
Abstract
Digital technologies such as virtual reality (VR) are increasingly designed and implemented to support people living with dementia who are at risk of loneliness and/or social isolation. Multi-user VR (MUVR), which involves simultaneous user engagement and a sense of being present together in VR, may promote and maintain social connectedness between people living with dementia and their support persons. This paper focuses on Phase 4 of a larger participatory action research (PAR) project, which aimed to explore the usability, acceptability and feasibility of a MUVR application and its potential to support the social connectedness of people living with dementia and their support persons. The study involved five people living with dementia and their five support persons, who trialed the application in their homes over two PAR cycles. The researcher gathered feedback through individual semi-structured interviews and observational field notes. Reflexive thematic analysis guided qualitative data analysis, and the findings suggested that MUVR is a usable, acceptable, and feasible application for this population. The findings also indicated that MUVR shows promise in promoting or maintaining social connectedness among people living with dementia and their support persons. Nonetheless, further refinement is necessary to enhance the usability, acceptability and feasibility of the MUVR application, and these areas of refinement are presented in this paper, through design recommendations for future work.
1. Introduction and background
It is estimated that 55 million people worldwide are affected by dementia, with this figure expected to rise to 152 million by 2050 (Patterson, Citation2018). Dementia is a progressive syndrome characterized by a deterioration in memory, thinking, behaviors and the ability to perform activities of daily living (World Health Organisation, Citation2012). One area often impacted by dementia is social health (Dröes et al., Citation2017). Social health, as defined by Huber et al. (Citation2011), involves a person’s “capacity to fulfill their potential and obligations, the ability to manage their life with some degree of independence despite a medical condition, and the ability to participate in social activities” (p. 236). Indeed, many researchers acknowledge the important role social health has in enabling individuals to live well with dementia (de Vugt & Dröes, Citation2017; Dröes et al., Citation2017; Vernooij-Dassen & Jeon, Citation2016; Vernooij-Dassen et al., Citation2018). Social connectedness, a key component of social health and wellbeing, refers to a short-term or momentary experience of relatedness or belonging between people (Van Bel et al., Citation2009). Van Bel et al. (Citation2009) proposed that social connectedness consists of several dimensions: closeness, relationship saliency, knowing each other’s experiences, contact quality and shared understanding.
Social connectedness may guard against cognitive decline and dementia and is also considered an essential component of healthy aging (Cooper et al., Citation2021; Di Marco et al., Citation2014; Pandey et al., Citation2021; Rutledge, Citation2011; Waycott et al., Citation2019). People living with dementia frequently experience difficulties communicating, often resulting in their withdrawal from previous social activities and networks, particularly as their condition progresses (Rausch et al., Citation2017; Van Orden & Heffner, Citation2022). This can lead to reduced self-efficacy and confidence, all of which can negatively impact social health and the ability of people living with dementia to stay socially connected (Alzheimer’s Society UK, Citation2013; Birt et al., Citation2020; Dröes et al., Citation2006; Vernooij-Dassen & Jeon, Citation2016; Yu et al., Citation2016). The progression of dementia can also negatively impact the social connections and relationships of people living with dementia resulting in fewer opportunities for social connectedness with their support persons (Hoel et al., Citation2022; Rausch et al., Citation2017; Van Orden & Heffner, Citation2022).
As of yet, there is no cure for dementia. Therefore, supporting people living with dementia to stay socially connected is vital to ensure they can “live well” with the condition (de Vugt & Dröes, Citation2017; Quinn et al., Citation2022; Vernooij-Dassen & Jeon, Citation2016). The importance of social connectedness for people living with dementia was further heightened because of the need for physical distancing during the COVID-19 pandemic, leading to an increased drive to identify ways of supporting social connections and, thereby, the social health of people living with dementia (de Vugt & Dröes, Citation2017; Hanna et al., Citation2021; Quinn et al., Citation2022; Tuijt et al., Citation2021; Vernooij-Dassen & Jeon, Citation2016).
Researchers in the human-computer interaction (HCI) community are increasingly exploring the role of digital technology in improving the social health of people living with dementia (Barbosa et al., Citation2024; Heins et al., Citation2021; Hoel et al., Citation2022; Hung et al., Citation2021; Pinto-Bruno et al., Citation2017). A recent HCI focus is on the development of technologies designed specifically to reduce loneliness and social isolation and support social connectedness. Such examples include telepresence robots (Moyle et al., Citation2017) and touch-screen tablets (Astell et al., Citation2010) to facilitate connections between people living with dementia and support persons, as well as virtual memory cafés to help maintain connections with peers (Masoud et al., Citation2021). These digital technologies have yielded positive outcomes for people living with dementia and demonstrate the potential role of innovative technologies to support social connectedness.
Another emerging digital technology is virtual reality (VR) (Flynn et al., Citation2022a). VR is considered “a computer-generated digital environment that can be experienced and interacted with as if that environment were real” (Jerald, Citation2015, p. 9). VR ranges from non-immersive, semi-immersive to fully immersive systems (Henderson et al., Citation2007; Martirosov et al., Citation2022). Fully immersive VR (the focus of this current paper) presents an artificial world and fully occludes the physical environment (Jerald, Citation2015; Martirosov et al., Citation2022). This is typically presented through a head-mounted display (HMD), accompanied by hand-held controllers, which enable users to interact and manipulate the virtual environment (VE) (Bryant et al., Citation2022; Martirosov et al., Citation2022; Orr et al., Citation2021). A unique feature of VR is its ability to facilitate people living with dementia to access virtual environments (VEs) that may no longer be accessible to them due to physical, cognitive, and/or environmental challenges (Hodge et al., Citation2018; Siriaraya & Ang, Citation2014). Additionally, VR can support single or multi-user experiences.
Single-user VR has been considered a useful, cost-effective, flexible and convenient means of delivering person-centered care for people living with dementia or those with mild cognitive impairment (MCI) (Kim et al., Citation2019). Similarly, VR (non-immersive to fully immersive) was described as an acceptable and usable technology that provides a positive user experience for people living with dementia (Flynn et al., Citation2022a). However, despite the positive associations of VR use in dementia contexts, the methodological quality of some VR research remains relatively low (Flynn et al., Citation2022a; Kim et al., Citation2019). Furthermore, most of the focus of VR use in dementia research has been on single-user experiences to address areas such as cognitive training and assessment, reminiscence or physical activity rather than multi-user experiences to support social outcomes (Afifi et al., Citation2021, Citation2023; Appel et al., Citation2021; Flynn et al., Citation2022a).
Multi-user VR (MUVR) or social VR enables two or more people to be simultaneously present in the same multi-user virtual environment (MUVE), whereby multiple users can engage and socialize with one another (Zamanifard & Freeman, Citation2023). A key feature of MUVR is avatar-mediated communication. Avatars are considered a digital representation of users, enabling them to co-exist, interact together in MUVR and experience an individual and shared sense of presence (Biocca et al., Citation2003; Kyrlitsias & Michael-Grigoriou, Citation2022; Nowak & Fox, Citation2018). This sense of social presence is important in MUVR to support social health (Baker et al., Citation2021) and may be a key component to support social connectedness. There are only a few research examples of MUVR focused on socially connecting older adults with their peers, family and grandchildren (Baker et al., Citation2021; Hung et al., Citation2023; Oppert et al., Citation2023; Sancho-Esper et al., Citation2022; Wei et al., Citation2023; Xu et al., Citation2023) and fewer still focusing specifically on people living with dementia (Afifi et al., Citation2021, Citation2023). Studies involving older adults (without dementia) have identified the value of MUVR in enriching interactions, communication and personal relationships between users (Baker et al., Citation2021; Sancho-Esper et al., Citation2022; Wei et al., Citation2023; Xu et al., Citation2023). Such studies showed that relatable and meaningful content in MUVR served as a conversation engager between users, presenting something novel that could be discussed together (Baker et al., Citation2021; Sancho-Esper et al., Citation2022; Wei et al., Citation2023; Xu et al., Citation2023). Excluding these studies, there remains a paucity of research investigating fully immersive MUVR use in gerontology and dementia contexts (Afifi et al., Citation2021; Brimelow et al., Citation2022; Muñoz et al., Citation2022; Sun et al., Citation2020). To date Afifi et al. (Citation2021, Citation2023) represent one of few studies specifically focused on the social aspects of fully immersive MUVR use between people living with dementia with their family members.
Afifi et al. (Citation2021) explored the feasibility of a MUVR application to connect older adults living with MCI and dementia with their family members who live at a distance. Their findings suggested that the MUVR application was feasible and acceptable for older adults living with MCI or dementia residing in a senior living community. Afifi et al. (Citation2023) provided further insights into their 2021 study, investigating the impact of the same MUVR application on the social relationships between the same group. This paper reported that older adults perceived that the MUVR enriched their relationships with family members. However, family members did not perceive a change in relationship quality after they used the MUVR application with people living with dementia, which may, as acknowledged by the authors, be attributed to the already pre-existing high-quality relationships reported at baseline. Afifi et al. (Citation2021, Citation2023) highlighted the promise of MUVR to enhance the social health of people living with dementia, MCI and their family members and emphasized the paucity of work in this area, calling for future research.
To address this knowledge gap, this study used participatory action research (PAR) to design, develop and explore the use of a MUVR application to promote or maintain the social connectedness of people living with dementia and their support person. The design and development of the MUVR application evolved over three previous PAR phases reported in separate publications (Flynn et al., Citation2022a, Citation2022b, Citation2024). This paper presents Phase 4, which explores the usability, acceptability and feasibility of the MUVR application and its potential to promote and maintain the social connectedness of people living with dementia and their support persons.
Within the context of this work, usability refers to the ease with which people living with dementia can interact and navigate within the MUVE as intended (Mahmoudi Asl et al., Citation2022; World Health Organisation, Citation2012; Yun et al., Citation2020). Acceptability relates to how people living with dementia and their support persons perceive the MUVR application and its ability to meet their needs (Ayala & Elder, Citation2011). Finally, feasibility relates to how the MUVR application can be successfully implemented and used in the home environment by people living with dementia and their support persons (Karsh, Citation2004). The potential to support social connectedness was considered in the context of exploring individual and social presence, observing people living with dementia and their support person’s engagement with the MUVR application during use. This work was also guided by the dimensions of social connectedness described in previous research (Van Bel et al., Citation2009; Visser et al., Citation2011).
2. Materials and methods
2.1. Study design
PAR was the chosen methodology to guide the larger PAR study and this Phase 4. As outlined in the literature, the active participation of people living with dementia and their support persons can support the safe and ethical design of VR applications (Flynn et al., Citation2022a; Muñoz et al., Citation2022). PAR provides one means of facilitating such active participation and has been successfully applied in various dementia studies (Dupuis et al., Citation2021; Goeman et al., Citation2016; Smith & Phillipson, Citation2021). A qualitative PAR design was therefore used to guide this work. Some key intents of PAR include participation, empowerment, reflexivity, mutual respect, collaborative action, learning and knowledge mobilization, and practicality (ICPHR, Citation2013; Kelly, Citation2005; Kemmis & McTaggart, Citation2014; MacDonald, Citation2012). PAR advocates a research approach that values the bottom-up input of key stakeholders, drawing on their personal experiences rather than relying solely on pre-existing theories (Muñoz et al., Citation2022; Trott et al., Citation2020). Focusing on the lived experiences of people living with dementia and their support persons ensures their design preferences are considered from the outset of the research and throughout the design process (Karaosmanoglu et al., Citation2021; Zheng et al., Citation2023). This bottom-up approach is achieved through several cycles of planning, acting and observing, and reflecting, where the outcome of each PAR cycle builds on the previous cycle (Hayes, Citation2012; Kelly, Citation2005; Kemmis & McTaggart, Citation2014; MacDonald, Citation2012). The number of PAR cycles or phases is not predetermined but co-constructed with co-researchers as the research progresses (Baum et al., Citation2006; Kemmis & McTaggart, Citation2014; Trott et al., Citation2020). At the outset of this study a Public and Patient Involvement (PPI) advisory group, consisting of two people living with dementia and their support person were consulted in relation to the proposed PAR phases, the ethics application and assisted with recruitment efforts for the main PAR group. This PAR group (consisting of people living with dementia and their support persons) participated in each phase of the entire PAR study which consisted of four phases (see Appendix A).
Phase 1 explored people living with dementia and their support persons’ experiences of using a VR technology probe in their homes (Flynn et al., Citation2022b). The technology probe familiarized users with single-user VR and its fundamental interactions and provided them with the knowledge of VR to contribute to the succeeding PAR design phases (Flynn et al., Citation2022b). Phase 2 delved into the lived experience of social connectedness, its barriers and facilitators and the perceived usefulness of a MUVR application to support social connectedness (Flynn et al., Citation2024). In Phase 3, online workshops were completed to elicit design preferences to inform the MUVR application development and determine how it could promote or maintain social connectedness. Following the data analysis in Phase 3, a list of design preferences to inform the MUVR application to support social connectedness was generated. These included activity preferences, communication preferences, multisensory content, and avatar design preferences. The MUVR application was then developed by a Games Developer using the Unity 3D game engine (version 2020.3.18). In Phase 4 the aim was to explore the usability, acceptability and feasibility of the MUVR application and its potential to promote or maintain social connectedness. The findings of this phase are the focus of this paper and will be presented below.
2.2. The design, development and introduction of the MUVR application
The commercially available Meta (formally Oculus) Quest 2 HMD and hand-held controllers were chosen for this research due to their lighter weight and higher resolution compared to other commercially available HMDs (Datta et al., Citation2022). Each user had the opportunity to select their avatar, which could be observed from a first-person perspective (i.e., as one would in the real world, looking down at their hands and feet) (see Appendix B). When viewing each other in the MUVE, users could see entire bodies (Kyrlitsias & Michael-Grigoriou, Citation2022). Through their avatars, users could verbally talk to, wave, and move toward one another in real time in the MUVE.
To gradually introduce users to the MUVR application, a three-step process was adopted (Flynn et al., Citation2022a, Citation2022b). Firstly, people living with dementia and their support persons were exposed to a single-user virtual environment (derived from Phase 1) (). The single-user virtual environment was a means of familiarizing and introducing users to the VE, giving them time to get acquainted with the controllers (e.g., grasping and picking up items and moving in the environment). Secondly, the users were introduced to a MUVE with a forested area and a pathway (). Thirdly, the users were introduced to a town square hosting five shared activities (derived from Phase 3), including 360-degree travel videos, gardening, a cinema, funfair games, and a dance hall (). A description of each activity is presented in Appendix C.
Figure 1. The single-user VR familiarization environment.
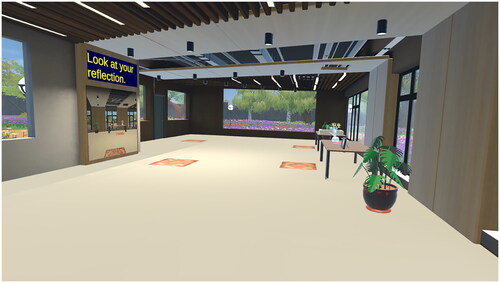
Figure 2. The MUVR forested area.

Figure 3. The MUVR social town square with shared activities.

2.3. The role of the researcher and support persons
The lead researcher, AF (an Occupational Therapist), applied her technical knowledge of the MUVR application and observations captured during its use, to tailor the level of assistance and support needed by people living with dementia and their support persons while using the MUVR application. Having worked with the same group over three PAR phases and four action cycles, the lead researcher had developed a good rapport with and an understanding of the functioning of each person living with dementia, for example, their previous VR use preferences and areas of difficulty. The lead researcher also used an iPad to view people living with dementia and their support person’s interactions in MUVR and provide safe and appropriate assistance. People living with dementia and their support persons were given the option to sit (ideally on a swivel chair) or stand (if deemed safe and appropriate by the researcher) while using MUVR. A boundary area was set up in the physical space (generally the living room or kitchen), which required a 2 m × 2 m physical space per user. Additionally, the lead researcher set up the HMD and controllers, connected them to the internet and loaded the MUVR application before each MUVR session.
During the MUVR experiences, person-centred and tailored support took the form of verbal instructions and physical assistance based on the user’s individual abilities, preferences and home environment. This included providing step-by-step instructions, verbal cueing to orientate their fingers to the controller buttons and adapting the environmental set-up for accessibility (e.g., repositioning their body in the chair). The support persons also brought a nuanced understanding of their family member living with dementia, to encourage engagement and gauge their assistance during MUVR use. As both people living with dementia and their support persons explored the MUVR application together, the support persons guided the person living with dementia in the MUVE and/or instructed them on which controller buttons to use. Support persons also engaged the person living with dementia in conversation, harnessing their abilities, life story, interests and familiarity with technology to increase communication and engagement. Appendices D and E present further details on the MUVR setup and safety procedures.
2.4. Recruitment
Ethical approval for the PAR study and the different phases were obtained from the University of Galway Research Ethics Committee (reference number 2022.08.004). The recruitment process for the larger PAR study as reported in previous publications (Flynn et al., Citation2024), involved recruiting a purposive sample of people living with dementia and their nominated support persons through online means such as a dementia research database and online memory cafés. All people living with dementia and their support persons were recruited during Phase 1 of this larger PAR study, with the same group involved across the various phases and cycles. Inclusion criteria for people living with dementia include those with a self-reported diagnosis of dementia, were over the age of 59 years, resided at home and had a nominated support person who also consented to participate in the research. Supports persons had to be over 18 years of age. The Alzheimer Society of Ireland (Citation2018) capacity assessment guidelines was used by the lead researcher to establish capacity and guide the consent process. Both written and verbal consent was obtained from people living with dementia and their support persons at the start of Phase 4 and process consent was observed throughout.
2.5. Methods of data collection- Phase 4
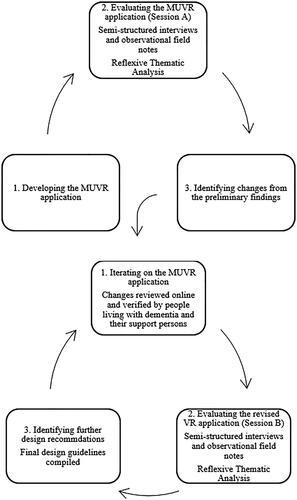
The MUVR application was tested over two sessions (A and B) and two PAR cycles. Both sessions were conducted in the homes of people living with dementia and facilitated by the lead researcher from November 2022 - March 2023. The data collection from session A, was used to refine the MUVR application’s design, which was then re-tested in session B. illustrates the two PAR corresponding cycles, which evolved over sessions A and B. Additionally, an overview of Phase 4 in the context of the entire PAR project is provided in Appendix A.
Figure 4. The two PAR cycles pertaining to Phase 4.
As outlined above, the MUVR application was evaluated over two testing sessions (A and B). Both sessions were conducted in the homes of people living with dementia and accompanied by the lead researcher (AF), with a two to three-month gap between sessions. Observational field notes and individual interviews were the chosen methods of data collection employed to understand and evaluate the application’s usability, acceptability and feasibility at an individual and shared level and it’s potential to promote or maintain social connectedness, consistent with previous work (O’Rourke et al., Citation2023). Separate interview guides were used to interview people living with dementia and their support persons, and probes were included to expand on shorter answers where appropriate (see Appendix F). The interview guides opened with a general discussion surrounding the experiences of people living with dementia and their support persons concerning the use of the MUVR application, opportunities and challenges surrounding its use, and their perceptions of its use to promote or maintain social connectedness. Observational field notes were also collected to capture the subjective experiences of people living with dementia and their support person and provide additional context to their interviews, such as verbal and non-verbal responses during MUVR use. The interview guides and observational field note template were guided by previous VR research conducted with an older adult population (without dementia) and people living with dementia (Mehrabi et al., Citation2022; Rose et al., Citation2019), the concepts of usefulness and ease of use from the Technology Acceptance Model (TAM) proposed by Davis (Citation1989), usability based on the System Usability Scale (Brooke, Citation1996) and presence based on the ITC Sense of Presence Inventory (Lessiter et al., Citation2001).
3. Data analysis
Interviews were audio-recorded, transcribed verbatim and uploaded to NVivo 20 alongside observational field notes to manage the data analysis process. Reflexive thematic analysis (TA) (Braun & Clarke, Citation2019) was used to analyze the interviews and observational field notes. This data analysis approach involved six stages: becoming familiar with the data, coding the data, developing initial themes, developing and reviewing themes, refining, defining and naming the themes, and writing up the report (Braun & Clarke, Citation2019). This approach facilitated an inductive analysis of the data, ensured the lived experiences of end-users were reflected in the findings, and identified the causal mechanisms associated with the application’s usability, acceptability, and feasibility. Coding was completed by the first author, who also carried out the interviews. Another author (WQK) also provided analytic insights into the initial themes and subthemes. Akin to other research, the wider research team (WQK, DC, AB, SR, MB, GR) provided analytic insights and refined the themes and subthemes. Additionally, people living with dementia and their support persons provided feedback on the design preferences arising from Session A and the initial themes and subthemes following Session B through member reflection. Their interpretations of the findings and feedback on the themes and subthemes were consistent with the lead researcher’s. Appendix G provides a detailed outline of the phases and implementation of TA. The findings from the analysis of both sessions (A and B) are presented together to provide a thorough and comprehensive report of the identified themes and subthemes, as described by Evans et al. (Citation2021).
4. Trustworthiness
In establishing trustworthiness, the criteria of Lincoln and Guba (Citation1985), namely, credibility, dependability, confirmability, and transferability, were followed as applied in previous PAR studies (Blanchfield & O'Connor, Citation2022; Bray et al., Citation2021, Citation2022; Cusack et al., Citation2018; Lotfi et al., Citation2020). Multiple data collection methods ensured the credibility and dependability of the findings, accounting for multiple perspectives (i.e., people living with dementia, support persons and the researcher) and sources of evidence (field notes and semi-structured interviews). Member reflections with people living with dementia and their support persons and peer-debriefing meetings with WQK ensured the analysis accurately reflected the experiences of people living with dementia and their support persons and contributed to the credibility and confirmability of the findings. Transferability was supported by detailing the characteristics of people living with dementia and their support persons and the inclusion of quotations to support primary data. An audit trail of the reflexive TA phases was also maintained using NVivo 20 data management software, ensuring transparency and confirmability of the findings.
5. Reflexive statement
Reflexivity played a crucial role in the PAR process and in establishing trustworthiness. Reflexive journaling assisted the lead researcher to remain vigilant for any potential biases that could influence the findings. AF and WQK were both OTs with experience working with people living with dementia, with particular experience in prescribing assistive technology for this population. DC also had extensive experience in dementia research, exploring technology-driven psychosocial interventions. They all, therefore, had unique perspectives on potential barriers and opportunities of digital technology. AF had also been involved in the earlier PAR Phases (1–3) and was heavily involved in designing the MUVR application. AF was particularly aware that their perception of how people living with dementia use technology may be different from first-hand experiences. Reflexive journaling also ensured that the positive aspects of the study were as balanced as possible and that acknowledgement was made of the areas of refinement needed for future work. AF also discussed the findings with people living with dementia and support persons. This provided an opportunity to ensure they reflected on their experience of using the MUVR application and verified the proposed causal mechanisms surrounding some of the challenges associated with MUVR use. This reflexive approach also contributed to the overall trustworthiness of the work.
Three research team members (GR, AB, SR) have experience working in Human-Computer Interaction (HCI), Computer Science and Games Development. They mainly contributed to the technical aspects of MUVR design. Therefore, AF observed the impact of technical additions from the perspective of people living with dementia. This ensured that design iterations were adequately addressed and that the research looked beyond the experiential elements to uncover the underlying technical reasons for the opportunities and challenges faced by people living with dementia and their support persons when using the MUVR application. Another member (MB) had expertise in HCI and the ethical aspects of technology design.
6. Findings
Five people living with dementia and their five family support persons participated in both home testing sessions (A and B). All people living with dementia and their support persons were white and resided in Ireland. People living with dementia were between 59 and 80+ years of age and had been experiencing memory difficulties for 1–7+ years. As noted in previously published PAR phases (Flynn et al., Citation2024), people living with dementia in this study were considered to have mild to moderate dementia, determined by the lead researcher’s clinical reasoning and guided by the National Institute of Aging (Dixon & Lazar, Citation2020) and the American Psychiatric Association (Citation2013) classification of dementia. All support persons were aged between 40 and 69 years and were either spouses or daughters of the people living with dementia. Further information regarding demographics and previous technology experience is provided in and .
Table 1. Demographic characteristics of people living with dementia.
Table 2. Demographic characteristics of the support persons.
Four main themes were created, namely: a) usability insights: getting tangled up and supporting usability, b) the acceptability of the MUVR application, c) the feasibility of using the MUVR application and d) supporting social connectedness. Some themes were also comprised of subthemes, as depicted in . Quotations from interviews and observational field notes extracts are presented to illustrate the findings, and codes are used to differentiate between the accounts of people living with dementia (PwD) and their support persons (SP).
Table 3. Themes and their descriptions.
6.1. Usability insights: “getting tangled up” and supporting usability
Overall, people living with dementia and their support persons considered the MUVR application usable. This was more apparent after session B, where they shared more positive sentiments than previously. This was attributed to revisions to the MUVR application, which were implemented between sessions A and B (summarized in Appendix H). Overall, most support persons indicated no difficulties interacting and navigating the MUVE during either session A or B. This was also mirrored by a few people living with dementia.
“Just moving around [was easy] [.] If I want to get over there, I can and then saying "no I want to go over there" I could go straight away [using the controllers]” (PwD6, session A)
“No, I didn’t find them [controllers] difficult at all!” (PwD2, session B)
“I thought it [interacting and navigating with the controllers] was easy” (SP2, session B)
After session A, there were some negative comments from people living with dementia and their support persons related to the usability of the controllers. The controller was considered “confusing” to operate and difficult for people living with dementia to use during interactive activities, especially activities which required actions such as picking up, throwing items or moving one’s avatar in the MUVE; this was observed to be frustrating for one person living with dementia.
“The circus activities appeared difficult for PwD3. They [PwD3] were unable to move in the MUVE or operate the controllers to engage in the basketball game (they had difficulty picking up the ball or throwing it using the controllers) [.] They [PwD3] became frustrated with the controllers asking, “What am I supposed to be doing?”” (Field note, session A)
More significant usability issues were observed in those people living with dementia who had less experience of using technology and/or who had prolonged memory difficulties across both sessions. A common observation among people living with dementia was that usability difficulties and unfamiliarity with the MUVR application hindered opportunities for social connectedness (especially during session A). Some people living with dementia and their support persons alluded to being “tangled up” in the mechanics of interacting, navigating, and acquainting themselves with the content of the MUVE instead of focusing on the shared experience. However, one couple reported they became more familiar with the MUVE as the sessions progressed or after their second use.
“Initially, maybe for the first half a minute, yeah [the controllers were difficult]. But after that, everything seemed to be streamlined” (PwD7, session A)
“We were caught up in the technology and how it worked today [.] I think we’d be much more relaxed in the environment once we’ve done it a couple of times” (SP7, session A)
Having the same familiar introductory environment within the MUVR each time was also considered important to support usability, as having the same environment was perceived as reassuring for people living with dementia.
“What’s useful is that once you have an environment set up, it will always be the same. So, it’d be familiar. So, for somebody doing it several times, every week or something like that, there’ll be something comforting about that. Nothing is going to change” (SP6, session B)
Despite experiencing challenges with the controllers, people living with dementia still reported that it was “good to have them” (PwD5, session A). Another person with dementia supported the use of one main button to point and click on content in the MUVE, stating that this was “great!” (PwD6, session A).
People living with dementia and their support persons reported that usability had improved in Session B due to revisions made to the MUVR application after Session A. One person with dementia reported:
“Last time was maybe a bit more difficult” (PwD7, session B)
“I thought it was nicer just to look around (engage in the passive, 360-degree travel content) kind of (instead of the more interactive activities requiring controllers in the MUVE)” (SP3, session B)
Engaging in less interactive activities reduced the requirement to use the controllers during session B, which was viewed favorably by people living with dementia.
“I thought it was a nice medium (not having to use the controllers for some activities)” (PwD7, session B)
People living with dementia also nominated their support person to select some of the content in the MUVE, such as multisensory content during activities. This decision was due to their previous usability challenges experienced during Session A, which involved more complex controller use. Despite this, people living with dementia were still required to use the controllers independently to select each desired activity and navigate their avatars in the MUVE.
Although people with dementia needed less assistance during Session B, some people living with dementia still indicated that they found the researcher’s presence supportive in helping them navigate the environment more efficiently.
“It was nice to have you [AF] there [.] When you are on your own, you don’t get as much done. When it’s the two of us, away you go!” (PwD2, session B)
Person-centred assistance was necessary to support the aforementioned usability challenges and create a safe and supportive environment. This assistance aligned with the individual needs of each person with dementia and manifested through verbal prompts and physical assistance from the researcher and their support persons.
“PwD2 was concerned about keeping the controllers by his side and tried to press the buttons. AF then needed to reassure him that he could relax, not use the controllers and just look around in the MUVE [.] He needed assistance orienting his fingers to the controllers, and AF provided hand-over-hand guidance to assist controller use and point and click in the MUVE.” (Field note, session B)
“PwD3 was concerned with clicking songs and needed reassurance from AF that their support person could play/pause the video for them if they desired” (Field note, session B)
One support person supported the notion of person-centred assistance and described how they encouraged their mother with dementia to use the controllers independently; they only intervened when necessary during the MUVR experience:
“It [using MUVR] is about encouraging the person to use the controls themselves” (SP5, session B)
6.2. Acceptability of the MUVR application
6.2.1. Acceptable avatar representation, design and content
Many people living with dementia and their support persons found that the avatar options offered a good variety, catering to various user preferences.
“When he [PwD6] saw the avatars, he noted that there was quite a lot [of avatar options] and also appeared surprised that there were options for both glasses or no glasses.” (Field note, session A)
“I think they [avatar options] were fine; they cross every level.” (SP3, Session B)
“I think it [having fantasy avatar options] is fun. Because I've gone through the other [male and female] options, and they just all looked a bit boring. So, it was nice to be able to choose something else.” (SP6, session B)
The ReadyPlayerMe (RPM) avatar appearance was considered acceptable, with many support persons commenting that they were more youthful, friendly and approachable than MakeHuman (MH) options. Support persons felt that MH options were “old,” “stern,” “masculine,” and “not approachable,” yet only a few people with dementia noted this. Aside from the avatar appearance, people living with dementia and their support persons alluded to the fact that the movement and posture of both RPM and MH in the MUVE were unfamiliar and unnatural as they appeared “crouched down” and “hunched over.”
Support persons were observed to select an avatar that would make it easier for the person living with dementia to recognize and approach them in the MUVE, despite maybe wanting to choose a different avatar.
“You went for the younger-looking, friendlier-looking avatar?” [AF].
“Only because I thought it would help Dad to recognise me. I really wanted to go for the Ninja! [jokingly]” (SP3, session B)
While a few people living with dementia took time to decide on their avatars, many were not concerned with how they were represented across Sessions A and B and required prompting and assistance from the researcher to select an avatar.
“PwD3 (male) chose a female avatar and did not seem interested in scrolling through avatar library options” (Field note, session A)
“PwD2 was not concerned regarding avatar appearance when selecting from the menu options” (Field note, session B)
“PwD7 was assisted by AF to select an avatar, he took time to decide on one that he liked, and that looked like himself” (Field note, session B)
The design of the MUVE and the content placed within the MUVR application were also reported as relatable and acceptable. Additionally, the less interactive travel and music-based activities received the most positive reactions and engagement among people living with dementia and their support persons compared to the more interactive activities (such as can knocking or basketball activities). Overall, the design, content and activities in the MUVR application sparked meaningful conversations about current and past experiences or familiar places, which supported social connectedness.
“It [the MUVR application] is a conversation engager. You can look at a place and discuss it here and make it a reminiscence piece” (SP5, session A)
“PwD5 commented that it was “like the Blaskets [islands]” and drew the connection to this Irish landmark from the 360-degree video content in MUVR” (Field note, session A)
“I think it is good [for social connectedness] [.] Anything that kind of makes someone go, “Oh, look at that. Oh, look at this”. That’s just a bonus in itself. And Dad [PwD3] had that a few times today, he even said he would wear a tutu! [when watching the Swan Lake video] [laughing]. I think it’s great!” (SP3, session A)
One support person described how they worked together with the person living with dementia to decide where to go and what to do in the MUVE:
“We were communicating…about where to go [.] we were able to make decisions between ourselves as to where to go, maybe or comment on the scenery” (SP7, session A)
6.2.2. Perceived usefulness of the MUVR application
People living with dementia and their support persons unanimously expressed a positive attitude toward the MUVR application and its future usefulness. They considered it a “very useful” technology for promoting or maintaining social connectedness among themselves and the wider dementia community. Additionally, they expressed a willingness to adopt and use the MUVR application in the future to promote or maintain social connectedness, further alluding to its acceptability.
“I think it is something that we would definitely use” (SP3, session B)
“Well, I wouldn’t turn it down! [laughing]” (PwD2, session B)
“I think this is something that would work really well here [in their home]” (SP5, session B)
Some support persons reported that the MUVR application’s usefulness and value lay in providing protected time for a shared experience to support social connectedness. One support person noted its ability to take “people out of their everyday environment to something completely different”. This view was further echoed by another support person, who highlighted the distinction between the fully immersive MUVR application and their existing activities:
“I suppose the everyday here [.] he goes for his coffees and whatnot. But it’s very mundane. To do something like that, I think it sparks something new. Just to even have those reactions, I think, is really amazing, and with one another.[.] I think it would be [useful for social connectedness] because we are here from day to day, but the headset is something different for him. It’s a more visual aspect, which is helping as well. So I think it would be good! [.] I think it’s a good idea to do something from here [home]” (SP3, session A)
“You’re taking time out together [when using the MUVR application], you’re doing something together, I’m not doing the housework, and [PwD7] is sitting, looking at a television, you’re working together” [SP7, session B]
“I suppose [using MUVR in the future] with some people that you’re not seeing them every day or something. I have a niece, who might be interested in it.” (PwD6, session A)
“You have the potential for a family member to record when they’re on holiday, and the two of you could experience that holiday [.] It has huge potential, and I think it’s really worth pursuing. It’s fantastic!”(SP5, session B)
6.3. The feasibility of using the MUVR application
This subtheme describes the technical feasibility and practical considerations of using the MUVR application in the home environment. The hardware was considered practical and feasible for use in the home. However, its feasibility depended on an appropriate HMD to support MUVR experiences, sufficient internet connectivity, adequate time spent in the MUVE, and appropriate accommodations in the physical space. Additionally, having the researcher present to assist with setup contributed to the feasibility of using the MUVR application in the home.
The internet connection strength in both urban and rural residences was sufficient to support the MUVR application for Sessions A and B. The Meta Quest 2 was considered comfortable by most people living with dementia and their support persons. In contrast, some stated it was “quite heavy” or strenuous on the head after Session A. Although many people living with dementia and their support persons reported no adverse side effects after either session, one support person did report having a headache after Session A on account of the weight of the HMD. This was rectified for Session B by changing the head strap and face padding on the HMD, with no negative implications reported after this change.
“I liked the sponging around the eye area and over the nose [related to the new face padding]. I found it very comfortable to wear” (SP5, session B)
During Session A, physical movement on standard dining chairs was considered demanding for some people with dementia and their support persons.
“It was stressful trying to turn in that [dining] chair because you couldn’t concentrate on what you were doing. If you had the swivel chair there now and you were going around, I think you’d be more relaxed, and it would make a whole lot of difference” (SP2, session A)
“The only thing is the turning around [on the dining chair]. I wasn’t even probably enjoying it as much as there was quite a bit of turning to be done” (SP7, session A)
By adding a joystick controller function in Session B, people living with dementia were observed to have increased independence and agency to move and rotate their avatar in the MUVE. It also reduced physical movement or strain, particularly for those who did not use a swivel chair. This made it feasible for people living with dementia and their support persons to interact without occupying much space in their home environment. It also enabled the researcher to rotate the user’s avatar position if assistance was required. Some support persons described the usefulness of the joystick to rotate their avatar in the MUVE as follows:
“I didn’t have a swivel chair, so I kept having to turn around. But I could just hit the [joystick] button” (SP3, session B)
“It’s more practical to have a button [joystick] to turn you around” (SP5, session B)
“We’re both a bit tired, so we didn’t last as long this time [during session B as opposed to session A]” [SP3, session B]
6.4. Supporting social connectedness
Overall, the MUVR application was considered to have the potential to promote or maintain the social connectedness of people living with dementia and their support persons. This was demonstrated through shared positive sentiments and observations regarding their experience using the MUVR application together. People living with dementia described the experience as “fantastic,” “interesting,” “mesmerising,” and “fascinating.” Throughout both sessions (A & B), people living with dementia and their support persons demonstrated shared understanding and knowledge of each other’s experience. They were observed to be mutually engaged in affectionate and reciprocal verbal and non-verbal communication, which facilitated social connectedness. An air of excitement and shared fun was observed as they smiled, laughed, waved and danced together when engaged in activities in the MUVE. Overall, as illustrated in the following quotations, the way in which people living with dementia and their support persons used the MUVR application appeared to promote or maintain social connectedness.
“I do think… [mother’s] reaction to it, that [sense of social connectedness] definitely happened” (SP5, session A)
“PwD3 waved as in real life and could see SP3 waving to him also. SP3 moved their hands to dance in the MUVE and PwD3 moved their hands to dance back” (Field note, session A)
“AF observed an instant shift in his [PwD7] body language. He started singing, waving his hands and dancing with the SP. They [PwD/SP7] were both singing with one another, smiling and laughing for the duration of the song. In the cinema room, they watched an ‘Only Fools and Horses’ video, and PwD7 exclaimed, “Delboy!”. They [PwD7 and SP7] laughed together when watching the comedy video” (Field note, session B)
“They [PwD and SP6] were both talking through how to pick up the balls and throw them, and were seen to be laughing when they knocked all of the cans down” (Field note, session A)
“Oh, yeah, it [MUVR] can [support social connectedness], definitely! [.] You could say, “Do you want to watch nature?,” then, start watching it or the comedy if you can find something that the two people in that room like together” (SP2, session B)
These positive sentiments were observed due to the MUVR application facilitating a sense of social presence, closeness and awareness of one another’s avatars in the MUVE. Many people living with dementia and their support persons reported a “sense of being in a virtual environment and exploring it” at an individual and shared level across both sessions.
“I felt like I was in a different place” (PwD7, session A)
“I felt that I was there” (SP5, session A)
“SP2 reported that she felt she was in the garden activity” (Field note, session A)
This sense of social presence and awareness of one another was supported by simple avatar-mediated communication in the MUVE. This made it possible for both users to see the other’s avatar, move toward one another, verbally communicate naturally through voice detection and recognition, and participate in shared activities.
“It was quite like being at home talking in the living room or something [.] quite natural” (PwD7, session A)
“I suppose some of it [contribution of social presence] was the visual in the VR, but also just that we were able to talk to each other in the same room” (SP6, session A)
“Anytime we were in somewhere, I could look around and see her, and then I’d click and go straight over to her” (PwD6, session A)
However, this sense of presence was observed to be limited during certain stages of both sessions when the support person’s avatar was outside the person living with dementia’s field of vision. In such instances, some people living with dementia did not navigate toward or seek their support person’s avatar within the MUVE and required prompting to do so.
“AF needed to physically re-position and prompt PwD2 to turn to see SP2’s avatar” (Field note, session A)
“It was evident that PwD5 required regular prompting to engage with the SP5 avatar, and PwD5 asked who the woman in front of her was, although she could read SP5’s nametag aloud” (Field note, session B)
Another support person reported that they felt that as the MUVR was refined and used more often this would result in more social engagement and support social connectedness:
“It [interacting with one another in MUVR] probably could be better, but that will probably come in time [.] But it was overall a lovely experience. And I think you know, with a few tweaks here and there, it will be perfect.” (SP3, session A).
7. Discussion
Previous studies have highlighted the potential of shared VR experiences to facilitate shared experiences between older adults and people with dementia (Afifi et al., Citation2021, Citation2023; Brimelow et al., Citation2022; Chaze et al., Citation2022; Flynn et al., Citation2022a; Hodge et al., Citation2022). Still, research on VR in dementia care, particularly regarding the application of MUVR, remains an under-researched area (Afifi et al., Citation2021, Citation2023). The findings from this paper suggest that the MUVR application is usable, acceptable, feasible and has the potential to promote or maintain the social connectedness of people living with dementia and their support persons.
Overall, people living with dementia and their support persons considered the MUVR application usable, particularly after the adaptations and revisions made between sessions A and B. During Session B, people living with dementia opted to engage in activities that were more suited to their needs. For example, some engaged in passive activities with less controller use, or they enabled their support persons to select content for them, which needed less reliance on the controllers. Meanwhile, other people living with dementia used the new joystick function to navigate their avatars. One person living with dementia expressed a desire to engage in more interactive and challenging activities with additional levels of complexity. Despite the positive perceptions of the revised MUVR in Session B, it was clear that future refinements are still necessary to support usability, particularly making the controllers easier to use. Indeed, there is inconsistency in VR and dementia research concerning the usability of the controllers for people living with dementia, with some studies reporting that people living with dementia have difficulty interacting with the controllers, while other studies suggest less difficulty (Muñoz et al., Citation2022b, Karaosmanoglu et al., Citation2021).
Notably, in Phase 1 of this PAR project, the same group of people living with dementia were observed to have fewer challenges using the same controller buttons than in Phase 4 (Flynn et al., Citation2022b). There are several potential explanations for this. First, using the MUVR application required additional cognitive and sensory demands, increased activity options, avatar selection, more communication demands and additional interactive content compared to the single-user application previously used in Phase 1. Second, people living with dementia may have experienced decreased functioning due to their dementia, in the period between Phases 1 and 4. Future work might assess the impact of having fewer activity options and avatar choices and using controller-free options or haptic gloves. These latter hands-free interaction methods are reportedly more intuitive and less challenging for older adults and people living with dementia (Astell et al., Citation2018; Mehrabi et al., Citation2022).
Notwithstanding, the MUVR application’s usability was largely contingent on people living with dementia having dedicated person-centred support and facilitation during use, congruent with broader VR literature focused on older adults with varying physical and cognitive difficulties (Abeele et al., Citation2021; Hung et al., Citation2023) and another MUVR study with people living with MCI or dementia (Afifi et al., Citation2021). The familiarity of the support persons and the researchers with the person living with dementia was essential during MUVR use to support usability. The support persons drew on their understanding of the person living with dementia to provide reassurance, gauge the required assistance level and promote engagement in shared activities. This finding is consistent with the broader dementia research (Hodge et al., Citation2018; Lee & Coughlin, Citation2015; Neves et al., Citation2018; Strandenæs et al., Citation2019; Wang et al., Citation2011). Had the MUVR application been facilitated or used with a stranger, it may have resulted in less engagement, as observed in a study by Shah et al. (Citation2022a) when older adults used MUVR with strangers.
Positive engagement and responses to meaningful activities and content indicated the acceptability of the MUVR application. Previous dementia research has also reported positive exchanges between people living with dementia, their peers and support persons when engaged in technology-mediated activities (Astell et al., Citation2010; Bradley et al., Citation2023). Although not explicitly focusing on MUVR, the value of familiar VR activities to increase interaction, engagement and reminiscence is extensively acknowledged in other research with older adults and people living with dementia (Chan et al., Citation2023; Goodall et al., Citation2021; Hodge et al., Citation2018; Kim et al., Citation2021; Matsangidou et al., Citation2023; Shah et al., Citation2022b). While most people living with dementia in this study were mainly satisfied with the MUVR activities, the youngest person living with dementia expressed a desire for more exciting activity options. This difference in preference may be due to their younger age, less time experiencing memory difficulties, or their limited difficulty to use the controllers compared to others. This finding underscores the importance of further diversifying and personalizing activities in future iterations of the MUVR application to sustain engagement (Abeele et al., Citation2021; Karaosmanoglu et al., Citation2021).
Although people living with dementia and their support persons informed the design of avatars during the previous PAR Phase, they expressed limited avatar acceptance in Phase 4 mainly due to their negative perception of the avatar movement and appearance. It must be noted that support persons mainly reported these negative avatar perceptions, while few people living with dementia were concerned with choosing their avatars or their appearance in MUVR. Although this limited avatar acceptance did not have a pronounced impact on the MUVR application’s overall acceptability, it warrants discussion. Despite informing the avatar designs, some avatar movements and appearances were still considered unappealing. Drawing on previous research, several factors could explain these negative avatar perceptions, including the limited available software packages and research to support avatar design for older adults or people living with dementia (Kalantari et al., Citation2023), not achieving the correct level of avatar realism (Baker et al., Citation2021; Carrasco et al., Citation2017), co-designing the avatars with people living with dementia and their support persons remotely rather than face to face in person, or the inability to change the avatar movement or appearance entirely between sessions A and B on account of resource constraints. Future research should focus on developing more advanced software packages and resources to support more sensitive and realistic avatar designs for use with older adults and people living with dementia.
Despite the aforementioned usability and acceptability challenges, people living with dementia and their support persons still indicated that the MUVR application was acceptable and expressed their desire to use it again. This was attributed to the immersive and multisensory nature of the MUVE, as well as the provision of protected time for people living with dementia and their support persons to engage in connected and shared activities. This latter finding was also reported by Afifi et al. (Citation2021). Similarly, research with adult users aged 18–65 years acknowledged that MUVR applications may immerse users in a safe and realistic space and offer opportunities for social connection (Maloney & Freeman, Citation2020). However, despite the ability of the MUVR to offer this immersive experience for social connectedness, older adults with or without dementia may be reluctant to adopt such digital technology due to their fears of it being a replacement for human interaction (Anderson et al., Citation2022; Finnegan & Campbell, Citation2023; Lion et al., Citation2023; Waycott et al., Citation2022). The authors do not suggest that a MUVR application should replace human engagement, rather, it should present a supplementary leisure, recreation and communication activity designed to facilitate shared experiences and social connectedness. This is in keeping with the focus of other VR and dementia research studies (Hodge & Morrissey, Citation2020; Moyle et al., Citation2022).
There is a dearth of VR research completed in the homes of people living with dementia and their support persons, with much of the previous work taking place in more controlled day centers, university or lab-based settings (Afifi et al., Citation2021; Kalantari et al., Citation2023; Xu et al., Citation2023). In the current study, each person living with dementia and their support person were open and enthusiastic to use the MUVR application and participate in both sessions A and B. This may be influenced by the fact that they were using it in their familiar home environment. This aligns with the study of Pardini et al. (Citation2023) involving older adults with cognitive impairment. They noted the importance of using VR in a familiar environment such as their private room within the long-term residential setting when introducing and engaging people to use VR. Moreover, the findings reported in this paper suggest that engaging with a MUVR application in the home environment is feasible, provided there is a comfortable HMD, adequate internet connectivity and a facilitator to assist with setting up and monitoring the MUVR application during use.
People living with dementia and their support person participating in this phase experienced no serious side effects during or after MUVR use, consistent with previous PAR Phases and another MUVR study with older adults (Shah et al., Citation2022b). However, one support person retrospectively reported experiencing a “tension headache” in the afternoon following their MUVR session, which they attributed to the HMD and the limited face padding afforded by the Meta Quest Comfort Strap. This has also been reported in other VR studies with older adults (Drazich et al., Citation2023; Niki et al., Citation2020; Saredakis et al., Citation2021). Similar to these studies, the symptoms reported in this paper were short-term and did not result in significant discomfort or serious risk. Adapting the HMD head straps and face padding for Session B was important to increase comfort and accords with calls for accessible and adaptable HMDs to suit a diverse range of users (Figueroa Jacinto & Kappler, Citation2022).
Koo and Vizer (Citation2019) and Stara et al. (Citation2021) acknowledge that the next generation of technology should transcend the focus on physiological and safety needs and concentrate on supporting higher-level needs such as social connectedness and self-actualization. In the case of this paper, the findings demonstrate the potential of the MUVR application to promote or maintain social connectedness. Visser et al. (Citation2011) mapped the design of their social awareness system to Van Bel et al. (Citation2009) dimensions of social connectedness. They reported a positive impact on the social connectedness of older adults and their family members. Similarly, in this study the design of the MUVR was based on the work of Van Bel et al. (Citation2009) which also yielded positive results. People living with dementia and their support persons, embodied as avatars, experienced a perceived sense of closeness or social presence and awareness of one another’s avatars in the MUVE. Furthermore, the activities and content in the MUVE scaffolded conversation and interaction with one another and allowed both the people living with dementia and their support persons to get to know each other by sharing current and past interests. For example, the findings denoted the positive shared engagement between people living with dementia and their support persons, particularly during the music activities. The benefits of music to support and sustain social relationships are also acknowledged in other dementia research (Creech, Citation2019; Elliott & Gardner, Citation2018). These meaningful activities may have elicited shared understanding, reciprocity and generated knowledge of their respective lived experiences, two dimensions of social connectedness.
However, despite the positive findings reported in this paper the usability and acceptability challenges identified need to be addressed so that the ability of the MUVR application to promote and maintain social connectedness can be enriched. While this paper explored the potential of MUVR to promote or maintain social connectedness within the same geographical area, future work should explore the feasibility of using the MUVR application to support social connectedness with extended family members, friends and/or peers who may live in diverse geographical locations.
In summary, people living with dementia and their support persons identified key challenges and areas for future refinement, which need to be addressed to increase the future acceptability, usability and feasibility of the MUVR application. These included additional interaction methods, further refinement of avatar movement, and greater personalization of the content in the MUVR application (further details of which are summarized in Appendix I). Despite these challenges, it was evident that people living with dementia and their support persons positively engaged with the MUVR application and socially connected and interacted with each other. Moreover, most people living with dementia and their support persons indicated that this technology has the potential to promote their social connectedness.
8. Limitations and strengths
While Phase 1 of the larger PAR project included nine people living with dementia and their nine support persons, only five people living with dementia and their five support persons participated in Phase 4. This was due to dementia-related functional decline over time or pre-existing personal commitments which could not be altered. While small sample sizes are common in PAR studies (Blair & Minkler, Citation2009), a larger sample may have reduced the impact of attrition as well as providing additional insights. This work also aimed to recruit a diverse group of people living with dementia and their support persons, however, the COVID-19 pandemic and physical distancing restrictions presented recruitment difficulties and resulted in an over-representation of males living with dementia (n = 4), female support persons (n = 5) and a lack of representation from those in minority ethnic communities. Future work should strive to recruit a more diverse and inclusive sample.
However, a key strength of this paper included the use of PPI to steer the project in an end-user driven manner, and the use of the PAR approach in the design of the MUVR application; an approach which focused on social connectedness from the outset. Prioritizing the experiential knowledge of people living with dementia and their support persons is often limited in technology usability and acceptability studies (Holthe et al., Citation2018). In the case of this paper, PAR facilitated experiential, hands-on time for people living with dementia and their support persons to use the MUVR application in their own homes. This provided a familiar environment with which to try this relatively novel technology and served to reduce some of the anxiety surrounding its use.
The methods of data collection which were adopted also constituted a strength of this work. Completing separate interviews with people living with dementia and their support persons enabled everyone to have their individual voices heard. Additionally, interviews and observational field notes facilitated triangulation and led to rich experiential insights into MUVR use for this population. Finally, engaging over two PAR cycles in Phase 4, provided people living with dementia and their support persons with the opportunity to review the findings and verify the proposed design preferences that emerged from session A. Their input following Session A subsequently set the agenda for Session B. People living with dementia and their support persons were, therefore, active agents of change within this PAR study beyond just the design process. Finally, the person-centred and holistic design approach adopted during PAR Phases 1–4 as recommended by Koh et al. (Citation2022), Lion et al. (Citation2023), and Waycott et al. (Citation2022), generated frank and open discussions with the participating people living with dementia and their support persons.
9. Conclusion
Research examining the application of MUVR with people living with dementia and their support persons is relatively unexplored. This research facilitated experiential, hands-on time for people living with dementia and their support persons to develop and then refine the MUVR application over two PAR cycles. The findings in this study showed that despite some limitations and challenges, a bespoke MUVR application designed with and for people living with dementia and their support persons was usable, acceptable and feasible and has the potential to promote or maintain their social connectedness. The findings and tangible design preferences generated from this work can be used to assist health and HCI researchers in designing future MUVR applications and inform future social connectedness and VR research.
Supplemental Material
Download PDF (692.4 KB)Acknowledgements
The research team would like to thank the Patient and Public Involvement (PPI) and PAR group members for their continued support and enthusiasm throughout this work. Their lived experiences have been invaluable in steering this research.
Data availability statement
The data that support the findings of this study are openly available in OSF at: https://osf.io/tkdjw/?view_only=68761d8b68dd4f6b9e99b7f3ffb47ea1
Disclosure statement
No potential conflict of interest was reported by the author(s).
Correction Statement
This article has been republished with minor changes. These changes do not impact the academic content of the article.
Additional information
Funding
Notes on contributors
Aisling Flynn
Aisling Flynn is a researcher and Lecturer in Occupational therapy at Bournemouth University. Her research is focused on the design of social technology for people living with dementia. She is dedicated to person-centred and holistic research to support the psychosocial wellbeing of people living with dementia.
Wei Qi Koh
Wei Qi Koh is a researcher and Lecturer in Occupational therapy at the University of Queensland. She is an occupational therapy clinician. Her research interests include supporting the health and wellbeing of older adults and people living with dementia, implementation research, and the use of digital technology to support care.
Gearóid Reilly
Gearóid Reilly is a doctoral candidate at the University of Galway, Ireland. He has experience as a game developer in Virtual Reality. His research is focused on the validation of multi-user social VR as a means of providing social interaction for people living with dementia.
Attracta Brennan
Attracta Brennan is a lecturer at the School of Computer Science at the University of Galway. Her research interests includes adaptive learning systems, serious game based learning, socio-technical systems to support older people, AR/VR and medical informatics especially in the area of osteoporosis, rheumatoid arthritis and other co-morbidities.
Sam Redfern
Sam Redfern is a lecturer at the School of Computer Science at the University of Galway. His current research interests include: virtual reality and multi-user networked virtual environments, game-based learning, and artificial intelligence applications within videogames.
Marguerite Barry
Marguerite Barry is an associate professor at the School of Information & Communication Studies at University College Dublin. She works in HCI and digital media studies on ethics and AI, ethical technology design for health and wellbeing, social expectations and public understanding of ethics and interactivity.
Dympna Casey
Dympna Casey is the established professor of Nursing at the School of Nursing & Midwifery University of Galway. She teaches and supervises students at undergraduate, Masters and PhD levels. Her research interests mainly focus on healthy and active aging, chronic disease management, and developing psychosocial interventions for people with dementia.
References
- Abeele, V. V., Schraepen, B., Huygelier, H., Gillebert, C., Gerling, K., & Ee, R. V. (2021). Immersive virtual reality for older adults: Empirically grounded design guidelines. ACM Transactions on Accessible Computing, 14(3), 1–30. https://doi.org/10.1145/3470743
- Afifi, T., Collins, N. L., Rand, K., Fujiwara, K., Mazur, A., Otmar, C., Dunbar, N. E., Harrison, K., & Logsdon, R. (2021). Testing the feasibility of virtual reality with older adults with cognitive impairments and their family members who live at a distance. Innovation in Aging, 5(2), igab014. https://doi.org/10.1093/geroni/igab014
- Afifi, T., Collins, N., Rand, K., Otmar, C., Mazur, A., Dunbar, N. E., Fujiwara, K., Harrison, K., & Logsdon, R. (2023). Using virtual reality to improve the quality of life of older adults with cognitive impairments and their family members who live at a distance. Health Communication, 38(9), 1904–1915. https://doi.org/10.1080/10410236.2022.2040170
- Alzheimer Society of Ireland. (2018). Position paper on the assisted decision making (capacity) act 2015. https://alzheimer.ie/wp-content/uploads/2018/12/ASI-Position-Assisted-Decision-Making-Capacity-Act-2015.pdf
- Alzheimer’s Society UK. (2013). Dementia 2013: The hidden voice of loneliness. https://www.alzheimers.org.uk/sites/default/files/migrate/downloads/dementia_2013_the_hidden_voice_of_loneliness.pdf
- American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (5th ed.). American Psychiatric Publishing.
- Anderson, M., Menon, R., Oak, K., & Allan, L. (2022). The use of technology for social interaction by people with dementia: A scoping review. PLOS Digital Health, 1(6), e0000053. https://doi.org/10.1371/journal.pdig.0000053
- Appel, L., Ali, S., Narag, T., Mozeson, K., Pasat, Z., Orchanian-Cheff, A., & Campos, J. L. (2021). Virtual reality to promote wellbeing in persons with dementia: A scoping review. Journal of Rehabilitation and Assistive Technologies Engineering, 8, 20556683211053952. https://doi.org/10.1177/20556683211053952
- Astell, A. J., Czarnuch, S., & Dove, E. (2018). System development guidelines from a review of motion-based technology for people with dementia or MCI. Frontiers in Psychiatry, 9, 189. https://doi.org/10.3389/fpsyt.2018.00189
- Astell, A. J., Ellis, M. P., Bernardi, L., Alm, N., Dye, R., Gowans, G., & Campbell, J. (2010). Using a touch screen computer to support relationships between people with dementia and caregivers. Interacting with Computers, 22(4), 267–275. https://doi.org/10.1016/j.intcom.2010.03.003
- Ayala, G. X., & Elder, J. P. (2011). Qualitative methods to ensure acceptability of behavioral and social interventions to the target population. Journal of Public Health Dentistry, 71(1), S69–S79. https://doi.org/10.1111/j.1752-7325.2011.00241.x
- Baker, S., Kelly, R. M., Waycott, J., Carrasco, R., Bell, R., Joukhadar, Z., Hoang, T., Ozanne, E., & Vetere, F. (2021). School’s back: Scaffolding reminiscence in social virtual reality with older adults. Proceedings of the ACM on Human-Computer Interaction, 4(CSCW3), 1–25. https://doi.org/10.1145/3434176
- Baker, S., Waycott, M., Carrasco, R., Kelly, R., Jones, A., Lilley, J., Dow, B., Batchelor, F., Hoang, T., & Vetere, F. (2021). Avatar-mediated communication in social VR: An in-depth exploration of older adult interaction in an emerging communication platform. In Proceedings of the 2021 CHI Conference on Human Factors in Computing Systems, pp. 1–13. https://doi.org/10.1145/3411764.3445752
- Barbosa, A., Ferreira, A. R., Smits, C., Hegerath, F.-M., Vollmar, H. C., Fernandes, L., Craven, M. P., Innes, A., Casey, D., Sezgin, D., Hopper, L., & Øksnebjerg, L. (2024). Use and uptake of technology by people with dementia and their supporters during the COVID-19 pandemic. Aging & Mental Health, 28(1), 83–94. https://doi.org/10.1080/13607863.2022.2163375
- Baum, F., MacDougall, C., & Smith, D. (2006). Participatory action research. Journal of Epidemiology and Community Health, 60(10), 854–857. https://doi.org/10.1136/jech.2004.028662
- Biocca, F., Harms, C., & Burgoon, J. K. (2003). Toward a more robust theory and measure of social presence: Review and suggested criteria. Presence: Teleoperators and Virtual Environments, 12(5), 456–480. https://doi.org/10.1162/105474603322761270
- Birt, L., Griffiths, R., Charlesworth, G., Higgs, P., Orrell, M., Leung, P., & Poland, F. (2020). Maintaining social connections in dementia: A qualitative synthesis. Qualitative Health Research, 30(1), 23–42. https://doi.org/10.1177/1049732319874782
- Blair, T., & Minkler, M. (2009). Participatory action research with older adults: Key principles in practice. The Gerontologist, 49(5), 651–662. https://doi.org/10.1093/geront/gnp049
- Blanchfield, D., & O'Connor, L. (2022). A participatory action research study to inform combined type 2 diabetes and chronic kidney disease care provided in the context of advanced practice nursing. Journal of Advanced Nursing, 78(10), 3427–3443. https://doi.org/10.1111/jan.15362
- Bradley, L., Shanker, S., Murphy, J., Fenge, L.-A., & Heward, M. (2023). Effectiveness of digital technologies to engage and support the wellbeing of people with dementia and family carers at home and in care homes: A scoping review. Dementia (London, England), 22(6), 1292–1313. https://doi.org/10.1177/14713012231178445
- Braun, V., & Clarke, V. (2019). Reflecting on reflexive thematic analysis. Qualitative Research in Sport, Exercise and Health, 11(4), 589–597. https://doi.org/10.1080/2159676X.2019.1628806
- Bray, E. A., George, A., Everett, B., Salamonson, Y., & Ramjan, L. (2021). Protocol for developing a healthcare transition intervention for young people with spinal cord injuries using a participatory action research approach. BMJ Open, 11(7), e053212. https://doi.org/10.1136/bmjopen-2021-053212
- Bray, E. A., Salamonson, Y., Everett, B., George, A., Chapman, I. A., & Ramjan, L. (2022). Transitioning between paediatric and adult healthcare services: A qualitative study of the experiences of young people with spinal cord injuries and parents/caregivers. BMJ Open, 12(11), e065718. https://doi.org/10.1136/bmjopen-2022-065718
- Brimelow, R. E., Thangavelu, K., Beattie, R., & Dissanayaka, N. N. (2022). Feasibility of group-based multiple virtual reality sessions to reduce behavioral and psychological symptoms in persons living in residential aged care. Journal of the American Medical Directors Association, 23(5), 831–837.e2. e832. https://doi.org/10.1016/j.jamda.2021.07.026
- Brooke, J. (1996). SUS: A “quick and dirty” usability scale. In P. Jordan, B. Thomas, & B. Weerdmeester (Eds.), Usability evaluation in industry (pp. 189–194). Taylor & Francis.
- Bryant, L., Sedlarevic, N., Stubbs, P., Bailey, B., Nguyen, V., Bluff, A., Barnett, D., Estela, M., Hayes, C., Jacobs, C., Kneebone, I., Lucas, C., Mehta, P., Power, E., & Hemsley, B. (2022). Collaborative co-design and evaluation of an immersive virtual reality application prototype for communication rehabilitation (DISCOVR prototype). Disability and Rehabilitation. Assistive Technology, 19(1), 90–99. https://doi.org/10.1080/17483107.2022.2063423
- Carrasco, R., Baker, S., Waycott, J., & Vetere, F. (2017). Negotiating stereotypes of older adults through avatars. In Proceedings of the 29th Australian Conference on Computer-Human Interaction, Brisbane, Queensland, Australia. https://doi.org/10.1145/3152771.3152795
- Chan, S. H. M., Qiu, L., Esposito, G., Mai, K. P., Tam, K.-P., & Cui, J. (2023). Nature in virtual reality improves mood and reduces stress: Evidence from young adults and senior citizens. Virtual Reality, 27, 3285–3300. https://doi.org/10.1007/s10055-021-00604-4
- Chaze, F., Hayden, L., Azevedo, A., Kamath, A., Bucko, D., Kashlan, Y., Dube, M., De Paula, J., Jackson, A., Reyna, C., Warren-Norton, K., Dupuis, K., & Tsotsos, L. (2022). Virtual reality and well-being in older adults: Results from a pilot implementation of virtual reality in long-term care. Journal of Rehabilitation and Assistive Technologies Engineering, 9, 20556683211072384. https://doi.org/10.1177/20556683211072384
- Cooper, C., Mansour, H., Carter, C., Rapaport, P., Morgan-Trimmer, S., Marchant, N. L., Poppe, M., Higgs, P., Brierley, J., Solomon, N., Budgett, J., Bird, M., Walters, K., Barber, J., Wenborn, J., Lang, I. A., Huntley, J., Ritchie, K., Kales, H. C., … Palomo, M. (2021). Social connectedness and dementia prevention: Pilot of the APPLE-Tree video-call intervention during the Covid-19 pandemic. Dementia (London, England), 20(8), 2779–2801. https://doi.org/10.1177/14713012211014382
- Creech, A. (2019). Using music technology creatively to enrich later-life: A literature review. Frontiers in Psychology, 10, 117. https://doi.org/10.3389/fpsyg.2019.00117
- Cusack, C., Cohen, B., Mignone, J., Chartier, M. J., & Lutfiyya, Z. (2018). Participatory action as a research method with public health nurses. Journal of Advanced Nursing, 74(7), 1544–1553. https://doi.org/10.1111/jan.13555
- Datta, P., Kaur, A., & Mantri, A. (2022). An exploratory analysis of head mounted displays for VR applications. In 2022 3rd International Conference on Computing, Analytics and Networks (ICAN) (pp. 1–6). IEEE. https://doi.org/10.1109/ICAN56228.2022.10007385
- Davis, F. D. (1989). Perceived usefulness, perceived ease of use, and user acceptance of information technology. MIS Quarterly, 13(3), 319–340. https://doi.org/10.2307/249008
- de Vugt, M., & Dröes, R.-M. (2017). Social health in dementia. Towards a positive dementia discourse. Aging & Mental Health, 21(1), 1–3. https://doi.org/10.1080/13607863.2016.1262822
- Di Marco, L. Y., Marzo, A., Muñoz-Ruiz, M., Ikram, M. A., Kivipelto, M., Ruefenacht, D., Venneri, A., Soininen, H., Wanke, I., Ventikos, Y. A., & Frangi, A. F. (2014). Modifiable lifestyle factors in dementia: A systematic review of longitudinal observational cohort studies. Journal of Alzheimer’s Disease: JAD, 42(1), 119–135. https://doi.org/10.3233/jad-132225
- Dixon, E., & Lazar, A. (2020). The role of sensory changes in everyday technology use by people with mild to moderate dementia. In Proceedings of the 22nd International ACM SIGACCESS Conference on Computers and Accessibility, Virtual Event, Greece. https://doi.org/10.1145/3373625.3417000
- Drazich, B. F., McPherson, R., Gorman, E. F., Chan, T., Teleb, J., Galik, E., & Resnick, B. (2023). In too deep? A systematic literature review of fully-immersive virtual reality and cybersickness among older adults. Journal of the American Geriatrics Society, 71(12), 3906–3915. https://doi.org/10.1111/jgs.18553
- Dröes, R. M., Chattat, R., Diaz, A., Gove, D., Graff, M., Murphy, K., Verbeek, H., Vernooij-Dassen, M., Clare, L., Johannessen, A., Roes, M., Verhey, F., & Charras, K. (2017). Social health and dementia: A European consensus on the operationalization of the concept and directions for research and practice. Aging & Mental Health, 21(1), 4–17. https://doi.org/10.1080/13607863.2016.1254596
- Dröes, R.-M., Boelens-Van Der Knoop, E. C. C., Bos, J., Meihuizen, L., Ettema, T. P., Gerritsen, D. L., Hoogeveen, F., De Lange, J., & SchöLzel-Dorenbos, C. J. M. (2006). Quality of life in dementia in perspective: An explorative study of variations in opinions among people with dementia and their professional caregivers, and in literature. Dementia, 5(4), 533–558. https://doi.org/10.1177/1471301206069929
- Dupuis, S., McAiney, C., Loiselle, L., Hounam, B., Mann, J., & Wiersma, E. C. (2021). Use of participatory action research approach to develop a self-management resource for persons living with dementia. Dementia (London, England), 20(7), 2393–2411. https://doi.org/10.1177/1471301221997281
- Elliott, M., & Gardner, P. (2018). The role of music in the lives of older adults with dementia ageing in place: A scoping review. Dementia (London, England), 17(2), 199–213. https://doi.org/10.1177/1471301216639424
- Evans, N., Boyd, H., Harris, N., Noonan, K., Ingram, T., Jarvis, A., Ridgers, J., & Cheston, R. (2021). The experience of using prompting technology from the perspective of people with Dementia and their primary carers. Aging & Mental Health, 25(8), 1433–1441. https://doi.org/10.1080/13607863.2020.1745145
- Figueroa Jacinto, R., & Kappler, E. (2022). A discussion on accessibility, inclusivity, cultural design considerations, and health & safety advisories for virtual reality head mounted displays. Proceedings of the Human Factors and Ergonomics Society Annual Meeting, 66(1), 1706–1710. https://doi.org/10.1177/1071181322661200
- Finnegan, D. J., & Campbell, S. (2023). Tackling loneliness and isolation in older adults with virtual reality: How do we move forward? Gerontology & Geriatric Medicine, 9, 23337214231186204. https://doi.org/10.1177/23337214231186204
- Flynn, A., Barry, M., Qi Koh, W., Reilly, G., Brennan, A., Redfern, S., & Casey, D. (2022b). Introducing and familiarising older adults living with dementia and their caregivers to virtual reality. International Journal of Environmental Research and Public Health, 19(23), 16343. https://doi.org/10.3390/ijerph192316343
- Flynn, A., Brennan, A., Barry, M., Redfern, S., & Casey, D. (2024). Social connectedness and the role of virtual reality: Experiences and perceptions of people living with dementia and their caregivers. Disability and Rehabilitation. Assistive Technology, 1–15. https://doi.org/10.1080/17483107.2024.2310262
- Flynn, A., Healy, D., Barry, M., Brennan, A., Redfern, S., Houghton, C., & Casey, D. (2022a). Key stakeholders’ experiences and perceptions of virtual reality for older adults living with dementia: Systematic review and thematic synthesis. JMIR Serious Games, 10(4), e37228. https://doi.org/10.2196/37228
- Goeman, D., Michael, J., King, J., Luu, H., Emmanuel, C., & Koch, S. (2016). Partnering with consumers to develop and evaluate a Vietnamese Dementia Talking-Book to support low health literacy: A qualitative study incorporating codesign and participatory action research. BMJ Open, 6(9), e011451. https://doi.org/10.1136/bmjopen-2016-011451
- Goodall, G., André, L., Taraldsen, K., & Serrano, J. A. (2021). Supporting identity and relationships amongst people with dementia through the use of technology: A qualitative interview study. International Journal of Qualitative Studies on Health and Well-Being, 16(1), 1920349. https://doi.org/10.1080/17482631.2021.1920349
- Hanna, K., Giebel, C., Tetlow, H., Ward, K., Shenton, J., Cannon, J., Komuravelli, A., Gaughan, A., Eley, R., Rogers, C., Rajagopal, M., Limbert, S., Callaghan, S., Whittington, R., Butchard, S., Shaw, L., & Gabbay, M. (2021). Emotional and mental wellbeing following COVID-19 public health measures on people living with dementia and carers. Journal of Geriatric Psychiatry and Neurology, 35(3), 344–352. https://doi.org/10.1177/0891988721996816
- Hayes, G. R. (2012). Taking action in your research. Interactions, 19(4), 50–53. http://doi.org/10.1145/2212877.2212890
- Heins, P., Boots, L. M. M., Koh, W. Q., Neven, A., Verhey, F. R. J., & de Vugt, M. E. (2021). The effects of technological interventions on social participation of community-dwelling older adults with and without dementia: A systematic review. Journal of Clinical Medicine, 10(11), 2308. https://doi.org/10.3390/jcm10112308
- Henderson, A., Korner-Bitensky, N., & Levin, M. (2007). Virtual reality in stroke rehabilitation: A systematic review of its effectiveness for upper limb motor recovery. Topics in Stroke Rehabilitation, 14(2), 52–61. https://doi.org/10.1310/tsr1402-52
- Hodge, J., & Morrissey, K. (2020). Sharing a virtual world with people living with dementia. In R. Brankaert & G. Kenning (Eds.), HCI and design in the context of dementia (pp. 237–253). Springer International Publishing. https://doi.org/10.1007/978-3-030-32835-1_15
- Hodge, J., Balaam, M., Hastings, S., & Morrissey, K. (2018). Exploring the Design of Tailored Virtual Reality Experiences for People with Dementia. In Proceedings of the 2018 CHI Conference on Human Factors in Computing Systems. ACM. https://doi.org/10.1145/3173574.3174088
- Hodge, J., Foley, S., Lambton-Howard, D., Booi, L., Montague, K., Coulter, S., Kirk, D., & Morrissey, K. (2022). Exploring participants’ representations and shifting sensitivities in a hackathon for dementia. ACM Transactions on Computer-Human Interaction, 30(3), 1–35. https://doi.org/10.1145/3571814
- Hoel, V., Ambugo, E. A., & Wolf-Ostermann, K. (2022). Sustaining our relationship: Dyadic interactions supported by technology for people with dementia and their informal caregivers. International Journal of Environmental Research and Public Health, 19(17), 10956. https://doi.org/10.3390/ijerph191710956
- Holthe, T., Halvorsrud, L., Karterud, D., Hoel, K.-A., & Lund, A. (2018). Usability and acceptability of technology for community-dwelling older adults with mild cognitive impairment and dementia: A systematic literature review. Clinical Interventions in Aging, 13, 863–886. https://doi.org/10.2147/CIA.S154717
- Huber, M., Knottnerus, J. A., Green, L., Van der Horst, H., Jadad, A. R., Kromhout, D., Leonard, B., Lorig, K., Loureiro, M. I., Van der Meer, J. W. M., & Schnabel, P. (2011). How should we define health? BMJ (Clinical Research ed.), 343(2), d4163–d4163. https://doi.org/10.1136/bmj.d4163
- Hung, L., Chow, B., Shadarevian, J., O'Neill, R., Berndt, A., Wallsworth, C., Horne, N., Gregorio, M., Mann, J., Son, C., & Chaudhury, H. (2021). Using touchscreen tablets to support social connections and reduce responsive behaviours among people with dementia in care settings: A scoping review. Dementia (London, England), 20(3), 1124–1143. https://doi.org/10.1177/1471301220922745
- Hung, L., Mann, J., Wallsworth, C., Upreti, M., Kan, W., Temirova, A., Wong, K. L. Y., Ren, H., To-Miles, F., Wong, J., Lee, C., Kar Lai So, D., & Hardern, S. (2023). Facilitators and barriers to using virtual reality and its impact on social engagement in aged care settings: A scoping review. Gerontology & Geriatric Medicine, 9, 23337214231166355. https://doi.org/10.1177/23337214231166355
- ICPHR. (2013). Position paper 2: Participatory health research: A guide to ethical principals and practice. Version: October 2013. http://www.icphr.org/uploads/2/0/3/9/20399575/ichpr_position_paper_2_ethics_-_version_october_2013.pdf
- Jerald, J. (2015). The VR book: Human-centered design for virtual reality. Morgan & Claypool Publishers. http://ebookcentral.proquest.com/lib/nuig/detail.action?docID=6952709
- Kalantari, S., Xu, T. B., Mostafavi, A., Kim, B., Dilanchian, A., Lee, A., Boot, W. R., & Czaja, S. J. (2023). Using immersive virtual reality to enhance social interaction among older adults: A cross-site investigation. Innovation in Aging, 7(4), igad031. https://doi.org/10.1093/geroni/igad031
- Karaosmanoglu, S., Rings, S., Kruse, L., Stein, C., & Steinicke, F. (2021). Lessons learned from a human-centered design of an immersive exergame for people with dementia. Proceedings of the ACM on Human-Computer Interaction, 5(CHI PLAY), 1–27. https://doi.org/10.1145/3474679
- Karsh, B. (2004). Beyond usability: Designing effective technology implementation systems to promote patient safety. Quality and Safety in Health Care, 13(5), 388–394. https://doi.org/10.1136/qshc.2004.010322
- Kelly, P. J. (2005). Practical suggestions for community interventions using participatory action research. Public Health Nursing (Boston, Mass.), 22(1), 65–73. https://doi.org/10.1111/j.0737-1209.2005.22110.x
- Kemmis, S., & McTaggart, R. (2014). The action research planner: Doing critical participatory action research. Springer.
- Kim, J.-H., Park, S., & Lim, H. (2021). Developing a virtual reality for people with dementia in nursing homes based on their psychological needs: A feasibility study. BMC Geriatrics, 21(1), 167. https://doi.org/10.1186/s12877-021-02125-w
- Kim, O., Pang, Y., & Kim, J.-H. (2019). The effectiveness of virtual reality for people with mild cognitive impairment or dementia: A meta-analysis. BMC Psychiatry, 19(1), 219. https://doi.org/10.1186/s12888-019-2180-x
- Koh, W. Q., Heins, P., Flynn, A., Mahmoudi Asl, A., Garcia, L., Malinowsky, C., & Brorsson, A. (2022). Bridging gaps in the design and implementation of socially assistive technologies for dementia care: The role of occupational therapy. Disability and Rehabilitation. Assistive Technology, 19(3), 595–603. https://doi.org/10.1080/17483107.2022.2111610
- Koo, B. M., & Vizer, L. M. (2019). Examining mobile technologies to support older adults with dementia through the lens of personhood and human needs: Scoping review. JMIR mHealth and uHealth, 7(11), e15122. https://doi.org/10.2196/15122
- Kyrlitsias, C., & Michael-Grigoriou, D. (2022). Social interaction with agents and avatars in immersive virtual environments: A survey. Frontiers in Virtual Reality, 2, 1–13. https://doi.org/10.3389/frvir.2021.786665
- Lee, C., & Coughlin, J. F. (2015). PERSPECTIVE: Older adults’ adoption of technology: An integrated approach to identifying determinants and barriers. Journal of Product Innovation Management, 32(5), 747–759. https://doi.org/10.1111/jpim.12176
- Lessiter, J., Freeman, J., Keogh, E., & Davidoff, J. (2001). A cross-media presence questionnaire: The ITC-sense of presence inventory. Presence: Teleoperators and Virtual Environments, 10(3), 282–297. https://doi.org/10.1162/105474601300343612
- Lincoln, Y. S., & Guba, E. G. (1985). Naturalistic inquiry. Sage.
- Lion, K. M., Murfield, J., Sriram, D., Sung, B., Cook, G., Estai, M., Jones, C., Klein, B., Liddle, J., Pu, L., Moyle, W., & Collaborative, T. A. (2023). Technology in aged care: A qualitative survey of academic, research, and technology industry professionals. Contemporary Nurse, 59(4–5), 311–322. https://doi.org/10.1080/10376178.2023.2242978
- Lotfi, M., Zamanzadeh, V., Ostadi, A., Jalili Fazel, M., Nobakht, A., & Khajehgoodari, M. (2020). Development of family-based follow-up care system for patients with burn in Iran: Participatory action research. Nursing Open, 7(4), 1101–1109. https://doi.org/10.1002/nop2.483
- MacDonald, C. (2012). Understanding participatory action research: A qualitative research methodology option. The Canadian Journal of Action Research, 13(2), 34–50. https://doi.org/10.33524/cjar.v13i2.37
- Mahmoudi Asl, A., Molinari Ulate, M., Franco Martin, M., & van der Roest, H. (2022). Methodologies used to study the feasibility, usability, efficacy, and effectiveness of social robots for elderly adults: Scoping review. Journal of Medical Internet Research, 24(8), e37434. https://doi.org/10.2196/37434
- Maloney, D., & Freeman, G. (2020). Falling asleep together: What makes activities in social virtual reality meaningful to users. In Proceedings of the Annual Symposium on Computer-Human Interaction in Play, Virtual Event, Canada. https://doi.org/10.1145/3410404.3414266
- Martirosov, S., Bureš, M., & Zítka, T. (2022). Cyber sickness in low-immersive, semi-immersive, and fully immersive virtual reality. Virtual Reality, 26(1), 15–32. https://doi.org/10.1007/s10055-021-00507-4
- Masoud, S. S., Meyer, K. N., Martin Sweet, L., Prado, P. J., & White, C. L. (2021). “We don’t feel so alone”: A qualitative study of virtual memory cafés to support social connectedness among individuals living with dementia and care partners during COVID-19. Frontiers in Public Health, 9, 660144. https://doi.org/10.3389/fpubh.2021.660144
- Matsangidou, M., Solomou, T., Frangoudes, F., Papayianni, E., & Pattichis, C. S. (2023). Offering outworld experiences to in-patients with dementia through virtual reality: Mixed methods study. JMIR Aging, 6, e45799. https://doi.org/10.2196/45799
- Mehrabi, S., Muñoz, J. E., Basharat, A., Boger, J., Cao, S., Barnett-Cowan, M., & Middleton, L. E. (2022). Immersive virtual reality exergames to promote the well-being of community-dwelling older adults: Protocol for a mixed methods pilot study. JMIR Research Protocols, 11(6), e32955. https://doi.org/10.2196/32955
- Moyle, W., Arnautovska, U., Ownsworth, T., & Jones, C. (2017). Potential of telepresence robots to enhance social connectedness in older adults with dementia: An integrative review of feasibility. International Psychogeriatrics, 29(12), 1951–1964. https://doi.org/10.1017/S1041610217001776
- Moyle, W., Pu, L., Murfield, J., Sung, B., Sriram, D., Liddle, J., Estai, M., & Lion, K. (2022). Consumer and provider perspectives on technologies used within aged care: An Australian qualitative needs assessment survey. Journal of Applied Gerontology: The Official Journal of the Southern Gerontological Society, 41(12), 2557–2565. https://doi.org/10.1177/07334648221120082
- Muñoz, J., Mehrabi, S., Li, Y., Basharat, A., Middleton, L. E., Cao, S., Barnett-Cowan, M., & Boger, J. (2022). Immersive virtual reality exergames for persons living with dementia: User-centered design study as a multistakeholder team during the COVID-19 pandemic. JMIR Serious Games, 10(1), e29987-e29987. https://doi.org/10.2196/29987
- Neves, B. B., Franz, R. L., Munteanu, C., & Baecker, R. (2018). Adoption and feasibility of a communication app to enhance social connectedness amongst frail institutionalized oldest old: An embedded case study. Information, Communication & Society, 21(11), 1681–1699. https://doi.org/10.1080/1369118X.2017.1348534
- Niki, K., Yahara, M., Inagaki, M., Takahashi, N., Watanabe, A., Okuda, T., Ueda, M., Iwai, D., Sato, K., & Ito, T. (2020). Immersive virtual reality reminiscence reduces anxiety in the oldest-old without causing serious side effects: A single-center, pilot, and randomized crossover study. Frontiers in Human Neuroscience, 14, 598161. https://doi.org/10.3389/fnhum.2020.598161
- Nowak, K. L., & Fox, J. (2018). Avatars and computer-mediated communication: A review of the definitions, uses, and effects of digital representations. Review of Communication Research, 6, 30–53. https://doi.org/10.12840/issn.2255-4165.2018.06.01.015
- Oppert, M. L., Ngo, M., Lee, G. A., Billinghurst, M., Banks, S., & Tolson, L. (2023). Older adults’ experiences of social isolation and loneliness: Can virtual touring increase social connectedness? A pilot study. Geriatric Nursing (New York, N.Y.), 53, 270–279. https://doi.org/10.1016/j.gerinurse.2023.08.001
- O’Rourke, H. M., Swindle, J., Chacinski, D., Dal Pizzol, F. L. F., Lee, H., Hoben, M., Hopper, T., McGilton, K. S., & Boscart, V. (2023). Connecting today: Feasibility and acceptability of a remote visiting program for people living with dementia in long-term care homes. Dementia (London, England), 22(7), 1321–1347. https://doi.org/10.1177/14713012231176858
- Orr, N., Yeo, N. L., Dean, S. G., White, M. P., & Garside, R. (2021). “It makes you feel that you are there”: Exploring the acceptability of virtual reality nature environments for people with memory loss. Geriatrics, 6(1), 27. https://doi.org/10.3390/geriatrics6010027
- Pandey, V., Astha, A., Mishra, N., Greeshma, R., Lakshmana, G., Jeyavel, S., Rajkumar, E., & Prabhu, G. (2021). Do social connections and digital technologies act as social cure during COVID-19? Frontiers in Psychology, 12, 634621. https://doi.org/10.3389/fpsyg.2021.634621
- Pardini, S., Gabrielli, S., Gios, L., Dianti, M., Mayora-Ibarra, O., Appel, L., Olivetto, S., Torres, A., Rigatti, P., Trentini, E., Leonardelli, L., Bernardi, M., Lucianer, M., Forti, S., & Novara, C. (2023). Customized virtual reality naturalistic scenarios promoting engagement and relaxation in patients with cognitive impairment: A proof-of-concept mixed-methods study. Scientific Reports, 13(1), 20516. https://doi.org/10.1038/s41598-023-47876-1
- Patterson, C. (2018). World Alzheimer report 2018. Alzheimer’s Disease International (ADI).
- Pinto-Bruno, Á. C., García-Casal, J. A., Csipke, E., Jenaro-Río, C., & Franco-Martín, M. (2017). ICT-based applications to improve social health and social participation in older adults with dementia. A systematic literature review. Aging & Mental Health, 21(1), 58–65. https://doi.org/10.1080/13607863.2016.1262818
- Quinn, C., Pickett, J. A., Litherland, R., Morris, R. G., Martyr, A., & Clare, L. (2022). Living well with dementia: What is possible and how to promote it. International Journal of Geriatric Psychiatry, 37(1), 1–7. https://doi.org/10.1002/gps.5627
- Rausch, A., Caljouw, M. A. A., & van der Ploeg, E. S. (2017). Keeping the person with dementia and the informal caregiver together: A systematic review of psychosocial interventions. International Psychogeriatrics, 29(4), 583–593. https://doi.org/10.1017/S1041610216002106
- Rose, V., Stewart, I., Jenkins, K. G., Tabbaa, L., Ang, C. S., & Matsangidou, M. (2019). Bringing the outside in: The feasibility of virtual reality with people with dementia in an inpatient psychiatric care setting. Dementia (London, England), 20(1), 106–129. https://doi.org/10.1177/1471301219868036
- Rutledge, P. (2011). Social networks: What Maslow misses. Psychology Today, 1–4.
- Sancho-Esper, F., Ostrovskaya, L., Rodriguez-Sanchez, C., & Campayo-Sanchez, F. (2022). Virtual reality in retirement communities: Technology acceptance and tourist destination recommendation. Journal of Vacation Marketing, 29(2), 275–290. https://doi.org/10.1177/13567667221080567
- Saredakis, D., Keage, H. A. D., Corlis, M., Ghezzi, E. S., Loffler, H., & Loetscher, T. (2021). The effect of reminiscence therapy using virtual reality on apathy in residential aged care: Multisite nonrandomized controlled trial. Journal of Medical Internet Research, 23(9), e29210. https://doi.org/10.2196/29210
- Shah, S. H. H., Hameed, I. A., Karlsen, A. S. T., & Solberg, M. (2022a). Towards a social VR-based exergame for elderly users: An exploratory study of acceptance, experiences and design principles. virtual, augmented and mixed reality: Design and development. In International Conference on Human-Computer Interaction (pp. 495–504). Springer International Publishing.
- Shah, S. H. H., Karlsen, A. S. T., Solberg, M., & Hameed, I. A. (2022b). A social VR-based collaborative exergame for rehabilitation: Codesign, development and user study. Virtual Reality, 27(4), 3403–3420. https://doi.org/10.1007/s10055-022-00721-8
- Siriaraya, P., & Ang, C. S. (2014). Recreating living experiences from past memories through virtual worlds for people with dementia. In Proceedings of the SIGCHI Conference on Human Factors in Computing Systems, Toronto, Ontario, Canada. https://doi.org/10.1145/2556288.2557035
- Smith, L., & Phillipson, L. (2021). Thinking through participatory action research with people with late-stage dementia: Research note on mistakes, creative methods and partnerships. International Journal of Social Research Methodology, 24(6), 775–780. https://doi.org/10.1080/13645579.2020.1810997
- Stara, V., Vera, B., Bolliger, D., Rossi, L., Felici, E., Di Rosa, M., de Jong, M., & Paolini, S. (2021). Usability and acceptance of the embodied conversational agent Anne by people with dementia and their caregivers: Exploratory study in home environment settings. JMIR Mhealth Uhealth, 9(6), e25891. https://doi.org/10.2196/25891
- Strandenæs, M. G., Lund, A., & Rokstad, A. M. M. (2019). Facilitation of activities for people with dementia in day care: A qualitative study exploring the experiences of staff. Journal of Multidisciplinary Healthcare, 12(null), 503–513. https://doi.org/10.2147/JMDH.S198024
- Sun, W., Horsburgh, S., Quevedo, A., Liscano, R., Tabafunda, A., Akhter, R., Lemonde, M., Kapralos, B., Tokuhiro, A., Bartfay, E., & Ashtarieh, B. (2020). Advancing reminiscence therapy through virtual reality application to promote social connectedness of persons with dementia. Gerontechnology, 19(s), 1–1. https://doi.org/10.4017/gt.2020.19.s.70041
- Trott, C. D., Sample McMeeking, L. B., & Weinberg, A. E. (2020). Participatory action research experiences for undergraduates: Forging critical connections through community engagement. Studies in Higher Education, 45(11), 2260–2273. https://doi.org/10.1080/03075079.2019.1602759
- Tuijt, R., Frost, R., Wilcock, J., Robinson, L., Manthorpe, J., Rait, G., & Walters, K. (2021). Life under lockdown and social restrictions - the experiences of people living with dementia and their carers during the COVID-19 pandemic in England. BMC Geriatrics, 21(1), 301. https://doi.org/10.1186/s12877-021-02257-z
- Van Bel, D. T., Smolders, K. C., IJsselsteijn, W. A., & De Kort, Y. (2009). Social connectedness: Concept and measurement [Paper presentation]. Proceedings of the 5th International Conference on Intelligent Environments, Barcelona, Spain.
- Van Orden, K. A., & Heffner, K. L. (2022). Promoting social connection in dementia caregivers: A call for empirical development of targeted interventions. The Gerontologist, 62(9), 1258–1265. https://doi.org/10.1093/geront/gnac032
- Vernooij-Dassen, M., & Jeon, Y.-H. (2016). Social health and dementia: The power of human capabilities. International Psychogeriatrics, 28(5), 701–703. https://doi.org/10.1017/S1041610216000260
- Vernooij-Dassen, M., Moniz-Cook, E., & Jeon, Y.-H. (2018). Social health in dementia care: Harnessing an applied research agenda. International Psychogeriatrics, 30(6), 775–778. https://doi.org/10.1017/S1041610217002769
- Visser, T., Vastenburg, M. H., & Keyson, D. V. (2011). Designing to support social connectedness: The case of SnowGlobe. International Journal of Design, 5(3), 129–142.
- Wang, A., Redington, L., Steinmetz, V., & Lindeman, D. (2011). The ADOPT model: Accelerating diffusion of proven technologies for older adults. Ageing International, 36(1), 29–45. https://doi.org/10.1007/s12126-010-9072-1
- Waycott, J., Kelly, R. M., Baker, S., Barbosa Neves, B., Thach, K. S., & Lederman, R. (2022). The role of staff in facilitating immersive virtual reality for enrichment in aged care: An ethic of care perspective. In Proceedings of the 2022 CHI Conference on Human Factors in Computing Systems (pp. 1–17). ACM. https://doi.org/10.1145/3491102.3501956
- Waycott, J., Vetere, F., & Ozanne, E. (2019). Building social connections: A framework for enriching older adults’ social connectedness through information and communication technologies. In B. B. Neves & F. Vetere (Eds.), Ageing and digital technology: Designing and evaluating emerging technologies for older adults (pp. 65–82). Springer Singapore. https://doi.org/10.1007/978-981-13-3693-5_5
- Wei, X., Gu, Y., Kuang, E., Wang, X., Cao, B., Jin, X., & Fan, M. (2023). Bridging the generational gap: Exploring how virtual reality supports remote communication between grandparents and grandchildren. In Proceedings of the 2023 CHI Conference on Human Factors in Computing Systems (pp. 1–15). ACM. https://doi.org/10.1145/3544548.3581405
- World Health Organisation. (2012). Dementia: A public health priority. https://www.who.int/publications/i/item/dementia-a-public-health-priority
- Xu, T. B., Mostafavi, A., Kim, B. C., Lee, A. A., Boot, W., Czaja, S., & Kalantari, S. (2023). Designing virtual environments for social engagement in older adults: A qualitative multi-site study. In Proceedings of the 2023 CHI Conference on Human Factors in Computing Systems (pp. 1–15). https://doi.org/10.1145/3544548.3581262
- Yu, J., Lam, C. L. M., & Lee, T. M. C. (2016). Perceived loneliness among older adults with mild cognitive impairment. International Psychogeriatrics, 28(10), 1681–1685. https://doi.org/10.1017/S1041610216000430
- Yun, S. J., Kang, M.-G., Yang, D., Choi, Y., Kim, H., Oh, B.-M., & Seo, H. G. (2020). Cognitive training using fully immersive, enriched environment virtual reality for patients with mild cognitive impairment and mild dementia: Feasibility and usability study. JMIR Serious Games, 8(4), e18127. https://doi.org/10.2196/18127
- Zamanifard, S., & Freeman, G. (2023). A surprise birthday party in VR: Leveraging social virtual reality to maintain existing close ties over distance. In International Conference on Information (pp. 268–285). Springer Nature Switzerland.
- Zheng, J., Gresham, M., Phillipson, L., Hall, D., Jeon, Y.-H., Brodaty, H., & Low, L.-F. (2023). Exploring the usability, user experience and usefulness of a supportive website for people with dementia and carers. Disability and Rehabilitation. Assistive Technology, 1–13. https://doi.org/10.1080/17483107.2023.2180546