
 ?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.
?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.Abstract
Purpose. This study aimed to investigate chemical injuries caused by cleaning agents and disinfectants by reviewing poison control data. Methods. We performed a 5-year retrospective analysis of calls to the Swedish Poisons Information Centre (PIC) concerning occupational use of cleaning agents and disinfectants. In addition, callers for 17 new cases were interviewed. Results. Out of 8240 occupationally related cases handled by the PIC during 2010–2014, 24% concerned cleaning agents and disinfectants (N = 1983). Of these, one-third were classified as major risk cases, generally due to potential for corrosive eye and skin injuries. The most frequent type of workplace was restaurants and caterers. However, information about occupation was only identifiable for 30% of the cases. Follow-up interviews exemplify how limited awareness of safety data sheets and disregard of protective equipment may contribute to health-related outcomes such as absence at work. Conclusions. Management and prevention strategies for cleaning agents should be improved. PIC records hold relevant information both for designing interventions and for future research on occupational health and safety management. We suggest that systematic collection by the PIC of information on occupation and age would further improve the usefulness for occupational injury surveillance purposes.
1 Introduction
Overviews of injuries and incidents provide an important basis for injury prevention and may identify problematic uses of chemicals or groups at risk. Data from calls made to poisons information centres have been used to investigate chemical injuries in schools [Citation1,Citation2] and in the workplace [Citation3–7] as well as for specific target groups such as pesticide exposures [Citation8], workers in small enterprises [Citation9], military personnel [Citation10] and adolescent workers [Citation11–13]. A recent comparison between the occupational cases found in the Swedish Poisons Information Centre (PIC) database and the official statistics of the Swedish Work Environment Authority (SWEA) showed that these two data sources reveal somewhat different pictures of chemical accidents at work [Citation7]. In particular, the PIC records revealed a substantially higher number, in both absolute and relative terms, of accidents involving cleaning agents. The same study also found that Swedish injury statistics lack details regarding the nature of chemical hazards involved, and that PIC records thus may offer valuable insight regarding incidents with hazardous substances at work [Citation7].
Cleaning agents and disinfectants are used in many different kinds of workplaces [Citation14]. The Swedish work environment survey from 2013 showed that 8% of men and 19% of women reported exposure to ‘cleaning agents and/or disinfectants (that comes in contact with the skin)’ during more than 25% of their working time [Citation15]. Proper management of risks with cleaning agents and disinfectants is thus an important factor for a substantial part of the Swedish workforce.
There are few data on the acute chemical injuries caused by cleaning agents. Many cleaning products are classified as corrosives and irritants [Citation14]. A pilot study on hospital cleaners noted that symptoms of irritation of the eyes, skin and respiratory tract were frequent; 21.3% experienced such symptoms daily or several times per week and only 43.7% reported no such symptoms in the past 12 months [Citation16]. The focus of cleaning agents’ chemical hazards often lies on the long-term effects. Wet-work in itself is an etiological factor of dermatitis, which may be exacerbated by co-exposure to cleaning agents [Citation14,Citation17]. Several studies point towards increased risk for both occupational asthma and workplace-exacerbated asthma among occupations frequently using cleaning agents and surface disinfectants. In particular, use of household cleaning sprays, bleach, ammonia, disinfectants and mixing products has been identified as risk factors [Citation18].
Access to reliable information and education on hazards and precautionary measures is a prerequisite for well-founded risk management [Citation14]. Safety data sheets (SDSs), provided to customers by suppliers of hazardous products, are intended to be one source of such information. Employees should have access to applicable SDSs, but several studies have shown poor compliance with these requirements [Citation19,Citation20]. In addition, shortcomings of the SDS information have been found, e.g., not identifying all hazards or sufficient risk management measures for cleaning agents [Citation21]. Furthermore, a recent Norwegian survey found that employers’ education of cleaning workers was ineffective from a chemicals risk management perspective [Citation22].
The objective of the present study was to describe workplace exposures to cleaning agents and disinfectants handled by the Swedish PIC, in particular focusing on the nature of the exposures and acute hazards involved in these incidents. The aim was to provide knowledge that can be used for occupational health and safety management.
2 Materials and methods
In Sweden, the PIC is centralized into one unit serving the whole country, offering a 24-h telephone consultation service open to all. The present study consists of a retrospective analysis of the PIC’s logged telephone consultations during a 5-year period (2010–2014) and follow-up interviews for calls made during the 3-month period of September–November 2016.
2.1 Retrospective analysis of PIC cases 2010–2014
During 2010–2014, the PIC received 9266 calls concerning 8240 individual occupational cases. Cleaning agents and disinfectants were involved in 1983 cases (24%).
The logged case data are entered by the PIC expert on call in real time during the telephone consultation. Each call receives a unique identifier, which is used to connect later calls about the same incident to the first call, allowing the identification of individual occupational cases. Besides recording whether the case is occupational or not, the PIC expert on call records the following information (examples of categories used):
Date and time of call.
Caller (public, hospital, primary care, ambulance).
Exposure route (eye, inhalation. skin, oral, several, injection, other/unknown).
Gender of exposed (female, male, unknown).
Question (free-text field).
Answer (free-text field).
Risk estimate (minor, moderate, major or undetermined).
Treatment advice (manage on site, seek health care, advice to health care professionals).
Risk estimates made by PIC experts are based on the reported exposure route, chemical product and symptoms. Minor risk corresponds to the risk of developing no or mild symptoms only, moderate risk to cases where pronounced or prolonged symptoms might occur and major risk to cases where severe symptoms are possible or reported.
We categorized the exposure agent logged by the PIC into chemical groups according to the major hazard as judged by the PIC expert on call. Minor editing was also made to the product category, grouping minor categories (up to 10 cases) into larger appropriate categories or into the general category ‘cleaning products’. In addition, free-text fields were read case by case for information on the workplace or occupation of the exposed, which was tabulated when available.
Analysis of data was performed using cross-tabulation and descriptive statistics, using R version 3.3.2.
2.2 Follow-up interviews 2016
During the 3-month follow-up period, 690 calls concerning 547 occupational cases with adults were recorded. Cleaning agents were involved in 26% of these cases (N = 142). Requests for study participation were only made if not delaying acutely required first aid measures. In total, 39 callers were asked whether a researcher could call back at a later time and inform about participation in this study and 32 agreed (Table ). We called consenting participants back within a week, placing calls at three different time points of the day. We reached 19 callers, and 17 consented to participate after receiving information about the study.
Table 1. Overview of number of cases concerning incidents with cleaning agents and disinfectants during the follow-up period, number that received a request to share contact details for further information about study participation and number of cases for which interviews were conducted.
Interviews were conducted over the telephone. After obtaining informed consent verbally, data on occupation and workplace were noted. Age of the exposed was only noted if speaking directly with the exposed person, gender was already noted in the PIC records. The participants were asked to describe the accident for which they had called the PIC. Follow-up questions concerned:
First aid measures.
Familiarity with the product.
Information sources about hazards, safe uses and first aid measures.
Contact with health care or leave of absence from work.
Interviews took about 15 min each, maximum 30 min. The interviewer (LS) took notes on a structured recording form containing the interview guide and wrote an anonymized summary directly after each interview. A content analysis was performed on the interview summaries by two of the authors (LS and KF). Both the retrospective study and the follow-up study were reviewed and approved by the regional ethical review (decisions 2015/1-31/5 and 2016/1295-31/5, respectively).
3 Results
3.1 Occupational cases handled by the Swedish Poisons Information Centre
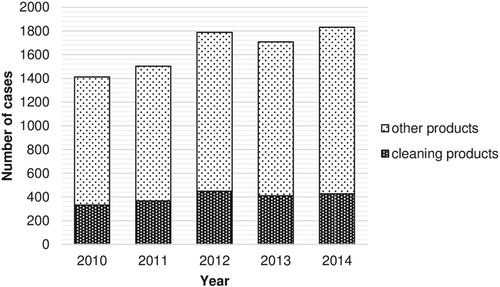
For the years 2010–2014, 23–25% of the occupational cases handled by the PIC concerned cleaning agents and disinfectants (Figure ), summing up to 1983 cases for the investigated period. The number of occupational cases handled by the PIC, both with cleaning agents and in general, increased by about 30% during the investigated period (Figure ).
Figure 1. Number of occupational cases and number of cases involving cleaning products, registered by the Swedish Poisons Information Centre for the period 2010–2014.
One-third of the cases concerning cleaning agents were judged by the PIC expert to pose a major risk (Table ). Eye exposure was more often judged to pose a major risk, while inhalation exposures and oral exposures were more frequently found to pose a minor risk ( = 180.4, p < 0.001; excluding cases where risk was undetermined and unknown/other routes). Major risk cases were most frequent for cases involving dishwasher detergents (55% major risk cases), oven and grill cleaners (50%), professional cleaning agents (48%), sanitary cleaning agents (43%) and caustic soda (37%). With the exception of the typically acidic sanitary cleaners, these groups are generally strongly alkaline (Table ).
Table 2. Overview of occupational cases involving cleaning agents and disinfectants recorded by the Swedish PIC for adults during 2010–2014: number of cases and proportion of minor, moderate and risk cases (%).
Females and males are relatively equally represented among cases concerning cleaning agents and disinfectants (Table ). However, men are over-represented among major risk cases ( = 38.4, p < 0.001; excluding cases where risk or gender was undetermined) and more often exposed to professional cleaning agents, whereas women more often call the PIC in relation to surface and hand disinfectants (Table ). Furthermore, exposure routes differ between genders; eye and oral (ingestion) exposures were more frequent among women, while skin exposures were more frequent among men (
= 26.4, p < 0.001; excluding cases with undetermined gender and unknown/other routes).
Information about the workplace or occupation was in most instances not possible to determine from the free-text entries. When identifiable (585 of 1983 cases), the most frequently occurring workplaces/occupations were restaurants and caterers (n = 215) and cleaners (n = 107), followed by other food production enterprises (n = 63) and dentistry, health and home care (n = 49).
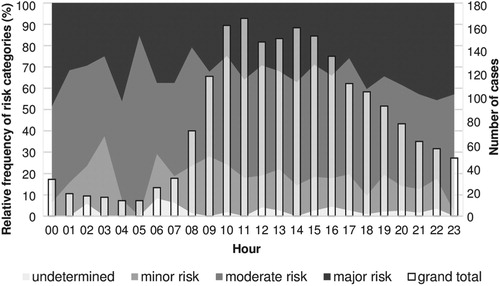
Based on the time of first call to the PIC, accidents involving cleaning agents occurred at all hours of the day (Figure ), albeit most of them during regular working hours between 09:00 and 17:00. However, the highest relative frequencies of major risk cases were found during late evenings and late nights ( = 9.18, p = 0.002, comparing incidents from 09:00 to 16:59 with incidents from 21:00 to 04:59).
Figure 2. Relative frequency of risk categories as judged by the Poisons Information Centre expert on calls stacked to 100% for each hour starting with 00:00–00:59 (left axis) and total number of occupational cases involving cleaning agents per hour for the years 2010–2014 (bars, right axis).
3.2 Follow-up interviews
During the 3-month follow-up period, 547 occupational cases with adults were recorded, of which cleaning agents were involved in 26% (N = 142). The two periods were compared to identify potential differences (Table ). We observed a slightly lower share of major risk cases during the follow-up period than during the retrospective period (26% vs 33%). However, this difference was not statistically significant, and neither were any of the other comparisons between the two periods presented in Table .
Table 3. Overall comparison between the datasets covered in the present study.
Primarily, the person calling the PIC was interviewed. In four cases, a manager (n = 3) or colleague (n = 1) was interviewed. Ten of the exposed individuals were male and seven were female. Age, only noted for 11 of the exposed individuals, ranged from 20 to 68 years with a median age of 42 years. Restaurants and caterers made up almost half of the interview cases (Table ); the remaining cases were spread across a wide range of sectors. The size of the workplaces also varied, although mostly the participants represented micro-sized or small and medium-sized enterprises (SME). Two were self-employed.
Table 4. Overview of interview cases, based on participants’ description of what happened and corresponding records from the Swedish PIC.
Our interviews revealed that the injuries/incidents in most cases occurred in connection to the use of the product: during dosing, application or dismantling of equipment (Table ). Almost half of the eye exposures were explained as caused by equipment failures. Although the extent to which these products are used in relation to worked hours differs considerably, most participants described themselves as experienced users of the products (Table ).
In almost all cases, the exposed person had not worn any protective equipment (Table ). Reasons for not using protective equipment ranged from it not being required, to it being unnecessary for short tasks to it being uncomfortable. In two cases, appropriate equipment was reportedly not available.
The appropriate first mitigation measure for eye and skin exposures was to rinse with water. Rinsing was initiated before contacting the PIC by 12 out of 14 persons with skin and eye exposure. One of the remaining persons did not have easy access to a first aid kit or water, and the other did not experience any immediate discomfort. In the three cases concerning other routes, no risk mitigation measures had been initiated before the call. The two persons exposed only via inhalation were judged as minor risk cases and were not advised health care examination; the follow-up calls also confirmed that no delayed respiratory effects had occurred. One individual was exposed via ingestion and advised to seek health care for examination. At the time of the follow-up call, the participant reported that no adverse health effects were found.
In terms of the PIC, experts risk estimate about half (6 out of 11) of moderate risk cases and all major risk cases (n = 4) were recommended to seek health care. This advice was also followed by all. In addition, five of the participants reported to have made one or more follow-up visit to a hospital or primary care, and three participants reported lost working days in addition to the day of injury (Table ).
Access to SDSs varied and only two participants stated that they read the SDS for information about first aid measures (Table ). In fact, most participants did not understand the question about access to SDSs and required a description of what an SDS is. These were told that it is a document provided by the supplier for many chemical products covering, amongst other things, information about hazards and first aid measures. Given this description, six of the participants referred to the package labelling (Table ), equating the two, either fully or with respect to information value.
4 Discussion
Occupational use of cleaning agents and disinfectants is widespread. In 2013, 8% of men and 19% of women reported exposure to these products for more than 25% of their working time [Citation15]. This is likely an underestimate of the population at risk for acute exposure, as these products are often used for shorter periods. Indeed, one-quarter of the Swedish PIC’s occupational cases involve cleaning agents or disinfectants. This is a considerably higher number, both in relative and absolute terms, compared with the official injury statistics based on employer’s reports [Citation7]. Hence, reviewing PIC data to learn from incidents and injuries is of interest for occupational health and safety management.
While certain cleaning agents inherently are low hazard products, such as all-purpose cleaners or hand sanitizers, many are hazardous. Overall, 33% of occupational cleaning agent cases are judged as major risk cases; the average for all chemical products is 21% [Citation6]. The potential harms involved in major risk cases are generally corrosive damage to eyes and skin, caused by alkali, acids and quaternary ammonium compounds. Improved risk management of cleaning agents thus has the potential to significantly reduce workplace injuries.
The high frequency of eye exposures (60% of all calls) indicates that safety glasses are not always used, which was supported by the follow-up interviews. Infrequent use of protective equipment has also been noted among hospital cleaners [Citation16]. In a number of cases, protective equipment was available to the participants but nevertheless not used. Hence, ensuring the use of protective equipment poses a deeper challenge than simply providing all employees with access and knowledge.
Failing to prevent exposure, the most important factor for the prognosis of corrosive eye exposures is immediate and thorough eye irrigation [Citation23]. Most of the participants suffering eye exposures had initiated eye flushing promptly. However, as noted in one interview case, lacking immediate access to water or eye-flushing kits could be one reason for delaying or ignoring eye irrigation. Considering the high number of eye exposures among PIC cases, managers should promote use of protective equipment but also ensure quick access to eye-flushing facilities, e.g., by storing eye-flushing kits together with relevant equipment, such as in cleaning trolleys.
Oral exposure/ingestion was an unexpected route of exposure in the workplace, yet constituting 8.8% of all investigated cases. One such case was included among our interviews. In this case, an unlabelled bottle of cleaning agent was mistaken for a water bottle, implicating the role of unlabelled or otherwise unsuitable containers. Mistaking cleaning agents for drinks has previously been pointed out as a typical scenario behind internal organ burns in South Korea [Citation24]. Such cases are preventable by systematic labelling and proper storage routines. An additional safeguard could be to add deterring colouring [Citation24].
Although males make up the majority of all occupational PIC cases (68% [Citation6]), the gender division is more equal among occupational cases concerning cleaning agents and disinfectants. However, as for the PIC occupational cases in general [Citation6], men are over-represented among major risk cases. These differences seem to reflect gender stratification in occupational use patterns; according to the PIC data, men more often call about often corrosive, professional cleaning agents and women more often about hand sanitizers, which generally are of low inherent hazard. Furthermore, men more frequently report skin exposures while women have a higher frequency of eye exposures. This raises the question of whether there are also structural factors connecting gender distribution and workplace safety precautions such as use of protective glasses.
While the PIC does not systematically register the workplace or occupation of the exposed, scrutiny of the free-text material indicates that restaurants and caterers are the most frequently implicated workplaces. Several previous studies have reported thermal and chemical burns as occupational injuries of cooks and food service workers. Horwitz and McCall [Citation25] found that workers in food service occupations were the occupational group most often filing workers’ compensation claims for thermal and chemicals burns. In a study on workers’ compensation claims due to burn injuries, Islam et al. [Citation26] found that 7% of cooks and food service workers had filed their claims due to chemical burns. The present work confirms that corrosive chemical products are an important occupational hazard in restaurants and caterers.
Horwitz and McCall [Citation25] found an increased risk for chemical burns among evening and nightshift workers across all food-service occupations. In the present study, we did note a higher relative frequency of major risk incidents during evenings and nights (Figure ). The diurnal variation might be related to night-specific work tasks, such as maintenance work, or to fatigue. Our observation is supported by other studies that found an increase in the risk of occupational injuries during evening and night-time work, mainly attributing the higher risk to sleepiness and fatigue [Citation27,Citation28].
Among the interview persons, labelling was clearly more important as an information source on hazards, precautionary measures and first aid than the SDS. Poor safety information could influence the frequency and severity of injuries due to insufficient information on proper use and/or first aid measures. Labelling is by design less detailed than the SDS, so future studies could investigate the role of different information sources in injury prevention for cleaning agents as well as the potential for adding certain safety information to labels.
Overall, we find that there were many insights to be gained regarding the nature of injuries and incidents involving cleaning agents and disinfectants from reviewing PIC data. However, there are also limitations to how the material from the PIC can be used for investigating occupational injuries. As discussed in previous work [Citation6,Citation7], the PIC does not register workplace data, meaning that we do not know the occupational context of these cases. In this study, we attempted to extract the information on occupation manually from free-text fields, which was only possible in 30% of cases. Detailed data on age would also be of interest as previous findings have indicated that younger and/or older workers are at higher risk for certain injuries. Hence, age-related data could identify such skewed risk relationships connected to, e.g., certain product groups.
We attempted to bridge some of the aforementioned knowledge gaps by follow-up interviews, but our two-step recruitment procedure was highly inefficient. Out of the 118 cases that our selection criteria targeted (i.e., callers from the public) we were only able to interview 16 (the 17th case being recruited through a call from health care). Low numbers are sensitive to stochastic effects, and while the interviews offer a range of examples of circumstances surrounding the occupational cases handled by the PIC, these findings are not generalizable, but can be seen as illustrations of real-life occupational accidents that include a consultation with the PIC. We conclude that identification of injury-prone occupations through PIC records is only practically feasible if the information is collected during PIC telephone consultations, as was done, e.g., by the Georgia Poison Center during their collaboration with the Occupational Safety and Health Administration [Citation5].
The main task of PICs is to provide advice to callers about management of (potential) poisoning cases. It is part of the PIC experts’ professionalism to work efficiently and only collect the most relevant information. Adding any demographic data to the standard information collected for occupational cases thus needs a clear purpose and recipient (e.g., a work environment agency). Furthermore, while adding such data would increase value for occupational injury surveillance and could possibly inform PIC practices as well, such a benefit has to be weighed against constraints such as potentially delaying first aid measures for the caller as well as callers in line.
5 Conclusions
The large number of occupational PIC cases shows there is a need for improved risk management concerning cleaning agents and disinfectants in Swedish workplaces. PIC data also offer insights about occupational incidents and injuries involving these products. However, there are challenges to using PIC data for occupational surveillance purposes. In particular, much value would be gained from recording occupation. In conclusion, we recommend work environment agencies and researchers to seek collaboration with PICs, and hope that the experiences described herein will contribute to efficient design of such collaborations.
Institution and ethics approval and informed consent
The work was performed at the Karolinska Institute. The study was reviewed and approved by the regional ethical review board in Stockholm (decisions 2015/1-31/5 and 2016/1295-31). Verbal informed consent was collected from the interview participants.
Acknowledgements
The authors thank the interview participants who graciously agreed to participate in the present study and the PIC experts on call who assisted in the recruitment of interview participants.
Disclosure statement
No potential conflict of interest was reported by the authors.
ORCID
Linda Schenk http://orcid.org/0000-0003-3799-4814
Additional information
Funding
References
- Bryant SM, Aks SE. Dropping acid at school: hydrochloric acid exposures in chemistry class. Clin Toxicol. 2012;50:449. doi: 10.3109/15563650.2012.675437
- Schenk L, Taher IA, Öberg M. Identifying the scope of safety issues and challenges to safety management in Swedish middle school and high school chemistry education. J Chem Educ. 2018;95:1132–1139. doi: 10.1021/acs.jchemed.8b00054
- Blanc PD, Olson KR. Occupationally related illness reported to a regional poison control center. Am J Public Health. 1986;76:1303–1307. doi: 10.2105/AJPH.76.11.1303
- Litovitz T, Oderda G, White JD, et al. Occupational and environmental exposures reported to poison centers. Am J Public Health. 1993;83:739–743. doi: 10.2105/AJPH.83.5.739
- Tustin AW, Jones A, Lopez GP, et al. Occupational chemical exposures: a collaboration between the Georgia Poison Center and the Occupational Safety and Health Administration. Clin Toxicol. 2018;56:55–62. doi: 10.1080/15563650.2017.1338718
- Schenk L, Feychting K, Annas A, et al. Records from the Swedish Poisons Information Centre as a means for surveillance of occupational accidents and incidents with chemicals. Saf Sci. 2018;104:269–275. doi: 10.1016/j.ssci.2017.10.021
- Schenk L, Öberg M. Comparing data from the Poisons Information Centre with employers’ accident reports reveal under-recognized hazards at the workplace. Ann Work Expo Health. 2018;62:517–529. doi: 10.1093/annweh/wxy009
- Trueblood AB, Shipp EM. Characteristics of occupational pesticide exposures reported to poison control centers in Texas, 2000–2015. Arch Environ Occup Health. 2017;12:1–8. doi: 10.1080/19338244.2017.1339011
- Hinnen U, Hotz P, Gossweiler B, et al. Surveillance of occupational illness through a national poison control center: an approach to reach small-scale enterprises? Int Arch Occup Environ Health. 1994;66:117–123. doi: 10.1007/BF00383367
- Lavon O, Bentur Y. Poison exposures in young Israeli military personnel: a national poison center data analysis. Clin Toxicol. 2017;55:322–325. doi: 10.1080/15563650.2016.1278225
- Rubenstein H, Bresnitz EA. The utility of Poison Control Center data for assessing toxic occupational exposures among young workers. J Occup Environ Med. 2001;43:463–466. doi: 10.1097/00043764-200105000-00006
- Woolf A, Alpert HR, Garg A, et al. Adolescent occupational toxic exposures. Arch Pediatr Adolesc Med. 2001;155:704–710. doi: 10.1001/archpedi.155.6.704
- Ziqubu-Page T, Forrester MB. Adolescent workplace exposures reported to Texan poison centers. Int J Adolesc Med Health. 2016;30(3):20160057. doi: 10.1515/ijamh-2016-0057
- European Agency for Safety and Health at Work. Preventing harm to cleaning workers. Luxemburg: European Agency for Safety and Health at Work; 2009. doi: 10.2802/10668
- SWEA – Swedish Work Environment Authority. The work environment 2013. Stockholm: Swedish Work Environment Authority; 2014. (Arbetsmiljöstatistik [Work Environment Statistics]; no. 2014:3). Swedish. https://www.av.se/globalassets/filer/statistik/arbetsmiljostatistik-arbetsmiljon-2013-rapport-2014-03.pdf
- Lee S-J, Nam B, Harrison R, et al. Acute symptoms associated with chemical exposures and safe work practices among hospital and campus cleaning workers: a pilot study. Am J Ind Med. 2014;57:1216–1226. doi: 10.1002/ajim.22376
- Bauer A. Contact dermatitis in the cleaning industry. Curr Opin Allergy Clin Immunol. 2013;13(5):521–524. doi: 10.1097/ACI.0b013e328364ec21
- Siracusa A, De Blay F, Folletti I, et al. Asthma and exposure to cleaning products – a European Academy of Allergy and Clinical Immunology task force consensus statement. Allergy. 2013;68:1532–1545. doi: 10.1111/all.12279
- Schenk L, Antonsson A-B. Implementation of the chemicals regulation REACH – exploring the impact on occupational health and safety management among Swedish downstream users. Saf Sci. 2015;80:233–242. doi: 10.1016/j.ssci.2015.08.001
- Nicol A-M, Hurell AC, Wahyuni D, et al. Accuracy, comprehensibility, and use of material safety data sheets: A review. Am J Ind Med. 2008;51:861–876. doi: 10.1002/ajim.20613
- Suleiman AM, Svendsen KVH. Are safety data sheets for cleaning products used in Norway a factor contributing to the risk of workers exposure to chemicals? Int J Occup Med Environ Health. 2014;27:840–853. doi: 10.2478/s13382-014-0302-8
- Suleiman AM, Svendsen KVH. Effectuality of cleaning workers’ training and cleaning enterprises’ chemical health hazard risk profiling. Saf Health Work. 2015;6:345–352. doi: 10.1016/j.shaw.2015.10.003
- Kuckelkorn R, Schrage N, Keller G, et al. Emergency treatment of chemical and thermal eye burns. Acta Ophthalmol Scand. 2002;80:4–10. doi: 10.1034/j.1600-0420.2002.800102.x
- Koh D-H, Lee S-G, Kim H-C. Incidence and characteristics of chemical burns. Burns. 2017;43:654–664. doi: 10.1016/j.burns.2016.08.037
- Horwitz IB, McCall BP. An analysis of occupational burn injuries in Rhode Island: workers’ compensation claims, 1998 to 2002. J Burn Care Rehabil. 2005;26:505–514. doi: 10.1097/01.bcr.0000185399.39280.bd
- Islam SS, Nambiar AM, Doyle EJ, et al. Epidemiology of work-related burn injuries: experience of a state-managed workers’ compensation system. J Trauma. 2000;49:1045–1051. doi: 10.1097/00005373-200012000-00012
- Dinges DF. An overview of sleepiness and accidents. J Sleep Res. 1995;4:4–14. doi: 10.1111/j.1365-2869.1995.tb00220.x
- Dembe AE, Erickson JB, Delbos RG, et al. Nonstandard shift schedules and the risk of job-related injuries. Scand J Work Environ Health. 2006;32:232–240. doi: 10.5271/sjweh.1004
