
ABSTRACT
Introduction
Risks and benefits of spinal manipulations and mobilization in pediatric populations are a concern to the public, policymakers, and international physiotherapy governing organizations. Clinical Outcome Assessments (COA) used in the literature on these topics are contentious. The aim of this systematic review was to establish the quality of clinician-reported and performance-based COAs identified by a scoping review on spinal manipulation and mobilization for pediatric populations across diverse medical conditions.
Method and analysis
Electronic databases, clinicaltrials.gov and Ebsco Open Dissertations were searched up to 21 October 2022. Qualitative synthesis was performed using Consensus-based Standards for the Selection of Health Measurement Instruments (COSMIN) guidelines to select studies, perform data extraction, and assess risk of bias. Data synthesis used Grading of Recommendations, Assessment, Development and Evaluations (GRADE) to determine the certainty of the evidence and overall rating: sufficient (+), insufficient (-), inconsistent (±), or indeterminate (?).
Results
Four of 17 identified COAs (77 studies, 9653 participants) with supporting psychometric research were classified as:
Performance-based outcome measures:
AIMS – Alberta Infant Motor Scale (n = 51); or:
Clinician-reported outcome measures:
LATCH – Latch, Audible swallowing, Type of nipple, Comfort, Hold (n = 10),
Cobb Angle (n = 15),
Postural Assessment (n = 1).
AIMS had an overall sufficient (+) rating with high certainty evidence, and LATCH had an overall sufficient (+) rating with moderate certainty of evidence. For the Cobb Angle and Postural Assessment, the overall rating was indeterminate (?) with low or very low certainty of evidence, respectively.
Conclusion
The AIMS and LATCH had sufficient evidence to evaluate the efficacy of spinal manipulation and mobilization for certain pediatric medical conditions. Further validation studies are needed for other COAs.
Introduction
Assessing the ethical acceptability of health-related research involving spinal manipulation and mobilization in diverse pediatric populations with varying medical conditions necessitates a crucial risk-benefit analysis. International policymakers, clinicians, and guardians are questioning whether the risks associated with spinal manipulation and mobilization exceed the anticipated benefits. The Australian Government in the state of Victoria has restricted the use of these techniques in infants [Citation1]. The International Federation of Orthopaedic Manipulative Physical Therapists (IFOMPT), in collaboration with the International Organisation of Physical Therapists in Paediatrics (IOPTP), has identified a great need to accurately map the scientific evidence and safety issues regarding manipulation and mobilization for infants, children, and adolescents with various conditions. Clinicians are seeking the evidence-basis of this care pathway to make safe clinical judgments, decision-making, and guide their clinical reasoning process. A scoping review [Citation2] for a pediatric population receiving spinal manipulation and mobilization established that there was a diverse listing of Clinical Outcome Assessments (COA) with poor reporting of their psychometric properties; COAs were defined by the United States Food and Drug Administration (FDA) as tools that ‘measure a patient’s symptoms, overall mental state, or the effects of a disease or condition on how the patient functions’ [Citation3]. Healthcare professionals and researchers typically use one or more of the four standardized assessment categories of COA to measure clinical benefit in treatment trials as follows:
patient-reported – patient’s self report of difficulty in completing a task or of feelings experienced during tasks of daily living.
clinician-reported – a trained health professional’s observation of a patient’s health condition involving clinical judgment and interpretation of the observable signs, behaviors, or other manifestations.
observer-reported – a report by a caregiver, guardian, or other observer of patients who cannot report for themselves (e.g., infant); this observation does not include clinical judgment.
performance-based – a trained observer administers and evaluates a standardized task(s) performed by the patient.
See for those COAs identified by Milne and colleagues [Citation2] in their scoping review.
Figure 1. Clinical outcome assessment (COA) categories that were identified by a scoping review on spinal manipulation and mobilisation in paediatric populations [Citation2]. Clinician-reported and performance-based outcome assessments were the focus of this report. All listed outcomes were included in our search however the bolded ones were those identified in the literature to have psychometric properties for paediatric populations.
![Figure 1. Clinical outcome assessment (COA) categories that were identified by a scoping review on spinal manipulation and mobilisation in paediatric populations [Citation2]. Clinician-reported and performance-based outcome assessments were the focus of this report. All listed outcomes were included in our search however the bolded ones were those identified in the literature to have psychometric properties for paediatric populations.](/cms/asset/25623607-e751-4207-b888-701ad23baa82/yjmt_a_2269038_f0001_oc.jpg)
Interpreting the effects of outcomes such as pain, function, motor development, mobility difficulties, and participation in life activities for infants, children, and adolescence before and following spinal manipulation and mobilization is critical. Foundational to the determination of the efficacy, effectiveness, and harm is the use of outcome measures with good measurement properties as established by COSMIN’s [Citation4] including:
Reliability:internal consistency, test-retest/intra-rater/inter-rater reliability, measurement error;
Validity
content validity including relevance, comprehensiveness, comprehensibility, outcome measurement items assessed and appropriately worded [Citation5]
structural validity,
hypothesis testing for construct validity,
cross-cultural validity,
criterion validity and
Responsiveness for each measurement.
Additionally, the interpretability and feasibility of the reported outcome measure is needed to formulate recommendations on the suitability for use in an evaluative application of the construct of interest and study population.
The aim of this systematic review was to evaluate the psychometric properties of clinician-reported and performance-based outcomes that were identified by a scoping review on spinal manipulation and mobilization in pediatrics, aged birth to 18 years across diverse medical conditions. These outcomes are related to the physical functioning, motor development, and mobility of infants, children, and adolescence.
Method
The protocol was registered with Open Science Framework (DOI 10.17605/OSF.IO/RN4UX). This review was part of a larger project designed to depict COAs by subcategories: Part 1. Patient-reported and Observer-reported Outcomes [Citation6]; Part 2. Clinician-reported and Performance-based Outcomes. The review was reported in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) statement [Citation7] and Consensus-based Standards for the Selection of Health Measurement Instruments (COSMIN) guideline for systematic reviews [Citation8].
Eligibility criteria
Type of participants: Pediatric (birth to 18 years of age) patients with medical conditions identified by a scoping review and managed with spinal manipulation and mobilization were considered [Citation2]. These conditions varied and included Enuresis, Otitis Media, Colic, Excessive Crying/Colic, Breastfeeding, Low Back Pain, Headaches, Cerebral Palsy, Neck Pain, Scoliosis, Attention Deficit Disorder, Autism, Torticollis, Asthma, Chronic Respiratory Illness, KISS (kinetic imbalances due to suboccipital strain), and Dysfunctional Voiding and could include healthy participants. If there were greater than 20% of the population older than 18 years old, the study was excluded.
Type of clinical outcome assessment (COA): Clinician-reported and performance-reported COAs were considered eligible for this study.
Type of psychometric outcome: Studies addressed a minimum of one psychometric property from any of the following three domains:
Validity: content validity (i.e., relevance, comprehensiveness, comprehensibility, outcome measurement items assessed and appropriately worded), structural validity, hypothesis testing for construct validity, cross-cultural validity, criterion validity.
Reliability: internal consistency, test–retest reliability, intra-rater reliability, inter-rater reliability, measurement error (i.e., standard error measure (SEM), smallest detectable change (SDC) or limit of agreement (LoA)).
Responsiveness (i.e., SDC, minimal important change (MIC), area under the curve (i.e., ROC – Receiver Operation Curve)).
Information on the interpretability (i.e., floor or ceiling effect) and feasibility of the reported outcome measure was also gathered. Trials where the COA was used as an outcome measure or in validation of another instrument were excluded.
Type of study design: All study designs (i.e., cohort, case-control, cross-sectional, case-series, randomized controlled trials) except for questionnaires, surveys, screening tools, and case reports were included.
Information sources and search strategy
A medical librarian and information specialist (JM) designed, tailored, and performed an electronic search of PUBMED, Embase, and CINAHL from inception to 26 February 2021 with an update to 21 October 2022 without language restriction. However, translation capacity of our research team and colleagues was English, Dutch, German, Spanish, French, Korean, Hungarian, Russian, and Croatian and non-translated studies were recorded. The search strategy was to combine each COA identified by a previously completed scoping review [Citation2] with a modified instrument properties search block for PUBMED created by [Citation9] as well as a measurement property filter: 1) for the Index to Chiropractic Literature created by JM, 2) for EMBASE translated by EP Jansma and 3) for CINAHL developed FS van Etten (COSMIN website). By selectively adding a chiropractic filter and a pediatric filter, we balanced the search strategy between recall and precision. A sample of the search parameters can be found in Box 1. We searched gray literature in clinicaltrials.gov and Ebsco Open Dissertations on 29 March 2021, and references of primary studies were checked by TH.
Box 1. A sample MEDLINE search strategy and parameters include a search block for psychometric properties and a search block for spinal manipulation and mobilization.
Search block for psychometric properties:
(MH ‘Psychometrics’) or (TI psychometr* or AB psychometr*) or (TI clinimetr* or AB clinimetr*) or (TI clinometr* OR AB clinometr*) or (MH ‘Outcome Assessment’) or (TI outcome assessment or AB outcome assessment) or (TI outcome measure* or AB outcome measure*) or (MH ‘Health Status Indicators’) or (MH ‘Reproducibility of Results’) or (MH ‘Discriminant Analysis’) or ((TI reproducib* or AB reproducib*) or (TI reliab* or AB reliab*) or (TI unreliab* or AB unreliab*)) or ((TI valid* or AB valid*) or (TI coefficient or AB coefficient) or (TI homogeneity or AB homogeneity)) or (TI homogeneous or AB homogeneous) or (TI ‘coefficient of variation’ or AB ‘coefficient of variation’) or (TI ‘internal consistency’ or AB ‘internal consistency’) or (MH ‘Internal Consistency+’) or (MH ‘Reliability+’) or (MH ‘Measurement Error+’) or (MH ‘Content Validity+’) or ‘hypothesis testing’ or ‘structural validity’ or ‘cross-cultural validity’ or (MH ‘Criterion-Related Validity+’) or ‘responsiveness’ or ‘interpretability’ or (TI reliab* or AB reliab*) and ((TI test or AB test) OR (TI retest or AB retest)) or (TI stability or AB stability) or (TI interrater or AB interrater) or (TI inter-rater or AB inter-rater) or (TI intrarater or AB intrarater) or (TI intra-rater or AB intrarater) or (TI intertester or AB intertester) or (TI inter-tester or AB inter-tester) or (TI intratester or AB intratester) or (TI intra-tester or AB intra-tester) or (TI interobserver or AB interobserver) or (TI inter-observer or AB inter-observer) or (TI intraobserver or AB intraobserver) or (TI intra-observer or AB intra-observer) or (TI intertechnician or AB intertechnician) or (TI inter-technician or AB inter-technician) or (TI intratechnician or AB intratechnician) or (TI intra-technician or AB intra-technician) or (TI interexaminer or AB interexaminer) or (TI inter-examiner or AB inter-examiner) or (TI intraexaminer or AB intraexaminer) or (TI intra-examiner or AB intra-examiner) or (TI intra-examiner or AB intraexaminer) or (TI interassay or AB interassay) or (TI inter-assay or AB inter-assay) or (TI intraassay or AB intraassay) or (TI intra-assay or AB intra-assay) or (TI interindividual or AB interindividual) or (TI inter-individual or AB inter-individual) OR (TI intraindividual or AB intraindividual) or (TI intra-individual or AB intra-individual) or (TI interparticipant or AB interparticipant) or (TI inter-participant or AB inter-participant) or (TI intraparticipant or AB intraparticipant) or (TI intra-participant or AB intra-participant) or (TI kappa or AB kappa) or (TI kappa’s or AB kappa’s) or (TI kappas or AB kappas) or (TI repeatab* or AB repeatab*) or (TI responsive* or AB responsive*) or (TI interpretab* or AB interpretab*)
Search block for spinal manipulation and mobilization:
‘spinal manipulation’ OR ‘spinal manipulations’ OR ‘spinal mobilization’ OR ‘spinal mobilizations’ OR ‘spinal mobilization’ OR ‘spinal mobilizations’ OR ‘spinal adjustment’ OR ‘spinal adjustments’ OR ‘spinal manual therapy’ OR ‘high velocity low amplitude thrust’ OR ‘HVLA’ OR ‘musculoskeletal of the spine’ OR ‘spinal musculoskeletal’ OR ‘manual therapy of the spine’ OR ‘cervical manual therapy’ OR ‘thoracic manual therapy’ OR ‘lumbar manual therapy’ OR ‘manual therapy of the lumbar spine’ OR ‘manual therapy of the thoracic spine’ OR ‘manual therapy of the cervical spine’ OR ‘spinal osteopathy’ OR ‘osteopathy of the spine’ OR ‘osteopathy of the cervical spine’ OR ‘osteopathy of the thoracic spine’ OR ‘osteopathy of the lumbar spine’ OR ‘spinal osteopathies’ OR ‘osteopathies of the spine’ OR ‘osteopathies of the cervical spine’ OR ‘osteopathies of the thoracic spine’ OR ‘osteopathies of the lumbar spine’ OR chirop* OR ‘spinal manipulative therapy’ OR ‘spinal manipulative therapies’
Key: TI = Title; AB = abstract; MH = MeSH heading (MeSH is the MEDLINE index).
Study identification and selection
The review manager Covidence (Veritas Health Innovation, Melbourne, Australia) was used for study screening, selection, and data extraction. Pre-piloted forms and two independent reviewers (screening and selection review teams: JP/TH, AB/AG, KO/DC, NM/OA). An initial screening of study title and abstract and full-text selection was performed after a 10-study calibration period and with two additional meetings between the authors to ensure consistency (Kappa values were set at 0.4 moderate to 0.75 good a priori). Disagreements were resolved by discussion and reference to a third reviewer when needed (JP; See ). For abstracts only, we conducted a second search to determine their publication status.
Data extraction and data items
A standardized data collection form was used by a pair of researchers (review teams: JP/TH, AB/TH, OA/AG) independently extracted data using a standardized pilot-tested form in addition to the COSMIN Risk of Bias checklist including:
1. Description and scoring of the assessment tool;
2. Population demographic characteristics, medical condition, country, number of participants, age, sex, professional involved;
3. Inclusion/exclusion criteria;
4. Results addressing psychometrics; and
5. Statistical methods used.
Missing data from primary studies were addressed by either consulting the outcome measurement website/administrator when available and the author for key data. We did not check if studies were registered prior to their start.
Risk of bias (RoB) assessment
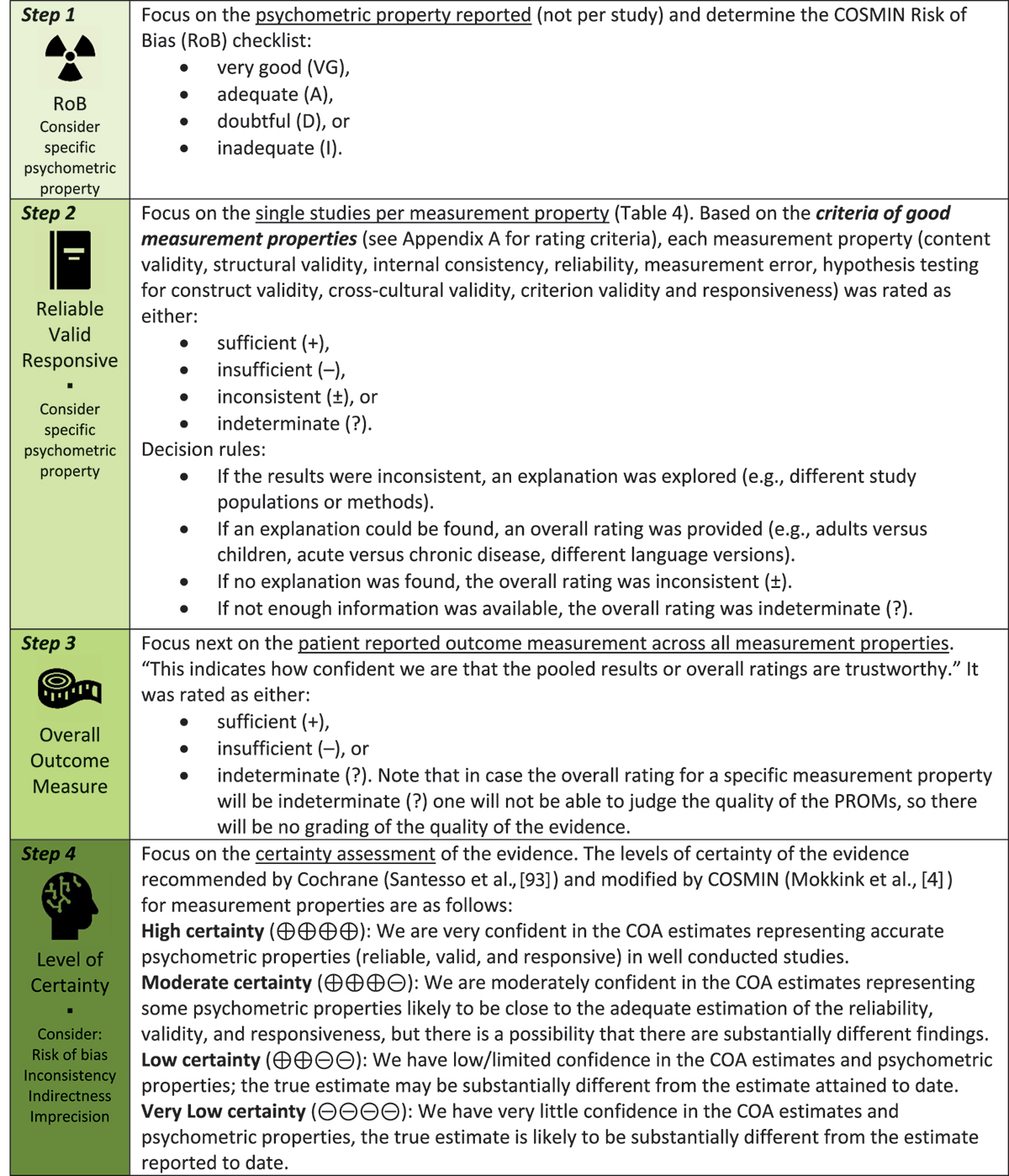
Using the valid and reliable COSMIN Risk of Bias checklist, two reviewers (review teams JP/AB, TH/OA) independently evaluated the RoB of each included study and resolved uncertainties through discussion [Citation4,Citation8]. Additionally, validation studies for clinician-reported and performance-based measures was conducted [Citation10,Citation11]. The COSMIN checklist uses a 4-point rating scale: very good (VG), adequate (A), doubtful (D), and inadequate (I) (see Box 2. – Step 1). The RoB of research was judged per psychometric property reported, not per study. The overall score for each measurement property on the COSMIN checklist was determined by a ‘worse score counts’ approach.
Measures of psychometric values
After qualitative evaluation of study population and the psychometric properties, no further quantitative analysis or meta-analysis was completed by psychometric value due to the heterogeneity of study populations and the properties evaluated. Statistics depicted in this paper are directly quoted as the authors presented them. Confidence Intervals (CI) and standard deviations (SD) are presented if they were reported.
Data synthesis and analysis methods
In , we summarized a descriptive synthesis of findings for the psychometric properties of each COA for identified studies. In , we detailed the updated criteria of good measurement properties established by COSMIN’s [Citation4]. We rated the results for reliability (internal consistency, test-retest/intra-rater/inter-rater reliability, measurement error), validity (a. content validity including relevance, comprehensiveness, comprehensibility, outcome measurement item’s assessed, and appropriately worded [Citation9]; b. structural validity, c. hypothesis testing for construct validity, cross-cultural validity, and criterion validity), responsiveness for each measurement property as sufficient (+), insufficient (–), or indeterminate (?) (see Box 2. – Step 2; see Appendix A for definitions) [Citation4; Citation88]. A qualitative summary using COSMIN defined criteria for an OVERALL RATING was completed on measurement properties; this was based on our reviewer’s consensus judgment as sufficient (+), insufficient (−), inconsistent (±), or indeterminate (?) (see Box 2. – Step 3). The interpretability (Appendix B) and feasibility (Appendix C) were reported as per COSMIN guidelines.
Table 1. Characteristics of included studies.
Table 2. Population per outcome measure.
Table 3. Summary of findings for each COA included 1) criteria rating for good measurement property (sufficient (+), insufficient (-), inconsistent (±), indeterminate (?); see gray highlighted ROW) for each measurement property (content validity, structural validity, internal consistency, reliability, measurement error, hypothesis testing for construct validity, cross-cultural validity, criterion validity, and responsiveness), 2) overall rating across measurement properties for each COA (sufficient (+), insufficient (–), or indeterminate (?); see gray highlight COLUMN), and 3) certainty of evidence (GRADE). Note that the author(s) with risk of bias score by psychometric property were rated as very good (VG), adequate (A), doubtful (D), or inadequate (I) (i.e. Allen 208 (D)).
Table 4. Summary of results for Alberta Infant motor Scale (AIMS).
Box 2. COSMIN steps in evaluating the evidence [Citation88] and box replicated from Hayton et al. 2024.
Certainty assessment
The adapted GRADE (Grading of Recommendations, Assessment, Development and Evaluations) approach was used to summarize the evidence across the psychometric elements as follows: 1. high, 2. moderate, 3. low, and 4. very low certainty (see Box 2. – Step 4 [Citation4; –] page 32–36 [Citation92,Citation93].
Results
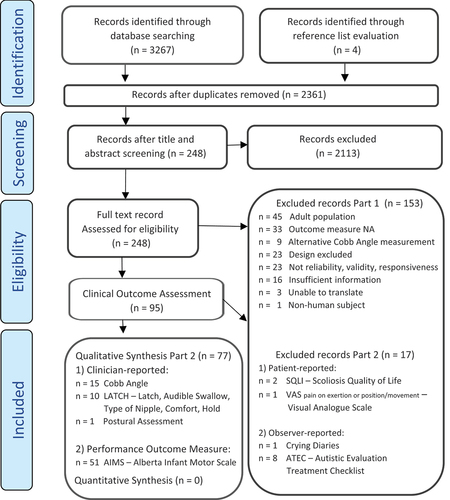
Of 2361 records left following deduplication, 248 were retrieved for full-text review, we selected 95 studies which met the inclusion criteria of which 77 studies concerned clinician-reported or performance-based outcomes ()
Figure 2. The PRISMA diagram for study flow.
Included studies
We included 77 studies and 9789 participants analyzed: AIMS – Alberta Infant Motor Skill (n = 51 studies), LATCH – Latch, Audible swallowing, Type of nipple, Comport, Hold (n = 10 studies), Cobb Angle (n = 15 studies), Postural Assessment (n = 1 study). cites the included studies by outcome measure and describes their characteristics, while details the population’s age and medical condition by outcome measure. Most studies assessed a spectrum of psychometric properties, and one COA (AIMS) was comprehensive (see for a detailed description). Most studies used convenience samples drawn from community and government supported healthcare centers, schools, and daycares. The ages of the participants reflected the purpose of the outcome measure used. Two studies [Citation81,Citation82] utilizing Cobb angles did consider participants as older than 18 years. The sex of the participants was distributed evenly except for postural assessment where males were exclusively studied. Of the full-text articles screened, nine studies cited in Appendix D, addressed the validity and reliability of the Cobb angle using alternative methods from that sited in the scoping review. Convenience samples drawn from community and government supported healthcare centers, schools, and daycares were predominately use. Gender varied by the diagnoses studied.
Table 5. Summary of results for LATCH.
Table 6. Summary of results for Cobb angle.
Table 7. Summary of results for postural assessment.
Excluded studies
We excluded 169 studies for the following reasons: 1) the participants were adults; 2) the COA was not on the pre-identified list from the scoping review; 3) more than 20% of the population under research was over 18 years of age; and 4) psychometric properties did not address reliability, validity, responsiveness, and information related to the interpretability and feasibility of the reported outcome measure.
Risk of bias
The quality of research was judged per psychometric property reported, not per study. Research quality was judged to be adequate or very good in 31% for reliability and 43% for validity with the most common sources of bias being poor statistical analysis, unclear methodology, and small population numbers (see ).
Main results by clinical outcome assessment
summarizes the main findings with overall ratings by COA and the GRADE with certainty of evidence and related reasons of downgrading. The main psychometric properties can be found in for AIMS, for LATCH, for Cobb angle, and for Postural.
Performance-based outcomes
Alberta Infant Motor Scale (AIMS)
The Alberta Infant Motor Scale has a predictive purpose to classify motor learning. It is an observational assessment scale that assesses gross motor maturation and skills in infants from ages 0 to 18 months with typical development or those with developmental delay or atypical patterns. It measures weight bearing, posture, and antigravity movements of infants. Fifty-one studies examined the psychometric properties of AIMS (). Population studies included healthy, preterm, chronically ill, neurologically compromised, and infants exposed to HIV (human immunodeficiency virus). Content validity (two studies, n = 1057) was assessed for relevance, comprehensiveness, comprehensibility, and appropriate wording. Forty-six properties of the validity domain were studied, including construct, predictive, criterion, concurrent, structural, and cultural validity. With the exception to one outlier [Citation47], there is a moderate to strong correlation with other outcome measures intended to evaluate motor performance of infants. Thirty-eight properties of the reliability domain were studied. If >0.70 is considered a significant ICC value, then all studies show an acceptable inter-rater reliability. Apart from one outlier [Citation48], the range showed acceptable inter-rater reliability ICC = 0.85 to 0.99. High certainty evidence supports the use of AIMS with responsiveness needing further research. The overall rating was sufficient (+). There were greater number of large studies of lower risk of bias across all psychometric domains exploring different aspects of reliability. Construct validity explored numerous hypotheses with large trials (see ).
Clinician-reported outcomes
LATCH
The quality of breastfeeding is evaluated using the evaluative measure LATCH [Citation95]; each letter of the acronym indicates an area of assessment. ‘L’ identifies how well the infant latches onto the breast. ‘A’ identifies the amount of audible swallowing noted. ‘T’ identifies the mother’s nipple type. ‘C’ identifies the mother’s level of comfort. ‘H’ indicates the amount of help the mother needs to hold her infant to the breast. Structural validity using confirmatory factor analysis on 4-items removing one item C (Comfort). Internal consistency improved with four items (α = 0.74) versus five items (α = 0.25 to 0.70) as well. Six further elements of validity and seven of inter-rater reliability were studied () in a population of healthy newborns and infants. The certainty of evidence was judged to be moderately downgraded due to imprecision (−1: total 10 studies, n < 100; no meta-analysis). The overall rating was sufficient (+) (see ).
Cobb Angle
Cobb Angle has a discriminative purpose used with scoliosis. It is a standard measurement to determine the presence of and track the advancement of scoliosis. Of 15 studies (see ), six assessed validity and 12 various aspects of reliability. All studies correlated different novel methods of digital measurements versus a traditional reading but did not directly address the validity of measuring the Cobb angle as an indication of disease severity. The certainty of the evidence was low downgraded due to limitation in inconsistency (−1: numerous studies are rated doubtful or inadequate in study design) and indirectness (−1: about 20% of population was between 18 to 40 years of age). The overall rating of the Cobb Angle was indeterminate (?) (see ).
Postural Assessment
A postural assessment can involve observation of static posture for symmetry and alignment of anatomic landmarks. It may be visual or use a palpation assessment. The patient is directed to stand with feet shoulder-width apart and arms relaxed to the sides. One study (Watson and Mac Donncha, 2020; ) examined intra-rater and inter-rater reliability of postural assessment in male adolescents using a photographic method. The certainty of the evidence was very low downgraded due to limitations in risk of bias (−2), imprecision (−1), and indirectness (−1). We could not find reports on validity or responsiveness. The overall rating of postural assessment was indeterminate (?) (see ).
Discussion
We evaluated the psychometric properties on four of 18 pre-identified COAs used to determine the effectiveness of spinal manipulation and mobilization for various medical conditions in a pediatric population [Citation2]. One performance-based outcome (AIMS) and one clinician-reported outcome measures (LATCH) had sufficient information; AIMS had high certainty evidence, and LATCH had moderate, but both lacked sufficient assessment on responsiveness.
Overall completeness and applicability of evidence
The context and purpose of this systematic review was to determine if the included COAs can and should be used to evaluate the effectiveness of spinal manipulation or mobilization for various medical conditions in a pediatric population. We questioned if the identified COAs were fit for this purpose. Whilst we determined that one performance-based outcome and one clinician-reported outcome measure have high to moderate levels of certainty, respectively, they both lacked assessment on responsiveness. The COA may have poor responsiveness to detect change, and a treatment effect may not be detected, when one exists, in other words, leading to a false-negative result or to a failed trial. Additionally, the greatest level of certainty is to use a COA that was developed and assessed in the target patient population in which it will be used. The construct underpinning the clinical reasoning in performing a manipulation and mobilization in diverse medical conditions remains unclear.
The AIMS is a well-researched performance-based outcome tool used to determine motor development in infants [Citation23]. We have high certainty that it is a reliable and valid tool that gives appropriate results for the staging of infants’ motor development. One randomized control study that utilized AIMS as a chosen outcome measure was identified through a scoping review. The effect of manual therapy on non-synostotic plagiocephaly were examined [Citation96]. It is beyond the scope of the paper to determine if manipulation or mobilization is an effective treatment technique for plagiocephaly; however, the scientific basis of this construct is in debate [Citation97]. Considering the objective of this study, AIMS was an appropriate outcome measure for assessing motor development; however, since responsiveness is not reported, it may be inadequate in this medical condition.
It has been suggested that chiropractic manipulation is an effective treatment option to improve breastfeeding due to mechanical restriction of the infant’s cervical spine and temporomandibular joint [Citation98–100]. Fry [Citation101] completed a literature review regarding the role of chiropractic care and breastfeeding. Chiropractic care was identified to be beneficial if there was a biomechanical limitation to breastfeeding. Successful treatment was aimed at the cranial sutures, temporomandibular joint, and cervical spine, particularly the atlantoaxial joint. Again, the scientific basis of this construct of thinking is lacking, and it is hard to find evidence for the relation between, for example, movement of the cranial sutures and breastfeeding. One randomized control study was identified by the scoping review [Citation2]. Mother-infant dyads were randomized to either a group with a lactation consultation and sham osteopathic treatment or a group with a lactation consultation and osteopathic treatment [Citation102]. The biological rationale does not seem plausible that manipulation or mobilization should have a positive effect on breastfeeding and is without any evidence. The LATCH tool was presented by Jensen and colleagues [Citation95] as a clinician-reported outcome that assesses the quality of the LATCH, audible swallowing, nipple type, comfort, and hold to measure the effectiveness of breastfeeding. Research from this review demonstrates that LATCH has a moderate certainty of evidence for reliability and validity. Regarding responsiveness, there was no evidence found. It is beyond the scope of this paper to draw conclusions regarding the effectiveness of treatment utilizing manipulation or mobilization, to improve the infant’s biomechanics of breastfeeding. It is unclear if the LATCH is an appropriate tool to measure responsiveness to changes in breastfeeding.
Quality of the evidence
A thorough methodological assessment of included studies using the robust and validated COSMIN checklist across a variety of outcome measures identified that the limitations in the retrieved articles were poor statistical analysis, poor methodological reporting, and low sample size. A thoughtful and strategic approach to instrument selection in clinical trials is a unique challenge.
Potential biases in the review process
Our medical information specialist was unable to limit the search parameters to the medical conditions discussed in the scoping review due to the vague definition of medical conditions within the identified studies in the scoping review [Citation2]. Additionally, we did have language restrictions, our search included only English, Spanish, Dutch, French, and German articles. We maximized the inter-rater reliability for the COSMIN score by organizing group consensus discussions on three occasions during the review process to ensure calibration and interpretation of checklist items.
Agreements and disagreements with other studies or reviews
No other systematic reviews assessing the psychometric properties of LATCH and posture assessment were identified for pediatric conditions. We found reviews on the measurement of the Cobb angle, but these reviews did not mention a pediatric population. Three systematic reviews regarding the AIMS agreed with our review [Citation49,Citation103,Citation104]. They concluded that the AIMS was valid and reliable but was not ideal for use with preterm infants and lacked predictive value. Spittle et al. [Citation89] concluded that the AIMS was good at predicting motor impairment of corrected age preterm infants, with the most consistent results at 4 months. Albuquerque et al. also found a small ceiling effect. Kjølbye et al. [Citation105] differed from our review in that they also stated that AIMS was valid for staging motor skills as confirmed with Peabody Developmental Gross Motor Scale and with Bayley Score of Infant Development. None of the reviews found data on responsiveness, similar to our findings.
Conclusion
The AIMS has a high and LATCH moderate certainty of evidence and demonstrated sufficient measurement properties to be used in clinical practice. Neither had sufficiently assessed responsiveness.
High-quality research assessing the psychometric properties of diagnostic and evaluative tools utilized with pediatric populations is needed to fill the gap for those utilizing spinal manipulation or mobilization to manage a variety of medical conditions in infants, children, and adolescents. Furthermore, a focus on responsiveness is needed.
Supplemental Material
Download PDF (631 KB)Acknowledgements
Jurgen Mollema, University of Applied Sciences, The Netherlands was our medical information specialist and research librarian. Derek Clewney, Duke University, USA, is a member of the collaborative International Federation of Orthopaedic Manipulative Physical Therapists (IFOMPT) and International Organisation of Physical Therapists in Paediatrics (IOPTP) Task Force on Spinal Manipulation in Children and assisted with data screening.
Disclosure statement
No authors have declared any conflict of interest.
Supplementary material
Supplemental data for this article can be accessed online at https://doi.org/10.1080/10669817.2023.2269038
Additional information
Funding
Notes on contributors
Tricia Hayton
Tricia Hayton is a private practitioner in Oakville, Ontario, Canada. She was a graduate student of the OMPT program at McMaster University and completed this work as part of her research requirements.
Anita Gross
Anita Gross is an Associate Clinical Professor at McMaster University on the School of Rehabilitation Sciences leading their advanced orthopedic musculoskeletal-manipulative physical therapy (OMPT) program. She is a lecturer in the Master’s of Clinical Science program in Manipulative Therapy at Western University and the Canadian Physiotherapy Association AIM program. She is the chair of the IFOMPT/IOPTP Taskforce on Pediatric Manipulation informing PT policy with systematic reviews and evidence gap maps. She is a clinician scientist and educator. She has over 150 peer reviewed publications, has been principal/co-investigator on 30 grants and has been an invited speaker at 20 international conferences. She coordinates the Cervical Overview Group, an International Network that conducts and maintains Cochrane systematic reviews on neck pain and participates in randomized clinical trials on back pain (Welback). She works in private practice OMPT and is a Fellow of the Canadian Academy of Manipulative Physiotherapy (FCAMPT).
Annalie Basson
Annalie Basson is a clinician and part-time lecturer at the University of Witwatersrand, Johannesburg, South Africa working in private practice in Pretoria.
Ken Olson
Ken Olson is the president and co-owner of the physical therapy private practice Northern Rehab Physical Therapy Specialists in DeKalb, Illinois and is adjunct faculty for Northern Illinois University. He is a Past-President of both the International Federation of Orthopaedic Manipulative Physical Therapists (IFOMPT) and the American Academy of Orthopaedic Manual Physical Therapists (AAOMPT).
Oliver Ang
Oliver Ang primary research interests are innovative interventions using digital technologies to address cervical disorders and contextual factors, particularly therapeutic alliance, in physical therapy treatments. He is currently involved in the Spinal Manipulation and Patient Self-Management for Preventing Chronic Back Pain (PACBACK), the Integrated Supported Biopsychosocial Self-Management for Back Related Leg Pain (SUPPORT) and Partners4Pain studies, funded by the US National Institute of Health (NIH). He is a member of the validity assessment team of the Cervical Overview Group.
Nikki Milne
Nikki Milne works as an Associate Professor of Physiotherapy (Paediatrics) at Bond University where she has worked for the past 16 years. Prior to starting work in the academic setting Nikki worked as a Paediatric physiotherapist for NSW Health which led to her research interests in child health and wellbeing and paediatric curriculum. Nikki has a special interest in child health, learning and paediatric physiotherapy and is passionate about the inclusion of paediatric curriculum in entry-level physiotherapy programs, to ensure that all graduates of accredited entry-level programs have knowledge and skills to safely and effectively work with children.
Jan Pool
Jan Pool has worked as Associate Professor Institute of Human Movement Studies, Faculty of Health Care and as a Coordinator/Head of Master Program Physical Therapy division; Orthopedic Manual Therapy. He was senior researcher of Research Group Lifestyle and Health, HU University of Applied Sciences Utrecht, Utrecht, The Netherlands. He worked as a manual therapist for over 30 years in a private clinic. His scientific interest culminated in a master degree in epidemiology in 2003 and a doctorate in medicine in 2007 both at the Free University Amsterdam. He wrote numerous articles on the topics neck pain, chronic pain and manipulative therapy and has a special interest in clinimetry. He was a member of the board of the Dutch Association of Manual therapy in The Netherlands (NVMT), from 1990 till 1998. From 2000-2016 he was a member of the Standard Committee of the International Federation of Manipulative Physical Therapy (IFOMPT).Jan became a member of the Spinal Manipulation Taskforce in 2020.
References
- Chiropractic Board. Chiropractic board of Australia policy statement: interim policy on spinal manipulation for infants and young children; Melbourne, 2019; p. 1–2. Available from: https://www.chiropracticboard.gov.au/Codes-guidelines/Position-statements/Interim-policy-on-spinal-manipulation.aspx.
- Milne N, Longeri L, Patel A, et al. Spinal manipulation and mobilisation in the treatment of infants, children, and adolescents: a systematic scoping review. BioMed Central Pediatr. 2022 Dec;22(1):1–24. doi: 10.1186/s12887-022-03781-6
- McKown S, Acquadro C, Anfray C, et al. Good practices for the translation, cultural adaptation, and linguistic validation of clinician-reported outcome, observer-reported outcome, and performance outcome measures. J Patient-Reported Outcomes. 2020 Dec;4(1):1–8. doi: 10.1186/s41687-020-00248-z
- Mokkink LB, Prinsen C, Patrick DL et al. COSMIN methodology for systematic reviews of patient-reported outcome measures (PROMs). User Manual. 2018 Feb;78(1): 27–29.
- Terwee CB, PrinsenCA,Chiarotto A, de Vet HC, Bouter LM, Alonso J, Westerman MJ, Patrick DL, Mokkink LB. COSIM methodology for assessing the content validity of PROMs – user manual. 2018 http://www/cosmin.nl/.
- Hayton T, Gross AR, Basson A, et al. Psychometric measurement properties of patient-reported and observer-reported outcome measures for spinal mobilisations and manipulation on paediatric subjects with diverse medical conditions: a systematic review. J Manual Manipulative Ther. 2023. in press.
- Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. Syst Rev. 2021 Dec;10(1):1–1. doi: 10.1186/s13643-021-01626-4
- Mokkink LB, Prinsen CA, Patrick DL et al. COSMIN Risk of Bias checklist for systematic reviews of Patient-Reported Outcome Measures. 27. Qual Life Res; 2019. pp. 1171–1179. doi:10.1007/s11136-017-1765-4.
- Terwee CB, Jansma EP, Riphagen II, et al. Development of a methodological PubMed search filter for finding studies on measurement properties of measurement instruments. Qual Life Res. 2009 Oct;18(8):1115–1123. doi: 10.1007/s11136-009-9528-5
- Bartels B, De Groot JF, Terwee CB. The six-minute walk test in chronic pediatric conditions: a systematic review of measurement properties. Phys Ther. 2013 Apr 1;93(4):529–541. doi: 10.2522/ptj.20120210
- D’hondt NE, Pool JJ, Kiers H, et al. Validity of clinical measurement instruments assessing scapular function: insufficient evidence to recommend any instrument for assessing scapular posture, movement, and dysfunction—a systematic review. J Orthop Sports Phys Ther. 2020 Nov;50(11):632–641. doi: 10.2519/jospt.2020.9265
- Aimsamrarn P, Janyachareon T, Rattanathanthong K, et al. Cultural translation and adaptation of the Alberta Infant motor Scale Thai version. Early Hum Dev. 2019 Mar 1;130:65–70. doi: 10.1016/j.earlhumdev.2019.01.018
- Albuquerque PL, Guerra MQF, Lima MC, et al. Concurrent validity of the Alberta Infant motor Scale to detect delayed gross motor development in preterm infants: a comparative study with the Bayley III. Dev Neurorehabil. 2018;21(6):408–414. doi: 10.1080/17518423.2017.1323974
- Almeida KM, Dutra MV, Mello RR, et al. Concurrent validity and reliability of the Alberta Infant motor Scale in premature infants. J Pediatr (Rio J). 2008;84(5):442–448. doi: 10.2223/JPED.1836
- Bartlett DJ, Fanning JEK. Use of the Alberta Infant motor Scale to characterize the motor development of infants born preterm at eight months corrected age. Phys Occup Ther Pediatr. 2003;23(4):31–45. doi: 10.1080/J006v23n04_03
- Blanchard Y, Neilan E, Busanich J, et al. Interrater reliability of early intervention providers scoring the Alberta Infant motor Scale. Pediatr Phys Ther. 2004 Apr 1;16(1):13–18. doi: 10.1097/01.PEP.0000113272.34023.56
- Boonzaaijer M, van Dam E, van Haastert IC, et al. Concurrent validity between live and home video observations using the Alberta Infant motor Scale. Pediatr Phys Ther. 2017 Apr;29(2):146. doi: 10.1097/PEP.0000000000000363
- Campbell SK, Kolobe TH. Concurrent validity of the test of infant motor performance with the Alberta Infant Motor Scale. Pediatr Phys Ther. 2000 Apr 1;12(1):2–9. doi: 10.1097/00001577-200012010-00002
- Campbell SK, Kolobe TH, Wright BD, et al. Validity of the test of Infant motor performance for prediction of 6-, 9- and 12-month scores on the Alberta Infant motor Scale. Dev Med Child Neurol. 2002 Apr;44(4):263–272. doi: 10.1017/S0012162201002043
- Campos D, Santos DC, Gonçalves VM, et al. Agreement between scales for screening and diagnosis of motor development at 6 months. J Pediatr (Rio J). 2006;82(6):470–474. doi: 10.2223/JPED.1567
- Chiquetti EM, Valentini NC, Saccani R. Validation and reliability of the test of infant motor performance for Brazilian infants. Phys Occup Ther Pediatr. 2020 Jul 3;40(4):470–485. doi: 10.1080/01942638.2020.1711843
- Darrah JM. Feasibility of early screening for neuromotor problems in at-risk infants: predictive validity of the Alberta Infant motor Scale. 1996. Available from: https://search.ebscohost.com/login.aspx?direct=true&db=rzh&AN=109842973&scope=site.
- Darrah J, Piper M, Watt MJ. Assessment of gross motor skills of at‐risk infants: predictive validity of the Alberta Infant motor Scale. Dev Med Child Neurol. 1998 Jul;40(7):485–491. doi: 10.1111/j.1469-8749.1998.tb15399.x
- Darrah J, Redfern L, Maguire TO, et al. Intra-individual stability of rate of gross motor development in full-term infants. Early Hum Dev. 1998b Sep 1;52(2):169–179. doi: 10.1016/S0378-3782(98)00028-0
- Darrah J, Bartlett D, Maguire TO, et al. Have infant gross motor abilities changed in 20 years? A re‐evaluation of the Alberta Infant motor Scale normative values. Dev Med Child Neurol. 2014 Sep;56(9):877–881. doi: 10.1111/dmcn.12452
- Dumas HM, Fragala-Pinkham MA, Rosen EL, et al. Pediatric evaluation of Disability Inventory Computer Adaptive Test (PEDI-CAT) and Alberta Infant Motor Scale (AIMS): validity and responsiveness. Phys Ther. 2015 Nov 1;95(11):1559–1568. doi: 10.2522/ptj.20140339
- Fauls JR, Thompson BL, Johnston LM. Validity of the ages and stages questionnaire to identify young children with gross motor difficulties who require physiotherapy assessment. Dev Med Child Neurol. 2020 Jul;62(7):837–844. doi: 10.1111/dmcn.14480
- Fetters L, Tronick EZ. Discriminate power of the Alberta Infant motor Scale and the Movement assessment of infants for prediction of Peabody Gross motor Scale scores of infants exposed in utero to cocaine. Pediatr Phys Ther. 2000 Apr 1;12(1):16–23. doi: 10.1097/00001577-200012010-00004
- Fleuren KM, Smit LS, Stijnen TH, et al. New reference values for the Alberta Infant motor Scale need to be established. Acta Paediatrica. 2007 Mar;96(3):424–427. doi: 10.1111/j.1651-2227.2007.00111.x
- Ga HY, Kwon JY. A comparison of the Korean-ages and stages questionnaires and Denver developmental delay screening test. Ann Rehabil Med. 2011 Jun 30;35(3):369–374. doi: 10.5535/arm.2011.35.3.369
- Harris SR, Backman CL, Mayson TA. Comparative predictive validity of the Harris Infant neuromotor test and the Alberta Infant motor Scale. Dev Med Child Neurol. 2010;52(5):462–467. doi: 10.1111/j.1469-8749.2009.03518.x
- Heineman KR, Bos AF, Hadders‐Algra M. The Infant motor profile: a standardized and qualitative method to assess motor behaviour in infancy. Dev Med Child Neurol. 2008 Apr;50(4):275–282. doi: 10.1111/j.1469-8749.2008.02035.x
- Heineman KR, Middelburg KJ, Bos AF, et al. Reliability and concurrent validity of the Infant motor profile. Dev Med Child Neurol. 2013 Jun;55(6):539–545. doi: 10.1111/dmcn.12100
- Hoskens J, Klingels K, Smits-Engelsman B. Validity and cross-cultural differences of the Bayley scales of Infant and toddler development, third Edition in typically developing infants. Early Hum Dev. 2018 Oct 1;125:17–25.45. doi: 10.1016/j.earlhumdev.2018.07.002
- Jeng SF, Yau KI, Chen LC, et al. Alberta Infant Motor Scale: reliability and validity when used on preterm infants in Taiwan. Phys Ther. 2000 Feb 1;80(2):168–178. doi: 10.1093/ptj/80.2.168
- Krosschell KJ, Bosch M, Nelson L, et al. Motor function test reliability during the NeuroNEXT spinal muscular atrophy infant biomarker study. JND. 2018 Jan 1;5(4):509–521. doi: 10.3233/JND-180327
- Lackovic M, Nikolic D, Filimonovic D, et al. Reliability, consistency and temporal stability of Alberta Infant motor Scale in Serbian infants. Children. 2020 Mar 2;7(3):16. doi: 10.3390/children7030016
- Lefebvre F, Gagnon MM, Luu TM, et al. In extremely preterm infants, do the Movement assessment of infants and the Alberta Infant motor Scale predict 18-month outcomes using the Bayley-III? Early Hum Dev. 2016 Mar 1;94:13–17. doi: 10.1016/j.earlhumdev.2016.01.012
- Morales-Monforte E, Bagur-Calafat C, Suc-Lerin N, et al. The Spanish version of the Alberta Infant Motor Scale: validity and reliability analysis. Dev Neurorehabil. 2017 Feb 17;20(2):76–82. doi: 10.3109/17518423.2015.1066461
- Pai-Jun ML, Campbell SK. Examination of the item structure of the Alberta Infant motor Scale. Pediatr Phys Ther. 2004 Apr 1;16(1):31–38. doi: 10.1097/01.PEP.0000114843.92102.98
- Pin TW, De Valle K, Eldridge B, et al. Clinimetric properties of the Alberta Infant Motor Scale in infants born preterm. Pediatr Phys Ther. 2010 Oct 1;22(3):278–286. doi: 10.1097/PEP.0b013e3181e94481
- Pin TW, Butler PB, Cheung HM, et al. Longitudinal development of segmental trunk control in full term and preterm infants-a pilot study: part II. Dev Neurorehabil. 2020 Apr 2;23(3):193–200. doi: 10.1080/17518423.2019.1629661
- Piper MC, Pinnell LE, Darrah J, et al. Construction and validation of the Alberta Infant motor Scale (AIMS). Can J Public Health = Revue Canadienne de Sante Publique. 1992 Jul 1;83:S46–50.
- Rizzi R, Menici V, Cioni ML, et al. Concurrent and predictive validity of the infant motor profile in infants at risk of neurodevelopmental disorders. BMC Pediatr. 2021 Dec;21(1):1–1. doi: 10.1186/s12887-021-02522-5
- Saccani R, Valentini NC. Reference curves for the Brazilian Alberta Infant motor Scale: percentiles for clinical description and follow-up over time. J Pediatr (Rio J). 2012;88:40–47. doi: 10.2223/JPED.2142
- Quezada-Villalobos L, Soto-García I, Escobar-Cabello M, et al. ‘Confiabilidad interevaluador’ de la Escala Motora Infantil de Alberta en niños de término y pretérmino de la provincia de Talca - Chile. Revista Ciencias de la Salud. 2010;8(2):21–32.
- Siegle CB, de Sá CD. Concurrent validity between instruments of assessment of motor development in infants exposed to HIV. Infant Behav Dev. 2018 Feb 1;50:198–206. doi: 10.1016/j.infbeh.2018.01.005
- Silva LP, Maia PC, Lopes MM, et al. Intraclass reliability of the Alberta Infant motor Scale in the Brazilian version. Revista da Escola de Enfermagem da USP. 2013;47(5):1046–1051. doi: 10.1590/S0080-623420130000500006
- Spittle AJ, Doyle LW, Boyd RN. A systematic review of the clinimetric properties of neuromotor assessments for preterm infants during the first year of life. Dev Med Child Neurol. 2008 Apr;50(4):254–266. doi: 10.1111/j.1469-8749.2008.02025.x
- Suir I, Boonzaaijer M, Nijmolen P, et al. Cross-cultural validity: Canadian norm values of the Alberta Infant motor Scale evaluated for Dutch infants. Pediatr Phys Ther. 2019 Oct 1;31(4):354–358. doi: 10.1097/PEP.0000000000000637
- Syrengelas D, Kalampoki V, Kleisiouni P, et al. Alberta Infant motor Scale (AIMS) performance of Greek preterm infants: comparisons with full-term infants of the same nationality and impact of prematurity-related morbidity factors. Phys Ther. 2016 Jul 1;96(7):1102–1108. doi: 10.2522/ptj.20140494
- Syrengelas D, Siahanidou T, Kourlaba G, et al. Standardization of the Alberta Infant Motor Scale in full-term Greek infants: preliminary results. Early Hum Dev. 2010 Apr 1;86(4):245–249. doi: 10.1016/j.earlhumdev.2010.03.009
- Tse L, Mayson TA, Leo S, et al. Concurrent validity of the Harris Infant neuromotor test and the Alberta Infant motor Scale. J Pediatr Nurs. 2008 Feb 1;23(1):28–36. doi: 10.1016/j.pedn.2007.07.009
- Tupsila R, Bennett S, Mato L, et al. Gross motor development of Thai healthy full-term infants aged from birth to 14 months using the Alberta Infant motor Scale: inter individual variability. Early Hum Dev. 2020 Dec 1;151:105169. doi: 10.1016/j.earlhumdev.2020.105169
- Valentini NC, Saccani R. Escala Motora Infantil de Alberta: validação para uma população gaúcha. Rev Paulista Pediatria. 2011;29(2):231–238. doi: 10.1590/S0103-05822011000200015
- Valentini NC, Saccani R. Brazilian validation of the Alberta Infant Motor Scale. Phys Ther. 2012 Mar 1;92(3):440–447. doi: 10.2522/ptj.20110036
- van Hus JW, Jeukens-Visser M, Koldewijn K, et al. Comparing two motor assessment tools to evaluate neurobehavioral intervention effects in infants with very low birth weight at 1 year. Phys Ther. 2013 Nov 1;93(11):1475–1483. doi: 10.2522/ptj.20120460
- van Schie PE, Becher JG, Dallmeijer AJ, et al. Motor testing at 1â??year improves the prediction of motor and mental outcome at 2â??years after perinatal hypoxicâ??ischaemic encephalopathy. Dev Med Child Neurol. 2010 Jan;52(1):54–59. doi: 10.1111/j.1469-8749.2009.03302.x
- Wang H, Li H, Wang J, et al. Reliability and concurrent validity of a Chinese version of the Alberta Infant motor Scale administered to high-risk infants in China. Bio Med Res Int. 2018 Jun 13;2018:1–10. doi: 10.1155/2018/2197163.
- Yeh KK, Liu WY, Wong AM, et al. Validity of general movement assessment based on clinical and home videos. Pediatr Phys Ther. 2020 Jan 1;32(1):35–43. doi: 10.1097/PEP.0000000000000664
- Adams D, Hewell S. Maternal and professional assessment of breastfeeding. J Hum Lact. 1997 Dec;13(4):279–283. doi: 10.1177/089033449701300412
- Altuntas N, Turkyilmaz C, Yildiz H, et al. Validity and reliability of the infant breastfeeding assessment tool, the mother baby assessment tool, and the LATCH scoring system. Breast Feeding Med. 2014 May 1;9(4):191–195. doi: 10.1089/bfm.2014.0018
- Chapman DJ, Doughty K, Mullin EM, et al. Reliability of lactation assessment tools applied to overweight and obese women. J Hum Lact. 2016 May;32(2):269–276. doi: 10.1177/0890334415597903
- DaConceição CM, Coca KP, Alves MD, et al. Validação para língua portuguesa do instrumento de avaliação do aleitamento materno LATCH. Acta Paul Enferm. 2017 Mar;30(2):210–216. doi: 10.1590/1982-0194201700032
- DaConceição CM, Nur M, De Amorim, et al. Cultural adaptation of breastfeeding assessment tool to the Portuguese language: ‘latch’. Pediatrics. 2018;141(1_MeetingAbstract):286. doi: 10.1542/peds.141.1MA3.286
- Dolgun G, İ̇nal S, Erdim L, et al. Reliability and validity of the Bristol breastfeeding assessment tool in the Turkish population. Midwifery. 2018 Feb 1;57:47–53. doi: 10.1016/j.midw.2017.10.007
- Kumar SP, Mooney R, Wieser LJ, et al. The LATCH scoring system and prediction of breastfeeding duration. J Hum Lact. 2006 Nov;22(4):391–397. doi: 10.1177/0890334406293161
- Lau Y, Htun TP, Lim PI, et al. Psychometric evaluation of 5-and 4-item versions of the LATCH breastfeeding assessment tool during the initial postpartum period among a multiethnic population. PLoS One. 2016 May 2;11(5):e0154331. doi: 10.1371/journal.pone.0154331
- Riordan JM, Koehn M. Reliability and validity testing of three breastfeeding assessment tools. J Obstet Gynaecol Gynecologic Neonatal Nur. 1997 Mar 1;26(2):181–187. doi: 10.1111/j.1552-6909.1997.tb02131.x
- Adam CJ, Izatt MT, Harvey JR, et al. Variability in Cobb angle measurements using reformatted computerized tomography scans. Spine. 2005 Jul 15;30(14):1664–1669. doi: 10.1097/01.brs.0000169449.68870.f8
- Al-Bashir AK, Al-Abed MA, Amari HK, et al. Computer-based Cobb angle measurement using deflection points in adolescence idiopathic scoliosis from radiographic images. Neural Comput Appl. 2019 May;31(5):1547–1561. doi: 10.1007/s00521-018-3614-y
- Allen S, Parent E, Khorasani M, et al. Validity and reliability of active shape models for the estimation of cobb angle in patients with adolescent idiopathic scoliosis. J Digit Imaging. 2008 Jun;21(2):208–218. doi: 10.1007/s10278-007-9026-7
- Brink RC, Wijdicks SPJ, Tromp IN, et al. A reliability and validity study for different coronal angles using ultrasound imaging in adolescent idiopathic scoliosis. Spine J. 2018 Jun 1;18(6):979–985. doi: 10.1016/j.spinee.2017.10.012
- De Carvalho A, Vialle R, Thomsen L, et al. Reliability analysis for manual measurement of coronal plane deformity in adolescent scoliosis. Are 30× 90 cm plain films better than digitized small films? Eur Spine J. 2007 Oct;16(10):1615–1620. doi: 10.1007/s00586-007-0437-4
- Gstoettner M, Sekyra K, Walochnik N, et al. Inter- and intraobserver reliability assessment of the Cobb angle: manual versus digital measurement tools. Eur Spine J. 2007 Oct;16(10):1587–1592. doi: 10.1007/s00586-007-0401-3
- Kumar VP, Thomas T, Menon KV. Content-based image retrieval of spine radiographs with scoliosis. Clin Spine Surg. 2009 Jun 1;22(4):284–289. doi: 10.1097/BSD.0b013e31816d8148
- Livanelioglu A, Kaya F, Nabiyev V, et al. The validity and reliability of “spinal mouse” assessment of spinal curvatures in the frontal plane in pediatric adolescent idiopathic thoraco-lumbar curves. Eur Spine J. 2016 Feb;25(2):476–482. doi: 10.1007/s00586-015-3945-7
- Loder RT, Spiegel D, Gutknecht S, et al. The assessment of intraobserver and interobserver error in the measurement of noncongenital scoliosis in children≤ 10 years of age. Spine. 2004 Nov 15;29(22):2548–2553. doi: 10.1097/01.brs.0000144828.72721.d8
- Marchetti BV, Candotti CT, Raupp EG, et al. Accuracy of a radiological evaluation method for thoracic and lumbar spinal curvatures using spinous processes. J Manipulative Physiol Ther. 2017 Nov 1;40(9):700–707. doi: 10.1016/j.jmpt.2017.07.013
- Mehta SS, Modi HN, Srinivasalu S, et al. Interobserver and intraobserver reliability of Cobb angle measurement: endplate versus pedicle as bony landmarks for measurement: a statistical analysis. J Pediatr Orthop. 2009 Oct 1;29(7):749–754. doi: 10.1097/BPO.0b013e3181b72550
- Pruijs JE, Stengs C, Keessen W. Parameter variation in stable scoliosis. Eur Spine J. 1995 Jun;4(3):176–179. doi: 10.1007/BF00298242
- Safari A, Parsaei H, Zamani A, et al. A semi-automatic algorithm for estimating cobb angle. J Biomed Phys Eng. 2019 Jun 1;9(3):317–326. doi: 10.31661/jbpe.v9i3Jun.730
- Stokes IA, Aronsson DD. Computer-assisted algorithms improve reliability of King classification and Cobb angle measurement of scoliosis. Spine. 2006 Mar 15;31(6):665–670. doi: 10.1097/01.brs.0000203708.49972.ab
- Xiaohua MH, KyeongAh J, HanSuk H, et al. A comparison of the validity and reliability between a digital radiographic imaging system and manual method in measuring the Cobb angle. Scoliosis. 2013 Sep;8(S2):1–2. doi: 10.1186/1748-7161-8-S2-O20
- Watson AW, Mac Donncha C. A reliable technique for the assessment of posture: assessment criteria for aspects of posture. J Sports Med Phys Fitness. 2000 Sep 1;40(3):260.
- Snyder P, Eason JM, Philibert D, et al. Concurrent validity and reliability of the Alberta Infant motor Scale in infants at dual risk for motor delays. Phys Occup Ther Pediatr. 2008 Jan 1;28(3):267–282. doi: 10.1080/01942630802224892
- Spittle AJ, Lee KJ, Spencer-Smith M, et al. Accuracy of two motor assessments during the first year of life in preterm infants for predicting motor outcome at preschool age. PLoS One. 2015 May 13;10(5):e0125854. doi: 10.1371/journal.pone.0125854
- Prinsen CA, Mokkink LB, Bouter LM, et al. COSMIN guideline for systematic reviews of patient-reported outcome measures. Qual Life Res. 2018 May;27(5):1147–1157. doi: 10.1007/s11136-018-1798-3
- Spittle AJ, Lee KJ, Spencer-Smith M, Lorefice LE, Anderson PJ, Doyle LW. Accuracy of two motor assessments during the first year of life in preterm infants for predicting motor outcome at preschool age. PLoS One. 2015 May 13;10(5):e0125854.
- Snyder P, Eason JM, Philibert D, Ridgway A, McCaughey T. Concurrent validity and reliability of the Alberta Infant Motor Scale in infants at dual risk for motor delays. Physical & occupational therapy in pediatrics. 2008 Jan 1;28(3):267–82.
- Báez León C, Blasco Contreras R, Martín Sequeros E, del Pozo Ayuso ML, Sánchez Conde AI, Vargas Hormigos C. Validation of the LATCH assessment tool into Spanish. Reliability analysis. Index de Enfermería. 2008;17(3):205–9.
- Watson AW, Mac Donncha C. A reliable technique for the assessment of posture: assessment criteria for aspects of posture. Journal of sports medicine and physical fitness. 2000 Sep 1;40(3):260.
- Santesso N, Glenton C, Dahm P, et al. GRADE guidelines 26: informative statements to communicate the findings of systematic reviews of interventions. J Clinical Epidemiol. 2020 Mar 1;119:126–135. doi: 10.1016/j.jclinepi.2019.10.014
- Báez León C, Blasco Contreras R, Martín Sequeros E, et al. Validación al castellano de una escala de evaluación de la lactancia materna: el LATCH. Análisis de fiabilidad. Index Enferm. 2008;17(3):205–209. doi: 10.4321/S1132-12962008000300012
- Jensen D, Wallace S, Kelsay P. LATCH: a breastfeeding charting system and documentation tool. J Obstet Gynaecol Gynecologic Neonatal Nur. 1994 Jan;23(1):27–32. doi: 10.1111/j.1552-6909.1994.tb01847.x
- Corso M, Cancelliere C, Mior S, et al. The safety of spinal manipulative therapy in children under 10 years: a rapid review. Chiropr Man Therap. 2020 Dec;28(1):1–8. doi: 10.1186/s12998-020-0299-y
- Ellwood J, Draper-Rodi J, Carnes D. The effectiveness and safety of conservative interventions for positional plagiocephaly and congenital muscular torticollis: a synthesis of systematic reviews and guidance. Chiropr Man Therap. 2020 Dec;28(1):1–1. doi: 10.1186/s12998-020-00321-w
- Alcantara J, Alcantara JD, Alcantara J. The chiropractic care of infants with breastfeeding difficulties. Explore. 2015 Nov 1;11(6):468–474. doi: 10.1016/j.explore.2015.08.005
- Hawk C, Minkalis A, Webb C, et al. Manual interventions for musculoskeletal factors in infants with suboptimal breastfeeding: a scoping review. J Evid Based Complementary Altern Med. 2018 Dec 11;23:2515690X18816971. doi: 10.1177/2515690X18816971
- Miller JE, Miller L, Sulesund AK, et al. Contribution of chiropractic therapy to resolving suboptimal breastfeeding: a case series of 114 infants. J Manipulative Physiol Ther. 2009 Oct 1;32(8):670–674. doi: 10.1016/j.jmpt.2009.08.023
- Fry LM. Chiropractic and breastfeeding dysfunction: a literature review. J Clin Chiropractic Pediatr. 2014 Mar;14(2):1151–1155.
- Herzhaft-Le Roy J, Xhignesse M, Gaboury I. Efficacy of an osteopathic treatment coupled with lactation consultations for infants’ biomechanical sucking difficulties: a randomized controlled trial. J Hum Lact. 2017 Feb;33(1):165–172. doi: 10.1177/0890334416679620
- Albuquerque PL, Lemos A, Guerra MQ, et al. Accuracy of the Alberta Infant motor Scale (AIMS) to detect developmental delay of gross motor skills in preterm infants: a systematic review. Dev Neurorehabil. 2015 Jan 2;18(1):15–21. doi: 10.3109/17518423.2014.955213
- Mokkink LB, Terwee CB, Knol DL, et al. The COSMIN checklist for evaluating the methodological quality of studies on measurement properties: a clarification of its content. BMC Med Res Methodol. 2010 Dec;10(1):1–8. doi: 10.1186/1471-2288-10-22
- Kjølbye CB, Drivsholm TB, Ertmann RK, et al. Motor function tests for 0-2-year-old children - a systematic review. Dan Med J. 2018 Jun 1;65(6):A5484.