
Abstract
Objective: To examine the relation between the consumption or avoidance of meat and psychological health and well-being.
Methods: A systematic search of online databases (PubMed, PsycINFO, CINAHL Plus, Medline, and Cochrane Library) was conducted for primary research examining psychological health in meat-consumers and meat-abstainers. Inclusion criteria were the provision of a clear distinction between meat-consumers and meat-abstainers, and data on factors related to psychological health. Studies examining meat consumption as a continuous or multi-level variable were excluded. Summary data were compiled, and qualitative analyses of methodologic rigor were conducted. The main outcome was the disparity in the prevalence of depression, anxiety, and related conditions in meat-consumers versus meat-abstainers. Secondary outcomes included mood and self-harm behaviors.
Results: Eighteen studies met the inclusion/exclusion criteria; representing 160,257 participants (85,843 females and 73,232 males) with 149,559 meat-consumers and 8584 meat-abstainers (11 to 96 years) from multiple geographic regions. Analysis of methodologic rigor revealed that the studies ranged from low to severe risk of bias with high to very low confidence in results. Eleven of the 18 studies demonstrated that meat-abstention was associated with poorer psychological health, four studies were equivocal, and three showed that meat-abstainers had better outcomes. The most rigorous studies demonstrated that the prevalence or risk of depression and/or anxiety were significantly greater in participants who avoided meat consumption.
Conclusion: Studies examining the relation between the consumption or avoidance of meat and psychological health varied substantially in methodologic rigor, validity of interpretation, and confidence in results. The majority of studies, and especially the higher quality studies, showed that those who avoided meat consumption had significantly higher rates or risk of depression, anxiety, and/or self-harm behaviors. There was mixed evidence for temporal relations, but study designs and a lack of rigor precluded inferences of causal relations. Our study does not support meat avoidance as a strategy to benefit psychological health.
Introduction
Background
Vegetarianism for ethical or religious reasons predates modern history (Leitzmann Citation2014; Spencer Citation1995; Whorton Citation1994). Yet the common practice of abstaining from animal flesh in the pursuit of health per se is a recent phenomenon that began in the nineteenth and early twentieth centuries (Porphyry Citation1823; Roe Citation1986; Whorton Citation1994). Given that a century ago nutrition science was in its infancy, the earliest arguments for the superiority of “meat-free” diets for health were shaped more by religious and moral sentiments than by empirical evidence (Whorton Citation1994). Nevertheless, as investigations of human nutrition and disease expanded in the twentieth century, vegetarianism for health gained scientific credibility to augment its traditional moral and ethical status (Rosenfeld Citation2018; Ruby Citation2012).
However, in the past few decades, research on the health effects of meat-abstention has become increasingly contradictory. For example, despite the fact that animal products, such as red meat (e.g., beef or lamb), provide a wide range of essential nutrients and bioactive substances (Neumann et al. Citation2003, Citation2007; Williams Citation2007), researchers reported potential health benefits associated with avoiding meat and that vegetarian diets may be used to prevent or treat disease (Kahleova, Levin, and Barnard Citation2018; Key et al. Citation1999; Singh, Sabaté, and Fraser Citation2003; Tong et al. Citation2019; Viguiliouk et al. Citation2019). As a consequence, the 2016 Position Statement of the Academy of Nutrition and Dietetics stated, “appropriately planned vegetarian, including vegan, diets are healthful, nutritionally adequate, and may provide health benefits for the prevention and treatment of certain diseases” (Melina, Craig, and Levin Citation2016, 1970).
In contrast, while it is well-established that the mortality of vegetarians compares positively with the general population (Appleby et al. Citation2016; Appleby and Key Citation2016), several reports demonstrated that there were no differences in mortality when vegetarians were compared to meat-consumers with similar socio-demographic characteristics (Appleby et al. Citation2016; Appleby and Key Citation2016; Chang-Claude et al. Citation2005). Thus, while some studies are suggestive of a reduction in mortality associated with vegetarianism, the larger body of evidence suggests that the health benefits associated with vegetarianism may not be due to the avoidance of meat per se, but other “lifestyle” factors associated with socio-economic status, such as adequate levels of physical activity (Archer, Lavie, and Hill Citation2018a), low alcohol and drug consumption (O’Keefe et al. Citation2018), or the avoidance of tobacco products.
Moreover, and in contrast to the positive associations between health and vegetarianism (Appleby and Key Citation2016; Dinu et al. Citation2017; Singh, Sabaté, and Fraser Citation2003; Viguiliouk et al. Citation2019), recent results suggest that individuals who abstain from meat and/or other animal-based foods may suffer from nutritional deficiencies (e.g., vitamins B12 and D, ω‐3 fatty acids, calcium, iron, and zinc; Craig Citation2010; Dwyer Citation1991) with concomitant poorer physical health (Appleby et al. Citation2007; Burkert et al. Citation2014b; Cofnas Citation2019; Iguacel et al. Citation2019). Furthermore, there is an emerging body of evidence that meat-abstention is linked to mental disorders (Perica and Delaš Citation2011; Young and Conquer Citation2005) and poorer psychological well-being (Baines, Powers, and Brown Citation2007; Hibbeln et al. Citation2018; Matta et al. Citation2018; Michalak, Zhang, and Jacobi Citation2012; Nezlek, Forestell, and Newman Citation2018; Rosenfeld Citation2018). Specifically, when compared to those who consume meat, vegetarians are more likely to suffer from or be diagnosed with major depression (Baines, Powers, and Brown Citation2007; Hibbeln et al. Citation2018; Jacka et al. Citation2012) and anxiety (Baines, Powers, and Brown Citation2007; Bas, Karabudak, and Kiziltan Citation2005), and are more likely to attempt self-harm (e.g., suicide) (Baines, Powers, and Brown Citation2007; Neumark-Sztainer et al. Citation1997; Perry et al. Citation2001).
However, the evidence linking vegetarianism with mental disorders is not unequivocal. In 2010 and 2015, investigators found that with respect to some facets of mental health assessment, vegetarians were healthier than meat-consumers (Beezhold et al. Citation2015; Beezhold, Johnston, and Daigle Citation2010).
Equivocal results and public health
Recently, Johnston et al. (Johnston et al. Citation2019) and Carroll and Doherty (Carroll and Doherty Citation2019) suggested that the evidence supporting public health recommendations to limit or eliminate meat consumption was based on questionable research and “inappropriate analyses” (Carroll and Doherty Citation2019, 767). This debate and the ever-increasing body of contrasting and conflicting results represent a challenge for both clinicians and public policy architects. Yet more importantly, equivocal and potentially biased research on meat-consumption has contributed to the growing confusion and incredulousness surrounding the value of nutrition science (Archer and Lavie Citation2019a, Citation2019b; Archer, Lavie, and Hill Citation2018b; Archer, Pavela, and Lavie Citation2015; Rowe and Alexander Citation2017).
The extant literature suggests that there are numerous factors that may explain the contradictory associations of meat-abstention and health. These include variations in research design, recruitment and sampling strategies (Baines, Powers, and Brown Citation2007; Matta et al. Citation2018; Michalak, Zhang, and Jacobi Citation2012), the disparity between self-reported and actual dietary intake (Archer, Marlow, and Lavie Citation2018d; Archer, Pavela, and Lavie Citation2015), the lack of validity of assessment protocols or metrics employed for exposures and outcomes (e.g., diagnosed conditions vs. subjective perceptions), and lack of understanding and control for confounding variables and/or effect modifiers.
Another important and oft-cited factor is the definition and characterization of vegetarians and/or those who abstain from meat consumption (Baines, Powers, and Brown Citation2007; Timko, Hormes, and Chubski Citation2012). For example, the comprehensive term “vegetarian” may be used to describe individuals who avoid only red meat (e.g., beef), avoid both red and white meat (e.g., pork, poultry) or those who simply consume predominantly plant-based diets. Furthermore, investigators frequently subdivide vegetarians into several groups categorized by the types of foods they exclude. While no definition is definitive and categories vary significantly, “vegans” exclude all foods and beverages derived from animals (e.g., fish, eggs, dairy, or meat) and may also avoid using any animal-based products (e.g., leather clothing). Ovo-lacto vegetarians consume no meat but will eat eggs and dairy, whereas pescatarians eat fish but not red meat or poultry, and flexitarians consume a predominantly plant-based diet while occasionally consuming meat. These inconsistent and intersecting definitions in concert with self-reported dietary status may lead to misclassification because there is a clear and important distinction between merely reporting that one avoids meat and actual meat-abstention. In other words, from a scientific perspective, it is clear that self-reported dietary intake is not the equivalent of actual dietary intake (Archer, Lavie, and Hill Citation2018b; Archer, Marlow, and Lavie Citation2018d; Archer, Pavela, and Lavie Citation2015).
Meat-abstention and mental health: the need for clarity
In 2017, the World Health Organization (WHO) reported that mental illness was the leading cause of disability worldwide (WHO Citation2017), and has a major impact on cardiovascular diseases (i.e., the leading cause of mortality globally; Lavie et al. Citation2016; O’Keefe, O’Keefe, and Lavie Citation2019). The WHO investigators estimated that over 300 million people suffered from depression (4.4% of the global population) and over 260 million people (3.6% of the global population) suffered from anxiety (Friedrich Citation2017; Kessler et al. Citation2005). These estimates reflected a substantial increase in the number of people living with mental disorders and illnesses over the past two decades (Lancet Citation2015; WHO Citation2017).
Given the global increase in psychological disorders (Lancet Citation2015; WHO Citation2017) in concert with increments in the advocacy and practice of vegetarianism (Leitzmann Citation2014; Statista 2019; Willett et al. Citation2019), there is a need to clarify the relation between meat-abstention and psychological health. Nevertheless, in addition to the inconsistent classification of vegetarians in research settings, there are limitations to the extant definitions and data on psychological outcomes. For example, the WHO defines mental health as “a state of well-being in which every individual realizes his or her own potential, can cope with the normal stresses of life, can work productively and fruitfully, and is able to make a contribution to her or his community” (WHO Citation2019). While this broad characterization provides a goal for individuals and the societies in which they live, it is extremely limited in its research and practical applications. More importantly, while some investigators examining diet-disease relations rely on physician-diagnosed disorders based on criteria from the Diagnostic and Statistical Manual of Mental Disorders (DSM-V; APA Citation2013; e.g., see (Michalak, Zhang, and Jacobi Citation2012)), others rely exclusively on self-reported mental health or subjective scales with untested validity. These conceptual and measurement issues lead to classification errors, ambiguous findings, and limited cross-study analyses.
Given the inconsistent and contradictory nature of the extant research, the objective of this systematic review was to formally but concisely identify the outcomes, strengths, limitations, and flaws in the scientific literature on the relation between the consumption or avoidance of meat and mental health, with a focus on depression, anxiety, and a limited number of secondary variables (e.g., self-harm). To avoid inconsistent definitions of vegetarianism, our analysis sought to capture studies that clearly differentiated between individuals who reported consuming meat and those reporting to be meat-abstainers, while acknowledging that the overall dietary patterns exhibited by both groups (and most humans) are varied.
Methods
Search strategy
Five online databases (PubMed, PsycINFO, CINAHL Plus, Medline with full text, and Cochrane Library) were searched using a broad set of keywords for primary research that examined psychological health in meat-consumers and meat-abstainers. The search included all papers published up to and including March 2019. The keywords and search strategy can be found in Supporting Information. The search strategy was created by the lead investigator; and two, two-person teams independently conducted the searches. Titles and abstracts of potentially relevant articles were independently identified and screened by both teams. The search strategy included examining reference lists from previous reviews and research papers. Initial search results were imported into reference-managing software (EndNote X9, Clarivate Analytics, 2019).
After duplicate articles were excluded, full texts of potentially relevant articles were obtained and critically assessed by both two-person teams and the lead investigator working independently. After this assessment, the teams and lead investigator met to arrive at a consensus on the inclusion/exclusion criteria for each paper (e.g., psychological assessment, strict definitions of dietary intake, etc.). Disputes were adjudicated by discussion with the final decision made by the lead investigator (UD). Consensus was obtained for all included articles.
Study inclusion criteria
This review sought to identify primary studies that examined the relation between meat-abstention and psychological health in humans, 10–99 years of age, with a primary focus on depression, anxiety, and a limited number of secondary variables. This focus was necessary because many psychological outcomes are vague, difficult to quantify (e.g., disordered eating, self-esteem), or are inherently biased against individuals who do not follow current norms (e.g., vegans). For example, in western, industrialized nations meat consumption is the social and economic norm. Therefore, the non-normative dietary exclusions espoused by vegans and strict vegetarians may lead to inflated or illusory rates of psychological dysfunction. For example, it is well-established that vegetarianism may be used as a strategy to mask disordered eating and that the endorsement of vegetarianism is highest in females with severe eating pathology (Klopp, Heiss, and Smith Citation2003; Zuromski et al. Citation2015). Given this evidence, self-reported vegetarianism per se has been posited to be a proxy for mental illness (Klopp, Heiss, and Smith Citation2003). Thus, we chose not to include outcomes that were less well-defined or difficult to quantify such as personality characteristics (e.g., neuroticism), or disordered eating and related phenomena (e.g., orthorexia), to achieve more definitive results and conclusions on the relation between meat-consumption and mental health.
All study designs were eligible (e.g., cross-sectional, retrospective, prospective, case control, randomized controlled trial (RCT), longitudinal). Studies were included if (1) they were written in English language, (2) the authors provided a clear distinction between participants who reported eating meat (i.e., meat-consumers; e.g., omnivores) and those who avoided meat consumption (i.e., meat-abstainers; e.g., vegans, vegetarians), and (3) included data on psychological health. Given the heterogeneity of definitions of vegetarianism or meat-avoidance, at times it was necessary to contact the authors of a particular study to gain further clarification.
Our goal was to create a comprehensive, yet rigorous and concise review. The eligible psychological outcomes were divided into primary and secondary categories based on the frequency with which they were examined in the relevant literature ().
Text Box 1. Included psychological outcomes.
Study exclusion criteria
Non-English studies were excluded, and studies examining meat consumption as a continuous or multi-level variable were excluded due to the failure of food frequency questionnaires (FFQs) and other self-report methods to accurately quantify actual dietary intake (Archer, Hand, and Blair Citation2013; Archer, Lavie, and Hill Citation2018b; Archer, Marlow, and Lavie Citation2018d; Archer, Pavela, and Lavie Citation2015; Schoeller et al. Citation2013).
Data extraction
Data extraction was conducted by both teams. The information extracted included study characteristics (e.g., citation, design, population, number of participants, age, etc.), psychological health outcomes, definition of meat-consumers/meat-abstainers, and key findings. The reviewers were not blinded and had full access to paper details, such as authors, affiliations, and journals during data extraction and compilation. The extraction tables were examined for accuracy and completeness by the lead investigator (UD). Once compiled, information from the selected studies was transferred to an “Evidence Summary Table” ().
Table 1. Summary table.
Methodologic rigor: risk of bias assessment and limitations
Quality assessments in systematic reviews necessitate the critical appraisal of multiple factors and domains within and between the included studies. To reduce the potential for biases in the appraisal process, final adjudication, and communication of results, reviewers’ judgments must be independent and constrained via a standardized protocol. As such, each study included in our review was assessed for methodologic rigor via qualitative critiques and quantitative analyses of the risk of bias, validity of interpretation, and confidence in findings by two investigators. These investigators worked independently while employing a 100-point scale of predetermined criteria that was specifically developed for this review via an amalgam of multiple tools and checklists (Hong et al. Citation2018; Weightman et al. Citation2004).
Specifically, each study was evaluated for design, sampling and recruitment biases, specification of outcome (i.e., dietary and psychological assessments), analysis of outcome (e.g., statistical design), validity of interpretation and communication of results (e.g., were the conclusions supported by the results). The 100-point scale used herein provided a standard procedure for both the evaluative process and subsequent communication of results while allowing the extensibility necessary to accommodate the interdisciplinary nature of the research question and the heterogeneity across the studies (Please see Supporting Information).
The studies were ranked and placed in five categories based on their score. Higher scores indicated greater methodologic rigor: scores 90–100 indicated high rigor, low risk of bias, and high confidence in results; scores 60–89 indicated moderate rigor and risk of bias, and modest confidence in results; scores 40–59 indicated a moderate-to-high risk of bias, and moderate-to-low rigor and confidence in results; scores 20–39 indicated a high risk of bias, and low rigor and confidence in results; and scores 0–19 indicated a severe risk of bias and very low rigor and confidence in results.
Results
Description of studies
The initial search resulted in 7102 potentially relevant articles. After de-duplication, the tiles and abstracts of 6840 papers were screened for inclusion/exclusion criteria. This resulted in 100 full-text articles which were read fully and critically assessed. This qualitative analysis resulted in 18 papers that met the inclusion/exclusion criteria. These included 16 cross-sectional, 1 mixed cross-sectional and longitudinal study, and 1 RTC. The total sample included 160,257 participants (85,843 females and 73,232 males) with 149,559 meat-consumers and 8584 meat-abstainers from geographic regions including Europe, Asia, North America, and Oceania. The sample sizes ranged from 38 to 90,380 participants with an age-range from 11 to 96 years. The articles were published from 1997 to January 2019.
As per PRISMA statement (Preferred Reporting Items for Systematic Review and Meta-Analyses; Moher et al. 2009), results from each stage of the review are displayed in .
Figure 1. PRISMA flow-chart: search results.
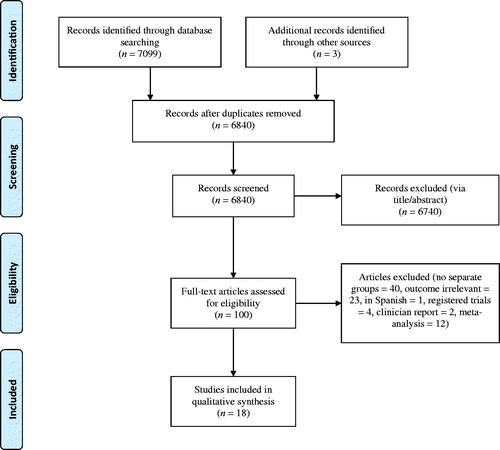
provides a summary of the studies included in the review in alphabetical order.
Methodologic rigor analysis
The results of the critical appraisal of methodologic rigor and concomitant confidence in results as well as significant strengths, limitations, and flaws are presented in Supporting Information. Analyses revealed that the studies ranged from high to low rigor with high to very low confidence in results, respectively. Results are presented in rank-order of rigor beginning with the most rigorous study. Inter-class correlations between reviewers were very high (ICC = 0.978; 95% CI: 0.942–0.992, p < .001).
General critique
The studies were placed in five categories based on their score for methodologic rigor. Two of the 18 selected studies had a low risk of bias; 5 had moderate risk; 4 had moderate-to-high risk; 4 had a high risk, and 3 studies had a severe risk of bias. The quality of the study appeared to affect the outcome of the study.
There were numerous issues that reduced the confidence in the published results. As detailed in our discussion, these issues included cross-sectional design, non-representative sampling, biased recruitment, the use of subjective (i.e., self-reported) dietary and psychological data, the failure to account for social desirability and observer-expectancy effects (e.g., reactivity), the failure to collect data on actual dietary intake, and statistical, interpretive, and communication errors such as the failure to correct for multiple comparisons, recognize regression to the mean, and the inappropriate use of causal language.
Summary of results
Primary outcomes: depression, anxiety, and related symptoms
Fourteen of the 18 studies examined depression, anxiety, and/or related symptoms (see ). Independent of methodologic rigor, 7 of the 14 studies found a higher prevalence or risk in participants who avoided meat consumption (Baines, Powers, and Brown Citation2007; Forestell and Nezlek Citation2018; Hibbeln et al. Citation2018; Lindeman Citation2002; Matta et al. Citation2018; Michalak, Zhang, and Jacobi Citation2012; Stokes, Gordon, and DiVasta Citation2011), 3 studies found no group differences (Beezhold and Johnston Citation2012; Perry et al. Citation2001; Timko, Hormes, and Chubski Citation2012), 2 studies demonstrated mixed results (e.g., higher rates in females only; Bas, Karabudak, and Kiziltan Citation2005; Lavallee et al. Citation2019), and 2 of the 14 studies found a higher prevalence or risk in meat-consumers (Beezhold et al. Citation2015; Beezhold, Johnston, and Daigle Citation2010; ). The four most rigorous studies demonstrated that the prevalence or risk of depression and/or anxiety (or related symptoms) was significantly greater in participants who avoided meat consumption (Baines, Powers, and Brown Citation2007; Hibbeln et al. Citation2018; Matta et al. Citation2018; Michalak, Zhang, and Jacobi Citation2012). The results of the five least rigorous studies were less clear; two studies demonstrated that meat-consumers had a higher risk or prevalence of depression and anxiety (Beezhold et al. Citation2015; Beezhold, Johnston, and Daigle Citation2010), one study found no group differences (Beezhold and Johnston Citation2012), and two found that meat-consumers had a lower risk or prevalence (Lindeman Citation2002; Stokes, Gordon, and DiVasta Citation2011).
Table 2. Primary outcomes.
The most rigorous study reviewed, Michalak, Zhang, and Jacobi (Citation2012), found a clear relation between the avoidance of meat and depression and anxiety in both a representative sample of German adults (n = 4181; including 3872 non-vegetarians and 54 “complete vegetarians”) and a socio-demographically matched subsample of non-vegetarians (n = 242). Meat-abstainers (i.e., “complete vegetarians”) had 1-month, 12-month, and lifetime prevalence of unipolar depressive disorders of 7.4%, 24.1%, and 35.2%, respectively. Conversely, the prevalence was substantially lower in meat-consumers: 6.3%, 11.9%, and 19.1% in the full sample, and 5.0%, 10.3%, and 20.7% in the matched sample. When comparing the “complete vegetarians” to the “matched non-vegetarians,” the Odds Ratios for 1-month, 12-month, and lifetime prevalence were 1.53 (95% CI: 0.48–4.95); 2.75 (95% CI: 1.30–5.82); and 2.09 (95% CI: 1.10–3.95), respectively. As the authors stated, “Prevalence rates of the complete vegetarians are nearly 15% higher than of the non-vegetarians” (Michalak, Zhang, and Jacobi Citation2012, 5).
The 1-month, 12-month, and lifetime prevalence of anxiety disorders for meat-abstainers was 20.4%, 31.5%, and 31.5%, respectively. As with their results for depression, the prevalence in meat-consumers was significantly lower: 10.7%, 17.0%, and 18.4% in the full sample and 8.7%, 13.2%, and 15.3% in the matched sample. When comparing the “complete vegetarians” to the “matched non-vegetarians” the Odds Ratios for 1-month, 12-month, and lifetime prevalence were 2.69 (95% CI: 1.12–5.99), 3.02 (95% CI: 1.52–5.98), and 2.55 (95% CI: 1.30–4.99), respectively. The authors wrote, “Prevalence rates for anxiety disorder were especially high (more than twice as high) in the completely vegetarian group than in the non-vegetarian matched group” (Michalak, Zhang, and Jacobi Citation2012, 5).
Similarly, the results from the largest and second most rigorous study in the review by Matta et al. (Citation2018) found that in an extremely large, nationally representative sample of French adults (n = 90,380), 28.4% of meat-abstainers had symptoms of depression, whereas only 16.2% of meat-consumers did. The odds of having depressive symptoms increased when meat was excluded from the diet (Matta et al. Citation2018).
Consistent with the more inclusive studies of Michalak, Zhang, and Jacobi (Citation2012) and Matta et al. (Citation2018), the largest study of women exclusively, Baines, Powers, and Brown (Citation2007; n = 9113) and the largest study of men exclusively, Hibbeln et al. (Citation2018; n = 9668), found a greater risk or prevalence of depression (Hibbeln et al. Citation2018) and depression and anxiety (Baines, Powers, and Brown Citation2007) in meat-abstainers. One particular strength of Baines et al.’s analysis was the inclusion of multiple assessments of psychological outcomes, including reports of prior diagnoses of depression or anxiety and the use of prescription medications. They found that the use of prescription medications for depression in women who abstained from meat was nearly twice that of women who ate meat (8.0% vs. 4.2%).
In contrast to the majority of the literature, in 2010 Beezhold, Johnston, and Daigle (Citation2010; n = 138) showed that meat-abstainers reported less depression and anxiety than meat-consumers, and in 2015, Beezhold et al. (Citation2015; n = 620) showed that meat-abstainers reported less anxiety than meat-consumers. The potential reasons for these contradictory findings are detailed in Supporting Information and our discussion.
Secondary outcomes ()
Ten of the 18 studies examined the secondary outcomes of self-harm, mood, stress perception, affective well-being, and QoL (). In contrast to the clear results on depression and anxiety, three studies found no differences between groups (Boldt et al. Citation2018; Pfeiler and Egloff Citation2018; Wirnitzer et al. Citation2018), three favored meat-abstainers (Beezhold et al. Citation2015; Beezhold and Johnston Citation2012; Beezhold, Johnston, and Daigle Citation2010), three studies favored meat-consumers (Baines, Powers, and Brown Citation2007; Neumark-Sztainer et al. Citation1997; Perry et al. Citation2001), and one study provided mixed results (Lavallee et al. Citation2019).
Table 3. Secondary outcomes.
Self-harm
Three studies examined self-harm behaviors. Baines, Powers, and Brown (Citation2007) found that in a large, representative sample Australian women (n = 9113), the prevalence of deliberate self-harm was over three times greater in meat-abstainers than meat-consumers (10.0% vs. 3.1%). Similarly, in a large sample of US adolescents (n = 4746), Perry et al. (Perry et al. Citation2001) found that suicide attempts were more than twice as prevalent in meat-abstainers compared to meat-consumers (18.3% vs. 8.6%), and the prevalence of suicide ideation (i.e., thinking about killing oneself) was 34.7% in meat-abstainers versus 24.9% in meat-consumers. Similarly, in a matched subsample of adolescents (n = 321) that was part of a larger study, Neumark-Sztainer et al. (Neumark-Sztainer et al. Citation1997) found that suicide attempts were more prevalent in meat-abstainers (25%) compared to meat-consumers (17%).
Mood and stress perception
Four studies examined mood and stress perceptions (Beezhold et al. Citation2015; Beezhold and Johnston Citation2012; Beezhold, Johnston, and Daigle Citation2010; Wirnitzer et al. Citation2018). Wirnitzer et al. examined stress perceptions in a sample of 245 European endurance runners (57% female) and found no differences between groups (Wirnitzer et al. Citation2018). Conversely, Beezhold, Johnston, and Daigle (Citation2010) examined mood states in Seventh Day Adventists (i.e., a religious group that espouses vegetarianism; n = 138) and found that meat-abstention was linked to more favorable mood states (Beezhold, Johnston, and Daigle Citation2010). In 2015, in a highly selected sample in which vegetarians and vegans were substantially over-represented (i.e., 283 vegans vs. 228 meat-consumers), Beezhold et al. found that those who abstained from meat reported better mood and lower stress than meat-consumers (Beezhold et al. Citation2015).
In 2012, Beezhold and Johnston (Citation2012) conducted a RCT in which 39 self-characterized omnivores (82% female) were assigned to one of three groups: lacto-vegetarian (i.e., avoided all animal foods except dairy), ovo-pescatarian (i.e., avoided meat and poultry but consumed fish and eggs), or omnivore (i.e., consumed meat and/or poultry at least once daily). Their results suggested that restricting meat, fish, and poultry improved some domains of short-term mood states. As detailed in our discussion, this study had major design flaws (e.g., potential observer-expectancy effects) and errors in interpretation and communication (e.g., nonequivalent groups at baseline, failure to recognize regression to the mean).
Well-being and QoL
Two studies examined well-being and QoL (Boldt et al. Citation2018; Pfeiler and Egloff Citation2018). In a sample of 281 endurance runners (57% female), Boldt et al. (Citation2018) found that QoL did not differ between groups (Boldt et al. Citation2018). Similarly, in a large sample of 4496 German adults, Pfeiler and Egloff (Citation2018) found that neither affective well-being nor current life-satisfaction differed between meat-abstainers and meat-consumers (Pfeiler and Egloff Citation2018).
Primary and secondary outcomes
presents the results of the primary outcomes, depression and anxiety, or related symptoms in rank order of rigor.
Discussion
Based on this systematic review comprising 160,257 participants from varied geographic regions, including Europe, Asia, North America, and Oceania, aged 11 to 96 years, there is clear evidence that meat-abstention is associated with higher rates or risk of depression, anxiety, and self-harm. The results with respect to mood states, affective well-being, stress perception and QoL are less clear and the majority of studies do not support unequivocal inferences.
Across all studies, there was no evidence to support a causal relation between the consumption or avoidance of meat and any psychological outcomes. However, three studies provided evidence suggesting (contradictory) temporal relations between meat-abstention and depression and anxiety. Michalak, Zhang, and Jacobi (Citation2012) demonstrated that the mean age at the adoption of meat-abstention (30.58 years) was substantially older than the mean age of the onset of metal disorder (24.69 years). These authors posited that mental disorders may lead to the adoption of a meat-less diet. The authors stated that individuals with mental disorders may “choose a vegetarian diet as a form of safety or self-protective behavior” (Michalak, Zhang, and Jacobi Citation2012, 6) due to the perception that plant-based diets are more healthful or because individuals with mental disorders may be “more aware of suffering of animals” (Michalak, Zhang, and Jacobi Citation2012, 2). Interestingly, these investigators also found that people with a lifetime diagnosis of psychological disorders consumed less fish and fast food. While these results conflict with previous research on fast food and mental health (Crawford et al. Citation2011), they support Matta et al.’s results and hypothesis that the exclusion of any food group, and especially meat and poultry, is associated with increased odds of having symptoms of psychological disorders (Matta et al. Citation2018).
Conversely, in their longitudinal analysis, Lavallee et al. (Citation2019) found that meat-abstention was linked to “slight increases over time” (Lavallee et al. Citation2019, 153) in depression and anxiety in Chinese students. One important caveat when considering these disparate results on temporal relations may be differences in the factors that led to meat-abstention (e.g., religious practices, health and ethical considerations, or socio-economic status). For example, economically disadvantaged individuals who do not consume meat due to its relative cost may be at risk for ill-health for myriad reasons independent of their lack of meat consumption. Thus, future research examining temporal relations should establish clear distinctions between individuals and populations that abstain from meat consumption due to ethical, religious, and health-related perceptions, or those who do not consume meat for economic reasons.
Strengths, limitations, and flaws of the extant literature
Psychological outcomes
The most rigorous studies used objective and/or multiple assessments of psychological outcomes. For example, Michalak, Zhang, and Jacobi (Citation2012) were the first investigators to use standardized and comprehensive assessment of mental disorders based on DSM criteria (APA Citation2013). Similarly, Baines, Powers, and Brown (Citation2007) provided multiple assessments of psychological outcomes that included reported physician-diagnosed conditions, and the use of prescription medication for depression and anxiety in concert with self-reported symptoms and behaviors (e.g., self-harm; Baines, Powers, and Brown Citation2007). Comparably, Hibbeln et al. (Citation2018) included detailed participant histories, including childhood contact with psychiatric services and family history of depression. Methodologically weaker studies employed a single questionnaire and, in some cases, employed a single-item examining psychological symptoms over a limited timeframe (e.g., the previous week).
Sampling
The most rigorous studies examined large, representative and/or matched samples (Baines, Powers, and Brown Citation2007; Matta et al. Citation2018; Michalak, Zhang, and Jacobi Citation2012), whereas the least rigorous used biased recruitment strategies and biased convenience sampling. For example, Michalak, Zhang, and Jacobi (Citation2012) employed both a large representative sample and a socio-demographically matched subsample for comparison. The strength of this approach cannot be understated. Similarly, Neumark-Sztainer et al. (Citation1997) employed a matched sample drawn from a much larger study population. Conversely, a number of studies attempted to over-sample vegans and vegetarians by directly targeting these groups via internet sources such as “social websites geared to VG and VEG [vegan and vegetarians]”(Beezhold et al. Citation2015) and vegan chat-rooms and/or magazines and vegetarian “fairs” (Boldt et al. Citation2018; Wirnitzer et al. Citation2018). As discussed below, these sampling strategies in concert with self-reported data are a major design flaw.
Investigators who seek to over-sample groups that are highly invested (e.g., ethically, socially, intellectually or emotionally) in their “lifestyle” or dietary choices should acquaint themselves with the large body of research on cognitive dissonance (Festinger Citation1962), social-desirability (Fisher Citation1993), and observer-expectancy effects (e.g., reactivity). This body of work is especially relevant when applied to the errors and biases of self-reported dietary intake data; for details, please see (Archer, Hand, and Blair Citation2013; Archer, Lavie, and Hill Citation2018b; Archer, Marlow, and Lavie Citation2018c, 2018Citationd; Archer, Pavela, and Lavie Citation2015; Hebert et al. Citation1995; Schoeller et al. Citation2013). This large and well-established body of research suggests that for individuals who maintain a strong group identity or affinity, meat consumption or avoidance may represent a significant ethical, intellectual, emotional, behavioral, social and/or spiritual investment that extends well-beyond a simple dietary choice. As such, many individuals (e.g., Paleo and “meat-only” dieters, vegans, vegetarians, Seventh Day Adventists) will be pre-disposed to report significantly higher levels of physical and psychological health to avoid cognitive dissonance and remain consistent with self- and/or group-appraisals.
These non-intentional biases in concert with the potential for a participant to intentionally misreport outcomes to support his or her ideological stances or religious beliefs may induce systematic and non-quantifiable errors when employing self-report protocols. As such, the oversampling of groups that are highly invested in their dietary regimes for health, religious, or ideologic concerns (e.g., animals rights) will lead to biased recruitment and extremely unreliable data. In fact, research on cognitive dissonance and social desirability suggests that the greater the motivation for adhering to one’s dietary or lifestyle pattern (or self-conception), the larger the potential error induced via the use of self-reports (Archer, Marlow, and Lavie Citation2018c; Festinger Citation1962). Future studies should employ objective data collection protocols when over-sampling groups that may be prone to intentional and/or non-intentional misreporting.
Assessment of dietary status (exposure)
One major limitation of all studies in this review was the use of self-reported dietary status. Currently, there is an escalating and contentious debate on the validity of self-reported dietary data and the use of food frequency questionnaires in nutrition (Archer and Lavie Citation2019b; Archer, Lavie, and Hill Citation2018b; Archer, Marlow, and Lavie Citation2018d; Archer, Pavela, and Lavie Citation2015; Ioannidis Citation2018; Martín-Calvo and Martínez-González Citation2018; Satija et al. Citation2015; Schoeller et al. Citation2013; Subar et al. Citation2015; Trepanowski and Ioannidis Citation2018). The debate revolves around two major criticisms. First, critics of self-reported data state that without objective corroboration of dietary self-reports, it is impossible to quantify measurement error due to intentional and nonintentional distorting factors, such as deliberate misreporting (i.e., deception/lying), social desirability, reactivity, misestimation, and false memories of dietary intake (Archer, Pavela, and Lavie Citation2015). Second, critics argue that pseudo-quantification (i.e., the transformation of reported foods and beverages into estimates of nutrient and caloric intake) created a fictional discourse on diet-disease relations (Archer, Hand, and Blair Citation2013; Archer, Lavie, and Hill Citation2018b). This latter argument is based on the fact that ∼65% of self-reported dietary data have been shown to be physiologically implausible [i.e., respondents cannot survive on the amount of foods and beverages reported (Archer, Hand, and Blair Citation2013; Archer, Pavela, and Lavie Citation2015; Ferrari et al. Citation2002; Goldberg et al. Citation1991)].
The first criticism is potentially applicable to our analyses. Nevertheless, the dichotomous nature of our classifications (i.e., meat-consumers versus meat-abstainers) reduces both its importance and impact. The second critique regarding pseudo-quantification is not relevant to our review, nor is it relevant to qualitative assessments of dietary intake.
Duration of dietary patterns
A number of studies failed to include information of the age at which meat-abstention began or the duration of non-consumption. If a relationship exists between the length of time an individual has abstained from meat consumption and physical or psychological health, these data are essential to future investigations. This is especially true since the nutritional deficiencies that are sometimes associated with veganism and vegetarianism may be more detrimental in children and adolescents (Cofnas Citation2019) and may take years to develop (Craig Citation2010; Dwyer Citation1991).
Other potential confounders
Clearly, diet is not the only determinant of psychological health (Archer Citation2018a, Citation2018b). Nevertheless, a number of the studies failed to include important potential confounders and effect modifiers. These include race, ethnic, or religious affiliation, social norms, as well as lifestyle behaviors that directly affect health (e.g., smoking, and alcohol use) and the physiologic determinants of dietary energy intake (e.g., physical activity, body cellularity; Archer Citation2018b; Archer, Lavie, and Hill Citation2018a; Archer et al. Citation2018e). Given that when compared to the general population, individuals who follow a vegetarian diet tend to be more health-conscious, more physically active, more highly educated, consume less alcohol, be nonsmokers and have higher socio-economic status (Appleby et al. Citation2016; Appleby and Key Citation2016; Chang-Claude et al. Citation2005), it is essential for future studies to include detailed information on participants’ health and behavioral histories and current characteristics.
Strengths and limitations of this review
This systematic review had several strengths, including our a priori decision to select only studies that provided a clear distinction between meat-consumers and meat-abstainers. This decision allowed for a clear and yet rigorous assessment. While myriad studies examined vegetarianism along a continuum, these were excluded simply because the lack of a clear distinction rendered inferences equivocal.
A second strength was our decision to limit our primary outcomes to well-defined mental disorders (i.e., depression, anxiety, and related symptoms) and a limited number of secondary outcomes (e.g., self-harm). This focus allowed for a concise yet rigorous review and ameliorated the effects of poorly operationalized psychological phenomena. For example, by excluding results on disordered eating, dietary restraint, orthorexia, and personality (e.g., neuroticism), we avoided the potential misclassification and concomitant pathologizing of those who simply wish to avoid specific foods or food groups (e.g., vegans).
Our study also had limitations. First, we excluded non-English language studies, that could potentially bias our results in favor of “Western” norms which include meat consumption. For example, our selection criteria excluded papers published in languages other than English. (e.g., Japanese, Hindi) and in non-English databases. Thus, our review may have omitted studies from geographic regions that follow predominantly vegetarian or plant-based dietary patterns. In these areas, the relation between meat-avoidance and psychological health may differ from “Western” nations. Nevertheless, our review included a large sample from China; so, this limitation may be trivial.
Second, while our search was clearly defined and comprehensive, our criteria excluded a large number of papers that provided data on this topic [e.g., see (Anderson et al. Citation2019; Barthels, Meyer, and Pietrowsky Citation2018; Burkert et al. Citation2014a; Cooper, Wise, and Mann Citation1985; Jacka et al. Citation2012; Larsson et al. Citation2002; Li et al. Citation2019; Northstone, Joinson, and Emmett Citation2018)]. Nevertheless, we think that a highly focused review has the potential to provide stronger evidence and, as such is more informative to the medical, research, and lay communities. Third, despite the high confidence we place in our finding that meat-abstention is linked to psychological disorders, study designs and lack of rigor precluded valid inferences of temporality and causality.
Fourth, meat consumption is often inconsistently classified in research and national surveillance settings (Gifford et al. Citation2017; O’Connor et al. Citation2020) as well as across languages. For example, in English, the broad category of “meat” subsumes both “red” and “white” meat (e.g., beef and poultry). However, in German, the term “meat” excludes poultry. As such, the results for the studies employing German samples were potentially more restrictive. Finally, inferences from our results are only as accurate as the data collected by the included studies. Given that all studies relied on self-reported dietary status, there is the possibility of misclassification because self-reported dietary consumption is not the equivalent of actual dietary consumption (Archer, Hand, and Blair Citation2013; Archer, Lavie, and Hill Citation2018b; Archer, Marlow, and Lavie Citation2018c, 2018Citationd; Archer, Pavela, and Lavie Citation2015). In other words, there is an obvious and important distinction between merely reporting that one avoids meat and actual meat-abstention; and research supports the fact that self-defined vegetarians and meat-abstainers may consume meat (Haddad and Tanzman Citation2003).
Suggestions for future direction
Future investigators should avoid the most common flaws detailed herein (e.g., uncorroborated self-reported data, biased sampling, confounding, etc.). First, the limitations of self-reported dietary data may be partially overcome with point-of-purchase (barcode) data (Ng and Popkin Citation2012). Nevertheless, while purchase data may be more objective, it is not necessarily an accurate proxy for actual consumption. Second, investigators must acknowledge and address the effects of biased sampling with the use of self-reported data. Individuals highly invested in specific dietary patterns may be predisposed to intentional and non-intentional misreporting. Third, detailed behavioral and health-related histories and current lifestyles should be considered essential. The use of physician-diagnosed disorders based on criteria from the DSM-V (APA Citation2013) is preferable to self-reported symptoms and would assist in producing more definitive results.
Given the results of this review, an interesting future direction would be to examine if meat consumption per se has psychological benefits. For example, there is evidence that a significant number of vegans and vegetarians return to meat consumption over time and that former vegetarians and vegans in the U.S. outnumber current meat-abstainers (Faunalytics Citation2016). As such, one research question that can be answered empirically is whether it is the nutritional properties of meat (as measured via serum biochemical analyses), the reduced social burden or stigma associated with omnivory, or other physiologic or social factors that drive the transition from meat-abstainer back to meat-consumer.
Conclusion
The purpose of this review was to provide evidence to inform both clinical practice and future research. Overall, the scientific literature examining the relation between the consumption or avoidance of meat and psychological health varied substantially in both rigor and validity of interpretation. Higher quality studies suggested that those who abstained from meat consumption had a greater risk or prevalence of depression, anxiety, and self-harm. With respect to clinical practice, the avoidance of meat may be a behavioral marker that signifies poorer mental health. Study designs and/or a lack of rigor precluded inference of causal relations and none should be inferred. However, our study does not support avoiding meat consumption for overall psychological health benefits.
Supplemental Material
Download Zip (81.8 KB)Disclosure statement
No potential conflict of interest was reported by the author(s).
Additional information
Funding
References
- Anderson, E. C., J. Wormwood, L. F. Barrett, and K. S. Quigley. 2019. Vegetarians’ and omnivores’ affective and physiological responses to images of food. Food Quality and Preference 71:96–105. doi: 10.1016/j.foodqual.2018.06.008.
- APA. 2013. Diagnostic and statistical manual of mental disorders (DSM-5®). Arlington, VA: American Psychiatric Association.
- Appleby, P., A. Roddam, N. Allen, and T. Key. 2007. Comparative fracture risk in vegetarians and nonvegetarians in EPIC-Oxford. European Journal of Clinical Nutrition 61 (12):1400–6. doi: 10.1038/sj.ejcn.1602659.
- Appleby, P. N., F. L. Crowe, K. E. Bradbury, R. C. Travis, and T. J. Key. 2016. Mortality in vegetarians and comparable nonvegetarians in the United Kingdom. The American Journal of Clinical Nutrition 103 (1):218–30. doi: 10.3945/ajcn.115.119461.
- Appleby, P. N., and T. J. Key. 2016. The long-term health of vegetarians and vegans. Proceedings of the Nutrition Society 75 (3):287–93. doi: 10.1017/S0029665115004334.
- Archer, E. 2018a. The demonization of ‘diet’ is nothing new. Progress in Cardiovascular Diseases 61 (3–4):386–7. doi: 10.1016/j.pcad.2018.07.013.
- Archer, E. 2018b. In defense of sugar: A critique of diet-centrism. Progress in Cardiovascular Diseases 61 (1):10–19. doi: 10.1016/j.pcad.2018.04.007.
- Archer, E., G. A. Hand, and S. N. Blair. 2013. Validity of U.S. Nutritional Surveillance: National Health and Nutrition Examination Survey caloric energy intake data, 1971-2010. PLoS One 8 (10):e76632. doi: 10.1371/journal.pone.0076632.
- Archer, E., and C. J. Lavie. 2019a. Is the PURE study pure fiction? European Heart Journal 40 (4):394. doi: 10.1093/eurheartj/ehy736.
- Archer, E., and C. J. Lavie. 2019b. Healthy diets and sustainable food systems. The Lancet 394 (10194):214–5. doi: 10.1016/S0140-6736(19)31130-4.
- Archer, E., C. J. Lavie, and J. O. Hill. 2018a. The contributions of ‘diet’, ‘genes’, and physical activity to the etiology of obesity: Contrary evidence and consilience. Progress in Cardiovascular Diseases 61 (2):89–102. doi: 10.1016/j.pcad.2018.06.002.
- Archer, E., C. J. Lavie, and J. O. Hill. 2018b. The failure to measure dietary intake engendered a fictional discourse on diet-disease relations. Frontiers in Nutrition 5:105. doi: 10.3389/fnut.2018.00105.
- Archer, E., M. L. Marlow, and C. J. Lavie. 2018c. Controversy and debate: Memory-based dietary assessment methods paper #3. Journal of Clinical Epidemiology 104:130–5. doi: 10.1016/j.jclinepi.2018.08.003.
- Archer, E., M. L. Marlow, and C. J. Lavie. 2018d. Controversy and debate: Memory-based methods paper 1: The fatal flaws of food frequency questionnaires and other memory-based dietary assessment methods. Journal of Clinical Epidemiology 104:113–24. doi: 10.1016/j.jclinepi.2018.08.003.
- Archer, E., G. Pavela, and C. J. Lavie. 2015. The inadmissibility of what we eat in America and NHANES dietary data in nutrition and obesity research and the scientific formulation of national dietary guidelines. Mayo Clinic Proceedings 90 (7):911–26. doi: 10.1016/j.mayocp.2015.04.009.
- Archer, E., G. Pavela, S. McDonald, C. J. Lavie, and J. O. Hill. 2018e. Cell-specific “competition for calories” drives asymmetric nutrient-energy partitioning, obesity, and metabolic diseases in human and non-human animals. Frontiers in Physiology 9:1053. doi: 10.3389/fphys.2018.01053.
- Baines, S., J. Powers, and W. J. Brown. 2007. How does the health and well-being of young Australian vegetarian and semi-vegetarian women compare with non-vegetarians? Public Health Nutrition 10 (5):436–42. doi: 10.1017/S1368980007217938.
- Barthels, F., F. Meyer, and R. Pietrowsky. 2018. Orthorexic and restrained eating behaviour in vegans, vegetarians, and individuals on a diet. Eating and Weight Disorders - Studies on Anorexia, Bulimia and Obesity 23 (2):159–66. doi: 10.1007/s40519-018-0479-0.
- Bas, M., E. Karabudak, and G. Kiziltan. 2005. Vegetarianism and eating disorders: Association between eating attitudes and other psychological factors among Turkish adolescents. Appetite 44:309–15. doi: 10.1016/j.appet.2005.02.002.
- Beezhold, B., C. Radnitz, A. Rinne, and J. DiMatteo. 2015. Vegans report less stress and anxiety than omnivores. Nutritional Neuroscience 18 (7):289–96. doi: 10.1179/1476830514Y.0000000164.
- Beezhold, B. L., and C. S. Johnston. 2012. Restriction of meat, fish, and poultry in omnivores improves mood: A pilot randomized controlled trial. Nutrition Journal 11 (1):9. doi: 10.1186/1475-2891-11-9.
- Beezhold, B. L., C. S. Johnston, and D. R. Daigle. 2010. Vegetarian diets are associated with healthy mood states: A cross-sectional study in seventh day adventist adults. Nutrition Journal 9 (1):26. doi: 10.1186/1475-2891-9-26.
- Boldt, P., B. Knechtle, P. Nikolaidis, C. Lechleitner, G. Wirnitzer, C. Leitzmann, T. Rosemann, and K. Wirnitzer. 2018. Quality of life of female and male vegetarian and vegan endurance runners compared to omnivores - results from the NURMI study (step 2). Journal of the International Society of Sports Nutrition 15 (1):33. doi: 10.1186/s12970-018-0237-8.
- Burkert, N. T., W. Freidl, F. Großschädel, J. Muckenhuber, W. J. Stronegger, and É. Rásky. 2014a. Nutrition and health: Different forms of diet and their relationship with various health parameters among Austrian adults. Wiener Klinische Wochenschrift 126 (3–4):113–8. doi: 10.1007/s00508-013-0483-3.
- Burkert, N. T., J. Muckenhuber, F. Großschädl, E. Rásky, and W. Freidl. 2014b. Nutrition and health–the association between eating behavior and various health parameters: A matched sample study. PLoS One 9 (2):e88278. doi: 10.1371/journal.pone.0088278.
- Carroll, A. E., and T. S. Doherty. 2019. Meat consumption and health: Food for thought. Annals of Internal Medicine 171 (10):767–8. doi: 10.7326/M19-2620.
- Chang-Claude, J., S. Hermann, U. Eilber, and K. Steindorf. 2005. Lifestyle determinants and mortality in German vegetarians and health-conscious persons: Results of a 21-year follow-up. Cancer Epidemiology Biomarkers & Prevention 14 (4):963–8. doi: 10.1158/1055-9965.EPI-04-0696.
- Cofnas, N. 2019. Is vegetarianism healthy for children? Critical Reviews in Food Science and Nutrition 59 (13):2052–60. doi: 10.1080/10408398.2018.1437024.
- Cooper, C. K., T. N. Wise, and L. S. Mann. 1985. Psychological and cognitive characteristics of vegetarians. Psychosomatics 26 (6):521–7. doi: 10.1016/S0033-3182(85)72832-0.
- Craig, W. J. 2010. Nutrition concerns and health effects of vegetarian diets. Nutrition in Clinical Practice 25 (6):613–20. doi: 10.1177/0884533610385707.
- Crawford, G. B., A. Khedkar, J. A. Flaws, J. D. Sorkin, and L. Gallicchio. 2011. Depressive symptoms and self-reported fast-food intake in midlife women. Preventive Medicine 52 (3–4):254–7. doi: 10.1016/j.ypmed.2011.01.006.
- Dinu, M., R. Abbate, G. F. Gensini, A. Casini, and F. Sofi. 2017. Vegetarian, vegan diets and multiple health outcomes: A systematic review with meta-analysis of observational studies. Critical Reviews in Food Science and Nutrition. 57 (17):3640–9. doi: 10.1080/10408398.2016.1138447.
- Dwyer, J. T. 1991. Nutritional consequences of vegetarianism. Annual Review of Nutrition 11 (1):61–91. doi: 10.1146/annurev.nu.11.070191.000425.
- Faunalytics. 2016. A summary of Faunalytics’ study of current and former vegetarians and vegans. Faunalytics. Accessed September 21, 2019. https://faunalytics.org/a-summary-of-faunalytics-study-of-current-and-former-vegetarians-and-vegans/.
- Ferrari, P., N. Slimani, A. Ciampi, A. Trichopoulou, A. Naska, C. Lauria, F. Veglia, H. B. Bueno-de-Mesquita, M. C. Ocke, M. Brustad, et al. 2002. Evaluation of under- and overreporting of energy intake in the 24-hour diet recalls in the European Prospective Investigation into Cancer and Nutrition (EPIC). Public Health Nutrition 5 (6b):1329–45. doi: 10.1079/PHN2002409.
- Festinger, L. 1962. A theory of cognitive dissonance, vol 2. Stanford, CA: Stanford University Press.
- Fisher, R. J. 1993. Social desirability bias and the validity of indirect questioning. Journal of Consumer Research 20 (2):303–15. doi: 10.1086/209351.
- Forestell, C. A., and J. B. Nezlek. 2018. Vegetarianism, depression, and the five factor model of personality. Ecology of Food and Nutrition 57 (3):246–59. doi: 10.1080/03670244.2018.1455675.
- Friedrich, M. J. 2017. Depression is the leading cause of disability around the world depression leading cause of disability Globally Global Health. JAMA 317:1517. doi: 10.1001/jama.2017.3826.
- Gifford, C. L., L. E. O’Connor, W. W. Campbell, D. R. Woerner, and K. E. Belk. 2017. Broad and inconsistent muscle food classification is problematic for dietary guidance in the U.S. Nutrients 9 (9):1027. doi: 10.3390/nu9091027.
- Goldberg, G. R., A. E. Black, S. A. Jebb, T. J. Cole, P. R. Murgatroyd, W. A. Coward, and A. M. Prentice. 1991. Critical evaluation of energy intake data using fundamental principles of energy physiology: 1. Derivation of cut-off limits to identify under-recording. European Journal of Clinical Nutrition 45 (12):569–81.
- Haddad, E. H., and J. S. Tanzman. 2003. What do vegetarians in the United States eat? The American Journal of Clinical Nutrition 78 (3):626S–32S. doi: 10.1093/ajcn/78.3.626S.
- Hebert, J. R., L. Clemow, L. Pbert, I. S. Ockene, and J. K. Ockene. 1995. Social desirability bias in dietary self-report may compromise the validity of dietary intake measures. International Journal of Epidemiology 24 (2):389–98. doi: 10.1093/ije/24.2.389.
- Hibbeln, J. R., K. Northstone, J. Evans, and J. Golding. 2018. Vegetarian diets and depressive symptoms among men. Journal of Affective Disorders 225:13–17. doi: 10.1016/j.jad.2017.07.051.
- Hong, Q. N., P. Pluye, S. Fàbregues, G. Bartlett, F. Boardman, M. Cargo, P. Dagenais, M.-P. Gagnon, B. Nicolau, and A. O’Cathain. 2018. Mixed methods appraisal tool (MMAT), version 2018. Gatineau, CA: IC Canadian Intellectual Property Office.
- Iguacel, I., M. L. Miguel-Berges, A. Gomez-Bruton, L. A. Moreno, and C. Julian. 2019. Veganism, vegetarianism, bone mineral density, and fracture risk: A systematic review and meta-analysis. Nutrition Reviews 77 (1):1–18. doi: 10.1093/nutrit/nuy045.
- Ioannidis, J. A. 2018. The challenge of reforming nutritional epidemiologic research. JAMA 320 (10):969. doi: 10.1001/jama.2018.11025.
- Jacka, F. N., J. A. Pasco, L. J. Williams, N. Mann, A. Hodge, L. Brazionis, and M. Berk. 2012. Red meat consumption and mood and anxiety disorders. Psychotherapy and Psychosomatics 81 (3):196–8. doi: 10.1159/000334910.
- Johnston, B. C., D. Zeraatkar, M. A. Han, R. W. M. Vernooij, C. Valli, R. El Dib, C. Marshall, P. J. Stover, S. Fairweather-Taitt, G. Wójcik, et al. 2019. Unprocessed red meat and processed meat consumption: Dietary guideline recommendations from the nutritional recommendations (NutriRECS) consortium. Annals of Internal Medicine 171 (10):756. doi: 10.7326/M19-1621.
- Kahleova, H., S. Levin, and N. D. Barnard. 2018. Vegetarian dietary patterns and cardiovascular disease. Progress in Cardiovascular Diseases 61 (1):54–61. doi: 10.1016/j.pcad.2018.05.002.
- Kessler, R. C., W. T. Chiu, O. Demler, K. R. Merikangas, and E. E. Walters. 2005. Prevalence, severity, and comorbidity of 12-month DSM-IV disorders in the National Comorbidity Survey Replication. Archives of General Psychiatry 62 (6):617–27. doi: 10.1001/archpsyc.62.6.617.
- Key, T. J., G. E. Fraser, M. Thorogood, P. N. Appleby, V. Beral, G. Reeves, M. L. Burr, J. Chang-Claude, R. Frentzel-Beyme, J. W. Kuzma, et al. 1999. Mortality in vegetarians and nonvegetarians: Detailed findings from a collaborative analysis of 5 prospective studies. The American Journal of Clinical Nutrition 70 (3):516s–24s. doi: 10.1093/ajcn/70.3.516s.
- Klopp, S. A., C. J. Heiss, and H. S. Smith. 2003. Self-reported vegetarianism may be a marker for college women at risk for disordered eating. Journal of the American Dietetic Association 103 (6):745–7. doi: 10.1053/jada.2003.50139.
- Lancet. 2015. Global, regional, and national incidence, prevalence, and years lived with disability for 301 acute and chronic diseases and injuries in 188 countries, 1990–2013: A systematic analysis for the Global Burden of Disease Study 2013. The Lancet 368 (9995):743–800.
- Larsson, C., K. Klock, A. Nordrehaugpstrom, O. Haugejorden, and G. Johansson. 2002. Lifestyle-related characteristics of young low-meat consumers and omnivores in Sweden and Norway. Journal of Adolescent Health 31 (2):190–8. doi: 10.1016/S1054-139X(02)00344-0.
- Lavallee, K., X. C. Zhang, J. Michalak, S. Schneider, and J. Margraf. 2019. Vegetarian diet and mental health: Cross-sectional and longitudinal analyses in culturally diverse samples. Journal of Affective Disorders 248:147–54. doi: 10.1016/j.jad.2019.01.035.
- Lavie, C. J., A. R. Menezes, A. De Schutter, R. V. Milani, and J. A. Blumenthal. 2016. Impact of cardiac rehabilitation and exercise training on psychological risk factors and subsequent prognosis in patients with cardiovascular disease. Canadian Journal of Cardiology 32 (10):S365–S73. doi: 10.1016/j.cjca.2016.07.508.
- Leitzmann, C. 2014. Vegetarian nutrition: Past, present, future. The American Journal of Clinical Nutrition 100 (suppl_1):496S–502S. doi: 10.3945/ajcn.113.071365.
- Li, X.-D., H.-J. Cao, S.-Y. Xie, K.-C. Li, F.-B. Tao, L.-S. Yang, J.-Q. Zhang, and Y.-S. Bao. 2019. Adhering to a vegetarian diet may create a greater risk of depressive symptoms in the elderly male Chinese population. Journal of Affective Disorders 243:182–7. doi: 10.1016/j.jad.2018.09.033.
- Lindeman, M. 2002. The state of mind of vegetarians: Psychological well-being or distress? Ecology of Food and Nutrition 41 (1):75–86. doi: 10.1080/03670240212533.
- Martín-Calvo, N., and M. Á. Martínez-González. 2018. Controversy and debate: Memory-based dietary assessment methods paper 2. Journal of Clinical Epidemiology 104:113–24. doi: 10.1016/j.jclinepi.2018.08.005.
- Matta, J., S. Czernichow, E. Kesse-Guyot, N. Hoertel, F. Limosin, M. Goldberg, M. Zins, and C. Lemogne. 2018. Depressive symptoms and vegetarian diets: Results from the constances cohort. Nutrients 10 (11):1695. doi: 10.3390/nu10111695.
- Melina, V., W. Craig, and S. Levin. 2016. Position of the academy of nutrition and dietetics: Vegetarian diets. Journal of the Academy of Nutrition and Dietetics 116 (12):1970–80. doi: 10.1016/j.jand.2016.09.025.
- Michalak, J., X. C. Zhang, and F. Jacobi. 2012. Vegetarian diet and mental disorders: Results from a representative community survey. International Journal of Behavioral Nutrition and Physical Activity 9 (1):67. doi: 10.1186/1479-5868-9-67.
- Moher, D., A. Liberati, J. Tetzlaff, D. Altman, and The PRISMA Group. 2009. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Medicine 6:e1000097. doi: 10.1371/journal.pmed.1000097.
- Neumann, C. G., N. O. Bwibo, S. P. Murphy, M. Sigman, S. Whaley, L. H. Allen, D. Guthrie, R. E. Weiss, and M. W. Demment. 2003. Animal source foods improve dietary quality, micronutrient status, growth and cognitive function in Kenyan school children: Background, study design and baseline findings. The Journal of Nutrition 133 (11):3941S–9S. doi: 10.1093/jn/133.11.3941S.
- Neumann, C. G., S. P. Murphy, C. Gewa, M. Grillenberger, and N. O. Bwibo. 2007. Meat supplementation improves growth, cognitive, and behavioral outcomes in Kenyan children. The Journal of Nutrition 137 (4):1119–23. doi: 10.1093/jn/137.4.1119.
- Neumark-Sztainer, D., M. Story, M. D. Resnick, and R. W. Blum. 1997. Adolescent vegetarians. A behavioral profile of a school-based population in Minnesota. Archives of Pediatrics & Adolescent Medicine 151 (8):833–8. doi: 10.1001/archpedi.1997.02170450083014.
- Nezlek, J. B., C. A. Forestell, and D. B. Newman. 2018. Relationships between vegetarian dietary habits and daily well-being. Ecology of Food and Nutrition 57 (5):425–38. doi: 10.1080/03670244.2018.1536657.
- Ng, S. W., and B. M. Popkin. 2012. Monitoring foods and nutrients sold and consumed in the United States: Dynamics and challenges. Journal of the Academy of Nutrition and Dietetics 112 (1):41–45. doi: 10.1016/j.jada.2011.09.015.
- Northstone, K., C. Joinson, and P. Emmett. 2018. Dietary patterns and depressive symptoms in a UK cohort of men and women: A longitudinal study. Public Health Nutrition 21 (5):831–7. doi: 10.1017/S1368980017002324.
- O’Connor, L. E., C. L. Gifford, D. R. Woerner, J. L. Sharp, K. E. Belk, and W. W. Campbell. 2020. Dietary meat categories and descriptions in chronic disease research are substantively different within and between experimental and observational studies: A systematic review and landscape analysis. Advances in Nutrition 11 (1):41–51.
- O’Keefe, E. L., J. J. DiNicolantonio, J. H. O’Keefe, and C. J. Lavie. 2018. Alcohol and CV health: Jekyll and Hyde J-curves. Progress in Cardiovascular Diseases 61:68–75. doi: 10.1016/j.pcad.2018.02.001.
- O’Keefe, E. L., J. H. O’Keefe, and C. J. Lavie. 2019. Exercise counteracts the cardiotoxicity of psychosocial stress. Mayo Clinic Proceedings 94 (9):1852–64. doi: 10.1016/j.mayocp.2019.02.022.
- Perica, M. M., and I. Delaš. 2011. Essential fatty acids and psychiatric disorders. Nutrition in Clinical Practice 26 (4):409–25. doi: 10.1177/0884533611411306.
- Perry, C. L., M. T. McGuire, D. Neumark-Sztainer, and M. Story. 2001. Characteristics of vegetarian adolescents in a multiethnic urban population. Journal of Adolescent Health 29 (6):406–16. doi: 10.1016/S1054-139X(01)00258-0.
- Pfeiler, T. M., and B. Egloff. 2018. Examining the ‘veggie’ personality: Results from a representative German sample. Appetite 120:246–55. doi: 10.1016/j.appet.2017.09.005.
- Porphyry. 1823. Select works of Porphyry. London: T. Rodd.
- Roe, D. A. 1986. History of promotion of vegetable cereal diets. The Journal of Nutrition 116 (7):1355–63. doi: 10.1093/jn/116.7.1355.
- Rosenfeld, D. L. 2018. The psychology of vegetarianism: Recent advances and future directions. Appetite 131:125–38. doi: 10.1016/j.appet.2018.09.011.
- Rowe, S. B., and N. Alexander. 2017. On post-truth, fake news, and trust. Nutrition Today 52 (4):179–82. doi: 10.1097/NT.0000000000000224.
- Ruby, M. B. 2012. Vegetarianism. A blossoming field of study. Appetite 58 (1):141–50. doi: 10.1016/j.appet.2011.09.019.
- Satija, A., E. Yu, W. C. Willett, and F. B. Hu. 2015. Understanding nutritional epidemiology and its role in policy. Advances in Nutrition 6 (1):5–18. doi: 10.3945/an.114.007492.
- Schoeller, D. A., D. Thomas, E. Archer, S. B. Heymsfield, S. N. Blair, M. I. Goran, J. O. Hill, R. L. Atkinson, B. E. Corkey, J. Foreyt, et al. 2013. Self-report-based estimates of energy intake offer an inadequate basis for scientific conclusions. The American Journal of Clinical Nutrition 97 (6):1413–5. doi: 10.3945/ajcn.113.062125.
- Singh, P. N., J. Sabaté, and G. E. Fraser. 2003. Does low meat consumption increase life expectancy in humans? The American Journal of Clinical Nutrition 78 (3):526S–32S. doi: 10.1093/ajcn/78.3.526S.
- Spencer, C. 1995. The heretic’s feast: A history of vegetarianism. Hanover: University Press New England. doi: 10.1086/ahr/102.1.85-a.
- Statista. 2019. Meat consumption and vegetarianism in Europe - Statistics and Facts. Statista.com Accessed February 25, 2020. https://www.statista.com/topics/3345/meat-consumption-and-vegetarianism-in-europe/.
- Stokes, N., C. M. Gordon, and A. DiVasta. 2011. Vegetarian diets and mental health in adolescents with anorexia nervosa. Journal of Adolescent Health 48 (2):S50. doi: 10.1016/j.jadohealth.2010.11.109.
- Subar, A. F., L. S. Freedman, J. A. Tooze, S. I. Kirkpatrick, C. Boushey, M. L. Neuhouser, F. E. Thompson, N. Potischman, P. M. Guenther, V. Tarasuk, et al. 2015. Addressing current criticism regarding the value of self-report dietary data. The Journal of Nutrition 145 (12):2639–45. doi: 10.3945/jn.115.219634.
- Timko, C. A., J. M. Hormes, and J. Chubski. 2012. Will the real vegetarian please stand up? An investigation of dietary restraint and eating disorder symptoms in vegetarians versus non-vegetarians. Appetite 58 (3):982–90. doi: 10.1016/j.appet.2012.02.005.
- Tong, T. Y., P. N. Appleby, K. E. Bradbury, A. Perez-Cornago, R. C. Travis, R. Clarke, and T. J. Key. 2019. Risks of ischaemic heart disease and stroke in meat eaters, fish eaters, and vegetarians over 18 years of follow-up: Results from the prospective EPIC-Oxford study. BMJ (Clinical Research ed.) 366:l4897. doi: 10.1136/bmj.l4897.
- Trepanowski, J. F., and J. P. Ioannidis. 2018. Perspective: Limiting dependence on nonrandomized studies and improving randomized trials in human nutrition research: Why and how. Advances in Nutrition 9 (4):367–77. doi: 10.1093/advances/nmy014.
- Viguiliouk, E., C. W. C. Kendall, H. Kahleová, D. Rahelić, J. Salas-Salvadó, V. L. Choo, S. B. Mejia, S. E. Stewart, L. A. Leiter, D. J. A. Jenkins, et al. 2019. Effect of vegetarian dietary patterns on cardiometabolic risk factors in diabetes: A systematic review and meta-analysis of randomized controlled trials. Clinical Nutrition 38 (3):1133–45. doi: 10.1016/j.clnu.2018.05.032.
- Weightman, A., M. Mann, L. Sander, and R. Turley. 2004. Health evidence bulletins Wales: A systematic approach to identifying the evidence. Project methodology 5. Cardiff: Information Services UWCM.
- WHO. 2017. Depression and other common mental disorders: Global health estimates. Geneva: World Health Organization.
- WHO. 2019. Mental health: A state of well-being. Geneva: World Health Organization. Accessed September 31, 2019. https://www.who.int/features/factfiles/mental_health/en/.
- Whorton, J. C. 1994. Historical development of vegetarianism. The American Journal of Clinical Nutrition 59 (5):1103S–9S. doi: 10.1093/ajcn/59.5.1103S.
- Willett, W., J. Rockström, B. Loken, M. Springmann, T. Lang, S. Vermeulen, T. Garnett, D. Tilman, F. DeClerck, A. Wood, et al. 2019. Food in the Anthropocene: The EAT-Lancet Commission on healthy diets from sustainable food systems. The Lancet 393 (10170):447–92. doi: 10.1016/S0140-6736(18)31788-4.
- Williams, P. 2007. Nutritional composition of red meat. Nutrition & Dietetics 64:S113–S9. doi: 10.1111/j.1747-0080.2007.00197.x.
- Wirnitzer, K., P. Boldt, C. Lechleitner, G. Wirnitzer, C. Leitzmann, T. Rosemann, and B. Knechtle. 2018. Health Status of Female and Male Vegetarian and Vegan Endurance Runners Compared to Omnivores-Results from the NURMI Study (Step 2). Nutrients 11 (1):29. doi: 10.3390/nu11010029.
- Young, G., and J. Conquer. 2005. Omega-3 fatty acids and neuropsychiatric disorders. Reproduction Nutrition Development 45 (1):1–28. doi: 10.1051/rnd:2005001.
- Zuromski, K. L., T. K. Witte, A. R. Smith, N. Goodwin, L. P. Bodell, M. Bartlett, and N. Siegfried. 2015. Increased prevalence of vegetarianism among women with eating pathology. Eating Behaviors 19:24–27. doi: 10.1016/j.eatbeh.2015.06.017.