
Abstract
Objective: The potential benefit or harm of immersion (egocentric perspective) and distancing (observer perspective) on negative experiences are unclear and have not been empirically investigated in therapy. This is a first exploratory study aimed to analyze and compare the perspectives adopted on reflection (immersion and distancing) of negative experiences across therapy and the relationship between them and depressive symptoms in contrasting therapeutic outcomes of emotion-focused therapy (EFT). Method: Three good-outcomes cases and three poor-outcomes cases of EFT, diagnosed with mild to moderate depression at the beginning of therapy, were randomly selected. Immersion and distancing on negative experiences were analyzed using the measure of immersed and distanced speech. The depressive symptoms were assessed by the Beck Depression Inventory-II. Results: Significant differences across sessions were only found in the good-outcome cases which showed a significant decrease of immersion and an increase of distancing, and this evolution pattern was found related to the reduction of symptoms. Moreover, at the beginning of therapy, distancing was higher in the poor-outcome cases rather than in the good-outcome cases. Conclusion: The progressive and significant evolution from higher immersion at the initial phase to higher distancing in the final phase may be helpful in EFT for depression.
Obiettivo: Il potenziale beneficio o danno dell'immersione (prospettiva egocentrica) e distanziamento (prospettiva osservatore) sulle esperienze negative non sono chiare e non sono state indagate empiricamente in terapia. Questo è un primo studio epslorativo che si propone di analizzare e confrontare le prospettive adottate sulla riflessione (immersione e distanziamento) di esperienze negative nel corso della terapia e la relazione tra esse e i sintomi depressivi nell'ostacolare gli esiti terapeutici della terapia focalizzata sulle emozioni (EFT). Metodo: Tre casi a buon esito e tre casi a esito negativo di EFT, diagnosticati con depressione da media a moderata all'inizio della terapia, sono stati selezionati casualmente. Immersione e distanziamento sulle esperienze negative sono state analizzate usando la misura del discorso immerso e distanziato. I sintomi depressivi sono stati valutati con il Beck Depression Inventory-II. Risultati: Differenze significative sono state trovate solo nei casi a buon esito che hanno mostrato un significativo decremento dell'immersione e un aumento del distanziamento, e questa pattern era associato alla riduzione dei sintomi. Inoltre, all'inizio della terapia, il distanziamento era più elevato nei casi a esito negativo più che nei casi a esito positivo. Conclusione: La progressiva e significativa evoluzione da una maggiore immersione nella fase iniziale a un distanziamento più elevato nella fase finale può essere utile nella EFT per la depressione.
Significato clinico o metodologico di questo articolo: Questo studio evidenzia che l'evoluzione della prospettiva adottata nella emotion-focused therapy (immersione/distanziamento) è associata alla condizione clinica dei clienti con sintomi depressivi, suggerendo che l'immersione e il distanziamento hanno un potenziale terapeutico che dovrebbe essere considerato per il trattamento della depressione.
Resumo
Objetivo: O potencial benefício ou dano da imersão (perspectiva egocêntrica) e distanciamento (perspectiva do observador) em experiências negativas não são claros e não foram investigados empiricamente na terapia. Este é um primeiro estudo exploratório, com o objetivo de analisar e comparar as perspectivas adotadas na reflexão (imersão e distanciamento) sobre experiências negativas na terapia e a relação entre elas e sintomas depressivos em resultados terapêuticos contrastantes da terapia focada na emoção (EFT). Método: Três casos com bom resultado e três com pobre resultado de EFT, diagnosticados com depressão leve a moderada no início da terapia, foram selecionados aleatoriamente. A imersão e o distanciamento em experiências negativas foram analisados através da medida da fala imersa e distanciada. Os sintomas depressivos foram avaliados pelo Inventário de Depressão de Beck II. Resultados: Diferenças significativas entre as sessões foram encontradas apenas nos casos de bom resultado, que mostraram uma diminuição significativa da imersão e um aumento do distanciamento, e esse padrão de evolução foi encontrado relacionado à redução dos sintomas. Além disso, no início da terapia, o distanciamento era maior nos casos de baixo resultado do que nos casos de pobre resultado. Conclusão: A evolução progressiva e significativa de maior imersão na fase inicial para maior distanciamento na fase final pode ser útil na EFT para depressão.
Significado clínico ou metodológico deste artigo: Este estudo destaca que o padrão de evolução da perspectiva adotada na terapia focada na emoção (imersa / distanciada) está associada à condição clínica de clientes com sintomas depressivos, sugerindo que a imersão e o distanciamento têm potencial terapêutico que deve ser considerado para o tratamento da depressão.
摘要
目的:目前還未有實證研究探討在心理治療中陷入負向經驗(自我中心觀點)以及與負向經驗保持距離 (觀察者觀點)之潛在效益與傷害。本研究為第一個致力於分析與比較在心理治療過程中從不同觀點的負向經驗反思 (陷入與保持距離),以及這些觀點與憂鬱症狀間的關係,以對比情緒取向治療(EFT)療效之探索性研究。方法:研究隨機選取自治療初期有輕微到中度憂鬱診斷,而最終有正向成效或負向成效的案例各三名。透過測量陷入與保持距離語言的工具來分析對於負向經驗採取的態度,並採取貝克憂鬱量表 II 來測量憂鬱症狀。結果:僅在正向成效案例中發現晤談中的顯著改變,此改變為陷入狀態的顯著減少與保持距離狀態的增加,且研究發現此進展的模 式與症狀減少相關。此外,治療初期負向成效組的保持距離狀態較正向成效組來得多。結論:情 緒取向治療從治療初期的較高陷入狀態到治療終期的較高保持距離狀態之累進且顯著進展或許對憂鬱症有幫助。
Palavras-chave:
Clinical or methodological significance of this article: This study highlights that the evolution pattern of the perspective adopted in emotion-focused therapy (immersed/distanced) is associated with the clinical condition of clients with depressive symptoms, suggesting that immersion and distancing have therapeutic potential that should be considered for treating depression.
Reflecting on a problematic experience is the key to making sense of the feelings it evokes (Pennebaker, Citation1997; Wilson & Gilbert, Citation2008). Immersion and distancing are two possible perspectives to such reflection. Immersion occurs when the person analyses the experience from a first-person (egocentric) perspective (McIsaac & Eich, Citation2004; Nigro & Neisser, Citation1983; Robinson & Swanson, Citation1993) whereas distancing involves analyzing the experience from a third person (observer’s) perspective (Nigro & Neisser, Citation1983; Robinson & Swanson, Citation1993). Experimental research suggests that immersion is a non-adaptive way of approaching negative experiences whereas distancing is more helpful (e.g., Ayduk & Kross, Citation2010a, Citation2010b). These results seem consistent with good psychotherapy outcomes, i.e., cases where the client becomes increasingly capable of distancing from problematic experiences. Nevertheless, some clinical and therapeutic models, such as the assimilation model and emotion-focused therapy (EFT) for depression, suggest that in psychotherapy there is a more complex, dynamic, and developmental relationship between distancing and immersion. Specifically, these two models admit that in the initial phases of therapeutic work, clients must be allowed to immerse themselves in their negative experiences, to pave the way for later distancing. In this study, we explore this more complex view, comparing the trajectories of immersion and distancing in six cases of EFT (poor-outcome n = 3; good-outcome n = 3).
Empirical Findings on Immersion and Distancing
During immersion people reflect on the experience from a first-person perspective (“I think …,” “I feel …”), i.e., according to their own point of view. The original thoughts, feelings, behaviors, and events repeat themselves (McIsaac & Eich, Citation2004; Nigro & Neisser, Citation1983; Robinson & Swanson, Citation1993) and verbal accounts of the experience are essentially concrete descriptions of its particularities (e.g., Kross, Ayduk, & Mischel, Citation2005; Kross, Gard, Deldin, Clifton, & Ayduk, Citation2012). The following quotation provides an example of a mother’s immersed perspective on a dispute with her child: “My son told me that I do not have time for him. I am a bad mother, it’s really painful.”
In contrast, a distanced perspective involves reflecting on the experience from an observer’s perspective (Nigro & Neisser, Citation1983; Robinson & Swanson, Citation1993), which promotes a broader and abstract view of feelings, thoughts, and behaviors, like a big picture about experience (Kross et al., Citation2012). Some authors consider that distancing amounts to the disidentification from one’s internal experiences, i.e., “the experience of internal states as separate from one’s self” (Bernstein et al., Citation2015, p. 6). Distanced verbal accounts focus less on the concrete details of the experience and more on explaining and exploring it, in way of insight or closure (e.g., Kross et al., Citation2005, Citation2012). A distanced perspective on the pain caused by the mother–child dispute above could take the following form: “The pain is because I know that I could do better if I spent less time at work. He was just asking for my attention, I know he loves me.”
There are several concepts related to and overlapping with distancing, such as decentering and metacognitive awareness. According to the metacognitive process model proposed by Bernstein et al. (Citation2015), distancing is one of the key processes in decentering. As a metacognitive ability to observe one’s own thoughts and feelings as temporary and objective events (Fresco et al., Citation2007; Safran & Segal, Citation1990), decentering involves a complex state of inter-related processes that can be described as follows: the awareness of subjective experience (metacognitive awareness, which can be deliberately promoted by mindfulness) initiates two related processes, namely the disidentification from internal experience and reduced-reactivity to thought content. Drawing on this model, one of the steps toward decentering and meta-awareness is self-distancing, which promotes the disidentification from internal experience. Self-distancing is reciprocally related to the reduction in reactivity to the content of the mind (which is related to cognitive defusion).
Studies on immersion and distancing have focused on experimental manipulation of self-observation. They indicate that people who assume an immersed perspective on negative experiences (i.e., personal experiences associated with painful emotional content) tend to describe a sequence of events, thoughts, feelings, or behaviors, that paints a simplistic picture of the experience and hinders broad, comprehensive analysis (Ayduk & Kross, Citation2010b; Kross et al., Citation2005, Citation2012; Kross & Ayduk, Citation2008, Citation2009). Furthermore, the focus on internal states may feed ruminative cycles. Rumination, in turn, exacerbates negative affect, which can become overwhelming (Nolen-Hoeksema, Citation1991; Nolen-Hoeksema, Wisco, & Lyubomirsky, Citation2008). Thus, immersion can give rise to rumination, which makes people feel worse and constrains the construction of new meanings (Ayduk & Kross, Citation2008, Citation2010a; Berman et al., Citation2011; Kross, Citation2009; Kross et al., Citation2005). The distress caused by immersion makes people physically and psychologically vulnerable. For example, immersion reduces the probability of cardiovascular recovery from stress episodes and reduces problem-solving ability (Ayduk & Kross, Citation2010b), as well as increases the probability of an angry or aggressive response to provocation (Mischkowski, Kross, & Bushman, Citation2012) and it is associated with psychopathological states (Brosschot, Gerin, & Thayer, Citation2006; Bushman, Citation2002; Nolen-Hoeksema et al., Citation2008). In particular, people with depression tend to analyze the experience from an immersed perspective (Kross et al., Citation2012; Kross & Ayduk, Citation2009; Kross, Davidson, Weber, & Ochsner, Citation2009), which enhances their emotional reactivity (Berman et al., Citation2011), particularly with respect to negative affect (Kross et al., Citation2012; Kross & Ayduk, Citation2008). All these findings suggest that immersion is a non-adaptive perspective on painful experiences, carrying health risks and hindering attempts to give meaning to those experiences (e.g., Ayduk & Kross, Citation2010b; Kross, Citation2009). In contrast, distancing is a different and more helpful way of reflecting on problematic experiences (e.g., Ayduk & Kross, Citation2010a, Citation2010b; Berman et al., Citation2011; Kross, Citation2009). Experimental studies have emphasized that distancing is an adaptive perspective in the reflection of painful experiences because it tends to involve more reconstruction and less recounting than immersion (Ayduk & Kross, Citation2010b; Kross & Ayduk, Citation2008, Citation2009). Distancing facilitates the attribution of new meanings and helps people to make sense of problematic experiences (Ayduk & Kross, Citation2008) and resolve problems (e.g., Ayduk & Kross, Citation2008, Citation2010b). Indeed, some therapeutic models are based on using a similar form of distanced self-reflection to create alternative narratives of an experience. For example, cognitive therapy encourages clients to assume an observer and distanced stance on their personal negative experiences and considers this an important technique for restructuring negative thoughts and promoting therapeutic change (e.g., Beck, Citation2011). Moreover, prioritizing reconstruction over recounting inhibits excessive increases in negative affect (Ayduk & Kross, Citation2008; Kross et al., Citation2012), i.e., promotes greater emotional control. Specifically, when a painful experience is analyzed from a distanced perspective, negative affect presents less reactivity (e.g., Ayduk & Kross, Citation2008, Citation2010b; Gruber, Harvey, & Johnson, Citation2009; Kross & Ayduk, Citation2009), duration (Kross & Ayduk, Citation2011; Verduyn, Mechelen, Kross, Chezzi, & Bever, Citation2012), and intensity (Ayduk & Kross, Citation2008; Kross et al., Citation2005; Kross & Ayduk, Citation2008) than when it is analyzed from an immersed perspective. All these results are consistent with the research on emotional regulation about the benefits of reappraisal strategies—which involve taking an observer’s perspective on a personal negative experience and reviewing one’s initial appraisal in order to create new and adaptive emotional meanings and responses (e.g., Gross, Citation2015; Gross & Thompson, Citation2007). Based on these findings, the experimental studies suggest that distancing may help to prevent rumination (Ayduk & Kross, Citation2008, Citation2010a; Berman et al., Citation2011; Kross, Citation2009; Kross et al., Citation2005). Particularly in depression, distancing is associated with lower levels of depressotypic thought accessibility (Kross et al., Citation2012), less depressive affect (Kross et al., Citation2012; Kross & Ayduk, Citation2008), and lower emotional reactivity (Kross & Ayduk, Citation2009) in comparison with immersion. All these empirical findings support the view that distancing, unlike immersion, is generally beneficial to physical and psychological health. Therefore, they suggest that immersion and distancing are opposite and independent perspectives.
The assimilation model of problematic experiences (negative experiences that were not assimilated into the self) offers a different and integrative understanding. According to this model, painful or even traumatic experiences tend to be automatically avoided if they evoke strong negative emotion (Stiles, Citation2011; Stiles et al., Citation1991), but this makes it difficult to achieve an adaptive integration of them. Thus, the assimilation model posits that clinical change is a sequential process that may involve both immersion and distancing at different points in the process (Caro Gabalda & Stiles, Citation2009; Stiles et al., Citation1991). Therapeutic change may involve progression from avoidance of the problem to deeper immersion in problematic contents, making them more available to subjective awareness, and only once the client has immersed in the experience will he or she be able to benefit from adopting a more distanced perspective in order to achieve a broader understanding and a greater mastery of the problem (Caro Gabalda & Stiles, Citation2009; Stiles, Citation2011; Stiles et al., Citation1991). Thus, the assimilation model suggests a developmental perspective on immersion and distancing. This interpretation is congruent with EFT for depression treatment.
Immersion and Distancing in EFT for Depression
The experiential therapies, such as EFT, promote immersion in the initial phase of treatment by encouraging contact with, and reflection on maladaptive emotional states that cause psychological distress, activating them so that they are re-experienced in the here-and-now (Elliott, Watson, Goldman, & Greenberg, Citation2004; Greenberg, Citation2002). This is in accordance with experimental studies regarding the potential of immersion for the activation of emotional content (e.g., Kross et al., Citation2012). However, EFT admits potential therapeutic benefits of immersion on the treatment of the depression. According to Pascual-Leone and Greenberg (Citation2007), EFT brings the individual closer to his or her personal experience (experience-near). The client needs to get in touch with his or her core maladaptive states in order to become aware of his or her internal states and then process and transform them. The guiding principle of EFT is that “the only way out is through” (Pascual-Leone & Greenberg, Citation2007, p. 875). Hence, clients are encouraged to reflect on painful emotions from a first-person perspective, in a welcoming and safe context (Elliott et al., Citation2004; Greenberg, Citation2002; Greenberg & Watson, Citation2006). All this emotional work relies on a safe and solid therapeutic alliance, based on empathy and the therapist’s presence. A secure therapeutic alliance promotes a collaborative focus on the client’s internal states and current sense of self (Greenberg & Watson, Citation2006; see Paivio, Citation2013). Exploratory empathic responses, which are typical from EFT, on a first phase, precisely envisage a deeper contact with painful underlying emotional experiences, which implies an immersed perspective. In summary, EFT encourages clients to adopt an immersed perspective as the first step toward emotional change and as a means of helping the client to process emotional states that were previously partially or totally avoided. This approach is also consistent with the assimilation model (e.g., Stiles, Citation2011).
In the later stages of the therapeutic process, treatment for depression involves specific therapeutic tasks that promote a different, more distanced perspective, allowing new meanings to emerge. In some of these therapeutic tasks (e.g., chair work) the client is invited to treat different parts of his or her self as different characters or “voices”, addressing them as a “you” or even using one’s own name. Recent research on immersion and distancing showed that referring to oneself by name enhanced distancing when talking about the self (Kross et al., Citation2014), which seems that also happens in chair work (Greenberg & Watson, Citation2006). Distinguishing between different parts of the self promotes a more differentiated view of one’s internal dynamics, feeding an observer perspective on the original problem and alternative ways of construing the experience. This more distanced perspective helps “clients and therapists define areas of inquiry that they can then pursue in the session to increase understanding of client functioning and to explore alternatives” (Greenberg & Watson, Citation2006, p. 213). These EFT assumptions are consistent with experimental studies on the benefits of distancing in the reconstruction of experience (Ayduk & Kross, Citation2010b; Kross & Ayduk, Citation2008, Citation2009), and with the assimilation model’s account of the association between distancing and more advanced stages of change (e.g., Stiles, Citation2011). EFT also provides techniques that promote emotional regulation through distancing (Elliott et al., Citation2004). For example, when clients feel overwhelmed by painful emotions, EFT therapists can use the “clearing a space” therapeutic task. The aim of the task is to help the client build a “working distance” between him or herself and the problematic issues. A working distance is defined as an observational perspective on a problematic object that involves an optimal and regulated state of emotional arousal. The role of distancing in promoting emotional regulation in EFT is consistent with experimental findings on the association between distancing and reduced duration of emotion (Kross & Ayduk, Citation2011; Verduyn et al., Citation2012). In fact, Carryer and Greenberg (Citation2010) have shown that emotional arousal is beneficial in experiential therapies when it is expressed in moderate amount. In other words, both marginal and overwhelming emotional arousal predict poorer outcomes to therapy. On the one hand, reduced amount of time expressing emotion may signal lack of involvement with emotional experience, like avoidance or intellectualization. On the other hand, spending too much time expressing emotion may be associated with emotional dysregulation, hindering emotional processing. These findings suggest that although immersion may play an important role in therapy by the contact with emotional experience, spending too much time immersed in one’s problematic experiences may be harmful, while distancing may be helpful to achieve a better reflection of the experience.
In short, there are several hypotheses to consider. First, it is legitimate to propose a development vision regarding immersion and distancing in therapy, namely in EFT for depression. We can hypothesize that the immersed perspective may be beneficial in the earlier phases of the therapeutic work, allowing the access to relevant emotional contents, while the distanced perspective may be more relevant in more advanced stages of therapy. Second, poor-outcomes to EFT for depression may be associated with an excessive focus on negative experiences from an immersed perspective. Excessive immersion may promote rumination, excessive emotional arousal, and emotional dysregulation, thus inhibiting the emotional control needed to reconstruct the experience in an adaptive way.
Purpose of the Study
Currently, there is a need for longitudinal research on immersion and distancing in clinical samples. This study sought to explore how and when immersion and distancing are associated with success in EFT for depression. To do this we compared how clients who had good- and poor-outcomes to EFT for depression reflected on their negative experiences during therapy. More specifically the aims were (a) to compare the frequency and evolution pattern of immersion and distancing in the two groups; (b) to analyze the relationship between changes in the frequency of immersion/distancing when reflecting on problematic experiences and changes in the scores of the depressive symptoms.
Method
Participants
Clients
Five women and one man aged between 23 and 48 years (M = 35.5, SD = 10.17) participated in the study. They were participating in a randomized clinical trial named “Decentering and change in psychotherapy—ISMAI Depression Study” (Salgado, Citation2014) comparing the effectiveness of cognitive behavioral therapy (CBT) and EFT as treatments for major depressive disorder. All participants in the clinical trial met the following inclusion criteria: diagnosis of major depressive disorder; not taking medication; Global Assessment of Functioning score higher than 50. The exclusion criteria were client currently receiving other treatment for depression; high risk of suicide; current or previous diagnosis of substance abuse; psychosis; bipolar disorder; eating disorder; panic disorder (DSM-IV Axis I disorders); and schizotypal, borderline, and antisocial disorder (DSM-IV Axis II disorders). These criteria were assessed by the Structural Clinical Interviews for the DSM-IV-TR I (First, Spitzer, Gibbon, & Williams, Citation2002) and II (First, Gibbon, Spitzer, Williams, & Benjamin, Citation1997), and the Beck Depression Inventory-II (BDI-II) for the Portuguese population (Coelho, Martins, & Barros, Citation2002). Clients who met the criteria for participation in the clinical trial received 16 weekly sessions of psychotherapy. Assignment to therapeutic modality (CBT or EFT) was random. All cases in the clinical trial were classified as having a good- or poor-outcome according to Jacobson and Truax’s (Citation1991) criteria. The good-outcome cases of the clinical trial showed reliable and clinically significant change in symptoms: at the end of therapy depressive symptoms were below the BDI-II cut-off score (13 points) and there was reliable change during therapy (see Jacobson, Roberts, Berns, & McGlinchey, Citation1999; Jacobson & Truax, Citation1991; McGlinchey, Atkins, & Jacobson, Citation2002), exceeding the Reliable Change Index of 7.75, calculated from the total sample of the clinical trial and taking into account the psychometric data for the Portuguese version of the BDI-II. Thus, all good-outcome cases of the clinical trial were recovered cases. The poor-outcome cases have not met at least one of the criteria mentioned above (depressive symptoms below the BDI-II cut-off score, and reliable change during therapy). Five EFT therapists participated in the clinical trial and there was no significant association between therapist and clinical outcome, χ2(5) = 2.80, p = .732.
For this study, we randomly selected three good-outcome and three poor-outcome cases from the pool of EFT cases in the clinical trial. As shown in , the good-outcome cases of this study met the two criteria for classification of good-outcome cases imposed by the clinical trial. In the poor-outcome cases, BDI-II scores in the last session were above the normal range (>13 points). One poor-outcome case was a “responder” (reliable change, but depressive symptoms in the last session did not change to the normative range). None of the poor-outcome cases showed evidence of deterioration (see ). The sociodemographic profiles of the good- and poor-outcome cases included in this study were similar with respect to gender, χ2(1) = 1.20, p = .273, age, U = 4.00, p = .827, civil status, χ2(2) = 1.33, p = .513, and education level, U = 3.00, p = .700.
Table I. Evolution of depressive symptoms in the six cases (BDI-II).
All clients gave their informed consent for using their data in scientific publications. According to ethics protocol of this clinical trial, as well as principles and standards of the American Psychological Association, clients received information about the purposes and procedures of the clinical trial and their personal information was de-identified to protect their anonymity.
Therapists
The good-outcome cases were treated by three therapists: two women and one man aged between 31 and 42 years (M = 35.5, SD = 4.97) with Ph.D. The duration of their experience as therapists ranged between 4 and 19 years (M = 11, SD = 6.16) and their experience with EFT ranged between 1 and 3 years (M = 2, SD = 0.82). The poor-outcome cases were treated by two male therapists aged between 31 and 44 years, one of them with Ph.D. and other with master’s degree. The duration of their experience as therapists ranged between 2 and 21 years (M = 14.33, SD = 8.73) and their experience with EFT ranged between 1 and 5 years (M = 3.33, SD = 1.70). The male therapist responsible for one of the good-outcome cases also treated two poor-outcome cases. All therapists received six months (80 hours) of training in the specific therapeutic protocol for the treatment of depression (see Elliott et al., Citation2004; Greenberg, Rice, & Elliott, Citation1993), as well as weekly supervision sessions during their intervention in cases pertaining to the clinical trial.
The protocol is based on working at the emotional level, seeking to influence cognitive and behavioral change. The goal in EFT is to promote emotional processing. The therapists help clients gain access to maladaptive emotional schemes, in order to transform them. Clients are then capable of understanding the differences between present and past experiences, and identifying their needs. In this process, new experience meanings will emerge, facilitating the adaptive resolution of the problematic experience (Elliott et al., Citation2004; Greenberg & Watson, Citation2006).
Process Measures
Measure of immersed and distanced speech
The measure of immersed and distanced speech (MIDS) allows for identifying the immersed and distanced perspectives concerning experience through client speech (immersed and distancing speech). This measure, based on theoretical definition and relevant prior research (e.g., Ayduk & Kross, Citation2010b; Kross et al., Citation2005, Citation2012; Kross & Ayduk, Citation2008, Citation2009; Nigro & Neisser, Citation1983; Robinson & Swanson, Citation1993), categorizes the client speech according to different statements (i.e., subcategories of immersed and distanced speech) which contents are representative of immersed or distanced perspective. The immersed and distanced perspectives are manifested in people’s speech respectively by the focus on the description of the experience or on the explanation/exploration of it. The immersed subcategories aim to identify the first-person perspective about experience, namely “what happened/ what did I think” (what statements), and “how did I feel” (attributive statements). They include client’s speech focused on the description of events, original thoughts, feelings, and behaviors as experienced by the client. The distanced subcategories aim to identify the observer perspective about experience. They include client speech focused on explaining and exploring different facets of the experience (insight statements) or a broader view, based on past and current experiences (closure statements). According to MIDS, the client’s speech that reveals closeness to the first-person experience (or an egocentric point of view) is categorized as immersed, while speech elaborating a broader picture about experience (or an observer point of view) is defined as distanced. This categorization is independent of the potential adaptive potential of that reflection. For example, when a client assesses a negative experience from a broader perspective, associating past and current experiences, or making conclusions about his/her feelings, that speech is classified as distanced (closure statements), even if the assessment and conclusions expressed by the client are not clinically productive or somehow biased. When none of immersed or distanced subcategories are identified, they are considered as other statements (see for more details).
Table II. Brief description of immersion and distancing subcategories.
Preliminary results of a study assessing the validity of MIDS (Barbosa, Silva, Castro, Pinto-Gouveia, & Salgado, Citation2017) indicate a high internal consistency for both immersion (α = .95) and distancing (α = .91) and good to strong inter-rater reliability (Hill & Lambert, Citation2004) for raters’ pairs (Cohen’s kappa ranged from .75 to .96).
Outcome Measures
BDI-II
This study used the BDI-II adapted for a Portuguese population by Coelho and collaborators (Citation2002), from Beck, Steer, and Brown (Citation1996). The BDI-II is a 21-item self-report inventory designed to measure the degree of depression. Responses on each item are scored on a scale ranging from 0 to 3. The total scores can range from 0 to 63. Specifically, scores below 13 are considered to be in the normal range, whereas scores between 14 and 19 indicate mild to moderate levels of depression, scores between 20 and 28 indicate moderate to severe depression, and a total of 29 or more indicates a severe level of depression. The internal consistency (Cronbach’s alpha) of the total BDI-II score was .89 (Coelho et al., Citation2002). The psychometrics qualities found in the Portuguese version of this measure were consistent with the ones found in the American version (Coelho et al., Citation2002).
Procedures
The six cases (three good-outcomes; three poor-outcomes) were randomly chosen from the EFT group in the larger clinical trial. We analyzed five sessions of therapy for each case (sessions 1, 4, 8, 12, and 16) in order to explore changes in immersion and distancing across therapy. These sessions were chosen because they belong to different phases of the therapeutic process (see Basto, Stiles, Rijo, & Salgado, Citationin press; Hill, Citation2009), allowing to obtain an overview about the evolution of the variable under study; and because they were the sessions in which the clinical trial protocol specified that clients should complete the BDI-II, thus allowing us to explore the association between this quantitative measure of depressive symptoms and qualitative measures. The sessions were transcribed according to the procedure described by Mergenthaler and Stinson (Citation1992) and then subjected to a two-step analysis. In the first step, for each case, the client’s main problematic experience was identified. Although this procedure is not necessary for the determination of the type of perspective used by the client in therapy, it has been applied in this study in order to ensure that immersion and distancing were only analyzed with respect to negative emotional content. In the second step, this experience was coded in terms of immersed and distanced speech. Symptoms were also assessed in the same sessions from the outcome measure (BDI-II), aiming to analyze the relationship between depressive symptoms and immersion/distancing during reflection on the main negative experience.
Identification of the main problematic experience
We followed the procedures adopted in previous studies regarding the identification and definition of relevant problematic experiences in psychotherapy (e.g., Brinegar, Salvi, Stiles, & Greenberg, Citation2006; Caro Gabalda & Stiles, Citation2013; Honos-Webb, Stiles, & Greenberg, Citation2003; Stiles, Meshot, Anderson, & Sloan, Citation1992). This task was conducted by a total of eight judges, one judge had a Ph.D. in clinical psychology, one was a Ph.D. student in clinical psychology and six were Master’s students in clinical and health psychology. In preparation, the judges read and discussed relevant prior studies about problematic experiences, as well as clinical sessions in which the procedures for identifying problematic experiences were applied. This training phase lasted two months and was guided by a researcher who was expert in this type of procedure. Each case was assessed by a team of two judges who carefully and independently read the five sessions, then jointly constructed a clinical formulation, identifying, by consensus, the problematic experiences (central clinical problems). Then the judges worked together to identify excerpts in the transcripts where each problematic experience appeared that were then marked with different colors. Specifically, the excerpts of the problematic experiences were identified from content (what was talked about) (Brinegar et al., Citation2006; Caro Gabalda & Stiles, Citation2013). Finally, the main problematic experience was identified through a consensual discussion between the two judges about the clinical relevance of the content. In all cases, the problematic experience selected in each session occupied more than 70% of the client’s speech (ranging from 72% to 86%).
Analysis of problematic experience in terms of immersion and distancing
The problematic experiences in all cases were analyzed in terms of immersion and distancing using the MIDS. The MIDS was applied by a Ph.D. student in clinical psychology, who was experienced in use of the measure, and three Master’s students in clinical and health psychology. There were two phases to application of the MIDS: the training phases and the identification phase in which judges identified the type of speech present in excerpts dealing with the previously identified problematic experiences. In the training phase, the judges received intensive training in identifying immersed and distanced speech. This involved reading relevant articles and manuals and practicing the coding procedures on material from therapy sessions until they achieved an acceptable Cohen’s kappa (Cohen’s kappa ≥ .75) (Hill & Lambert, Citation2004). This phase lasted about three months. In the second phase, each Master’s student randomly coded two cases with the Ph.D. student. The Ph.D. student was aware of the clinical outcome of the cases analyzed but the other judges were blind to this condition. The five sessions of each case were rated independently by the two judges. Representative excerpts dealing with problematic experience were analyzed to determine the presence of the various subcategories of immersion (what statements and attributive statements) and distancing (insight statements and closure statements). If none of the subcategories were present, the statement was classified as other. The rating process involved defining, within the parts of the transcript involving a problematic experience, the beginning and the end of stretches of speech belonging to a subcategory. The beginning of the stretch was delimited by the presence of contents that characterize that subcategory. In turn, the end of the stretch was delimited by the absence of those contents and/or the presence of contents that characterize another subcategory, or by the end of excerpt analyzed (see ). When the classification of the judges did not coincide, this was considered a disagreement, which was later solved by consensual discussion between them (see Hill et al., Citation2005). Cohen’s kappa for judge pairs ranged from .75 to .83. When aggregated the subcategories of immersion and subcategories of distancing, Cohen’s kappa ranged from .78 to .86. These results indicate strong inter-rater reliability (Cohen’s kappa > .75; Hill & Lambert, Citation2004). The main output variable was the relative frequency of each type of speech (immersed or distanced), which was calculated taking into account the number of words occupied by each type of speech and the total number of words per session. Specifically, for each session, the stretches identified with subcategories of immersed speech were grouped, as well as, the stretches identified with subcategories of distanced speech. After that, the number of words for each group (immersed speech and distanced speech) was counted. In calculating the total number of words per session we ignored the number of words coded “other”, as they represented very small passages of the session (M = 2.8% per session) in which the judges were not able to identify the type of underlying speech. The Mann–Whitney U test was used to analyze the differences between the good- and poor-outcome groups regarding the presence of immersion and distancing in therapy. The Friedman test was used to analyze within-group changes during therapy.
We also selected representative excerpts of immersed and distanced speech from one good-outcome case (Elizabeth) and one poor-outcome case (Peter) to illustrate the quantitative results. The client names are fictitious.
Outcome assessment
In all cases clients completed the BDI-II at sessions 1, 4, 8, 12, and 16. In this study, the results of BDI-II in these sessions were used to obtain a general description of the depressive symptoms in the good- and poor-outcome groups across sessions ( and ). In order to analyze the relationship between changes in the immersion/distancing and changes in the depressive symptoms, we used the results of BDI-II at the first and last session (sessions 1 and 16, respectively). We calculated the changes in BDI-II scores and in the relative frequencies of immersed/distanced speech between these sessions. Spearman’s rho correlations were used to assess the relationships between depressive symptoms and immersion/distancing.
Figure 1. Evolution of immersed and distanced speech and clinical symptoms in the good-outcome group.
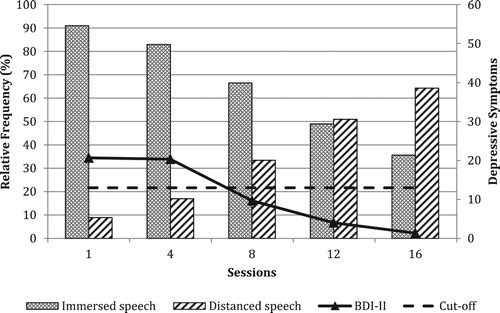
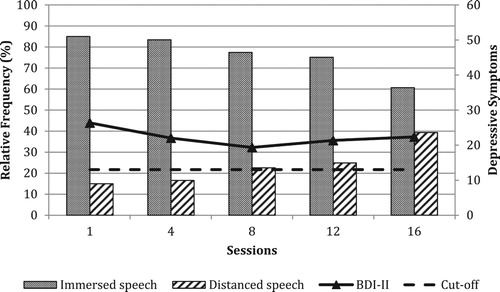
Figure 2. Evolution of immersed and distanced speech and clinical symptoms in the poor-outcome group.
Should be noted that in this study, we reported only the results found concerning to the distanced speech due to the dependence of the data on the relative frequencies of immersed and distanced speech, ensuring adequate statistical evidence. Actually, since the category “Other” was residual, the values of immersion and distancing are almost symmetrical, and clearly dependent (see and ). Thus, the results we will report about distanced speech are symmetrical to the ones regarding immersed speech. There was only one exception to this decision in our report of results: we reported the frequencies of both distancing and immersion in and in order to make it clear the dependency of these two categories.
Results
Occurrence of Distancing in Good- and Poor-Outcome Groups
At the beginning of therapy, the good- and poor-outcome groups had similar levels of depressive symptoms as measured by the BDI-II, U = 2.00, z = −1.09, p = .275.
The good- and poor-outcome groups presented significant differences on overall relative frequency of distanced speech during the therapeutic process, U = 0.00, z = −1.96, p = .050, r = −.80. The relative frequency of distanced speech was higher in the good-outcome group (M = 35.13; SD = 5.88, 95% CI [20.52, 49.75]) than in the poor-outcome group (M = 22.43; SD = 5.06, 95% CI [9.85, 35.00]). Regarding the relative frequency of distanced speech produced in each session (see ), in good-outcome group it ranged from 6.65% to 80.63%, whereas in poor-outcome group it ranged from 8.57% to 52.28%. The distanced speech was the speech less used across sessions in the poor-outcome cases, except in one session of the case 5, in which the distanced speech was dominant in the last session (relative frequency of distanced speech was 52.27%). In the good-outcome cases, there was a dominance reversal in the speech used in the last session of all cases and session 12 in one of the cases (case 2), in which the distanced speech became the more frequent speech (ranging from 50.85% to 80.63%).
Table III. Evolution of distanced speech in the six cases.
Evolution of Distancing in Good- and Poor-outcome Groups
In the first session of the therapy, all poor-outcome cases showed higher relative frequency of distanced speech (ranging from 11.38% to 19.36%) than the good-outcome cases (ranging from 7.21% to 11.12%). Comparing the first and last sessions of each case, both poor- and good-outcome cases showed higher relative frequency of the distanced speech in the last session (see and and ).
Overall, in both good- and poor- outcome groups, the distanced speech increased throughout the therapy. Although this evolution has been common to all cases, the good-outcome cases showed a more pronounced evolution than the poor-outcome cases (see and and ). For example, one good-outcome case (case 1) and one poor-outcome case (case 4) started therapy with very similar relative frequencies of distanced speech (11.12% and 11.38%, respectively), however, when comparing the evolution of the speech in the two cases, the distanced speech in the good- outcome case had a more accentuated, steeper increase of distanced speech across sessions, reaching a higher relative frequency of the distanced speech in the last session than the poor-outcome case (61.52% and 46.43%, respectively; see ). Friedman’s test was used to evaluate the differences between groups in distanced speech across sessions. In the good-outcome group, the distanced speech showed significant changes: the relative frequency of distanced speech increased during the course of therapy, χ²(4) = 10.93, p = .027. shows that this trend was most pronounced between session 8 and the end of therapy, with distanced speech being the more frequent speech, especially in the last session (ranging from 50.85% to 80.63%; see ). Conversely, in the poor-outcome group there was no significant differences in the relative frequencies of distanced speech across sessions, χ²(4) = 6.67, p = .155. shows that distanced speech remained considerably low throughout the therapy in all cases. The increase of distanced speech in the poor-outcome group was less pronounced than in the good-outcome group and more evident in last session (ranging from 19.29% to 52.27%; see ).
The following passages are taken from the initial, middle, and final phases of therapy in a good-outcome case and a poor-outcome case. The text coded as immersion is shown in italics and text coded as distancing is underlined. First, we present passages from the good-outcome case (Elizabeth) which deal with the problematic experience of feeling worthless as mother and as woman. In the first passage (session 1, initial phase) Elizabeth adopted an immersed speech, focusing on the specific events associated with her divorce and expressing her feelings, her inner experience, and her thoughts and perceptions.
It did not have to be like this—just as I think that my parents did not have to do that to us [she is referring to her childhood experience of family violence], my children did not have to go through their parents’ separation either (…) He [her ex-husband] was extremely selfish, the money could not be lacking for his things, even if that means their children would starve and I: did not tolerate this type of things and … when my children were sick, he left home and said to me “look if you need anything you have the telephone here” … I feel there was a great injustice (…) but in relation to my children of course I disappoint them, of course [referring to her divorce] I destroyed everything they wanted for themselves.
In the next passage (session 8, middle phase) Elizabeth’s speech was characterized by more frequent, more coordinated transitions between immersion and distancing. In her immersed speech, she described her private experiences and thoughts about the impact of divorce on her children. In her distanced speech, she established connections between the experiences and thoughts, creating new meanings.
I feel I destroyed the dreams of my children to have a house (…); but recovering some situations, maybe now they feel the house like a real home . Before, my children were always willing to leave the house (…) they could have the same motivation as me, because I was also willing to leave the house too, right? (…) Now they really feel well!
The last passage of the good-outcome case (session 16, final phase) is dominated by distanced speech, which was more frequent than in the previous phases. Elizabeth explored the differences between how she was in the past and how she is now, providing an overview of the changes and how they occurred. She explored how her perceptions of her childhood experiences and their overall impact had changed.
Let’s say I was illiterate, now I know how to read—I am exactly the same person but with completely different attitudes and: initially, everything was very confusing, there were those two voices in my head, if one of them said “yes”, another said “no”. I think that maybe it was what made me stress a lot, because I was having a conflict with myself, right? (…) after all, I had many good times and I wasn’t remembering them. I needed to feel that I was there too, I was also a child (…) life goes on and it depends on me now.
The next passages were taken from a poor-outcome case (Peter) in which the problematic experience was feeling a failure. The first passage illustrates the predominance of immersed speech. Peter focused on his internal state, activating painful emotions in relation to himself passively and repeatedly. Distanced speech occurred when the client represented his experience in metaphorical terms.
(…) I do not like my personality I feel huge shame about how I am. I also do not like my way of thinking (…)
Therapist: But when you say that you feel ashamed, you feel ashamed because you are not able to make progress with work for your thesis?
I am ashamed by the development my life has taken (…)
(…) it’s like a cone turned upside down, a cone-shaped building turned upside down … a bench full of people looking at me and throwing something at me.
Even after a few sessions (session 8, middle phase), Peter continued to consider himself a failure and to focus on his fears. Unlike in the good-outcome case, his speech continued to deal repetitively with the internal states associated with the problematic experience.
I’m afraid of the novelty, I’m afraid of making a wrong decision, I’m afraid I’m disappointing people, I’m afraid of many things
That’s a lot of fears
yes (hmm hmm) basically I’m quiet even when I’m right
In the last passage (session 16, final phase) Peter uses more distanced speech than in the other phases, taking a broader perspective and analyzing his potential, but most of his distanced speech consists of a metaphorical description of his painful experiences. In other words, Peter’s use of distanced speech was largely restricted to metaphorical descriptions of his problematic experience and he quickly returned to an immersive perspective:
I think I’m better because I’m more aware of things that happen and I can analyze them in a way, I’m better at analyzing them (…) but there are things that I could not make progress with, because of me (…) I get a bit frustrated, sometimes I feel a bit useless, and this ends up affecting my self-esteem a bit and that’s already not high (…) I feel humiliated, it’s like being in the middle of a million people and someone kicks a ball and the ball hits me in the face, that’s the feeling that annoys me.
Distancing and Depressive Symptoms
and provide an overview of the evolution of depressive symptoms in good- and poor-outcome groups, respectively. shows that in the good-outcome cases, the depressive symptoms had a clear decrease throughout sessions. In turn, shows that in poor-outcome cases depressive symptoms were steady throughout sessions. In more detail, in the good-outcome cases, two cases presented no significant clinical depressive symptoms from session 8 onwards (cases 2 and 3, with BDI-II scores of 0 and 11, respectively) and one case from session 12 onwards (case 1, with BDI-II score of 8; see ). It is important to underline that in these sessions the BDI-II scores were below the clinical threshold and distanced speech was still the less frequent speech (relative frequency of distanced speech ranged from 29.02% to 47.23%; see and and ). In the poor-outcome group, all cases remained symptomatic across sessions (BDI-II scores ranged from 16 to 32; see and ).
Statistical analysis showed that there were strong correlation (rs > ±.70, p < .05; Cronk, Citation2006) between change in depressive symptoms (the difference between BDI-II scores at the session 1 and at the session 16) and change in relative frequency of the type of speech. Specifically, the change in depressive symptoms over the entire course of therapy was negatively correlated with change in distanced speech, rs = −.81, p = .05.
Discussion
This study suggests that at the beginning of therapy high immersion was common to both good- and poor-outcome cases, providing corroboration for the notion that depression is associated with an immersed perspective (Kross et al., Citation2012: Kross & Ayduk, Citation2009). However, the good- and poor-outcome groups differed in terms of the frequency of immersion/distancing and the course of changes in their relative frequency during therapy. The differences between groups were consistent with several aspects of our initial hypotheses. First, the good-outcome group spent a higher proportion of therapy in distancing than the poor-outcome group (and correspondingly adopted an immersed perspective for a lower proportion of the time). This difference was linked to significant changes in immersion/distancing during the course of effective EFT. In the good-outcome cases distancing increased (and correspondingly immersion decreased) during the course of therapy, whereas it remained stable in poor-outcome cases. Additionally, unlike in the poor-outcome group, in the good-outcome group distancing predominated at the end of therapy. These results suggest some support to the hypothesis about the association between the poor outcomes to EFT for depression and the excessive and continuous focus on negative experiences from an immersed perspective.
Second, the differences between groups in the evolution of immersion/distancing were not related to the intensity of symptoms at the start of therapy as there was no group difference in BDI-II scores at the beginning of therapy. The change in perspective over the course of therapy was, however, related to change in depressive symptoms, which is also aligned with the hypothesis that a progressive increase in distancing would be associated with therapeutic success. This is consistent with theory concerning the relationships between distancing and symptom relief (Ayduk & Kross, Citation2008, Citation2010b; Kross et al., Citation2005, Citation2012; Kross & Ayduk, Citation2008; Verduyn et al., Citation2012) and problem solving (Ayduk & Kross, Citation2010b; Stiles, Citation2011). Our result may be interpreted in two opposing ways. It is possible that, in this sample, change in the severity of depressive symptoms prompted changes in the perspective adopted during reflection on negative experiences. Alternatively, changes in perspective may have promoted change in the severity of depressive symptoms. Of course, we also need to acknowledge the possibility of a third variable causing both changes in depression and in the reflective perspective.
Third, unlike what might have been expected given the results of previous experimental studies (e.g., Ayduk & Kross, Citation2010b; Kross et al., Citation2012), distancing was more frequent in the poor-outcome cases than the good-outcome cases in the first session, suggesting that more frequent distancing early in therapy is not necessarily a predictor of good therapeutic outcome. This result also suggests that in this sample, it is the progressive transition from immersion to distancing that distinguishes between cases with good- and poor-outcomes, rather than the frequency of immersion/distancing at a given moment. Moreover, the high levels of immersion early in therapy possibly had a positive impact, promoting adaptive reflection on the problematic experience. This is in accordance with our hypothesis that immersion may initially have positive therapeutic effects, but needs to be followed by an increase of the distanced perspective about experience. Another interesting aspect of our results was that the good-outcome cases had subclinical levels of depression even when immersion was high. This suggests that reflecting on problematic experience from an immersed perspective may be an important part of the therapeutic process. In other words, while our results show an association between the increasing of the distanced perspective and decreasing of depressive symptoms, they do not show to be beneficial avoiding the immersed perspective in therapy. Actually, this suggests that, at least in this sample, immersion may have been an important element of the process—and actually an opportunity to promote clinical change and distancing. However, our results also showed that immersion does not always result in such opportunities being taken, since in the poor-outcome cases immersion remained relatively stable and high throughout therapy. It seems likely that continuous immersion results in persistent activation of clinical symptoms; this interpretation is consistent with experimental findings on how immersion affects the duration (Kross & Ayduk, Citation2011; Verduyn et al., Citation2012) and intensity of symptoms (Ayduk & Kross, Citation2008; Kross et al., Citation2005; Kross & Ayduk, Citation2008). If further confirmed with new studies and larger samples this gives rise to the hypothesis that immersion may be helpful when it is regulated, i.e., not continuous or indefinite. On the one hand, reflection on problematic experience from a regulated immersed perspective may promote increased awareness and acceptance of it and hence the adoption of a new perspective (distanced perspective), which in turn allows for the creation of new meanings. This suggestion is consistent with studies showing that egocentric contact with painful experience allows one to access, tolerate, and accept it and thus facilitates evaluation of its meaning (see Kennedy-Moore & Watson, Citation2001). On the other hand, it is also possible that a progressive increase of distancing facilitates emotional regulation and hence avoidance of uncontrolled, persistent immersion. This suggestion is consistent with experimental studies and EFT regarding the benefits of distancing in emotional control (Ayduk & Kross, Citation2008; Elliott et al., Citation2004; Kross et al., Citation2012). All this reflection need to be tasted.
There are other issues that are not yet clear. Immersion and distancing co-occurred in all therapeutic processes, with immersion the dominant perspective overall. There are several possible interpretations of this finding and they are not mutually exclusive. One is that EFT makes use of immersion; its focus on feeling and processing painful emotions may necessarily involve immersion in difficult experiences (Elliott et al., Citation2004; Greenberg, Citation2002; Greenberg & Watson, Citation2006). A second interpretation assumes that immersion is the perspective most commonly taken by clients in psychotherapy. Revealing the difficult and painful experiences for which one is seeking help may be a necessary preliminary step in the therapeutic process. Lastly, some therapeutic tasks, such as chair work, may imply the two perspectives. In this task, for example, the client may start by contact with inner feelings from an immersed perspective, but in later phases, a distanced perspective may dominate in order to feed new meaning-making.
Conclusion, Limitations and Future Studies
When analyzing the good-outcome cases, we found a trend that suggests a progressive transition from immersion, which dominates the initial phase, to distancing, which is used more frequently in the final phase. At the same time, immersion still accounts for a large part of the therapeutic conversation even in later phases of the process, and even when symptoms are already within the normative range. Finally, the poor-outcome cases and good-outcome cases showed an equivalent level of distancing at the beginning of the process. Based on these observations, we are putting forward a hypothesis that immersion and distancing play complementary roles in clinical change.
This study had some limitations that restrict the conclusions that can be drawn. They should be addressed in future studies. First, we analyzed immersion and distancing in a small sample of clients who were all suffering from depression and all went through the same kind of therapy. The very small sample did not permit more formal analyses of trajectories of change that account for dependency in data. It would be interesting to attempt to replicate our findings with a larger sample and to investigate whether they generalize to other therapies and other disorders. Second, one of the judges involved in qualitative analysis of the data was aware of the clinical outcomes, and with knowledge on the previous experimental studies on distancing and immersion. This may have worked as a potential confound. Nevertheless, we limited this potential effect in two ways: by always having a second judge blind to the results; and by always having the two judges coding 100% of the material. The Cohen’s kappa values also reveal a satisfactory agreement, which gives credit to the coding process. Third, only passages referring to problematic experiences of five sessions of therapy were analyzed in each case and so our findings need to be interpreted with caution. However, measures were taken to minimize bias in the data generated: coding was carried out by pairs of judges; a large number of judges was used; the six cases were randomly chosen; the sessions analyzed were taken from different phases of therapy in order to reflect as closely as possible any changes occurring during the therapeutic process; the excerpts analyzed dealt with the problematic experience in order to ensure that analysis of immersion and distancing was limited to negative emotional content.
Finally, our results create a hypothesis that deserves further study, namely, that regulated use of immersion and distancing has therapeutic benefits. For clinical and theoretical reasons, it is important to test this hypothesis and to investigate the processes involved in regulation of immersion. A moment-by-moment detailed analysis of immersion and distancing might provide insight about the potentialities of the dynamic between them for clinical change. These types of studies may lead to improvements in therapy by enabling therapists to promote the use of the most appropriate perspective at each stage in therapy.
ORCID
EUNICE BARBOSA http://orcid.org/0000-0002-8790-3581
JOÃO SALGADO http://orcid.org/0000-0003-0822-9267
Additional information
Funding
References
- Ayduk, Ö, & Kross, E. (2008). Enhancing the pace of recovery, self-distanced analysis of negative experiences reduces blood pressure reactivity. Psychological Science, 19, 229–231. doi: 10.1111/j.1467-9280.2008.02073.x
- Ayduk, Ö., & Kross, E. (2010a). Analyzing negative experiences without ruminating: The role of self-distancing in enabling adaptive self-reflection. Social and Personality Psychology Compass, 4, 841–854. doi: 10.1111/j.1751-9004.2010.00301.x
- Ayduk, Ö., & Kross, E. (2010b). From a distance: Implications of spontaneous self-distancing for adaptive self-reflection. Journal of Personality and Social Psychology, 98, 809–829. doi: 10.1037/a0019205
- Barbosa, E., Silva, S., Castro, D., Pinto-Gouveia, J., & Salgado, J. (2017). Development and validation of the measure of immersed and distanced speech. Manuscript in preparation.
- Basto, I., Stiles, W. B., Rijo, D., & Salgado, J. (in press). Does assimilation of problematic experiences predict a decrease in symptom intensity? Clinical Psychology & Psychotherapy. doi: 10.1002/cpp.2130
- Beck, A. T., Steer, R. A., & Brown, G. K. (1996). Manual for the Beck Depression Inventory-II (BDI-II). San Antonio, TX: Psychological Corporation.
- Beck, J. S. (2011). Cognitive behavior therapy: Basic and beyond (2nd ed.). New York, NY: The Guilford Press.
- Berman, M. G., Peltier, S., Nee, D. E., Kross, E., Deldin, P. J., & Jonides, J. (2011). Depression, rumination and the default network. Social Cognitive and Affective Neuroscience, 6, 548–555. doi: 10.1093/scan/nsq080
- Bernstein, A., Hadash, Y., Lichtash, Y., Tanay, G., Shepherd, K., & Fresco, D. (2015). Decentering and related constructs: A critical review and meta-cognitive processes model. Perspectives on Psychological Science, 10(5), 599–617. doi: 10.1177/1745691615594577
- Brinegar, M. G., Salvi, L. M., Stiles, W. B., & Greenberg, L. S. (2006). Building a meaning bridge: Therapeutic progress from problem formulation to understanding. Journal of Counseling Psychology, 53, 165–180. doi: 10.1037/0022-0167.53.2.165
- Brosschot, J. F., Gerin, W., & Thayer, J. F. (2006). The perseverative cognition hypothesis: A review of worry, prolonged stress-related physiological activation, and health. Journal of Psychosomatic Research, 60, 113–124. doi: 10.1016/j.jpsychores.2005.06.074
- Bushman, B. J. (2002). Does venting anger feed or extinguish the flame? Catharsis, rumination, distraction, anger, and aggressive responding. Personality and Social Psychology Bulletin, 28, 724–731. doi: 10.1177/0146167202289002
- Caro Gabalda, I., & Stiles, W. (2009). Retrocessos sno contexto da terapia linguística de avaliação [Setbacks in the context of linguistic therapy of evaluation]. Análise Psicológica, 27, 199–212. doi: 10.14417/ap.205
- Caro Gabalda, I., & Stiles, W. B. (2013). Irregular assimilation progress: Reasons for setbacks in the context of linguistic therapy of evaluation. Psychotherapy Research, 23, 35–53. doi: 10.1080/10503307.2012.721938
- Carryer, J., & Greenberg, L. (2010). Optimal levels of emotional arousal in experiential therapy of depression. Journal of Consulting and Clinical Psychology, 78(2), 190–199. doi: 10.1037/a0018401
- Coelho, R., Martins, A., & Barros, H. (2002). Clinical profiles relating gender and depressive symptoms among adolescents ascertained by the Beck Depression Inventory-II. European Psychiatry, 17, 222–226. doi: 10.1016/S0924-9338(02)00663-6
- Cronk, B. C. (2006). How to use SPSS: A step-by-step guide to analysis and interpretation (4th ed.). Glendale, CA: Pyrczak.
- Elliott, R., Watson, J., Goldman, R., & Greenberg, L. S. (2004). Learning emotion focused therapy: The process-experiential approach to change. Washington, DC: America Psychology Association.
- First, M. B., Gibbon, M., Spitzer, R. L., Williams, J. B. W., & Benjamin L. S. (1997). Structured clinical interview for DSM-IV Axis II personality disorders (SCID-II). (J. Pinto-Gouveia, A. Matos, D. Rijo, P. Castilho, & M. Salvador, Trans.). Washington, DC: American Psychiatric Press.
- First, M. B., Spitzer, R. L, Gibbon, M., & Williams, J. B.W. (2002). Structured clinical interview for DSM-IV-TR Axis I disorders, research version (SCID-I-RV). (A. Costa Maia, Trans.). New York, NY: Biometrics Research.
- Fresco, D., Moore, M., Van Dulmen, M., Segal, Z., Ma, S., Teasdale, J., & Williams, J. M. (2007). Initial psychometric properties of the experiences questionnaire: Validation of a self-report measure of decentering. Behavior Therapy, 38(3), 234–246. doi: 10.1016/j.beth.2006.08.003
- Greenberg, L. S. (2002). Emotion-focused therapy: Coaching clients to work through their feelings. Washington, DC: America Psychology Association.
- Greenberg, L. S., Rice, L. N., & Elliott, R. K. (1993). Facilitating emotional change: The moment-by moment process. New York, NY: Guilford Press.
- Greenberg, L. S., & Watson, J. (2006). Emotion-focused therapy for depression. Washington, DC: American Psychological Association.
- Gross, J. J. (2015). Emotion regulation: Current status and future prospects. Psychological Inquiry, 26(1), 1–26. doi: 10.1080/1047840X.2014.940781
- Gross, J. J., & Thompson, R. A. (2007). Emotion regulation: Conceptual foundations. In J. J. Gross (Ed.), Handbook of emotion regulation (pp. 3–24). New York: Guilford Press.
- Gruber, J., Harvey, A., & Johnson, S. (2009). Reflective and ruminative processing of positive emotional memories in bipolar disorder and healthy controls. Behaviour Research and Therapy, 47, 697–704. doi: 10.1016/j.brat.2009.05.005
- Hill, C. E. (2009). Helping skills: Facilitating exploration, insight, and action (3rd ed.). Washington, DC: American Psychological Association.
- Hill, C. E., Knox, S., Thompson, B. J., Williams, E. N., Hess, S. A., & Ladany, N. (2005). Consensual qualitative research: An update. Journal of Counseling Psychology, 52, 196–205. doi: 10.1037/0022-0167.52.2.196
- Hill, C. E., & Lambert, M. J. (2004). Methodological issues in studying psychotherapy processes and outcomes. In M. J. Lambert (Ed.), Bergin and Garfield’s handbook of psychotherapy and behavior change (5th ed., pp. 84–136). Hoboken, NJ: Wiley.
- Honos-Webb, L., Stiles, W. B., & Greenberg, L. S. (2003). A method of rating assimilation in psychotherapy based on markers of change. Journal of Counseling Psychology, 50, 189–198. doi: 10.1037/0022-0167.50.2.189
- Jacobson, N. S., Roberts, L. J., Berns, S. B., & McGlinchey, J. B. (1999). Methods for defining and determining the clinical significance of treatment effects: Description, application, and alternatives. Journal of Consulting and Clinical Psychology, 67, 300–307. doi: 10.1037/0022-006X.67.3.300
- Jacobson, N. S., & Truax, P. (1991). Clinical significance: A statistical approach to defining meaningful change in psychotherapy research. Journal of Consulting and Clinical Psychology, 59, 12–19. doi: 10.1037/0022-006X.59.1.12
- Kennedy-Moore, E., & Watson, J. (2001). How and when does emotional expression help? Review of General Psychology, 5, 187–212. doi: 10.1037/1089-2680.5.3.187
- Kross, E. (2009). When the self becomes other: Toward an integrative understanding of the processes distinguishing adaptive self-reflection from rumination. Annals of the New York Academy of Sciences, 1167, 35–40. doi: 10.1111/j.1749-6632.2009.04545.x
- Kross, E., & Ayduk, Ö. (2008). Facilitating adaptive emotional analysis: Distinguishing distanced-analysis of depressive experiences from immerseds-analysis and distraction. Personality and Social Psychology Bulletin, 34, 924–938. doi: 10.1177/0146167208315938
- Kross, E., & Ayduk, Ö. (2009). Boundary conditions and buffering effects: Does depressive symptomology moderate the effectiveness of selfdistancing for facilitating adaptive emotional analysis? Journal of Research in Personality, 43, 923–927. doi: 10.1016/j.jrp.2009.04.004
- Kross, E., & Ayduk, Ö. (2011). Making meaning out of negative experiences by self-distancing. Current Directions in Psychological Science, 20, 187–191. doi: 10.1177/0963721411408883
- Kross, E., Ayduk, Ö, & Mischel, W. (2005). When asking “why’ does not hurt: Distinguishing rumination from reflective processing of negative emotions. American Psychological Society, 16, 709–715. doi: 10.1177/0963721411408883
- Kross, E., Bruehlman-Senecal, E., Park, J., Burson, A., Dougherty, A., Shablack, H., … Ayduk, O. (2014). Self-talk as a regulatory mechanism: How you do it matters. Journal of Personality and Social Psychology, 106, 304–324. doi: 10.1037/a0035173
- Kross, E., Davidson, M., Weber, J., & Ochsner, K. (2009). Coping with emotions past: The neural bases of regulating affect associated with negative autobiographical memories. Biological Psychiatry, 65, 361–366. doi: 10.1016/j.biopsych.2008.10.019
- Kross, E., Gard, D., Deldin, P., Clifton, J., & Ayduk, Ö. (2012). “Asking why” from a distance: Its cognitive and emotional consequences for people with major depressive disorder. Journal of Abnormal Psychology, 121, 559–569. doi: 10.1037/a0028808
- McGlinchey, J. B., Atkins, D. C., & Jacobson, N. S. (2002). Clinical significance methods: Which one to use and how useful are they? Behavior Therapy, 33, 529–550. doi: 10.1016/S0005-7894(02)80015-6
- McIsaac, H. K., & Eich, E. (2004). Vantage point in traumatic memory. Psychological Science, 15, 248–253. doi: 10.1111/j.0956-7976.2004.00660.x
- Mergenthaler, E., & Stinson, C. (1992). Psychotherapy transcription standards. Psychotherapy Research, 2, 125–142. doi: 10.1080/10503309212331332904
- Mischkowski, D., Kross, E., & Bushman, B. J. (2012). Flies on the wall are less aggressive: Self-distancing “in the heat of the moment” reduces aggressive thoughts, angry feelings and aggressive behavior. Journal of Experimental Social Psychology, 48, 1187–1191. doi: 10.1016/j.jesp.2012.03.012
- Nigro, G., & Neisser, U. (1983). Point of view in personal memories. Cognitive Psychology, 15, 467–482. doi: 10.1016/0010-0285(83)90016-6
- Nolen-Hoeksema, S. (1991). Responses to depression and their effects on the duration of depressive episodes. Journal of Abnormal Psychology, 100, 569–582. doi: 10.1037/0021-843X.100.4.569
- Nolen-Hoeksema, S., Wisco, B. E., & Lyubomirsky, S. (2008). Rethinking rumination. Perspectives on Psychological Science, 3, 400–424. doi: 10.1111/j.1745-6924.2008.00088.x
- Paivio, S. C. (2013). Essential processes in emotion-focused therapy. Psychotherapy, 50(3), 341–345. doi: 10.1037/a0032810
- Pascual-Leone, A., & Greenberg, L. S. (2007). Emotional processing in experiential therapy: Why “the only way out is through”. Journal of Consulting and Clinical Psychology, 75, 875–887. doi: 10.1037/0022-006X.75.6.875
- Pennebaker, J. W. (1997). Writing about emotional experience as a therapeutic process. Psychological Science, 8(3), 162–166. doi: 10.1111/j.1467-9280.1997.tb00403.x
- Robinson, J. A., & Swanson, K. K. (1993). Field and observer modes of remembering. Memory (Hove, England), 1, 169–184. doi: 10.1080/09658219308258230
- Safran, J. D., & Segal, Z. V. (1990). Interpersonal process in cognitive therapy. Jason: Aronson.
- Salgado, J. (2014). ISMAI depression project: Results of a comparative clinical trial of EFT and CBT. Paper presented at 45th International Annual Meeting of Society for Psychotherapy Research, Copenhagen, Denmark.
- Stiles, W. B. (2011). Coming to terms. Psychotherapy Research, 21, 367–384. doi: 10.1080/10503307.2011.582186
- Stiles, W. B., Meshot, C. M., Anderson, T. M., & Sloan, W. W. (1992). Assimilation of problematic experiences: The case of John Jones. Psychotherapy Research, 2, 81–101. doi: 10.1037/0033-3204.38.4.462
- Stiles, W. B., Morrison, L. A., Haw, S. K., Harper, H., Shapiro, D. A., & Firth-Cozens, J. (1991). Longitudinal study of assimilation in exploratory psychotherapy. Psychotherapy: Theory, Research, Practice, Training, 28, 195–206. doi: 10.1037/0033-3204.28.2.195
- Verduyn, P., Mechelen, I. V., Kross, E., Chezzi, C., & Bever, F. V. (2012). The relationship cetween self-distancing and the duration of negative and positive emotional experiences in daily life. Emotion, 12, 1248–1263. doi: 10.1037/a0028289
- Wilson, T. D., & Gilbert, D. T. (2008). Explaining away a model of affective adaptation. Perspectives on Psychological Science, 3, 370–386. doi: 10.1111/j.1745-6924.2008.00085.x