
Abstract
Objective. The aim of this qualitative study was to explore how ergonomists experienced an e-learning concept as a tool for knowledge translation; furthermore, to explore what, if any, impact the knowledge translation had regarding the ergonomists’ work with risk assessments. Methods. Twelve Swedish ergonomists employed in the occupational health service (OHS) participated in a research project, which included an e-learning program in risk assessment training. Focus group interviews and individual interviews were used for data collection. Results. The ergonomists appreciated the e-learning concept, e.g., its flexibility enabled them to decide when and where to practice. The concept was considered feasible within the context of the OHS. The ergonomists experienced an increased knowledge of different observation-based risk assessment tools, which expanded their professional toolboxes. Additionally, they began to reflect more regarding the reliability of risk assessment tools and how to enhance quality in risk assessment assignments. Conclusion. This study showed that e-learning may comprise an efficient knowledge translation for improved risk assessments in the OHS. The program contributed to changes in ergonomists’ risk assessment procedures, e.g., in the selection of tools, increasing the number of observers, employing a participatory approach and more often actively involving stakeholders during the risk assessment process.
1 Introduction
The prevalence of work-related musculoskeletal disorders (MSDs) continues to be high in Europe [Citation1], and many workplace parties are not aware of the relation between work and MSDs [Citation2]. Risk assessment is fundamental for targeting risk-reducing interventions to prevent MSDs [Citation3]. Therefore, it is essential that ergonomics practitioners are comfortable in assessing exposure and risks related to MSDs, in order to support workplaces with risk assessment. Several types of methods can be used for assessment of MSD risks [Citation4–6]. The use of risk assessment methods is reported to help anchor ergonomics into organizational processes [Citation7], which ought to facilitate risk-reducing interventions.
Observation-based risk assessment tools (OBRATs) are often considered useful for occupational health service (OHS) ergonomics practitioners, since they are time-efficient, flexible and considered less costly compared to direct measurements [Citation4,Citation8]. A study among Swedish OHS-employed ergonomists on the use of OBRATs showed a general low level of use, and that education or training in OBRATs was a facilitating factor for use of OBRATs [Citation9], a finding also reported by Arezes et al. [Citation10]. Diego-Mas et al. [Citation11] classify lack of information/training as one of the most common problems in the implementation of OBRATs. Furthermore, they emphasized that information regarding a particular OBRAT can be difficult to access and that training and the ease with which information can be accessed can influence the extent to which practitioners perceive a method to be applicable and useful [Citation11].
1.1 Study context
Globally, ergonomics practitioners come from many different professional backgrounds, e.g., in North America, they are common with a background in engineering, psychology and other health science disciplines. In Sweden, ergonomists employed in OHS most often have a background as registered physical therapists with further education in physical ergonomics. They can either be employed by an ‘in-house OHS’, which is incorporated into the ‘client’ company/industry, municipality or county council, or be employed by an ‘external OHS provider’, which is the most common type of employment. External OHS providers refer to a multi-professional OHS organization, in which the practitioners are consultants to several client companies within different sectors. OHS ergonomists require competence and skills for making risk assessments, in order to fulfill the requirements of providing expertise to employers within different sectors. However, risk assessment assignments are a minor part of the Swedish OHS ergonomist’s work [Citation9]. More commonly, the work often includes activities such as treating patients, supporting rehabilitation, health examinations and educational assignments [Citation12]. Therefore, opportunities may be limited for OHS ergonomists to participate in comprehensive courses regarding risk assessment. Additionally, there is a lack of more informal, easy-to-access educational material with a focus on training in specific risk assessment tools. This might lead to difficulties in maintaining competence regarding risk assessment. Brämberg et al. [Citation13] reported that there is a need and willingness among OHS practitioners to use evidence-based methods and tools in their practice. However, the use is often seen to be the responsibility of the individual practitioner and not of the organization (OHS provider) [Citation13]. Change does not occur by itself, and passive approaches, such as leaving the responsibility to the individual practitioner, have been shown to be ineffective [Citation14]. Graham et al. [Citation15] describe that knowledge translation builds upon continuing education and continuing professional development. Continuing education strategies are known to be effective in transferring knowledge to practitioners [Citation15]. As for knowledge translation regarding risk assessments and its influences on ergonomists, there is a lack of research. By learning from experiences of how knowledge translated from a research project influences practitioners, and possibly also influences practices, information can be gathered regarding practical issues to consider in further development of, e.g., tools such as OBRATs or practice guidelines to aid the translation of research into practice settings [Citation15,Citation16]. In a research project aimed to test the reliability of six OBRATs for risk assessment of repetitive and hand-intensive work [Citation17], OHS ergonomists were trained in different OBRATs through an e-learning program. By participation in the research project, knowledge should be transferred to each of the ergonomists, which might have practical impact in the OHS contexts in which the ergonomists operate.
The aim of this study was to explore how the ergonomists who participated in a research project, which included an e-learning program in risk assessment training, experienced the e-learning concept as a tool for knowledge translation in the OHS ergonomists’ context. Furthermore, the study aimed to explore what, if any, impact the knowledge translation had regarding the ergonomists’ work with risk assessments.
2 Method
2.1 Study design
This study was a sub-study within a larger research project of reliability tests of six OBRATs (Appendix 1) for risk assessment of repetitive and hand-intensive work [Citation17]. This sub-study was designed as a qualitative exploratory study. The regional ethical vetting board in Stockholm has given ethical approval (2013/308–31/3) for the research project.
2.2 Sampling and participants
The recruitment of ergonomists was based on a purposeful sampling strategy of key informants [Citation18]. The ergonomists were recruited from two different regions in Sweden and formed three groups: one group in the south (n = 5) and two groups in the Stockholm region (n = 4, n = 3). The criteria for inclusion were that the ergonomist was employed by an OHS company (or the equivalent) and had at least 1 year of work experience with risk assessments. They were recruited through contact with OHS providers or through social media posts targeting members of the Swedish Ergonomics and Human Factors Society. In total, 12 female ergonomists, all registered physical therapists, were recruited to participate. All ergonomists were women, and the work experience in ergonomics ranged from 4 to 26 years at baseline. The ergonomists’ characteristics are presented in .
Table 1. Characteristics of the participating ergonomists: year of birth (YOB), years of work experience within the field of ergonomics at baseline, employment in type of occupational health service company (OHS) and frequency of performing risk assessments at both baseline and follow-up.
2.3 Study setting
The overarching research project aimed to test the reliability of six OBRATs for risk assessment of repetitive and hand-intensive work [Citation17]. This project included that the ergonomists would train and practice on the different OBRATs using a theoretical and practical e-learning program.
2.3.1 The e-learning program in risk assessment and use of observational-based risk assessment tools
The ergonomists were invited to an introductory meeting in each region, where they were introduced to the project and the e-learning program. The e-learning program was designed as a 6-week self-paced course and encompassed: (a) a pre-recorded lecture about the risk assessment process; (b) pre-recorded instructional videos for the six selected OBRATs presented in Appendix 1; (c) self-supported training using a video library of different work tasks.
The lecture about risk assessment included a thorough review of the risk assessment process, including the planning and risk assessment phases. The planning phase was presented as a phase that could include visits to the workplace and meetings with stakeholders to plan the assessment. The risk assessment phase described how the use of risk assessment tools, such as OBRATs, can be applied in order to describe and quantify exposures, and how to ultimately conclude whether the risk level is acceptable or not.
In the pre-recorded instructional videos for the six selected OBRATs, the tools were described; the use of each tool was exemplified with a ‘walk-through’ risk assessment, in which the OBRAT was applied to various work tasks. The self-supported training used a video library with film clips (2–6 min) of different work tasks. Several of the work task film clips displayed three synchronized camera angles, including close-ups on hand and wrist movements, although some films displayed a single camera angle. Each film was accompanied by written information about the work task, e.g., daily exposure time with the task, breaks, weights of handled goods, ratings of force exertion, discomfort and work demands. The manuals and the protocols for all six tools were available for download from the e-learning platform.
During a first, self-paced e-learning period of 3 weeks, the ergonomists trained using three of the OBRATs. Thereafter, they returned for an on-site training session, where they conducted risk assessments of 10 new video-recorded work tasks, using each of these three OBRATs. The complete procedure was repeated for the remaining three tools (). Thereafter, the e-learning training was accomplished. However, the ergonomists had continuing access to the e-learning platform and could watch the instructional videos whenever they wanted.
Figure 1. The data collection process.

2.4 Data collection
provides an overview of the data collection process and the methods used for data collection.
The baseline questionnaire included questions about the ergonomists’ background as presented in . After completion of the theoretical and practical e-learning program for all six OBRATs, three focus group face-to-face interviews were conducted, with three to five ergonomists in each group. The interviews were semi-structured and followed an interview guide. The content of the interview questions comprised usability aspects of the included OBRATs and questions about the concept of the e-learning program. The interviews were 60–90 min long and were conducted by the third author (T.N.), accompanied by one observer who asked supplementary questions. All interviews were digitally recorded and transcribed verbatim.
After 4 years, all 12 ergonomists were contacted regarding participation in the follow-up study that included a short questionnaire and an individual telephone interview (). Eight ergonomists participated, while four ergonomists dropped out because they no longer worked with risk assessments. In the follow-up questionnaire, the questions from the baseline questionnaire on conducting risk assessments were repeated (). The following telephone interview followed a semi-structured interview guide with questions about if, and how, the research project had added knowledge that was practically applicable for the ergonomists, regarding choices of risk assessment tools and the risk assessment process. In the interviews, the ergonomists were asked about their typical risk assessment process and the rationale behind their choice of tools. The interview guide was piloted on two ergonomists (non-participants). The first author (K.E.) conducted the interviews by telephone, and they lasted 40–60 min. All interviews were digitally recorded and transcribed verbatim.
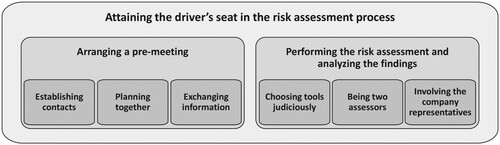
Figure 2. The ergonomists described a development in their role in a risk assessment process by ‘Attaining the driver’s seat in the risk assessment process’, which was described by the sub-categories ‘Arranging a pre-meeting’ and ‘Performing the risk assessment and analyzing the findings’.
2.5 Data analysis
Data derived from the interviews as well as from open-ended questions in the follow-up questionnaire were analyzed by qualitative content analysis [Citation19]. NVivo version 12 was used to manage the qualitative data. All transcribed interviews were read through. The inductive analysis was kept on a manifest level [Citation20]. For each interview, meaning units related to the research questions were marked and labeled with codes. Codes from respective interviews were then compared with the other interviews and consolidated into sub-categories; related sub-categories constituted categories. The analysis was mainly conducted by the first author. To ensure credibility, the codes, sub-categories and categories were discussed with the third author during the analysis phase.
3 Results
The results are presented in two sections relating to the dual aims. The first sections present the ergonomists’ experience of the e-learning program. The second section presents the ergonomists’ experience regarding the knowledge translation from participation in the research project and its influence on their practice concerning risk assessment assignments. Verbatim quotations from the ergonomists, translated from Swedish, are used to illustrate their experiences.
3.1 The ergonomists’ experience of the e-learning concept
The ergonomists experienced that it was feasible to use the e-learning concept as an educational tool for continuous professional development in OHS organizations. They were favorably inclined toward the design of the education due to factors related to the distance learning concept, e.g., the ability to determine on your own when to practice, the possibility of watching the film multiple times and being able to pause when needed. Concerning the instructional videos for risk assessment, the participants appreciated the ‘walk-through’ examples and the opportunity to follow ‘the expert’ performing the risk assessment on the video. However, they requested a greater variety of sample films. Regarding the format of the films of different work tasks, the interviewees preferred the films with three synchronized camera angles, which they thought gave a more comprehensive impression of the work tasks than the films from a single camera. A drawback in the e-learning program was the lack of interaction possibilities (synchronized as well as unsynchronized) with the teacher and the other participants during the e-learning period:
I appreciated being able to decide for myself when to practice [on the OBRATs]. Sometimes, I fast-forwarded/rewound back and forth [in the videos], and sometimes I played forward a bit and later went back to something. In that way, I went on back and forth. I began to watch the whole, and thereafter went back to something that I had to consider more. I thought it was good. However, many questions arose. (Ergonomist group 3)
3.2 The ergonomists’ experience of the knowledge translation
The ergonomists described that participation in the research project, in which the participants were trained in six OBRATs and made 10–20 risk assessments with each tool, had resulted in self-reflection regarding how they approached risk assessment assignments and their role and performance in the process. The research project had increased the ergonomists’ knowledge of, and interest in, risk assessment tools in general, not only those in which they were trained. All ergonomists described that they had developed an increased self-confidence and self-esteem regarding risk assessment not only with their clients but also within their own OHS company. For example, the interviews revealed that several of the ergonomists now served as a coach or mentor to other OHS ergonomist colleagues.
The analysis formed the category ‘Attaining the driver’s seat in the risk assessment process’, followed by the two sub-categories ‘Arranging a pre-meeting’ and ‘Performing the risk assessment and analyzing the findings’, as illustrated in .
3.2.1 Arranging a pre-meeting
The ergonomists described that arranging a pre-meeting with relevant representatives in the client company was an important step in the planning phase when a new risk assessment assignment was initiated. The pre-meeting targeted several objectives: establishing contacts, providing support for the planning of the risk assessment and exchanging information.
The ergonomists emphasized the importance of the pre-meeting, serving the purpose of establishing contact with different stakeholders (e.g., management, occupational health and safety representatives, human resources). The ergonomists described that for a new assignment, where the client company was unknown to the ergonomist, the meeting allowed for the opportunity to be introduced and to understand the client company and its production and work environment challenges. The meeting served as an arena for discussions with different representatives concerning where and how to focus the risk assessment, and was especially important to structure and plan the whole risk assignment process. One ergonomist described a pre-meeting:
They describe their operation and show me around, and talk and show things in general. Based on that I can get back to them later regarding a proposal for how much time is needed and an outline of the risk assessment assignment. (Ergonomist 4)
Some ergonomists explained that they asked the stakeholders to provide them with information prior to the assessment about factors that did not require active observation, such as information regarding work scheduling, exposure time and weight of handled goods. This strategy was something that contributed to make the stakeholders engage in the risk assessment, but also contributed to efficiency with the upcoming assessment since information about such factors was readily available in advance. The ergonomists further described that the exchange of information provided an opportunity to inform and educate the client in ergonomics and risk assessment, which served the purpose of raising awareness concerning the work environment responsibilities of the employer:
I see that this preparatory work meets several purposes. I get good information to start with, and the employer is prepared because he/she has understood the meaning of these factors such as how often, for how long, how heavy, and that sort of things … (Ergonomist 7)
Furthermore, the pre-meeting also facilitated the ergonomist to explore the client’s expectations and possibilities for ergonomic improvement actions after the completed risk assessment. After the dialogue, the ergonomist described that they had gathered enough relevant information to make a thorough calculation regarding how much time was needed for the assignment. It was described that after participation in the research project, the ergonomists had a deeper insight into the requirement of time for risk assessments, and increased confidence to allocate enough time for assignments. Some described that they nowadays, already in the planning phase, also allocated time for follow-ups:
I usually try to explain that if they [the clients] are not prepared to take any actions, then they should think about things a while longer and ask themselves if it is right to carry on with this risk assessment – or will it only raise expectations among workers … (Ergonomist 2)
3.2.2 Performing the risk assessment and analyzing the findings
Participation in the research project had increased the ergonomists’ awareness of strengths as well as weaknesses in OBRATs, and all ergonomists described changes in how they currently performed the risk assessment and the following analysis. Three aspects were identified: choosing tools judiciously, being two observers and involving the working group. These changes were all related to increasing the reliability of risk assessments.
3.2.2.1 Choosing tools judiciously
The ergonomists described how they had increased their awareness of new and other risk assessment tools, which resulted in them expanding their ‘toolboxes’ with a greater variety of tools. They also described that the use of research-based tools gave a serious and professional impression toward the stakeholders. Furthermore, they felt that the use of OBRATs promoted communication with both the workers and the stakeholders, aiding the ergonomist in the dialog, facilitating risk communication as well as helping to identify where to focus further work environment actions. One ergonomist expressed that:
It is of importance, for the clients’ internal work with improvements that the tool illustrates that here is something [work task/station] that is red. (Ergonomist 7)
During the research project, the ergonomists expressed that they increased their awareness of deficiencies in reliability in the OBRATs. This resulted in more well-judged choices regarding tools for specific exposures, but also led to the ergonomists combining different tools in one risk assessment. One ergonomist described this increased awareness:
… you got a whole new understanding of risks and risk assessments and all the tools and such. And, I’m sure that on the basis of that, I’ve clearly seen what I need, ‘this,’ ‘this,’ and ‘that’ in order to assess these kinds of risks and those kinds of risks … (Ergonomist 2)
From the ergonomists’ practical perspective, they wanted to use OBRATs that they knew were reliable, easy to use and versatile in their design, providing the possibility to choose between using a ‘pen and paper’ or being able to use the tool digitally (using a computer or tablet). Furthermore, several expressed that they sought the workers’ participation in the risk assessment and, consequently, found it supportive if the tool involved the workers in the assessment. Other aspects highlighted as being useful were tools that included assessment of multiple exposures (including visual aspects) and workload in multiple body parts, e.g., workload in the neck and back as well as in the shoulder, arm and hand. Other positive factors were consideration of breaks and periods of recovery. Some ergonomists stressed that when OBRATs were used in individual rehabilitation cases, to identify whether adjustments in a workplace are needed, they have a need for OBRATs to incorporate the individual workers’ work technique in the assessment, which was a factor they found to be lacking in OBRATs.
3.2.2.2 Being two observers
Some ergonomists descri-bed that they nowadays tried to arrange for two observers when they were assigned to a risk assessment project. The observers could be two ergonomists or one ergonomist and one occupational safety engineer. They could work together either throughout the assessment project or at least in the assessment and analysis phase. In instances when this strategy had been implemented, it had not encountered any resistance from the clients. However, it was still more common to carry out assignments alone.
3.2.2.3 Involving company representatives
Anotherchange that was highlighted by some ergonomists was to actively involve representatives (workers, managers) from the client company. In cooperation with, and guided by, the ergonomist, they undertook the analysis of risk factors and completed the risk assessment together. This participation-based analysis became a way to give the client ownership of the analysis and the following actions. One ergonomist described:
The point of doing the analysis together, both employees and employers, is that you instill an engagement, since this is a joint commitment. (Ergonomist 12)
4 Discussion
Knowledge translation is important for development and changes in practice [Citation15,Citation16]. However, knowledge of practitioners’ experiences is important to enhance knowledge regarding practitioners’ needs related to the context in which they operate. This qualitative study explored ergonomics practitioners’ experiences after participation in a research project. By participation in the research project, knowledge is transferred to each of the ergonomists. Two separate inquiries were explored in this study: (a) experiences of an e-learning concept as a tool for knowledge translation; (b) whether participation in the research project influenced the ergonomists’ work regarding risk assessments.
Overall, the ergonomists were satisfied with the e-learning concept, and e-learning seems to be suitable for knowledge translation within the Swedish OHS context. The present study did not compare the e-learning program to traditional on-site (campus) education. In a review by Vaona et al. [Citation21], e-learning was compared to traditional learning. They found that e-learning results in little or no difference in patient outcomes or health professionals’ behaviors; however, in terms of differences in health professionals’ skills, the effect is unclear. e-Learning as a pedagogical model is accessible, affordable for professionals and consulting companies (minimizing time away from work), and relatively easy to administrate. The Swedish OHS sector is commercialized, and the employed ergonomics practitioners have sales targets, which may hamper participation in comprehensive courses, since such courses often mean that the ergonomist needs to take time away from work. The ergonomists are often interested in increasing their professional knowledge. This study indicates that in the context of OHS practitioners, such as the ergonomists in the present study, this concept of continuing education can fulfill a need to disseminate knowledge concerning, e.g., new guidelines and work tools, such as risk assessment tools. However, based on the experience of the participants in the present study, emphasis needs to be placed on increasing the interaction between participants (peer learning) and feedback from teachers, in the design of such web-based models for risk assessment training. This is something that needs to be balanced against practical issues and needs to be explored further.
The ergonomists experienced that participation in the research project generated knowledge and resulted in changes in their risk assessment process. An expected finding was that they had increased their knowledge in risk assessment tools, they had become more alert and updated about different risk assessment tools in general. A somewhat unexpected but interesting result was the finding that the ergonomists experienced that their increased knowledge had influenced their risk assessment process, and how they now undertook risk assessment assignments. Most of them had started employing a more participatory approach, which was illustrated in their description of activities, their roles and an increased consciousness regarding quality assurance in the risk assessment process. They actively involved workers and stakeholders in all phases of the process and afforded the ownership of the risk assessment process to the client company. These are factors that are characteristic of participatory ergonomics [Citation22,Citation23]. The overall research project regarding inter-observer and intra-observer reliability in the included OBRATs had showed lower reliability than expected [Citation17,Citation24]. The ergonomists’ awareness of these deficiencies might have contributed to reflection, concerning weaknesses in the traditional risk assessment process. In some cases, this insight had strengthened the participants to arrange for two observers to take part in the whole risk assessment process or parts thereof. Another approach to enhance the quality of the risk assessments was the participatory analysis, in which a team, consisting of workers, the manager and the ergonomist, assessed the risks together. Those approaches may increase the reliability and strengthen the quality aspects of risk assessment, leading to a more comprehensive analysis because the work tasks are observed by ‘another set of eyes’. Engagement of several observers is also a cost-efficient approach [Citation25,Citation26].
In the present study, the ergonomists described that they often took an active role as a leader throughout the whole process; specifically, they initiated pre-meetings at the start of the process and planned the assignment together with the client, and actively led the client through the process and included the client in the process. This matches the description of the ergonomists’ role in participatory programs [Citation27–29]. Further, the ergonomists described their role as being similar to the results from a study by Berlin et al. [Citation30], which identified that ergonomists’ behavioral strategies, e.g., employing a guiding-expert function and a translator or go-between role, enhanced their influence concerning workplace changes. Whysall et al. [Citation31] stated that ergonomics consultancy can be improved by a problem-solving, collaborative approach. In this present study, and also supported by Berlin et al. [Citation30], we see a trend among the participants toward this approach and development of the ergonomist role. This development can be seen as a step toward a more holistic risk assessment process, which, according to Macdonald and Oakman [Citation32], is better suited for assessing risk exposure related to MSDs due to its complexity.
In previous studies exploring how ergonomists approach the risk assessment process, the professional background of the participating ergonomists is not reported [Citation7,Citation31]. In those studies, the ergonomists are solely described as being ‘certified ergonomists’. In Sweden, ergonomist professionals most often have a university degree in medical sciences, but they can also have a background within engineering or behavioral sciences. There is no national certification organization of ergonomists, but ergonomics practitioners, regardless of their professional background, may apply to the Centre for Registration of European Ergonomists (CREE) to gain a European Ergonomist certificate [Citation33]. Depending on their professional background, ergonomists may have different experiences and needs in the ergonomics field, and they might be working in different contexts. The contextual framework in the present study is Swedish OHS organizations, and almost all OHS ergonomists in Sweden have a background in medical sciences – as physical therapists – so the findings in the study need to be interpreted within this context. The knowledge generated from the participants’ experiences regarding how their risk assessment process developed contributes, among other things, to valuable aspects for consideration in the development of ergonomists’ education in risk assessment, e.g., it is essential in education and guidelines to emphasize the surrounding risk assessment process and not only focus on the tools. Furthermore, knowledge has also been translated to us researchers regarding the e-learnings concept, which can be valuable to the development of forthcoming e-learning programs in an OHS context.
4.1 Methodological considerations
In this qualitative study, we had the opportunity to follow eight ergonomists, all located at different OHS companies (both in-house and external ergonomics practitioners), and to explore their experiences of the e-learning concept as well as how knowledge translation influenced their practice. Irrespective of the different contexts in which they operated, they all described similar development regarding changes in their risk assessment process, which strengthens the results. In a qualitative study one wants to sample information-rich cases, participants who can yield insight and in-depth understanding, rather than generalizations [Citation18]. In the present study, a purposeful sampling strategy of key informants was used, which means that the participants have great knowledge of and interest in the inquiry issues [Citation18]. The study participants all had a special interest in risk assessment. Therefore, it is very interesting and valuable to take part in their insights and development. The insights into and progress in the risk assessment process shown among this sample might not have been revealed if another sampling strategy was used. The aim is not to generalize the findings; however, the context of the Swedish OHS ergonomists is thoroughly described, and the findings from this study might justifiably be applied to similar contexts [Citation34].
To ensure the credibility of the findings, the transcribed meaning units and codes were kept close to the interview data, and the analysis process went back and forth between the codes and the interviews in several steps, and were discussed between the first and third authors [Citation35].
Four years passed between the ergonomists’ participation in the research program and the follow-up. Thus, other factors, in addition to the ergonomists’ participation in the research project, may have affected their risk assessment procedure. It was a conscious choice to let a few years pass, to allow possible changes to be implemented and tested and to be considered as manifest by the ergonomists. If we had wanted to evaluate outcomes directly related to the e-learning program, it would have been necessary to use a different study design and to include a control group. However, the aim of the present study was to explore the key informants’ experiences. The results from the study may contribute new knowledge for the development of OHS ergonomists’ risk assessments.
5 Conclusions
This study showed that e-learning may comprise efficient knowledge translation for improved risk assessments in OHS. However, it is important to include different types of interactions between the participants during training. Furthermore, education in risk assessment tools should be combined with education in the risk assessment process as a whole and discussions about deficiencies in risk assessment tools. The program contributed to changes in their risk assessment procedures, e.g., in the selection of tools, increasing the number of observers, employing a participatory approach and more often actively involving stakeholders during the risk assessment process.
A suggestion for future research is to explore the implementation of e-learning concepts. Furthermore, future research should explore the risk assessment approach described as being developed by the ergonomists in the study – an approach in which the ergonomist’s role is that of a facilitator (in contrast to executor) in the risk assessment process, to guide the client throughout the assessment and analysis. Moreover, further research is needed to evaluate whether such an approach facilitates implementation of risk-controlling activities leading to improvements in the work environment.
Acknowledgements
The authors would like to acknowledge the other members of the observation project team: Katarina Kjellberg, Per Lindberg, Peter Palm and Ida-Märta Rhen. Further, they would like to give special thanks to Per Lindberg for his work with the risk-assessment lecture included in the e-learning program. Finally, the authors wish to acknowledge the participating ergonomists for sharing their experiences.
Disclosure statement
No potential conflict of interest was reported by the authors.
Additional information
Funding
References
- de Kok J, Vroonhof P, Snijders J, et al. Work-related musculoskeletal disorders: prevalence, costs and demographics in the EU. European Risk Observatory Report. Luxembourg: European Agency for Safety and Health at Work – EU-OSHA; 2019.
- Yazdani A, Wells R. Barriers for implementation of successful change to prevent musculoskeletal disorders and how to systematically address them. Appl Ergon. 2018;73:122–140. doi: 10.1016/j.apergo.2018.05.004
- Hignett S. Intervention strategies to reduce musculoskeletal injuries associated with handling patients: a systematic review. Occup Environ Med. 2003;60:1–8. doi: 10.1136/oem.60.9.e6
- David G. Ergonomic methods for assessing exposure to risk factors for work-related musculoskeletal disorders. Occup Med. 2005;55:190–199. doi: 10.1093/occmed/kqi082
- Neumann P. Inventory of human factors tools and methods – a work system design perspective. Technical report. Ryerson University: Human Factors Engineering Laboratory; 2007.
- Takala EP, Pehkonen I, Forsman M, et al. Systematic evaluation of observational methods assessing biomechanical exposures at work. Scand J Work Environ Health. 2010;36:3–24. doi: 10.5271/sjweh.2876
- Wells RP, Neumann WP, Nagdee T, et al. Solution building versus problem convincing: ergonomists report on conducting workplace assessments. IIE Trans Occup. 2013;1:50–65.
- Chiasson M-È, Imbeau D, Aubry K, et al. Comparing the results of eight methods used to evaluate risk factors associated with musculoskeletal disorders. Int J Ind Ergon. 2012;42(5):478–488. doi: 10.1016/j.ergon.2012.07.003
- Eliasson K, Lind CM, Nyman T. Factors influencing ergonomists’ use of observation-based risk-assessment tools. Work. 2019;64:93–106. doi: 10.3233/WOR-192972
- Arezes PM, Miguel AS, Colim AS. Manual materials handling: knowledge and practices among Portuguese health and safety practitioners. Work. 2011;39:385–395. doi: 10.3233/WOR-2011-1189
- Diego-Mas J-A, Poveda-Bautista R, Garzon-Leal D-C. Influences on the use of observational methods by practitioners when identifying risk factors in physical work. Ergonomics. 2015;58:1660–1670. doi: 10.1080/00140139.2015.1023851
- Laring J, Neumann P, Nagdee T, et al. Human factors tool use among Swedish ergonomists. In: Proceedings of the 38th Annual Association of Canadian Ergonomists (ACE) Conference; 2007 Oct 14–17:1–9. The Association of Canadian Ergonomists (ACE), Toronto.
- Brämberg EB, Nyman T, Kwak L, et al. Development of evidence-based practice in occupational health services in Sweden: a 3-year follow-up of attitudes, barriers and facilitators. Int Arch Occ Env Hea. 2017;90(4):335–348. doi: 10.1007/s00420-017-1200-8
- Grimshaw JM, Shirran L, Thomas R, et al. Changing provider behavior: an overview of systematic reviews of interventions. Med Care. 2001;39(8 Suppl 2):II2–45.
- Graham ID, Logan J, Harrison MB, et al. Lost in knowledge translation: time for a map? J Contin Educ Health Prof. 2006;26(1):13–24. doi: 10.1002/chp.47
- Straus SE, Tetroe J, Graham I. Defining knowledge translation. Can Med Assoc J. 2009;181:165–168. doi: 10.1503/cmaj.081229
- Forsman M, Eliasson K, Rhen I-M, et al. Reliability in twelve ergonomists’ three-category risk ratings in ten video recorded work tasks. In: Proceedings of the 19th Triennial Congress of the IEA; 2015 Aug 9–14; International Ergonomics Association, Melbourne, VIC.
- Patton MQ. Qualitative research & evaluation methods: integrating theory and practice. 4th ed. Thousand Oaks (CA): SAGE; 2014.
- Graneheim UH, Lundman B. Qualitative content analysis in nursing research: concepts, procedures and measures to achieve trustworthiness. Nurse Educ Today. 2004;24(2):105–112. doi: 10.1016/j.nedt.2003.10.001
- Elo S, Kyngaes H. The qualitative content analysis process. J Adv Nurs. 2008;62(1):107–115. doi: 10.1111/j.1365-2648.2007.04569.x
- Vaona A, Banzi R, Kwag KH, et al. E-learning for health professionals. Cochrane Database Syst Rev. 2018;1(1):1–78.
- Nagamachi M. Requisites and practices of participatory ergonomics. Int J Ind Ergon. 1995;15(5):371–377. doi: 10.1016/0169-8141(94)00082-E
- Wilson JR, editor. Ergonomics and participation. 2nd ed. London: Taylor & Francis; 1995.
- Rhén IM, Forsman M. Inter- and intra-rater reliability of the OCRA checklist method in video-recorded manual work tasks. Appl Ergon. 2020;84:103025. doi: 10.1016/j.apergo.2019.103025
- Mathiassen SE, Liv P, Wahlström J. Cost-efficient measurement strategies for posture observations based on video recordings. Appl Ergon. 2013;44(4):609–617. doi: 10.1016/j.apergo.2012.12.003
- Mathiassen SE, Liv P, Wahlström J. Cost-efficient observation of working postures from video recordings – more videos, more observers or more views per observer? Work. 2012;41:2302–2306. doi: 10.3233/WOR-2012-0456-2302
- van Eerd D, Cole D, Irvin E, et al. Process and implementation of participatory ergonomic interventions: a systematic review. Ergonomics. 2010;53(10):1153–1166. doi: 10.1080/00140139.2010.513452
- Haines H, Wilson JR, Vink P, et al. Validating a framework for participatory ergonomics (the PEF). Ergonomics. 2002;45(4):309–327. doi: 10.1080/00140130210123516
- Burgess-Limerick R. Participatory ergonomics: evidence and implementation lessons. Appl Ergon. 2018;68:289–293. doi: 10.1016/j.apergo.2017.12.009
- Berlin C, Neumann WP, Theberge N, et al. ‘Power base’ tactics for workplace change – an interview study with industrial engineers and ergonomists. Ergonomics. 2017;60(5):613–627. doi: 10.1080/00140139.2016.1213886
- Whysall ZJ, Haslam RA, Haslam C. Processes, barriers, and outcomes described by ergonomics consultants in preventing work-related musculoskeletal disorders. Appl Ergon. 2004;35(4):343–351. doi: 10.1016/j.apergo.2004.03.001
- Macdonald W, Oakman J. Requirements for more effective prevention of work-related musculoskeletal disorders. BMC Musculoskelet Disord. 2015;16(1):1–9. doi: 10.1186/s12891-015-0750-8
- CREE. Certification of professional ergonomists in Europe [Internet]; [cited 2019 Dec 12]. Available from: https://eur-erg.eu/.
- Shenton AK. Strategies for ensuring trustworthiness in qualitative research projects. Education for Information. 2004;22(2):63–75. doi: 10.3233/EFI-2004-22201
- Krefting L. Rigor in qualitative research: the assessment of trustworthiness. Am J OccupTher. 1991;45(3):214–222. doi: 10.5014/ajot.45.3.214
- Ferreira J, Gray M, Hunter L, et al. Development of an assessment tool for repetitive tasks of the upper limbs (ART). Health and Safety Executive, Derbyshire; 2009. (Research report; no. RR707).
- Douwes M, de Kraker H. Development of a non-expert risk assessment method for hand–arm related tasks (HARM). Int J Ind Ergon. 2014;44(2):316–327. doi: 10.1016/j.ergon.2013.09.002
- Douwes M, de Kraker H. HARM overview and its application: some practical examples. Work. 2012;41(Suppl 1):4004–4009. doi: 10.3233/WOR-2012-0700-4004
- Occhipinti E, Colombini D. A checklist for evaluating exposure to repetitive movements of the upper limbs based on the OCRA index. In: Karwowski W, editor. International encyclopedia of ergonomics and human factors. 2nd ed. Boca Raton (FL): CRC Press; 2006. p. 2535–2541.
- David G, Woods V, Li G, et al. The development of the quick exposure check (QEC) for assessing exposure to risk factors for work-related musculoskeletal disorders. Appl Ergon. 2008;39(1):57–69. doi: 10.1016/j.apergo.2007.03.002
- Moore JS, Garg A. The strain index: a proposed method to analyze jobs for risk of distal upper extremity disorders. Am Ind Hyg Assoc J. 1995;56(5):443–458. doi: 10.1080/15428119591016863
- Swedish Work Environment Authority. AFS 2012:2 Belastningsergonomi [Physical ergonomics]. 2012. Swedish Work Environment Authority, Stockholm..
Appendix 1
Observational-based risk assessment tools (OBRATs) included in the e-learning program:
• Assessment of repetitive tasks (ART) [Citation36]
• Hand–arm risk assessment method (HARM) [Citation37,Citation38]
• Occupational repetitive actions checklist (OCRA) [Citation39]
• Quick exposure checklist (QEC) [Citation40]
• Strain index (SI) [Citation41]
• Repetitive work model (Physical ergonomics: provisions of the Swedish Work Environment Authority [SWEA-AFS]) [Citation42]