
Abstract
Objectives. The aim of this systematic review was to describe interventions which promote safe patient handling and movement (PHM) among workers in healthcare by reviewing the literature on their effectiveness for work and health-related outcomes. Methods. Databases were searched for studies published during 1997–2018. Measures were operationalized broadly, capturing outcomes of work and health. Only randomized controlled trials (RCTs) and cohort studies with a control group were included. Quality was assessed using evidence-based checklists by the Swedish Agency for Health Technology Assessment and Assessment of Social Services. Results. The systematic review included 10 RCTs and 19 cohort studies. Providing work equipment and training workers is effective: it can increase usage. Training workers to be peer coaches is associated with fewer injuries. Other effective strategies are participatory ergonomics and management engagement in collaboration with workers, facilitating safe PHM. Conclusions. This systematic review suggests that interventions for safe PHM with an impact of health-related outcomes should include access to work equipment, training as well as employer and employee engagement. The additional impact of multifaceted interventions is inconclusive.
Practitioner summary
In clinical practice, there is a need for employers in healthcare to provide healthcare workers access to suitable work equipment and to provide training on how to use work equipment to prevent work-related injuries. Furthermore, the study also indicates that training and appointing peer coaches can facilitate safe manual handling and movement (PHM), and that it can be beneficial to involve workers in a participatory approach.
1. Introduction
Patient handling and movement (PHM) is one of the most common healthcare situations in which work-related musculoskeletal injuries occur. Until now, the scientific literature has mainly described outcomes such as work-related injuries in the lower back, neck and shoulder among healthcare workers such as nurses and nurse assistants [Citation1–3]. Frequent patient transfers, heavy lifting and patient mobilizations have been shown to be risk factors for lower back pain (LBP) [Citation4,Citation5]. The risk of musculoskeletal disorders (MSDs) and sickness absence is also reported to be high among occupational groups such as nurses and assistant nurses since their work is physically demanding [Citation6]. Organizational and social factors in the work environment, such as high workload or under-staffing, can also give rise to work injuries. In a review, Bernal et al. [Citation7] found a relationship between psychosocial risk factors and increased incidence of MSDs among nurses and nurse assistants. We can conclude that the risk factors for MSDs are multifactorial and interact with one another: physical workload; organizational and psychosocial factors; individual factors [Citation4,Citation7]. A combination of interventions is therefore needed to facilitate safe PHM, promote health and prevent MSDs among healthcare workers. There is today greater interest among employers and employees in healthcare in implementing strategies for safe PHM. Although such strategies are not easy to implement, a growing literature on implementation strategies provides guidance on how to translate research into practice and how to cope with the multiple barriers and facilitators, which can vary between occupational groups and between different types of workplace [Citation8]. Worldwide, a range of studies have identified interventions that promote safe PHM and prevent work-related MSDs. Most of these involve greater use of work equipment and assistive devices, training and lifting techniques, and manual handling and training programmes [Citation3,Citation9,Citation10]. The outcome measures in these studies have largely focused on the effect on MSDs, use of work equipment and assistive devices, biomechanical loading, physical exertion and sick leave. There are other relevant outcomes that can reflect consequences of unsafe PHM, e.g., sick leave and work injuries. However, there is a lack of up-to-date systematic reviews based on workplace-oriented interventions to promote safe PHM in healthcare, with no restriction of work and health-related outcomes in the search strategy. The aim of this systematic review was, accordingly, to describe interventions which promote safe PHM among workers in healthcare by reviewing the literature about their effectiveness for work and health-related outcomes.
2. Methods
A systematic literature search with a broad search strategy was conducted by the three authors. The search looked at interventions promoting safe PHM.
2.1. Search strategy
The PICO model is established by others. We used PICO in our study and the search strategy: population (workers in health and social care, ambulance and transportation); intervention (any intervention aiming to promote safe PHM); control (any available intervention, no restriction); outcomes (work and health-related outcomes – sickness absence, sick leave, injuries, pain, increased use of safe PHM). The search was based on the PICO model, but to further operationalize it we decided to use the SPICE (setting, perspective, intervention, comparison, evaluation) framework for the search strategy. In the SPICE approach, the PICO population component is divided into two parts: setting and perspective. Furthermore, outcomes are replaced by an evaluation in the SPICE approach, targeting a broader evaluation framework. We wanted to identify a variety of interventions on an individual, group and organizational level. We also wanted to include studies that covered different types of work and health-related outcomes. Another inclusion criterion in this systematic review was that studies must have been published in English between 1997 and 2018. Search terms, including free terms and MeSH terms, are presented in Table .
Table 1. Presenting the search strategy based on search terms according to the SPICE approach using Boolean operators (ORs).
2.2. Study selection
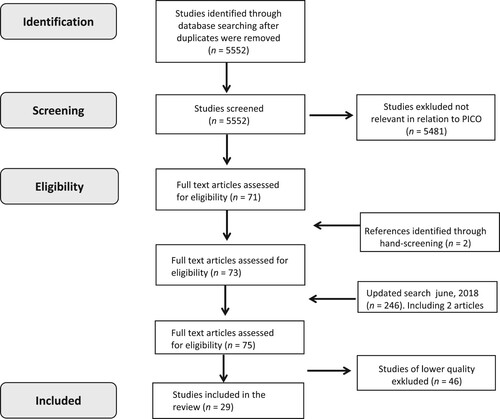
The search was guided by the SPICE framework and systematically performed in December 2017 in scientific electronic databases. We found the following: Academic Search Complete, 555 studies; AMED, 81 studies; Cinahl Complete, 1019 studies; Cochrane Library, 286 studies; Embase, 2951 studies; Engineering Village, 95 studies; Psycinfo, 380 studies; PubMed, 2095 studies; Scopus, 1148 studies; Soc Index, 32 studies. The total number of hits was 8632, and after removing duplicates was 5552. All authors screened the abstract and title of the first 500 references independently. The authors discussed these articles and reached over 95% agreement about whether to include or exclude articles, based on relevance. On the basis of this high level of agreement, the rest of the records were divided among the three authors with each author independently screening references based on the title and abstract. These individual assessments of relevance were then discussed by all three authors, until agreement was reached. A total of 71 articles were potentially eligible and read in full text by all three authors. Reference lists of all included articles were manually searched for additional studies. Two such articles were included, giving a total of 73 articles to assess for relevance. To ensure that the most recently published articles were included, a supplementary search was conducted in June 2018. This found a further 246 (duplicates 94) potentially eligible references. Of these, only two articles were finally included, giving a total of 75 full-text articles to assess for relevance. In the review process, the chosen studies were assessed for relevance by all three authors using standardized checklists provided by the Swedish Agency for Health Technology Assessment and Assessment of Social Services [Citation11]. In the last step, we included randomized controlled trials (RCTs) and cohort studies with a concurrent control group, hereafter called cohort studies. This systematic literature review comprises 29 articles. Details of the selection process are shown in Figure .
Figure 1. Flow chart of study identification and inclusion. Note: PICO = population, intervention, control, outcomes.
2.3. Risk of bias assessment
Risk of bias (low, moderate, high) for each individual study was independently and systematically assessed by two of the authors (E.N.S., K.S.) using standardized checklists provided by the Swedish Agency for Health Technology Assessment and Assessment of Social Services [Citation11]. These checklists [Citation12] cover the same factors that are recommended and used in international guidelines for reporting standards. A similar checklist is used when performing Cochrane reviews. Disagreements about the quality rating of each study were solved via discussion with a third reviewer (C.W.). Table presents information about how risk of bias was assessed for each study.
Table 2. Presentation of the ratings for risk of bias (low, moderate or high) for the included studies: 10 randomized controlled trials (RCTs) and 19 cohort studies with a control group.
2.4. Definitions of interventions
The range of evaluated interventions was broad. For this reason, studies were categorized into four groups according to the description of the intervention: work equipment, including studies chiefly interested in the effect of using ceiling lifts and other equipment; education and training, involving interventions that train healthcare workers in practical PHM and movement training, ergonomics and coaching programme training; participatory ergonomics (PE), including interventions that actively involved healthcare workers in developing and implementing changes at the workplace for better productivity, safety and health, and for promoting safe PHM; and, lastly, multifaceted interventions for promoting safe PHM, comprising several components and taking place within the framework of a programme or policy which was sanctioned at management level. The programmes varied slightly but usually included access to appropriate work equipment, specially trained workers to support safe PHM and some form of risk assessment and policy.
3. Results
We included 10 RCTs and 19 cohort studies. Their main results are presented in Tables . The studies have a widely varying study population and encompass nurses, non-registered nurses and healthcare employees with or without health complaints at the start of the study. The studies also represent a wide range of both interventions and work and health-related outcomes. The outcomes were divided into the following categories: reported work injuries, sick leave/absenteeism, health complaints such as pain and other work-related outcomes, usefulness of intervention (e.g., use of equipment).
Table 3. Characteristics of the included studies based on intervention with work equipment for safe patient handling and movement: two randomized controlled trials (RCTs) and four cohort studies with a control group.
Table 4. Characteristics of the included studies based on interventions with training for safe patient handling and movement: four randomized controlled trials (RCT) and eight cohort studies with a control group.
Table 5. Characteristics of the included studies based on interventions with participatory ergonomics (PE) (n = 4): three randomized controlled trials (RCTs) and one cohort study.
3.1. The risk of bias assessment
Three categories (low, moderate, high) were used to assess risk of bias, as presented in Table . According to the ratings, two studies had high risk of bias, 22 studies had moderate risk of bias and five studies had low risk of bias.
3.2. Interventions for safe PHM
The studies are presented in four groups, based on the type of work intervention as already described. They are presented in detail in the corresponding tables [Citation3–6]. The results are structured according to the evaluated intervention’s content and outcomes, with the results for RCTs presented first.
3.2.1. Work equipment
Work equipment for safe PHM was evaluated in two RCTs [Citation12,Citation13] and four cohort studies [Citation14–17], all conducted in North America. All of the studies looked at effect compared with no intervention. Work-related musculoskeletal injury was the most common outcome. Characteristics and main results of these studies are summarized in Table . One RCT from Canada by Yassi et al. [Citation12] found that healthcare professionals performed less manual patient handling, were more likely to use work equipment and perceived less fatigue after an intervention with training and greater access to work equipment/assistive devices (transfer belts, sliding devices and other manual assistive devices). For one of the intervention groups, the use of a total body lift significantly increased at 6-month follow-up and was sustained at 1-year follow-up. However, the incidence of reported musculoskeletal injuries related to PHM was similar in the intervention and control groups at 12-month follow-up [Citation12]. In another RCT by Kraus et al. [Citation13], the group of homecare workers that received a back-belt had a lower rate of lower back injuries than those who received advice about lifting and back health and those who received no intervention. For the two RCTs, insufficient description of the randomization, outcomes and interventions were the main sources of moderate risk of bias (Table ). Four cohort studies found that the introduction of work equipment and training reduced the incidence of reported musculoskeletal injuries, the perceived risk of injury and perceived exertion, compared with no intervention [Citation14–17]. One cohort study was rated as having low risk of bias and the other three as moderate because of unclear descriptions of drop-out, sampling procedures and interventions (Table ).
3.2.2. Education and training
Twelve of the 29 studies evaluated education and training for safe PHM. Five of them also included training programmes with workers as coaches (Table ). The studies were conducted in Brazil, Canada, Denmark, France, Hungary, Iran, Sweden and the USA. Four studies were designed as RCTs [Citation18–21] and eight were cohort studies [Citation22–29]. The studies evaluated effect compared with no or brief intervention. Incidence or frequency of pain, pain intensity, perceived exertion, and lifting and handling techniques were the most common outcomes, but injury claims and costs were also reported.
In an RCT by Jensen et al. [Citation20], training nurses and nurse assistants in PHM and training instructors to supervise colleagues demonstrated no effect on LBP intensity or perceived exertion. Interventions comprising physical exercise and education for nurses and nurse assistants with LBP were evaluated in two RCTs [Citation18,Citation19]. The study by Járomi et al. [Citation19] evaluated the effect of physical exercise and education on pain intensity among nurses with LBP. The programme consisted of theory of biomechanics, ergonomics, safe patient handling and strengthening exercises. The results demonstrated the effect of a reduction of LBP intensity, improved lumbar range of motion and lifting techniques in the intervention groups (Table ). Another RCT by Alexandre et al. [Citation18] which evaluated a similar comprehensive intervention found no differences between groups in LBP intensity, although reduced neck pain intensity and improved lifting techniques were found. Risk of bias was assessed as low in the RCT by Járomi et al. [Citation19] and as moderate in the other two RCTs [Citation18,Citation20].
The effect of education and training in PHM for nurses or nurse assistants was evaluated in four cohort studies [Citation22,Citation24,Citation26,Citation28]. These cohort studies gave somewhat conflicting results. The study by Shojaei et al. [Citation28] demonstrated that an educational programme with physical exercises reduced LBP intensity. Similar findings were reported in a study into the incidence of LBP after training in PHM. However, statistical significance did not remain when only the same respondents from baseline to follow-up were included [Citation22]. Another study demonstrated an unchanged incidence of neck pain, shoulder pain and LBP [Citation24]. The proportion of nurses with LBP and other physical disorders fell in the groups receiving education and training [Citation24,Citation26], but there was no effect on perceived exertion [Citation24,Citation26]. Risk of bias was assessed as high in one cohort study [Citation24] and moderate in the other studies [Citation22,Citation26,Citation28].
Interventions featuring training programmes with workers as coaches (peer coaching programmes) were evaluated in one RCT [Citation21] and four cohort studies [Citation23,Citation25,Citation27,Citation29]. According to the RCT by Warming et al. [Citation21], training in manual patient handling with peer coaching, as a single intervention or in combination with physical exercise, had no effect on the occurrence of LBP, pain intensity or sick leave. Risk of bias was deemed as moderate in this RCT. One cohort study by Hartvigsen et al. [Citation25] found that training in patient handling with peer coaching had no effect on the number of days or episodes of LBP in the previous year. The other three cohort studies found that the rate of reported injury was reduced with peer coaching about overhead lift use [Citation29] or as part of a transfer, lifting and repositioning programme [Citation23,Citation27]. These two cohort studies were based on the same data [Citation23,Citation27]. The concept involves experts training a number of nurses or nurse assistants to be peer coaches or trainers, who will pass on the knowledge and practical skills in patient handling and use of work equipment to their colleagues. The cost–benefit analysis by Tompa et al. [Citation29] showed that the peer coaching programme reduced patient-handling injuries with a modest cost investment for coaches’ working hours. Risk of bias was rated moderate to high in the cohort studies.
3.2.3. Participatory ergonomics
Interventions comprising PE were evaluated in five articles based on data from three RCTs and one cohort study (Table ). The studies were conducted in Thailand [Citation30], Denmark [Citation31–33] and the USA [Citation34]. The effect of PE was evaluated on the following outcomes: LBP intensity, number of days with LBP and use of work equipment, compared with control groups without intervention. In two RCTs, pain intensity was reduced by an intervention consisting of PE, physical training and cognitive behavioural therapy [Citation32] or after an intervention with the active involvement of employees [Citation30]. The third RCT found no group differences in pain intensity or self-reported lumbar injury [Citation31]. Improvements in physical capacity and fear avoidance were found, but no effect on self-reported work ability or sickness absence [Citation33]. The PE interventions resulted in a reduced amount of lifting without work equipment [Citation33] and more general use of work equipment [Citation31]. Jakobsen et al. [Citation31] found improved communication, better guidance on performing PHM and greater collegial encouragement to use work equipment. Two of the RCTs were assessed as having low risk of bias and one RCT as moderate. The cohort study by Evanoff et al. [Citation34] demonstrated that the participatory programme that was launched at a hospital reduced injuries, absence and experience of musculoskeletal pain. The participants in the intervention also saw an improvement in job satisfaction and psychosocial aspects.
3.2.4. Multifaceted interventions
The present review included five cohort studies with a control group looking at multifaceted interventions (Table ). The studies were conducted in England [Citation35], Turkey [Citation36], Denmark [Citation37], the USA [Citation34,Citation38] and Canada [Citation39]. The studies covered multifaceted interventions, as described earlier, and a large number of outcomes were presented. The Danish study [Citation37] found that the participants in the intervention group made greater use of equipment and had a more positive attitude towards it. One other positive effect was that fewer aggressive episodes occurred. Two other studies [Citation38,Citation40] also found that the multifaceted intervention significantly increased the use of work equipment. Smedley et al. [Citation35] found no improvement in non-manual transferring, but concluded that there was an association between back pain and psychosocial risk factors. The number of work injuries did not decrease in three studies [Citation35,Citation37,Citation38], but did so in another study with a 12-month follow-up [Citation40]. Craib et al. [Citation39] found increased rates of reported injuries in combination with reduced absence. Two other studies [Citation36,Citation37] found no differences in absence. In four studies [Citation35–38] no reduction in musculoskeletal pain was seen. Compared to the control group, registered nurses who took part in an intervention programme had a reduced risk of developing upper limb symptoms and improved their physical activity [Citation36]. Four of the included studies were judged to have a moderate risk of bias, and one study as having a high risk of bias [Citation40].
Table 6. Characteristics of the included studies based on multifaceted intervention for safe patient handling and movement, including six cohort studies with a control group.
4. Discussion
The aim of this study was to provide up-to-date information about the effects on work and health-related outcomes of a broad spectrum of interventions aiming to promote safe PHM.
4.1. Summary of findings
The findings of this systematic literature review demonstrate that providing work equipment and training healthcare workers how to use it is effective because they subsequently perform less manual handling and make greater use of the equipment. Participative ergonomics had an impact on the use of work equipment and improving back pain. Training employees to be peer coaches is associated with fewer work injuries but does not help to reduce symptoms. Education and training in PHM as a single intervention does not prevent the risk of injuries or back pain. However, exercise programmes for healthcare workers can reduce the occurrence and intensity of MSD. Management engagement and support to encourage workers to become actively involved in developing safe PHM are factors for success. Providing peer coaches reduced the number of work injuries but did not impact symptoms. The results for multifaceted interventions varied.
4.2. Usefulness of work equipment
It was commonly concluded in the reviewed studies that the use of work equipment and assistive devices is important for preventing injuries and promoting PHM. However, it is necessary to give training in how to use work equipment such as mobile lifts, wall lifts and overhead ceiling lifts, transfer belts and sliding devices. The review underlined the need for accessible work equipment in care units. The results of our review are in line with a previous systematic literature review by Hegewald et al. [Citation41] that evaluated the usefulness of work equipment in PHM. However, their outcome measure focused on the effect of preventing MSDs. There is a lack of studies focusing on interventions promoting safe PHM for healthcare workers in paramedic services. We identified only one study showing that implementation of powered stretchers and load systems reduced MSDs [Citation14]. The paramedic setting is very different from the hospital setting, yet both involve physically and mentally demanding work where the use of equipment can reduce the workload. Paramedic services is an area in which more research is needed to evaluate the specific effect of promoting safe PHM and preventing work-related MSDs.
4.3. Education and training
The findings of this review reveal that providing physical exercise as a component in a programme for safe PHM can reduce LBP intensity for nurses and nurse assistants [Citation19,Citation28]. Physical capacity may be one important risk factor for LBP and long-term sick leave [Citation42]. The importance of strengthening the physical capacity of healthcare workers by means of physical training in the workplace has been suggested in previous research which gave positive results in the form of reduced MSDs [Citation43,Citation44]. Further research is needed into what the successful components of these workplace-based interventions may be as well as the dose–response. However, the causes of pain and disability among healthcare workers are multifactorial, and physical capacity is only one aspect. In a study by Andersen et al. [Citation4], a high number of daily patient transfers was a risk factor for LBP. Measures for prevention of LBP included providing necessary assistive devices and facilitating good collaboration between co-workers. This is in line with the findings of this literature review.
4.4. Participatory ergonomics
The studies included in this review suggest that the use of PE in healthcare settings shows promising results in relation to pain [Citation30,Citation32,Citation34] and use of work equipment [Citation31,Citation33]. In line with a previous review by van Eerd et al. [Citation45] we found that it is essential to involve managers, healthcare workers and specialists or advisors when planning and improving the work environment in order to promote safe PHM. Furthermore, healthcare workers need to control their own work activities, being motivated, receiving support and finding a way forward on how to promote safe PHM, to influence desired positive health and work-related outcomes. Using PE can also improve social support at work between colleagues and employers. It has been emphasized that the timely and integrated implementation of methods in the actual work situation is the real challenge when promoting safe PHM, preventing injuries and increasing the use of lifting devices [Citation46]. A Danish RCT by Jakobsen et al. [Citation31] evaluated the effect of a participatory organizational intervention, which led to greater general use of assistive devices and improved communication and guidance in the use of assistive devices. A culture in which risk prevention features prominently and which includes a participatory approach to promoting occupational safety and health (OSH) in the workplace may benefit both healthcare workers and their patients. We need to eliminate risks at source.
4.5. Multifaceted interventions with a system approach
In a recent meta-analysis by Teeple et al. [Citation47], multifaceted interventions were found to reduce the risk of injuries and promote safe PHM. Our systematic review found diverging results and it is not possible to conclude that such interventions had any effect on work injuries. The same holds for the effect of multifaceted interventions on sick leave. In line with Richardson et al.’s [Citation48] review, we found no support for such interventions having any effect on musculoskeletal pain. This contradicts the results of a review by Tullar et al. [Citation49], who found some support for the effectiveness of multifaceted interventions on musculoskeletal health. We found three studies indicating that multifaceted interventions can promote safe PHM situations if work equipment is used. However, it is always difficult to evaluate the effects of interventions that include differing components. Having a policy was a component of most of the studies of multifaceted interventions. This may be an important aspect of the intervention; it can provide guidance to both healthcare workers and patients on how the PHM safely can be conducted. Two studies emphasize the importance of performing a risk assessment for each patient and of updating it regularly [Citation50,Citation51]. We found that risk assessments were often integrated into multifaceted interventions. Various risk assessment tools are mentioned, sometimes developed by the authors. As always, however, it is important to use reliable methods for assessment. OSH legislation requires employers to conduct risk assessments to prevent risks. In hospitals and other healthcare settings, there are a number of situations in which both patient and healthcare professionals are at risk of injury [Citation2,Citation52]. Risk assessments need to simultaneously take a variety of risks and perspectives into account. For example, the bariatric or the aggressive patient can be a very manually demanding type of patient in terms of care, transportation and PHM. Research by Dennerlein et al. [Citation38] suggests that safe patient handling and mobility equipment and practices should be used in relation to the specific and individualized care plan for each patient in the hospital. The safety of patients and healthcare workers goes hand in hand, and there is a strong relationship between patient safety climate and occupational safety climate [Citation53]. Previous research has highlighted the value of a system-oriented approach in healthcare for integrating human factors, safety management and organizational factors, and promoting OSH. The systems engineering initiative for patient safety (SEIPS) model, presented by Carayon et al. [Citation54], is one of the most widely used models globally.
4.6. Strengths and limitations of this review
The broad search strategy including all types of interventions with the intention to promote safe PHM and using the PICO model can be seen as both a strength and a weakness. We wanted to be able to describe results from a broad spectrum of interventions and outcomes. This poses difficulties when summarizing the results, but it also provides a more complete description of important interventions that can impact safe PHM and health-related outcomes. We categorized the results according to type of intervention. This was not generally a problem, although some studies needed discussion to determine the correct category. We categorized studies as multifaceted interventions if they were described as such in the publication. If not, we scrutinized the description of the intervention and based our decision on the descriptions by Adamszyk [Citation55] and Tullar et al. [Citation49], in order to distinguish interventions that should be categorized into the other groups (work equipment, education and training and participatory interventions). The search and inclusion process is described in detail. All three authors were involved in judging the relevance of the studies. We also used a well-established method to assess risk of bias. In general, there was a good degree of agreement between the evaluators. When disagreement did arise, the authors went back to the study and discussed until agreement was reached.
4.6.1. Assessment of quality
We included 10 RCTs and 19 cohort studies with control groups. The quality of these 29 studies was assessed with the aid of well-established protocols. Most of the studies were judged as having moderate risk of bias. Two were assessed as having a high risk of bias; both were cohort studies. One of these was a pilot study [Citation40]. Four of five studies having low risk bias were RCTs. One-third of the studies in this review were RCTs, which can be seen as a strength. We decided also to include control studies in order not to miss important interventions. Our quality assessments found them generally to be studies of moderate quality. The RCTs are not evenly distributed between the three categories. None of the RCTs was found to be a multifaceted intervention. This adds further doubts as to how to interpret the results. To evaluate the overall effect of interventions promoting safe PHM we need more high-quality studies to be able to evaluate the effect of multifactorial interventions. On the basis of our systematic review, we can conclude that there are too few high-quality studies of policies and system-based approaches to enable us to evaluate the effect of multifaceted interventions promoting safe PHM.
4.7. Clinical implications
This literature review offers guidance for workplaces on what type of evidence-based interventions can contribute to safe PHM. For these interventions to be successful, an implementation strategy is needed in which management and healthcare workers collaborate, and preferably with the help of an appointed internal facilitator [Citation37]. The prevention of MSDs is urgently needed by healthcare workers, in Europe and globally. It is one of the most prevalent work-related problems, causing sickness absence and sickness presence [Citation4–7].
5. Conclusions
This review has a broad approach encompassing a diversity of interventions and health-related outcomes and provides up-to-date evidence about interventions designed to promote safe PHM in healthcare and social care. We found employer involvement and the provision of work equipment and adequate training for healthcare workers to be the factors which have the greatest effect on outcomes. Involving workers in a participatory approach may also be beneficial. However, it is not possible to conclude that multifaceted interventions had additional impact on work injuries or on sick leave. To be able to evaluate these outcomes it is important to formulate the intention and goal of the interventions in advance.
Acknowledgements
The authors would like to acknowledge the support of information specialists Carola Tilgmann and Matthias Bank at Lund University library, Sweden, in designing and performing the systematic search strategy. This study was partly supported by the Swedish Work Environment Authority, where a Swedish report was completed [Citation56]. For this systematic review, the authors did not receive any specific grant from funding agencies in the public, commercial or not-for-profit sectors. This study was a collaboration between three authors from three different Swedish regions. The authors would like to thank all of the organizations for enabling them to conduct this study.
Disclosure statement
No potential conflict of interest was reported by the authors.
References
- Davis KG, Kotowski SE. Prevalence of musculoskeletal disorders for nurses in hospitals, long-term care facilities, and home health care: a comprehensive review. Hum Factors. 2015;57(5):754–792. doi:10.1177/0018720815581933
- Wåhlin C, Kvarnström S, Öhrn A, et al. Patient and healthcare worker safety risks and injuries. Learning from incident reporting. Eur J Physiother. 2020;22(1):44–50. doi:10.1080/21679169.2018.1549594
- Pompeii LA, Lipscomb HJ, Schoenfisch AL, et al. Musculoskeletal injuries resulting from patient handling tasks among hospital workers. Am J Ind Med. 2009;52(7):571–578. doi:10.1002/ajim.20704
- Andersen LL, Vinstrup J, Villadsen E, et al. Physical and psychosocial work environmental risk factors for back injury among healthcare workers: prospective cohort study. Int J Environ Res Public Health. 2019;16(22):4528. doi:10.3390/ijerph16224528
- Serranheira F, Sousa-Uva M, Sousa-Uva A. Hospital nurses tasks and work-related musculoskeletal disorders symptoms: a detailed analysis. Work. 2015;51(3):401–409. doi:10.3233/WOR-141939
- Andersen LL, Clausen T, Mortensen OS, et al. A prospective cohort study on musculoskeletal risk factors for long-term sickness absence among healthcare workers in eldercare. Int Arch Occup Environ Health. 2012;85(6):615–622. doi:10.1007/s00420-011-0709-5
- Bernal D, Campos-Serna J, Tobias A, et al. Work-related psychosocial risk factors and musculoskeletal disorders in hospital nurses and nursing aides: a systematic review and meta-analysis. Int J Nurs Stud. 2015;52(2):635–648. doi:10.1016/j.ijnurstu.2014.11.003
- Powell BJ, Fernandez ME, Williams NJ, et al. Enhancing the impact of implementation strategies in healthcare: a research agenda. Front Public Health. 2019;7:3. doi:10.3389/fpubh.2019.00003
- Hignett S. Intervention strategies to reduce musculoskeletal injuries associated with handling patients: a systematic review. Occup Environ Med. 2003;60(9):E6. doi:10.1136/oem.60.9.e6
- Engkvist IL. Evaluation of an intervention comprising a no lifting policy in Australian hospitals. Appl Ergon. 2006;37(2):141–148. doi:10.1016/j.apergo.2005.05.008
- Statens beredning för medicinsk och social utvärdering (SBU). Utvärdering av metoder I hälso- och sjukvården: en handbok. Swedish Agency for Health Technology Assessment and Assessment of Social Services. A handbook. Stockholm: SBU; 2013.
- Yassi A, Cooper JE, Tate RB, et al. A randomized controlled trial to prevent patient lift and transfer injuries of health care workers. Spine. 2001;26(16):1739–1746. doi:10.1097/00007632-200108150-00002
- Kraus JF, Schaffer KB, Rice T, et al. A field trial of back belts to reduce the incidence of acute low back injuries in New York City home attendants. Int J Occup Environ Health. 2002;8(2):97–104. doi:10.1179/oeh.2002.8.2.97
- Armstrong DP, Ferron R, Taylor C, et al. Implementing powered stretcher and load systems was a cost effective intervention to reduce the incidence rates of stretcher related injuries in a paramedic service. Appl Ergon. 2017;62:34–42. doi:10.1016/j.apergo.2017.02.009
- Engst C, Chhokar R, Miller A, et al. Effectiveness of overhead lifting devices in reducing the risk of injury to care staff in extended care facilities. Ergonomics. 2005;48(2):187–199. doi:10.1080/00140130412331290826
- Miller A, Engst C, Tate RB, et al. Evaluation of the effectiveness of portable ceiling lifts in a new long-term care facility. Appl Ergon. 2006;37(3):377–385. doi:10.1016/j.apergo.2005.05.012
- Owen BD, Keene K, Olson S. An ergonomic approach to reducing back/shoulder stress in hospital nursing personnel: a five year follow up. Int J Nurs Stud. 2002;39(3):295–302. doi:10.1016/S0020-7489(01)00023-2
- Alexandre NM, de Moraes MA, Correa Filho HR, et al. Evaluation of a program to reduce back pain in nursing personnel. Rev Saude Publica. 2001;35(4):356–361. doi:10.1590/S0034-89102001000400004
- Járomi M, Kukla A, Szilágyi B, et al. Back School programme for nurses has reduced low back pain levels: a randomised controlled trial. J Clin Nurs. 2018;27(5/6):e895–e902. doi:10.1111/jocn.13981
- Jensen LD, Gonge H, Jørs E, et al. Prevention of low back pain in female eldercare workers: randomized controlled work site trial. Spine. 2006;31(16):1761–1769. doi:10.1097/01.brs.0000227326.35149.38
- Warming S, Ebbehoj NE, Wiese N, et al. Little effect of transfer technique instruction and physical fitness training in reducing low back pain among nurses: a cluster randomised intervention study. Ergonomics. 2008;51(10):1530–1548. doi:10.1080/00140130802238606
- Best M. An evaluation of manutention training in preventing back strain and resultant injuries in nurses. Safety Science. 1997;25(1–3):207–222. doi:10.1016/S0925-7535(97)00003-9
- Black TR, Shah SM, Busch AJ, et al. Effect of transfer, lifting, and repositioning (TLR) injury prevention program on musculoskeletal injury among direct care workers. J Occup Environ Med Hyg. 2011;8(4):226–235. doi:10.1080/15459624.2011.564110
- Fanello S, Jousset N, Roquelaure Y, et al. Evaluation of a training program for the prevention of lower back pain among hospital employees. Nurs Health Sci. 2002;4(1–2):51–54. doi:10.1046/j.1442-2018.2002.00098.x
- Hartvigsen J, Lauritzen S, Lings S, et al. Intensive education combined with low tech ergonomic intervention does not prevent low back pain in nurses. Occup Environ Med [Internet]. 2005;62(1):13–17. doi:10.1136/oem.2003.010843
- Kindblom-Rising K, Wahlström R, Nilsson-Wikmar L, et al. Nursing staff’s movement awareness, attitudes and reported behaviour in patient transfer before and after an educational intervention. App Ergon. 2011;42(3):455–463. doi:10.1016/j.apergo.2010.09.003
- Lim HJ, Black TR, Shah SM, et al. Evaluating repeated patient handling injuries following the implementation of a multi-factor ergonomic intervention program among health care workers. J Safety Res. 2011;42(3):185–191. doi:10.1016/j.jsr.2011.05.002
- Shojaei S, Tavafian SS, Jamshidi AR, et al. A multidisciplinary workplace intervention for chronic low back pain among nursing assistants in Iran. Asian Spine J. 2017;11(3):419–426. doi:10.4184/asj.2017.11.3.419
- Tompa E, Dolinschi R, Alamgir H, et al. A cost–benefit analysis of peer coaching for overhead lift use in the long-term care sector in Canada. Occup Environ Med. 2016;73(5):308–314. doi:10.1136/oemed-2015-103134
- Chanchai W, Songkham W, Ketsomporn P, et al. The impact of an ergonomics intervention on psychosocial factors and musculoskeletal symptoms among Thai hospital orderlies. Int J Environ Res Public Health. 2016;13(5):464. doi:10.3390/ijerph13050464
- Jakobsen M, Aust B, Kines P, et al. Participatory organizational intervention for improved use of assistive devices in patient transfer: a single-blinded cluster randomized controlled trial. Scand J Work Environ Health. 2019;45(2):146–157. doi:10.5271/sjweh.3769
- Rasmussen CD, Holtermann A, Bay H, et al. A multifaceted workplace intervention for low back pain in nurses’ aides: a pragmatic stepped wedge cluster randomised controlled trial. Pain. 2015;156(9):1786–1794. doi:10.1097/j.pain.0000000000000234
- Rasmussen CDN, Holtermann A, Jørgensen MB, et al. A multi-faceted workplace intervention targeting low back pain was effective for physical work demands and maladaptive pain behaviours, but not for work ability and sickness absence: stepped wedge cluster randomised trial. Scand J Public Health. 2016;44(6):560–570. doi:10.1177/1403494816653668
- Evanoff BA, Bohr PC, Wolf LD. Effects of a participatory ergonomics team among hospital orderlies. Am J Ind Med. 1999;35(4):358–365. doi:10.1002/(SICI)1097-0274(199904)35:4<358::AID-AJIM6>3.0.CO;2-R
- Smedley J, Trevelyan F, Inskip H, et al. Impact of ergonomic intervention on back pain among nurses. Scand J Work Environ Health. 2003;29(2):117–123. doi:10.5271/sjweh.713
- Sezgin D, Esin MN. Effects of a PRECEDE-PROCEED model based ergonomic risk management programme to reduce musculoskeletal symptoms of ICU nurses. Intensive Crit Care Nurs. 2018;47:89–97. doi:10.1016/j.iccn.2018.02.007
- Risor BW, Casper SD, Andersen LL, et al. A multi-component patient-handling intervention improves attitudes and behaviors for safe patient handling and reduces aggression experienced by nursing staff: a controlled before–after study. App Erg. 2017;60:74–82. doi:10.1016/j.apergo.2016.10.011
- Dennerlein JT, O’Day ET, Mulloy DF, et al. Lifting and exertion injuries decrease after implementation of an integrated hospital-wide safe patient handling and mobilisation programme. Occ Environ Med. 2017;74(5):336–343. doi:10.1136/oemed-2015-103507
- Craib K, Hackett G, Back C, et al. Injury rates, predictors of workplace injuries, and results of an intervention program among community health workers. Public Health Nursing. 2007;24(2):121–131. doi:10.1111/j.1525-1446.2007.00616.x
- Zadvinskis IM, Salsbury SL. Effects of a multifaceted minimal-lift environment for nursing staff: pilot results. West J Nurs Res. 2010;32(1):47–63. doi:10.1177/0193945909342878
- Hegewald J, Berge W, Heinrich P, et al. Do technical aids for patient handling prevent musculoskeletal complaints in health care workers? – A systematic review of intervention studies. Int J Environ Res Public Health. 2018;15(3):476. doi:10.3390/ijerph15030476
- Rasmussen CD, Andersen LL, Clausen T, et al. Physical capacity and risk for long-term sickness absence: a prospective cohort study among 8664 female health care workers. J Occup Environ Med. 2015;57(5):526–530. doi:10.1097/JOM.0000000000000395
- Andersen LL, Poulsen OM, Sundstrup E, et al. Effect of physical exercise on workplace social capital: cluster randomized controlled trial. Scand J Public Health. 2015;43(8):810–818. doi:10.1177/1403494815598404
- Jakobsen MD, Sundstrup E, Brandt M, et al. Effect of workplace- versus home-based physical exercise on musculoskeletal pain among healthcare workers: a cluster randomized controlled trial. Scand J Work Environ Health. 2015;41(2):153–163. doi:10.5271/sjweh.3479
- van Eerd D, Cole D, Irvin E, et al. Process and implementation of participatory ergonomic interventions: a systematic review. Ergonomics. 2010;53(10):1153–1166. doi:10.1080/00140139.2010.513452
- Burdorf A, Koppelaar E, Evanoff B. Assessment of the impact of lifting device use on low back pain and musculoskeletal injury claims among nurses. Occup Environ Med. 2013;70(7):491–497. doi:10.1136/oemed-2012-101210
- Teeple E, Collins JE, Shrestha S, et al. Outcomes of safe patient handling and mobilization programs: a meta-analysis. Work. 2017;58(2):173–184. doi:10.3233/WOR-172608
- Richardson A, McNoe B, Derrett S, et al. Interventions to prevent and reduce the impact of musculoskeletal injuries among nurses: a systematic review. Int J Nurs Stud. 2018;82:58–67. doi:10.1016/j.ijnurstu.2018.03.018
- Tullar J, Brewer S, Amick BC, III, et al. Occupational safety and health interventions to reduce musculoskeletal symptoms in the health care sector. J Occup Rehab. 2010;20(2):199–219. doi:10.1007/s10926-010-9231-y
- Hignett S. Systematic review of patient handling activities starting in lying, sitting and standing positions. J Adv Nurs. 2003;41(6):545–552. doi:10.1046/j.1365-2648.2003.02566.x
- Thomas DR, Thomas YL. Interventions to reduce injuries when transferring patients: a critical appraisal of reviews and a realist synthesis. Int J Nurs Stud. 2014;51(10):1381–1394. doi:10.1016/j.ijnurstu.2014.03.007
- Strid E N, Wahlin C, Ros A, et al. Health care workers’ experiences of workplace incidents that posed a risk of patient and worker injury: a critical incident technique analysis. BMC Health Serv Res. 2021;21(1):511. doi:10.1186/s12913-021-06517-x
- Pousette A, Larsman P, Eklöf M, et al. The relationship between patient safety climate and occupational safety climate in healthcare – a multi-level investigation. J Safety Res. 2017;61:187–198. doi:10.1016/j.jsr.2017.02.020
- Carayon P, Wetterneck TB, Rivera-Rodriguez AJ, et al. Human factors systems approach to healthcare quality and patient safety. Appl Ergo. 2014;45(1):14–25. doi:10.1016/j.apergo.2013.04.023
- Adamczyk MA. Reducing intensive care unit staff musculoskeletal injuries with implementation of a safe patient handling and mobility program. Crit Care Nurs Q. 2018;41(3):264–271. doi:10.1097/CNQ.0000000000000205
- Wåhlin C, Stigmar K, Nilsing Strid E. Säkrare personförflyttningar. Åtgärder i arbetsmiljön för medarbetare inom hälso- och [Safe patient handling. Interventions in the work environment for employees in health care and social care] sjukvård samt omsorg. Kunskapssammanställning 2019:6. Stockholm: Arbetsmiljöverket; 2019.
