

Physical therapists use a number of tools for pain management, including exercise, education, thermal and electrical agents, and orthopedic manual therapy (OMT). Orthopedic manual therapy comprises a heterogeneous set of interventions such as thrust (TM) and non-thrust manipulation (NTM), soft-tissue manipulation, and neurodynamic movements. The use of OMT in clinical practice is supported across a wide body of literature [Citation1–5] and has been endorsed by clinical practice guidelines (CPGs) [Citation6–11]. Despite this evidential support, it is well known that results differ markedly across patient populations that are treated with OMT [Citation12–18]. Additionally, specific application of OMT techniques may not result in superior outcomes when compared to randomly selected or nonspecific application of said techniques [Citation19–23].
The aforementioned findings involving OMT are similar to those of other efficacious interventions. Clinical studies on chronic pain syndromes such as fibromyalgia and osteoarthritis have shown great inconsistency in therapeutic responses between individuals, even when efficacious interventions such as exercise or medications are used [Citation24–26]. Variability in therapeutic response is partly explained by psychosocial factors and individual differences in how pain is modulated at the patient levelCitation27 and the failure to precisely characterize the pathophysiologic mechanisms that influence subgroups of patients [Citation27]. This has prompted researchers to attempt the subgrouping of patients to better identify responders and non-responders to dedicated interventions: this is a concept known as phenotyping.
Phenotyping has been defined as ‘the ensemble of observable characteristics displayed by an organism’ [Citation28]. Historically, phenotyping was associated with an individual’s interactions between their genotype and the environment. Only recently have researchers incorporated the use of clinical phenotyping, attempting to define groups of patients who may respond to specifically targeted treatments. Clinical phenotypes are based mainly on observable clinical and physiological measures. Clinical ‘pain’ phenotyping (whereby described as pain phenotyping) characterizes patients based on their pain experience and their response to dedicated interventions [Citation28,Citation29–31].
With respect to OMT, it has historically been assumed that the clinical effectiveness of the approach was associated with the technique selected (specialized training) and the skill of the clinician who applies the technique. We theorize that the differences in responses seen in clinical practice are reflective of variations in pain phenotypes and less reflective of techniques used or provider skill. While evidence suggests that higher-level training promotes better outcomes, we propose that this is related to improved ability to identify individuals who will have a favorable response to care rather than improved skill of OMT application [Citation32]. The purpose of this paper is to reinforce the assumption that the likelihood of achieving a positive outcome with an OMT approach depends on selecting a patient with an amenable pain phenotype. To support our theory, we will present work supporting: (1) Different OMT techniques provide similar and consistent mechanisms in preclinical research; (2) current non-OMT pain phenotyping approaches support the assumption that patient-related factors are associated with a given pain response; (3) pain profiling in clinical trials has failed to consistently identify individuals with favorable outcomes to OMT; and (4) with the appropriate research, clinicians have the capacity to identify potential pain phenotype in their clinical assessment.
Different OMT techniques provide similar and consistent mechanisms in preclinical research
The term ‘mechanism’ reflects the steps or processes through which intervention (independent variable) actually unfolds and produces the change (outcome variable). The National Institutes of Health defines mechanistic studies as designed to understand a biological or behavioral process, the pathophysiology of a disease, or the mechanism of action of an intervention [Citation33].
Neurophysiological mechanisms of all OMT forms have been well established as a significant driver of the analgesic response [Citation34–39]. Neurophysiological mechanisms combine to create a peripheral, spinal, and supraspinal modulatory response which is thought to be the cornerstone for pain inhibition [Citation34,Citation40]. Peripheral pain inhibition in response to OMT has been demonstrated with a local increase in pain pressure threshold (PPT) without the same response remotely [Citation41]. It is proposed that this peripheral mechanism is attributed to a modification in inflammatory markers [Citation34,Citation40,Citation42]. All forms of OMT reduce inflammatory mediator expression leading to increased PPT and reduction in temporal summation [Citation43–45].
Changes in PPT locally without remote changes are not consistent; therefore, when congruent changes occur locally and remotely, a central inhibitory effect is suggested [Citation41,Citation46]. This effect is proposed to be related to changes in pain-modulating peptides and neurotransmitters influenced by OMT. Serotonin and dopamine are altered with OMT [Citation35] and act as pain-modulating neurotransmitters altering the affective component of pain [Citation47]. The proposed sites of action for both dopamine and serotonin are widespread, including the dorsal horn of the spinal cord, periaqueductal gray, thalamus, basal ganglia, insular cortex, and cingulate cortex [Citation48,Citation49]. Oxytocin is another pain-modulating peptide affected by OMT [Citation35], mitigating pain at the brain and spinal cord level [Citation50]. At the spinal level, reviews on both humans and animals have established the effect OMT has on improved descending inhibition [Citation35,Citation51,Citation52]. Studies on temporal summation, a measure of dorsal horn excitability, support direct inhibition with OMT [Citation53–55].
Autonomic nervous system (ANS) response to OMT is assessed through measuring skin temperature, skin conduction, heart rate, and cortisol level changes [Citation40]. A recent review concluded that OMT techniques affect the ANS with a combination of sympathetic and parasympathetic nervous system reactions [Citation42]. The same review was not able to find evidence to support any differences in ANS response with differing manual techniques; however, this was not measured in most of the included studies [Citation42].
Pre-clinical research involving TM and NTM produces consistent mechanistic responses across animal and human populations including transient neurophysiological (peripheral and central pain modulation), biomedical (immune and inflammatory systems and musculoskeletal stiffness), and psychological (contextual) mechanisms. These findings are supported by a number of systematic reviews involving preclinical research [Citation35,Citation41,Citation43,Citation51,Citation52,Citation56]. Although it is clear that the translation of these mechanisms to clinical outcomes is woefully understudied, it is unlikely that differences in mechanisms alone account for the great variability we see in clinical outcomes reported by patients.
Current pain phenotyping approaches support the assumption that patient-related factors are associated with a given pain response
Phenotyping studies use cluster and latent class analysis to identify characteristics of those with favorable analgesic response. These analyses identify patterns in multiple dependent variables and correlate them to related outcome variables to develop groups. Pain phenotyping trials have used both predictors of pain state (pain intensity, temporal summation, and conditioned pain modulation) and response to analgesic management as outcomes within these models.
Cross-sectional designs develop phenotypic groups based on characteristics demonstrated by those with optimal versus impaired pain states [Citation57–62]. Grouping by conditioned pain modulation and temporal summation demonstrates the interaction between pain intensity, locations, and threshold contributing to phenotype, while psychological variables did not contribute [Citation62]. Grouping patients with osteoarthritis based on the persistence of knee pain demonstrates the interaction between PPT and temporal summation contributing to phenotype, while similarly no interaction from psychological variables is demonstrated [Citation59]. Grouping by self-reported functional limitations, pain intensity, gait speed, and health-care utilization demonstrates the interaction between pain intensity, locations, threshold, psychological distress, and number of comorbidities contributing to phenotype [Citation61]. Grouping LBP based on pain intensity and variability demonstrates the interaction between fatigue, pain qualities, and presence of central sensitization contributing to phenotype [Citation60]. Grouping patients with chronic pain based on pain characteristics (intensity, location, and duration) demonstrates the interaction between psychological strain, comorbid fibromyalgia diagnosis, social distress, and gender contributing to phenotype [Citation57]. Grouping based on the presence of somatic widespread symptoms demonstrates the interaction between anxiety, depression, and emotional stability contributing to phenotype [Citation58].
Phenotyping based on responsiveness to analgesic intervention has also demonstrated contributions from patient-specific characteristic [Citation63–64]. Grouping patients with chronic pain receiving multimodal inpatient care based on reported measures of pain burden shows presence of depression, previous pharmacological and psychological intervention, and patient age all interacting to contribute to phenotype [Citation63]. Individuals with high pain burden at baseline demonstrate improved pain outcomes, while those in other subgroups of pain burden show only improvement in depression and anxiety outcomes [Citation63].
Higher baseline pain intensity is phenotypic for treatment effect size following lumbar spinal manipulative therapy (SMT) [Citation65]. Patient expectations of recovery and comfort during treatment are phenotypic for response following thoracic SMT, while biomechanical parameters of SMT do not alter response [Citation66]. Grouping based on local response to sustained noxious stimulation (pain adaptability) has identified two phenotypes both in healthy controls [Citation64] and in patients with musculoskeletal painCitation67: those who are pain adaptable (demonstrate a reduction in pain over time) and those who are non-pain adaptable (demonstrate no reduction in pain over time). Latency to peak pain was the only variable that significantly correlated with pain adaptability. In these studies [Citation64,Citation67], conditioned pain modulation did not contribute to adaptability phenotype, suggesting another rationale for analgesia independent of central pain modulation.
The use of pain profiling in clinical trials has failed to consistently identify individuals with favorable outcomes to OMT
Clinical trials [Citation68–71] and reviews [Citation72–74] support OMT’s direct effect on reducing pain sensitivity locally and remotely. This is consistent regardless of the persistent or episodic nature of pain [Citation75]. These findings are not specific to one technique with similar findings with manipulation, mobilization, and sham procedures [Citation68,Citation69,Citation76]. Increased sensitivity at baseline correlates with larger increases in PPT; however, this association did not translate to between-group difference in clinical pain outcomes [Citation71,Citation72].
Early clinical studies attempted to associate changes in hypoalgesia with clinical response following TM [Citation71,Citation77,Citation78]. Remote and local changes in PPT were not correlated with clinical SMT response in the short and medium term [Citation78]. This corroborates previous work finding minimal correlation between changes in pain sensitivity and clinical outcomes [Citation79]. Improved local hypoalgesia was identified following SMT in individuals with favorable outcomes regardless of the level of TM, while only SMT targeting the most painful segment was correlated with improved hypoalgesia irrespective of response [Citation71]. These findings suggest a segmental reflexive modulation response promoting the hypoalgesia [Citation71]. Current literature has failed to consistently identify factors associated with favorable OMT response. The overall lack of correlation between pain profile and clinical pain outcome suggests that nonspecific underlying factors such as a patient’s pain adaptability phenotype contribute to the analgesic response. Clinical research should investigate factors such as pain adaptability in an attempt to better identify those who will have a favorable response to OMT.
With the appropriate research, clinicians have the capacity to identify potential pain phenotypes in their clinical assessment
Preliminary observational work suggests that the early positive response is indicative of better long-term outcomes [Citation12,Citation80,Citation81]. In these studies, the authors have associated clinical characteristics identified early in the examination with improved outcomes at discharge and up to 6 months. Specifically, a 30% reduction of pain from baseline was identified with repeated posterior to anterior mobilizations, and this response led to a 2.5–5.0 increased odds of an improved outcome versus a lack of this finding. In each of the studies, OMT was a focus of the treatment approach, causing the authors to assume a link between the initial 30% and the ultimate clinical outcomes with an OMT treatment, as other influencing variables were not controlled. While these findings may appear promising, the studies failed to distinguish whether or not the early clinical findings are specific to OMT; at this point, the findings are purely prognostic. We hypothesize that the clinical characteristic identified early in the examination is related to the patient’s endogenous pain-modulating capacity. In other words, the positive outcome with an OMT approach depended on the individual patient with an amenable pain phenotype, a term known as pain adaptive behaviorCitation64,Citation65
To confirm the association of the aforementioned response with pain adaptive behavior, one would need to complete a concurrent validity study that includes both a clinical assessment and a laboratory-based exploration of one’s endogenous pain modulation. One can investigate endogenous pain modulation using the cold pressor test, which explores an individual’s ability to respond to sustained or repeated noxious stimuli locally by either decreasing sensitivity to the stimuli (adaptable) or increasing sensitivity (non-adaptable) [Citation64,Citation67]. If the adaptability and 30% change with the posterior–anterior mobilization are concurrent and strongly associated, it provides initial evidence of a proxy clinical measure for identifying pain adaptability. However, to explore whether this phenomenon is unique to OMT, one needs to go a step further and perform a responder analysis.
Typically, responder analyses are performed concurrently with a parallel, randomized controlled trial, in which patients are randomized to receive the treatment of interest or a comparator. A responder’s analysis involves identifying the number of responders in the treatment of interest group and comparing them to the number of responders who are in the comparison group [Citation82]. This design assumes a counterfactual comparator. Historically, researchers have identified percent or point change (or some other clinically important designations) as a milestone to identify whether someone was a responder or not. Unfortunately, this method is fraught with error.
The problem with a comparison of responders in parallel trials is that the counterfactual (the supposed comparison person in a parallel, randomized controlled trial) does not truly exist [Citation83]. A crossover trial, a design in which the same patient receives both treatments (a true counterfactual), is the only true way of determining treatment superiority. In this type of trial (), patients are randomized to either manual therapy or exercise as the first intervention, followed by a wash-out phase to remove the effects of that approach, before assessing the second intervention. An a priori determination of how strong of a difference between interventions is needed to determine who truly responded to one intervention and not another.
Figure 1. Cross-over trial needed for responder’s analyses.
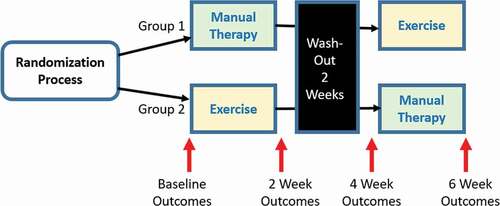
A cross-over trial is extremely difficult to do, and it is especially challenging with musculoskeletal conditions. The greatest change in patient-reported outcomes occurs very early in the care of the patient. Patients assigned to either manual therapy or exercise first will notably change in comparison to those assigned to the interventions second, and it is questionable whether an adequate interventional wash-out can occur. Cross-over trials require careful mathematical adjustments to the data to truly distinguish responders; otherwise, the order effect of the care received is likely the strongest effect that will be identified in the calculations.
Conclusion
We proposed that the likelihood of achieving a positive outcome with an OMT approach depends on the patient having an amenable pain phenotype. We provided evidence that mechanisms associated with an OMT technique are similar across pre-clinical animal and human studies. We identified studies that have characterized pain phenotypes based on treatment response, pain outcomes, and patient characteristics. These findings emphasize the value of patient-specific factors in clinical outcomes. We promote rather than attributing OMT effectiveness to the technique applied clinicians attribute the response to the patient’s pain phenotype and therefore modifications to the plan of care should be based on this concept. We proposed two research study designs needed to assess the value of a clinical examination approach toward identifying a pain phenotype construct and then identifying whether OMT leads to unique responses in that specific pain phenotype. Our suggested designs should help control against the well-known moderating and mediating variables of the patient and patient–clinician interactions associated with OMT [Citation11,Citation12]. Further research is needed to verify our suggestions, but we argue that these are the most important questions that require answering for OMT research.
Disclosure statement
Additional information
Funding
References
- Namnaqani FI, Mashabi AS, Yaseen KM, et al. The effectiveness of McKenzie method compared to manual therapy for treating chronic low back pain: a systematic review. J Musculoskelet Neuronal Interact. 2019;19(4):492–499.
- Cumplido-Trasmonte C, Fernández-González P, Alguacil-Diego IM, et al. Manual therapy in adults with tension-type headache: a systematic review. Neurol Engl Ed. 2021;36(7):537–547.
- Espí-López GV, Arnal-Gómez A, Balasch-Bernat M, et al. Effectiveness of manual therapy combined with physical therapy in treatment of patellofemoral pain syndrome: systematic review. J Chiropr Med. 2017;16(2):139–146.
- Lozano, J, López C, Mesa, JL, et al. Efficacy of manual therapy in the treatment of tension-type headache. A systematic review from 2000-2013. Neurología. 2016;31(6):357–369.
- Xu Q, Chen B, Wang Y, et al. The effectiveness of manual therapy for relieving pain, stiffness, and dysfunction in knee osteoarthritis: a systematic review and meta-analysis. Pain Physician. 2017;20(4):229–243.
- Lin I, Wiles L, Waller R, et al. What does best practice care for musculoskeletal pain look like? Eleven consistent recommendations from high-quality clinical practice guidelines: systematic review. Br J Sports Med. 2020;54(2):79–86.
- Bier JD, Wgm S-P, Staal JB, et al. Clinical practice guideline for physical therapy assessment and treatment in patients with nonspecific neck pain. Phys Ther. 2018;98(3):162–171.
- Oliveira CB, Maher CG, Pinto RZ, et al. Clinical practice guidelines for the management of non-specific low back pain in primary care: an updated overview. Eur Spine J. 2018;27(11):2791–2803.
- Pangarkar SS, Kang DG, Sandbrink F, et al. VA/DoD clinical practice guideline: diagnosis and treatment of low back pain. J Gen Intern Med. 2019;34(11):2620–2629.
- Blanpied PR, Gross AR, Elliott JM, et al. Neck Pain: revision 2017: clinical practice guidelines linked to the international classification of functioning, disability and health from the orthopaedic section of the American Physical Therapy Association. J Orthop Sports Phys Ther. 2017;47(7):A1–A83.
- George SZ, Fritz JM, Silfies SP, et al. Interventions for the management of acute and chronic low back pain: revision 2021: clinical practice guidelines linked to the international classification of functioning, disability and health from the academy of orthopaedic physical therapy of the American Physical Therapy Association. J Orthop Sports Phys Ther. 2021;51(11):1–60.
- Cook CE, Showalter C, Kabbaz V, et al. Can a within/between-session change in pain during reassessment predict outcome using a manual therapy intervention in patients with mechanical low back pain? Man Ther. 2012;17(4):325–329.
- Alonso-Perez JL, Lopez-Lopez A, La Touche R, et al. Hypoalgesic effects of three different manual therapy techniques on cervical spine and psychological interaction: a randomized clinical trial. J Bodyw Mov Ther. 2017;21(4):798–803.
- Plaza Manzano G, Delgado de la Serna P, Díaz Arribas MJ, et al. Influence of clinical, physical, psychological, and psychophysical variables on treatment outcomes in somatic tinnitus associated with temporomandibular pain: evidence from a randomized clinical trial. Pain Pract. 2021;21(1):8–17.
- Bishop MD, Mintken P, Bialosky JE, et al. Patient expectations of benefit from interventions for neck pain and resulting influence on outcomes. J Orthop Sports Phys Ther. 2013;43(7):457–465.
- Palmlöf L, Holm LW, Alfredsson L, et al. Expectations of recovery: a prognostic factor in patients with neck pain undergoing manual therapy treatment. Eur J Pain. 2016;20(9):1384–1391.
- Licciardone JC, Kearns CM, Minotti DE. Outcomes of osteopathic manual treatment for chronic low back pain according to baseline pain severity: results from the OSTEOPATHIC Trial. Man Ther. 2013;18(6):533–540.
- Mintken PE, Cleland JA, Carpenter KJ, et al. Some factors predict successful short-term outcomes in individuals with shoulder pain receiving cervicothoracic manipulation: a single-arm trial. Phys Ther. 2010;90(1):26–42.
- Nim CG, Downie A, O’Neill S, et al. The importance of selecting the correct site to apply spinal manipulation when treating spinal pain: myth or reality? A systematic review. Sci Rep. 2021;11(1):23415.
- Karas S, Olson Hunt MJ, Temes B, et al. The effect of direction specific thoracic spine manipulation on the cervical spine: a randomized controlled trial. J Man Manip Ther. 2018;26(1):3–10.
- Schomacher J. The effect of an analgesic mobilization technique when applied at symptomatic or asymptomatic levels of the cervical spine in subjects with neck pain: a randomized controlled trial. J Man Manip Ther. 2009;17(2):101–108.
- Aquino RL, Caires PM, Furtado FC, et al. Applying joint mobilization at different cervical vertebral levels does not influence immediate pain reduction in patients with chronic neck pain: a randomized clinical trial. J Man Manip Ther. 2009;17(2):95–100.
- Slaven EJ, Goode AP, Coronado RA, et al. The relative effectiveness of segment specific level and non-specific level spinal joint mobilization on pain and range of motion: results of a systematic review and meta-analysis. J Man Manip Ther. 2013;21(1):7–17.
- Baron R, Förster M, Binder A. Subgrouping of patients with neuropathic pain according to pain-related sensory abnormalities: a first step to a stratified treatment approach. Lancet Neurol. 2012;11(11):999–1005.
- Bartley EJ, Robinson ME, Staud R. Pain and fatigue variability patterns distinguish subgroups of fibromyalgia patients. J Pain. 2018;19(4):372–381.
- de Koning EJ, Timmermans EJ, van Schoor NM, et al. Within-person pain variability and mental health in older adults with osteoarthritis: an analysis across 6 European cohorts. J Pain. 2018;19(6):690–698.
- Baron R, Dickenson AH. Neuropathic pain: precise sensory profiling improves treatment and calls for back-translation. Pain. 2014;155(11):2215–2217.
- Edwards RR, Dworkin RH, Turk DC, et al. Patient phenotyping in clinical trials of chronic pain treatments: IMMPACT recommendations. Pain. 2016;157(9):1851–1871.
- Meints SM, Edwards RR, Gilligan C, et al. Behavioral, psychological, neurophysiological, and neuroanatomic determinants of pain. J Bone Jt Surg. 2020;102(Suppl 1):21–27.
- Young EE, Lariviere WR, Belfer I. Genetic basis of pain variability: recent advances. J Med Genet. 2012;49(1):1–9.
- Stamer UM, Stüber F. Genetic factors in pain and its treatment. Curr Opin Anaesthesiol. 2007;20(5):478–484.
- Rodeghero J, Wang YC, Flynn T, et al. The impact of physical therapy residency or fellowship education on clinical outcomes for patients with musculoskeletal conditions. J Orthop Sports Phys Ther. 2015;45(2):86–96.
- “What is a mechanistic study?” | NIH: National Institute of Allergy and Infectious Diseases. cited 2021 Dec 20. https://www.niaid.nih.gov/grants-contracts/what-mechanistic-study
- Bialosky JE, Beneciuk JM, Bishop MD, et al. Unraveling the mechanisms of manual therapy: modeling an approach. J Orthop Sports Phys Ther. 2018;48(1):8–18.
- Vigotsky AD, Bruhns RP. The role of descending modulation in manual therapy and its analgesic implications: a narrative review. Pain Res Treat. 2015;2015:1–11.
- Geri T, Viceconti A, Minacci M, et al. Manual therapy: exploiting the role of human touch. Musculoskelet Sci Pract. 2019;44:102044.
- Rabey M, Hall T, Hebron C, et al. Reconceptualising manual therapy skills in contemporary practice. Musculoskelet Sci Pract. 2017;29:28–32.
- Karas S, Mintken P, Brismée JM. We need to debate the value of manipulative therapy and recognize that we do not always understand from what to attribute our success. J Man Manip Ther. 2018;26(1):1–2.
- Oostendorp RAB. Credibility of manual therapy is at stake ‘Where do we go from here? J Man Manip Ther. 2018;26(4):189–192.
- Bialosky JE, Bishop MD, Price DD, et al. The mechanisms of manual therapy in the treatment of musculoskeletal pain: a comprehensive model. Man Ther. 2009;14(5):531–538.
- Voogt L, de Vries J, Meeus M, et al. Analgesic effects of manual therapy in patients with musculoskeletal pain: a systematic review. Man Ther. 2015;20(2):250–256.
- Roura S, Álvarez G, Solà I, et al. Do manual therapies have a specific autonomic effect? An overview of systematic reviews. PLOS ONE. 2021;16(12):e0260642.
- Haavik H, Niazi IK, Kumari N, et al. The potential mechanisms of high-velocity, low-amplitude, controlled vertebral thrusts on neuroimmune function: a narrative review. Medicina (Mex). 2021;57(6):536.
- Teodorczyk-Injeyan JA, Triano JJ, Gringmuth R, et al. Effects of spinal manipulative therapy on inflammatory mediators in patients with non-specific low back pain: a non-randomized controlled clinical trial. Chiropr Man Ther. 2021;29(1):3.
- Teodorczyk-Injeyan JA, Injeyan HS, Ruegg R. Spinal manipulative therapy reduces inflammatory cytokines but not substance p production in normal subjects. J Manipulative Physiol Ther. 2006;29(1):14–21.
- Lascurain-Aguirrebeña I, Newham D, Critchley DJ. Mechanism of action of spinal mobilizations: a systematic review. Spine (Phila Pa 1976). 2016;41(2):159–172.
- Singh AK, Zajdel J, Mirrasekhian E, et al. Prostaglandin-mediated inhibition of serotonin signaling controls the affective component of inflammatory pain. J Clin Invest. 2017;127(4):1370–1374.
- Viguier F, Michot B, Hamon M, et al. Multiple roles of serotonin in pain control mechanisms – implications of 5-HT7 and other 5-HT receptor types. Eur J Pharmacol. 2013;716(1–3):8–16.
- Wood PB. Role of central dopamine in pain and analgesia. Expert Rev Neurother. 2008;8(5):781–797.
- Rash JA, Aguirre-Camacho A, Campbell TS. Oxytocin and pain: a systematic review and synthesis of findings. Clin J Pain. 2014;30(5):453–462.
- Lima CR, Martins DF, Reed WR. Physiological responses induced by manual therapy in animal models: a scoping review. Front Neurosci. 2020;14:430.
- Arribas-Romano A, Fernández-Carnero J, Molina-Rueda F, et al. Efficacy of physical therapy on nociceptive pain processing alterations in patients with chronic musculoskeletal pain: a systematic review and meta-analysis. Pain Med. 2020;21(10):2502–2517.
- Bialosky JE, George SZ, Horn ME, et al. Spinal manipulative therapy–specific changes in pain sensitivity in individuals with low back pain (NCT01168999). J Pain. 2014;15(2):136–148.
- George SZ, Bishop MD, Bialosky JE, et al. Immediate effects of spinal manipulation on thermal pain sensitivity: an experimental study. BMC Musculoskelet Disord. 2006;7(1):68.
- Bialosky JE, Bishop MD, Robinson ME, et al. Spinal manipulative therapy has an immediate effect on thermal pain sensitivity in people with low back pain: a randomized controlled trial. Phys Ther. 2009;89(12):1292–1303.
- Pickar JG, Bolton PS. Spinal manipulative therapy and somatosensory activation. J Electromyogr Kinesiol. 2012;22(5):785–794.
- Bäckryd E, Persson EB, Larsson AI, et al. Chronic pain patients can be classified into four groups: clustering-based discriminant analysis of psychometric data from 4665 patients referred to a multidisciplinary pain centre (a SQRP study). Moitra E, ed. PLOS ONE. 2018;13(2):e0192623.
- Burri A, Hilpert P, McNair P, et al. Exploring symptoms of somatization in chronic widespread pain: latent class analysis and the role of personality. J Pain Res. 2017;10:1733–1740.
- Carlesso LC, Segal NA, Frey Law L, et al. Pain susceptibility phenotypes in those free of knee pain with or at risk of knee osteoarthritis: the multicenter osteoarthritis study. Arthritis Rheumatol. 2019;71(4):542–549.
- Carlesso LC, Tousignant-Laflamme Y, Shaw W, et al. Exploring pain phenotypes in workers with chronic low back pain: application of IMMPACT recommendations. Can J Pain. 2021;5(1):43–55.
- Kittelson AJ, Stevens-Lapsley JE, Schmiege SJ. Determination of pain phenotypes in knee osteoarthritis: a latent class analysis using data from the osteoarthritis initiative: identifying phenotypes of pain in knee OA. Arthritis Care Res. 2016;68(5):612–620.
- Vaegter HB, Graven-Nielsen T. Pain modulatory phenotypes differentiate subgroups with different clinical and experimental pain sensitivity. Pain. 2016;157(7):1480–1488.
- Obbarius A, Fischer F, Liegl G, et al. A step towards a better understanding of pain phenotypes: latent class analysis in chronic pain patients receiving multimodal inpatient treatment. J Pain Res. 2020;13:1023–1038.
- Zheng Z, Wang K, Yao D, et al. Adaptability to pain is associated with potency of local pain inhibition, but not conditioned pain modulation: a healthy human study. Pain. 2014;155(5):968–976.
- Licciardone JC, Gatchel RJ, Aryal S. Targeting patient subgroups with chronic low back pain for osteopathic manipulative treatment: responder analyses from a randomized controlled trial. J Osteopath Med. 2016;116(3):156–168.
- Pasquier M, Young JJ, Lardon A, et al. Factors associated with clinical responses to spinal manipulation in patients with non-specific thoracic back pain: a prospective cohort study. Front Pain Res. 2022;2:742119.
- Wan DWL, Arendt-Nielsen L, Wang K, et al. Pain adaptability in individuals with chronic musculoskeletal pain is not associated with conditioned pain modulation. J Pain. 2018;19(8):897–909.
- Krouwel O, Hebron C, Willett E. An investigation into the potential hypoalgesic effects of different amplitudes of PA mobilisations on the lumbar spine as measured by pressure pain thresholds (PPT). Man Ther. 2010;15(1):7–12.
- Bond BM, Kinslow CD, Yoder AW, et al. Effect of spinal manipulative therapy on mechanical pain sensitivity in patients with chronic nonspecific low back pain: a pilot randomized, controlled trial. J Man Manip Ther. 2020;28(1):15–27.
- Fernández-Carnero J, Cleland JA, Arbizu RLT. Examination of motor and hypoalgesic effects of cervical vs thoracic spine manipulation in patients with lateral epicondylalgia: a clinical trial. J Manipulative Physiol Ther. 2011;34(7):432–440.
- Nim CG, Weber KA, Kawchuk GN, et al. Spinal manipulation and modulation of pain sensitivity in persistent low back pain: a secondary cluster analysis of a randomized trial. Chiropr Man Ther. 2021;29(1):10.
- Coronado RA, Gay CW, Bialosky JE, et al. Changes in pain sensitivity following spinal manipulation: a systematic review and meta-analysis. J Electromyogr Kinesiol. 2012;22(5):752–767.
- Millan M, Leboeuf-Yde C, Budgell B, et al. The effect of spinal manipulative therapy on experimentally induced pain: a systematic literature review. Chiropr Man Ther. 2012;20(1):26.
- Aspinall SL, Leboeuf-Yde C, Etherington SJ, et al. Manipulation-induced hypoalgesia in musculoskeletal pain populations: a systematic critical review and meta-analysis. Chiropr Man Ther. 2019;27(1):7.
- Aspinall SL, Jacques A, Leboeuf-Yde C, et al. Pressure pain threshold and temporal summation in adults with episodic and persistent low back pain trajectories: a secondary analysis at baseline and after lumbar manipulation or sham. Chiropr Man Ther. 2020;28(1):36.
- Aspinall SL, Jacques A, Leboeuf-Yde C, et al. No difference in pressure pain threshold and temporal summation after lumbar spinal manipulation compared to sham: a randomised controlled trial in adults with low back pain. Musculoskelet Sci Pract. 2019;43:18–25.
- Nim CG, Kawchuk GN, Schiøttz-Christensen B, et al. Changes in pain sensitivity and spinal stiffness in relation to responder status following spinal manipulative therapy in chronic low back pain: a secondary explorative analysis of a randomized trial. BMC Musculoskelet Disord. 2021;22(1):23.
- Aspinall SL, Leboeuf-Yde C, Etherington SJ, et al. Changes in pressure pain threshold and temporal summation in rapid responders and non-rapid responders after lumbar spinal manipulation and sham: a secondary analysis in adults with low back pain. Musculoskelet Sci Pract. 2020;47:102137.
- Coronado RA, Bialosky JE, Bishop MD, et al. The comparative effects of spinal and peripheral thrust manipulation and exercise on pain sensitivity and the relation to clinical outcome: a mechanistic trial using a shoulder pain model. J Orthop Sports Phys Ther. 2015;45(4):252–264.
- Cook C, Lawrence J, Michalak K, et al. Is there preliminary value to a within- and/or between-session change for determining short-term outcomes of manual therapy on mechanical neck pain? J Man Manip Ther. 2014;22(4):173–180.
- Tuttle N. Do changes within a manual therapy treatment session predict between-session changes for patients with cervical spine pain? Aust J Physiother. 2005;51(1):43–48.
- Cates C, Karner C. Clinical importance cannot be ruled out using mean difference alone. Bmj. 2015;351(nov20 4):h5496–h5496.
- Henschke N, van Enst A, Froud R, et al. Responder analyses in randomised controlled trials for chronic low back pain: an overview of currently used methods. Eur Spine J. 2014;23(4):772–778.