
Abstract
Objective
Understanding the efficacy of each module of cognitive behavioral therapy (CBT) may inform efforts to improve outcomes for youth depression, but effects of specific modules have been difficult to examine. Idiographic interrupted time series models offer a robust way to estimate module effects on an individual’s symptoms. This study examined the association of specific CBT modules for depression on internalizing symptoms among depressed youths who received modular CBT in a randomized trial.
Methods
Individual models were created for three youths who met study criteria. Youths completed weekly symptom reports, and clinicians completed records of modules delivered. First order auto-regressive models quantified the change in average internalizing symptom severity between pre- and post-module delivery.
Results
All youths had 1–3 modules that were significantly associated with symptom reduction and 1–3 modules associated with deterioration. The 5 modules associated with improvement in at least one youth also lacked association (engagement, relaxation, cognitive reframing), or were associated with worsening (activity selection, parent psychoeducation) in others. Seven modules showed no measurable benefit, or detriment to any youth.
Conclusion
This study demonstrated that specific modules have measurable effects, but more work is needed to build an evidence base of specific module effects to inform treatment personalization for youth depression.
Clinical or methodological significance of this article: Idiographic models can be used estimate the effects of specific CBT modules in individuals. Only a few CBT modules (cognitive, behavioral, relaxation, engagement, and psychoeducation) demonstrated measurable benefit to at least one of three depressed youths and the modules associated with improvement in at least one youth lacked association, or were associated with worsening in others. Many modules showed no measurable benefit, suggesting a role for other factors and encouraging further examination into the specific effects of modules.
There is a pressing need to improve the efficacy of psychotherapy for youth depression. Across meta-analyses, psychotherapy for youth depression have demonstrated small to medium effect sizes (g = 0.29–0.48)—significantly smaller than that for adults with depression (Cuijpers et al., Citation2020), and significantly smaller than that for youths with anxiety, or conduct problems (Weisz et al., Citation2017a). Furthermore, interventions have not been made more efficacious over the years—mean effect size of therapies targeting youth depression has decreased significantly (Weisz et al., Citation2019). These findings indicate that youth depression treatments, including CBT, have a great deal of room for improvement.
CBT is based on the theory that one’s thoughts, behaviors, and feelings influence one another and that internalizing problems, which include anxious, depressive, and somatic symptoms (Achenbach et al., Citation2016), can be treated by changing maladaptive thoughts and behaviors that contribute to these problems (Reinecke & Ginsberg, Citation2008). These disorders are commonly comorbid – 74% of youths diagnosed with depression also have an anxiety disorder (Ghandour et al., Citation2019). CBT for youth depression typically uses a toolbox approach, wherein multiple modules are introduced, including psychoeducation, problem-solving, cognitive restructuring, relaxation, social skills and behavioral activation (Chorpita & Weisz, Citation2009; Weisz et al., Citation2017b). For example, cognitive restructuring could be used to coach youths to identify negative thoughts contributing to low mood, whereas behavioral activation could be used to help youths engage in rewarding activities they avoid. Identifying the effective ingredients of CBT could inform efforts to intensify, or prioritize specific modules to be used earlier to bring about greater, quicker symptom relief. Others have argued that identifying the evidence-based kernels of treatments could help facilitate dissemination (Embry & Biglan, Citation2008; Weisz et al., Citation2011). Unfortunately, efforts to identify the effective ingredients of therapies have produced inconclusive results. Dismantling and additive studies (i.e., randomized controlled trials [RCTs] comparing the effect of a therapy to that of the same therapy with one module removed, or added) were designed to test whether a specific module is efficacious. Meta-analyses of dismantling and additive studies have failed to identify efficacious modules in adult populations (Ahn & Wampold, Citation2001; Cuijpers, Reijnders, et al., Citation2019). Moreover, therapy is a complex and highly individualized process—pooling results across multiple participants and trials may obscure interpersonal variation that must be understood in order to learn what therapy works best for whom, and under what circumstances (Barlow & Nock, Citation2009; Paul, Citation1967).
An idiographic approach may help advance research in identifying effective ingredients (Ng & Weisz, Citation2016). Idiographic approaches examine repeatedly assessed variables within an individual, whereas nomothetic approaches (e.g., additive and dismantling studies) examine the average response across a group of individuals (Barlow & Nock, Citation2009). Aggregation across individuals, although useful for many purposes, may have limited the understanding of the main, or interactive effects of specific treatment modules on outcomes (Watkins et al., Citation2016). Idiographic designs offer benefits that can complement those of additive and dismantling studies. They are useful for examining intensively measured key variables over the course of an intervention and have been recommended for testing intervention–outcome relationships (Barlow & Nock, Citation2009; Persons & Boswell, Citation2019). Idiographic analyses enable direct testing of intrapersonal change—when conducted with multiple participants, assessing individual patterns of change can shed light on interpersonal differences that may not be apparent in RCTs (Barlow & Nock, Citation2009) Although small sample sizes may raise concerns about whether findings generalize to a broader population, the detailed examination of the individual possible with idiographic approaches aligns well with routine clinical practice (Persons & Boswell, Citation2019) and can be used to generate hypotheses to be tested with larger, more representative samples.
Studies of adults have used advanced idiographic analytic techniques such as the interrupted time series model to estimate the effects of specific treatment modules. Interrupted time series models are well-suited to the study of within-person change (Velicer & Colby, Citation2005) because they allow researchers to examine a pattern of change over time, rather than evaluating a single point, or estimating an average score. Interrupted time series are considered quasi-experimental designs and conceptualized as an extension of a pretest-posttest design (Reichardt, Citation2019). These models can be used to leverage existing RCT data with frequent (e.g., weekly) measurements of outcomes and module delivery. One study examined the temporal patterns of anxiety and depression symptoms in relation to the introduction of modules from the Unified Protocol (UP) and the introduction of a separate relaxation intervention (Boswell & Schwartzman, Citation2018). The introduction of the relaxation intervention was associated with a change in the level of average anxiety symptoms post-intervention (but not depression symptoms) compared to average symptoms pre-intervention, whereas the introduction of other UP modules were not. By modeling within-person processes of interest over time, this single case demonstrated that the relaxation intervention had a quantifiable association with anxiety symptoms. Other work has examined the temporal patterns of putative change constructs such as mindfulness, cognitive reappraisal and emotion avoidance, along with anxiety and depression symptoms, in relation to the introduction of UP modules (Boettcher & Barlow, Citation2019; Boswell et al., Citation2014, Citation2019; Boswell & Bugatti, Citation2016). Collectively, these studies suggest that modules may be differentially associated with symptom change across individuals. The independent efficacy of CBT modules for depression on improvement, or deterioration in symptoms has not been tested in youths. Quantifying module associations with symptoms will help identify which modules may be most helpful, or even harmful, and whether they differ across youths.
Objectives
The present study examined the association of specific CBT modules from a modular treatment protocol targeting depression on internalizing symptom outcomes among a sample of youths in a randomized effectiveness trial (Weisz et al., Citation2012). Our primary aim was to investigate whether specific therapy modules for depression have a measurable unique association with youths internalizing outcomes. Given the relevant literature with adults, we anticipated that specific modules would have a measurable association with internalizing outcomes. Our secondary aims were to explore which modules demonstrated measurable association and whether these modules differed across youths. Prior work with adults has demonstrated considerable heterogeneity as to which modules (if any) demonstrated an association on changes in symptoms (Boettcher & Barlow, Citation2019; Boswell et al., Citation2014, Citation2019; Boswell & Bugatti, Citation2016). Others have examined whether certain modules are associated with sudden gains in the same youth sample from which we drew our participants (Dour et al., Citation2013); however, sudden gains did not predict posttreatment internalizing symptoms, thus this work did not inform our hypotheses. The dearth of research on the effects of specific CBT modules did not justify hypotheses identifying the practices that might be most strongly associated with change in internalizing symptoms. The study design did not allow a test of whether modules differed from one another in effects, thus, our secondary aims were exploratory in nature, useful to inform hypothesis generation for future group designs.
Methods
Participants
Participants were drawn from a randomized effectiveness trial of treatment-seeking youths aged 7–13 years, who met the criteria for a DSM-IV diagnosis, or had clinically elevated levels of anxiety, depression, or conduct problems (Weisz et al., Citation2012). Informed consent and assent were obtained from caregivers and youths prior to study enrollment and all study procedures were approved by the institutional review boards of Judge Baker Children’s Center (affiliated with Harvard Medical School) and the University of Hawaii at Manoa. For the present study, we included youths who met the following criteria: (i) were randomized to modular therapy, (ii) had a diagnosis of depression and received at least 1 MATCH depression module, (iii) completed weekly ratings over at least 30 weeks during treatment, (iv) had less than 40% missing data on weekly youth-rated symptoms, and (v) displayed improvement in internalizing symptoms across treatment. The criterion for 30, or more weekly observations was implemented to ensure that the parameters of the time series models could be estimated accurately (SAS Institute Inc, Citation2015); fewer observations would not permit accurate and interpretable estimations. Procedures for handling missing time series data have been found to accurately estimate multiple parameters when up to 40% of the data is missing (Velicer & Colby, Citation2005), therefore this was the cutoff that we used. Improvement was defined as at least a 25% change (Tang et al., Citation2005) on the internalizing symptom broadband scale of the Youth Self Report (YSR; Achenbach & Rescorla, Citation2001), comparing baseline assessment to the first post-treatment clinical assessment. Out of the 174 youths in the original sample, 62 received modular therapy, of which 15 of had a diagnosis of depression. Of these 15, two did not receive any MATCH modules for depression, one youth did not demonstrate at least a 25% improvement in symptoms, one had >40% missing data, and another eight had fewer than 30 weeks of reports, resulting in three youths who met study criteria. Participant demographics, treatment duration, baseline and post-treatment symptoms are reported in . The three participants included in this sample had significantly higher parent-rated baseline externalizing scores compared to the 12 who were excluded as described above but did not differ in terms of baseline, or follow up internalizing scores, number of weeks in therapy, or number of sessions attended. See Supplemental Table 1 for details. Full procedures of the trial have been reported elsewhere (Weisz et al., Citation2012).
Table I. Participant demographics and treatment characteristics
Modular Treatment
Participants received the Modular Approach to Therapy for Children with Anxiety, Depression, Trauma, or Conduct Problems (MATCH; Chorpita & Weisz, Citation2009). The version of MATCH used in this trial included three decision flowcharts containing modules of evidence-based treatments for three problem areas: anxiety, depression, and disruptive behavior. Flowcharts were used to guide module selection in a flexible manner. A therapist might begin by selecting a flowchart corresponding to the youth’s presenting problem but could adjust module selection and sequence based on the youth’s presence of comorbid problems, treatment response, or treatment-interfering behaviors. Therapists could skip modules, repeat modules, or use modules targeting any problem area. Thus, two youths with the same presenting problem may not have received the same modules, same number of modules, or modules in the same order.
Measures
Therapist report of modules
Therapists, all employed in community outpatient clinics, completed weekly reports in collaboration with project supervisors detailing the content of each session using the Consultation Record (Ward et al., Citation2013). Therapist demographics and specialties are reported in . Therapists reports of modules they covered each session (fully, partially, or none), were validated against the ratings of trained coders who reviewed session recordings and completed a similar record, and who had already established interrater reliability with an index coder (Ward et al., Citation2013). Therapist reports of module coverage demonstrated acceptable agreement (mean ICC = 0.74, range = 0.42–1.0) with coder ratings and were used in the present analyses.
Youth symptoms
The YSR and the Child Behavior Checklist (CBCL; Achenbach & Rescorla, Citation2001), parallel youth- and parent-rated inventories of youth psychopathology, were administered at baseline, post-treatment, and at 3, 6, 9, and 18-month follow-up phone calls. The subset of YSR items at baseline assessment that comprise the Brief Problem Checklist (BPC; Chorpita et al., Citation2010) was used as the first observation in the time series models so that each model included at least one observation prior to the introduction of any therapy modules. Subsequent BPC observations were obtained via weekly phone calls. The BPC (Chorpita et al., Citation2010) is a twelve-item checklist (six internalizing items, six externalizing items, each rated on scale of 0-2) developed using item response theory and factor analysis on the CBCL and the YSR. The BPC has demonstrated robust reliability and validity; and has predicted clinical change in youth-rated symptoms during treatment (Chorpita et al., Citation2010). Discrepancies between child and parent reports are well documented (Achenbach, Citation2006; De Los Reyes, Citation2011) and may be present for internalizing symptoms because they are less observable to parents, or other informants (De Reyes & Kazdin, Citation2005). Therefore, we focused only on youth-rated symptoms on the BPC in the present study.
Data Analysis
Binning of weekly reports
Although the service programs generally aimed for weekly treatment sessions, there was considerable variability in the length of time between sessions among participants in the trial, (M = 11.46 days between sessions, SD = 6.99 days, range = 5–28 days) reflecting the conditions of community-based youth mental health services. Similarly, weekly phone call assessments, which were scheduled independently of treatment, varied within and across participants (M = 7.31 days between calls, SD = 3.48, range = 1–19 days). Because equally spaced observations are recommended for time series analyses (Nelson, Citation1998), we sought to equalize the units of time between observations. Dates of treatment sessions and youth reports of symptoms were organized into week-long bins. We maximined the number of weekly bins containing a session that was paired with youth report of symptoms in the subsequent bin. A full description of this procedure can be found in the Supplement. Analyses were conducted in R 3.5.1 and SAS 9.4.
Missing data and model selection
Missing weekly symptom report data were imputed using R packages forecast and imputeTS (Hyndman et al., Citation2020; Moritz & Bartz-Beielstein, Citation2017), which take into account time dependencies (see Supplement for details). An interrupted time series model was used to evaluate the association of the introduction of specific modules on internalizing symptoms. Separate models were tested for each participant. Models were estimated using PROC ARIMA in SAS (SAS Institute Inc, Citation2015). This model accounts for autocorrelation between sequential data points. An autocorrelation coefficient is used to represent correlation among symptom scores for a given lag in time (e.g., Yt and Yt−1). As our data was organized into weekly bins, a lag of 1 reflects the correlation between two scores at adjacent time points (a period of 7 days).
Given the nature of our univariate data, we anticipated and thus examined autocorrelation among internalizing symptom scores. A χ2 statistic was estimated to test the null hypothesis that none of the autocorrelations in the series were significantly different from zero. For all three participants, the null hypothesis could be rejected (all p < 0.05, see Supplemental Table 3), indicating that the data were nonstationary (i.e. the way that the data changes over time is not constant) and that it was appropriate to proceed with a time series model (SAS Institute Inc, Citation2015). Autocorrelation function (ACF) plots were used to aid the determination of which time series model would be best suited to analyze the data. ACF plots revealed that autoregressions decayed gradually over time, suggesting that autoregressive (AR) models would be appropriate (see Supplemental Figure 1). In AR models, current residuals are dependent on prior residuals. The model estimates the change in an outcome variable as an average change, plus some fraction of the previous change, plus a random error (Box et al., Citation2015). We selected an AR model with a lag of 1, meaning estimates for a given observation were dependent on the preceding observation. We sought to represent the data accurately and parsimoniously with few parameters. This aids interpretation and is recommended when selecting a model (Cryer & Chan, Citation2008).
Interrupted time series analysis
The association of the introduction of a given therapy module (e.g., problem solving) was tested by adding an intervention variable for each module to the model. These variables were coded as a step function, with values coded as “0” for every week prior to the introduction of the modules and coded as “1” for the week after the module was introduced and every week thereafter, ensuring that all symptom ratings used to evaluate the association of a module took place after the module was introduced. If a module was never introduced in full, the first date of its partial introduction was used. It was common for participants to receive modules multiple times over the course of therapy. Although models exist that can account for multiple intervention periods, such as a pulse model (Cryer & Chan, Citation2008), we opted for the step function because MATCH encourages practicing of skills and sustained learning, suggesting a youth would continue to use these skills after the session had ended (Chorpita & Weisz, Citation2009).
We tested one interrupted time series model per participant, including every dummy coded variable for each module a participant received over the course of treatment. In the event that multiple modules were introduced in the same week, one dummy coded variable was used to represent both modules. Consistent with the exploratory nature of our secondary aims, we examined every module that a given participant received, including those designed to treat anxiety, or conduct problems. Our rationale is that finding a lack of unique effects of some modules, including those not designed to target internalizing disorders, would strengthen conclusions that only specific modules have measurable effects on internalizing symptoms.
Model parameters estimated by maximum likelihood were examined to determine the association of the introduction of a given module on internalizing symptoms. Parameter estimates quantified the change in level of average internalizing symptoms from pre-module delivery to post-module delivery could be uniquely attributed to the introduction of that module. The proportion of explained variance in the time series models explained by each module was determined by calculating an R2 value for each module. Each R2 value was calculated as one minus the sum of the squared residual for each module divided by the sum of squares for internalizing symptoms for a given participant.
After estimating each AR model, a χ2 statistic was estimated to test whether the residuals from each model were uncorrelated. The null hypothesis of the χ2 test for autocorrelation of residuals for each model could not be rejected, indicating the AR model was an appropriate choice for each participant’s data (SAS Institute Inc, Citation2015; see ).
Table II. Chi-Square test for correlated residuals of estimated models for all participants
Results
For all youths, specific modules were significantly associated with changes in the level of average youth-reported internalizing symptoms from pre-module delivery to post-module delivery. The number of modules associated with changes in symptom varied among youths (range of modules with significant associations = 2–6, range of modules received = 11–15). illustrates the introduction of modules over the course of treatment associated with a significant change in level of average internalizing symptoms. Modules received by each participant and the associated parameter estimates across imputation methods are reported in . Which modules were associated with changes depended on the participant (see ). Four modules—Getting Acquainted (engagement), Learning About Depression – Parent (parent-focused psychoeducation), Learning to Relax (relaxation) and Cognitive Coping – TLC (cognitive reframing)—were significantly associated with a decrease in average symptoms for one youth each. A fifth module, Activity Selection (activity scheduling), was significantly associated with a decrease in symptoms for two youths. However, three modules—Activity Selection, Learning about Depression – Parent, Presenting a Positive Self (social skills), and Cognitive Coping – BLUE (cognitive reframing)—were significantly associated with an increase in symptoms for one youth each; and a fourth—Learning about Depression – Child—was significantly associated with an increase for two youths. Additionally, 7 modules—Problem Solving, Plans for Coping (maintenance), Quick Calming (relaxation), Talents & Skills (talent or skill building), Praise, Active Ignoring (differential reinforcement) and Wrap Up—were not associated with any significant change in symptoms for any participant. As our analyses were idiographic, we summarize the results for each participant below.
Figure 1. Introduction of specific MATCH modules from the depression set of modules in relation to youth - rated internalizing symptoms over time. Note. Components associated with a significant change in average internalizing symptom severity between the baseline rating of youth-rated symptoms and the delivery of the component are indicated by vertical lines. Lines indicate when a component was introduced, dotted lines indicate the introduction of the component was associated with significant increase in symptoms, dashed, a decrease
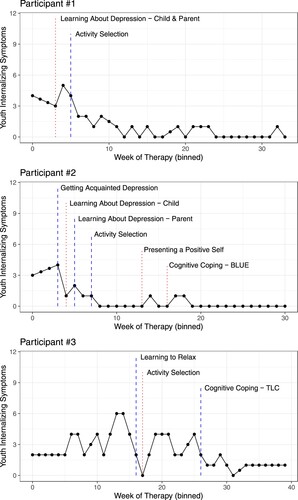
Table III. Time series parameter estimates for participant #1 across different imputation methods
Table IV. Time series parameter estimates for participant #2 across different imputation methods
Table V. Time series parameter estimates for participant #3 across different imputation methods
Table VI. Summary of results by module across participants
Participant #1 was an 11-year-old white male with a primary diagnosis of depression and comorbid anxiety disorders and ADHD. His self-identified presenting problems were feeling sad, cranky, angry, and anxious. The majority of the modules Participant #1 received targeted depression, with two additional modules targeting conduct problems. During week 3 of treatment both parent and child psychoeducation modules were introduced. They were significantly associated with an increase in the level of average symptoms from pre- to post-module delivery, B = 1.85, SE = 0.55, p = <0.01, R2 = 0.040. During week 5, pleasant activity scheduling was introduced and was associated with a decrease in symptoms, B = −2.01, SE = 0.55, p = <0.01, R2 = 0.099. Praise and differential reinforcement were introduced to address oppositional behavior. No other modules were associated with symptom change.
Participant #2 was a 10-year-old African American male with a primary diagnosis of depression and comorbid ODD and ADHD. His self-identified presenting problems were not listening to his mother, becoming angry easily, and difficulty calming himself when worried. He received only modules targeting depression. The therapist noted that the participant had difficulty engaging in treatment at first, but eventually completed most of the depression modules. An engagement module was introduced in week 3 and was associated with a decrease in level of average internalizing symptoms from pre- to post-module delivery, B = −3.0, SE = 0.37, p = <0.01. The following week, child psychoeducation was introduced and associated with an increase in symptoms, B = 0.99, SE = 0.37, p = <0.01, R2 = 0.005. During week 5 and 7, parent psychoeducation and activity selection were introduced and were both associated with a decrease in symptoms, B = −1.02, SE = 0.36, p = 0.01, R2 = 0.035 and B = −1.03, SE = 0.36, p = <0.01, R2 = 0.018. Other modules covering problem solving and relaxation were introduced later in treatment but were not associated with symptom change. During week 13 and 16, social skills and cognitive restructuring were introduced, and both were associated with symptom increases, B = 0.91, SE = 0.36, p = 0.01, R2 = 0.004 and B = 0.9, SE = 0.36, p = 0.01, R2 = 0.009.
Participant #3 was an 11-year-old white female with a primary diagnosis of depression and comorbid ADHD and social phobia. Her self-identified presenting problems were feeling like nothing was fun, a fear of heights, not listening and having trouble focusing. She received modules primarily targeting depression. Modules administered early in treatment (e.g., psychoeducation and problem solving were not associated with changes in symptoms). During week 16, relaxation was associated with decrease in symptoms, B = −3.18, SE = 1.16, p = 0.01, R2 = 0.086. The following week, activity scheduling was associated with an increase in symptoms, B = 2.52, SE = 1.23, p = 0.04, R2 = 0.020. A social skills module was introduced during week 20 but was not associated with symptom change. Cognitive restructuring was introduced during week 26 and was associated with a decrease in symptoms. No subsequent modules were associated with symptom change. The final module (wrap up) could not be examined as there were no symptom ratings recorded after the introduction of the module.
Discussion
Our primary aim was to investigate whether specific MATCH modules for depression have measurable and identifiable association with youth internalizing outcomes, as this has not been previously demonstrated in youths. As expected, specific modules showed measurable unique associations with decreases in the level of average internalizing symptoms for all youths, however some modules were associated with increases in symptoms and many modules were not associated with significant changes at all. In addressing our second aim, we found marked variability across participants in the modules that were associated with changes in the level of average youth-rated internalizing symptoms from pre- to post-module delivery. As all youths were selected for reliable reductions in their youth-rated internalizing symptoms, CBT as a whole was effective for these youths, but our results suggest that only a few CBT modules may be particularly beneficial to each youth. Indeed, only five out of 13 modules designed to target depression—pleasant activity scheduling, engagement, parent-focused psychoeducation, relaxation, and cognitive reframing—were associated with symptom reduction in any youth. Moreover, the modules demonstrating benefit differed substantially across individual youths.
Specific Modules with Measurable Associations with Improvement, or Deterioration
Overall, our findings suggest that some modules may be effective for some youths but may have no effect, or may even be iatrogenic for others. Although cognitive reframing is an active ingredient in CBT (Reinecke & Ginsberg, Citation2008) and therapist adherence to cognitive strategies during CBT with depressed adults has been found to predict treatment outcomes (Strunk et al., Citation2010), our findings related to cognitive reframing were mixed. One cognitive reframing module (TLC, focused on identifying friends to talk to and finding a silver lining) was associated with a decrease in symptoms for only one of the three youths (Participant #3) who received it. A second cognitive reframing module (BLUE, focused on identifying and evaluating the evidence for negative thoughts) was associated with an increase in symptoms for one other youth (Participant #2). It is possible some types of cognitive reframing may be more helpful, or accessible to preteens, who made up our sample. One time series analysis with one adult found cognitive reframing to be effective, (e.g., Boswell et al., Citation2014) however the generalizability of this finding is limited by the idiographic approach, as are our own results. A similar pattern of findings emerged for activity scheduling, which was associated with reductions in internalizing symptoms for two youths, but was associated with a worsening of symptoms for the third youth. Many of the skills introduced in CBT require practice to master. It is possible that the increase in symptoms in the weeks after the module was introduced (such as cognitive restructuring, or social skills) may be due to a lack of initial skill mastery and resulting frustration. Alternatively, it is possible that activity selection and cognitive reframing, two core modules of CBT depression, may be detrimental for some youths but beneficial, or ineffectual for others. Given our limited sample, more work is needed to determine for whom these modules are helpful, or harmful.
Relaxation was associated with symptom reduction in one youth, consistent with findings that relaxation treatments reduce depressive symptoms in youths (Kahn et al., Citation1990; Reynolds & Coats, Citation1986). However, relaxation was not effective for the other two youths, which stands in contrast to prior work on sudden gains using data from the same effectiveness trial. Dour et al. (Citation2013) found that therapist coverage of relaxation during the course of therapy was associated with sudden gains. However, the presence of sudden gains did not predict final internalizing symptoms, so it is possible that relaxation is less impactful for depressed youths.
In our sample, parent-focused psychoeducation was associated with symptom reduction for one youth and child-focused psychoeducation was associated with symptom increases for two youths. Psychoeducation has not been linked to changes in symptoms in time series models with adults (Boswell & Bugatti, Citation2016). Studies that did not have assessments prior to the first treatment session and used the first session (psychoeducation) as a starting point could not evaluate psychoeducation (e.g., Boswell et al., Citation2014). For Participant #1, both parent- and child-focused modules were introduced in the same week, therefore it is unclear which one, or both, contributed to the increase in symptoms. One cause for misalignment could be that some of the youth’s self-defined top problems (e.g., not listening, becoming angry) may not have corresponded with the therapist’s explanation of depression and youth-therapist disagreement on goals has important treatment implications (Hawley & Weisz, Citation2003). Perhaps when psychoeducation is the focus of early sessions without devoting time to engagement, or rapport, youth may feel disengaged. More work is needed to investigate the effectiveness of this module for youth depression (Bevan Jones et al., Citation2018).
Some CBT modules for depression may not produce the desired reduction in symptoms for depressed youths. Perhaps most striking is the absence of measurable association by more than half of the CBT modules introduced. Modules designed to target conduct problems were not associated with any changes in internalizing symptoms. Additionally, multiple modules designed to target depression, focused on problem solving, skill building, relaxation and maintenance were not associated with any significant change in symptoms for any participant. Half of the modules showed no association with symptom change, and the few modules that did, each accounted only for a small percentage of variance in the outcome (mean = 0.02 range = >−0.001-0.099). CBT for youth depression has been shown to have only modest effects in meta-analyses (Eckshtain et al., Citation2020) and has failed to outperform placebo in other trials (TADS Team, Citation2004). Additionally, when asked to report coping strategies they perceive to be effective, youths report some, but not all, strategies that align with evidence-based practice. For example, youth reported behavioral activation and seeking social support as effective, but did not report goal setting, self-monitoring, or other components from well-established treatments (Ng et al., Citation2016). One way to interpret these findings is that other unmeasured factors may matter as much as specific CBT modules, in driving therapeutic change (Ahn & Wampold, Citation2001). These factors may include therapeutic alliance, expectations about treatment, and other factors common to psychotherapies across orientations (Cuijpers, Reijnders, et al., Citation2019). Patient treatment expectations (Constantino et al., Citation2018) is also associated with improved outcomes. Thus, it is plausible that common factors were partially responsible for our study participants’ symptom improvement.
Another way to interpret our findings is that which specific CBT modules for depression are used for whom matter a great deal. Our findings that only one to three modules were associated with improvement for each youth, with a wide range in variance explained by each module, provide preliminary evidence that the toolbox approach may not be optimal for depressed youths. Given our findings that some modules were associated with increases in symptoms for some youths, it may be the case that some modules are not helpful for some youths, or may be detrimental if applied at the wrong time. The heterogeneity of symptom presentation in youth depression suggests that treating youth depression may require an approach where the treatment is matched to the youth (Eckshtain et al., Citation2020). Problem solving, one module not associated with any increases, or decreases in our sample, was a mediator of depression remission only among a subset of adolescents whose mothers had low depressive symptoms (Dietz, Citation2014). Although the literature about the unique associations of specific therapy modules is small, we contribute the first results from a youth sample and suggest that cognitive reframing, activity selection, relaxation, parent-focused psychoeducation, and engagement be examined further. Further work is needed both in the dismantling and mediator literature (Cuijpers, Cristea, et al., Citation2019; Ng et al., Citation2020) and convergent findings from idiographic and nomothetic designs would strengthen the evidence base for the specific effects of these five modules.
It is noteworthy that some modules linked with benefit in one youth were associated with lack of improvement, or even deterioration in others. The differential association of modules across individuals has implications for the selection of treatments, or their modules as a way to personalize therapy. There is evidence that depressed individuals have different optimal treatments that depend in part on their personal and clinical characteristics (Cohen & Derubeis, Citation2018; DeRubeis et al., Citation2014). One study found that youths matched to treatment that aligned with their type of risk for depression (e.g., CBT for youths exhibiting negative cognitive styles and interpersonal psychotherapy for youths with family conflict, or low peer-support) showed greater improvement compared to youths who received the other treatment (Young et al., Citation2021). These findings suggest that the same strategies may work differently across youths who vary in risk factors and other characteristics. MATCH algorithms facilitate personalized selection of modules to address comorbid diagnoses and treatment interference, they do not dictate options for personalizing treatment within a diagnostic category. Although module selection is informed by therapists and consultants, the algorithm does not determine whether a patient might benefit most by starting therapy with a specific module based on empirical evidence linking module effects to risk factors and personal characteristics. Our findings about specific modules—if replicated in larger samples–suggest that identifying modules likely to be helpful to an individual and delivering them early, or in increased doses could shorten treatment and increase the efficacy of therapy. However, we note that MATCH was effective overall for these youths despite moments of non-improvement, or deterioration. Although MATCH does not prescribe a personalized sequence of depression-specific modules in advance, its built-in flexibility, in tandem with a measurement feedback system, facilitates selection of modules to optimize response during the course of treatment. We believe that the best outcomes will result from personalized treatment selection and sequencing plus ongoing tailoring based on outcome monitoring.
Limitations
The three participants in the present study may differ from the other participants with a depression diagnosis in the trial on important, but unmeasured, characteristics. In particular, selecting youths with 30, or more weeks of data was necessary for building our models, but eliminated more than half of the MATCH participants with depression. Given that CBT typically lasts 16–20 sessions (Reinecke & Ginsberg, Citation2008), our sample may have had more treatment obstacles, more severe comorbidities,, or slower progress than their peers. Our sample had higher baseline externalizing symptoms, but did not differ on other factors, including weeks of therapy.
There are many unmeasured factors that could have contributed a participant’s treatment trajectory. Our analyses did not account for other factors such as external events that may have occurred outside of therapy. Therapist competency, or measures of therapeutic alliance were mot measured, and both could have influenced module delivery and effectiveness across participants. Given the large number of modules tested, there is also a possibility of chance findings.
Interrupted time series models are limited in several ways. First, they accord more power to modules delivered earlier in treatment. However, sequence effects are unlikely to account for all our findings given the wide range of weeks in which modules with measurable associations were introduced (3 through 26). Second, these models produce findings that are specific to the individuals examined. As with all idiographic methods, the flexibility of these models to estimate module effects within highly personalized intervention sequences comes with tradeoffs in the generalizability of the findings produced. Finally, as our study was specific to depressed youth in one MATCH trial, our findings cannot generalize to other CBT protocols, disorders, or trials.
Future Directions
Because of their capacity for probing patterns of intra-individual change and shedding light on individual differences, we join other researchers (e.g., Barlow & Nock, Citation2009) in advocating for greater use of idiographic approaches. Specifically, single-case designs that involve experimental manipulation of module introduction and real-time monitoring of changes in symptoms could provide stronger evidence of specific module effects (Kazdin, Citation2019). Future work would do well to incorporate measures of hypothesized change mechanisms, to consider the role of common factors on treatment trajectories, and measure factors such as therapeutic alliance, therapist competence and participant expectations about treatment. Measuring change in a mechanism (e.g., use of cognitive strategies) accompanied by symptom reduction following introduction of the relevant module (e.g., cognitive reframing) would increase confidence that the symptom reduction is indeed attributed to that module (Boswell et al., Citation2014). Case studies, or multiple case experiments can match module introduction with case formulations and client presentations to examine module-specific effects. Analyzing recordings, or transcripts of sessions may further illuminate change processes that occur within sessions. Qualitative data collected from therapists and patients throughout therapy could provide additional context to support findings from idiographic analyses, revealing for example life events that might have contributed to improvement, or worsening of symptoms. Such data, even in RCTs, could contribute to our ability to understand why a certain treatment technique might be effective for a given youth.
Nomothetic designs such as randomized fractional factorial and Sequential Multiple Assignment Randomized Trials (SMARTs) can be used to determine the main effect of modules (Watkins et al., Citation2016) and compare the sequence, dose, and timing at which interventions are administered (Lei et al., Citation2012). However, there is an upper limit to the different module subsets and sequences that can be feasibly tested. Therefore, we suggest that researchers leverage idiographic designs, or idiographic analyses of existing RCT data, as we have done, to identify modules to prioritize in future studies utilizing nomothetic designs.
Our use of a novel idiographic approach provided evidence that some specific modules of CBT for depression have measurable and unique associations with the internalizing symptom outcomes of depressed youths. Many modules were not associated with changes in symptoms, and some modules were associated with increases in symptoms for some youths. Our results offer preliminary evidence that only a few of the CBT modules delivered may be beneficial for each depressed youth, and these modules may differ across individuals. However, their modest effects leave room for other unmeasured factors to play a substantial role in therapeutic change. To the extent that specific modules are effective for each youth, identifying these modules and the characteristics of individuals that predict which modules will be most helpful, could offer a way to personalize CBT and improve treatment response among youths with depression.
Supplemental Material
Download Zip (408.6 KB)Acknowledgements
These data were as part of a collection of projects by the Research Network on Youth Mental Health, a collaborative network funded by the John D. and Catherine T. MacArthur Foundation. Network Members at the time this work was performed included: John Weisz, Ph. D. (Network Director), Bruce Chorpita, Ph. D., Robert Gibbons, Ph. D., Charles Glisson, Ph.D., Evelyn Polk Green, M.A., Kimberly Hoagwood, Ph.D., Kelly Kelleher, M.D., John Landsverk, Ph.D., Stephen Mayberg, Ph.D., Jeanne Miranda, Ph.D., Lawrence Palinkas, Ph.D., Sonja Schoenwald, Ph.D.
Disclosure Statement
The authors declare the following potential competing interests: Bruce Chorpita and John Weisz are co-authors of the MATCH manual used in treatment of the youths in this study, and both receive income from sales of the manual.
Correction Statement
This article has been corrected with minor changes. These changes do not impact the academic content of the article.
Additional information
Funding
References
- Achenbach, T. M. (2006). As others see us clinical and research implications of cross-informant correlations for psychopathology. Current Directions in Psychological Science, 15(2), 94–98. https://doi.org/10.1111/j.0963-7214.2006.00414.x
- Achenbach, T. M., Ivanova, M. Y., Rescorla, L. A., Turner, L. V., & Althoff, R. R. (2016). REVIEW internalizing/externalizing problems: Review and recommendations for clinical and research applications. Journal of the American Academy of Child & Adolescent Psychiatry, 55(8), 647–656. www.jaacap.org. https://doi.org/10.1016/j.jaac.2016.05.012
- Achenbach, T. M., & Rescorla, L. A. (2001). Manual for the ASEBA school-age forms & profiles: An integrated system of multi-informant assessment. University of Vermont, Research Center for Children, Youth, & Families.
- Ahn, H. N., & Wampold, B. E. (2001). Where Oh where are the specific ingredients? A meta-analysis of component studies in counselling and psychotherapy. Journal of Counseling Psychology, 48(3), 251–257. https://doi.org/10.1037/0022-0167.48.3.251
- Barlow, D. H., & Nock, M. K. (2009). Why can’t we be more idiographic in our research? Perspectives on Psychological Science, 4(1), 19–21. https://doi.org/10.1111/j.1745-6924.2009.01088.x
- Bevan Jones, R., Thapar, A., Stone, Z., Thapar, A., Jones, I., Smith, D., & Simpson, S. (2018). Psychoeducational interventions in adolescent depression: A systematic review. Patient Education and Counseling, 101(5), 804–816. https://doi.org/10.1016/J.PEC.2017.10.015
- Boettcher, H., & Barlow, D. H. (2019). The unique and conditional effects of interoceptive exposure in the treatment of anxiety: A functional analysis. Behaviour Research and Therapy, 117, 65–78. https://doi.org/10.1016/j.brat.2018.12.002
- Boswell, J. F., Anderson, L. M., & Barlow, D. H. (2014). An idiographic analysis of change processes in the unified transdiagnostic treatment of depression. Journal of Consulting and Clinical Psychology, 82(6), 1060–1071. https://doi.org/10.1037/a0037403
- Boswell, J. F., Anderson, L. M., Oswald, J. M., Reilly, E. E., Gorrell, S., & Anderson, D. A. (2019). A preliminary naturalistic clinical case series study of the feasibility and impact of interoceptive exposure for eating disorders. Behaviour Research and Therapy, 117, 54–64. https://doi.org/10.1016/j.brat.2019.02.004
- Boswell, J. F., & Bugatti, M. (2016). An exploratory analysis of the impact of specific interventions: Some clients reveal more than others. Journal of Counseling Psychology, 63(6), 710–720. https://doi.org/10.1037/cou0000174
- Boswell, J. F., & Schwartzman, C. M. (2018). An exploration of intervention augmentation in a single case. Behavior Modification, 0145445518796202. https://doi.org/10.1177/0145445518796202
- Box, G. E. P., Jenkins, G. M., Reinsel, G. C., & Ljung, G. M. (2015). Time series analysis: Forecasting and control. John Wiley & Sons.
- Chorpita, B., & Weisz, J. (2009). MATCH-ADTC: Modular Approach to Therapy for Children (MATCH) with anxiety, depression, trauma, or conduct problems.
- Chorpita, B. F., Reise, S., Weisz, J. R., Grubbs, K., Becker, K. D., & Krull, J. L. (2010). Evaluation of the brief problem checklist: Child and caregiver interviews to measure clinical progress. Journal of Consulting and Clinical Psychology, 78(4), 526–536. https://doi.org/10.1037/a0019602
- Cohen, Z. D., & Derubeis, R. J. (2018). Treatment selection in depression. Annual Review of Clinical Psychology, 14(1), 209–236. https://doi.org/10.1146/annurev-clinpsy-050817-084746
- Constantino, M. J., Visla, A., Coyne, A. E., & Boswell, J. F. (2018). A meta-analysis of the association between patients’ early treatment outcome expectation and their posttreatment outcomes. Psychotherapy, 55(4), 473–485. https://doi.org/10.1037/pst0000169
- Cryer, J. D., & Chan, K.-S. (2008). Time series analysis: with applications in R. Springer Science & Business Media.
- Cuijpers, P., Cristea, I. A., Karyotaki, E., Reijnders, M., & Hollon, S. D. (2019). Component studies of psychological treatments of adult depression: A systematic review and meta-analysis. Psychotherapy Research, 29(1), 15–29. https://doi.org/10.1080/10503307.2017.1395922
- Cuijpers, P., Karyotaki, E., Eckshtain, D., Ng, M. Y., Corteselli, K. A., Noma, H., Quero, S., & Weisz, J. R.. (2020). Psychotherapy for depression across different age groups: A systematic review and meta-analysis. JAMA Psychiatry, 77(7), 694–702. https://doi.org/10.1001/jamapsychiatry.2020.0164
- Cuijpers, P., Reijnders, M., & Huibers, M. J. H. (2019). The role of common factors in psychotherapy outcomes. Annual Review of Clinical Psychology, 15(1), 207–231. https://doi.org/10.1146/annurev-clinpsy-050718-095424
- De Los Reyes, A. (2011). Introduction to the special section: More than measurement error: Discovering meaning behind informant discrepancies in clinical assessments of children and adolescents. Journal of Clinical Child & Adolescent Psychology, 40(1), 1–9. https://doi.org/10.1080/15374416.2011.533405
- De Reyes, A. L., & Kazdin, A. E. (2005). Informant discrepancies in the assessment of childhood psychopathology: A critical review, theoretical framework, and recommendations for further study. Psychological Bulletin, 131(4), 483–509. https://doi.org/10.1037/0033-2909.131.4.483
- DeRubeis, R. J., Cohen, Z. D., Forand, N. R., Fournier, J. C., Gelfand, L. A., & Lorenzo-Luaces, L. (2014). The personalized advantage index: Translating research on prediction into individualized treatment recommendations. A demonstration. PLoS ONE, 9(1), e83875. https://doi.org/10.1371/journal.pone.0083875
- Dietz, L. J. (2014). Social problem solving among depressed adolescents is enhanced by structured psychotherapies. Journal of Consulting and Clinical Psychology, 82(2), 202. https://doi.org/10.1037/A0035718
- Dour, H. J., Chorpita, B. F., Lee, S., Weisz, J. R., Chorpita, B., Garland, A., Gibbons, R., Glisson, C., Green, E. P., Hoagwood, K., Kelleher, K., Landsverk, J., Mayberg, S., Miranda, J., Palinkas, L., & Schoenwald, S. (2013). Sudden gains as a long-term predictor of treatment improvement among children in community mental health organizations. Behaviour Research and Therapy, 51(9), 564–572. https://doi.org/10.1016/j.brat.2013.05.012
- Eckshtain, D., Kuppens, S., Ugueto, A., Ng, M. Y., Vaughn-Coaxum, R., Corteselli, K., & Weisz, J. R. (2020). Meta-Analysis: 13-year follow-up of psychotherapy effects on youth depression. Journal of the American Academy of Child and Adolescent Psychiatry, 59(1), 45–63. https://doi.org/10.1016/j.jaac.2019.04.002
- Embry, D. D., & Biglan, A. (2008). Evidence-based kernels: Fundamental units of behavioral influence. Clinical Child and Family Psychology Review, 11(3), 75–113. https://doi.org/10.1007/S10567-008-0036-X
- Ghandour, R. M., Sherman, L. J., Vladutiu, C. J., Ali, M. M., Lynch, S. E., Bitsko, R. H., & Blumberg, S. J. (2019). Prevalence and treatment of depression, anxiety, and conduct problems in US children. Journal of Pediatrics, 206, 256–267. https://doi.org/10.1016/j.jpeds.2018.09.021
- Hawley, K. M., & Weisz, J. R. (2003). Child, parent, and therapist (dis)agreement on target problems in outpatient therapy: The therapist’s dilemma and its implications. Journal of Consulting and Clinical Psychology, 71(1), 62–70. https://doi.org/10.1037/0022-006X.71.1.62
- Hyndman, R. J., Athanasopoulos, G., Bergmeir, C., Caceres, G., Chhay, L., O’Hara-Wild, M., Petropoulos, F., Razbash, S., & Wang, E. (2020). Package ‘forecast.’ CRAN.
- Kahn, J. S., Kehle, T. J., Jenson, W. R., & Clark, E. (1990). Comparison of cognitive-behavioral, relaxation, and self-modeling interventions for depression among middle-school students. School Psychology Review, 19(2), 196–211. https://doi.org/10.1080/02796015.1990.12085457
- Kazdin, A. E. (2019). Single-case experimental designs. Evaluating interventions in research and clinical practice. Behaviour Research and Therapy, 117, 3–17. https://doi.org/10.1016/j.brat.2018.11.015
- Lei, H., Nahum-Shani, I., Lynch, K., Oslin, D., & Murphy, S. A. (2012). A “SMART” design for building individualized treatment sequences. Annual Review of Clinical Psychology, 8(1), 21–48. https://doi.org/10.1146/annurev-clinpsy-032511-143152
- Moritz, S., & Bartz-Beielstein, T. (2017). imputeTS: Time series missing value imputation in R. R Journal, 9(1), 207–218. https://doi.org/10.32614/rj-2017-009
- Nelson, B. K. (1998). Time series analysis using autoregressive integrated moving average (ARIMA) models. Academic Emergency Medicine, 5(7), 739–744. https://doi.org/10.1111/j.1553-2712.1998.tb02493.x
- Ng, M. Y., DiVasto, K. A., Cootner, S., Gonzalez, N., & Weisz, J. R. (2020). What do 30 years of randomized trials tell us about how psychotherapy improves youth depression? A systematic review of candidate mediators. Clinical Psychology: Science and Practice, 00, e12367. https://doi.org/10.1111/cpsp.12367
- Ng, M. Y., Eckshtain, D., & Weisz, J. R. (2016). Assessing Fit between evidence-based psychotherapies for youth depression and real-life coping in early adolescence. Journal of Clinical Child and Adolescent Psychology, 45(6), 732–748. https://doi.org/10.1080/15374416.2015.1041591
- Ng, M. Y., & Weisz, J. R. (2016). Annual research review: Building a science of personalized intervention for youth mental health. Journal of Child Psychology and Psychiatry, and Allied Disciplines, 57(3), 216–236. https://doi.org/10.1111/jcpp.12470
- Paul, G. L. (1967). Strategy of outcome research in psychotherapy. Journal of Consulting Psychology, 31(2), 109–118. https://doi.org/10.1037/h0024436
- Persons, J. B., & Boswell, J. F.. (2019). Single case and idiographic research: Introduction to the special issue. Behaviour Research and Therapy, 117, 1–2. https://doi.org/10.1016/j.brat.2019.03.007
- Reichardt, C. S. (2019). Quasi-Experimentation: A guide to design and analysis. Guilford Publications.
- Reinecke, M. A., & Ginsberg, G. S. (2008). Cognitive behavioral treatment of depression in children and adolescents. In J. R. Z. Abela, & B. L. Hankin (Eds.), Depression in children and adolescents (pp. 179–206). Guilford Press.
- Reynolds, W. M., & Coats, K. I. (1986). A comparison of cognitive-behavioral therapy and relaxation training for the treatment of depression in adolescents. Journal of Consulting and Clinical Psychology, 54(5), 653–660. https://doi.org/10.1037//0022-006x.54.5.653
- SAS Institute Inc. (2015). SAS/STAT 14.1 user’s guide. SAS Institute Inc.
- Strunk, D. R., Brotman, M. A., & DeRubeis, R. J. (2010). The process of change in cognitive therapy for depression: Predictors of early inter-session symptom gains. Behaviour Research and Therapy, 48(7), 599–606. https://doi.org/10.1016/j.brat.2010.03.011
- TADS Team. (2004). Fluoxetine, cognitive-behavioral therapy, and their combination for adolescents with depression: Treatment for adolescents With depression study (TADS) randomized controlled trial. JAMA, 292(7), 807–820. https://doi.org/10.1001/JAMA.292.7.807
- Tang, T. Z., Beberman, R., DeRubeis, R. J., & Pham, T. (2005). Cognitive changes, critical sessions, and sudden gains in cognitive-behavioral therapy for depression. Journal of Consulting and Clinical Psychology, 73(1), 168–172. https://doi.org/10.1037/0022-006X.73.1.168
- Velicer, W. F., & Colby, S. M. (2005). A comparison of missing-data procedures for arima time-series analysis. Educational and Psychological Measurement, 65(4), 596–615. https://doi.org/10.1177/0013164404272502
- Ward, A. M., Regan, J., Chorpita, B. F., Starace, N., Rodriguez, A., Okamura, K., Daleiden, E. L., Bearman, S. K., Weisz, J. R., & The Research Network on Youth Menta (2013). Tracking evidence based practice with youth: Validity of the MATCH and standard manual consultation records. Journal of Clinical Child & Adolescent Psychology, 42(1), 44–55. https://doi.org/10.1080/15374416.2012.700505
- Watkins, E., Newbold, A., Tester-Jones, M., Javaid, M., Cadman, J., Collins, L. M., Graham, J., & Mostazir, M. (2016). Implementing multifactorial psychotherapy research in online virtual environments (IMPROVE-2): study protocol for a phase III trial of the MOST randomized component selection method for internet cognitive-behavioural therapy for depression. BMC Psychiatry, 16(1), https://doi.org/10.1186/s12888-016-1054-8
- Weisz, J., Bearman, S. K., Santucci, L. C., & Jensen-Doss, A. (2017a). Initial test of a principle-guided approach to transdiagnostic psychotherapy with children and adolescents. Journal of Clinical Child & Adolescent Psychology, 46(1), 44–58. https://doi.org/10.1080/15374416.2016.1163708
- Weisz, J. R., Chorpita, B. F., Palinkas, L. A., Schoenwald, S. K., Miranda, J., Bearman, S. K., Daleiden, E. L., Ugueto, A. M., Ho, A., Martin, J., Gray, J., Alleyne, A., Langer, D. A., Southam-Gerow, M. A., Gibbons, R. D., & Research Network on Youth Mental Health (2012). Testing standard and modular designs for psychotherapy treating depression, anxiety, and conduct problems in youth: A randomized effectiveness trial. JAMA Psychiatry, 69(3), 274–282. https://doi.org/10.1001/archgenpsychiatry.2011.147
- Weisz, J. R., Kuppens, S., Ng, M. Y., Eckshtain, D., Ugueto, A. M., Vaughn-Coaxum, R., Jensen-Doss, A., Hawley, K. M., Krumholz Marchette, L. S., Chu, B. C., Robin Weersing, V., & Fordwood, S. R. (2017b). What five decades of research tells us about the effects of youth psychological therapy: A multilevel meta-analysis and implications for science and practice. American Psychologist, 72(2), 79–117. https://doi.org/10.1037/a0040360
- Weisz, J. R., Kuppens, S., Ng, M. Y., Vaughn-Coaxum, R. A., Ugueto, A. M., Eckshtain, D., & Corteselli, K. A. (2019). Are psychotherapies for young people growing stronger? Tracking trends over time for youth anxiety, depression, attention-deficit/hyperactivity disorder, and conduct problems. Perspectives on Psychological Science, 14(2), 216–237. https://doi.org/10.1177/1745691618805436
- Weisz, J. R., Ugueto, A. M., Herren, J., Afienko, S. R., & Rutt, C. (2011). Kernels vs. Ears, and other questions for a science of treatment dissemination. Clinical Psychology: Science and Practice, 18(1), 41–46. https://doi.org/10.1111/J.1468-2850.2010.01233.X
- Young, J. F., Jones, J. D., Gallop, R., Benas, J. S., Schueler, C. M., Garber, J., & Hankin, B. L. (2021). Personalized depression prevention: A randomized controlled trial to optimize effects through risk-informed personalization. Journal of the American Academy of Child & Adolescent Psychiatry, 60(9), 1116–1126.e1. https://doi.org/10.1016/J.JAAC.2020.11.004