i.e., high-dimensional data). To overcome the dimensionality issue, a preferable approach in the future may collapse levels together (e.g., in the case of ‘name of training organization’ collapse to the choices of ‘university,’ ‘NGO,’ ‘industry’). Advanced modeling techniques such as ensemble methods, which utilize multiple learning models, can better learn correlation across levels. However, such approaches may be difficult to interpret.
Conclusion
Global wheelchair provision knowledge trends related to key variables such as training, occupation, and income setting have been preliminarily explored. In the future, we aim to expand this work by conducting additional outcome measure validation, exploring further associations between additional test taker characteristics and pass rates, and linking knowledge outcomes to additional outcome measures. The ability to explore interactions between income setting and other key variables, such as professions, was limited in the current dataset but will be possible to do as it expands in the future. As part of this effort, we may explore outreach to and training of other health care providers including nurses, community-based rehabilitation, and other lay health workers. This will allow for more discrete analyses highlighting the need for advocacy and resource allocation in particular professions and settings beyond rehabilitation.
Future work will also explore the association between provider knowledge and client outcome measures. For example, the ISWP has developed a Minimum Uniform Dataset (Toro-Hernández, Augustine et al., Citation2020) for wheelchair services worldwide with the intent to inform policy, practice, and drive investment. The addition of wheelchair provider characteristics, e.g., whether they have passed the ISWP WSPBKT or received certification (e.g., ISWP Wheelchair Service Provider Certification (CitationProfessionals IS of W)) based on passing the test and receiving training, may prove to be associated with improved client outcomes. This work may result in additional policy efforts to standardize and recognize services at the government level, and the ISWP Wheelchair Service Provider Certification, which uses the ISWP WSPBKT to validate knowledge, may serve as a mechanism for quality assurance and a basis for reimbursement.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Additional information
Funding
References
- Alqahtani, S., Joseph, J., and Dicianno, B. et al. (2019). Stakeholder perspectives on research and development priorities for mobility assistive-technology: A literature review. Disability and Rehabilitation: Assistive Technology 16(4), 1–15. https://doi.org/10.1080/17483107.2019.1650300
- Ardianuari, S., Goldberg, M., Pearlman, J., & Schmeler, M. (2020a, August 29). Development, validation and feasibility study of a remote basic skills assessment for wheelchair service providers. Disability and Rehabilitation: Assistive Technology, 1–11. https://doi.org/10.1080/17483107.2020.1799250
- Ardianuari, S., Goldberg, M., Pearlman, J., & Schmeler, M. (2020b, August 29). Development, validation and feasibility study of a remote basic skills assessment for wheelchair service providers. Disability and Rehabilitation: Assistive Technology. https://doi.org/10.1080/17483107.2020.1799250
- Armstrong, J., & Ager, A. (2006). Physiotherapy in Afghanistan: An analysis of current challenges. Disability and Rehabilitation, 28(5), 315–322. https://doi.org/10.1080/09638280500160337
- Best, K. L., Miller, W. C., & Routhier, F. (2015). A description of manual wheelchair skills training curriculum in entry-to-practice occupational and physical therapy programs in Canada. Disability and Rehabilitation: Assistive Technology, 10(5), 401–406. https://doi.org/10.3109/17483107.2014.907368
- Bilogur, A. (2018). Missingno: A missing data visualization suite. Journal of Open Source Software, 3(22), 547. https://doi.org/10.21105/joss.00547
- Borg, J., Lindström, A., & Larsson, S. (2009). Assistive technology in developing countries: National and international responsibilities to implement the convention on the rights of persons with disabilities. The Lancet, 374(9704), 1863–1865. https://doi.org/10.1016/S0140-6736(09)61872-9
- Brienza, D., Kelsey, S., Karg, P., Allegretti, A., Olson, M., Schmeler, M., Zanca, J., Geyer, M. J., Kusturiss, M., & Holm, M. (2010). A randomized clinical trial on preventing pressure ulcers with wheelchair seat cushions. Journal of the American Geriatrics Society, 58(12), 2308–2314. https://doi.org/10.1111/j.1532-5415.2010.03168.x
- Brown, G. T., & Greenwood, J. (1999). Occupational therapy and physiotherapy: Similar, but separate. British Journal of Occupational Therapy, 62(4), 163–170. https://doi.org/10.1177/030802269906200406
- Brubaker, C. E. (1986). Wheelchair prescription: An analysis of factors that affect mobility and performance. Journal of Rehabilitation R&D, 23(4), 19–26. https://pubmed.ncbi.nlm.nih.gov/3820118/
- Burrola-Mendez, Y., Bonilla-Escobar, F. J., Goldberg, M., Pearlman, J., & Federici, S. (2019). Comparing the effectiveness of a hybrid and in-person courses of wheelchair service provision knowledge: A controlled quasi-experimental study in India and Mexico. PLOS ONE, 14(5), e0217872. https://doi.org/10.1371/journal.pone.0217872
- Burrola-Mendez, Y., Goldberg, M., Gartz, R., Pearlman, J., & Federici, S. (2018). Development of a hybrid course on wheelchair service provision for clinicians in international contexts. PLOS ONE, 13(6), e0199251. https://doi.org/10.1371/journal.pone.0199251
- Burrola-Mendez, Y., Toro-Hernández, M. L., Goldberg, M., Pearlman, J., & Federici, S. (2018). Implementation of the hybrid course on basic wheelchair service provision for Colombian wheelchair service providers. PLOS ONE, 13(10), e0204769. https://doi.org/10.1371/journal.pone.0204769
- Carver, J., Ganus, A., Ivey, J. M., Plummer, T., & Eubank, A. (2016). The impact of mobility assistive technology devices on participation for individuals with disabilities. Disability and Rehabilitation: Assistive Technology, 11(6), 468–477. https://doi.org/10.3109/17483107.2015.1027295
- Clarkson, D. B., Fan, Y., & Joe, H. (1993). A remark on algorithm 643: FEXACT: An algorithm for performing fisher’s exact test in r x c contingency tables. ACM Transactions on Mathematical Software, 19(4), 484–488. https://doi.org/10.1145/168173.168412
- Coolen, A. L., Kirby, R. L., Landry, J., MacPhee, A. H., Dupuis, D., Smith, C., Best, K. L., MacKenzie, D. E., & MacLeod, D. A. (2004). Wheelchair skills training program for clinicians: A randomized controlled trial with occupational therapy students. Archives of Physical Medicine and Rehabilitation, 85(July), 1160–1167. https://doi.org/10.1016/j.apmr.2003.10.019
- Development USAI. World Learning. Wheelchair Stakeholders’ Meeting: Meeting Report. 2018.
- Fisher, R. A. (1970). Statistical methods for research workers. Oliver & Boyd.
- Footer, C. B., Tsegaye, H. S., Yitnagashaw, T. A., Mekonnen, W., Shiferaw, T. D., Abera, E., & Davis, A. (2017). Empowering the physiotherapy profession in Ethiopia through leadership development within the doctoring process. Frontiers in Public Health, 5, 51. https://doi.org/10.3389/fpubh.2017.00051
- Fung, K. H. et al. (2017). Wheelchair service provision education in academia. African Journal of Disability, 6, 340. https://doi.org/10.4102/ajod.v6i0.340
- Fung, K. H., Rushton, P. W., Gartz, R., Goldberg, M., Toro, M. L., Seymour, N., & Pearlman, J. (2017). Wheelchair service provision education in academia. African Journal of Disability, 6, 1–8. https://doi.org/10.4102/ajod.v6i0.340
- Fung, K., Miller, T., and Rushton, P. W. et al. (2019). Integration of wheelchair service provision education: Current situation, facilitators and barriers for academic rehabilitation programs worldwide. Disability and Rehabilitation: Assistive Technology, 15(5), 553–562. https://doi.org/10.1080/17483107.2019.1594408
- Gartz, R., Goldberg, M., and Miles, A. et al. (2016, April 21). Development of a contextually appropriate, reliable and valid basic wheelchair service provision test. Disability and Rehabilitation: Assistive Technology 12(4) , 1–8. https://doi.org/10.3109/17483107.2016.1166527
- Gartz, R., Goldberg, M., and Miles, A. et al. (2017). Development of a contextually appropriate, reliable and valid basic Wheelchair Service Provision Test. Disability and Rehabilitation: Assistive Technology, 12(4), 333–340. https://doi.org/10.3109/17483107.2016.1166527
- Goldberg, M., Pearlman, J., Rushton, P., & Cooper, R. (2018, August 21). The International Society of Wheelchair Professionals (ISWP): A resource aiming to improve wheelchair services worldwide. British Journal of Occupational Therapy 81(12) , 0308022618793056. https://doi.org/10.1177/0308022618793056
- Gowran, R. J., Bray, N., Goldberg, M., Rushton, P., Barhouche Abou Saab, M., Constantine, D., Ghosh, R., & Pearlman, J. (2021). Understanding the global challenges to accessing appropriate wheelchairs: Position paper. International Journal of Environmental Research and Public Health, 18(7), https://doi.org/10.3390/ijerph18073338
- Gowran, R. J., Goldberg, M., and Comanescu, G. et al. (2019). Developing country-specific wheelchair service provision strategic plans for Romania and the Philippines. Disability and Rehabilitation: Assistive Technology, 14(6), 612–627. https://doi.org/10.1080/17483107.2018.1539131
- Greer, N., Brasure, M., & Wilt, T. J. (2012). Wheeled mobility (wheelchair) service delivery: Scope of the evidence. Annals of Internal Medicine, 156(2), 141–146. https://doi.org/10.7326/0003-4819-156-2-201201170-00010
- Gupta, N., Castillo-Laborde, C., & Landry, M. D. (2011). Health-related rehabilitation services: Assessing the global supply of and need for human resources. BMC Health Services Research, 11(1), 276. https://doi.org/10.1186/1472-6963-11-276
- International Society of Wheelchair Professionals (2017). ISWP Home | International Society of Wheelchair Professionals [Online]. http://www.wheelchairnet.org/
- Kamalakannan, S., Rushton, P. W., and Giesbrecht, E. et al. (2020). Wheelchair service provision education for healthcare professional students, healthcare personnel and educators across low- to high-resourced settings: A scoping review protocol. Disability and Rehabilitation: Assistive Technology, 1–7. https://doi.org/10.1080/17483107.2020.1852325
- Kanny, E. M., & Anson, D. K. (1998). Current trends in assistive technology education in entry-level occupational therapy curricula. American Journal of Occupational Therapy, 52(7), 586–591. https://doi.org/10.5014/ajot.52.7.586
- Kay, E., Kilonzo, C., & Harris, M. J. (1994). Improving rehabilitation services in developing nations: The proposed role of physiotherapists. Physiotherapy, 80(2), 77–82. https://doi.org/10.1016/S0031-9406(10)61012-7
- Khasnabis, C., & Mines, K., Organization WH. (2013). Wheelchair service training package: Intermediate level/edited by Chapal Khasnabis and Kylie Mines. World Health Organization
- Kirby RL, Rushton PW, Smith C, Routhier F, Best KL, Boyce J, Cowan R, Giesbrecht E, Kenyon LK, Koontz A, et al. (2019). Wheelchair Skills Program Manual Version 5.0. Halifax, Nova Scotia, Canada: Published electronically at Dalhousie University.
- Kirkner, A., & Dworak, P. (2008). Seeking a proper fit. Rehab Management, 21(8). Pubmed ID: 18972756.
- MacPhee, A. H., Kirby, R. L., Coolen, A. L., Smith, C., MacLeod, D. A., & Dupuis, D. J. (2004). Wheelchair skills training program: A randomized clinical trial of wheelchair users undergoing initial rehabilitation. Archives of Physical Medicine and Rehabilitation, 85(January), 41–50. https://doi.org/10.1016/S0003-9993(03)00364-2
- Matter, R., Harniss, M., Oderud, T., Borg, J., & Eide, A. H. (2017). Assistive technology in resource-limited environments: A scoping review. Disability and Rehabilitation: Assistive Technology, 12(2), 105–114. https://doi.org/10.1080/17483107.2016.1188170
- McFadden, D. (1977). Quantitative methods for analyzing travel behavior of individuals: Some recent developments. Institute of Transportation Studies, University of California.
- McSweeney, E., & Gowran, R. J. (2019a). Wheelchair service provision education and training in low and lower middle income countries: A scoping review. Disability and Rehabilitation: Assistive Technology, 14(1), 33–45.
- McSweeney, E., & Gowran, R. J. (2019b). Wheelchair service provision education and training in low and lower middle income countries: A scoping review. Disability and Rehabilitation: Assistive Technology, 14(1), 33–45. https://doi.org/10.1080/17483107.2017.1392621
- Microsoft Azure. (2021). (Version 21.04) [Computer program]. Microsoft.
- Millman, J., Bishop, C. H., & Ebel, R. (1965). An analysis of test-wiseness. Educational and Psychological Measurement, 25(3), 707–726. https://doi.org/10.1177/001316446502500304
- Morgan, K. A., Engsberg, J. R., & Gray, D. B. (2017). Important wheelchair skills for new manual wheelchair users: Health care professional and wheelchair user perspectives. Disability and Rehabilitation: Assistive Technology, 12(1), 28–38. https://doi.org/10.3109/17483107.2015.1063015
- Munera, S., Goldberg, M., Kandavel, K., & Pearlman, J. (2017). Development and evaluation of a wheelchair service provision training of trainers programme. African Journal of Disability (Online), 6, 1–13. https://doi.org/10.4102/ajod.v6i0.360
- Múnera, S., Pearlman, J., Toro, M., Worobey, L., Boninger, M., & Cooper, R. A. (2019, June 6). Development and efficacy of an online wheelchair maintenance training program for wheelchair personnel. Assistive Technology 33(1) , 1–7. https://doi.org/10.1080/10400435.2019.1619632
- Organization WH, USAID. (2015) . Wheelchair service training of trainers package. World Health Organization.
- Organization WH. (2015). Wheelchair service training package for managers. World Health Organization.
- Organization WH. (2016). Global strategy on human resources for health: Workforce 2030.
- Organization WH. (2017). The need to scale up rehabilitation. World Health Organization.
- Python. (2020). (Version 3.9.0) [Computer program].
- Robin Jones, C. O. T. A. R. O. H. (2010). Specialized knowledge and skills in technology and environmental interventions for occupational therapy practice. The American Journal of Occupational Therapy, 64(6), S44. https://doi.org/10.5014/ajot.2010.64S44
- Rushton, P. W., Fung, K., Gauthier, M., Goldberg, M., Toro, M., Seymour, N., & Pearlman, J. (2020). Development of a toolkit for educators of the wheelchair service provision process: The Seating and Mobility Academic Resource Toolkit (SMART). Human Resources for Health, 18(1), 1–9. https://doi.org/10.1186/s12960-020-0453-6
- Rushton, P. W., Kirby, R. L., & Miller, W. C. (2012). Manual wheelchair skills: Objective testing versus subjective questionnaire. Archives of Physical Medicine and Rehabilitation, 93(12), 2313–2318. https://doi.org/10.1016/j.apmr.2012.06.007
- Skinner, A., & Turner-Stokes, L. (2006). The use of standardized outcome measures in rehabilitation centres in the UK. Clinical Rehabilitation, 20(7), 609–615. https://doi.org/10.1191/0269215506cr981oa
- statsmodels. (2021). (Version 0.12.2) [Computer program].
- Steel, E. J., Buchanan, R., Layton, N., & Wilson, E. (2017). Currency and competence of occupational therapists and consumers with rapidly changing technology. Occupational Therapy International, 2017, 1–5. https://doi.org/10.1155/2017/5612843
- Sugawara, A. T., Ramos, V. D., Tsukimoto, D. R., Pedroso, T. D., & Battistela, L. R. (2018). Building the capacity of wheelchair service providers in the state of Sao Paulo, Brazil. Annals of Physical and Rehabilitation Medicine, 61, e529. https://doi.org/10.1016/j.rehab.2018.05.1231
- Tableau Desktop. (2020). (Version 2020.2) [Computer program]
- Toro-Hernández, M. L., Alvarez, L., Vargas-Chaparro, M. C., & Goldberg, M. (2020). Final year students’ knowledge on basic manual wheelchair provision: The state of occupational therapy programs in Colombia. Occupational Therapy International, 2020, 1–8. https://doi.org/10.1155/2020/3025456
- Toro-Hernández, M. L., Augustine, N., Kankipati, P., Karg, P., Rispin, K., Schein, R. M., Kandavel, K., D’Innocenzo, M. E., Goldberg, M., & Pearlman, J. (2020). Preliminary steps of the development of a minimum uniform dataset applicable to the international wheelchair sector. PLOS ONE, 15(9), e0238851. https://doi.org/10.1371/journal.pone.0238851
- Toro-Hernández, M. L., Kankipati, P., Goldberg, M., Contepomi, S., Tsukimoto, D. R., & Bray, N. (2019). Appropriate assistive technology for developing countries. Physical Medicine and Rehabilitation Clinics, 30(4), 847–865. https://doi.org/10.1016/j.pmr.2019.07.008
- Toro-Hernández, M. L., Mondragón-Barrera, M. A., Torres-Narváez, M. R., Velasco-Forero, S. E., & Goldberg, M. (2020). Undergraduate physiotherapy students’ basic wheelchair provision knowledge: A pilot study in two universities in Colombia. Disability and Rehabilitation: Assistive Technology, 15(3), 336–341. https://doi.org/10.1080/17483107.2019.1580776
- Toro, M. L., Bird, E., Oyster, M. et al. (2017). Development of a wheelchair maintenance training programme and questionnaire for clinicians and wheelchair users. Disability and Rehabilitation: Assistive Technology, 12(8), 843–851. https://doi.org/10.1080/17483107.2016.1277792
- United Nations Convention on the Rights of Persons with Disabilities. (2020). https://www.un.org/development/desa/disabilities/convention-on-the-rights-of-persons-with-disabilities.html
- Visagie, S., Mlambo, T., Van der Veen, J., Nhunzvi, C., Tigere, D., & Scheffler, E. (2016). Impact of structured wheelchair services on satisfaction and function of wheelchair users in Zimbabwe. African Journal of Disability, 5(1). https://doi.org/10.4102/ajod.v5i1.222
- Walters, R., Britz, M., & Van der Westhuizen, E. (2020). Disability inclusion in the Northern Cape: A community-based wheelchair service project. South African Health Review, 2020(1), 147–153. https://www.hst.org.za/publications/South%20African%20Health%20Reviews/SAHR_Chapter%2015_15122020_Final.pdf
- WHO. (2008). Guidelines on the provision of manual wheelchairs in less resourced settings.
- World Bank. (2018.). Disability inclusion. Published. http://www.worldbank.org/en/topic/disability
- World Health Organization. (2005). Wheelchair service training package - Basic level. Retrieved May 5, 2015, from http://www.who.int/disabilities/technology/wheelchairpackage/en/
- World Health Organization. (2011). World report on disability 2011.
- Worobey, L., Pearlman, J., Dyson-Hudson, T., & Boninger, M. (2016). Clinician competency with wheelchair maintenance and the efficacy of a wheelchair maintenance training program. Archives of Physical Medicine and Rehabilitation, 97(10), e55. https://doi.org/10.1016/j.apmr.2016.08.165