
Abstract
Phenomenon: This study aimed to investigate how students can develop their understanding of trauma biomechanics by means of technology-enhanced learning—an interactive visualization tool developed to enhance understanding of the biomechanics underlying an injury via dynamic imaging sequences. Approach: Students were invited to explore the content as a learning resource during an interprofessional clinical placement on an orthopedic ward. Thirty volunteer medical, nursing, and physiotherapy/occupational therapy students participated in 10 interprofessional groups of three participants. They were video recorded while interacting with learning software that was divided into five sections: Work Up, General Information, Biomechanical Case Study, Biomechanical Risk Assessment, and Treatment. Investigators probed students’ learning experiences via four focus group discussions. A sociomaterial perspective was adopted, directing the analytical focus to how students’ made use of talk, gestures, bodies, and material objects to understand the visualized phenomena. Findings: When connecting the visualization to a patient case, certain features of the technology stood out as important for promoting engagement and understanding trauma mechanisms. Decreased tempo, showing the directions and dynamics of trauma biomechanics in slow-motion, and color coding of the strain on the affected structures were especially important for evoking the emotional responses. The visualization tool also supported students’ explorations of causal relationships between external forces and their biomedical effects. These features emphasize the sociomaterial relation between the design of the technology and the student activities. Insights: Dynamic visualization of biomechanical events has the potential to improve the understanding of injury mechanisms and specifically to identify anatomical structures at high risk of injury. Dynamic visualizations for educational purposes seem to promote possibilities for learners to contextualize visual representations relative to one’s own body. Educational methods and practice need explicit attention and development in order to use the full potential of the visualization technology for learning for the health care professions.
Introduction
Learning about trauma biomechanics requires basic knowledge of human musculoskeletal system anatomy. Anatomy may also be seen as the foundation for clinical examination and medical knowledge across specialties and thereby as important for all undergraduate health professional students to learn.Citation1 Learning anatomy involves understanding how three-dimensional entities relate to the human body and its constituent structures. Keenan and ben AwadhCitation1 argued that such understanding is one of the most demanding concepts for medical students to acquire.
Today, learning normal and pathological anatomy can be supported by visualization. Computed Tomography (CT) and Magnetic Resonance Imaging (MRI) pictures are examples of static visualization. Static visualization of different diagnoses for clinical application and treatment is an expanding area of healthcare. However, so-called dynamic visualization of trauma mechanics in virtual reality is in its infancy. While dynamic visualizations are depictions that change continuously over time, and represent a continuous flow of motion, static visualizations only depict specific states within a flow of motion.Citation2 Technological advancements in visualization foreshadow the possibility of designing educational arrangements directed toward competencies that are difficult to obtain through traditional forms of university-based education.
One example is simulation-based skills training including 3 D visualization, which is increasingly being integrated into surgical education as an important teaching method across sub-specialties.Citation3 Such technology-enhanced education can alleviate clinical placement shortages and possibly catalyze professional learning in practice. Although these expectations seem too broad for empirical investigation, we believe there is a need to study specific technologies, like dynamic visualization, to identify the new possibilities it offers to learning trauma biomechanics and its implications for understanding clinical problems more generally.
Anatomy education, of central concern in teaching trauma biomechanics, has been described as being ‘at the forefront of integrating innovative technologies into its curricula.’Citation4, p. 303 A recent systematic review showed, however, that most evaluation studies of technology-enhanced learning (TEL) in anatomy curricula are based on learner satisfaction, followed by module or course learning outcomes.Citation4 Clunie et al.Citation4 conclude the majority of studies seek simple correlations between the introduction of TEL and improved student feedback. They argue for studies exploring meaningful relationships between TEL resources and improvement of learning.Citation4
Keenan and ben AwadhCitation1 follow this line of reasoning, suggesting that it is important to account for how students engage behaviorally and cognitively as well as emotionally, when using and implementing new TEL. However, there is a lack of empirical studies on how bodily and emotional engagement plays out in student’s real-time use of such tools and their reflections on such experiences. Seeking to bridge this knowledge gap, the present study investigates students’ actual performance when interacting in a TEL environment and the role that embodied actions play in their understanding of trauma biomechanics. Further, students’ reflections on their experiences are explored to deepen understanding of the learning processes involved. We explore students’ use of a computerized patient case combined with a finite element modelCitation5,Citation6 to visualize the anatomy and trauma biomechanics of cervical spine injury.
Theoretical framing
This study’s approach and perspective build on recent theorizations of professional learning, emphasizing learning as being enacted and embedded in practices.Citation7,Citation8 In these theorizations “practice” is seen as both an enactment of and a vehicle for learning, where knowledge and action are interwoven with conversation and affect in purposeful and formalized human activity.Citation9 This perspective implies a rejection of traditional views of learning and cognition as purely individual mental activities. Instead, sociomaterial approaches examine how material and discursive practices are connected and entangled in everyday practice. Such a perspective also includes how bodies, gestures, and interaction with material objects are enacted.Citation10 Sociomaterial research has identified that experts’ abilities in radiology,Citation11–13 anesthesiology,Citation14 surgery,Citation15 as well as in law and archaeologyCitation16,Citation17 rely on practices for classifying phenomena, including talk, gestures, and object manipulations. Consistent with these studies, IvarssonCitation13 has shown that one’s own body and gestures serve as fundamental resources in experts’ readings of radiographs, e.g. to discriminate between pathological and non-pathological structures.
Alluding to Thomas Fuchs’s writings,Citation18 Schmidsberger and Löffler-StastkaCitation19 argue that “The body is co-constitutive for the cognitive and emotional life.”Citation19(p. 3) In a post-Cartesian theory where body and mind are not separated, they argue that emotions are experienced and expressed through our bodies, so called bodily resonance, and further that these bodily actions are central to expressions of empathy and social understanding. FuchsCitation18 emphasizes that emotions do not appear as entities in themselves, but are characterized by directedness, toward people, objects, and situations, and further that they carry an affordance – that they exist because they are important. These entities together may serve as mediators for learning.
This study investigated how an interactive visualization tool contributed to students’ emerging understanding of trauma biomechanics. Analytical focus was placed on a) students’ interaction with each other and the technology to develop a shared understanding of the visualized phenomena and b) how students reflected on their experiences in hindsight. Further, our ambition was to discuss the pedagogical affordances of such tools and the wider potentials for advancing health care education. Special focus was on medical, nursing, physiotherapy, and occupational therapy students’ efforts to understand biomedical processes as they interacted with the patient case and the visualizations offered through learning software.
Material and methods
This study built on video-recordings and focus group interviews with 30 students, of which 22 female and 8 male, enrolled in different education programs at Karolinska Institutet, Stockholm, Sweden. The participants were between 22-34 years of age and comprised of 10 medical, 10 nursing, 6 physiotherapy and 4 occupational therapy students. Students were doing an interprofessional clinical placement on an orthopedic ward, medical students during semester 7 out of 11, all other students during semester 6 out of 6).
First, we describe the learning software that the students explored in the study. Next, we describe how the video-recordings and the focus group interviews were conducted and analyzed. Finally, we present how analyses from the video-recordings and the focus group interviews were coded and merged into four descriptive themes that comprise the study’s main findings ().
Table 1. Extracts from triangulation of data from video observations and focus group interviews resulting in merged themes.
Learning software
A PC-based learning software application that combined a virtual patient case with a cervical spine fracture and finite-element visualization of fracture biomechanics was developed.Citation5,Citation20 The case involved an elderly woman who had fallen against a table in her home and arrived at the hospital with neck pain. The patient was later diagnosed with an odontoid fracture of the second vertebral body (axis).
The learning software was developed to enhance understanding of the biomechanics behind an injury via dynamic imaging sequences. We have previously shown that active visualization with this finite element-based model of cervical spine injury increased self-efficacy in medical students,Citation5 and was more stimulating and engaging for orthopedics residents than was a traditional lecture.Citation6 The content was divided into five phases: Work Up, General Information, Biomechanical Case Study, Biomechanical Risk Assessment, and Treatment. Participants followed the patient from arrival to the hospital until treatment. In the first two phases, Work Up and General Information, participants examined the patient and gathered general epidemiological and anatomical information about odontoid fractures. Throughout the Work Up and Treatment phases, participants were asked to suggest and discuss spinal examinations, laboratory tests, and imaging, as well as treatment options. After that, pre-programmed feedback was provided through the program. In the Biomechanical Case Study phase, participants could view video sequences of finite-element simulations of the woman falling backward, sideways, or forward and impacting on a table. Effects on the vertebrae, muscles, and ligaments were visualized. In the Biomechanical Risk Assessment phase, simulations demonstrated what could happen to an untreated patient with an odontoid fracture when engaging in normal physical activity, with special focus on space available for the spinal cord (for an illustration of the program and how students interacted with the it, see https://www.youtube.com/watch?v=v6_MbJOPJlU&feature=youtu.be)
Video recordings
Students were invited to explore the software as a learning resource during an interprofessional clinical placement on an orthopedic ward. They were divided into 10 interprofessional groups of 3 participants. Before each session, a certified orthopedic surgeon gave a standardized introduction to the learning software. While interacting with the software, the student groups were video recorded from the front and behind. The orthopedic surgeon present during the whole learning event could immediately settle technical issues and questions relating to the learning program.
Video recordings were analyzed using an inductive approach according Heath et al.’sCitation21 principles for video-analysis in the social sciences. These principles imply a focus on how participants, in the midst of action, are able to make sense of and achieve a shared understanding of their situation, in our case how students interact in response to what plays out in the visualizations in front of them. Analytical focus was placed not only on students’ speech, but also on how gestures, such as pointing out specific anatomical structures, and other non-verbal actions were employed to understand head/neck-trauma mechanics.
First, illustrative examples were observed by the whole research group to get an overview, then again by two researchers (JC, HR) for a more fine-grained analysis in order to structure and categorize the reviewed recordings. As a result of this analysis themes were suggested. Thereafter, an independent more comprehensive analysis of the entire material was performed to suggest restructuring of the material, look for variation, and delineate the themes (HM, JC). Ambiguities and differences in the interpretations were negotiated and resolved by discussion (HM, JC, HR).
Focus group interviews
Following interaction with the learning software, investigators probed students’ experiences via four focus group discussions, to which video recorded students were invited to attend at their own convenience. Twenty-four students participated in the focus group discussions. Focus groups comprised 3-11 students from 2-4 different professional programs. The purpose of focus group research is generally to identify a range of perspectives on a joint topic, and to get an understanding of the issues from the participants themselves.Citation22 In this case, the aim of the focus group discussions was to assist the video analysis with a different kind of data that could contribute to understanding the observations from the video-analysis.
One researcher acted as moderator (HR) and two researchers acted as observers (HM, LFT) who could also participate in the discussion or ask follow-up questions. The focus group discussions were recorded and transcribed verbatim. The focus group interview followed a semi-structured approach. The interview guide comprised an open invitation to the participants to reflect on themes like the experienced possibilities and limitations/difficulties of the learning software and visualization, and in what ways it contributed to their understanding.
Analysis began with the observation and coding of the video-data (HM, JC, HR). The second step was to scrutinize and discuss the findings within the whole research group. The third step comprised analysis and coding of the focus group interviews (MAD) as a means of triangulating data.Citation23 Analysis of the focus group interviews aimed at tracing how the visualization emerged as a learning context for the students. Consistent with the theoretical framing,Citation7–13 particular focus was placed on how social and material aspects of the situation were related.
As a final step, the analytical findings were scrutinized and merged into four descriptive themes. The themes illustrate how students engaged with the visualization and how this contributed to their learning. displays examples of how excerpts from observed video data and focus group data were described and coded and combined to build up the themes.
The study was approved by the regional ethics committee (Dnr 2016/450-31) and participation was on a voluntary basis.
Findings
The effects of the head/neck-trauma visualizations on participants could be described through four themes: Embodying and articulating pain, Mirroring trauma mechanisms in their own bodies, Exploring the biomechanics preconditions, and Relating patient case to clinical reasoning. These themes will be further described below.
Embodying and articulating pain
While observing the visualizations, students frequently displayed empathizing signs of pain or agony, such as facial expressions, covering their faces, and uttering sounds of distress (). When presented with the case description this did not occur, but it did occur specifically during the slow-motion sequences of the fall in which stress, tension, and the subsequent fracture was demonstrated as the patient’s head impacted the table. These sequences were commonly observed by the participants in silence with focus directed toward the computer screen.
Figure 1. Embodying and articulating pain. Left: medical student (front camera Session 4, time 17:21). Middle: nursing student (front camera, Session 2 time 25:44). Right: medical student (front camera Session 1, time 34:37).

Figure 2. Mirroring trauma mechanisms. Left: nursing student (front camera Session 1, time 34:46). Middle: medical student (front camera Session 4, time 17:41).

Figure 3. Exploring the biomechanics preconditions. Left: physiotherapy student (front camera Session 2 time 13:13). Right: nursing student (front camera Session 1, time 34:42).

The visualization’s slow-motion feature and, in some instances, the ability to add color coding to the anatomical parts receiving the greatest stress seemed to provoke these reactions among students even though the simulated human was simply a schematic drawing of skeletal parts. Clearly the students connected the represented trauma situation to their understanding of how such a fall could inflict harm to a real person with resulting pain, fractures, and possible permanent injuries. Although no discussions occurred during these visualizations, in some instances members of the group pointed at the screen to emphasize or highlight what was going on.
In the focus group discussions, students described how trauma visualization induced emotionally loaded affective responses and that these feelings were connected to their understandings of the case description and what had happened in the body of the patient. The following excerpt from the dialogue in Focus Group 2 illustrates this:
Student 1: You can almost see the pain. it is just like, aaaww…
Student 2: Yes, and it was like the whole neck and head was pushed to the side, almost…
Student 3: Exactly, the stress was really high, and it felt not good, not safe. so we were not comfortable…
Student 4: Yes, I watched the film in a different group. the film was emotionally touching, in a way…
Student 1: You kind of shy away, like, aaaww…
Student 2: Yes, it is almost as if you could feel the pain yourself actually. so it is a little unpleasant…
Students also experienced the visualization as agreeable and useful, promoting a broader understanding of case complexity, as the following quotations illustrate.
I thought it was fun, I liked the films, it felt like you got a picture of the whole problem and what had caused it. (Focus Group 3)
I liked the video, it was really simple to understand how it works, but maybe a bit to slow. you could do it a bit faster, because if you watch the video all the time, it becomes a bit boring… (Focus Group 2)
Mirroring trauma mechanisms
The data included several examples of students mirroring and mimicking with their own bodies the movements displayed on screen as the visualizations took place. Such actions included bending of the neck (), but also tilting, touching, and feeling how the fall would occur as well as trying out the range of movement, as illustrated in .
The trying out of range of movement occurred particularly in more extreme motions during the visualizations, provoking, perhaps challenging the students to evaluate the mere authenticity of such movements. These behaviors occurred throughout the visualizations and appeared as a confirming or reflective process of what was occurring on screen. The quotation below illustrates how visualization supported the embodiment of biomechanics, as the student realized the limitations of neck movement and what forces and pain the trauma caused the patient.
Really instructive for me, I am a “physio,” and it is a very important part of our profession to have a check on the anatomy././to me it was very interesting to see how violence from different directions and how the forces impact on ligament and muscles. (Focus Group 1)
Exploring the biomechanics preconditions
In the videos, students often connected the visualized human anatomy with their own bodies by touching and watching themselves. In this way they appeared to relate the structures and graphics on the screen to their own bodies, which served as a real-world anatomical reference map. The quotations below from three students, from Focus Group 2 and 3 respectively, demonstrate how students connected the dynamic visualization of anatomical structures to the coloring of strain, graphs or forces, and trauma mechanisms.
I remember the coloring, mostly that the parts where the most red color was, was where the strain was highest. I thought it stuck with me, also this with the different bony structures, and when you hit backwards, there was extra much violence, or how to say, force.yes. (Focus Group 2)
Personally, I took with me parts also from the rest of the case, not just these graphs, that was perhaps not the most interesting, I thought the whole exercise, to do this interactively was very good.//(Focus Group 2)
Interesting with the rather advanced graphics showing how the energy peaked and visualized that.ok, that is why you get one of those fractures. otherwise, if you read in a book, it only says that if you fall forward the fracture will be like this, but you do not understand why until you see it like this. that’s why I think this program is good at. (Focus Group 3)
At times, students spoke the name of anatomical structures visualized or sought confirmation from other group members as to whether their understanding of which structures were involved, or their previous knowledge, was correct. At still other times it seemed as if the lack of correct anatomical terms could be bridged by just pointing toward the screen, or oneself, as seen in , and using indexical expressions such as “this one,” “there.”
Relating the visualization to the patient case
During the visualization students repeatedly connected what they saw with the case they read about previously in the session. Moving back and forth they discussed how the sequence of events evolved in the scenario and used clinical reasoning partly based on findings from the visualizations to figure this sequence out. In doing so, there was discussion of which previous knowledge and specific professional knowledge was relevant. Students had the opportunity to address profession-specific topics and in some cases, they were addressed by others as being representatives of their professional community. Arguments based on established forms of clinical reasoning were mixed with personal experiences and knowledge obtained in their profession-specific education, and connections were made to the roles and responsibilities of other professions, and how these could be linked to the responsibilities of their own profession, as illustrated in the following quotation from one nursing student and one occupational therapy student:
From that history we got about the fall, it did not look like she actually was severely injured. She had a little wound on the head and pain in the neck, she had fallen in the kitchen or something. And sometimes you could maybe just pass and think that this is not so dangerous, just a little pain. But if you have this kind of deeper knowledge about what actually can have happened, then you maybe would give this patient a higher triage/priority. Or from the start say that you have to keep the neck still, because this could possibly be a neck injury, just to do some preparatory interventions before the doctor arrives. (Focus Group 4)
.as an occupational therapy student you are perhaps more interested in the home situation and other things related to going back home, than the pure mechanics, or exactly what has happened in the body. (Focus Group 3)
Comments in the focus group interviews also illustrated how the visualization experience triggered recontextualization of the learning both to the visualized case, and to possible clinical reasoning in similar cases.
OK, now when the patient has this injury, I get an understanding of what happens in the neck, and I can connect to, well, should we lay the patient with a neck collar on a spine board until we know more, should we as nurses focus on pain relief, she is obviously in severe pain. Yes, I thought I could gain a lot from that. (Focus Group 2)
I am not sure how closely I will come to work with cervical spine fractures, but if some similar was available for several other injuries, e.g., the knee or hip joints, that would help me understand many injuries././to understand the concept of why certain structures get injured and others not, that could help to understand what it is we should rehabilitate.” (Focus Group 1)
The students identified that reasoning through the trauma biomechanics in the acute case could be relevant and helpful to understanding how the patient should be handled on the ward. They could also connect to other cases where deeper knowledge of trauma biomechanics would have been helpful.
Discussion
This study demonstrates the affordances of dynamic visualization for supporting students’ efforts to develop shared understandings of objects and processes in trauma biomechanics. Further, it illustrates the role of embodied actions in articulating what students observe and the significance of color coding and tempo for supporting their reasoning.
The first theme identified, embodying and articulating pain, underlines how the visualizations affected students emotionally. Certain visualization elements in particular seemed to prompt such behavior, an impression that was supported by several comments from the focus group interviews. We argue that these types of reactions are not expected in other learning situations, e.g. when seeing static visualizations or reading about biomechanics. The visualization of trauma and the embodied reactions, or bodily resonance, clearly evoked empathy as a modality of learning, in addition to the cognitive understanding.Citation19
Further, it is notable that visualization serves as a resource for articulating processes by creating a shared perceptual field in which events and objects are discerned and highlighted through deictic gestures directed toward the screen, such as aligning pointing and utterances like “this,” “that,” and “there.”Citation16,Citation24 In this way visualization offers a shortcut for understanding biomechanical processes by compensating for a limited mastery of medical terminology and by providing opportunities for collaborative sense-making across professional domains.
When interpreting our observations of how the students connected, it was clear that the students referred to their own bodies. Instead of merely verbally acknowledging the anatomical structures and biomechanical happenings, students enacted anatomy and biomechanics. It appears that, for the students, participating in anatomy and biomechanics visualization is more a matter of doing than of naming and acknowledging. GreenCitation25 articulates this as the empirical body. Also, he argues that the body carries knowledge and learns. By using their bodies, students could connect to previous knowledge and test and incorporate new understanding. Dieckmann et al.Citation26 also discuss the importance of the body in professional learning and how the body can be conceptualized in different ways depending on its particular function.
FenwickCitation9 argues that learning by “participation” often is used as a contrast to the “acquisition” concept of learning, which views learning as cognitive, conceptual, and individual, and claims that learning by participation is undertheorized and often equated with “activity,” “engagement,” or doing. A sociomaterial perspective on practice foregrounds not only the material dimensions of the human activities and human bodies, but also the non-human participants in a practice, such as texts, instruments, technologies, etc.Citation9 The findings of our study show how different ways of participating, in this case interacting with the visualizations, are linked to different kinds of learning that could support the integration of basic science concepts and clinical knowledge. The importance of integrating basic and clinical sciences across diverse training contexts to improve understanding has been a widespread educational model for teaching in medical school curricula ever since the Flexner report.Citation28 Bandiera et al.Citation29 emphasize that the curricular integration of various contexts of learning might not be enough to guarantee that understanding is improved. There is an important lesson for educators, they argue, to understand how instruction should be arranged in order to “explicitly integrate basic science mechanisms with clinical manifestations, including knowledge about the ways in which contexts might impact understanding.”Citation29, p. 82
In this study, detailed observations and analyses of students’ interactions in technology-enhanced learning suggest that cognitive integration of basic science concepts and clinical understanding is made possible, and that embodiment and empathy play important roles in this process. More specifically, as shown by Koschmann and Zemel,Citation17 novices’ understanding of new domains relies on embodied actions to achieve a shared view on the problems they encounter. Our study shows how students, when interacting with the visualization, related the structures, movements, and forces represented on the screen to their own bodies and how embodied actions functioned as resources for making sense of what the visualization showed. In parallel, to research on how radiology experts interpret evidence or agree on a diagnosis,Citation13 we argue that embodied actions are crucial also in students’ learning by means of dynamic visualization.
It is debatable to what degree visualization in itself can contribute to affective and empathic responding, and whether such responding to stand-alone visualization—without association to a case history—would occur. It can be argued that without knowledge about a person, a full sense of empathy may be difficult. The visualization’s link to the person and case history also was obvious; during the visualization, students often referred to the crudely simulated human being as” her.” Therefore, it is evident that having the case history as background and starting point for the biomechanical visualizations provided a context for the students to frame the exercise as concerning a living patient, which offered a basis for both engagement and authenticity.Citation27
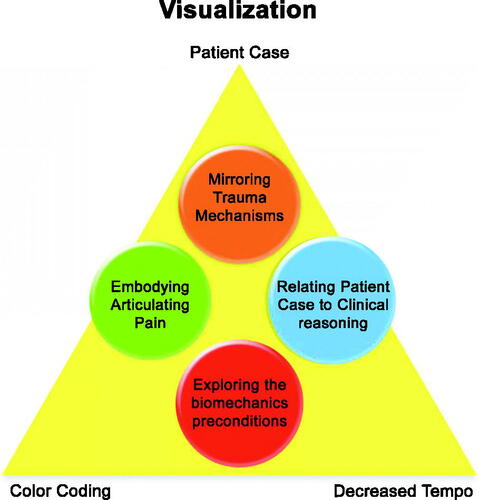
Besides embedding the visualization in a patient case, other features of the technology stood out as important for promoting engagement and understanding of trauma mechanisms. It was apparent from both video and interview data, that the decreased tempo, showing the directions and dynamics of trauma biomechanics in slow-motion with a simultaneous display in color coding of the strain on the affected structures, were especially important for evoking the emotional responses and for promoting students’ understanding of causal relationships between external forces and biomechanical effects. It is notable that these features of the technology–patient case, tempo, color–do not themselves determine changes in the students’ learning activities. Rather, the activities, as represented by the four themes – embodying/articulating, mirroring trauma, exploring, biomechanics, relating to the patient case – were enabled through the ways in which these technological features were brought to life in and through the students’ interaction. The following figure shows the sociomaterial relation between technology design and student activities, which is aimed to illustrate how the visualization offered unique resources for learning ().
Figure 4. The relation between the design of the visualization – patient case, decreased tempo, color – and the four themes forming the results.
A methodological remark is that our observations are dependent on the social context in which they were made. If students sat alone or with unfamiliar others, their behavior might be quite different. Our argument, however, is that dynamic visualization’s pedagogical potential can only be assessed when it is brought to life in an educational context. Our observations illustrate how dynamic visualization can support reasoning across professional boundaries. Still, cervical spine injury is a rather specific topic, and one cannot assume that all dynamic visualizations lend themselves to interprofessional learning purposes. For instance, our results indicate that trauma biomechanics may not be equally relevant for students from all programs. Therefore, in drawing conclusions from our study, it is important to account for visualization content and in what ways the chosen topic can bridge various professional domains. It is evident from our observations that students’ talk and embodied actions, together with deictic gestures directed toward the screen, served as fundamental resources for making sense of visualized biomechanical processes. This may be of special importance for novices, but as shown by Ivarsson,Citation13 similar ways of understanding phenomena are salient also in expert reasoning. Therefore, we stress the importance of focusing analytically on both verbal and embodied actions in exploring how novices develop their knowledge of dynamic processes that are partially new for them.
Insights
This study shows that visualization of biomechanical events has the potential to improve understanding of injury mechanisms and specifically to identify anatomical structures at high risk of injury. Since knowledge of the mechanisms and biomechanics of injury is important, but seldom used by physicians, nurses, physiotherapists, or occupational therapists today, we validated the system in an interprofessional learning context. Our contention is that a combination of virtual environments for advanced medical simulation and visualization provide unique possibilities to gain further insight into this new paradigm for training and how it can be enacted. This is promising for gaining new knowledge on how proficiency can be acquired and maintained that truly would advance the leading edge of healthcare education in the interest of patient safety. One of the most promising features of dynamic visualization for educational purposes seems to be the possibilities for learners to contextualize the visual representations relative to one’s own body. This, in turn, can partially compensate for a varied mastery of medical terminology among students since peer-contributions can help to extend one another’s content knowledge. A caution to consider if similar software is integrated into on-line applications is the broad range of communication modalities involved in students’ efforts to grapple with the subject matter. Further, as is known with other technical developments, educational benefits automatically follow adoption of new technology. Educational methods and practice need explicit attention and development in order to use the full potential of visualization technology for learning in the health care professions.
Declaration of interest statement
The authors have no conflicts of interests to declare.
Additional information
Funding
Funding
References
- Keenan ID, Ben Awadh A. Integrating 3D visualisation technologies in undergraduate anatomy education. In: Rea P, ed. Biomedical Visualisation. Advances in Experimental Medicine and Biology. Vol. 1120. Cham, Switzerland: Springer; 2019:39–53. doi:https://doi.org/10.1007/978-3-030-06070-1_4.
- Kühl T, Scheiter K, Gerjets P, Gemballa S. Can differences in learning strategies explain the benefits of learning from static and dynamic visualizations?Comput Educ. 2011;56(1):176–187. doi:https://doi.org/10.1016/j.compedu.2010.08.008.
- Hedman LR, Felländer-Tsai L. Simulation-based skills training in non-performing orthopedic surgeons: skills acquisition, motivation, and flow during the COVID-19 pandemic. Acta Orthop. 2020;91(5):520–522. doi:https://doi.org/10.1080/17453674.2020.1781413.
- Clunie L, Morris NP, Joynes VCT, Pickering JD. How comprehensive are research studies investigating the efficacy of technology-enhanced learning resources in anatomy education? A systematic review. Anat Sci Educ. 2018;11(3):303–319. doi:https://doi.org/10.1002/ase.1762.
- Hedman L, Fahlstedt M, Schlickum M, Möller H, von Holst H, F, Tsai L. A pilot evaluation of an educational program that offers visualizations of cervical spine injuries: medical students’ self-efficacy increases by training. Inform Health Soc Care 2014; 39(1):33–46. doi:https://doi.org/10.3109/17538157.2013.834343.
- Courteille O, Fahlstedt M, Ho J, et al. Learning through a virtual patient vs. recorded lecture: a comparison of knowledge retention in a trauma case. Int J Med Educ. 2018; 9:86–92. doi:https://doi.org/10.5116/ijme.5aa3.ccf2.
- Hager P. Theories of practice and their connections with learning: a continuum of more and less inclusive accounts. In: Hager P, Lee A, Reich A, eds. Practice, Learning and Change: Practice-Theory Perspectives on Professional Learning. Vol. 8. Dordrecht, Netherlands: Springer; 2012:17–32. doi:https://doi.org/10.1007/978-94-007-4774-6_1.
- Fenwick T, Nerland M, eds. Reconceptualising Professional Learning in Turbulent Times: Changing Knowledges, Practices, and Responsibilities. London, UK: Routledge; 2014.
- Fenwick T. Matterings of knowing and doing: sociomaterial approaches to understanding practice. In: Hager P, Lee A, Reich A, eds. Practice, Learning and Change: Practice-Theory Perspectives on Professional Learning. Vol. 8. Dordrecht, Netherlands: Springer; 2012:67–83. doi:https://doi.org/10.1007/978-94-007-4774-6_5.
- Abrandt Dahlgren M, Rystedt H, Nyström S, Felländer-Tsai L, eds. Interprofessional Simulation in Health Care: Materiality, Embodiment, Interaction. Vol. 26. Dordrecht, Netherlands: Springer; 2019. DOI doi:https://doi.org/10.1007/978-3-030-19542-7.
- Slack R, Hartswood M, Procter R, Rouncefield M. Cultures of reading: on professional vision and the lived work of mammography. United Kingdom. In: Hester S, Francis D, eds. Orders of Ordinary Action. Europe: Ashgate; 2007:175–193.
- Alac M. Working with brain scans: digital images and gestural interaction in fMRI laboratory. Soc Stud Sci. 2008;38 (4):483–508. doi:https://doi.org/10.1177/0306312708089715.
- Ivarsson J. Visual expertise as embodied practice. Frontline Learn Res. 2017;5(3):123– 127. doi:https://doi.org/10.14786/flr.v5i3.253.
- Sanchez Svensson M. Monitoring practice and alarm technology in anaesthesiology. Health Informatics J. 2007;13(1):9–21. doi:https://doi.org/10.1177/1460458207073649.
- Koschmann T, LeBaron C, Goodwin C, Zemel A, Dunnington G. Formulating the triangle of doom. Gesture. 2007; 7(1):97–118. doi:https://doi.org/10.1075/gest.7.1.06kos.
- Goodwin C. Professional vision. Am Anthropol. 1994;96(3):606–633. doi:https://doi.org/10.1525/aa.1994.96.3.02a00100.
- Koschmann T, Zemel A. Optical pulsars and black arrows: discoveries as occasioned productions. J Learn Sci. 2009; 18(2):200–246. doi:https://doi.org/10.1080/10508400902797966.
- Fuchs T. Intercorporeality and interaffectivity. In: Meyer J, Streeck J, Jordan S, eds. Intercorporeality: Emerging Socialities in Interaction. Oxford, UK: Oxford University Press; 2017:3–24. doi:https://doi.org/10.1093/acprof:oso/9780190210465.003.0001.
- Schmidsberger F, Löffler-Stastka H. Empathy is proprioceptive: the bodily fundament of empathy - a philosophical contribution to medical education. BMC Med Educ. 2018;18(1):69. doi:https://doi.org/10.1186/s12909-018-1161-y.
- Hedenstierna S, Halldin P. How does a three-dimensional continuum muscle model affect the kinematics and muscle strains of a finite element neck model compared to a discrete muscle model in rear-end, frontal, and lateral impacts. Spine. 2008;33(8):E236–E245. doi:https://doi.org/10.1097/BRS.0b013e31816b8812.
- Heath C, Hindmarsh J, Luff P. Video Analysis and Qualitative Research: Analysing Interaction in Social Life. London, UK: Sage; 2010. doi:https://doi.org/https://dx.doi.org/10.4135/9781526435385.
- Hennink M. Focus Group Discussions. Oxford, UK: Oxford University Press; 2014. doi:https://doi.org/10.1093/acprof:osobl/9780199856169.001.0001.
- Fusch P, Fusch E, Ness LR. Denzin’s paradigm shift: revisiting triangulation in qualitative research. Soc Change. 2018;10(1):19–32. doi:https://doi.org/10.5590/JOSC.2018.10.1.02.
- Kendon A. Gesture: Visible Action as Utterance. Cambridge, UK: Cambridge University Press; 2004. doi:https://doi.org/10.1080/15427580701340790.
- Green B. Thinking bodies: practice theory, deleuze, and professional education. In: Green B, Hopwood N, eds. The Body in Professional Practice Learning and Education. Vol. 11. Dordrecht, Netherlands: Springer; 2015:121–136. doi:https://doi.org/10.1007/978-3-319-00140-1_8.
- Dieckmann P, Johnson E, Hopwood N. Bodies in simulation. In: Abrandt Dahlgren, M, Rystedt, H, Felländer-Tsai L, Nyström S, eds. Interprofessional Simulation in Health Care: Materiality, Embodiment, Interaction. Vol. 26. Dordrecht, Netherlands: Springer; 2019:175–195. doi:https://doi.org/10.1007/978-3-030-19542-7_8.
- Rystedt H, Sjöblom B. Realism, authenticity, and learning in healthcare simulations: rules of relevance and irrelevance as interactive achievements. Instructional Sci. 2012;40(5):785–789. doi:https://doi.org/10.1007/s11251-012-9213-x.
- Flexner A. Medical Education in the United States and Canada: A Report to the Carnegie Foundation for the Advancement of Teaching. New York. Carnegie Foundation for the Advancement of Teaching; 1910.
- Bandiera G, Kuper A, Mylopoulos M, et al. Back from basics: integration of science and practice in medical education. Med Educ. 2018;52(1):78–85. DOI:https://doi.org/10.1111/medu.1338.