
Abstract
Phenomenon: Pharmacology is a fundamental healthcare discipline, but it can be difficult and counterintuitive for learners to learn. Navigation toward understanding pharmacology can be troublesome, but once the threshold to comprehension is crossed, learners can experience a transformative shift in their ways of thinking and practicing. We conducted an in-depth examination of threshold concepts within pharmacology, aiming to identify and prioritize their learning to improve the medical curriculum and enhance medical treatment and patient safety. Approach: We carried out a consensus generation process using the Nominal Group Technique (NGT) to identify potential threshold concepts in pharmacology. Participant groups of pharmacology experts and medical students considered, identified, reviewed, and ranked potential pharmacology threshold concepts within their own group. Then, using a logical, step-by-step approach, we combined the final ranked data from these multiple NGT sessions. We further analyzed these data using an abductive analysis approach; data were coded, categorized, reorganized, and conceptually mapped after critical evaluation. Conceptual themes were established corresponding to different phases of cognitive schema development. Findings: Six comprehensive conceptual themes were identified: Drug Mechanism of Action; Pharmacotherapeutics; Pharmacokinetics; Drug Receptor Interactions; Drug Terminology and Nomenclature; and Signaling Pathways. These concepts align with many of the key attributes of threshold concepts (e.g., troublesome, integrative and transformative). The cognitive schematic themes generated were (i) acquisition-troublesome; (ii) acquisition-transformative; (iii) automation-troublesome; (iv) automation-transformative. Insights: Transformative learning involves different stages of cognitive schema evolution, including acquisition, elaboration, and automation, and is influenced by both the inherent challenges of the concepts and limitations of human cognition. The high interactivity of these troublesome concepts challenge schema acquisition and automation. Troublesome concepts underpinning procedures or skills, while not easily explained by cognitive rules, can lead to slow, awkward, error-prone performance, creating additional barriers for practice. Integrating concepts into a coherent structure leads to the irreversible assimilation of knowledge and the transferability of both knowledge and skills, influencing learners’ epistemological transitions and ontological transformations at theoretical and professional levels. Further work on designing instructional models around assisting and automating schemas around identified troublesome knowledge, while addressing the impact of cognitive load, has the potential to promote transformational learning.
Introduction
Medical students find certain pharmacology concepts difficult to comprehend because of the inherently troublesome nature of the content. This difficulty can be detected in students’ struggles to learn and apply flexibly the required concepts.Citation1 The routine application of disciplinary concepts without any apparent connection to real-world situations can render them ritual and, respectively, inert.Citation1,Citation2 In addition, the language or terminology used within academic disciplines can cause conceptual problems due to its specific meaning and usage within that discipline.Citation1,Citation2 Reportedly, final-year medical and nursing students were able to define pharmacological terms but lacked the ability to discuss the meaning and clinical relevance of these terms in depth.Citation3 If concepts are not contextually explained, students may end up rote-learning them without fully understanding their meaning.Citation4 Without a clinical context for pharmacology, conventional teaching methods neither initiate global understanding nor impart life-long transferability. In fact, these methods tend to be teacher-driven, unidirectional, and do not foster the analytical skills necessary for pharmacological reasoning inherent to patient care.Citation5
A well-grounded knowledge base helps learners to function in various environments, organize complex situations, direct their attention appropriately, and coordinate cognitive tasks.Citation6 Inadequate knowledge base development may lead learners to use inefficient methods for acquiring new information, overloading working memory and diverting cognitive resources from the learning process.Citation6,Citation7 Within the realm of learning, two fundamental mechanisms hold significance: (i) the acquisition or construction of schemas, and (ii) automation. The former entails the establishment of cognitive frameworks to capture meaningful concepts from diverse experiences, providing adaptable frameworks for various scenarios. The latter involves learners developing specific cognitive and psychomotor rules that trigger precise mental or physical responses. It demands iterative practice and constitutes a vital component of schema formation.Citation8
Conceptual understanding is an integrated process; students can become stuck at a point when they have some surface knowledge but are not yet able to coordinate and transfer conceptual knowledge that requires integration.Citation9 In pharmacology specifically, acquired knowledge must be translated into various professional skills in high-pressure clinical settings. The complex skill of prescribing requires a broad understanding of pharmacological concepts to provide medications, dosages, and combinations within a treatment plan tailored to the patient. Due to a lack of hands-on prescribing opportunities during medical school, junior doctors often have difficulty proactively transferring essential inert and ritual knowledge into diverse clinical scenarios.Citation10 Knowledge transition will continue to present a challenge for students studying pharmacology if they are not able to translate their understanding of drugs into rational pharmacotherapeutic plans in various clinical settings.
Within these challenges there are likely to be distinctive “threshold concepts” that influence students’ epistemic modes of reasoning and interpretation. In 2005, Meyer and Land theorized that learners need to pass through "conceptual gateways or portals" (p. 375) to arrive at advanced ways of understanding while transitioning into a suspended or "transformational state of liminality" (p. 380) consisting of three phases: preliminal, liminal, and post-liminal.Citation11 This process of learning progression is transformative, yielding a valuable outcome of cognitive evolution within learners’ mindset.Citation12 Within a given disciplinary discourse, threshold concepts (TCs) are delineated based on several key attributes, such as being transformative, irreversible, integrative, bounded, and inherently troublesomeCitation11,Citation13 However, cognitive processes and their evolution in dealing with TCs in pharmacology remain inadequately explored.
When learners encounter troublesome knowledge, they must integrate prior and new knowledge and reshape their thinking to facilitate deeper understanding.Citation14,Citation15 This results in an ontological shift into the post-liminal phase where knowledge becomes consolidated (irreversible).Citation14 Thus, the threshold concept framework (TCF) offers a way to enhance understanding of development within a subject area, allowing educators to design curricula that guide students through the key learning milestones and disciplinary conceptual gateways. This study aimed to explore the specific challenges to disciplinary learning in pharmacology and to identify and prioritize student learning, improve the quality of medical curriculum, and ultimately contributes to improving medical treatment and patient safety.
Method
Overview
Our focus on TCs as a theoretical lens prompted our methodological decision to use the consensus generation method of Nominal Group Technique (NGT), which fosters a “learning as a practitioner” perspective. NGT facilitated a transactional curriculum inquiry, incorporating a wider diversity of participants than those usually recommended, to include academics, students, and educational developers.Citation16 We explored the NGT findings using abductive analysis, which facilitated understanding of the subtleties of each idea together with alignment to the key attributes of TCs.
Data collection
With approval from Western Sydney University’s Human Research Ethics Committee (H13822), our recruitment process began by sending email invitations to a structured small-group discussion to relevant participants, including medical doctors, subject experts, medical educators, and Western Sydney University (WSU) medical students. NGT combines quantitative and qualitative data collection in a structured reflective, face-to-face process.Citation17 Because the COVID pandemic restrictions were in effect in New South Wales, Australia, at the time of this study, we developed a virtual NGT (vNGT) model, using Zoom© as the online videoconferencing tool. It is relatively easy to use, cost-effective, has data management features, and recording and security features.Citation18
During the orientation session, participants were encouraged not to conflate threshold concepts with core concepts, as the former entail a significant shift in understanding, characterized by their key attributes. Core concepts, forming the foundation of knowledge as essential building blocks, do not entail the profound cognitive shift associated with threshold concepts.Citation11,Citation13,Citation19 Nevertheless, this transformative leap in understanding is essential for advancing student learning. The study began with a nominal question: "What constitutes the troublesome knowledge/threshold concepts of pharmacology?" Participants provided their ideas and contributed to a collaborative effort aimed at gathering insights on specific issues.Citation20,Citation21 In line with Murphy et al. we provided participants with information as early as possible in the process through a shared video, giving insights into the different steps of NGT.Citation20,Citation22
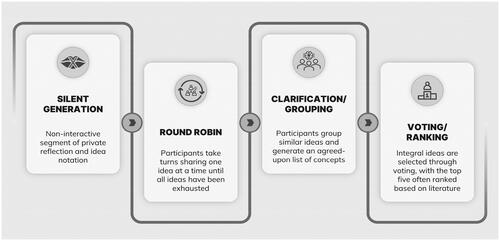
This process () started with “silent generation” in which participants brainstormed individually to identify troublesome knowledge of pharmacology and attempt to align each idea with the TC criteria. Participants were given a matrix template (Supplemental Appendix) to help them record their concepts and ideas privately. In the second step, round-robin phase, participants collectively shared their identified concepts. Subsequently, through a clarification process, considering each idea and its suggested alignment with TC criteria, these concepts were refined and grouped leading to consensus. At the end of each NGT session, participants voted on what they considered the five most significant threshold concepts within pharmacology.
Figure 1. Schematic diagram of the classical steps of NGT.
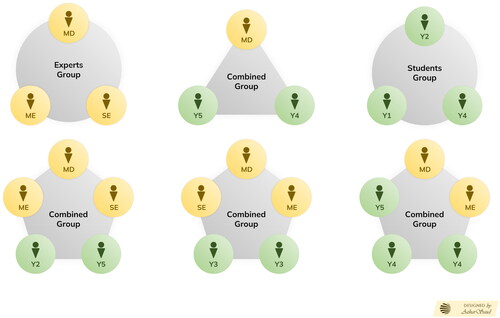
We conducted six vNGT sessions in total, all facilitated by FK. For exploratory purposes, we assembled homogenous groups where all participants had a similar level of experience, and heterogeneous groups (i.e., students and experts).Citation23,Citation24 We started with two homogeneous sessions, each with three experts or three students, while the remaining sessions ran as heterogeneous groups, each with three to five participants as shown in .
Figure 2. Group configurations and key demographics: This visual representation showcases crucial participant demographics, categorizing medical doctors (MD), subject experts (SE), medical educators (ME), and students from different years (Y1–Y5). The configurations encompass both homogenous (students or experts only) and heterogenous (combined) groups, with the number of participants indicated for each group.
Each session was audio-video recorded using Zoom, and a backup recording was made using a dictaphone. Participants verbally consented to being recorded before participating. We transcribed the recordings using professional transcription services. Following the transcription and de-identification, we separated and arranged the identified TCs and imported them into the qualitative data analysis software Atlas.ti, a Computer-Aided Qualitative Data Analysis Software (CAQDAS) used by educators and healthcare professionals.Citation25 Concept saturation was achieved after six sessions, which resulted in over 18 h of audio recordings.
Data analysis
By engaging participants in both homogeneous and heterogeneous group configurations, a beneficial agreement was reached in identifying and prioritizing TCs through fostering discussion and clarification, avoiding assumptions and misconceptions, and leveraging shared perspectives.Citation26 Using the matrix template, participants aligned the identified TCs with their respective key attributes. We found that the most of the TCs aligned with attributes of being troublesome and integrative and embracing the transformative quality, which is pivotal, as these attributes have a profound impact on shaping disciplinary mindsets, guiding student learning, and facilitating the exploration of threshold concepts.Citation27–30 In a personal communication with Professor Ray Land, a prominent TC theorist, it was underscored that these qualities—transformative, troublesome, and integrative—are deemed essential, in line with the perspective of influential authors in this field.
Quantitative Data Analysis: To process and quantify the data from each NGT session, we entered individual participant votes into an Excel spreadsheet and calculated the priorities for each item (concept). Data were combined into a single dataset using the methodology developed by Van Breda.Citation31 A key component of Van Breda’s analytical approach is to consider not just the strength of concepts (sum of votes) or their relative importance, but their voting frequency, which represents how prevalent the concept is within the participant cohort.Citation31
Qualitative Data Analysis: We began our thematic data analysis using the abductive approach based on Timmermans and Tavory’s basic methods.Citation32 This entails revisiting the same observation repeatedly, challenging our familiarity with the known world (defamiliarization), and considering alternative interpretations of our observations (alternative casing). In addition, to ensure a comprehensive understanding, we utilized abductive thematic analysis guidelines provided by Thompson where necessary.Citation33 Our aim was to make the process understandable for novice researchers attempting it for the first time. FK initiated the process, which then proceeded in iterative cycles with FK, IH, RT, and EO to establish the TCs and cognitive categorical themes. We also engaged an external coder (BN) who participated in the process of organizing and critically evaluating the data. The stepwise approach to our analysis follows.
Familiarization/Active Reading: The initial step to data analysis is familiarization achieved through active reading during or after transcription. This facilitates meaning-making of data and understanding contexts beyond mere narratives.Citation34,Citation35
Coding Round (Initial): Active reading paved way to first cycle of coding, establishing a link between empirical data and its cognitive interpretations. This enables the extraction of as much explicit and surface meaning (semantic codes) from the dataset as possible.
Revisiting the Phenomenon: This step allows deeper understanding of the dataset beyond initial interpretation, revealing evolving insights over time. With transcribed data as our primary tool, we used detailed field notes, coding, and memo writing to uncover nuanced relationships between identified TCs. Iterative reading through participants’ narratives and reflections, guided by Charmaz’s methodology, uncovered deeper insights into both overt actions/statements and the implicit aspects behind them.Citation36 For instance, in our discussion of the threshold nature of drug-target interaction, participants often referenced terms or phenomena that sounded similar, yet carried distinct meanings, without explicitly articulating them. Through this process we unveiled essential unspoken concepts in drug interactions, such as specificity, selectivity, and specific antagonism, which participants indirectly alluded to. We carefully examined “troublesome knowledge and threshold concept” networks through a cyclical examination of language and metaphors, including individual elements and themes generated during the vNGT sessions.
Coding Cycle (Subsequent): With a more selective approach, the subsequent coding round helped to consolidate the codes that can be grouped under a single heading and eliminating codes deemed insignificant or not repeated.Citation37
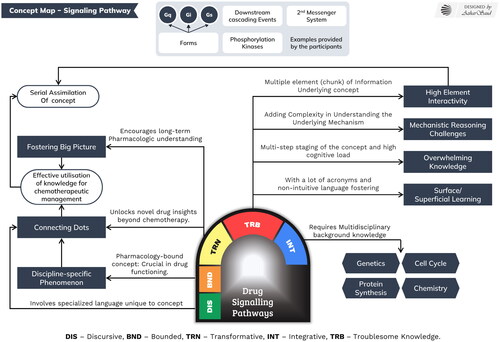
Concept Mapping: We used a conceptual mapping approach guide the formation of knowledge pathways to clarify and examine the links between these codes.Citation38 The concept map for signaling pathways in offers semantic codes and a reflection of how the concept aligns with TCs’ troublesome, transformative, and integrative attributes. Building upon this, we created concept maps for all the comprehensive themes/categories of concepts that we identified.
Theme Generation in conjunction with Defamiliarization: We comprehensively examined narrative, language, and conversational data to reconstruct students’ challenging experiences with pharmacologyCitation39 for a holistic understanding.Citation40 Revisiting the data line by line, examining the relationship between different codes helped us to categorize codes into meaningful themes. FK and BN performed the initial analysis manually using Atlas.ti for Windows.
Transitioning from semantic to latent thematic exploration involves more than revisiting data; it requires challenging assumptions about identified concepts, especially those considered troublesome with a threshold character. By confronting everyday experiences as unfamiliar, we sought to gain deeper appreciation and fresh perspectives.Citation39 Shifting focus to atextual sources, like Zoom-generated video footage, helped us defamiliarize the data, uncovering nuanced layers of meaning and complexity not easily apparent through text alone. Defamiliarizing enhances the abductive approach as it prompts us to reconsider things we overlooked, thus fostering generation of meaningful (latent) themes.Citation32,Citation39
Theorizing to Alternative Casing: With theorization, we engaged with existing theoretical frameworks while remaining open to new interpretations, ensuring that our conclusions aligned with both data and theory.Citation33 This process is mirrored in alternative casing, where researchers explore multiple theoretical frameworks to analyze data from different angles.Citation39 While the TC theoretical framework aligned well with the data, various facets prompted us to continuously adjust and refine our analysis. Abstract concepts and meaningful categorical themes, reflecting various stages of cognitive schema evolution, enabled us to draw parallels between the TCs and cognitive load theory.
Figure 3. Thematic analysis driven concept map of drug signaling pathways.
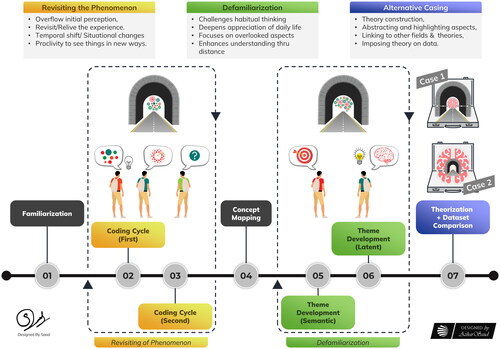
Starting with familiarizing ourselves with our data, revisiting it during the course of coding and theme generation, we then pulled back for defamiliarization. This process enabled the drawing of parallels between identified concepts and cognitive changes underlying schema evolution. Transitioning from the theorization of data, which involves considering existing theoretical frameworks but not restricting analysis to fit these frameworks, to the final step of alternative casing, we abstracted facets of the identified threshold concepts, rendering them comparable to different phenomena, and connected them to a diverse theoretical framework depicted in .
Figure 4. A schematic approach to thematic analysis with visual representation of abductive reasoning phases. Using a preexisting concept map for familiarization, the bystander observes scattered dots representing phenomena/concepts. Subsequent revisits prompt reassessment and connection of dots into shapes. Defamiliarization transforms overlooked objects into various shapes, including archery/dartboard shapes. Iterative cycles enable diverse perspective comparisons. Recognizing dots as a cognitive center and looking through the threshold, as shown in case 1, the bystander applies cognitive load theory, placing “threshold” in the brain’s framework, as depicted in case 2.
Results
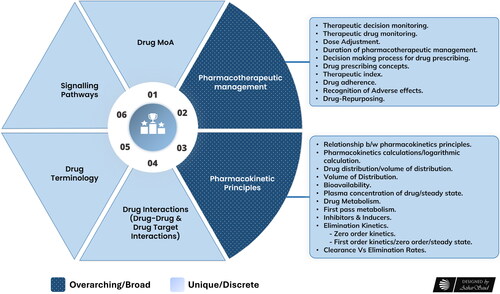
During the NGT sessions, numerous concepts and ideas were presented, from which we developed six preliminary comprehensive categories or themes. Our study identified several essential sub-concepts within the broader themes of pharmacotherapeutics and pharmacokinetics, as illustrated in . This deepened our understanding of how these concepts transform students and enhance their holistic ways of thinking and practicing with this troublesome subject.
Figure 5. Visual depiction of the top 6 identified threshold concepts. Four of the concepts (drug mechanism of action (MoA), signalling pathways, drug terminology, drug interactions) describe more discrete concepts. The two broader themes of pharmacotherapeutics and pharmacokinetics are shown with the finer granularity of underlying concepts identified by participants.
Through cross-case comparisons, data interrogation, and discussions with coauthors, the data aligned with the instructional design theory of cognitive load. This set the stage for the development of a coding matrix informed by cognitive load theory (CLT), as shown in .Citation41 This matrix visually represents interconnections among themes, subthemes, and codes, serving as a structured framework for systematic analysis of the dataset.Citation42,Citation43 Engaging an external coder provided us with reflexive benefits, such as exploring interpretations, sense-checking ideas, and enhancing findings credibility through triangulation of all data sources.Citation44,Citation45
Table 1. Advanced coding framework showing the relationship between the identified threshold concepts, high-level codes, and meaningful themes supported by participants’ quotes.
Following the analysis, categorical themes indicated an association between different phases of cognitive schema evolution. Learning mechanisms such as cognitive schema acquisition and automation play significant roles in preventing cognitive overload.Citation46 We observed that the “troublesome” and “transformative” attributes of identified threshold concepts can affect the process of cognitive schema acquisition and automation.
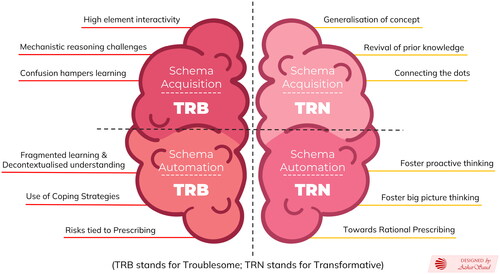
During the analysis, four themes were identified, encompassing our 12 high-level codes (). The themes included: (i) acquisition-troublesome; (ii) acquisition-transformative; (iii) automation-troublesome; (iv) automation-transformative. The four themes evolved from Perkin’sCitation47 Framework of Troublesome Knowledge, which led to the TC Framework with links to CLT. We found that these four themes and 12 high-level codes were related to how these TCs impacted learners’ cognitive schema development and disciplinary ways of thinking and reasoning in pharmacology.
Figure 6. The brain image depicts the four categorical themes (i) acquisition-troublesome; (ii) acquisition-transformative; (iii) automation-troublesome; (iv) automation-transformative), aligned with the twelve high-level codes resulting from abductive analysis (TRB stands for troublesome; TRN stands for transformative); the four quadrants depict the interrelationships between the themes and codes.
Schema acquisition-troublesome
Many concepts identified by participants as troublesome and threshold fall under the category of being highly interactive, such as Drug Mechanism of Action (as shown in ). This complex concept requires simultaneous understanding and processing of multiple sub-concepts and elements, which may lead to a troubled understanding attributed to various phenomena such as the recognition and distribution of receptors (target proteins), physiological processes, and subcellular events. The ability to learn through schema acquisition can alleviate the workload imposed by high element interactivity information from working memory,Citation48 which has limited in capacityCitation49,Citation50 and is short-lived.Citation51 However, it is not uncommon for schema acquisition to be troublesome given the high level of interactivity embedded deep within these concepts.
Schema automation-troublesome
Schema automation, complementing schema acquisition, conserves cognitive resources by facilitating analogy-based problem-solving.Citation52 In its absence, performance becomes sluggish, awkward, and error-prone.Citation41 For instance, medical professionals often overlook medication nonadherence, where healthcare providers’ communication of content and impact are underemphasized despite their significance.Citation53,Citation54 Patient education and consistent ability of a provider to communicate at the lay-level are crucial for ensuring patient comprehension and adherence to medication regimens.Citation55 Moreover, patients may face challenges in expressing medication adherence barriers. Adherence-focused discourse and empathic listening help uncover issues, fostering patient-centered solutions. Continuous patient education and empowerment aids in understanding and promoting medication adherence.
Health professionals develop automated schemas through extended evidence-based practice, enabling accurate execution of recurrent aspects, reducing errors, and conserving cognitive resources.Citation56 This perspective underscores that medical non-adherence could potentially stem from a lack of opportunities for healthcare providers to repeatedly apply and develop these complex skills, thus hindering the effective automation of relevant schemas. In light of this, “medical drug adherence” is not an example of troublesome schema automation but rather a “Threshold Concept,” reflecting challenges such as inadequate learning opportunities for procedural/part-task practice, underdeveloped conditional logics, and insufficient feedback. Furthermore, clinical reasoning, encompassing declarative and procedural knowledge, is identified as a threshold skill that demands ongoing practice for sustained proficiency, emphasizing the need for ample opportunities for practice.Citation57
Schema acquisition-transformative
Through knowledge elaboration, learners can uncover the “hidden relationships” between concepts or elements by integrating new information into existing knowledge structures, allowing them to organize and refine knowledge into a coherent structure, which, at more advanced levels of learning, may also include the generalization of disciplinary schemas.Citation6,Citation58 We found that students’ familiarity with drug identification and nomenclature improved their integration of knowledge of different drug classes and names, which enhanced their understanding and retention of drug uses in the clinical context. For example, the generic names of statins all end with "-statin," which helps students recognize that they are used to lower cholesterol levels. Additionally, while many drug interactions are difficult to recall, a sound understanding of pharmacodynamics may help students identify which drugs share common pathways or mechanisms that may interact. Integrating prior understanding into a concept is certainly “transformative” because it changes the way learners perceive their knowledge. As a concept integrates many facets of a learner’s prior understanding, it has a greater chance of becoming “irreversible” and more concretely incorporated.Citation9
Schema automation-transformation
Our findings suggest that the identified procedural threshold of “selecting drug dosage” is governed by cognitive rules that guide schema automation in the context of the TCs of pharmacotherapeutics, as shown in . As an example, participants used conditional logics/arguments based on “IF condition, THEN action” for selecting the doses and durations of anti-psychotic medications and antimicrobial therapy in different cases. Also, participants agreed that rationalizing the therapeutic regimen should be done proactively; opportunistic deployment is an approach to thinking or disciplinary practice aimed at helping learners identify and deal with situations that might otherwise be overlooked.Citation10,Citation47
A highly integrated knowledge base is organized in interrelated cognitive schema networks, similar to the Davies and Mangan “web of threshold concepts” crucial to gaining an understanding of the “big picture.”Citation9 Automated schemas in this integrated knowledge base are applicable to routine aspects of transfer tasks, such as drug dose adjustment or administration. However, general, or abstract schemas within this integrated knowledge base facilitate a general understanding of a novel situation and its application to a new situation without an increased cognitive load.Citation59 Our research found that physicians’ patient-centered approach offers a big-picture perspective for identifying therapeutic opportunities with readily available drugs. Additionally, our findings suggest that learners must undergo an ontological shift, embracing high-level abstract knowledge when identifying new therapeutic indications for known drugs, highlighting the importance of TCs in “Drug repurposing.” This shift in thinking and acquisition of disciplinary discourse is an integral aspect of “crossing the threshold” enabling individuals to operate at a higher theoretical level and communicate effectively within their field.Citation11,Citation60
Discussion
Our study delved into the challenging content of pharmacology that potentially introduces various thresholds to learners’ comprehension and practice. We identified these threshold concepts as integrative and transformative, shaping learners’ perception and identity within the subject through reflective practice and discourse transformation. The Threshold Concept Framework (TCF) offers a perspective on learners’ progression over time and a focus on the evolution of their cognitive schemas, helping to delineate their learning trajectory. Additionally, understanding the cognitive underpinnings assists pharmacology educators in curricular reforms with innovative pedagogy for the effective translation of theoretical knowledge into rational pharmacotherapeutic approaches.
The TCF allows us to visualize the transition of learners from a naive or intuitive understanding of the discipline to more sophisticated ways of reasoning and practicing. After discovering the TCs, we observed that these concepts correspond to distinct stages of learning, encountered by pharmacology learners. These stages represent varying levels of cognitive processing in learning pharmacology: (a) “Subliminal”: Tacit understanding without full comprehension (b) “Pre-liminal”: Initial perception and approach (c) “Liminal”: Unique engagement in understanding (d) “Post-liminal”: Acquiring new knowledge, shaping future learning trajectories.Citation61–63 These stages reflect students’ variable positions of along the learning trajectory, resulting in distinct differences in TCs between novice and advanced learners, contrasting with expert viewpoints.
Having identified the landmarks of transition from a troublesome to a transformative journey, our next step is to deepen our understanding of how these thresholds shape learners’ thinking, reasoning, and practice in pharmacology. Moving iteratively between the empirical data and theoretical framework using abductive reasoning helped us discover unforeseen findings, embracing an ongoing creative process.Citation32,Citation39 The meaningful themes derived through data deconstruction fostered our observations and guided us without being constrained by preconceived notions/theoretical framework. An in-depth understanding of the identified TCs reveals how these complex concepts evolve within the cognitive framework of learners, impacting the acquisition, elaboration, and automation of relevant schemas that make up the knowledge base. By examining the cognitive processes involved in grasping and integrating these TCs, we gained insights into the transformative learning process of pharmacology.
Firstly, pharmacology education presents challenges, as we need to change how we think, understand deeply, and deal with the cognitive limitations of working memory when encountering new and troublesome content. Novices struggle to develop relevant cognitive schemas due to a lack of structured pedagogical frameworks considering the cognitive loads associated pharmacology concepts. Our study participants faced challenges in connecting disparate knowledge, particularly with drug names and nomenclature. This aligns with observations from another study which emphasized that simpler methods of recalling drug names (retrieval) can paradoxically hinder pharmacy students’ ability to remember them. Moreover, adding more details about drugs during study sessions doesn’t necessarily result in improved learning outcomes.Citation64 Likewise, our study demonstrated that inadequate instructional design exacerbates cognitive load, posing challenges for learners in understanding complex concepts such as drug mechanisms and signaling pathways. The inherent complexity of pharmacology concepts, along with learners’ mental effort, not only increases the intrinsic load but also exacerbates the extraneous load due to inadequate pedagogical design in presenting those concepts.Citation48,Citation65 Engaging with pharmacology’s TCs using low-level schemas may prompt learners to employ coping strategies, leading to “stuck places” at the subliminal to liminal stages, as described by Ellsworth, where understanding is akin to mimicry.Citation7,Citation66
As learners progress, certain threshold concepts require automation, thus subconsciously guiding behavior to evoke specific actions under particular conditions.Citation15 However, with a relatively low-level schema and insufficient knowledge base of pharmacology, this challenge is compounded, prolonging the already time-consuming process of schema automation.Citation48 For instance, the threshold nature of drug signaling pathways, attributed to their inherent complexity often keeps learners in a liminal phase for an extended period. The automation of these concepts is integral for effective therapeutic management, as revealed during our exploration, especially with novel drugs targeting specific chemotherapy checkpoints. Understanding signal transduction mechanics is vital for grasping personalized medicine, which targets specific signaling pathways up-regulated in certain cancers.Citation67 Customizing Bosutinib (signal transduction inhibitor) treatment for Chronic Myeloid Leukemia (CML) patients suggests the use of IF-THEN rules or decision-making frameworks to optimize outcomes and manage adverse events throughout therapy, considering individual patient characteristics and treatment responses.Citation68 Similarly, we observed that in fragmented curricula, students may focus on equation manipulation, like logarithmic transformations for pharmacokinetic calculations, as a plausible coping strategy,Citation69 rather than understanding underlying principles. This diverts their grasp from fully automating declarative knowledge into procedural skills.
Moving along the continuum of schema acquisition and automation for meaningful learning, elaboration connects existing knowledge to novel information,Citation59 developing a rich knowledge base and fostering a structural understanding of the subject matter.Citation15 The process of elaboration reveals hidden connections between new information and existing cognitive schemas, mirroring the “integrative” trait of TCF. This leads to the acquisition of higher-level schema and development of generalized, domain-specific knowledge structures.Citation6 Additionally, it provides valuable executive guidance for flexible problem-solving.Citation6,Citation26,Citation70,Citation71 Bereft of an adequate knowledge base, our participants considered numerous potential drug interactions to be challenging to remember, hindering their understanding of practical pharmacotherapy applications. With transformative learning, cognitive schemas evolve through these complex concepts, integrating knowledge into coherent higher-level schemas, enabling more effective application in various contexts.Citation6,Citation72 Advancements in medical education recognize curricula emphasizing learners’ knowledge base, in conjunction with self-regulated learning and critical thinking, but also the adaptability to uncertainty.Citation15,Citation73
As learners advance, transformations instigate with activities such integrating and restructuring/reconstructing knowledge at different generality levels based on the specific task situation and the learner’s current knowledge level, such as making generalizations on domain-specific schema.Citation74 In this study, we found that participants’ elaboration on the basic pharmacodynamics of drug-target interactions and identification of shared pathways or mechanisms helped in generalizing domain-specific knowledge, thus preparing them for evidence-based pharmacotherapy. This process of learners’ transition into the post-liminal phase, replaces coping mechanisms with more effective cognitive strategies crucially involving the deliberate use of cognitive schemas to effectively steer problem-solving behavior.Citation15 These strategies impose germane load and encourage schema construction and automation in learners.Citation75 Moreover, this provides advanced learners/experts with access to a diverse set of skills/repertoire readily available for tackling any present challenge, as described by Perkins as the epistemic base or fluency.Citation76,Citation77 These "ways of knowing" employ methods for justification, explanation, problem-solving, and inquiry. In pharmacology, a robust epistemic foundation is indispensable for rational pharmacotherapeutic management, encompassing complex concepts like pharmacokinetics, drug mechanisms, monitoring, and safety.
In the post-liminal phase, transformation continues as experts develop elaborate, automated schemas for conditions (‘illness scripts’) and therapies (‘therapy scripts’) informing clinical decisions.Citation78 These illness scripts reflect germane load optimization by enabling learners to organize complex information and enhancing disease diagnosis efficiency.Citation79 In contrast, novice learners and new clinicians encounter difficulties in developing and applying robust illness scripts.Citation80 Driven by the challenges specified, our research emphasizes decision-making for rational prescription writing as a crucial TC. Novice learners must assimilate vast knowledge on patient health, medications, drug interactions, adverse effects, and adhere to best practices and evidence-based approaches. While experts, who frequently automate their behavior, often struggle to articulate their decisions and the tacit heuristic knowledge that guides them, they inadvertently omit crucial information that would be beneficial for novices to understand.Citation15,Citation81 Physicians’ reliance on illness scriptsCitation70,Citation75,Citation79,Citation82 adds a threshold to learners’ prescribing decision-making, leading to biased clinical judgment and diversion from evidence-based practices. The teaching/training that overlooks these factors presents significant challenges for junior doctors when it comes to prescribing.Citation83
Further on, transformative learning actively engages learners in cognitive processing, fostering critical questioning and prompting the reconstitution of cognitive schemas,Citation14 which starts in working memory and integrates borrowed elements with prior knowledge in long-term memory,Citation84 encouraging learners to abandon or reshape preconceptions about concepts.Citation57 These refined schemas govern their clinical judgment and therapeutic decision-making, ensuring effective pharmacotherapeutic care, management, and patient safety.Citation10,Citation11 This conceptual restructuring empowers learners to enhance prescribing efficiency by integrating reflective decision-making for optimal therapeutic decisions.Citation85 In tandem, proactive restructuring, with periodic review leading to the discontinuation of unnecessary medications, embodies our identified TC of deprescribing, fostering reflexive practice for adaptive, patient-centered care.
This study unveils shifts in learners’ thinking and practice through the TCF, guiding discourse transformation toward enhanced understanding and application.Citation11,Citation13,Citation86 For instance, physician-patient communication is shaped by the foundation of evidence-based medicine and patient-centered care, prioritizing medical evidence and physician expertise and encouraging patient participation.Citation87–89 Our study identified non-adherence to medications and drug repurposing as threshold concepts in pharmacotherapy. Non-adherence stems from clinicians’ high expectations for patient compliance, while effective communication with patients maximizes drug repurposing’s potential by broadening existing drug utility based on evidence and human experiences. Overcoming these TCs, among others, reflects a transformative experience gained through practical skills, shaping discipline-specific narratives and arguments.Citation11,Citation13,Citation90
Practical implications
We emphasize the need for innovative teaching methods aligned with evidence-based instructional design principles aiming to improve learning effectiveness through a task-centric approach, the Four component instructional Design (4 C/ID) Model. The blueprint we developed aligns with CLT, reducing unnecessary cognitive load and facilitating schema construction and automation for deep understanding. We emphasize that understanding the epistemological characteristics within pharmacology is crucial for students to develop professional problem-solving skills.Citation91 Practical implications include enhancing pedagogy, curriculum design, and assessment as well as offering tailored-made professional development programs for pharmacology educators, benefiting both educators and learners in pharmacology education.
Limitations
The TCF has limitations, including challenges in articulating TCs, implementing curriculum changes, and addressing confounding variables and diverse student timelines.Citation86,Citation92 We worked to ensure a more rigorous, comprehensive, and systematic approach to TC identification through consensus-generating activities like the NGT, engaging stakeholders ranging from novice students to experts. This process revealed both overlapping and variable perspectives across stakeholders, and the top 6 identified concepts achieved consensus agreement. Our abductive analysis allowed for creative interpretations of empirical findings. We originally planned a transcontinental data collection approach but due to COVID-related constraints, focused on medical students from our university, limiting the sample size. We would need a broader and more diverse sample to make conclusions applicable on a wider scale. Nevertheless, our research provides valuable insights into TCs in pharmacology within our university context.
Conclusion
Using a transactional curriculum investigation approach, we explored participants’ pharmacology education experiences, unveiling transformative thresholds throughout their learning journey. This analysis sheds light on the levels of tacit comprehension across the preliminal, liminal, and postliminal phases while emphasizing the differences in TC identification between students and experts. Successfully navigating these thresholds led to profound and persistent transformations in thinking and practice throughout one’s career. Employing abductive reasoning allowed us to focus on the cognitive mechanisms underlying concept navigation.
The challenges learners face in grasping TCs in pharmacology, particularly in the evolution of their schemas, profoundly influences their epistemological transition and professional development, both in theory and practice. Navigating these thresholds of knowledge acquisition, elaboration, and automation mindfully, through the application of rational problem-solving cognitive strategies, could result in a transformative shift in their approach to pharmacotherapeutic management and patient safety. An instructional model that addresses these identified TCs and aligns them with schema evolution phases would facilitate a seamless learning experience in pharmacology, fostering the provision of quality education
Supplemental Material
Download PDF (214.7 KB)Acknowledgements
I, Faraz Khurshid, extend my heartfelt gratitude to my esteemed mentor, the late Prof. Jeroen van Merriënboer, for his invaluable guidance and support during the early stages of my project at Maastricht University. His insights continued to shape my work until his passing. The reflective approach and enduring support, alongside that of other distinguished professors and scholars from around the world, were instrumental in shaping the final outcome, and I deeply appreciate their contributions. Additionally, I am sincerely grateful to Dr. Gregg Maynard from Charles Sturt University for his expert guidance during the data analysis. I want to convey my thanks to Mr. Azhar Saud Ansari and Saad Azam, whose creative outputs and imaginative images helped bring to life the manuscript that was inspired by my own ideas. Without their contributions, the publication would not have been as rich and meaningful. I am grateful for their hard work and dedication, and for applying their graphic design skills to this important project. Finally, I extend my gratitude to all the participants whose busy schedules of education and practice did not deter them from generously contributing to the study. Their unwavering support was critical to the successful completion of this work. I am truly fortunate to have had such a fantastic group of individuals on this project, and I extend my sincerest appreciation to each and every one of them.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Additional information
Funding
References
- Perkins D. The many faces of constructivism. Educ Leadersh. 1999;57(3):6–11.
- Polanyi M. Logic and psychology. Am Psychol. 1968;23(1):27.
- Aronsson P, Booth S, Hägg S, et al. The understanding of core pharmacological concepts among health care students in their final semester. BMC Med Educ. 2015;15(1):235–235. doi:10.1186/s12909-015-0522-z.
- Land R, Meyer JH, Flanagan MT. Threshold Concepts in Practice. Vol. 68. Rotterdam: Sense Publishers; 2016.
- Kumar A, Vandana V, Aslami A. Introduction of case-based learning for teaching pharmacology in a rural medical college in Bihar. Natl J Physiol Pharm Pharmacol. 2016;6(5):427–430. doi:10.5455/njppp.2016.6.0411305052016.
- Kalyuga S. Knowledge elaboration: A cognitive load perspective. Learn Instr. 2009;19(5):402–410. doi:10.1016/j.learninstruc.2009.02.003.
- Kalyuga S. Schema acquisition and sources of cognitive load. In: Cognitive Load Theory. Cambridge: Cambridge University Press; 2010:48–64.
- van Merriënboer JJG, Sweller J. Cognitive load theory and complex learning: Recent developments and future directions. Educ Psychol Rev. 2005;17(2):147–177. doi:10.1007/s10648-005-3951-0.
- Davies P, Mangan J. Threshold concepts and the integration of understanding in economics. Studies in Higher Education. 2007;32(6):711–726. doi:10.1080/03075070701685148.
- Khurshid F, Bashir S, Noushad B. Prescription writing through the lens of the threshold concept framework: a narrative review. Res Dev Med Educ. 2020;9(1):11–11. doi:10.34172/rdme.2020.011.
- Meyer J, Land R. Threshold concepts and troublesome knowledge (2): epistemological considerations and a conceptual framework for teaching and learning. High Educ. 2005;49(3):373–388. doi:10.1007/s10734-004-6779-5.
- Walker G. A cognitive approach to threshold concepts. High Educ. 2013;65(2):247–263. doi:10.1007/s10734-012-9541-4.
- Meyer J, Land R. Threshold Concepts and Troublesome Knowledge: Linkages to Ways of Thinking and Practising within the Disciplines. Vol. 10. Improving Student Learning; Improving Student Learning Theory and Practice - 10 Years On. Oxford: Oxford Centre for Staff & Learning Development; 2003.
- Meyer J, Land R, Baillie C. Threshold Concepts and Transformational Learning. Vol. 42. Rotterdam: Sense Publishers Rotterdam; 2010:ix–xlii.
- Van Merriënboer JJ, Kirschner PA. Ten Steps to Complex Learning: A Systematic Approach to Four-Component Instructional Design. Abingdon: Routledge; 2017.
- Cousin G. Transactional curriculum inquiry: Researching threshold concepts. In: Cousin G, ed. Researching Learning in Higher Education: An Introduction to Contemporary Methods and Approaches. 2009:201–212. New York: Routledge.
- Delbecq AL, Van de Ven AH, Gustafson DH. Group Techniques for Program Planning: A Guide to Nominal Group and Delphi Processes. Glenview, IL: Scott, Foresman and Company; 1975:124.
- Archibald MM, Ambagtsheer RC, Casey MG, Lawless M. Using Zoom videoconferencing for qualitative data collection: perceptions and experiences of researchers and participants. Int J Qual Methods. 2019;18:160940691987459. doi:10.1177/1609406919874596.
- Wright AL, Gilmore A. Threshold concepts and conceptions: Student learning in introductory management courses. J Manage Educ. 2012;36(5):614–635. doi:10.1177/10525629114294.
- Humphrey-Murto S, Varpio L, Gonsalves C, Wood TJ. Using consensus group methods such as Delphi and Nominal Group in medical education research. Med Teach. 2017;39(1):14–19. doi:10.1080/0142159x.2017.1245856.
- Foth T, Efstathiou N, Vanderspank-Wright B, et al. The use of Delphi and Nominal Group Technique in nursing education: A review. Int J Nurs Stud. 2016;60:112–120. doi:10.1016/j.ijnurstu.2016.04.015.
- Murphy M, Black N, Lamping D, et al. Consensus development methods, and their use in clinical guideline development. Health Technol Assess. 1998;2(3):i-88. doi:10.3310/hta2030.
- Muijeen K, Kongvattananon P, Somprasert C. The key success factors in focus group discussions with the elderly for novice researchers: a review. JHR. 2020;34(4):359–371. doi:10.1108/JHR-05-2019-0114.
- Krueger RA. Participants in a Focus Group. In: Richard A, Krueger MAC, eds. Focus Groups-A Practical Guide for Applied Research. 5th ed. Thousand Oaks, CA: SAGE Publication Inc.; 2014:63–81, chap 4.
- Friese S. Qualitative Data Analysis with ATLAS.ti. Thousand Oaks, CA: Sage; 2019.
- Barradell S, Peseta T. Promise and challenge of identifying threshold concepts: a cautionary account of using transactional curriculum inquiry. J Furth High Educ. 2016;40(2):262–275. doi:10.1080/0309877X.2014.971105.
- Barradell S. The identification of threshold concepts: a review of theoretical complexities and methodological challenges. High Educ. 2013;65(2):265–276. doi:10.1007/s10734-012-9542-3.
- Timmermans JA, Meyer JHF. A framework for working with university teachers to create and embed ‘Integrated Threshold Concept Knowledge’ (ITCK) in their practice. International Journal for Academic Development. 2019;24(4):354–368. doi:10.1080/1360144X.2017.1388241.
- Baillie C, Bowden JA, Meyer JHF. Threshold capabilities: threshold concepts and knowledge capability linked through variation theory. High Educ. 2013;65(2):227–246. doi:10.1007/s10734-012-9540-5.
- Barradell S, Fortune T. Bounded - the neglected threshold concept characteristic. Innovations in Education and Teaching International. 2020;57(3):296–304. doi:10.1080/14703297.2019.1657034.
- Van Breda A. Steps to analysing multiple-group NGT data. Soc Work Pract Res. 2005;17(1):1–14.
- Tavory I, Timmermans S. Abductive Analysis: Theorizing Qualitative Research. Chicago, IL: University of Chicago Press; 2014.
- Thompson J. A guide to abductive thematic analysis. TQR. 2022;27:1410–1421. doi:10.46743/2160-3715/2022.5340.
- Boyatzis RE. Transforming Qualitative Information: Thematic Analysis and Code Development. New Delhi: Sage Publications; 1998.
- Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. 2006;3(2):77–101. doi:10.1191/1478088706qp063oa.
- Charmaz K. Grounded Theory in the 21st Century: Applications for Advancing Social Justice Studies. New Delhi: Sage Publications Ltd; 2005.
- Saldaña J. The Coding Manual for Qualitative Researchers. 2021:1–440. London: Sage.
- Kinchin I, Cabot LB, Hay DB. Visualising expertise: towards an authentic pedagogy for higher education. Teach Higher Educ. 2008;13(3):315–326. doi:10.1080/13562510802045345.
- Timmermans S, Tavory I. Theory construction in qualitative research: from grounded theory to abductive analysis. Sociol Theory. 2012;30(3):167–186. doi:10.1177/0735275112457914.
- Hesse-Biber SN, Leavy P. Focus group interviews. In: The Practice of Qualitative Research. 2011:163–192. London: Sage.
- Sweller J. Cognitive load theory, learning difficulty, and instructional design. Learn Instr. 1994;4(4):295–312. doi:10.1016/0959-4752(94)90003-5.
- Labra O, Castro C, Wright R, Chamblas I. Thematic analysis in social work: a case study. Global Social Work Cutting Edge Iss Crit Reflect. 2020;10(6):1–20.
- Smith J, Firth J. Qualitative data analysis: the framework approach. Nurse Res. 2011;18(2):52–62. doi:10.7748/nr2011.01.18.2.52.c8284.
- Byrne D. A worked example of Braun and Clarke’s approach to reflexive thematic analysis. Qual Quant. 2022;56(3):1391–1412. doi:10.1007/s11135-021-01182-y.
- Atkinson P. Ethnography: Principles in Practice. London: Routledge; 2007.
- Sweller J. Cognitive load during problem solving: effects on learning. Cogn Sci. 1988;12(2):257–285. doi:10.1207/s15516709cog1202_4.
- Perkins D. Beyond understanding. Threshold Concepts within the Disciplines. Rotterdam: Brill Sense; 2008:1–19.
- Sweller J. Cognitive load theory. Psychology of Learning and Motivation. San Diego, CA: Elsevier; 2011:37–76.
- Cowan N. The magical number 4 in short-term memory: a reconsideration of mental storage capacity. Behav Brain Sci. 2001;24(1):87–114. doi:10.1017/s0140525x01003922.
- Miller GA. The magical number seven, plus or minus two: some limits on our capacity for processing information. Psychol Rev. 1956;101(2):343–352. doi:10.1037/h0043158.
- Peterson L, Peterson MJ. Short-term retention of individual verbal items. J Exp Psychol. 1959;58(3):193–198. doi:10.1037/h0049234.
- Van Merriënboer JJG, Paas FG. Automation and schema acquisition in learning elementary computer programming: implications for the design of practice. Comput Human Behav. 1990;6(3):273–289. doi:10.1016/0747-5632(90)90023-A.
- Kleinsinger F. The unmet challenge of medication nonadherence. Perm J. 2018;22:18–033. doi:10.7812/TPP/18-033.
- Lampert SL, Feldman ECH, Durkin LK, Davies WH, Greenley RN. Medication adherence among emerging adults: the influence of provider communication and patient personality. Child Health Care. 2022;51(1):101–117. doi:10.1080/02739615.2021.1971986.
- Kim J, Combs K, Downs J, Tillman F. Medication adherence: the elephant in the room. US Pharm. 2018;43(1):30–34.
- Frerejean J, van Merriënboer JJ, Condron C, Strauch U, Eppich W. Critical design choices in healthcare simulation education: a 4C/ID perspective on design that leads to transfer. Adv Simul. 2023;8(1):5. doi:10.1186/s41077-023-00242-7.
- Pinnock R, Anakin M, Jouart M. Clinical reasoning as a threshold skill. Med Teach. 2019;41(6):683–689. doi:10.1080/0142159X.2019.1569754.
- Kalyuga S, Plass JL. Evaluating and managing cognitive load in games. In: Handbook of Research on Effective Electronic Gaming in Education. London: IGI Global; 2009:719–737.
- Van Merriënboer J. How people learn. In: The Wiley Handbook of Learning Technology. 2016:15–34. Hoboken, NJ: John Wiley & Sons, Inc.
- Thompson R. A Vygotskian Exploration of Medical Students’ Critical Thinking within Threshold Concept Liminal Spaces. Sydney: UNSW Sydney; 2019. doi:10.26190/unsworks/21580.
- Meyer JH, Land R, Davies P. Threshold concepts and troublesome knowledge (4): Issues of variation and variability. In: Threshold Concepts within the Disciplines. Rotterdam: Brill Sense; 2008:59–74.
- Meyer JH. Threshold Concepts within the Disciplines. Rotterdam: Sense Publishers; 2008.
- McCune V, Hounsell D. The development of students’ ways of thinking and practising in three final-year biology courses. High Educ. 2005;49(3):255–289. doi:10.1007/s10734-004-6666-0.
- Terenyi J, Anksorus H, Persky AM. Optimizing the spacing of retrieval practice to improve pharmacy students’ learning of drug names. Am J Pharm Educ. 2019;83(6):7029. doi:10.5688/ajpe7029.
- Sweller J, van Merriënboer JJ, Paas F. Cognitive architecture and instructional design: 20 years later. Educ Psychol Rev. 2019;31(2):261–292. doi:10.1007/s10648-019-09465-5.
- Ellsworth E. Teaching Positions: Difference, Pedagogy, and the Power of Address. 1st ed. New York, NY: Teachers College Press; 1997.
- Emtage L, Bradbury L, Coleman N, Devenport D, Nietzel A, Grew J. Cell signaling pathways: a case study approach. CS. 2016;3. doi:10.24918/cs.2016.9.
- Zaker E, Nouri N, Sorkhizadeh S, Ghasemirad H, Hajijafari AH, Zare F. The importance of personalized medicine in chronic myeloid leukemia management: a narrative review. Egypt J Med Hum Genet. 2023;24(1):31. doi:10.1186/s43042-023-00411-3.
- Persky AM, Robinson JD. Moving from novice to expertise and its implications for instruction. Am J Pharm Educ. 2017;81(9):6065. doi:10.5688/ajpe6065.
- Kalyuga S. Enhancing transfer by learning generalized domain knowledge structures. Eur J Psychol Educ. 2013;28(4):1477–1493. doi:10.1007/s10212-013-0176-3.
- Rumelhart DE, Norman DA. Accretion, tuning and restructuring: Three modes of learning. 1976. https://www.dsoergel.com/UBLIS571DS-06.1a-1Reading10RumelhartAccretionTuningAndRestructuring.pdf
- Janssen-Noordman A, Merriënboer JJ, Van der Vleuten CP, Scherpbier AJ. Design of integrated practice for learning professional competences. Med Teach. 2006;28(5):447–452. doi:10.1080/01421590600825276.
- McHugh D, Yanik AJ, Mancini MR. An innovative pharmacology curriculum for medical students: promoting higher order cognition, learner-centered coaching, and constructive feedback through a social pedagogy framework. BMC Med Educ. 2021;21(1):90. doi:ARTN 90 doi:10.1186/s12909-021-02516-y.
- van Merriënboer JJG. Perspectives on problem solving and instruction. Comput Educ. 2013;64:153–160. doi:10.1016/j.compedu.2012.11.025.
- Young JQ, Van Merrienboer J, Durning S, Ten Cate O. Cognitive load theory: implications for medical education: AMEE Guide No. 86. Med Teach. 2014;36(5):371–384. doi:10.3109/0142159X.2014.889290.
- Land R, Rattray J, Vivian P. Learning in the liminal space: a semiotic approach to threshold concepts. High Educ. 2014;67(2):199–217. doi:10.1007/s10734-013-9705-x.
- Perkins D. Constructivism and Troublesome knowledge. In: Meyer JHF, Land R, editors. Overcoming Barriers to Student Understanding: Threshold Concepts and Troublesome Knowledge. London and New York. Routledge; 2006: 33–47.
- Croskerry P. Clinical cognition and diagnostic error: applications of a dual process model of reasoning. Adv in Health Sci Educ. 2009;14(S1):27–35. doi:10.1007/s10459-009-9182-2.
- van Merriënboer JJG, Sweller J. Cognitive load theory in health professional education: design principles and strategies. Med Educ. 2010;44(1):85–93. doi:10.1111/j.1365-2923.2009.03498.x.
- Fall LH, English R, Fulton TB, et al. Thinking slow more quickly: development of integrated illness scripts to support cognitively integrated learning and improve clinical decision-making. Med Sci Educ. 2021;31(3):1005–1007. doi:10.1007/s40670-021-01293-z.
- Frerejean J, van Geel M, Keuning T, Dolmans D, van Merriënboer JJ, Visscher AJ. Ten steps to 4C/ID: training differentiation skills in a professional development program for teachers. Instr Sci. 2021;49(3):395–418. doi:10.1007/s11251-021-09540-x.
- Strasser J, Gruber H. Learning processes in the professional development of mental health counselors: knowledge restructuring and illness script formation. Adv Health Sci Educ Theory Pract. 2015;20(2):515–530. doi:10.1007/s10459-014-9545-1.
- Omer U, Danopoulos E, Veysey M, Crampton P, Finn G. A rapid review of prescribing education interventions. Med Sci Educ. 2021;31(1):273–289. doi:10.1007/s40670-020-01131-8.
- Kalyuga S. Enhancing instructional efficiency of interactive e-learning environments: a cognitive load perspective. Educ Psychol Rev. 2007;19(3):387–399. doi:10.1007/s10648-007-9051-6.
- Mamede S, Schmidt HG. The twin traps of overtreatment and therapeutic nihilism in clinical practice. Med Educ. 2014;48(1):34–43. doi:10.1111/medu.12264.
- Nicola-Richmond K, Pépin G, Larkin H, Taylor C. Threshold concepts in higher education: a synthesis of the literature relating to measurement of threshold crossing. Higher Educ Res Dev. 2018;37(1):101–114. doi:10.1080/07294360.2017.1339181.
- Street RL. The many “Disguises” of patient-centered communication: problems of conceptualization and measurement. Patient Educ Couns. 2017;100(11):2131–2134. doi:10.1016/j.pec.2017.05.008.
- Masic I, Miokovic M, Muhamedagic B. Evidence based medicine–new approaches and challenges. Acta Inform Med. 2008;16(4):219. doi:10.5455/aim.2008.16.219-225.
- Liao D, Kelpinski LF, Guntzviller LM. Using normative rhetorical theory to identify dilemmas and responses in internal medicine patient-provider communication. Health Commun. 2023;38(8):1581–1590. doi:10.1080/10410236.2021.2021691.
- Mortari L, Silva R. Analyzing how discursive practices affect physicians’ decision-making processes: A phenomenological-based qualitative study in critical care contexts. INQUIRY: The Journal of Health Care Organization, Provision, and Financing. 2017;54:0046958017731962.
- Perkins DN. Epistemic games. International Journal of Educational Research. 1997;27(1):49–61. doi:10.1016/S0883-0355(97)88443-1.
- Meyer J, Land R. Overcoming Barriers to Student Understanding: Threshold Concepts and Troublesome Knowledge. New York, NY: Routledge; 2006.