
Abstract
Purpose. This study aimed to investigate the effects of using hand grip or resisted wrist extension as the reference contraction, and two electrode positions, on field recordings of forearm extensor muscle activity. Materials and methods. Right forearm extensor muscle activity was recorded using two electrode pairs (over the most prominent part (position 2) and proximal to that (position 1)) during one working day in 13 female hotel housekeepers. Each subject performed the two maximal voluntary contractions (MVCs), and the electrical activity obtained during these (maximal voluntary electrical activity (MVE)) was used for normalization. Each set of recordings was analysed twice, once using hand grip as the MVC and once using resisted wrist extension. Results. Resisted wrist extension showed a higher group mean MVE than hand grip. Position 2 had higher correlation between MVE and force during the MVCs. The workload during cleaning was lower when using resisted wrist extension as reference than when using hand grip (24%MVE vs 46%MVE; p = 0.002 at position 2) for the 90th percentile. The workload (99th percentile) was overestimated in two subjects when using hand grip as reference. Conclusions. Problems associated with poorly activated forearm extensors can be overcome by using resisted wrist extension as reference.
1 Introduction
Surface electromyography (EMG) of the forearm muscles is one of the tools used to assess prolonged and forceful arm/hand exertions in, e.g., industrial and manual work [Citation1–3]. Such work is performed in a wide range of postures and with varying forces, and the forearm muscles can thus be involved to different degrees in different situations [Citation4]. It may therefore be necessary to record the muscle activity from several forearm muscles to obtain a complete description of the forearm exertion during work. However, this may not be feasible in field recordings of physical workloads, as the time required to apply and calibrate the equipment may make employers reluctant to give permission for workplace recordings. Furthermore, analysing the vast amount of data collected would also be time consuming [Citation5]. Having to work with multiple measuring equipment may also interfere with the participants’ mobility and comfort. A common strategy is to record the muscle activity in the extensor carpi radialis brevis and longus as a proxy for forearm muscle exertion during work [Citation2,Citation6]. Exposure–response relationships have been found between the peak load on these muscles (i.e., the 90th percentile of the amplitude distribution) and reported complaints in the elbow/hand during the past 12 months and past 7 days [Citation7].
The recorded EMG amplitudes should be normalized to a reference contraction, as they are influenced by, e.g., skin conductance and subcutaneous thickness [Citation8]. A proxy for the applied muscle force relative to the subject's strength can be obtained using the maximal voluntary contraction (MVC) as a reference and expressing the electrical activity obtained during work as a percentage of the electrical activity obtained during the MVC (the maximal voluntary electrical activity (MVE)). A commonly used reference contraction is the maximal voluntary power grip (here denoted hand grip) in a mid-pronated forearm posture [Citation2,Citation9,Citation10]. This grip can be used for both flexor and extensor muscles, but has been shown to give lower EMG amplitudes than, e.g., maximal resisted flexor and extensor efforts [Citation11,Citation12]. This means that the extensor muscles are not fully activated during the hand grip, which may result in overestimation of the recorded workload.
The most appropriate way to perform a reference contraction of the forearm muscles has been discussed in several studies [Citation11–14], although no consensus has yet been reached. For example, Ngo and Wells [Citation11] proposed that EMG amplitudes obtained during power gripping tasks should be normalized to resisted flexor and extensor MVCs, for better approximation of the magnitude of maximum activation of the forearm muscles. They also suggested that a hand grip could be performed to allow comparison with previous studies in which this has been used as a reference contraction.
Recommendations on the type and positioning of electrodes, signal processing and modelling were established for 27 different muscles by the European Concerted Action SENIAM (surface EMG for non-invasive assessment of muscles) in 1999 [Citation15], but no such recommendations were established for the forearm. During nearly 30 years of research, our group has placed the EMG electrodes on the most prominent part of the extensor muscles. However, it has been suggested that this position should be avoided, as this is where the innervation zone is likely to be [Citation16]. In addition, previous studies have also shown that the EMG amplitude varies depending on the electrode position [Citation17–19]. There is therefore a need to study different electrode positions on the forearm.
We have previously found a variation in the EMG amplitude when recording the hand grip on different days. In a laboratory mock-up of an industrial setting, the coefficient of variation (CV) of the EMG recorded during the hand grip contraction was found to be as high as 29% [Citation6]. We occasionally also see higher EMG amplitudes during work than those obtained with the hand grip. Therefore, we compared the EMG amplitude and reproducibility of two different MVCs (hand grip and resisted wrist extension) and four electrode positions, and found the highest group mean EMG amplitude and the lowest CV for resisted wrist extension with the electrodes positioned closest to the elbow [Citation12]. However, that study was conducted in a laboratory setting with recordings of MVCs. The present study was therefore carried out to investigate the effects of hand grip and resisted wrist extension on recordings of forearm extensor muscle activity at two electrode positions in whole-day field recordings during hotel cleaning.
2 Materials and methods
2.1 Study design and subjects
Thirteen right-handed female hotel housekeepers participated in the study. Their median age was 40 years (range 22–55), height was 164 cm (range 157–177; data missing for one subject) and weight was 62 kg (range 50–73; data missing for three subjects). The electrical activity of the right forearm extensor muscles was recorded by two pairs of electrodes at different locations during a normal working day for each subject. All subjects performed three efforts of each of two types of MVC (hand grip and resisted wrist extension, see section 2.3) before they started work. The researcher asked the subject to maintain each contraction for about 5 s and encouraged her to perform at her best. The subject sat on a chair and body movements were controlled during each attempt. Every other subject started with the hand grip, and the remaining subjects started with the resisted wrist extension. All subjects cleaned hotel rooms. A researcher followed each subject during her working day and noted the exact starting and stopping times of different work tasks and lunch breaks. The study was approved by the Regional Ethics Committee in Lund (No. 2015/416). All subjects gave their written informed consent.
2.2 Electromyography
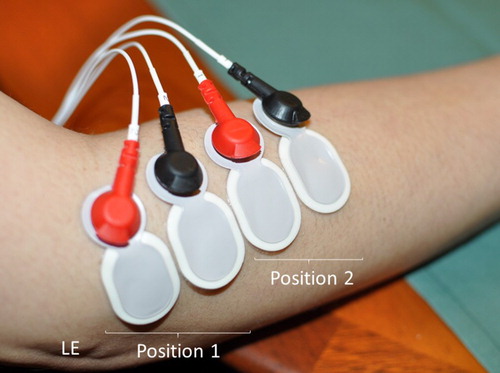
The extensor carpi radialis longus and brevis were located in the right forearm by palpation, while the subject performed a voluntary contraction with the forearm resting on a table, with a pronated forearm and an extended wrist. The skin was cleansed with alcohol and rubbed with emery cloth. We applied two Ag/AgCl electrodes (Ambu Neuroline 720, Denmark) to the skin above the most prominent part of the muscles, which was approximately one third of the distance from the lateral epicondyle to the styloid process of the ulna (position 2; Figure ) [Citation6]. Two additional electrodes were applied proximally to the original pair (position 1; Figure ). In this way, recordings could be made at two positions for each subject. Position 2 is the location used in our previous studies of workload [Citation2]. Positions 1 and 2 correspond to positions A and C, respectively, in the study by Dahlqvist et al. [Citation12]. The centre-to-centre distance between the electrodes was 20 mm, and the active diameter of the electrodes was 6 mm.
Figure 1. Positions of the electrodes (1 and 2) on the right forearm extensor muscles. Note: LE = lateral epicondyle.
The signals were amplified, filtered (10–400 Hz) and sampled at a rate of 2048 Hz, and were stored on a 2-GB memory card in a Mobi-8 data logger (TMS International, The Netherlands). After recording, the data were transferred to a computer for quality assurance and analysis. The EMG signals were digitally band-pass filtered (30–400 Hz) to remove electrical signals from the heart, and were notch filtered (mains frequency, 50 Hz, and all harmonics). The root mean square value was calculated for periods of 0.125 s, and the noise was subtracted in a power sense [Citation20]. A moving window with a width of 0.5 s was used to find the highest EMG activity resulting from the three efforts of MVCs for each kind of contraction [Citation20,Citation21].
2.3 Maximal voluntary contractions
2.3.1 Resisted wrist extension
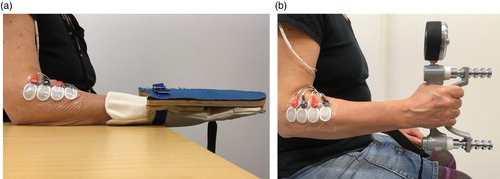
The subject sat on a chair without armrests, with the elbow flexed and with the forearm pronated and supported on a table (Figure a). The subject inserted her hand into a glove, on the dorsal side of which a piece of plywood was attached. A metal ring was attached to the underside of the plywood, through which the middle finger of the glove was passed. A strap was also passed through the ring and attached to a force transducer connected to a metal plate on the floor. The subject was asked to perform maximal extension of the wrist. Before recording the MVC, the strap was adjusted so the piece of plywood remained horizontal during the MVCs. The exerted force was registered for all three MVCs [Citation12].
Figure 2. Maximal voluntary contractions: (a) resisted wrist extension; and (b) hand grip.
2.3.2 Hand grip
The subject performed a maximal isometric grip using a Jamar hand dynamometer (Sammons Preston, USA) with the elbow flexed at 90° with no support of the forearm or hand (Figure b) [Citation12].
2.4 Data analysis
The highest electrical activity resulting from the two types of MVC (MVE) was recorded at both electrode pairs. Each recording made during cleaning was analysed twice – once using hand grip as the reference contraction and once using resisted wrist extension as the reference – resulting in four separate results for each subject (2 MVCs × 2 positions). The 90th and 99th percentiles of the amplitude distribution (muscular activity during work, expressed as %MVE) and time for recovery (% of time; EMG amplitude below 0.5% MVE) during work were calculated for each subject for the four sets of data. The group means were calculated for comparisons between the four sets of data using the Wilcoxon signed-rank test. The highest maximal exerted force (MEF; Newtons) recorded during the three efforts of each of the two MVCs was used to calculate the individual ratios and the group mean ratios between resisted wrist extension and hand grip at both electrode positions. The ratios (resisted wrist extension/hand grip) were also calculated for the MVE and %MVE (99th percentile). The correlation between the MEF and the MVE for all four sets of data was calculated in terms of the Pearson correlation coefficient. The MEF was then the independent variable and the MVE was the dependent variable. The electrode position with the highest correlation coefficient for both types of contraction was used when plotting the MVE ratio versus the %MVE (99th percentile) when using hand grip as the reference. SPSS version 24.0 was used for the statistical analyses; p < 0.05 was used to indicate a statistically significant difference.
3 Results
3.1 Resisted wrist extension/hand grip ratios for MEF and MVE
The individual ratios of the MEF ranged from 0.18 to 0.31 (Table ). The group mean ratio was 0.25. The group mean MVE for resisted wrist extension recorded at position 1 was 2.3 times higher than that for hand grip. The individual MVE ratios at position 1 ranged from 1.0 to 3.7. At position 2, the group mean MVE for resisted wrist extension was 1.8 times higher than that for hand grip, and the individual ratios ranged from 0.9 to 3.4.
Table 1. Maximal exerted force (MEF) and maximal voluntary electrical activity (MVE) of the maximal voluntary contractions (resisted wrist extension and hand grip).
3.2 MEF versus MVE
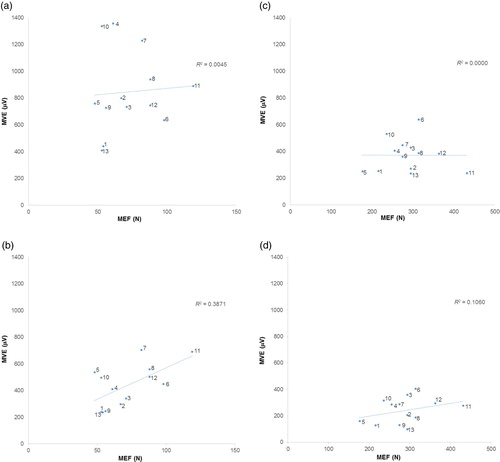
The correlation between the MEF and MVE recorded with resisted wrist extension was lower at position 1 (r = 0.07, p = 0.828; Figure a) than at position 2 (r = 0.62, p = 0.023; Figure b). The values for hand grip were r = 0.01 (p = 0.985) at position 1 (Figure c) and r = 0.33 (p = 0.278) at position 2 (Figure d).
Figure 3. Maximal voluntary electrical activity (MVE) versus maximal exerted force (MEF) for 13 female hotel housekeepers: (a) resisted wrist extension at electrode pair position 1; (b) resisted wrist extension at electrode pair position 2; (c) hand grip at electrode pair position 1; and (d) hand grip at electrode pair position 2.
3.3 Muscular load and time for recovery during work
The group mean %MVE (90th and 99th percentiles) was lower when resisted wrist extension was used as the reference contraction than when hand grip was used, at both electrode positions (Table ). At position 1, the mean of ratios for the 99th percentile was 0.48 (95% confidence interval [CI] [0.36, 0.59]), while the corresponding value at position 2 was 0.58 (95% CI [0.44, 0.71]). The %MVE recorded was above 100% in three subjects at position 1 and in two subjects at position 2 when using hand grip as the reference.
Table 2. Workload (%MVE; 90th and 99th percentiles) and time for recovery (% of time) during hotel housekeeping at two electrode positions (1 and 2) when using hand grip and resisted wrist extension as reference contractions.
The group means of the time for recovery were higher when resisted wrist extension was used as the reference than when hand grip was used, at both electrode positions (Table ). The mean values of the ratios for the time for recovery at position 1 were 2.9 (95% CI [2.1, 3.7]) and 2.3 (95% CI [1.6, 3.0]) at position 2 (data not presented).
3.4 %MVE versus MVE ratio
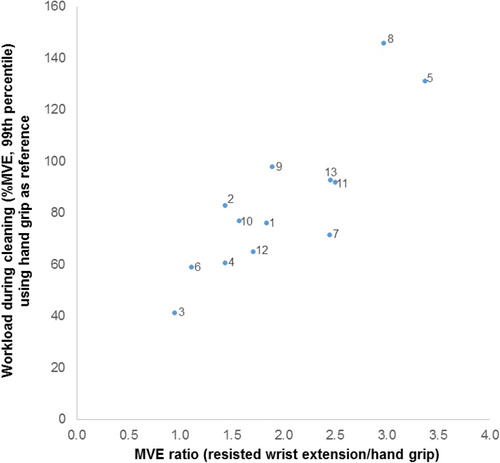
The two subjects with %MVE (99th percentile) above 100% at position 2 when hand grip was used as the reference contraction had MVE ratios of 3.0 and 3.4. All other subjects had ratios below 2.5 (Figure ).
Figure 4. Workload (% MVE; 99th percentile) during hotel room cleaning at electrode position 2 when using hand grip as the reference contraction versus the ratio of the maximal voluntary electrical activity (MVE) for resisted wrist extension and hand grip for 13 female hotel housekeepers.
4 Discussion
Resisted wrist extension showed higher group mean MVEs than hand grip at both electrode positions. The correlation between the MEF and the MVE was higher at position 2 than at position 1 for both resisted wrist extension and hand grip. At position 2, this correlation was higher for resisted wrist extension than for hand grip. When using hand grip as the reference, two subjects showed %MVE above 100% at position 2 during cleaning (99th percentile). These subjects also had an MVE ratio between resisted wrist extension and hand grip greater than 3.0.
4.1 MVE and MVE ratios for the two reference contractions
Twelve of the 13 subjects exhibited higher MVEs with resisted wrist extension than with hand grip, which is in accordance with our findings in the laboratory setting, where this was the case in 11 of 12 subjects [Citation12].
4.2 Correlations
We believe that the MVE, to some degree, reflects the MEF that is used when performing the MVC. However, several studies have shown that, e.g., the subcutaneous thickness, electrode positioning and different arm positions also influence the MVE [Citation8,Citation16,Citation22,Citation23], which of course will affect the correlation. In the current study, we found an R2 value of 0.39 between the resisted wrist extension MVE at position 2 and the MEF. Thus, 39% of the variance in the MVE could be explained by the MEF. The corresponding value for hand grip was only 11%. No correlations were found at position 1, which may be a consequence of electrode positioning. Therefore, in spite of the possible drawbacks resulting from positioning the electrodes over the innervation zone, we recommend position 2 for forearm extensor EMG recordings.
4.3 Muscular load during work and MVE ratios
When using hand grip as the reference, values of %MVE above 100% were obtained for two subjects. Upon inspecting the data, we noted that these subjects (numbers 5 and 8) had hand grip MVEs for electrode position 2 that were among the lower values, while their MVEs for resisted wrist extension were among the highest. Furthermore, the ratios of the MEF between the two types of contraction for these subjects were the same as for the other participants, while their MVE ratios were the two highest. It thus appears that they activated their extensor muscles to a lesser extent than the others during the hand grip, resulting in overestimation of the muscular load during work when using hand grip as the reference. It is not possible to determine whether a subject activates the extensor muscles maximally by studying the hand grip force and MVE only. Instead, the MVE ratio for resisted wrist extension and hand grip can be used to distinguish individuals who fully activate their extensor muscles from those who do not.
4.4 Strengths and limitations
Differences in EMG amplitudes of the forearm muscles between different maximal efforts and/or with the arm in different positions have been reported in several previous studies [Citation11,Citation14,Citation24]. However, these studies only compared the amplitudes during these specific maximal efforts in the laboratory, and it is difficult to estimate the consequences of different contractions in real working situations using such an approach. To the best of our knowledge, the present study is the first in which different reference contractions have been used and compared in field recordings of real work using different electrode positions. We recorded the muscular load in an occupation with very strenuous work tasks, and enabled us to reveal two subjects in which the workload was obviously overestimated due to poor activation of the forearm extensors in the hand grip contraction.
The main limitations of this study were the small number of participants and the fact that only women were studied. Despite this, we saw differences in amplitude between the two types of reference contraction, and the results from our previous laboratory study were confirmed [Citation12].
4.5 Practical implications
The results of this study show that the muscular load during work can be overestimated when using hand grip as the reference contraction for the normalization of EMG data. Furthermore, the correlation between the MEF and the MVE was higher for resisted wrist extension than for hand grip at position 2. This suggests that resisted wrist extension may be used to normalize EMG data. However, hand grip has been used in many previous studies, and comparisons to these studies would be lost. One approach to overcome this could be to perform both resisted wrist extension and hand grip contractions and report both. Another approach could be to report data that have been normalized to hand grip, and exclude subjects with an MVE ratio above a certain level (3 in the current study). A somewhat lower %MVE could then be expected on the group level (41%MVE instead of 46%MVE in this study) compared with previous studies, as these are likely to include subjects with an overestimated workload.
5 Conclusions
Resisted wrist extension showed higher MVEs than hand grip for both electrode positions. A higher correlation was also found between the MEF and the MVE for resisted wrist extension than for hand grip, at position 2. When using hand grip as the reference, the muscular load during work was overestimated in two subjects. Resisted wrist extension may therefore be more valid for the normalization of EMG recordings of muscular load during work. However, many studies have used the hand grip as reference. Therefore, both resisted wrist extension and hand grip could be performed and reported. To avoid overestimation when using hand grip as the reference, subjects with an MVE ratio over a certain threshold (> 3.0 in the current study) should be excluded.
Acknowledgements
The authors wish to thank the subjects, the hotels and the cleaning companies that participated in this study.
Disclosure statement
No potential conflict of interest was reported by the authors.
Correction Statement
This article has been republished with minor changes. These changes do not impact the academic content of the article.
Additional information
Funding
Related Research Data
References
- Chen HC, Chang CM, Liu YP, et al. Ergonomic risk factors for the wrists of hairdressers. Appl Ergon. 2010;41(1):98–105. doi: 10.1016/j.apergo.2009.05.001
- Hansson G-Å, Balogh I, Ohlsson K, et al. Physical workload in various types of work: part I. Wrist and forearm. Int J Ind Ergon. 2009;39(1):221–233. doi: 10.1016/j.ergon.2008.04.003
- Barrero LH, Pulido JA, Berrio S, et al. Physical workloads of the upper-extremity among workers of the Colombian flower industry. Am J Ind Med. 2012;55(10):926–939. doi: 10.1002/ajim.22102
- Roman-Liu D, Bartuzi P. The influence of wrist posture on the time and frequency EMG signal measures of forearm muscles. Gait Posture. 2013;37(3):340–344. doi: 10.1016/j.gaitpost.2012.07.027
- David GC. Ergonomic methods for assessing exposure to risk factors for work-related musculoskeletal disorders. Occup Med (Lond). 2005;55(3):190–199. doi: 10.1093/occmed/kqi082
- Nordander C, Balogh I, Mathiassen SE, et al. Precision of measurements of physical workload during standardised manual handling. Part I: surface electromyography of m. trapezius, m. infraspinatus and the forearm extensors. J Electromyogr Kinesiol. 2004;14(4):443–454. doi: 10.1016/j.jelekin.2003.12.003
- Nordander C, Ohlsson K, Åkesson I, et al. Exposure–response relationships in work-related musculoskeletal disorders in elbows and hands – a synthesis of group-level data on exposure and response obtained using uniform methods of data collection. Appl Ergon. 2013;44(2):241–253. doi: 10.1016/j.apergo.2012.07.009
- Nordander C, Willner J, Hansson GA, et al. Influence of the subcutaneous fat layer, as measured by ultrasound, skinfold calipers and BMI, on the EMG amplitude. Eur J Appl Physiol. 2003;89(6):514–519. doi: 10.1007/s00421-003-0819-1
- Blangsted AK, Hansen K, Jensen C. Muscle activity during computer-based office work in relation to self-reported job demands and gender. Eur J Appl Physiol. 2003;89(3):352–358. doi: 10.1007/s00421-003-0805-7
- Bao S, Silverstein B. Estimation of hand force in ergonomic job evaluations. Ergonomics. 2005;48(3):288–301. doi: 10.1080/0014013042000327724
- Ngo BPT, Wells RP. Evaluating protocols for normalizing forearm electromyograms during power grip. J Electromyogr Kinesiol. 2016;26:66–72. doi: 10.1016/j.jelekin.2015.10.014
- Dahlqvist C, Nordander C, Granqvist L, et al. Comparing two methods to record maximal voluntary contractions and different electrode positions in recordings of forearm extensor muscle activity: refining risk assessments for work-related wrist disorders. Work. 2018;59:231–242. doi: 10.3233/wor-172668
- Burden A. How should we normalize electromyograms obtained from healthy participants? What we have learned from over 25 years of research. J Electromyogr Kinesiol. 2010;20(6):1023–1035. doi: 10.1016/j.jelekin.2010.07.004
- Barr AE, Goldsheyder D, Ozkaya N, et al. Testing apparatus and experimental procedure for position specific normalization of electromyographic measurements of distal upper extremity musculature. Clin Biomech (Bristol, Avon). 2001;16(7):576–585. doi:S0268-0033(01)00046-8 doi: 10.1016/S0268-0033(01)00046-8
- Hermens HJ, Freriks B, Merletti R, et al. European Recommendations for Surface ElectroMyoGraphy, results of the SENIAM project. Enschede: Roessingh Research and Development; 1999. p. 1–122.
- Mesin L, Merletti R, Rainoldi A. Surface EMG: the issue of electrode location. J Electromyogr Kinesiol. 2009;19(5):719–726. doi: 10.1016/j.jelekin.2008.07.006
- Takala EP, Toivonen R. Placement of forearm surface EMG electrodes in the assessment of hand loading in manual tasks. Ergonomics. 2013;56(7):1159–1166. doi: 10.1080/00140139.2013.799235
- Ghapanchizadeh H, Ahmad SA, Ishak AJ, editors. Recommended surface EMG electrode position for wrist extension and flexion. In: Proceedings of 2015 IEEE Student Symposium in Biomedical Engineering & Sciences (ISSBES). Kuala Lumpur, Malaysia: IEEE; 2015. p. 108–112. doi: 10.1109/ISSBES.2015.7435877
- Huebner A, Faenger B, Schenk P, et al. Alteration of surface EMG amplitude levels of five major trunk muscles by defined electrode location displacement. J Electromyogr Kinesiol. 2015;25(2):214–223. doi: 10.1016/j.jelekin.2014.11.008
- Hansson G-Å, Asterland P, Skerfving S. Acquisition and analysis of whole-day electromygraphic field recordings. In: Hermens HJ, Hägg G, Freriks B, editors. Proceedings of the second general SENIAM (Surface EMG for non-invasive assessment of muscles) workshop. Stockholm: Roessingh Research and Development; 1997. p. 19–27.
- Jensen C, Vasseljen Jr O, Westgaard RH. Estimating maximal EMG amplitude for the trapezius muscle: on the optimization of experimental procedure and electrode placement for improved reliability and increased signal amplitude. J Electromyogr Kinesiol. 1996;6(1):51–58. doi: 10.1016/1050-6411(94)00012-3
- Mogk JPM, Keir PJ. Crosstalk in surface electromyography of the proximal forearm during gripping tasks. J Electromyogr Kinesiol. 2003;13(1):63–71. doi: 10.1016/S1050-6411(02)00071-8
- Farina D, Cescon C, Merletti R. Influence of anatomical, physical, and detection-system parameters on surface EMG. Biol Cybern. 2002;86(6):445–456. doi: 10.1007/s00422-002-0309-2
- Greig M, Wells R. A systematic exploration of distal arm muscle activity and perceived exertion while applying external forces and moments. Ergonomics. 2008;51(8):1238–1257. doi: 10.1080/00140130802037289