
Abstract
Purpose. The aim of this article was to evaluate the effects of cycle and treadmill desks on energy expenditure and cardiovascular and biochemical indicators in sedentary workers. Materials and methods. In February 2018, six databases were searched. Both parallel and crossover design studies evaluating workplace cycle and treadmill desks compared to a conventional seated condition were included. Results. Twenty-two studies met the inclusion criteria. Cycle and treadmill desks significantly increased energy expenditure (standard mean difference [SMD] = 3.84, p < 0.001, I2 = 95%) and the heart rate (SMD = 1.68, p < 0.001, I2 = 91%), and lowered blood glucose and insulin levels (SMD = –0.54, p < 0.001, I2 = 0% and SMD = –3.13, p < 0.001, I2 = 76%, respectively). The interventions had no effect on blood pressure and other biochemical indicators. Conclusion. Cycle and treadmill desks may positively influence energy expenditure in sedentary workers and could be effective for reducing negative effects of workplace-related sedentary behaviour. However, considerable heterogeneity is present in the measuring protocols for energy expenditure.
1. Introduction
Insufficient physical activity (PA) levels and obesity are issues of considerable concern in modern society [Citation1]. The prevalence of obesity in adults is up to 40% in the USA [Citation2] and up to 47.6% in Europe [Citation3]. In Canada, up to 37% of the adult population is abdominally obese [Citation4]. Moreover, Toselli et al. [Citation5] report that in North Africa 1.3–47.8% of adults are overweight or obese, with great differences between the rural and the urban residents. In China, the prevalence of overweight male adults significantly increased from 8 to 17% in the years between 1992 and 2009; the increase was also significant in female adults [Citation6]. Similar increases in overweight and obese adults are recognized in other parts of Asia [Citation6,Citation7].
Additionally, there has been an increase in sedentary behaviour, which is identified as an independent risk factor for the development of non-communicable diseases [Citation8,Citation9]. Sick leave is often related to sedentary behaviour [Citation10] and insufficient PA [Citation11]. PA can be effective in preventing obesity [Citation12] and reducing body mass [Citation13]. The results of objectively measured PA among adults in the USA show that fewer than 5% reach the recommended 30 min of moderate PA per day [Citation14]. Similarly, in Canada only 5% of adults accumulate 150 min of moderate to vigorous PA per week [Citation15].
The increase in energy intake and the decrease in PA-related energy expenditure (EE) are amongst the main reasons for obesity [Citation16]. In the last 50 years, the number of adults employed in sedentary occupations increased by 76% in the USA [Citation17]. It has been reported that people expend about 75–85 kcal/h in seated positions [Citation18], whereas when walking at approximately 1.5 km/h the EE will increase to 250 kcal/h [Citation19]. It has been estimated that office workers spend up to 80% of their working time sedentary [Citation20] and do not compensate by sitting less in their leisure time [Citation21]. There are several reasons for physical inactivity among working adults, including a lack of time, family responsibilities, scheduling constraints and work [Citation22,Citation23]. Therefore, implementing PA during working hours is a reasonable recommendation.
Workplace interventions such as cycle and treadmill desks enable the user to be physically active while working. Meta-analyses to date have focused mostly on the effects of workplace interventions on sedentary behaviour and PA levels [Citation24–29]. Only one meta-analysis targeted EE [Citation30]. These meta-analyses included studies with different interventions (active breaks, educational workshops, prompts, sit-to-stand desks, cycle and treadmill desks, etc.). The effects of cycle and treadmill desks on EE and cardiovascular and biochemical indicators have not yet been determined. Moreover, the volume of research regarding active workstations has expanded rapidly in recent years, since new solutions have been proposed to counteract sedentarism and insufficient PA. Therefore, there is a need to re-evaluate the effects of these interventions.
The aim of the present article is to systematically review and, using a meta-analytical approach, assess the studies evaluating cycle and treadmill desk workplace interventions. We hypothesized that the interventions would increase EE and favourably affect cardiovascular and biochemical indicators.
2. Methods
2.1. Study selection criteria
The inclusion criteria were determined based on the PICOS search tool [Citation31]:
Population (P): sedentary workers (e.g., office workers) aged between 18 and 65 years with no medical conditions.
Intervention (I): cycle desk or treadmill desk.
Comparisons (C): conventional sitting.
Outcome (O): objectively measured EE and cardiovascular (heart pressure, heart rate) and biochemical (blood glucose and insulin, cholesterol, triglycerides, cortisol, dopamine) indicators.
Study design (S): randomized controlled trials (RCTs), non-randomized parallel group design study and crossover (CO) study designs.
Other inclusion criteria were peer-reviewed articles published in the English language.
2.2. Search strategy and study selection
Two authors independently searched six databases in February 2018 (PubMed, ScienceDirect, Scopus, Embase, Web of Science, PEDro). The search strategy was based on the search terms within four main elements: (a) sedentary behaviour and its synonyms; (b) workplace PA and its synonyms; (c) types of intervention and its synonyms; (d) outcome parameters. Titles and abstracts were searched in all databases using search terms merged with ‘AND’ and ‘OR’. Additionally, reference lists of relevant published systematic review papers were reviewed. The complete list of search terms and the list of systematic reviews are shown in Supplementary File 1.
The study selection process consisted of three phases. In the first phase, two reviewers independently screened the article titles. In the second phase, the abstracts of all articles selected from the first phase were reviewed and assessed by two reviewers independently. In the final phase, the remaining articles were fully reviewed by two reviewers using the pre-determined inclusion criteria. Any disagreement between reviewers was solved by the third author.
2.3. Quality assessment
Two authors independently assessed the methodological quality of all the studies included with a 10-level PEDro scale (10–9 = excellent, 8–6 = good, 5–4 = fair, < 4 = poor [Citation32]) for the following domains: (a) subjects were randomly allocated to groups; (b) allocation was concealed; (c) the groups were similar at baseline regarding the most important prognostic indicators; (d) there was blinding of all subjects; (e) there was blinding of all therapists who administered the therapy; (f) there was blinding of all assessors who measured at least one key outcome; (g) measures of at least one key outcome were obtained from more than 85% of the subjects initially allocated to groups; (h) all subjects for whom outcome measures were available received the treatment or control condition as allocated or, where this was not the case, data for at least one key outcome were analysed by ‘intention to treat’; (i) the results of between-group statistical comparisons are reported for at least one key outcome; (j) the study provides both point measures and measures of variability for at least one key outcome [Citation33]. The PEDro scale has been identified as a reliable tool for assessing study quality [Citation33]. Moreover, this scale is the eligible methodological assessment tool for all study designs included, as it covers the four main types of biases suggested by the Cochrane Collaboration: (a) selection bias; (b) performance bias; (c) attrition bias; (d) detection bias [Citation34].
2.4. Data extraction
The study design, intervention type, duration and intensity, the number of participants and participants’ sex, mean age and mean body mass index (BMI), the environment (laboratory, office) and outcome data from the eligible studies were extracted and entered into Microsoft Excel version 2016. Where the data were incompletely reported, the authors were contacted to obtain the missing data.
2.5. Data synthesis and analysis
Analyses were conducted in Review Manager version 5.3 using the inverse variance method and the random effects model. The effect sizes were estimated using the standard mean difference (SMD) due to the heterogeneity in the measurement protocol and the measurement equipment. The differences between the intervention group and the control group or between the condition after or during the intervention (depending on study protocol) were analysed. When pre/post values were reported, the mean difference of these values was used, andthe mean standard deviation was calculated using the equation SD = √[(SD12 + SD22) − (2 × r × SD1 × SD2)], applying a correlation value of 0.9. Statistical heterogeneity among studies was determined by calculating I2. The significance threshold was set at p ≤ 0.05. The subgroup analyses were based on the intervention type (cycling, walking) and the measurement time (worktime, daily).
Only studies reporting EE at the workplace in kilocalories were included in the meta-analysis. Studies were divided according to the intervention type (cycle desk and treadmill desk). Moreover, the results of the intervention group – evaluating the effects on EE at different intensities – were included separately in the meta-analysis. The intervention intensities are defined in the forest plots. Only studies in which the heart rate and blood pressure were evaluated during worktime or during an intervention were included in the meta-analysis.
3. Results
3.1. Literature search and study characteristics
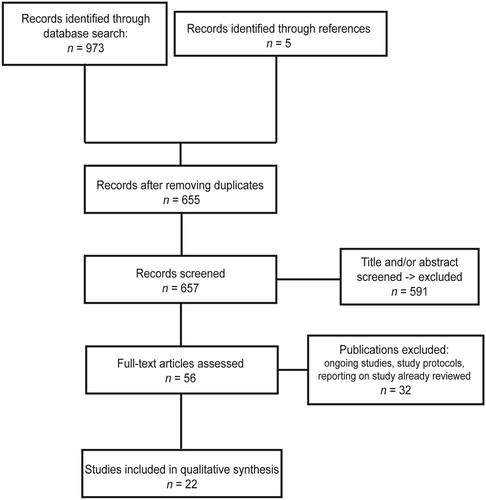
The database search identified 973 studies. Altogether, 22 studies met the inclusion criteria and were included in the qualitative synthesis (see Figure ). The mean age of study participants was 36.7 ± 8.8 years and their mean BMI was 28.8 ± 3.7. In total, 622 participants took part (229 males, 311 females, 82 unidentified). One study was a RCT [Citation35], one study was of a non-randomized parallel group design [Citation36] and 20 studies were CO in design [Citation37–56]. Seven studies evaluated a cycling intervention, 13 studies evaluated a walking intervention and two studies evaluated both types of intervention (see Supplementary File 2). Five studies were conducted in operating workplaces [Citation36,Citation43,Citation44,Citation47,Citation50] and 17 in laboratory environments. The intervention duration varied from 1 day in the laboratory [Citation7,Citation54] to interventions lasting several weeks [Citation36,Citation50]. The quality of the studies was fair (mean PEDro score 5.2/10, median PEDro score 5). Five studies published in the PEDro database [Citation35,Citation41,Citation43,Citation47,Citation50] already had a quality evaluation, and the others were evaluated by the authors (see Supplementary File 3).
Figure 1. Flow diagram of the study selection protocol.
3.2. Measures of EE
There was substantial heterogeneity regarding the methodological approaches in determining EE (see Table ). EE was reported either as the metabolic equivalent (MET) or in kilocalories. Botter et al. [Citation45] and Carr et al. [Citation44] reported the EE values in both METs and kilocalories. Two studies reported daily EE in kilocalories [Citation36,Citation47] and four studies reported on worktime-specific EE in kilocalories [Citation39,Citation49,Citation53,Citation55]. Among these studies, Koepp et al. [Citation55] and Levine and Miller [Citation53] reported EE with and without normalization by body mass.
Table 1. Measuring tools used in the included studies.
3.3. The effects of interventions on EE
Eight studies were included in the systematic review of EE in sedentary workers (see Supplementary File 2). Cycling interventions were evaluated in four studies [Citation36,Citation39,Citation44,Citation49] and treadmills were evaluated in four studies [Citation45,Citation47,Citation53,Citation55]. EE in the studies by Carr et al. [Citation44] and Elmer and Martin [Citation39] varied from 1.7 to 3.25 METs in the intervention group and from 0.8 to 1.3 METs in the control group. The EE in kilocalories varied from 198 to 450 kcal in the intervention group and from 59 to 191 kcal in the control group, respectively. Daily EE was evaluated in two studies [Citation36,Citation47], which observed expenditures from 1200 ± 27 to 2328 ± 343 kcal/day in the intervention group and from 896 ± 16 to 2356 ± 490 kcal/day in the control group.
Altogether, five studies were included in the meta-analysis (see Figure ), which indicated a significant increase in total EE in the intervention group (SMD = 3.84, 95% CI [2.44, 5.23], p < 0.001, I2 = 95%). Cycling interventions alone significantly increased EE (SMD = 6.50, 95% CI [3.26, 9.74], p < 0.001, I2 = 95%), as did walking interventions (SMD = 2.23, 95% CI [1.22, 3.25], p < 0.001, I2 = 89%). The differences between the intervention types were statistically significant (p = 0.010) and the heterogeneity between the studies was considerable (p < 0.001, I 2 = 83.5%).
Figure 2. Effects of interventions on energy expenditure.
Note: IV = inverse variance; CI = confidence interval; 3.1 [Citation49] = cycling intervention at 20% of maximal aerobic power; 3.2 [Citation49] = cycling intervention at 50% of maximal aerobic power: 4.1 [Citation55] = walking intervention at speed 1.6 km/h; 4.2 [Citation55] = walking intervention at speed 3.2 km/h; 4.3 [Citation55] = walking intervention at speed 4.8 km/h; 5.1 [Citation53] = walking intervention at speed 1.6 km/h; 5.2 [Citation53] = walking intervention at speed 3.2 km/h; 5.3 [Citation53] = walking intervention at speed 4.8 km/h.
![Figure 2. Effects of interventions on energy expenditure.Note: IV = inverse variance; CI = confidence interval; 3.1 [Citation49] = cycling intervention at 20% of maximal aerobic power; 3.2 [Citation49] = cycling intervention at 50% of maximal aerobic power: 4.1 [Citation55] = walking intervention at speed 1.6 km/h; 4.2 [Citation55] = walking intervention at speed 3.2 km/h; 4.3 [Citation55] = walking intervention at speed 4.8 km/h; 5.1 [Citation53] = walking intervention at speed 1.6 km/h; 5.2 [Citation53] = walking intervention at speed 3.2 km/h; 5.3 [Citation53] = walking intervention at speed 4.8 km/h.](/cms/asset/8c5a1548-8e92-474b-b256-928107b83b2e/tose_a_1562688_f0002_ob.jpg)
The study by Tronarp et al. [Citation49] was included twice because the authors evaluated the EE at two different intensities. In the Forest plot (Figure ), 3.1 [Citation49] presents the EE values obtained for low-intensity cycling and 3.2 [Citation49] those for high-intensity cycling. The results of 3.2 [Citation49] (cycling at an intensity of 50% of maximal aerobic power) were outstanding compared to the other results (EE in the intervention group 450 ± 43 kcal compared to 84 ± 6 kcal in the control group) (Figure ). If the results of 3.2 [Citation49] were not included in the meta-analysis, the overall effect of interventions was lower, as was study heterogeneity (SMD = 3.07, 95% CI [1.93, 4.21], p < 0.001, I 2 = 93%).
3.4. The effects of interventions on cardiovascular indicators
Ten studies were included in the meta-analysis of cardiovascular indicators (see Supplementary File 2). Separate meta-analyses were conducted for the heart rate, systolic blood pressure and diastolic blood pressure (see Supplementary File 4). The heart rate measured during worktime in the studies varied from 77 to 110.6 bpm in the intervention group and from 71 to 82 bpm in the control group. Studies evaluating the daily heart rate [Citation38,Citation46] observed a mean value of 78–80 bpm in the intervention group and 70–72 bpm in the control group. The pooled effect size showed a significant increase in heart rate (SMD = 1.68, 95% CI [1.13, 2.23], p < 0.001, I2 = 91%) in the intervention group. When analysed separately, both interventions significantly increased the heart rate (cycling SMD = 1.71, 95% CI [0.33, 3.10], p = 0.020, I2 = 94%; walking SMD = 1.67, 95% CI [1.10, 2.25], p < 0.001, I2 = 89%). The differences between the intervention types were not statistically significant (p = 0.820) and heterogeneity between studies was not present (p < 0.001, I2 = 0%).
Seven studies investigated the effects of the interventions on blood pressure (see Supplementary File 2). The meta-analysis revealed no effect on either systolic blood pressure (p = 0.420) or diastolic blood pressure (p = 0.350). Moreover, cycling or walking interventions alone did not have an influence on blood pressure values.
3.5. The effects of interventions on biochemical indicators
Five studies examined the effects of cycle and treadmill desks on biochemical indicators (see Supplementary File 4). High-density lipoprotein cholesterol (HDL) and triglyceride levels were assessed in two studies [Citation35,Citation55]. One study assessed low-density lipoprotein cholesterol (LDL) and overall cholesterol levels [Citation35]. Blood glucose levels were assessed by three studies [Citation41,Citation50,Citation52] and insulin levels by two studies [Citation41,Citation52]. One study [Citation46] assessed dopamine levels and two studies [Citation46,Citation56] assessed cortisol levels.
Interventions lowered both blood glucose and insulin levels (SMD = –0.54, p < 0.001, I2 = 0% and SMD = –3.13, p < 0.001, I2 = 76%, respectively). All included studies used the treadmill desk intervention and were performed in a laboratory environment.
The meta-analysis showed no effect on triglyceride levels (p = 0.230). Furthermore, the meta-analysis showed no effect on whole (p = 0.770), HDL (p = 0.860) or LDL (p = 0.200) cholesterol. No effect was shown either on dopamine (p = 0.810) or cortisol (p = 0.190).
Five studies assessed workers’ perceived exertion (122 participants). The meta-analysis indicated a significant increase in perceived exertion among the participants in the intervention group (SMD = 2.95, p < 0.001, I2 = 92%), with greater exertion on treadmills (SMD = 4.01, p < 0.001) compared to cycle desks (SMD = 2.41, p < 0.001). The differences between intervention types were statistically significant (p = 0.010).
4. Discussion
The aim of the present study was to objectively evaluate the effects of workplace cycle and treadmill desks on EE and cardiovascular and biochemical indicators in sedentary workers. The results suggest a significant increase in EE and heart rate, a decrease of blood glucose and insulin levels, and no effect on blood pressure and biochemical indicators (cholesterol, triglycerides, cortisol, dopamine) due to cycle and treadmill desk implementation.
Because of the evidential intervention condition (cycling and walking), blinding participants and therapists in the related studies was impossible. Thus, the studies were unable to avoid blinding bias. Other study weaknesses included short intervention durations [Citation41,Citation45,Citation46,Citation52,Citation53,Citation57] and small sample sizes [Citation38,Citation39,Citation45,Citation54].
The heterogeneity between studies included in these meta-analyses on EE was considerable, varying from 89 to 95%. When interpreting the results of the meta-analysis, differences in sample size, intervention duration and intensity, and the use of different measuring methods in the included studies must be considered. The sample size among included studies varied from 10 [Citation39] to 36 [Citation49] participants. Two studies defined the cycling intensity by revolutions per minute and in Watts [Citation39,Citation44], one study defined the cycling intensity as the percentage of maximal heart rate [Citation49] and two studies defined walking intensity in kilometres per hour [Citation53,Citation55]. The equipment for measuring EE varied substantially among the studies (heart rate monitor, accelerometers, indirect calorimetry, spirometry). Spirometry remains the gold standard for evaluating EE [Citation58]. EE data derived from the SenseWear (BodyMedia, Inc., USA) accelerometers were shown to be reliable during light-intensity stepping [Citation59]. Moreover, the simultaneous heart rate monitor technique, using a Polar heart rate transmitter (Polar Electro, Finland), was shown to be an accurate predictor of EE during activity in comparison to indirect calorimetry [Citation60]. The EE values were presented either in METs or in kilocalories. The MET is a widely used physiological concept for expressing the energy cost of physical activities. However, it has been shown that expressing EE in METs is not suitable for everyone and that 1 MET of 1 kcal × kg–1 × h−1 overestimates the resting EE by 20% for a large heterogeneous sample [Citation61]. Also, when EE is presented in kilocalories, normalization by the body mass is needed. Only two studies included in this meta-analysis [Citation53,Citation55] reported the EE values normalized by the body mass. Despite the discrepancies among the included studies, the meta-analysis was conducted to objectively and quantitatively evaluate the overall effect of cycle and treadmill desk interventions.
The results of this article demonstrate a significant increase in daily and worktime EE when using cycle or treadmill desks. Similar results have been demonstrated in a meta-analysis by Cao et al. [Citation30]. Nevertheless, the results are not completely comparable since Cao et al. [Citation30] did not conduct a separate meta-analysis for cycle and treadmill desk conditions. Also, additional new papers are included in the present meta-analysis. The review by Torbeyns et al. [Citation62] reported an increase in EE from 100 to 405 kcal when using treadmill desks. For an adult with a body mass of 70 kg, this could increase the EE up to 5.7 MET. This increase in EE could reduce sedentary behaviour and increase both low and moderate PA. This increase in PA is desired since performing moderate-intensity PA might reduce the risks associated with being overweight, obesity and cardiovascular disease [Citation63].
This meta-analysis indicated a significant increase of heart rate and revealed no effect of interventions on systolic and diastolic blood pressure. These results are consistent with the meta-analysis by Reed et al. [Citation28]. However, Reed et al. [Citation28] evaluated the effects of the interventions that included counselling, fitness testing, messages and email prompts, diet and health promotion on working-age woman whereas this meta-analysis reports the effects of cycle and treadmill desks on sedentary workers. Two studies included in this meta-analysis [Citation37,Citation38] focused primarily on the effects of cycle and treadmill desk interventions on blood pressure compared to a seated condition. In a study by Zeigler et al. [Citation37], subjects with prehypertension were included (prehypertension was defined as mean systolic blood pressure of 120–139 mmHg and mean diastolic blood pressure of 80–90 mmHg). Similarly, in another study by Zeigler et al. [Citation38], the inclusion criteria were prehypertension and BMI > 25. Other studies did not have such inclusion criteria and the assessment of blood pressure was a collateral measurement. Performing low and moderate-intensity PA is related to lower blood pressure in adults [Citation64,Citation65]. Nevertheless, the cycle and treadmill desks have not been shown to influence blood pressure, possibly due to the short duration of the interventions. The long-term effects of cycle and treadmill desks on the cardiovascular parameters should be additionally evaluated by studies with longer duration (several weeks, months) of the interventions.
Among the biochemical indicators examined, only blood glucose and insulin levels were affected by cycle and treadmill desk interventions. Similar results are reported in the meta-analysis by Reed et al. [Citation28]. Reed et al.’s paper [Citation28] revealed that cycle and treadmill desks have a comparable effect to single and multi-component interventions. Studies included in this meta-analysis examining blood glucose levels differed substantially regarding the study environment and the inclusion criteria of the participants. Two studies were conducted in a laboratory environment [Citation41,Citation52] and one in an office environment [Citation55]. The study by Dunstan et al. [Citation41] only included participants with BMI > 25, whereas the other two studies had no such inclusion criteria. The two studies examining insulin levels were both conducted in a laboratory environment [Citation41,Citation52]. Because of the substantial heterogeneity between the studies, the results for blood glucose and insulin levels must be interpreted with caution. They reflect acute rather than long-term effects of treadmill desk interventions. Studies with longer intervention periods are desired to investigate the long-term effects of workplace cycling and walking on biochemical indicators in sedentary workers. The treadmill desk intervention induced greater perceived exertion in sedentary workers compared to cycle desks (p = 0.010). This result is justifiable since the seated cycling posture results in smaller movement of the upper body compared to walking and is therefore possibly less disruptive for the user. Perceived exertion might be decreased in the case of long-term use of cycle and treadmill desks since performing two independent motor tasks simultaneously may be improved with practice [Citation66,Citation67].
Different aspects of PA, EE and sitting time in sedentary workers should be considered when designing new studies. Leisure-time PA is shown to be associated with a reduced risk of pre-mortality [Citation68], therefore more focus could be given to assess the effects of workstations on leisure-time EE and PA. The long-term effectiveness of active workstations is also unclear. Koepp et al. [Citation69] showed a decrease after 6 months and renewed increase in sedentary behaviour after 12 months of intervention. As non-communicable chronic diseases are a risk to the health of the population [Citation70], further studies need to focus particularly on the possible impacts the active workstation may have on chronic disease. Most of the studies included in the present article involved relatively healthy participants. Different effects might be observed in populations already suffering from a chronic disease.
Reviews conducted to date show mostly positive effects of active workstations on sedentary behaviour, PA, EE, cognitive function and contrasting results in work performance [Citation24–30,Citation62,Citation71,Citation72]. Most papers have focused on reducing sedentary behaviour and increasing PA in workers and included studies with different types of interventions, such as sit-to-stand desks, cycle and treadmill desks, active breaks, counselling, health promotion, etc. For example, Chu et al. [Citation24] included studies that combined mixed environmental and educational interventions. Ojo et al. [Citation72] focused on the effects of active workstations on work and cognitive performance, whereas Reed et al. [Citation28] focused on studies evaluating the effects on cardiometabolic parameters and included studies only with female participants. In the review by Shrestha et al. [Citation29] the focus was on sedentary behaviour and EE, with the studies included evaluating different interventions (sit-to-stand, cycle desks, etc.). One meta-analysis targeted EE [Citation30]. No review and meta-analysis to date has evaluated the effects of cycle and treadmill desks alone on EE and cardiometabolic parameters.
There are certain limitations associated with the present article. Firstly, only papers published in English were included. Secondly, only peer-reviewed papers were evaluated. Although this could have induced a selection bias, it ensured that the papers included were of sufficient quality. Cycle and treadmill desks as methods to promote individuals’ health have only recently become prominent areas of research, and many studies which have assessed the effects of such interventions are preliminary and short. Nevertheless, this article indicates that the use of cycle and treadmill desks could be effective in promoting health and is worth further investigation. The results show that cycle and treadmill desks could positively influence EE, blood glucose and insulin levels. No effect of interventions was found for blood pressure and biochemical indicators (cholesterol, triglycerides, dopamine, cortisol), possibly due to the short durations of the interventions.
5. Conclusion
Cycle and treadmill desks could be effective in reducing the negative effects of sedentary work. Studies including participants who already have chronic diseases and studies with larger sample sizes and longer evaluation periods are desired to further explore and determine the effects of cycle and treadmill desks on EE and cardiovascular and biochemical indicators.
Supplemental File 1
Download MS Word (18.6 KB)Supplemental File 2
Download MS Word (20.6 KB)Supplemental File 3
Download MS Word (25.5 KB)Supplemental File 4
Download MS Word (366.4 KB)Acknowledgements
The authors gratefully acknowledge the European Commission for funding the InnoRenew CoE project and the Republic of Slovenia.
Disclosure statement
No potential conflict of interest was reported by the authors.
Supplemental data
Supplemental data for this article can be accessed at https://doi.org/10.1080/10803548.2018.1562688.
Additional information
Funding
Related Research Data
References
- Street SJ, Wells JCK, Hills AP. Windows of opportunity for physical activity in the prevention of obesity. Obes Rev. 2015;16(10):857–870.
- Ogden CL, Fakhouri TH, Carroll MD, et al. Prevalence of obesity among adults, by household income and education – United States, 2011–2014. MMWR Morb Mortal Wkly Rep. 2017;66(50):1369–1373.
- Gallus S, Lugo A, Murisic B, et al. Overweight and obesity in 16 European countries. Eur J Nutr. 2015;54(5):679–689.
- Janssen I. The public health burden of obesity in Canada. Can J Diabetes. 2013;37(2):90–96.
- Toselli S, Gualdi-Russo E, Boulos DN, et al. Prevalence of overweight and obesity in adults from North Africa. Eur J Public Health. 2014;24(1):31–39.
- Xi B, Liang Y, He T, et al. Secular trends in the prevalence of general and abdominal obesity among Chinese adults, 1993–2009. Obes Rev. 2012;13(3):287–296.
- Cai L, Han X, Qi Z, et al. Prevalence of overweight and obesity and weight loss practice among Beijing adults, 2011. PLoS One. 2014;9(9):e98744. doi: 10.1371/journal.pone.0098744
- Wilmot EG, Edwardson CL, Achana FA, et al. Sedentary time in adults and the association with diabetes, cardiovascular disease and death: systematic review and meta-analysis. Diabetologia. 2012;55(11):2895–2905.
- Katzmarzyk PT, Church TS, Craig CL, et al. Sitting time and mortality from all causes, cardiovascular disease, and cancer. Med Sci Sports Exerc. 2009;41(11):998–1005.
- Martínez-López E, Saldarriaga-Franco J. Sedentariness and absenteeism in the work setting. Rev Salud Publica (Bogota). 2008;10(2):227–238.
- Losina E, Yang HY, Deshpande BR, et al. Physical activity and unplanned illness-related work absenteeism: data from an employee wellness program. PLoS One. 2017;12(5):e0176872. doi: 10.1371/journal.pone.0176872
- Jakicic JM, Davis KK. Obesity and physical activity. Psychiatr Clin North Am. 2011;34(4):829–840.
- Pavey TG, Peeters GMEE, Gomersall SR, et al. Long-term effects of physical activity level on changes in healthy body mass index over 12 years in young adult women. Mayo Clin Proc. 2016;91(6):735–744.
- Troiano RP, Berrigan D, Dodd KW, et al. Physical activity in the United States measured by accelerometer. Med Sci Sport Exerc. 2008;40(1):181–188.
- Colley RC, Garriguet D, Janssen I, et al. Physical activity of Canadian adults: accelerometer results from the 2007 to 2009 Canadian Health Measures Survey. Health Rep. 2011;22(1):7–14.
- Levine JA. Nonexercise activity thermogenesis (NEAT): environment and biology. Am J Physiol Metab. 2004;286(5):e675–e685.
- Brownson RC, Boehmer TK, Luke DA. Declining rates of physical activity in the United States: what are the contributors? Annu Rev Public Health. 2005;26(1):421–443.
- Roemmich JN. Height-adjustable desks: energy expenditure, liking, and preference of sitting and standing. J Phys Act Health. 2016;13(10):1094–1099.
- Vernillo G, Savoldelli A, Pellegrini B, et al. Validity of the sensewear armband to assess energy expenditure in graded walking. J Phys Act Health. 2015;12(2):178–183.
- Parry S, Straker L. The contribution of office work to sedentary behaviour associated risk. BMC Public Health. 2013;13:296.
- Jans MP, Proper KI, Hildebrandt VH. Sedentary behavior in Dutch workers: differences between occupations and business sectors. Am J Prev Med. 2007;33(6):450–454.
- Justine M, Azizan A, Hassan V, et al. Barriers to participation in physical activity and exercise among middle-aged and elderly individuals. Singapore Med J. 2013;54(10):581–586.
- Mailey EL, Huberty J, Dinkel D, et al. Physical activity barriers and facilitators among working mothers and fathers. BMC Public Health. 2014;14(1):657.
- Chu AHY, Ng SHX, Tan CS, et al. A systematic review and meta-analysis of workplace intervention strategies to reduce sedentary time in white-collar workers. Obes Rev. 2016;17(5):467–481.
- Neuhaus M, Eakin EG, Straker L. Reducing occupational sedentary time: a systematic review and meta-analysis of evidence on activity-permissive workstations. Obes Rev. 2014;15(10):822–838.
- Martin A, Fitzsimons C, Jepson R. Interventions with potential to reduce sedentary time in adults: systematic review and meta-analysis. Br J Sports Med. 2015;49(16):1056–1063.
- Prince SA, Saunders TJ, Gresty K. A comparison of the effectiveness of physical activity and sedentary behaviour interventions in reducing sedentary time in adults: a systematic review and meta-analysis of controlled trials. Obes Rev. 2014;15(11):905–919.
- Reed JL, Prince SA, Elliott CG, et al. Impact of workplace physical activity interventions on physical activity and cardiometabolic health among working-age women. Circ Cardiovasc Qual Outcomes. 2017;10(2):e003516. doi: 10.1161/CIRCOUTCOMES.116.003516
- Shrestha N, Kukkonen-Harjula KT, Verbeek JH, et al. Workplace interventions for reducing sitting at work. Cochrane Database Syst Rev. 2016;3:CD010912.
- Cao C, Liu Y, Zhu W, et al. Effect of active workstation on energy expenditure and job performance: a systematic review and meta-analysis. J Phys Act Health. 2016;13(5):562–571.
- Methley AM, Campbell S, Chew-Graham C. PICO, PICOS and SPIDER: a comparison study of specificity and sensitivity in three search tools for qualitative systematic reviews. BMC Health Serv Res. 2014;14(1):579.
- Hariohm K, Prakash V, Saravankumar J. Quantity and quality of randomized controlled trials published by Indian physiotherapists. Perspect Clin Res. 2015;6(2):91–97.
- Maher CG, Sherrington C, Herbert RD. Reliability of the PEDro scale for rating quality of randomized controlled trials. Phys Ther. 2003;83(8):713–721.
- Furlan AD, Pennick V, Bombardier C, et al. Updated method guidelines for systematic reviews in the Cochrane Back Review Group. Spine (Phila. Pa. 1976). 2009;34(18):1929–1941.
- Carr LJ, Karvinen K, Peavler M. Multicomponent intervention to reduce daily sedentary time: a randomised controlled trial. BMJ Open. 2013;3(10):e003261. doi: 10.1136/bmjopen-2013-003261
- Torbeyns T, de Geus B, Bailey S, et al. Bike desks in the office: physical health, cognitive function, work engagement, and work performance. J Occup Environ Med. 2016;58(12):1257–1263.
- Zeigler ZS, Swan PD, Bhammar DM, et al. Walking workstation use reduces ambulatory blood pressure in adults with prehypertension. J Phys Act Health. 2015;12(1):S119–S127.
- Zeigler ZS, Mullane SL, Crespo NC, et al. Effects of standing and light-intensity activity on ambulatory blood pressure. Med Sci Sports Exerc. 2016;48(2):175–181.
- Elmer SJ, Martin JC. A cycling workstation to facilitate physical activity in office settings. Appl Ergon. 2014;45(4):1240–1246.
- Ehmann PJ, Brush CJ, Olson RL, et al. Active workstations do not impair executive function in young and middle-age adults. Med Sci Sports Exerc. 2017;49(5):965–974.
- Dunstan DW, Kingwell BA, Larsen R, et al. Breaking up prolonged sitting reduces postprandial glucose and insulin responses. Diabetes Care. 2012;35(5):976–983.
- Cox RH, Guth J, Siekemeyer L, et al. Metabolic cost and speech quality while using an active workstation. J Phys Act Health. 2011;8(3):332–339.
- Chia M, Chen B, Suppiah H. Office sitting made less sedentary – a future-forward approach to reducing physical inactivity at work. Monten J Sports Sci Med. 2015;4(2):5–10.
- Carr L, Maeda H, Luther B, et al. Acceptability and effects of a seated active workstation during sedentary work: a proof of concept study. Int J Work Health Manag. 2014;7(1):2–15.
- Botter J, Ellegast RP, Burford E-M, et al. Comparison of the postural and physiological effects of two dynamic workstations to conventional sitting and standing workstations. Ergonomics. 2016;59(3):449–463.
- Bergouignan A, Legget KT, De Jong N, et al. Effect of frequent interruptions of prolonged sitting on self-perceived levels of energy, mood, food cravings and cognitive function. Int J Behav Nutr Phys Act. 2016;13(1):113.
- Ben-Ner A, Hamann DJ, Koepp G, et al. Treadmill workstations: the effects of walking while working on physical activity and work performance. PLoS One. 2014;9(2):e88620. doi: 10.1371/journal.pone.0088620
- Alderman BL, Olson RL, Mattina DM. Cognitive function during low-intensity walking: a test of the treadmill workstation. J Phys Act Health. 2014;11(4):752–758.
- Tronarp R, Nyberg A, Hedlund M. Office-cycling: a promising way to raise pain thresholds and increase metabolism with minimal compromising of work performance. BioMed Res Int. 2018;2018(4):1–12.
- Thompson WG, Koepp GA, Levine JA. Increasing physician activity with treadmill desks. Work. 2014;48(1):47–51.
- Straker L, Pollock C, Burgess-Limerick R, et al. The impact of computer display height and desk design on muscle activity during information technology work by young adults. J Electromyogr Kinesiol. 2008;18(4):606–617.
- Pulsford RM, Blackwell J, Hillsdon M, et al. Intermittent walking, but not standing, improves postprandial insulin and glucose relative to sustained sitting: a randomised cross-over study in inactive middle-aged men. J Sci Med Sport. 2017;20(3):278–283.
- Levine J, Miller MJ. The energy expenditure of using a ‘walk-and-work’ desk for office workers with obesity. Br J Sports Med. 2007;41(9):558–561.
- Koren K, Pišot R, Šimunič B. Active workstation allows office workers to work efficiently while sitting and exercising moderately. Appl Ergon. 2016;54:83–89.
- Koepp GA, Moore G, Levine JA. An under-the-table leg-movement apparatus and changes in energy expenditure. Front Physiol. 2017;8:318.
- Gilson ND, Hall C, Renton A, et al. Do sitting, standing, or treadmill desks impact psychobiological indicators of work productivity? J Phys Act Health. 2017;14(10):793–796.
- Straker L, Levine J, Campbell A. The effects of walking and cycling computer workstations on keyboard and mouse performance. Hum Factors. 2009;51(6):831–844.
- Lam YY, Ravussin E. Analysis of energy metabolism in humans: a review of methodologies. Mol Metab. 2016;5(11):1057–1071.
- Wetten AA, Batterham M, Tan SY, et al. Relative validity of 3 accelerometer models for estimating energy expenditure during light activity. J Phy Act Heal. 2014;11(3):638–647.
- Strath SJ, Swartz AM, Bassett DR, et al. Evaluation of heart rate as a method for assessing moderate intensity physical activity. Med Sci Sports Exerc. 2000;32(9):S465–S470.
- Byrne NM, Hills AP, Hunter GR, et al. Metabolic equivalent: one size does not fit all. J Appl Physiol. 2005;99(3):1112–1119.
- Torbeyns T, Bailey S, Bos I, et al. Active workstations to fight sedentary behaviour. Sports Med. 2014;44(9):1261–1273.
- Koolhaas CM, Dhana K, Schoufour JD, et al. Impact of physical activity on the association of overweight and obesity with cardiovascular disease: the Rotterdam study. Eur J Prev Cardiol. 2017;24(9):934–941.
- The CH, Chan YY, Lim KH, et al. Association of physical activity with blood pressure and blood glucose among Malaysian adults: a population-based study. BMC Public Health. 2015;15(1):1205.
- Carson V, Ridgers ND, Howard BY, et al. Light-intensity physical activity and cardiometabolic biomarkers in US adolescents. PLoS One. 2013;8(8):e71417. doi: 10.1371/journal.pone.0071417
- Ruffieux J, Keller M, Lauber B. Changes in standing and walking performance under dual-task conditions across the lifespan. Sports Med. 2015;45(12):1739–1758.
- Pashler H, Johnston JC, Ruthruff E. Attention and performance. Annu Rev Psychol. 2001;52:629–651.
- Arem H, Moore SC, Patel A, et al. Leisure time physical activity and mortality: a detailed pooled analysis of the dose–response relationship. Intern Med. 2015;175(6):959–967.
- Koepp GA, Manohar CU, McCrady-Spitzer SK, et al. Treadmill desks: a 1-year prospective trial. Obesity. 2013;21(4):705–711.
- Barcelo A, Gregg EW, Gerzoff RB, et al. Prevalence of diabetes and intermediate hyperglycemia among adults from the first multinational study of noncommunicable diseases in six central American countries: the Central America Diabetes Initiative (CAMDI). Diabetes Care. 2012;35(4):738–740.
- MacEwen BT, Saunders TJ, MacDonald DJ, et al. Sit–stand desks to reduce workplace sitting time in office workers with abdominal obesity: a randomized controlled trial. J Phys Act Health. 2017;14(9):710–715.
- Ojo SO, Bailey DP, Chater AM, et al. The impact of active workstations on workplace productivity and performance: a systematic review. Int J Environ Res Public Health. 2018;15(3):417–434. doi: 10.3390/ijerph15030417