
ABSTRACT
Neuroscience can provide evidence in some cases of legal matters, despite its tenuous nature. Among others, arguing for diminished capacity, insanity, or pleading for mitigation is the most frequent use of neurological evidence in the courtroom. While there is a plethora of studies discussing the moral and legal matters of the practice, there is a lack of studies examining specific cases and the subsequent applications of brain knowledge. This study details the capital punishment trial of Kelvin Lee Coleman Jr., charged in 2013 with double murder in Tampa, Florida, to illustrate the extent that expert opinions – based on neuroimaging, neurological, and neuropsychiatric examinations – had an impact on the court’s decisions. The defendant was sentenced to life imprisonment without the possibility of parole. According to the comments of the trial’s jury, the most influential reason for not sentencing the defendant to death is the fact that during the incident was that he was under extreme mental and emotional disturbance. Other reasons were evidence of brain abnormalities resulting from neurological insult, fetal alcohol syndrome, and orbitofrontal syndrome contributing to severely abnormal behavior and lack of impulse control.
Introduction
The rapid development of neurosciences and technology has yet to unravel all the mysteries of the brain and mind. The neuroscientific toolbox is not yet well established despite its wide usability to numerous ends, nor is it static due to its constant advancement. Therefore, the usability and credibility of new tools must be constantly evaluated. This might be the reason why the use of neuroscience, neuropsychology, and neurology in the legal field is one of the most debatable legal matters right now. Despite the debate, in many cases, neuroscientific evidence is admissible for a spectrum of purposes. Among them, arguing for diminished capacity, insanity, or pleading for mitigation is the most frequent use of neurological evidence in the courtroom (Farahany, Citation2016; Seiden, Citation2004). Such evidence can impact the outcome of trials and in some cases may be influential in deciding between life and death (Miller, Citation2010). The potential significance of its impact is reflected upon the presence of structural brain scans in the vast majority of capital case courtrooms (Aono et al., Citation2019). However, the real significance of its impact remains variable and it is yet to be established. Previous studies have shown differential persuasiveness for different disorders. For instance, defendants diagnosed as psychopathic received fewer sentences to death when brain scans were presented at the court, but schizophrenic defendants received increased judgments of responsibility(Saks et al., Citation2014). Considering that in many cases neurological evidence draws the line between life and death, the establishment of clear guidelines is imperative. Here, through the lens of a case study, we evaluate the extent to which neuroscientific evidence can be persuasive and trustworthy enough for use as mitigating evidence in capital punishment cases.
Despite the wide admissibility of brain-related evidence, some considerations should be addressed (Rusconi & Mitchener-Nissen, Citation2013). First, neuroscience, at least in its current state of research, cannot challenge the basic premise of criminal law that choosing to commit a crime is blameworthy (Slobogin, Citation2017). Second, neuroimaging and statistical analyses can be persuasive (McCabe & Castel, Citation2008), especially to the nonspecialist eye, but are based on the result of the scientists’ manipulations, assumptions, and interpretations that should be made obvious. Consequently, it is the responsibility of the scientist expert witness to understand and explain the limitations of neuroscientific tools and take responsibility for their interpretation. Equally important, is that the judges and lawyers are informed and up to date with the developments in the neuroscientific field to be able to consider the validity of the science presented and the credibility of the expert witness. The purpose of the neuroscientist as an expert witness is to present pieces of evidence without judging the guilt of the individual. Neuroscience can in some cases offer a partial possible explanation of human behavior, but the normative question of mitigation is up to the judgment of the lawmakers, judge, or jury. For instance, it is not in the scope of neuroscience to assess the relationship between the lack of capacity or insanity and the justification of mitigation.
The literature body on the intersection of neuroscience and law, especially the section concerning the morality of the practice, does not cease to expand in parallel with the increased and diverse use of neuroscientific evidence during trials (Shen, Citation2016). However, there is currently a lack of studies integrating a specific case and its neuroscientific evidence. Case studies can serve as examples of the integration of neuroscience in the legal field or specific cases, as well as triggers the dialogue on the standardized and responsible use of neuroscience in the legal field. Furthermore, the implications of case studies could benefit brain scientists, judges, jurors, and legal scholars among others. The present study utilizes the case of State of Florida v. Kelvin Lee Coleman Jr. No. 2013-CF-000851-A-W to illustrate the extent to which expert opinions -based on neuroimaging, neurological, and neuropsychological examinations- had an impact on the court’s decisions. This study does not look into the legal aspect of deciding on guiltiness, nor on the sentence, instead, it is primarily concerned with the role and methodology of the science presented in court.
The relevance of brain-related evidence in a courtroom is strictly tied to its nature. It might be considered relevant in affecting the judge’s or the jury’s favor. However, the ‘genuine’ relevance of neuroscience and therefore its admissibility and usefulness are harder to establish as described by Slobogin (Citation2017) where five types of relevant neuroscientific evidence are identified. Firstly, evidence that the defendant has a neurological impairment or neurological abnormality. Secondly, evidence that this impairment is a common cause of criminal activity. For instance, a research study showing an increased occurrence of specific neurological abnormalities among criminals. The third type of evidence is a link supporting that the neurological impairment predisposed the defendant to commit the crime. For instance, a study showing that when people with neurological impairment at stake are compared to normal controls, those with the impairment are more likely to commit a crime. The fourth type of evidence is a neuropsychological comparison of the defendant against a known control performance baseline. Last, the above-mentioned neuropsychological evidence must be comparable with impairments that the law recognizes as mitigating. Examples would be previous similar cases that evaded death sentence rulings or exhibited similarities with a mental state for which a death sentence is unconstitutional such as that of a minor. While, the first, fourth, and fifth types of evidence mentioned above were presented to the court by the experts during the trials of the case in question, we also present studies falling under the second and fourth types of evidence as they were considered complementary for the discussion of the matter in this study.
We first describe the events leading to the trial of the defendant, followed by his neurological and neurophysiological assessment. How neuroscience was used and to what extent it had an impact is discussed along with the court outcome.
Case study: events and courtroom proceedings
On 12 March 2013, an argument took place between, Penny Coleman, a resident of the Vacation Host Inn located at Ocala, Florida, since January 2013, Rebecca Crew, a motel employee concerning Mrs. Coleman’s children riding their bikes near the motel’s windows. Based on the police reports examined, Mrs. Coleman called her husband informing him about the argument, and later in the day, the Marion County Sheriff’s Office was called by a front office clerk at the inn to investigate a confrontation between Mr. Coleman and the front office staff at the Vacation Host Inn. The police saw no evidence of a direct threat and left the scene. As multiple witnesses testified, five hours later, Mr. Coleman returned to the inn and fired twice at Lester Carter, resident, and maintenance man at the inn, once at Glendora Johnson, a maid at the inn, and a final time at an occupied room. Mr. Carter and Ms. Johnson succumbed to their injuries. Mr. Coleman was arrested after authorities found bullets, matching the ones found at the scene while searching his mother’s house where he was located shortly after the incident. The murder weapon was never located, and Mr. Coleman claimed he was innocent.
In the case, 2013-CF-000851-W, The State of Florida v. Kelvin Lee Coleman Jr., Mr. Coleman was accused of two counts of first-degree murder and attempted first-degree murder which warranted the death penalty. During the trial, expert testimonies informed the jury of potential mitigating factors that might have substantially impaired the capacity of the defendant to conform his conduct to the requirement of law and to understand and appreciate the criminality of his actions. To this end, positron emission tomography (PET) brain scans, diffusion tensor imaging (DTI) scans, and quantitative volumetrics (QV) were used along with neuropsychological exams and complete neurological evaluation. The neuroimaging analysis showed patterns consistent with traumatic brain injury (TBI), fetal alcohol spectrum disorder (FASD), and a presumptive case of chronic traumatic encephalopathy (CTE). Upon the recommendation of the jury, the court sentenced Mr. Coleman to life imprisonment without the possibility of parole.
The methodology of the neurological and neuropsychological assessment
The neuroimaging methods used were chosen per the neuropsychological exams as the most appropriate means of analyzing the specific neuropathology. The magnetic resonance imaging scans were collected on 14 September 2016 (roughly six months after the incident) at Rose Radiology Tampa, Florida, using a 3 Tesla MRI scanner.
Fluorodeoxyglucose (18F-FDG) PET scans were used to compare the glucose uptake of the defendant’s brain with healthy controls. PET scans are widely used in clinical settings to assess regional brain metabolism in a wide variety of conditions and to discriminate between abnormal scans from normal controls. The technique can be used to detect abnormalities associated with a fetal alcohol spectrum disorder, TBI, and CTE (Alavi & Newberg, Citation1996; Barrio et al., Citation2015; Byrnes et al., Citation2014; Clark et al., Citation2000; Coles & Li, Citation2011; Kato et al., Citation2007; Langfitt et al., Citation1986; Roberts et al., Citation1995; Sundman et al., Citation2015). On several occasions, PET scans have been subjected to Daubert and Frye challenges and have prevailed (California vs. Miguel Carrizalez. No. VCF-169926-C Kelly-Frye hearing, 261–262, 18–19 November 2010) (Rushing & Langleben, Citation2011). Areas of significantly abnormal positive or negative metabolic activity (z-score ≤ 0.05) were identified after comparison with the images of 16 neurologically normal controls. The controls’ age and sex were matched to the defendant. Positive and negative Z-Maps were constructed using Statistical Parametric Mapping (SPM) (Wellcome Department of Imaging Neuroscience, University College London). The defendant’s brain metabolic activity was then compared to previous findings in the FDG-PET, MRI, and computerized tomography literature regarding FASD, TBI, and CTE (Alavi & Newberg, Citation1996; Barrio et al., Citation2015; Byrnes et al., Citation2014; Clark et al., Citation2000; Coles & Li, Citation2011; Kato et al., Citation2007; Langfitt et al., Citation1986; Roberts et al., Citation1995; Sundman et al., Citation2015). Statistical comparisons were performed both on the whole brain level as well as for specific regions of interest, including the cerebellum and the neocortical region. Such statistical analysis of regions of interest (ROIs) can complement the evaluation of the neurologist (Bowman et al., Citation2007). Also, such analysis was shown to yield more accurate results and be more sensitive in the detection of smaller metabolic abnormalities as compared to a non-quantitative visual inspection of an image for Alzheimer’s disease patients (Partovi et al., Citation2017).
Moreover, diffusion-weighted MRI DTI scans were used. The defendant’s DTI scans were compared to the scans of 12 controls which were neurologically normal and matched the defendant’s age and sex (). DTI scans can detect abnormal fractional anisotropy due to brain injury (Asken et al., Citation2018; Lipton et al., Citation2012; Lo et al., Citation2009), FASD (Donald et al., Citation2015; Fan et al., Citation2016; Ma et al., Citation2005; Wozniak et al., Citation2006), or as early indicators of CTE by assessing the white matter tract integrity which is associated with the disorder with a generally low error rate (Assaf & Pasternak, Citation2008; Galgano et al., Citation2016; Johnson et al., Citation2013; Stern et al., Citation2013; Wang et al., Citation2008). DTI scans have been repeatedly admissible to courts and prevailed to Daubert and Frye challenges (Jungbauer & Bowman, Citation2014).Footnote1,
Furthermore, based on the MRI data collected, specific regions of the defendant’s brain were assessed volumetrically using the NeuroQuant (NQ) quantitative volumetric software. The program quantified the defendant’s overall brain and specific area volume in cm3 and computed the percentage of intracranial volume (Luo et al., Citation2015). Statistical comparative analysis was performed between the defendant’s data and 17 age and sex-matched controls with neurologically normal brain scans. QV is useful in computing regional and total brain volumes from neuroimaging scans. Although it is a relatively new method, it provides a valuable contribution of precision to brain volumetric study and analysis. The use of the NQ software enabled the use of highly replicable data to assess the various brain volumes of the defendant’s brain (Ross et al., Citation2012, Citation2013). Furthermore, NQ is believed to be more sensitive than visual inspection by a neurologist (Lebel et al., Citation2011; Ross et al., Citation2012, Citation2013), even though literature regarding FASD, TBI, and CTE volumes are performed using predominantly human experts’ image analysis procedures (Archibald et al., Citation2001; Li et al., Citation2008), a combination of software for image analysis (i.e. FreeSurfer) and visual examination by experts (Dickstein et al., Citation2016; Treit et al., Citation2017), or software alone (Kornguth et al., Citation2017).
The neuropsychological tests administered included evaluation of intelligence by the Wechsler Abbreviated Scale of Intelligence – Second Edition (WAIS-II) and the Wechsler Adult Intelligence Scale – Fourth Edition (WAIS-IV). Moreover, the Woodcock-Johnson Achievement Testing, the Woodcock-Johnson Cognitive Ability Testing, the Wechsler Memory ScaleIV (WMS-IV), the Visual Memory Test (VMT), and the Continuous Visual Memory Test (CVMT) were used to assess the defendant’s memory. The tests were administered on the 7th and 8th of April 2016 (roughly two months after the incident) by a licensed psychologist specializing in forensic psychology. Although the defendant had provided his written consent, two attempts to administer the exams were unsuccessful due to the defendant’s noncompliance. The administering psychologist reported that despite his occasionally guarded behavior, he gave his full effort while completing the test. Additional tests administered included the finger tapping test, the Rey Complex Figure and Recognition Trial (RCFT), the Personality Assessment Inventory, and the Validity Indicator Profile, as well as several subtests of the Delis-Kaplan Executive Function System (D-KEFS).
Overall, the results of brain scans and neuropsychological tests supplemented by the defendant’s personal medical history, family medical history, and reports of past behavior were interpreted by a neurologist, a psychiatrist, and two licensed psychologists.
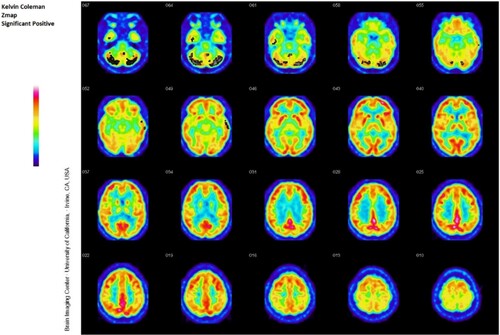
Figure 2. Quantitative Z-map statistical analysis of the defendant’s PET scan. Areas showing abnormal positive activation as compared to age and gender-matched controls are shown in black. The above z-map shows significant positive metabolic values in the cerebellum.
Results and diagnosis
Brain imaging and statistical analyses
The PET scans’ statistical comparison of regions of interest showed a significantly increased metabolic activity (p-value = 3.6 × 10−3) of the cerebellum (see ). The neocortex showed a normal metabolic activity as compared to the metabolic activity of the control population’s neocortex. However, the defendant’s ratio of metabolic activity of the neocortex to the metabolic activity of the cerebellum, was significantly smaller (p-value ≤ 0.05) than that of age and gender-matched controls. The decreased neocortical to cerebellar activity ratio in combination with the increased cerebellum metabolic activity is an indication of TBI (Madsen et al., Citation2017). Decreased activity in the thalamus is evidence of FAS. The defendant’s right thalamus was within the range for normal metabolic activity, but when compared to age and gender-matched controls, the ratio of the right thalamus to cerebellar activity was significantly smaller (p-value ≤ 0.05).
Figure 3. Neocortical to Cerebellum Region of Interest (ROI) analysis of the defendant. The defendant’s cerebellum is pictured on the left. Increased metabolic rate in the cerebellum (left) is indicated by gray and black areas according to the intensity. The statistical comparisons with controls yielded a significantly increased metabolic activity (p-value = 3.6 × 10−3). The patient’s neocortex (right) shows a normal rate of metabolic activity. This patient has a decreased neocortical to cerebellar activity ratio as indicated in the tables below.
The DTI scan, showed decreased fractional anisotropy (FA) as a function of white matter integrity in the mid posterior corpus callosum and pons regions of the brain () which further points to a diagnosis of FASD (Donald et al., Citation2015; Fan et al., Citation2016). FASD cerebral volume studies have reported a collection of decreases, notably total brain volume, the forebrain, and deep gray matter structures (Archibald et al., Citation2001; Donald et al., Citation2015; Fan et al., Citation2016; Lebel et al., Citation2011; Li et al., Citation2008; Treit et al., Citation2017). The significance of decreases in forebrain volumes lies in the importance of the forebrain, especially of the prefrontal cortex and its development, in executive function (Diamond, Citation2013).
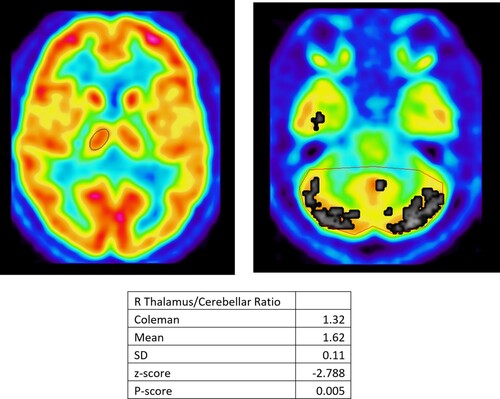
Figure 4. Right Thalamus to Cerebellar Ratio, Region of Interest (ROI) analysis. The right thalamus is pictured on the left. The cerebellum is pictured on the right. The defendant’s right thalamus would appear to be within range for normal metabolic activity, compared to age gender-matched controls, displayed by the absence of black/gray regions. The defendant’s cerebellum appears to be functioning at a higher than normal activity level when compared to age gender-matched controls, displayed by the presence of gray/black regions. However, when taking the ratio of the right thalamus to cerebellar activity, the defendant has a significant (P-score ≤ 0.05) decreased ratio of activity compared to age, gender-matched controls. Decreased activity in the thalamus is evidence of FAS.
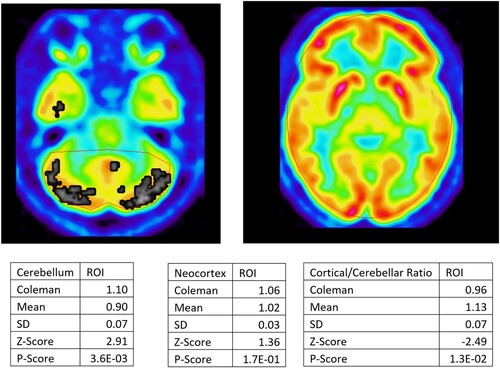
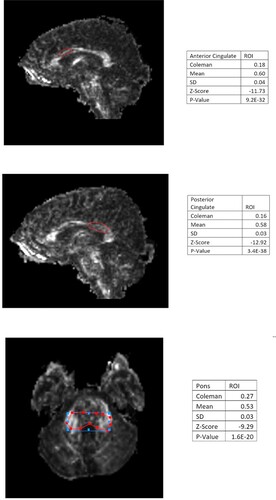
Figure 1. Diffusion Tensor Imaging (DTI) Statistical Analysis. DTI scans of the defendant were compared to scans of 12 age gender-matched controls. Regions of the defendant’s brain that have a significantly decreased Fractional Anisotropy (FA) value compared to controls were outlined in red, using Vinci. On the left, is the statistical analysis summary of the corresponding region. (A) Mr. Coleman’s anterior cingulate has an FA value of 0.18 compared to the control average FA value of 0.60. This is 11.73 standard deviations away from the average FA value of the control population’s anterior cingulate. (B) The defendant’s posterior cingulate has an FA value of 0.16 compared to the control average FA value of 0.58. This is 12.92 standard deviations away from the average FA value of the control population’s anterior cingulate. (C) The defendant’s pons has an FA value of 0.27 compared to the control average FA value of 0.53. This is 9.29 standard deviations away from the average FA value of the control population’s anterior cingulate. The statistically significant decreases in FA in the anterior cingulate, posterior cingulate, and pons are evidence of TBI.
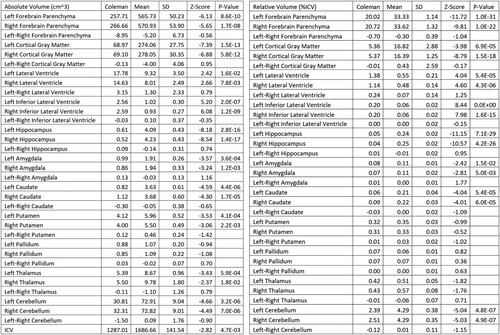
QV analysis showed that the defendant had a significantly lower than normal brain volume compared to the age and sex-matched controls. Many specific brain areas showed deficits. Specifically, a significant (p < 8.6×10−10) volumetric deficit of the defendant’s left forebrain parenchyma was shown with a volume of 257.71 cm3 as compared to the mean 565.73 cm3 of the control group. Other significant volumetric deficits were seen in the cortical gray matter, ventricles, hippocampus amygdala, caudate, putamen, thalamus, and cerebellum (see ). Reduced brain volume in general, as well as in the specific areas reported above, may contribute to decreased executive function, memory, and impaired ability to regulate or understand his aggressive actions (Elderkin-Thompson et al., Citation2008). They also indicate FASD (Donald et al., Citation2015; Lebel et al., Citation2011; Ma et al., Citation2005; Treit et al., Citation2017). The MRI DTI, MRI quantitative volumetrics, and PET scans were consistent with the defendant having had sustained a traumatic brain injury (Alavi & Newberg, Citation1996; Asken et al., Citation2018; Byrnes et al., Citation2014; Johnson et al., Citation2013; Kato et al., Citation2007; Langfitt et al., Citation1986; Lipton et al., Citation2012; Lo et al., Citation2009; Roberts et al., Citation1995; Sundman et al., Citation2015; Wang et al., Citation2008).
Figure 5. NeuroQuant Analysis. The defendant’s NeuroQuant data is present under the ‘Coleman’ column. The control population average NeuroQuant data is under the ‘Mean’ column. Areas of the defendant’s brain that were statistically abnormal compared to the control population, have a numerical P-value. Areas of the defendant’s brain that were not statistically different have a blank box under P-value. It is important to note that the defendant had an overall reduced intracranial volume 2.82 standard deviations below age and gender-matched controls and had extremely reduced relative volumes of parenchyma, gray matter, ventricle, hippocampus, caudate, and cerebellum, compared to his already reduced total intracranial volume, all-around or greater than 4 standard deviations below age gender-matched controls.
Events in the defendant’s medical and personal history could support the above diagnoses. Such events include alcohol consumption by the mother during pregnancy, a brain injury at the age of 11 that caused a loss of consciousness (of unspecified duration), and eventually a drop in language and reading scores. Later, at the age of 24, the defendant was struck multiple times on the head by a hammer. Such TBIs such as those mentioned above can lead to the development of CTE. Moreover, a comprehensive neurological evaluation reveals a family history of mental disorders of both the maternal and paternal lineages.
Neuropsychological assessment
The results of the neuropsychological assessment suggested impaired working memory capacity. There was evidence to indicate impairment in executive functioning and tasks mediated by the temporal lobe. Results were consistent with the abnormal PET scan and FAS. Analytically, based on the WAS-IV, the defendant has a full-scale IQ of 77, which is in the 6th percentile and suggests borderline deficiency. The WASI-II indicated that the defendant’s full-scale intelligence quotient (FSIQ) was in the 14th percentile with a score of 84 (low-average range). In the Woodcock-Johnson Tests of Cognitive abilities, the defendant scored 81 for general intellectual ability, 87 for short-term memory, and 80 for cognitive efficiency found in the 11th, 19th, and 9th percentile accordingly.
The psychologist interpreted the results supporting that the defendant’s intellectual deficits impacted his ability for abstract reasoning and planning and caused difficulty in learning from past experiences and consequences of previous behavior. He also identified signs of paranoia that previously were under-reported. The reporting of paranoia was partly based on letters written in prison by the defendant. While writing the letters, the defendant would often alternate between blaming the prison staff for attempts to poison him and praising them.
The psychological report made also included statements about the past experiences of the defendant stretching back to his childhood. These included reports that the defendant’s mother was a lifelong alcoholic who drank heavily during her pregnancy, reports of malnutrition, substance abuse, and criminal activity of other family members, and stating that the defendant had witnessed repeatedly domestic violence as well as sexual assault of family members. Moreover, based on family reports and the individual’s general history, a psychologist suggested that the defendant might have bipolar disorder which explained issues with agitation, aggressiveness, behavior control, and impulsivity. The expert witness suggested that the defendant was hypersensitive to racism and prejudice and had the perception that he and his family were being attacked.
Mr. Coleman had previously fired a gun on 18 April 1997 when he was 21 years old. He and his wife Celiani and his kids had been staying at his mother’s home but the mother was evicting Mr. Coleman after he and his family stayed there for 2 weeks. His wife’s sister and her husband, David Alvarado, drove up in a Pontiac and offered to take Celiani and the kids elsewhere but Celiani refused. When Kelvin Coleman arrived, he started shooting the Pontiac four times because he is upset that his wife and kids are being evicted. David Alvarado asked Mr. Coleman why was shooting. Mr. Coleman came up to the car and aimed his gun and started shooting David Alvaarado who was asking ‘What are you doing, why are you going to shoot me?’ Mr. Alvarado is severely wounded but is able to scramble out of the car on the opposite side. This previous shooting incident illustrates Mr. Coleman’s inability to calibrate his anger and his tendency to illogically overreact in an aggressive manner and is characteristic of patients with fetal alcohol syndrome.
The neurological report
The neurological report states that bearing in mind the history of prenatal alcohol exposure, the central nervous abnormalities shown during the neurological examination, the facial phenotype of the defendant, the ptosis and underdeveloped ears, and other cranial dimorphisms, the history of growth deficiency, and the abnormalities noted on cerebral imaging, the diagnosis of FASD is unambiguous. According to the report, multiple analytic studies confirm the sensitivity (100%) and specificity (99%) of the identified facial features to FAS. The report continues that the NQ data that demonstrated severe atrophy of every cortical structure can also, given his history, only be the result of prenatal toxin exposure with the most probable toxin being alcohol and the defendant’s examination and imaging findings lead the clinician to a characterization of the defendant’s FAS as severe. According to the neurologist, the psychological consequences of FAS is an emotional level of development below the chronological age of the defendant, an ability to function in society well below that suggested by the defendant’s IQ score, attention and memory deficits, difficulties with abstraction, impaired problem solving and poor judgment, behavioral immaturity, hyperactivity and explosive episodes, vulnerability to peer pressure, difficulty learning from consequences and repeating mistakes multiple times. The behavioral consequences identified were very similar to those identified by the psychologists mentioned above.
Concerning the diagnosis of TBI, the neurologist diagnosed the defendant with a right nasal visual field deficit. The retro-orbital location of the lesion might explain the behavioral history of the defendant characterized by disinhibition, emotional lability, inappropriate affect, distractibility, impulsive behavior, poor judgment, and poor insight suggestive of an ‘orbitofrontal syndrome’. Besides, the neurologist suggests that although the diagnosis of CTE can only be made at autopsy, the defendant endorses several symptoms which are consistent with the sequelae of severe head trauma and also consistent with CTE, including dizzy spells, concentration problems, attention problems, headache, coordination deficits, depression, anxiety, nervousness, irritability, and a single episode of nocturnal urinary incontinence. Additionally, his history demonstrates excessive emotionality, poor judgment, and poor impulse control. Whether simply the sequelae of traumatic brain injury or harbingers of CTE, these signs and symptoms are strongly suggestive of focal brain damage superimposed upon the diffuse brain damage secondary to FAS. It should also be noted that following head trauma, there is often an amplification of pre-existing personality traits as well as changes in personality with irritability, restlessness, excessive emotionality, and aggression becoming common.
The neurologist diagnosed the defendant with frontal lobe dysfunction of which the effects shown in the defendant’s behavior are executive dysfunction including irritability, disinhibition, paranoia, and hypersexuality. Other brain structures involved in behavioral regulation and executive function such as the amygdala, the caudate nucleus, the temporal lobes, the anterior cingulate cortex, and the posterior cingulate cortex are profoundly atrophied as demonstrated by the NQ Triage Brain Atrophy Report. The neurologist completed his report by stating that the neurological insults of the defendant starting before his birth and continuing throughout his life make the question ‘if not for X, his behavior might have been different’ exceedingly difficult to answer.
Ruling and reasoning
It is of interest, to examine the impact of neuroimaging evidence and expert opinion on the outcome of the case described in this study. In this direction, it is useful to outline some specificities of the law applied in this case. Firstly, the State of Florida requires both an illegal act (actus reus) and criminal intent (mens rea) to attribute full responsibility for a crime. Secondly, the defendant was the first person to be trialed after the U.S. Supreme Court Hurst v. State of Florida decision was applied to require a unanimous vote of the Florida 12-membered jury that the aggravating factors are sufficient to impose death.Footnote2 Interestingly, the Hurst v. State of Florida also involved an abnormal neuroimaging PET scan that was analyzed by one of the co-authors (JCW) and was used by the public defender as evidence for consideration of mitigation in capital punishment.
At trial, four defensive arguments might be mitigating for the defendant. A claim that the defendant’s act was involuntary, a claim that the defendant lacked mens rea, a claim of defendant insanity due to cognitive impairment, and a claim that the defendant was insane due to volitional impairment. Moreover, a partial inability to form criminal intent or to fully appreciate the reasoning behind the death penalty may allow the defense to claim diminished capacity. Moreover, it should be noted that during the capital sentencing stage types of evidence not previously admissible can at this point be presented. In Florida statutes, mitigating circumstances for capital punishment relevant to this discussion include ‘the capital felony was committed while the defendant was under the influence of extreme mental or emotional disturbance’ and ‘the capacity of the defendant to appreciate the criminality of his or her conduct or to conform his or her conduct to the requirements of law was substant Diminished capacity can be used to mitigate the severity of punishment.Footnote3 In addition, the inability to understand the death penalty as a result of an abnormal mental state prevents punishment by means of execution, as a violation of the 8th amendment of the U.S. Constitution’s prohibition of cruel and unusual punishment.Footnote4
The jury unanimously found that the State of Florida was able to prove, beyond a reasonable doubt, the existence of aggravating factors. Firstly, the defendant was previously convicted of a felony involving the use or threat of violence to a person. Secondly, the murders of Mr. Carter and Ms. Johnson were committed in a cold, calculated, and premeditated manner, without the pretense of legal or moral justification. This was based on the five-hour delay between the time the defendant found out about the confrontation and the time he committed the murder. A third possible aggravating factor concerning the nature of the first-degree murder being especially heinous, atrocious, or cruel, was not voted unanimously (11 For vs. 1 Against) by the jury and was not used against the defendant. Despite that, the jury found the above-described factors sufficient to warrant the death penalty.
During the trial, the expert witnesses, supported claims that the defendant was unable to control his behavior, was diagnosed with FASD, TBI, and an IQ deficit grew up in a neglectful home, and had bad familial relationships. One of the expert witnesses testified that the trauma suffered by the defendant when growing up, changed his worldview. The state challenged the opinion of the expert witnesses that the defendant was mentally ill, by pointing out that the defendant was never diagnosed with a mental illness before the trial. One expert witness counter-argued that the defendant was attempting to cover up his symptoms.
In addition, due to the U.S. Constitution’s fifth amendment which gives defendants the right not to be compelled to be a witness against themselves, the defendant’s report of his affect or how he felt was not presented in the trial and is not available. If he were to go on the stand and testify about these things, he would have waived his right to not incriminate himself when he would have been cross-examined by the prosecutor.
The most relevant mitigating factor was that the defendant was under the influence of extreme mental and emotional disturbance at the time of the crime (4 yes to 8 no). Also, the jury was convinced that the defendant’s mother was consuming alcohol, tobacco, and drugs during her pregnancy and that the defendant suffered from FASD, resulting in impaired judgment, lack of impulse control, and difficulty controlling his actions. The jury agreed that the defendant was at a below-average intelligence level. It is worth noting, that the jury also found that the defendant grew up in an unstable household without a proper guardian or role model. The evidence of brain abnormalities resulting from neurological insult and fetal alcohol syndrome contributing to severely abnormal behavior and lack of impulse control was voted with 4 yes and 8 no. Also, an orbitofrontal syndrome that contributes to severely abnormal behavior and lack of impulse control was only voted for by one member of the jury.
Finally, the jury found that the mitigating circumstances outweighed the aggravating factors, resulting in the defendant’s sentence of life imprisonment without the possibility of parole.
Discussion
While this study addresses a single case, similar cases have in the past reached similar rulings. The evasion of death sentences has been especially common after the Hurst v. State decision requiring an anonymous jury vote before sentencing defendants to death.Footnote5 One such case is the State of Florida v. Luis Toledo which took place in 2017. The defendant was not sent to death despite killing his wife and her two children because of the mitigation claims of neurological illness and epilepsy. Similarly, in the case of State of Florida v. Byron Burch in 2015, first-degree murder and burglary charged to a defendant with a lengthy criminal record, did not result in a death sentence due to mitigating evidence of brain damage and presumptive chronic traumatic encephalopathy (CTE). Both cases had PET neuroimaging analyzed by one of the coauthors (JCW). After quantitative electroencephalography was inadmissible to the court, the defense attorney presented PET scans to claim brain damage that hindered impulse control. The jurors decided on a sentence to life in prison without parole which the judge ultimately decided upon.
While evidence on the existence of brain damage seems to suffice in some cases for a sentence to life in prison without parole, it is of interest to examine further the link between brain damage and criminality. This is linked to two questions: First, how common is brain damage among criminals, and second, how much does brain damage impact the likeliness of criminality. Several studies have looked at the prevalence of brain damage and psychiatric disorders among incarcerated individuals. Mental illness is significantly over-represented in death-row samples relative to the general population (Cunningham & Vigen, Citation2002). TBI is particularly prevalent among criminals, with one study reporting that 82% of the 164 incarcerated individuals interviewed have sustained a TBI, 79% have sustained a TBI with loss of consciousness, and 43% have sustained more than four or more TBIs (Schofield et al., Citation2006). Other psychiatric conditions like depression, mania, and schizophrenia have reportedly significantly higher prevalence rates among general samples of individuals from jails and specific samples of homicide charged individuals as compared to the rest of the population (Teplin, Citation1990; Wallace et al., Citation1998). It is of interest to see that mental disorders are usually accompanied by substance abuse and in many cases substance, especially alcohol abuse was confounded with associations between TBI and criminal offense (Wallace et al., Citation1998).
Concerning the second question, a retrospective cohort study has shown an association of TBI with any conviction (Schofield et al., Citation2015). Specifically, males with TBI had a hazard ratio (HR) for conviction of 1.58 (0.05 level of significance) while females had 1.52 HR. In the same study, TBI-exposed males had an HR of 1.69 as compared to same-sex full-sibling controls. Results for females were insignificant. Similarly, Fazel et al. (Citation2011) in a longitudinal population and sibling-controlled study, found that people who had sustained a TBI had a significantly increased risk of doing a violent crime (Fazel et al., Citation2011). Multiple studies have repeatedly found similar patterns of higher chances of earlier or more violent crimes in individuals (see Williams et al., Citation2018 for a review).
Much of the skepticism about the use of neuroimaging in courtrooms is not due to the limitations of the method but due to its impact on the jury. It can be argued that neuroimaging can be disproportionately persuasive in relation to the actual findings (Baker et al., Citation2017). Past studies have explored the persuasiveness of neuroscientific claims with and without brain images with initial findings reporting higher persuasiveness for claims paired with images (McCabe & Castel, Citation2008). However, recent studies have not replicated the initial results and have shown that persuasiveness and overall judgment of the quality of information do not depend on the brain images but the prestige of neuroscience as a subject (Gruber & Dickerson, Citation2012; Hook & Farah, Citation2013). Concerning the impact of neuroscience (not limited to only brain scans), Fernandez-Duque et al. (Citation2015) argue that a possible reason why neuroscience is compelling is the level of explanatory power it can offer to imply that the brain is the cause of the actions (Fernandez-Duque et al., Citation2015). However, if that is the case during a trial, such reductionist approaches may impede the further search for the cause of the actions and their punishment. Weisberg et al. (Citation2015) have shown that when choosing between true and false explanations of people’s beliefs and behaviors, subjects choose correctly in general except when neuroscience evidence is used in the faulty explanation (Skolnick Weisberg et al., Citation2015). They have also shown that this is not a result of being seduced by scientific jargon but rather any reference to the brain is sufficient to make faulty explanations seem logical and therefore chosen. Interestingly, when neuroscience information was described as causally related to the explanation, the effect was even stronger proving the general bias of humans towards teleological information (Lombrozo & Carey, Citation2006). The above findings suggest that neuroscientific data are indeed persuasive, indeed sometimes wrongfully.
Another consideration is how well can the jury, attorney, or judge estimate how knowledgeable the expert is and therefore adjust the credibility of the testimony accordingly. Interestingly, Parrot et al. (Citation2015) showed that jurors’ decisions and judgments of credibility could not be predicted by the level of expert knowledge although they did notice variations of knowledge (Parrott et al., Citation2015). Other factors that may play a role in affecting mock juror decisions are the complexity of testimony and their credentials. (Cooper et al., Citation1996; Greenberg & Wursten, Citation1988). More specifically, as complexity increases, jurors tend to rely more on the credentials of the expert and less on the content of the testimony (Cooper et al., Citation1996). In a related note, Greenberg and Wursten (Citation1988) found that jurors were biased towards giving more credibility and weight to the testimonies of medical professionals (MD – psychiatrists) instead of those of psychologists (Ph.D.), especially when they testified on the prosecution’s side (Greenberg & Wursten, Citation1988). In previous simulations, the effect of neuroimaging and genetic evidence on jurors has been found inconsistent (Appelbaum et al., Citation2015), although simulations are often inadequate in depicting real-life situations (Scurich, Citation2018). A recent review has reported that neuroscientific evidence does have mitigating effects although neuroimaging does not have any particular effects (Aono et al., Citation2019). The above findings suggest the importance that science should be presented in a predetermined way and the audience should be sufficiently acquainted with the material presented to be able to understand the level of expertise of the expert witness. However, it is questionable if such confidence about the material presented is in the scope of knowledge of the jurors or the judge. An independent body establishing the credibility of the science presented might be useful in this case. Although his most serious criminal act was carried out in ‘a calculated and premeditated way’, there are examples of other cases of individuals with CTE in which homicides superficially appear to be ‘cold and calculated’ but which are associated with severe neurological pathology which evidently caused severe impulse control problems that occur over a prolonged period of time. For example, Chris Benoit, a professional wrestler, committed a double murder suicide over a three-day period ending 25 June 2007 during which he bound his wife feet and wrists and asphyxiated her and then killed his son by asphyxia as he lay in bed. He then hung himself in the weight room. He had planned his murder carefully. A pathological examination showed that he had chronic traumatic encephalopathy in all regions of the brain (Omalu et al., Citation2010). Another example is Aaron Hernandez who was drafted by the New England Patriots and had a $40 million dollar contract. He shot a friend Odin Lloyd who was dating the sister of Aaron Hernandez’s fiancée with multiple gunshot wounds to the back and chest with no motive that was ever explained. He was also indicted for the double homicide of Daniel de Abreu and Safiro Furtado but was found not guilty of their murders. After Aaron Hernandez committed suicide in prison, he was also found to have severe CTE (Gregory, Citation2020).
Although multiple studies have shown that certain behaviors are linked to abnormal brain scans, our understanding of the brain and its abnormalities is far from complete. While it is evident that an abnormal brain is related to abnormal behavior, we are still unable to integrate all the levels of data obtained from the brain. There exists no strict correlation between the amount of brain tissue lost and the extent of the impact on behavior. Apart from the enormous complexity, our limited understanding is a result of not being able to directly manipulate the living human brain to a great extent and extrapolating results from other organisms or simulations (Markram, Citation2013). The exact process in which increased or decreased brain tissue of any type leads to decreased executive control and eventually to a violent outburst is unclear. Therefore, the teleological information neuroscience might offer in the courtroom should be approached through the lens of our inability to completely understand and predict its patterns. Currently, there is insufficient research to be able to determine how much brain abnormality is sufficient to warrant a judgment of diminished responsibility. It is currently decided on a case-by-case basis by different juries who independently determine if the abnormalities found are sufficient. In general, cases that are referred for neuroimaging such as PET, MRI DTI, and MRI QV have significant neurological and psychiatric histories and significant neuropsychological abnormalities. Marginal cases with no significant neurological or psychiatric history or no significant neuropsychological findings are generally not referred for expensive neuroimaging testing. In part, this may reflect a fear by the public defenders that such tests may turn out to be normal in these cases and such results would significantly harm their client in a trial. In such cases, it is the author’s experience that 90% of these cases have juries return a verdict that reflects the juries’ opinion that there is sufficient mitigating evidence to warrant life in prison vs. the death penalty. In the author’s experience, those cases in which this type of evidence is presented, and the jury returns the death penalty are generally extremely heinous cases such as kidnapped child sex murder cases.
Limitations and future directions
The nature of this case study does not allow it to be viewed as a set of standards for the use of neuroscientific tools in the legal proceedings as the practices used are adapted, as they ought to be, to the specificity of this trial. However, it is an example of the use of the current neuroscientific tools in the courtroom. This study does not intend to legitimize or justify criminal acts, nor to suggest that cause of the criminal act were the brain abnormalities. Further study is needed to establish whether the lack of standard protocols on the use of neuroscience enhances or hinders the fairness of trials.
Furthermore, considering the impact that neuroscientific evidence can have on the outcome of the trial and the fact that many of the defendants have not been officially diagnosed with brain disorders before the trials, it is difficult to evaluate the brain before or at the time of the crime.
It is also worth noting that this cannot be used as a guide for identifying brain regions or disorders associated with criminality. Individuals that had a similar neurological and psychological profile but did not commit the violent crimes the defendant committed would be an excellent study control to identify brain regions/functions (beyond the neurological conditions) that are associated with criminality. However, in this case, this was not our primary goal, and including this kind of control was not possible. To address, the fact that people with such severe brain damage might not commit any crimes we included bibliographic references presenting how much more likely an individual is to commit a crime if they sustain a neurological indult, as well as references presenting how prevalent brain injuries are among incarcerated populations.
Last, although this study is primarily concerned with the impact of neuroscience tools on the outcome of the trial, we should emphasize that the most important mitigating factor according to the jury was the claim that the defendant was under extreme mental and emotional disturbance and not his claims of diminished capacity. However, it should be pointed out that the evidence presented by the expert witnesses on the defendant’s mental and neurological condition might have served as a relevant description of the defendant’s character and therefore affect the judgment of the reasonableness of the defendant’s conduct (Robinson, Citation2016). It is evident that the jury could not unanimously decide that Mr. Coleman’s case deserved the death penalty which suggests that some of the juries felt that there were neurological or psychiatric mitigating factors that were described.
Conflicts of interest
Using neuroscience for the defense of murder is tangent to moral and philosophical considerations. However, this is a factual report of the events aiming to illustrate the practice of using neuroscientific and neuropsychological evidence and does not by any means aim to support or criticize the morality of any of the stakeholders.
Bearing in mind the aims of medical research investigations and those of medical care which are not entirely overlapping but have both been among the responsibilities of some of the co-authors, we believe that the decisions on the selection of research and analytic methods, including the statistical analysis; and the presentation and interpretation of the results, including decisions regarding what to publish and where to publish it have been taken so that the research work presented in this study can benefit the scientific community and not serve any foreseeable personal interest.
Acknowledgments
Thanks to Morris Carranza, Lake County Public Defender, for his insights and to Dr. Michael Cummings of Patton State Hospital for his contribution to the ruling and reasoning section.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Correction Statement
This article has been republished with minor changes. These changes do not impact the academic content of the article.
Notes
1 Ruppel v. Kucanin, No. 3:08-CV-591-JTM, 2011 WL 2470621, 7 (N.D. Ind. July 20, 2011).
Roach v. Hughes, No. 4:13-CV-00136-JHM, 2016 WL 9460306, 3 (W.D. Ky. March 9, 2016).
Marsh v. Celebrity Cruises Inc, No. 1:17-CV-21097-UU, 2017 WL 6987718, 4 (S.D. Fla. December15, 2017).
Barnett v. National Continental Ins. Co., No. 3:17-CV-153-JWD-EWD, 2019 WL 126732, 6 (M.D. La. January 8, 2019).
2 Hurst v. State, 202 So. 3d 40 (Fla. 2016).
3 People v. Patterson, 39 N.Y. 2d. 288, 303 (1976).
4 Ford v. Wainwright, 477 U.S. 399, 400 (1986). Atkins v. Virginia, 536 U.S. 304, 311-21 (2002). Hall v. Florida, 572 U.S. 701, 12–16 (2014).
5 Hurst v. State, 202 So. 3d 40 (Fla. 2016). In January 2020, in the case State v. Poole the Supreme Court of Florida ruled that the jury must be unanimous only in finding the existence of a statutory aggravating circumstance beyond a reasonable doubt and not in recommending death. Therefore, partially receding from the Hurst v. State decision.
References
- Alavi, A., & Newberg, A. B. (1996). Metabolic consequences of acute brain trauma: Is there a role for PET? Journal of Nuclear Medicine, 37(Issue 7), 1170–1172. https://www.researchgate.net/publication/14242959
- Aono, D., Yaffe, G., & Kober, H. (2019). Neuroscientific evidence in the courtroom: A review. Cognitive Research: Principles and Implications, 4(Issue 1), 40. https://doi.org/10.1186/s41235-019-0179-y
- Appelbaum, P. S., Scurich, N., & Raad, R. (2015). Effects of behavioral genetic evidence on perceptions of criminal responsibility and appropriate punishment. Psychology, Public Policy, and Law, 21(2), 134–144. https://doi.org/10.1037/law0000039
- Archibald, S. L., Fennema-Notestine, C., Gamst, A., Riley, E. P., Mattson, S. N., & Jernigan, T. L. (2001). Brain dysmorphology in individuals with severe prenatal alcohol exposure. Developmental Medicine & Child Neurology, 43(3), 148–154. https://doi.org/10.1111/j.1469-8749.2001.tb00179.x
- Asken, B. M., DeKosky, S. T., Clugston, J. R., Jaffee, M. S., & Bauer, R. M. (2018). Diffusion tensor imaging (DTI) findings in adult civilian, military, and sport-related mild traumatic brain injury (mTBI): A systematic critical review. Brain Imaging and Behavior, 12(Issue 2), 585–612. https://doi.org/10.1007/s11682-017-9708-9
- Assaf, Y., & Pasternak, O. (2008). Diffusion tensor imaging (DTI)-based white matter mapping in brain research: A review. Journal of Molecular Neuroscience, 34(Issue 1), 51–61. https://doi.org/10.1007/s12031-007-0029-0
- Baker, D. A., Ware, J. M., Schweitzer, N. J., & Risko, E. F. (2017). Making sense of research on the neuroimage bias. Public Understanding of Science, 26(2), 251–258. https://doi.org/10.1177/0963662515604975
- Barrio, J. R., Small, G. W., Wong, K. P., Huang, S. C., Liu, J., Merrill, D. A., Giza, C. C., Fitzsimmons, R. P., Omalu, B., Bailes, J., & Kepe, V. (2015). In vivo characterization of chronic traumatic encephalopathy using [F-18]FDDNP PET brain imaging. Proceedings of the National Academy of Sciences, 112(16), E2039–E2047. https://doi.org/10.1073/pnas.1409952112
- Bowman, F. D. B., Guo, Y., & Derado, G. (2007). Statistical approaches to functional neuroimaging data. Neuroimaging Clinics of North America, 17(Issue 4), 441–458. https://doi.org/10.1016/j.nic.2007.09.002
- Byrnes, K. R., Wilson, C. M., Brabazon, F., von Leden, R., Jurgens, J. S., Oakes, T. R., & Selwyn, R. G. (2014). FDG-PET imaging in mild traumatic brain injury: A critical review. Frontiers in Neuroenergetics, 5(JAN), 13. https://doi.org/10.3389/fnene.2013.00013
- Clark, C. M., Li, D., Conry, J., Conry, R., & Loock, C. (2000). Structural and functional brain integrity of fetal alcohol syndrome in nonretarded cases. Pediatrics, 105(5), 1096–1099. https://doi.org/10.1542/peds.105.5.1096
- Coles, C. D., & Li, Z. (2011). Functional neuroimaging in the examination of effects of prenatal alcohol exposure. Neuropsychology Review, 21(Issue 2), 119–132. https://doi.org/10.1007/s11065-011-9165-y
- Cooper, J., Bennett, E. A., & Sukel, H. L. (1996). Complex scientific testimony: How do jurors make decisions? Law and Human Behavior, 20(4), 379–394. https://doi.org/10.1007/BF01498976
- Cunningham, M., & Vigen, M. (2002). Death row inmate characteristics, adjustment, and confinement: A critical review of the literature. Behavioral Sciences and the Law, 20(1–2), 191–210. https://doi.org/10.1002/bsl.473
- Diamond, A. (2013). Executive functions. Annual Review of Psychology, 64(1), 135–168. https://doi.org/10.1146/annurev-psych-113011-143750
- Dickstein, D. L., Pullman, M. Y., Fernandez, C., Short, J. A., Kostakoglu, L., Knesaurek, K., Soleimani, L., Jordan, B. D., Gordon, W. A., Dams-O’Connor, K., Delman, B. N., Wong, E., Tang, C. Y., DeKosky, S. T., Stone, J. R., Cantu, R. C., Sano, M., Hof, P. R., & Gandy, S. (2016). Cerebral [18F]T807/AV1451 retention pattern in clinically probable CTE resembles pathognomonic distribution of CTE tauopathy. Translational Psychiatry, 6(9), e900–e900. https://doi.org/10.1038/tp.2016.175
- Donald, K. A., Eastman, E., Howells, F. M., Adnams, C., Riley, E. P., Woods, R. P., Narr, K. L., & Stein, D. J. (2015). Neuroimaging effects of prenatal alcohol exposure on the developing human brain: A magnetic resonance imaging review. Acta Neuropsychiatrica, 27(Issue 5), 251–269. https://doi.org/10.1017/neu.2015.12
- Elderkin-Thompson, V., Ballmaier, M., Hellemann, G., Pham, D., & Kumar, A. (2008). Executive function and MRI prefrontal volumes among healthy older adults. Neuropsychology, 22(5), 626–637. https://doi.org/10.1037/0894-4105.22.5.626
- Fan, J., Jacobson, S. W., Taylor, P. A., Molteno, C. D., Dodge, N. C., Stanton, M. E., Jacobson, J. L., & Meintjes, E. M. (2016). White matter deficits mediate effects of prenatal alcohol exposure on cognitive development in childhood. Human Brain Mapping, 37(8), 2943–2958. https://doi.org/10.1002/hbm.23218
- Farahany, N. A. (2016). Neuroscience and behavioral genetics in US criminal law: An empirical analysis. Journal of Law and the Biosciences, 2(3), lsv059–lsv509. https://doi.org/10.1093/jlb/lsv059
- Fazel, S., Lichtenstein, P., Grann, M., & Långström, N. (2011). Risk of violent crime in individuals with epilepsy and traumatic brain injury: A 35-year Swedish population study. PLoS Medicine, 8(12), 1–8. https://doi.org/10.1371/journal.pmed.1001150
- Fernandez-Duque, D., Evans, J., Christian, C., & Hodges, S. D. (2015). Superfluous neuroscience information makes explanations of psychological phenomena more appealing. Journal of Cognitive Neuroscience, 27(5), 926–944. https://doi.org/10.1162/jocn_a_00750
- Galgano, M. A., Cantu, R., & Chin, L. S. (2016). Chronic traumatic encephalopathy: The impact on athletes. Cureus, 8(3), 1–10. https://doi.org/10.7759/cureus.532
- Greenberg, J., & Wursten, A. (1988). The psychologist and the psychiatrist as expert witnesses: Perceived credibility and influence. Professional Psychology: Research and Practice, 19(4), 373–378. https://doi.org/10.1037/0735-7028.19.4.373
- Gregory, H. (2020). Making a murderer: Media renderings of brain injury and Aaron Hernandez as a medical and sporting subject. Social Science & Medicine, 244, 112598. https://doi.org/10.1016/j.socscimed.2019.112598
- Gruber, D., & Dickerson, J. A. (2012). Persuasive images in popular science: Testing judgments of scientific reasoning and credibility. Public Understanding of Science, 21(8), 938–948. https://doi.org/10.1177/0963662512454072
- Hook, C. J., & Farah, M. J. (2013). Look again: Effects of brain images and mind-brain dualism on Lay evaluations of research. Journal of Cognitive Neuroscience, 25(9), 1397–1405. https://doi.org/10.1162/jocn_a_00407
- Johnson, V. E., Stewart, W., & Smith, D. H. (2013). Axonal pathology in traumatic brain injury. Experimental Neurology, 246, 35–43. https://doi.org/10.1016/j.expneurol.2012.01.013
- Jungbauer, W. G., & Bowman, C. W. (2014). Daubert, Frye and DTI: Hijacking the right to trial by jury. AJOB Neuroscience, 5(2), 16–23. https://doi.org/10.1080/21507740.2014.885096
- Kato, T., Nakayama, N., Yasokawa, Y., Okumura, A., Shinoda, J., & Iwama, T. (2007). Statistical image analysis of cerebral glucose metabolism in patients with cognitive impairment following diffuse traumatic brain injury. Journal of Neurotrauma, 24(6), 919–926. https://doi.org/10.1089/neu.2006.0203
- Kornguth, S., Rutledge, N., Perlaza, G., Bray, J., & Hardin, A. (2017). A proposed mechanism for development of CTE following concussive events: Head impact, water hammer injury, neurofilament release, and autoimmune processes. Brain Sciences, 7(12), 1–15. https://doi.org/10.3390/brainsci7120164
- Langfitt, T. W., Obrist, W. D., Alavi, A., Grossman, R. I., Zimmerman, R., Jaggi, J., Uzzell, B., Reivich, M., & Patton, D. R. (1986). Computerized tomography, magnetic resonance imaging, and positron emission tomography in the study of brain trauma. Preliminary observations. Journal of Neurosurgery, 64(5), 760–767. https://doi.org/10.3171/jns.1986.64.5.0760
- Lebel, C., Roussotte, F., & Sowell, E. R. (2011). Imaging the impact of prenatal alcohol exposure on the structure of the developing human brain. Neuropsychology Review, 21(Issue 2), 102–118. https://doi.org/10.1007/s11065-011-9163-0
- Li, Z., Coles, C. D., Lynch, M. E., Ma, X., Peltier, S., & Hu, X. (2008). Occipital-temporal reduction and sustained visual attention deficit in prenatal alcohol exposed adults. Brain Imaging and Behavior, 2(1), 39–48. https://doi.org/10.1007/s11682-007-9013-0
- Lipton, M. L., Kim, N., Park, Y. K., Hulkower, M. B., Gardin, T. M., Shifteh, K., Kim, M., Zimmerman, M. E., Lipton, R. B., & Branch, C. A. (2012). Robust detection of traumatic axonal injury in individual mild traumatic brain injury patients: Intersubject variation, change over time and bidirectional changes in anisotropy. Brain Imaging and Behavior, 6(2), 329–342. https://doi.org/10.1007/s11682-012-9175-2
- Lo, C., Shifteh, K., Gold, T., Bello, J. A., & Lipton, M. L. (2009). Diffusion tensor imaging abnormalities in patients with mild traumatic brain injury and neurocognitive impairment. Journal of Computer Assisted Tomography, 33(2), 293–297. https://doi.org/10.1097/RCT.0b013e31817579d1
- Lombrozo, T., & Carey, S. (2006). Functional explanation and the function of explanation. Cognition, 99(2), 167–204. https://doi.org/10.1016/j.cognition.2004.12.009
- Luo, W., Airriess, C., & Albright, J. (2015). The NeuroQuant normative database comparing individual brain structures. In CORTECHS LABS WHITE PAPER.
- Ma, X., Coles, C. D., Lynch, M. E., LaConte, S. M., Zurkiya, O., Wang, D., & Hu, X. (2005). Evaluation of corpus callosum anisotropy in young adults with fetal alcohol syndrome according to diffusion tensor imaging. Alcoholism: Clinical & Experimental Research, 29(7), 1214–1222. https://doi.org/10.1097/01.ALC.0000171934.22755.6D
- Madsen, K., Hesby, S., Poulsen, I., Fuglsang, S., Graff, J., Larsen, K. B., Kammersgaard, L. P., Law, I., & Siebner, H. R. (2017). Comparison of analytical methods of brain [18F]FDG-PET after severe traumatic brain injury. Journal of Neuroscience Methods, 291, 176–181. https://doi.org/10.1016/j.jneumeth.2017.07.032
- Markram, H. (2013). Seven challenges for neuroscience. Functional Neurology, 28(3), 145–151. https://doi.org/10.11138/FNeur/2013.28.3.145
- McCabe, D. P., & Castel, A. D. (2008). Seeing is believing: The effect of brain images on judgments of scientific reasoning. Cognition, 107(1), 343–352. https://doi.org/10.1016/j.cognition.2007.07.017
- Miller, G. (2010). Brain Exam May Have Swayed Jury in sentencing convicted murderer. Science Insider. https://www.sciencemag.org/news/2010/12/brain-exam-may-have-swayed-jury-sentencing-convicted-murderer
- Omalu, B. I., Fitzsimmons, R. P., Hammers, J., & Bailes, J. (2010). Chronic traumatic encephalopathy in a professional American wrestler. Journal of Forensic Nursing, 6(3), 130–136. https://doi.org/10.1111/j.1939-3938.2010.01078.x
- Parrott, C. T., Neal, T., Wilson, J. K., & Brodsky, S. L. (2015). Differences in expert witness knowledge: Do mock jurors notice and does it matter? The Journal of the American Academy of Psychiatry and TheLaw, 43(1), 69–81. PMID: 25770282
- Partovi, S., Yuh, R., Pirozzi, S., Lu, Z., Couturier, S., Grosse, U., Schluchter, M. D., Nelson, A., Jones, R., O’Donnell, J. K., & Faulhaber, P. (2017). Diagnostic performance of an automated analysis software for the diagnosis of Alzheimer’s dementia with 18F FDG PET. American Journal of Nuclear Medicine and Molecular Imaging, 7(1), 12–23. http://www.ncbi.nlm.nih.gov/pubmed/28123864
- Roberts, M. A., Manshadi, F. F., Bushnell, D. L., & Hines, M. E. (1995). Neurobehavioural dysfunction following mild traumatic brain injury in childhood: A case report with positive findings on positron emission tomography (PET). Brain Injury, 9(5), 427–436. https://doi.org/10.3109/02699059509008202
- Robinson, P. H. (2016). Abnormal mental state mitigations of murder: The US perspective. In Loss of control and diminished responsibility (pp. 291–310). Routledge.
- Ross, D. E., Ochs, A. L., Seabaugh, J. M., Demark, M. F., Shrader, C. R., Marwitz, J. H., & Havranek, M. D. (2012). Progressive brain atrophy in patients with chronic neuropsychiatric symptoms after mild traumatic brain injury: A preliminary study. Brain Injury, 26(12), 1500–1509. https://doi.org/10.3109/02699052.2012.694570
- Ross, D. E., Ochs, A. L., Seabaugh, J. M., & Shrader, C. R. (2013). Man versus machine: Comparison of radiologists’ interpretations and NeuroQuantspi® volumetric analyses of brain MRIs in patients with traumatic brain injury. The Journal of Neuropsychiatry and Clinical Neurosciences, 25(1), 32–39. https://doi.org/10.1176/appi.neuropsych.11120377
- Rusconi, E., & Mitchener-Nissen, T. (2013). Prospects of functional magnetic resonance imaging as lie detector. Frontiers in Human Neuroscience, 7(Issue SEP), 1–12. https://doi.org/10.3389/fnhum.2013.00594
- Rushing, S. E., & Langleben, D. D. (2011). Relative function: Nuclear brain imaging in United States courts. The Journal of Psychiatry & Law, 39(Issue 4), 567–593. https://doi.org/10.1177/009318531103900404
- Saks, M. J., Schweitzer, N. J., Aharoni, E., & Kiehl, K. A. (2014). The impact of neuroimages in the sentencing phase of capital trials. Journal of Empirical Legal Studies, 11(1), 105–131. https://doi.org/10.1111/jels.12036
- Schofield, P. W., Butler, T. G., Hollis, S. J., Smith, N. E., Lee, S. J., & Kelso, W. M. (2006). Traumatic brain injury among Australian prisoners: Rates, recurrence and sequelae. Brain Injury, 20(5), 499–506. https://doi.org/10.1080/02699050600664749
- Schofield, P. W., Malacova, E., Preen, D. B., D’Este, C., Tate, R., Reekie, J., Wand, H., & Butler, T. (2015). Does traumatic brain injury lead to criminality? A whole-population retrospective cohort study using linked data. PLoS ONE, 10(7), 1–12. https://doi.org/10.1371/journal.pone.0132558
- Scurich, N. (2018). What do experimental simulations tell us about the effect of neuro/genetic evidence on jurors? Journal of Law and the Biosciences, 5(Issue 1), 204–207. https://doi.org/10.1093/jlb/lsy006
- Seiden, J. A. (2004). The criminal brain: Frontal lobe dysfunction evidence in Capital Proceedings (Vol. 437). http://secondsightresearch.tripod.com/zine/id56.html
- Shen, F. (2016). The overlooked history of neurolaw. Fordham Law Review, 85(2). https://ir.lawnet.fordham.edu/flr/vol85/iss2/13
- Slobogin, C. (2017). Neuroscience nuance: Dissecting the relevance of neuroscience in adjudicating criminal culpability. Journal of Law and the Biosciences, 4(3), 577–593. https://doi.org/10.1093/jlb/lsx033
- Stern, R. A., Daneshvar, D. H., Baugh, C. M., Seichepine, D. R., Montenigro, P. H., Riley, D. O., Fritts, N. G., Stamm, J. M., Robbins, C. A., McHale, L., Simkin, I., Stein, T. D., Alvarez, V. E., Goldstein, L. E., Budson, A. E., Kowall, N. W., Nowinski, C. J., Cantu, R. C., & McKee, A. C. (2013). Clinical presentation of chronic traumatic encephalopathy. Neurology, 81(13), 1122–1129. https://doi.org/10.1212/WNL.0b013e3182a55f7f
- Sundman, M., Doraiswamy, P. M., & Morey, R. A. (2015). Neuroimaging assessment of early and late neurobiological sequelae of traumatic brain injury: Implications for CTE. Frontiers in Neuroscience, 9(Issue SEP), 334. https://doi.org/10.3389/fnins.2015.00334
- Teplin, L. A. (1990). The prevalence of severe mental disorder among male urban jail detainees: Comparison with the epidemiologic catchment area program. American Journal of Public Health, 80(6), 663–669. https://doi.org/10.2105/AJPH.80.6.663
- Treit, S., Chen, Z., Zhou, D., Baugh, L., Rasmussen, C., Andrew, G., Pei, J., & Beaulieu, C. (2017). Sexual dimorphism of volume reduction but not cognitive deficit in fetal alcohol spectrum disorders: A combined diffusion tensor imaging, cortical thickness and brain volume study. NeuroImage: Clinical, 15, 284–297. https://doi.org/10.1016/j.nicl.2017.05.006
- Wallace, C., Mullen, P., Burgess, P., Palmer, S., Ruschena, D., & Browne, C. (1998). Serious criminal offending and mental disorder: Case linkage study. British Journal of Psychiatry, 172(JUNE), 477–484. https://doi.org/10.1192/bjp.172.6.477
- Wang, J. Y., Bakhadirov, K., Devous, M. D., Abdi, H., McColl, R., Moore, C., Marquez De La Plata, C. D., Ding, K., Whittemore, A., Babcock, E., Rickbeil, T., Dobervich, J., Kroll, D., Dao, B., Mohindra, N., Madden, C. J., & Diaz-Arrastia, R. (2008). Diffusion tensor tractography of traumatic diffuse axonal injury. Archives of Neurology, 65(5), 619–626. https://doi.org/10.1001/archneur.65.5.619
- Weisberg, D. S., Taylor, J. C., & Hopkins, E. J. (2015). Deconstructing the seductive allure of neuroscience explanations. Judgment and Decision making, 10(5), 429.
- Williams, W. H., Chitsabesan, P., Fazel, S., McMillan, T., Hughes, N., Parsonage, M., & Tonks, J. (2018). Traumatic brain injury: A potential cause of violent crime? The Lancet Psychiatry, 5(10), 836–844. https://doi.org/10.1016/S2215-0366(18)30062-2
- Wozniak, J. R., Mueller, B. A., Chang, P. N., Muetzel, R. L., Caros, L., & Lim, K. O. (2006). Diffusion tensor imaging in children with fetal alcohol spectrum disorders. Alcoholism: Clinical and Experimental Research, 30(10), 1799–1806. https://doi.org/10.1111/j.1530-0277.2006.00213.x