
ABSTRACT
Teaching hypothetico-deductive clinical reasoning (CR) should be an essential part of the physiotherapy education system, but currently there are very few learning tools for teachers in the musculoskeletal discipline. The aim of this article was to describe and present the rules of a new game-based and structured didactic tool that can be used by teachers for ‘players’ (students and licensed clinicians) to learn systematic CR in musculoskeletal physiotherapy.
Our tool is based on the ‘Happy Families’ card game, and we propose to use it as part of a classic musculoskeletal subjective examination-based hypothesis category framework and the International Classification of Functioning, Disability and Health model. It allows players to dynamically formulate hypotheses from clinical case studies. Each 'Family' of cards represents a hypothesis category. The game highlights the missing information and trains players to consider it in their CR.
This game should efficiently structure all components of CR and is an interesting resource for all teachers. Its greatest strength is that it can be used with other category frameworks. Further studies are needed to assess the efficacy and efficiency of such a tool and to measure students’ actual progress in learning the CR.
Introduction
Clinical reasoning (CR) can be defined as a reflective process of inquiry and analysis undertaken by a health professional in collaboration with the patient or client with the aim of understanding the person, their context and their clinical problem(s) in order to guide evidence-based practice [Citation1]. The key points of this definition are that CR involves processes of both investigation (e.g. physiotherapy examination) and analysis, and that it is not a one-way process but requires collaboration between the patient and their physiotherapist (PT). While a key aim is to understand the patient’s health problem, PT treatment also requires an assessment and understanding of the patient’s personal circumstances (e.g. attitude/expectations and beliefs), and any psychosocial factors that may contribute to their problem.
CR is an essential competency to develop in PT practice [Citation2–4] and its learning develops over time in PT education programmes [Citation5] but remains a challenge for students throughout their curriculum. Research and theory of CR across the health professions, including physiotherapy [Citation6], suggest CR should occur throughout the examination and ongoing patient management. Indeed, PTs use CR from the moment they review patient records and get to know the patient, through assessment, treatment, and monitoring of treatment outcomes. This includes perception of potentially relevant information, interpretation and synthesis of information to make clinical judgments about the person, their health problem and best practice management. CR is often described as involving non-analytic and analytic processes [Citation7–11]. The principle non-analytic process used is intuition (e.g. recognizing problems and solutions without conscious awareness) and is ineffective by itself, especially for students learning PT. In contrast, conscious pattern recognition of problems, causes and solutions learned through theoretical knowledge (e.g. clinical features of common clinical problems and research evidence of best practice) and clinical experience, is a characteristic of expert clinical practice when engaged with familiar presentations [Citation6]. There are multiple methods for approaching CR (e.g. pattern recognition, schema group diagnostics of pathophysiology and/or causality) [Citation12], but the variations and complexity of real patient presentations require that students are concurrently taught a hypothetico-deductive analytic reasoning process that involves generating and testing hypotheses rather than relying solely on pattern recognition [Citation4,Citation7,Citation13,Citation14]. In this way, the analysis of the subjective examination (questioning the patient about their health problem and personal circumstances) guides the planning of the physical examination. Analysis of the complete examination guides the overall management and selection of specific therapeutic interventions. The effects of all treatments are evaluated to determine their effectiveness and guide further management. In other words, the hypothesis-oriented CR process is applied from the beginning of the patient examination and through each treatment that is administered.
Understanding the person, their context and their clinical problem(s) to guide evidence-informed management requires a range of clinical judgments. While there is no definitive list of essential clinical judgments, some authors have proposed a ‘hypothesis category framework’ identifying broad categories of clinical judgment in PT that have evolved through professional discussion to their latest version [Citation14]. There is research evidence on the focus of musculoskeletal clinicians CR, including reasoning across and within these different categories [Citation4,Citation15–19]. In conjunction with the reflective discourse of experienced clinicians and clinical educators, the relevance and use of these specific hypothesis categories is widely supported [Citation4,Citation14–17,Citation20]. Nevertheless, because they are the result of a dynamic thought process based on scientific evidence and clinical needs, these specific hypothesis categories are not recommended for uncritical use in educational programs [Citation12]. Rather, they are cited as an example of a structured framework of clinical judgments that can help PT students and clinicians reflect and learn CR. Educational programs are encouraged to adopt the categories of clinical judgment that are consistent with the philosophy of practice and the clinical judgments they consider important.
Learning theories of clinical reasoning
There are a variety of theories about the learning process [Citation21]. Two broad learning theories relevant to CR are the cognitivist and the socio-constructivist learning theories [Citation22,Citation23]. These frameworks provide a pedagogical rationale upon which PT education can be built to facilitate understanding and skilled application of CR [Citation24].
Cognition and metacognition are central to the learning theory of cognitivism. Indeed, learning CR, both for the hypothetico-deductive process and pattern recognition, requires cognition [Citation25–28].
Cognition in CR begins with the perception of what is relevant. Perception is closely related to knowledge and involves recognizing potentially relevant cues from medical records/reports and patient information (verbal and non-verbal) obtained directly from questioning and physical examination. A student’s reasoning may be limited solely by an inability to recognize important information. Specific patient information perceived as potentially relevant must then be interpreted for meaning and significance. Since individual pieces of information rarely provide definitive answers, it is best if these interpretations, or inferences, are not absolute but are formulated as hypotheses in the therapist’s analysis. As more information is obtained through questioning (subjective examination) and testing (physical examination), it must be synthesized. Synthesizing information is a higher level of cognition that involves the amalgamation of information that is analyzed for what it tells you when considered collectively. For example, a patient may report joint pain as the main symptom, but further examination reveals less bothersome pains in other joints that when considered (analyzed) together, may elicit a hypothesis of a broader systemic process affecting multiple joints. Sometimes the information collected is simply to get a full picture of the person’s problems, symptoms, and history, that is you are conducting a structured examination. At other times, you collect information with a specific hypothesis in mind. In this case we call this a form of ‘hypothesis testing’. This form of purposeful assessment (questioning or physical examination) is another example of how cognition plays a role in CR.
Metacognition or self-awareness is the ability to reflect and critique oneself in the moment and in hindsight. For example, an experienced therapist can immediately recognize if they have not phrased a question clearly. Similarly, they can detect when a physical procedure has not been done well, for example, if the grip was not comfortable, and immediately adjust or repeat the procedure. It is also important to have a metacognitive awareness of one’s own knowledge. This leads the experienced therapist to investigate immediately if they do not know something (e.g. a medication they are not familiar with).
Metacognition is necessary for therapists to be able to ‘think on their feet’ and modify their analysis and assessment or treatment in response to that analysis in real time [Citation29]. During PT education, students receive regular formative and summative assessments and feedback to facilitate learning. However, when they graduate, this level of supervision will no longer be available. Therefore, it is important that they develop their metacognitive abilities during their PT education. Metacognition can then be described as the conscious engagement with problem solving in the hypothetico-deductive process through reflection and critique of one’s reasoning and performance through the patient examination and treatment. It helps the student improve their application of CR theory to practice [Citation30]. Strategies for facilitating metacognition include instruction in CR theory and practice (e.g. through case studies in the classroom and real patients in the clinic) combined with feedback. Feedback on CR through a case, and not simply at the end of the case, is important to facilitate students’ ability to metacognitively think on their feet as information unfolds. There are numerous methods for eliciting reflection in the moment including thinking aloud protocols, reflection worksheets, self-explanation methods, and judgment comprehension assignments [Citation28].
Although the construction of knowledge is something personal, it also takes place within a social framework. The social and cultural environment in learning is therefore important. Supported by socio-constructivist learning theory [Citation31,Citation32], learning and motivation to learn are enhanced by exchanges within and between groups that lead to social interaction and interactions with peers (players) [Citation23]. It is interesting to note that social learning is an index of students’ ability to make their own decisions [Citation22] and therefore facilitates the autonomy needed when PT students graduate.
While there is now considerable literature on the teaching and learning of CR (e.g [Citation6]), there is no gold standard [Citation6,Citation33]. The activities perceived by students and teachers as most effective in facilitating CR learning were patient management demonstrations, discussions, feedback and evaluation [Citation22]. These activities can also provide the mentor with valuable strategies to optimize the student’s CR proficiency required of a new graduate and the metacognitive capability required for lifelong learning without continual supervision. The method used should create different learning situations necessary to learn to distinguish and then analyze clinically important elements in a patient presentation. Distinguishing important elements involves perceiving relevant information; interpretation and synthesis of information into hypotheses related to understanding of the patient, their context and their clinical problem(s) [Citation34]. To carry out these activities, a variety of tools, both individual and group, have been proposed to develop the complex cognitive and metacognitive processes necessary to learn CR in a hypothetico-deductive mode. By providing novices with a systematic means of gathering information to guide CR and reflection, these tools can assist to facilitate their formulation of hypotheses based on patient information and to test alternative competing hypotheses during further examination and treatment. Examples of such tools include ‘SCRIPT’ and ‘The Physical Therapy Clinical Reasoning and Reflection Tool’ [Citation35,Citation36]. In a world driven by digitalization, game-based learning has demonstrated educational value [Citation37] in health professions’ education [Citation38] consistent with cognitive and socio-constructivist learning theories [Citation38] by, for example, promoting students’ enjoyment of active learning and engagement [Citation38] and stimulating students’ attention [Citation39]. ‘Serious Games’ are specific types of game-based learning which are specially developed to learn something or to achieve a specific learning outcome [Citation40–42]. In this context, learning CR through Serious Games [Citation43,Citation44] and simulation web games [Citation45,Citation46] have already been successfully used in nursing education. The good acceptance of Serious Games by nursing students [Citation43] and medical students [Citation47] may justify the use of Serious Games in PT education.
For our team, it was therefore necessary to develop a tool that maintains the necessary learning objectives such as enjoyment of the learning activity, facilitation and development of cognition and metacognition, and integration of feedback obtained through the interaction between players and teachers. All this aims to promote the clinical attitudes required in a real situation [Citation22,Citation24,Citation26,Citation48,Citation49]. We then developed a new tool that has all the characteristics mentioned above and provides a structured educational framework for teaching PT students or PT’s in post-professional education. This tool is based on the card game ‘Happy Families’. To develop the stated learning objectives integrated to the ‘Hypothesis Family Game’, this lends itself as a variation of the aforementioned tools with a dimension of fun and enjoyment that are fundamental aspects of learning [Citation50,Citation51], integrated to enhance the didactic learning activities provided to improve musculoskeletal students practice in learning CR [Citation52].
The game is comprehensive and structured based on existing models that have been already taught such as the framework of the hypothesis categories and the International Classification of Functioning, Disability and Health (ICF) [Citation53] and the International Federation of Orthopaedic Manipulative Physical Therapists (IFOMPT) educational standards [Citation20].
Description and rules of the hypothesis families card game
'Happy Families'
Our ‘Happy Families’ is based on a traditional card game and one of the most played in Europe. In The Netherlands, Germany and Austria, the game is known as ‘Kwartet’, ‘Quartett’ or ‘Ablegspiel’ respectively and in the United States of America as ‘Go Fish’. The original game is usually composed of a specially made set of picture cards, featuring illustrations of fictional images, or different ‘families’, and within each 'Family' four to eight cards. The object of the game is to collect as many as possible complete and accurate families.
Here, we create our own 'Happy Families' card game to learn CR in musculoskeletal PT. The game involves progressive presentation of information from the patient characteristics and subjective examination of a clinical case for students to practice formulating and revising hypotheses. The information given about the clinical case can vary, ranging from little information to a lot. In addition, the estimated level of difficulty of the clinical case is also variable, ranging from less to greater complexity, according to the players’ (e.g. students’) stage of education. While the overarching purpose of the 'Happy Families' learning activity is to facilitate participants’ CR and associated knowledge construction, specific thinking and learning skills to be emphasized should be considered. Learning objectives should be specific to the activity. There are numerous possibilities including specific critical thinking skills such as identifying or critiquing the questions and assessments required to understand the clinical presentation; recognizing what information is important for each category of clinical judgment being considered; understanding key concepts underpinning the different clinical judgments (e.g. essential biomedical and psychosocial concepts related to pain and disability); recognizing and challenging assumptions made in information presented and analyses made; recognizing viewpoints considered in the presentation and analysis and alternative viewpoints; and critiquing the logic and validity of analyses. Learning objectives could also be framed around students’ abilities to demonstrate application of core CR processes such as: perception of potentially relevant information; clarity and thoroughness of questioning to obtain an accurate and complete overview of the clinical presentation; ability to generate logical hypotheses regarding the problem, its management and the prognosis; ability to modify hypotheses as information unfolds; ability to translate judgments in one category of analysis (e.g. problem classification, safety considerations) to other categories of judgment (e.g. implications to management and prognosis). Regardless of which of these many skills are targeted, the designer of the game case should be explicit regarding what they want to achieve and integrate that into specific learning objectives with criteria for how each objective will be evidenced.
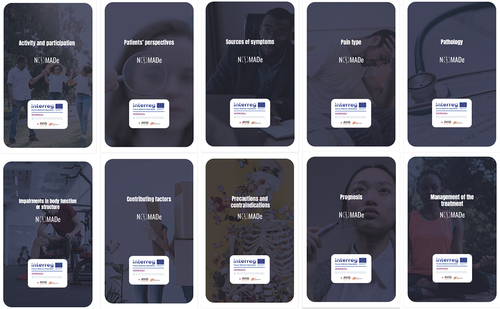
The specific categories of clinical judgment to use (e.g. from the hypothesis categories framework or others), like the learning and reasoning skills options discussed above, is not fixed and teachers are free to use any categories of clinical judgment they feel are important to clinical practice as promoted in their curriculum or area of practice. In the card game, facilitated by a simple visual presentation, each ‘Family’ represents a single hypothesis category (). This allows students to be explicit regarding the category of clinical judgment they are formulating a hypothesis about. Information from the patient’s case may also elicit hypotheses in one or more categories, such as severity, irritability, nature, stage, and stability (SINSS concept), which would have implications for precautions and contraindications, management and prognosis [Citation54]. Requiring students to be explicit in the basis for their hypotheses allows for feedback on the accuracy of hypotheses and associated rationale. Relevance of key information missed, such as SINNS or a red flag can be addressed in feedback [Citation54]. It is essential that the Families of hypotheses used are defined beforehand by the teacher, for example during a theoretical course with explanation and discussion regarding each category of clinical judgment teachers want students to be able to formulate and what patient information assist in making each judgment. To be more explicit, we propose here to use the categorical hypotheses described by Jones and Rivett [Citation14], based on subjective and physical investigations. These include 10 categories (named 'Family' in our card game) related to the patient’s biopsychosocial sphere, with: (a) Activities and participation, (b) Psychosocial ('Patients’ perspectives' in this version of the card game), (c) Source of the symptoms or dysfunction, (d) Pain type, (e) Pathology, (f) Impairments in body function or structure, (g) Contributing factors, (h) Precautions and contraindications to examination and treatment, (i) Management of the treatment, and (j) Prognosis.
Figure 1. Illustration of Families of hypotheses on the back of which students can write their hypotheses. An example played is available in .
The rules
The game can be played in a traditional small group class or workshop. Starting with an oral [Citation55,Citation56] or written [Citation57,Citation58] clinical case proposed by the teacher or by the students once they are familiar with the essential components of information to include in a case presentation and have learned the procedure and rules of the game. At a minimum, each clinical case should include the patient characteristics (age, work, living circumstances), subjective examination, main problem, description and location of associated symptoms; behavior of symptoms (e.g. activity and participation restrictions and capabilities with details regarding aggravating factors, easing factors, night, daily pattern); general health and red flag screening, history of present complaint; past medical history; psychosocial screening (e.g. understanding/beliefs, expectations/goals, distress and relationship to symptoms, coping strategies, etc.).
The basic rules are as follows. Based on the information contained in the clinical case, the group of interacting students then selects the cards representing the ‘Families of Hypotheses’ to list their specific case hypotheses for each of the families as understood from their prior learning (). This list is written on the back of the cards. The rationale for each hypothesis (possible explanatory elements/logic of the chosen hypothesis) should be based on the information in the case and associated theoretical concepts (e.g. pain mechanisms, biomechanics, etc.). The students also indicate which of the hypotheses considered in each 'Family'/hypothesis category they consider their primary (i.e. first choice) hypothesis at this stage. This judgment should then guide their plan for physical examination and management. For example, a hypothesis regarding motor control as a potential contributing factor would guide prioritization of this in the physical examination and early consideration of targeting this in management depending on its assessment. Secondary hypotheses regarding diagnosis (e.g. pathology, syndrome, source of symptoms) will typically also be considered in the physical examination as part of a ‘differential diagnosis’. Reasoning about management would need to take into consideration different classification systems [Citation59], expected physical findings for the systems used, clinical practice guidelines and how the guideline would need to be tailored to the patient’s individual presentation.
Once all hypotheses have been indicated, a group of students can present their reasoning on each of the hypothesis families to another(other) group(s) of participants and take questions from classmates regarding their analysis. This process can be conducted with either two groups of students presenting their reasoning on the same clinical case or groups can work on different cases to present and discuss. A small group of students per course/workshop/tutorial can ensure the efficiency of discussions between groups during group presentations. During the game, discussion and feedback with other players allow players to reflect and critique chosen hypotheses and rationale. The game ends when the player(s) and the teacher have gone through all the possible hypotheses together. In our experience, the best number of students to play for a clinical case study seems to be between three and five students per group. For the time needed, we also recommend that the instructor set aside two consecutive hours to play. The first hour should be dedicated to discussion and filling in the cards/families within each group, and the second hour should be dedicated to each group presenting the hypothesized families to the other students in the class. This second hour is important because it allows for discussion among students and staff providing opportunity for the presenters to be challenged on their clinical judgments and rationale and feedback regarding alternative analyses. An example of clinical case study played is given in . The students were given the following characteristics and subjective examination about the patient. The patient is a 50-year-old man, married. He has been experiencing neck pain for the past 4 months for no apparent reason. This is not the first episode of neck pain, but it has never lasted this long, indeed similar episodes resolved within 2 or 3 days without any treatment. Furthermore, he could not recall any change in his lifestyle or work position that might have explained this episode or prolonged it beyond normal. He went to the general practitioner (GP) 3 days ago. The GP wrote him a prescription for PT. The GP told the patient that he needed an MRI if conservative treatment did not work. GP prescribed him nonsteroidal anti-inflammatory drugs but the patient is not taking them. The patient continues to work in a desk job (sitting but he can adjust the height of his chair and tries to stand up frequently). Nights are restless, but the patient does not know if he wakes up by moving or if the pain wakes him up spontaneously. The patient wakes up and getting up is very painful. During the day, the pain is more tolerable. In the evening, the patient finds it difficult to stay in the chair and watch television. The patient's pain is mainly caused by head extension and turning the head to the left side more than to the right side. The patient rates the average pain intensity on a numerical scale from 0 (no pain) to 10 (the worst pain imaginable): neck and arm pain at 3/10 and forearm pain at 1/10 and acute pain at 7/10 and forearm pain at 5/10. Active movements of the neck cause pain that lasts for a few seconds. The patient has no other comorbidities and no weight loss was reported. He has not experienced dizziness, nausea or tinnitus. He has not noticed any alteration in gait or dexterity. He has not noticed any decrease in strength when using his right hand and no history of accidents or fractures. The patient considers himself in good physical and mental health and exercises 3 times a week: in the fitness room and jogging. The patient considers his neck problem as something ”not serious” but does not provide any information on what he thinks the problem is: ”he doesn't know”.
Figure 2. a. Body chart of the clinical case study played in b. On the body chart, next to the site “1” are written: ”constant”, ”variable”, ”deep” and next to the site “2” are written: ”not constant”, ”deep”, ”tingling”, ”numbness”. ”√” means that the patient does not mention any symptoms in these body areas. b. Example of clinical case study played by a group of students, with initial case hypotheses and brief notations of rationale for each of the 10 families of hypotheses. Note that the hypotheses for some families are arranged in a kind of decision tree. The clinical case example presented is not intended to show the only correct way to present a clinical case to students. Indeed, we leave it up to each teacher to construct his or her case as he or she sees fit, for example by deliberately omitting information’s (this depends on what the teacher wants to develop as learning for the students).
The simplicity of the rules of the game gives the teacher opportunity to adapt the complexity of the case and organization of the groups to suit the student group and class size. For a shorter option, the teacher can proceed with the subjective examination of the clinical case in a progressive way, deciding on the information to be distilled, and stopping, depending on the time available, at any stage of the subjective examination for the students to propose their hypotheses for the families of hypotheses the teacher wants to focus on. According to the time available, the teacher may also decide to address only one section of the subjective examination, e.g. the body chart, and ask the students for the families of hypotheses related to that. Even a single section of the subjective examination such as this can provide opportunity for formation and discussion of hypotheses from different families such as ‘pain type/mechanisms’, ‘precautions/contraindications’, and ‘potential sources of symptoms’.
The rules can be adapted to any level of learning or area of PT practice with learning objectives adjusted accordingly. For example, for students who are just learning CR, the playing cards can be already pre-filled with hypotheses. In this way, students only need to select the correct ones.
Evaluating clinical reasoning of players
At this stage, effectiveness of the game as a learning activity for CR has not been evaluated beyond internal survey of students (see ). Nevertheless, the importance of formative evaluation and feedback to student learning is well established [Citation61,Citation62] and therefore must be incorporated through the game. The feedback can address any aspect of the students’ CR such as their applied understanding of the hypothesis families, their recognition of incomplete information, their hypotheses and rationale, their knowledge of essential theoretical concepts inherent in the case, etc. How much discussion and feedback through the case versus at the end of the case, or even at a second session when treatment information might be presented, is at the discretion of the teacher.
Figure 3. Results of the internal survey. For illustrative purposes only, we present a pilot survey of student feedback on the 'Happy Families' game. This feedback was conducted opportunistically during a class session. The evaluation of this session was based on a questionnaire (ASPECT) developed by [Citation60]. The survey aims to assess students’ perspective on their engagement in an active-learning classroom. Twenty-seven physiotherapists in post-professional training (“OMT students”) used the game during an CR activity supervised by two teachers (RH & AF). In general, this assessment reveals the importance of group interactions and the key role of the teacher(s), in mastering the game and being helpful without being intrusive. In addition, the implementation of the game seems to have increased the students’ attractiveness for the subject concerned, i.e. CR. These results and their interpretation need to be nuanced as the evaluation was conducted on a heterogeneous group of PT students, without any inclusion and exclusion criteria, such as their relationship with games, gender, culture or professional experience. The survey items were: Q1: The instructor enthusiasm made me more interested in the activity, Q2: The topic activity increased my understanding of the clinical reasoning, Q3: The instructor put a good deal of effort into my learning for today's class, Q4: I had fun during today's 'Happy Families' group activity, Q5: Overall, the other members of my group made valuable contributions during the 'Happy Families' activity, Q6: The instructor seemed prepared for the 'Happy Families' activity, Q7: I would prefer to take a class that includes this 'Happy Families' activity over one that does not include today's group 'Happy Families' activity, Q8: I'm confident in my understanding of the material presented during today's 'Happy Families' activity, Q9: I made a valuable contribution to my group today, Q10: The instructor and assistants were available to answer questions during the 'Happy Families' activity, Q11: The 'Happy Families' activity increased my understanding of the clinical reasoning, Q12: I was focused during today's 'Happy Families' activity, Q13: The 'Happy Families' stimulated my interest in clinical reasoning, Q14: I worked hard during today's 'Happy Families' activity .
![Figure 3. Results of the internal survey. For illustrative purposes only, we present a pilot survey of student feedback on the 'Happy Families' game. This feedback was conducted opportunistically during a class session. The evaluation of this session was based on a questionnaire (ASPECT) developed by [Citation60]. The survey aims to assess students’ perspective on their engagement in an active-learning classroom. Twenty-seven physiotherapists in post-professional training (“OMT students”) used the game during an CR activity supervised by two teachers (RH & AF). In general, this assessment reveals the importance of group interactions and the key role of the teacher(s), in mastering the game and being helpful without being intrusive. In addition, the implementation of the game seems to have increased the students’ attractiveness for the subject concerned, i.e. CR. These results and their interpretation need to be nuanced as the evaluation was conducted on a heterogeneous group of PT students, without any inclusion and exclusion criteria, such as their relationship with games, gender, culture or professional experience. The survey items were: Q1: The instructor enthusiasm made me more interested in the activity, Q2: The topic activity increased my understanding of the clinical reasoning, Q3: The instructor put a good deal of effort into my learning for today's class, Q4: I had fun during today's 'Happy Families' group activity, Q5: Overall, the other members of my group made valuable contributions during the 'Happy Families' activity, Q6: The instructor seemed prepared for the 'Happy Families' activity, Q7: I would prefer to take a class that includes this 'Happy Families' activity over one that does not include today's group 'Happy Families' activity, Q8: I'm confident in my understanding of the material presented during today's 'Happy Families' activity, Q9: I made a valuable contribution to my group today, Q10: The instructor and assistants were available to answer questions during the 'Happy Families' activity, Q11: The 'Happy Families' activity increased my understanding of the clinical reasoning, Q12: I was focused during today's 'Happy Families' activity, Q13: The 'Happy Families' stimulated my interest in clinical reasoning, Q14: I worked hard during today's 'Happy Families' activity .](/cms/asset/962bbc0b-ce95-4b74-a911-dafe5c2bfabb/yjmt_a_2132346_f0003_oc.jpg)
Discussion and conclusion
CR is now recognized as an essential competency in health professions education necessitating explicit instruction, practice and feedback to assist students to learn this important skill [Citation6]. Based on a hypothetico-deductive framework of CR combined with a framework of different categories of hypotheses considered important to PT clinical reasoning [Citation14], and situated within cognitivist and socio-constructivist learning theories [Citation22,Citation23], we have described a new learning activity to facilitate students’ CR called the 'Happy Families' game. The game follows the familiar format of a case study discussion with the main difference being it is run as a game. It aims to assist learners to develop their CR proficiency through analysis of the subjective and physical examinations of a given patient. To help learners develop adaptive expertise, teachers need to help them recognize and adapt their diagnostic approach to the clinical scenario and become familiar with clinical uncertainty [Citation63]. Systematic CR should be actively taught to students within a skill-teaching framework and as they progress through their studies [Citation64]. Our new learning tool meets these principles because it can be used and easily integrated into any musculoskeletal PT curriculum, beginning in the early years.
The logistics of its potential implementation in an educational setting would depend on the existing curriculum and pedagogy. For example, it requires students receive explicit instruction in CR theory, ideally linked to frameworks such as the biopsychosocial model, hypothetico-deductive reasoning and pattern recognition, and consideration of essential categories of judgment. Teachers running the 'Happy Families' game similarly need to be familiar with the theory of CR plus have skills in small group teaching, facilitating students’ reasoning and feedback. It is not possible to stipulate the optimal frequency or duration of the activity but our experience shows a use of two clinical cases per quadrimester played with the game has been effective. In addition, this game can be used in different formats. The online development of the card game in the form of a website, named the SCALENEo project, is currently being planned and funded by the European Erasmus+ programme.
The greatest weakness of the card game is that its use can be compromised if students are not familiar with hypothetical-deductive CR process and its greatest strength is that it can focus on any aspect of reasoning or category of judgment and can be used in education of any area of PT practice. The learning process in the form of a structured ‘Happy Families’ card game should effectively promote the structured component of CR. As a reminder, it is based on an active learning process that could support the learning process leading up to the formative and certificate-based assessments. For the certificated level, further work developing a specific scoring system must be planned and tested among students. At this stage, this card game seems to be a promising tool to engage students in CR learning and improve awareness of cognitive biases and the use of reflective practice [Citation65].
Evaluation of the efficacy, efficiency, playability and the enjoyment of this new learning tool, of course, remains to be tested. We have yet to demonstrate that it is sensitive to measuring actual student learning progress. In addition, the long-term benefit of CR learning needs to be assessed. One approach would be to develop an evaluation tool that includes criteria for assessing thinking and reasoning. It seems that these criteria would be relevant for assessing students’ reasoning performance with the card game. Another important point when using the game is the quality of the clinical cases proposed by the teacher. This topic is outside the scope of this paper. However, it is the teacher’s responsibility to propose high fidelity clinical cases containing relevant (or even deliberately erroneous) information and in line with their level of development of CR (from basic to expert level) in order to optimize learning. In this perspective, learner progression is an important aspect, and we recommend using the five categories of Hendrick et al. (e.g. category B for our clinical case example) to prepare the clinical case studies [Citation66]. These latter may be based on the World Health Organization’s ICF model as a guiding framework [Citation67] to gain in quality.
Supplemental Material
Download MS Word (214.6 KB)Supplemental Material
Download MS Word (4 MB)Disclosure statement
No potential conflict of interest was reported by the author(s).
Supplementary material
Supplemental data for this article can be accessed online at https://doi.org/10.1080/10669817.2022.2132346.
Additional information
Funding
References
- Harris P, Nagy S, Vardaxis N. Mosby's dictionary of Medicine, Nursing and Health Professions, 3rd ed. Edinburgh: Mosby Elsevier; 2014;379.
- Parodis I, Andersson L, Durning SJ, et al. Clinical reasoning needs to be explicitly addressed in health professions curricula: recommendations from a European consortium. Int J Environ Res Public Health. 2021;18(21): 11202.
- Ajjawi R, Smith M. Clinical reasoning capability: current understanding and implications for physiotherapy educators. FOHPE. 2010;12(1):60–73.
- Edwards I, Jones M, Carr J, et al. Clinical reasoning strategies in physical therapy. Phys Ther. 2004;84(4):312–330.
- Wainwright SF, Gwyer J. How can we understand the development of clinical reasoning? J Phys Ther Educ. 2017;31(1):4–6.
- Higgs J, Jensen G, Loftus S, et al. Clinical reasoning in the health professions. 4th ed. Edinburgh: Elsevier; 2019.
- Jones MA. Clinical reasoning in manual therapy. Phys Ther. 1992;72(12):875.
- Croskerry P. Clinical cognition and diagnostic error: applications of a dual process model of reasoning. Adv Health Sci Educ Theory Pract. 2009;14 Suppl 1(S1):27–35.
- Croskerry P. A universal model of diagnostic reasoning. Acad Med. 2009;84(8):1022–1028.
- Kahneman DT. Fast and Slow. London: Allen Lane; 2011.
- Marcum JA. An integrated model of clinical reasoning: dual-process theory of cognition and metacognition. J Eval Clin Pract. 2012;18(5):954–961.
- Jones M, Edwards I, Jensen G. Clinical reasoning in physiotherapy. In: Higgs J, Jensen G, Loftus S Christensen N, editors. Clinical reasoning in the health professions. 4th ed. Edinburgh: Elsevier; 2019. pp. 247–260.
- Bowen JL. Educational strategies to promote clinical diagnostic reasoning. N Engl J Med. 2006;355(21):2217–2225.
- Jones M, Rivett D. Clinical reasoning in musculoskeletal practice. 2nd ed. Edinburgh: Elsevier; 2019.
- Smart K, Doody C. The clinical reasoning of pain by experienced musculoskeletal physiotherapists. Man Ther. 2007;12(1):40–49.
- Barlow S. Physiotherapy outpatient’s chronic pain management: realizing the potential. Health Education and Training Institute, NSW Government; 2012.
- Jensen G, Hack L, Gwyer J, Shepard, K. Expertise in physical therapy practice. 2nd ed. St Louis: Saunders Elsevier; 2007.
- Doody C, McAteer M. Clinical reasoning of expert and novice physiotherapists in an outpatient orthopaedic setting. Physiotherapy. 2002;88(5):258–268.
- Rivett DA, Higgs J. Hypothesis generation in the clinical reasoning behavior of manual therapists. J Phys Ther Educ. 1997;11(1):40–45.
- Rushton ABB, Jordaan K, Langendoen R, et al. Educational standards in orthopeadic manipulative therapy (IFOMPT) (2016).
- Lacasse M, Douville F, Gagnon J, et al. Theories and models in health sciences education – a literature review. Can J SoTl. 2019;10(3).
- Ernstzen DV, Bitzer E, Grimmer-Somers K. Physiotherapy students’ and clinical teachers’ perceptions of clinical learning opportunities: a case study. Med Teach. 2009;31(3):e102–15.
- Bandura A. Social cognitive theory: an agentic perspective. Annu Rev Psychol. 2001;52:1–26.
- Patton N, Higgs J, Smith M. Using theories of learning in workplaces to enhance physiotherapy clinical education. Physiother Theory Pract. 2013;29(7):493–503.
- Balogh EP, Miller BT, Ball JR. Committee on Diagnostic error in health, care board on health care, services institute of, medicine the national academies of sciences, engineering medicine improving diagnosis in health care. Washington (DC): National Academies Press (US); 2015.
- Norman GR, Monteiro SD, Sherbino J, et al. The causes of errors in clinical reasoning: cognitive biases, knowledge deficits, and dual process thinking. Acad Med. 2017;92(1):23–30.
- Elstein AS. Thinking about diagnostic thinking: a 30-year perspective. Adv Health Sci Educ Theory Pract. 2009;14 Suppl 1(S1):7–18.
- Medina MS, Castleberry AN, Persky AM. Strategies for Improving learner metacognition in health professional education. Am J Pharm Educ. 2017;81(4):78.
- Royce CS, Hayes MM, Schwartzstein RM. Teaching critical thinking: a Case for instruction in cognitive biases to reduce diagnostic errors and improve patient safety. Acad Med. 2019;94(2):187–194.
- Wainwright SF, Shepard KF, Harman LB, et al. Novice and experienced physical therapist clinicians: a comparison of how reflection is used to inform the clinical decision-making process. Phys Ther. 2010;90(1):75–88.
- Clark I, Dumas G. Toward a neural basis for peer-interaction: what makes peer-learning tick? Front Psychol. 2015;6:28.
- Hickey DT. Motivation and contemporary socio-constructivist instructional perspectives. Educ Psychol. 1997;32(3):175–193.
- Lekkas P, Larsen T, Kumar S, et al. No model of clinical education for physiotherapy students is superior to another: a systematic review. Aust J Physiother. 2007;53(1):19–28.
- Monteiro SM, Norman G. Diagnostic reasoning: where we’ve been, where we’re going. Teach Learn Med. 2013;25(1):S26–32.
- Atkinson HL, Nixon-Cave K. A tool for clinical reasoning and reflection using the international classification of functioning, disability and health (ICF) framework and patient management model. Phys Ther. 2011;91(3):416–430.
- Baker SE, Painter EE, Morgan BC, et al. Systematic Clinical Reasoning in Physical Therapy (SCRIPT): tool for the purposeful practice of clinical reasoning in orthopedic manual physical therapy. Phys Ther. 2017;97(1):61–70.
- Tolks D, Lampert C, Dadaczynski K, et al. Game-based approaches to prevention and health promotion: serious games and gamification. Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz. 2020;63(6):698–707.
- Giannakas F, Kambourakis G, Papasalouros A, et al. A critical review of 13 years of mobile game-based learning. Educ Technol Res Dev. 2017;66(2):341–384.
- García-Redondo P, García T, Areces D, et al. Serious Games and their effect improving attention in students with learning disabilities. Int J Environ Res Public Health. 2019;16(14):2480.
- Haoran G, Bazakidi E, Zary N. Serious games in health professions education: review of trends and learning efficacy. Yearb Med Inform. 2019;28(1):240–248.
- Bergeron B. Developing serious games. Hingham Charles River Media; 2006;398.
- Gorbanev I, Agudelo-Londoño S, González RA, et al. A systematic review of serious games in medical education: quality of evidence and pedagogical strategy. Med Educ Online. 2018;23(1):1438718.
- Koivisto JM, Haavisto E, Niemi H, et al. Design principles for simulation games for learning clinical reasoning: a design-based research approach. Nurse Educ Today. 2018;60:114–120.
- Blanié A, Amorim MA, Benhamou D. Comparative value of a simulation by gaming and a traditional teaching method to improve clinical reasoning skills necessary to detect patient deterioration: a randomized study in nursing students. BMC Med Educ. 2020;20(1):53.
- Cant RP, Cooper SJ. Simulation-based learning in nurse education: systematic review. J Adv Nurs. 2010;66(1):3–15.
- Lapkin S, Fernandez R, Levett-Jones T, et al. The effectiveness of using human patient simulation manikins in the teaching of clinical reasoning skills to undergraduate nursing students: a systematic review. JBI Libr Syst Rev. 2010;8(16):661–694.
- Tubelo RA, Portella FF, Gelain MA, et al. Serious game is an effective learning method for primary health care education of medical students: a randomized controlled trial. Int J Med Inform. 2019;130:103944.
- Graafland M, Schraagen JM, Schijven MP. Systematic review of serious games for medical education and surgical skills training. Br J Surg. 2012;99(10):1322–1330.
- Miller PA Pattern recognition is a clinical reasoning process in musculoskeletal physiotherapy. University of Newcastle Research Higher Degree Thesis. 2009.
- Granero-Gallegos A, Baena-Extremera A, Pérez-Quero FJ, et al. Analysis of motivational profiles of satisfaction and importance of physical education in high school adolescents. J Sports Sci Med. 2012;11(4):614–623.
- Baena-Extremera A, Granero-Gallegos A, Del Mar Ortiz-Camacho M. Quasi-experimental study of the effect of an adventure education programme on classroom satisfaction. Physical Self-Concept and Social Goals in Physical Education Psychologica Belgica. 2012;52(4):369–386.
- Yeung E, Woods N, Dubrowski A, et al. Sensibility of a new instrument to assess clinical reasoning in post-graduate orthopaedic manual physical therapy education. Man Ther. 2015;20(2):303–312.
- World Health Organization. International classification of functioning, disability and health (ICF) WHO; 2001.
- Petersen EJ, Thurmond SM, GM J. Severity, Irritability, Nature, Stage, and Stability (SINSS): a clinical perspective. J Man Manip Ther. 2021;29(5):297–309.
- Melvin L, Cavalcanti RB. The Oral Case Presentation: a key tool for assessment and teaching in competency-based medical education. JAMA. 2016;316(21):2187–2188.
- Haber RJ, Lingard LA. Learning oral presentation skills: a rhetorical analysis with pedagogical and professional implications. J Gen Intern Med. 2001;16(5):308–314.
- Dory V, Gagnon R, Charlin B, et al. In Brief: validity of case Summaries in written examinations of clinical reasoning. Teach Learn Med. 2016;28(4):375–384.
- Garrocho-Rangel A, Flores-Arriaga JC, Saadia M, et al. Case report in clinical pediatric dentistry: how to review, organize and prepare a manuscript. J Clin Pediatr Dent. 2019;43(1):1–4.
- Masaracchio M, Kirker K, Collins CK, et al. AN intervention-based clinical reasoning framework to guide the management of thoracic pain in a dancer: a case report. Int J Sports Phys Ther. 2016;11(7):1135–1149.
- Wiggins B L, Eddy S L, Wener-Fligner L, Freisem K, Grunspan D Z, Theobald E J, Timbrook J, Crowe A J and Momsen J. ASPECT: A Survey to Assess Student Perspective of Engagement in an Active-Learning Classroom. CBE-Life Sciences Education. 2017;16(2):ar32
- Larsen DP, Butler AC, Roediger HL. 3rd. Test-enhanced learning in medical education. Med Educ. 2008;42(10):959–966.
- Roediger HL, Karpicke JD. Test-enhanced learning: taking memory tests improves long-term retention. Psychol Sci. 2006;17(3):249–255.
- Eva KW. What every teacher needs to know about clinical reasoning. Med Educ. 2005;39(1):98–106.
- Linn A, Khaw C, Kildea H, et al. Clinical reasoning - a guide to improving teaching and practice. Aust Fam Physician. 2012;41(1–2):18–20.
- Reilly JB, Ogdie AR, Von Feldt JM, et al. Teaching about how doctors think: a longitudinal curriculum in cognitive bias and diagnostic error for residents. BMJ Qual Saf. 2013;22(12):1044–1050.
- Hendrick P, Bond C, Duncan E, et al. Clinical reasoning in musculoskeletal practice: students’ conceptualizations. Phys Ther. 2009;89(5):430–442.
- Davenport TE. Clinical Case reporting in the peer-reviewed physical therapy literature: time to move toward functioning. Physiother Res Int. 2015;20(4):220–230.