
Abstract
Objectives. This study aimed to investigate the consistency between results of the American Conference for Governmental Occupational Hygienists (ACGIH) threshold limit value (TLV) for hand activity and proposed action levels of objective measurements in risk assessments of work-related musculoskeletal disorders. Methods. Wrist velocities and forearm muscular load were measured for 11 assemblers during one working day. Simultaneously, each assembler’s hand activity level (HAL) during three sub-cycles was rated twice on two separate occasions by two experts, using a HAL scale. Arm/hand exertion was also rated by the assemblers themselves using a Borg scale. In total, 66 sub-cycles were assessed and assigned to three exposure categories: A) below ACGIH action limit (AL) (green); B) between AL and TLV (yellow); and C) above TLV (red). The median wrist velocity and the 90th percentile of forearm muscular load obtained from the objective measurements corresponding to the sub-cycles were calculated and assigned to two exposure categories: A) below or C) above the proposed action level. Results. The agreement between ACGIH TLV for hand activity and the proposed action level for wrist velocity was 87%. Conclusions. The proposed action level for wrist velocity is highly consistent with the TLV. Additional studies are needed to confirm the results.
1. Introduction
Repetitive work in combination with excessive and/or prolonged muscular load is common in many workplaces, e.g., in the assembly industry and in food and package handling. Such activities may lead to a high prevalence of work-related wrist disorders [Citation1,Citation2]. Although these risk factors have been known for a considerable time, knowledge concerning the specific levels that may cause complaints and disorders is limited. This makes it difficult to introduce regulations on physical workload. However, some guidelines on the identification of harmful workload have been implemented, an example of which is the American Conference for Governmental Occupational Hygienists (ACGIH) threshold limit value (TLV) for hand activity [Citation3]. This is based on observations and assessments of hand movements (hand activity level [HAL]) and estimated hand force (peak hand force). According to the ACGIH, there is a risk of developing a work-related musculoskeletal disorder (WMSD) if the TLV is exceeded. The ACGIH has also determined an action limit (AL). If this is exceeded, a risk assessment of the work task should be carried out, and if necessary, measures should be taken to reduce the level of exposure. The HAL is assessed by an expert, while arm/hand exertions can be estimated by an expert or by the employee. Assessments are generally based on experience and expertise, yet the results for the same work task can vary, both within and between experts and between observation methods [Citation4,Citation5]. It has therefore been suggested that visual assessments should, when feasible, be replaced by objective measurements [Citation6]. Surface electromyography (sEMG) and goniometry are examples of methods that can be used to obtain quantitative measures of forces and activities of, e.g., the forearm and hand. The methods can be used in a wide range of settings, e.g., to evaluate the effects on the physical workload when new techniques or new technical appliances are implemented. For example, by using goniometry and sEMG, Rislund et al. [Citation7] could conclude that the effects of using a miniature steering wheel in a forklift cab environment, compared to a normal one, indicated an increased risk for overexertion of the left wrist and forearm. Furthermore, in a study carried out by Colim et al. [Citation8], sEMG was used to examine three different inspection devices (for use in aircraft manufacturing settings), in terms of inter alia the best ergonomic conditions. A reduction of muscular effort in e.g., the forearm could be seen when using handle 1. The methods are also useful when studying the muscular load of different work tasks. In Åkesson et al. [Citation9], goniometry and sEMG was used to conclude that use of an ultrasonic scaler by dental hygienists reduced their load on the right forearm extensor muscles and lowered wrist velocities compared to manual scaling.
The Division of Occupational and Environmental Medicine in Lund, Sweden, has studied the relationship between physical workload and WMSDs for almost 30 years. This research has consisted of objective measurements of the physical workload on employees in many occupations. Clinical examinations of the same groups have also been carried out to identify and register complaints and diagnoses in the neck and upper extremities. This research has allowed us to calculate the exposure–response relationship between physical workload and the prevalence of WMSDs [Citation1,Citation10,Citation11]. Based on this knowledge, we have proposed ‘action levels’ for the prevention of WMSDs for whole-day work exposure, and specific cut-off levels have been determined based on experience and expertise [Citation12]. If one or more of these proposed action levels is exceeded, there is a high risk of developing WMSDs. However, levels below the proposed action levels provide no guarantee that WMSDs will be avoided, even if the group mean is below the action level, as there might be a variation in workload between individuals depending on physique, disposition or working technique. Factors such as the need of force and the use of vibrating tools should also be considered. We have proposed an action level for wrist velocities of 20°/s as the median load (50th percentile) over the whole working day [Citation12]. If a considerable amount of force is necessary, or vibrating tools are used, the proposed action level is instead 15°/s. The proposed action level for muscular load in the forearms, in terms of the peak load (90th percentile), is 30% of the maximal voluntary electrical activity (MVE) [Citation12].
Various types of limits and levels have been suggested for risk assessment of physical workloads, based on both subjective and objective methods. However, no study has been carried out to determine whether they are consistent. The aims of this study were therefore: to compare experts’ assessments of HAL with recorded wrist velocity; to compare workers’ self-assessments of exertion of the forearm/hand with recorded forearm muscular load; to examine the inter-rater reliability between experts (in two pairs) using the ACGIH TLV for hand activity; and to examine the consistency between the results of ACGIH TLV for hand activity and proposed action levels for wrist velocity and forearm muscular load, based on objective measurements.
2. Materials and methods
2.1. Study design and participants
Eleven right-handed assembly workers, eight men and three women, volunteered to participate in the study. Their median age was 36 years (range 27–58), height 175 cm (range 167–190) and weight 91 kg (range 63–132). The inclusion criteria were being right-handed and at least 3 months of work experience for all the work tasks included in the assembler’s workstation. The study was carried out at a company that manufactures construction machines. The machines were produced on a production line consisting of several assembly stations, and the work was performed in cycles lasting 40 min. Three of these stations (denoted A, B and C) were included in the study. The selection of workstations was decided in consultation with the production management and was considered representative for all the work at the production line. Each station consisted of three different work tasks. During the workday the assemblers alternated between these three work tasks. The tasks consisted of assembling a variety of components and were carried out using vibrating tools such as screwdrivers and nut drivers, and various non-vibrating hand tools such as rubber mallets and ratchet wrenches.
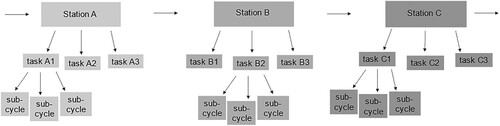
Wrist velocities and muscular load in the forearm extensor muscles were recorded bilaterally for one assembler at a time, during a full working day, using goniometry and sEMG. Two ergonomist experts alternately followed each assembler during the working day and noted the exact starting and stopping times of different work tasks and lunch breaks. This engagement resulted in limited time to perform HAL assessments, and therefore only one task at each station was selected, on the basis that the task was considered (by the assemblers) to be the most strenuous. In the current study, the three selected tasks were divided into three assembling periods (sub-cycles) to be able to assess the workload of them separately (Figure ). Each sub-cycle lasted on average ∼13 min. The three sub-cycles contained different amounts of work and the assemblers had slightly different work pace and work order. Therefore, the sub-cycles ranged from 2 to 23 min for Station A, from 8 to 20 min for Station B and from 11 to 19 min for Station C (Figure ). The HAL and the self-estimated exertion during each sub-cycle were assessed, resulting in three assessments per work cycle. The procedure was repeated twice during the same day, by the two different experts. This meant that each assembler estimated their exertion on two different occasions when performing the same work task; in total, six estimates by each assembler. A total of 66 assessments were thus carried out. As the exact starting and stopping times of each sub-cycle were noted, the expert assessments of HAL and the self-estimated exertion of arm/hand force could be compared with recorded wrist velocities and forearm muscular load. The distribution of the number of assessments at each station varied since the experts performed three pilot objective measurements at Station A. During these, the work at all three stations was studied as preparation for the HAL assessments. Therefore, 12 assessments were carried out for Station A, while 30 assessments were performed at Station B and 24 assessments at Station C.
Figure 1. Three selected workstations A, B and C, which were parts of the production line at the company. Note: Each station consisted of three different work tasks. One task at each station was selected for the hand activity level (HAL) assessments. Each task was divided into three assembling periods (sub-cycles). The exact starting and stopping times of each sub-cycle were noted to be able to compare the assessed hand activity and self-estimated exertion with recorded wrist velocities and forearm muscular load.
The study was approved by the Swedish Ethical Review Authority (No. 2019-04776). All assemblers gave their written informed consent to participate in the study.
2.2. Assessment of workload using the ACGIH TLV for hand activity
The HAL in the 66 sub-cycles was rated by four different ergonomist experts (in two pairs, all well experienced in ergonomics and occupational health and all with a doctoral degree within the field) using a HAL 0–10 scale (visual analogue scale for rating repetition/hand activity) [Citation13]:
0 = hands idle most of the time; no regular exertions
2 = consistent, conspicuous, long pauses; or very slow motions
4 = slow steady motion/exertion; frequent brief pauses
6 = steady motion/exertion; infrequent pauses
8 = rapid steady motion/exertion; no regular pauses
10 = rapid, steady motion/difficulty keeping up or continuous exertion
The verbal anchors from a translated (to Swedish) version of the HAL scale [Citation14] was used to make it easier for the experts to use the scale during assessments in the field. Due to private circumstances, experts 1 and 2 (pair A) assessed 24 sub-cycles each while experts 3 and 4 (pair B) assessed nine sub-cycles each.
The exertion of the forearm/hand was self-estimated by the assemblers using the Borg CR-10 scale (Table ) [Citation15]. A peak force index was then calculated for the TLV and AL, according to Yung et al. [Citation16]. If the peak force index was >1.0 for AL or TLV, the respective limit was exceeded. Moreover, a value <0 of the peak force index for AL also indicated that the AL was exceeded. The results from the assessed sub-cycles were divided into three exposure categories: A) less than the AL (green, no measures required); B) between the AL and the TLV (yellow, measures recommended); and C) greater than the TLV (red, measures required).
Table 1. The Borg CR-10 scale used by the 11 assemblers to estimate forearm/hand exertion.
2.3. Goniometry
Biaxial flexible electro-goniometers (SG75; Biometrics Ltd, UK) were used to record wrist velocities. The electro-goniometers were mounted bilaterally over the wrists, one block on the third metacarpal bone and the other at the midline between the radius and ulna. The reference position (0° flexion and deviation) was defined with the forearm and hand resting on a table with the elbow joint flexed at 90°. The hand was adjusted so that the third metacarpal bone of the middle finger and the midline between the forearm bones pointed along the same reference line, with a sight line between the ulna and third metacarpal bone [Citation17]. The signals were stored on a 2-GB memory card in a Mobi-8 data logger (TMS International, the Netherlands), worn by the assembler, at a sampling rate of 128 Hz. After the measurement, the data were transferred to a computer for further processing, quality assurance and analysis in the software suite EMINGO, developed by the Division of Occupational and Environmental Medicine in Lund, using MATLAB version 2019b.
2.4. Surface electromyography
The extensor carpi radialis longus and brevis in the forearm were located by palpation, while the subject performed a voluntary contraction with the forearm pronated [Citation18]. The skin was cleaned with alcohol and rubbed with an emery cloth. Two Ag/AgCl electrodes (Neuroline 720; Ambu, Denmark) were applied perpendicular to the muscle fibres, on the skin above the most prominent part of the muscles, i.e., at approximately one-third of the distance from the lateral epicondyle to the styloid process. The active diameter of the electrodes was 6 mm, and the centre-to-centre distance was 22 mm. Both muscles were covered when using this centre-to-centre distance, which means that one common output signal from the two muscles was obtained, i.e., longus and brevis were analysed as one muscle. The signals were amplified, filtered (10–400 Hz) and sampled at a rate of 2048 Hz, and were stored on a 2-GB memory card in the Mobi-8 data logger. Each assembler performed three maximal voluntary contractions using a Jamar dynamometer (Sammons Preston, USA) with the elbow flexed at 90° and with no support of the forearm or hand. The highest MVE obtained during the maximal voluntary contractions was later used for normalization of the electrical activity during work (%MVE). After the measurement, the data were transferred to a computer for further processing and analysis in EMINGO. Initially, the sEMG signals were digitally band-pass filtered (30–400 Hz) to remove electrical signals from the heart, and were notch filtered (mains frequency, 50 Hz and all harmonics). The root mean square value was calculated for periods of 0.125 s, and the noise was subtracted in a power sense [Citation19]. A moving window with a width of 0.5 s was used to find the highest MVE [Citation19,Citation20].
2.5. Considerations made for calculation of the consistency between the methods
The ACGIH TLV for hand activity contains two dimensions (hand activity and estimated exertion), while each of the two proposed action levels contains only one dimension (either wrist velocity or forearm muscular load). This complicates comparisons between the results obtained with the two methods. However, as both methods have been defined as risk estimators for the development of WMSDs in the forearm/hand when their limit values are exceeded (the ACGIH TLV and the proposed action levels of either wrist velocity or forearm muscular load, based on objective measurements), investigation of the consistency between the methods are of high value. Consistency was defined as the case when the ACGIH TLV and one or both proposed action levels for wrist velocity or forearm muscular load were exceeded.
2.6. Data analysis
Due to technical problems, objective data were lost for 11 of the 66 sub-cycles (five for wrist velocities and six for forearm muscular load). In addition, the sEMG data from one assembler were excluded due to a methodological error (six sub-cycles). Objective data were therefore obtained for 49 sub-cycles. The 50th percentile of the angular velocity distribution and the 90th percentile of the amplitude distribution (electrical activity during work, expressed as %MVE) were calculated for each participant.
2.7. Statistical analysis
Statistical analysis was carried out with SPSS version 24.0. Spearman’s ρ was used to calculate correlations between expert assessments of hand activity and recorded wrist velocities, and between self-estimated exertion and recorded muscular load. p < 0.05 was considered statistically significant. The weighted κ was used for calculation of the inter-rater reliability between separate experts regarding the ACGIH TLV for hand activity (expert 1 versus expert 2 in pair A, and expert 3 versus expert 4 in pair B). A κ value between 0.10 and 0.20 was considered slight agreement, between 0.21 and 0.40 fair agreement, between 0.41 and 0.60 moderate agreement, between 0.61 and 0.80 good agreement and between 0.81 and 1.00 excellent agreement [Citation21,Citation22]. The percentage of absolute agreement between the experts within the two pairs was also calculated. A value between 75 and 90% was considered acceptable agreement [Citation23].
For comparisons between the ACGIH TLV for hand activity and objective measurements of wrist velocity and forearm muscular load, the results of the sub-cycles obtained with the two methods were divided into exposure categories. For the ACGIH, the results were divided into the three categories mentioned earlier: A) green, B) yellow and C) red. As the proposed action levels do not have a yellow exposure category, wrist velocity and forearm muscular load were grouped separately into A) green (below the proposed action level) and B) red (above the proposed action level). The action level for wrist velocity was set at 15°/s, as the assemblers used vibrating tools during a considerable amount of their work time. The results of those sub-cycles that were categorized as belonging to the yellow exposure category were excluded from these comparisons. The percentage of absolute agreement between the methods was then calculated. Finally, by assuming the ACGIH TLV for hand activity to be the reference standard, the accuracy of the two proposed action levels was derived by calculating sensitivity (true positive rate) and specificity (true negative rate) values.
3. Results
3.1. ACGIH TLV for hand activity
The combination of HAL and self-estimated exertion in five (less than 10%) of the 66 sub-cycles was categorized into the green exposure category (below the AL), 14 (about 20%) were categorized into the yellow category (between the AL and the TLV) and 47 (about 70%) were categorized into the red category (exceeding the TLV). The lowest value used on the HAL 0–10 scale was 2 and the highest was 8. The most frequent value was 6, and at this level the wrist velocities varied between 13 and 40°/s. The lowest and highest values used on the Borg CR-10 scale were 0 and 7, respectively. The most frequent value was 3, and at this level the muscular load varied between 8 and 34%MVE.
3.2. Goniometry and sEMG
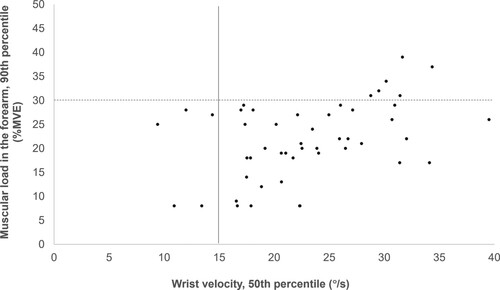
The results for wrist velocity and the forearm muscular load for the 49 sub-cycles are presented in Figure . Forty-four (90%) of the values exceeded the proposed action level for wrist velocity, and six (12%) of these also exceeded the proposed action level for the muscular load. Neither of the two proposed action levels were exceeded in five (10%) of the sub-cycles studied.
Figure 2. Median wrist velocity versus the muscular load (90th percentile) of the right forearm and hand in 49 sub-cycles (three to six sub-cycles per assembler) of assembling work (N = 11). Note: Vertical solid line = proposed action level for wrist velocity (15°/s, as the assemblers used vibrating tools during a considerable amount of their work time); horizontal dashed line = proposed action level for the muscular load in the forearm (30%MVE). N = number of assembly workers; %MVE = percentage of the maximal electrical activity (obtained during the maximal voluntary contractions).
3.3. Correlations between subjective assessments and objective measurements
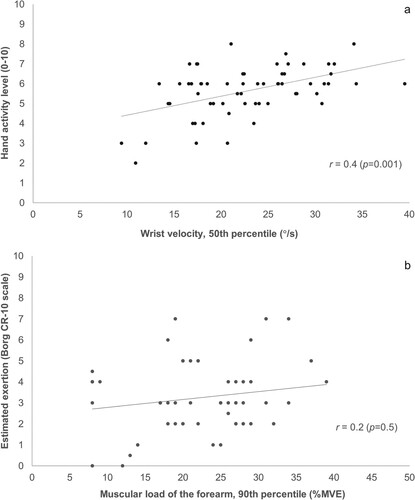
The correlation between HAL assessed by the experts and wrist velocity was 0.4 (p = 0.001) (Figure a). For estimated exertion (estimated by the assemblers) and the forearm muscular load, the correlation was 0.2 (p = 0.5) (Figure b).
Figure 3. Correlations between (a) HAL assessed by the experts and objectively measured wrist velocity, and (b) exertion estimated by the assemblers (see Table ) and objectively measured forearm muscular load for 49 sub-cycles (three to six sub-cycles per assembler). Notes: HAL = hand activity level; %MVE = percentage of the maximal electrical activity (obtained during the maximal voluntary contractions).
3.4. Inter-rater reliability in the experts’ assessments of ACGIH TLV for hand activity
The ACGIH TLV for hand activity assessed by the two separate expert pairs (experts 1 and 2 in pair A, and experts 3 and 4 in pair B) including the self-estimated exertion, colour coded into the exposure categories green, yellow and red, is presented in Table . The agreement was 75% for pair A (18 of 24 assessments) and 78% for pair B (seven of nine assessments). The inter-rater reliability between the experts was κw = 0.50 for pair A, 95% confidence interval (CI) [0.17, 0.84] and κw = 0.68 for pair B, 95% CI [0.31, 1.0].
Table 2. The ACGIH TLV for hand activity for 66 sub-cycles (six sub-cycles per assembler) at three different workstations (A, B and C). The assessments were carried out in two pairs of experts, 24 sub-cycles each for experts no. 1 and 2 and 9 sub-cycles each för experts no. 3 and 4. (N = 11)
3.5. Consistency between the TLV and proposed action levels
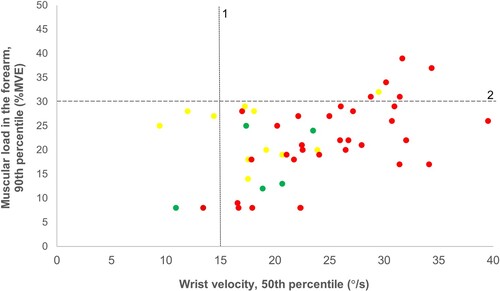
In 32 of 38 sub-cycles (11 of the 49 sub-cycles were excluded, as they were assigned to the ACGIH’s yellow exposure category), both the TLV and the proposed action level for wrist velocity were exceeded (Figure ). In five of the 32 sub-cycles, the proposed action level for forearm muscular load was also exceeded. None of the limits was exceeded in one of the 38 sub-cycles. The TLV was not exceeded (green category) in four of the 38 sub-cycles, while the proposed action level for wrist velocity was exceeded (but not the proposed action level for forearm muscular load). Finally, the TLV was exceeded in one of the sub-cycles, but neither of the proposed action levels was exceeded.
Figure 4. Median wrist velocity versus muscular load (90th percentile) of the right forearm and hand in 49 sub-cycles (three to six sub-cycles per assembler) of assembling work. Note: Data are colour-coded according to the exposure categories of the American Conference for Governmental Occupational Hygienists (ACGIH) threshold limit value (TLV) for hand activity. Data assigned to the yellow exposure category of TLV were excluded from the calculations of the consistency between the TLV and proposed action levels as there is no analogous (yellow) category for the proposed action levels. 1 = proposed action level for wrist velocity (15°/s, as the assembler used vibrating tools during a considerable amount of their work time); 2 = proposed action level for the muscular load in the forearm (30%MVE). %MVE = percentage of the maximal electrical activity (obtained during the maximal voluntary contractions). The full colour version of this figure is available online.
3.5.1. Absolute agreement
The absolute agreement between the TLV and the proposed action level for wrist velocity was 87%, while that between the TLV and the proposed action level for forearm muscular load was 26%.
3.5.2. Sensitivity and specificity
If the ACGIH TLV for hand activity is assumed to be the reference standard, the sensitivity for the proposed action level for wrist velocity was 97% and the specificity was 20%. The sensitivity for the proposed action level for the forearm muscular load was 15% and the specificity was 100%.
4. Discussion
The results of this study show that the TLV and the proposed action level for wrist velocity agreed to a large extent. However, the agreement between the TLV and the proposed action level for the forearm muscular load was low.
Concerning the two separate dimensions of the ACGIH TLV for hand activity, the correlation between assessed hand activity and objectively measured wrist velocity was statistically significant. However, no such correlation was found between self-estimated exertion and objectively measured forearm muscular load.
4.1. Correlations between subjective assessments and objective measurements
There was a large variation in the objectively measured wrist velocities for the various ratings on the HAL 0–10 scale, as can be seen for e.g., the rating value 6 (steady motion/exertion; infrequent pauses), which corresponded to measured velocities of 13–40°/s. This demonstrates that it is difficult to assess wrist velocities by observation [Citation24,Citation25]. However, the correlation between assessed hand activity and measured wrist velocity was statistically significant. Thus, we believe that the HAL 0–10 scale may be useful for screening of ergonomic exposure. However, objective measurements should be carried out for a detailed description of wrist velocity.
Self-estimated exertion is very individual, with a high variance between subjects depending on factors such as personality, sensitivity and pain. For example, Balogh et al. [Citation26] reported that subjects with pain rated their exertion higher than those without pain, even though objective measurements showed a lower load in those with pain. Furthermore, self-estimations have been reported to have lower precision than objective measurements and observational video analysis [Citation24]. In the present study, no correlation was found between self-estimated exertion and measured forearm muscular load, which may be explained by the factors mentioned earlier. How the instructions are given may also influence the outcome of the self-estimation, which in turn may affect the correlation. In this study, the assemblers were carefully instructed how to estimate their exertion in their forearms during the sub-cycle. Thus, the instructions were clear, and we do not think that this contributed to the low correlation. To obtain reliable results regarding exertion during work, objective measurements are preferred.
4.2. Inter-rater reliability in the experts’ assessments of the ACGIH TLV for hand activity
Although no correlation was found between self-estimated exertion and the forearm muscular load in this study, the inter-rater reliability in the two pairs of experts in assessing the ACGIH TLV for hand activity was high (expressed in terms of green, yellow and red). This may be partly explained by the fact that the assemblers estimated the exertion in their arms and hands similarly on the two occasions (only four of 33 pairwise sub-cycles differed by more than one unit on the Borg CR-10 scale; Table ), regardless of the actual workload measured using sEMG. Therefore, the two ratings of self-estimated exertion for each assessment did not influence which exposure category it was assigned to.
The inter-rater reliability of the ACGIH TLV for hand activity in this study showed moderate agreement for one pair of experts and good agreement for the other pair, which can be regarded as acceptable reliability. Similar levels of agreement between experts have been reported for different observational methods in previous studies [Citation27,Citation28].
4.3. Consistency between the TLV and proposed action levels
4.3.1. Agreement
When using the ACGIH TLV for hand activity as the reference standard, our findings showed that the proposed action level for wrist velocity overestimated the workload in four of 38 (10%) sub-cycles and underestimated the workload in one, compared to the TLV. However, the TLV and the proposed action level for wrist velocity were consistent as both exceeded their respective limit in almost 90% of the sub-cycles. This implies that the proposed action level for wrist velocity has been set at a level that agrees well with the TLV.
The agreement between the ACGIH TLV and the proposed action level for forearm muscular load was low. This could partly be explained by the low correlation between the self-estimated exertion and the measured forearm muscular load. The assembly tasks in the current study most likely activated not only the forearm extensor muscles, but also the forearm flexor muscles. We speculate that this probably was to such a large proportion that the recorded muscular load (forearm extensors) was not fully representative for the actual load. Thus, the proposed action level for the forearm muscular load was not consistent with the TLV.
4.3.2. Sensitivity
The sensitivity of the proposed action level for wrist velocity was high (97%). A high sensitivity is important for preventive purposes, as it is desirable to identify all of the individuals in a workplace who are at risk of developing WMSDs. However, neither the TLV nor the proposed action level for wrist velocity define a definitive boundary between safe and dangerous workload and are not statutory limits for workloads. Furthermore, individual and organizational factors should be considered as they are well-known risk factors for WMSDs [Citation29,Citation30].
4.4. Methodological considerations
To the best of our knowledge, the present study is the first in which quantitative limit values (proposed action levels) of physical workload on the forearm and wrist have been compared with an observation method such as the ACGIH TLV for hand activity. The results indicate that the TLV and the proposed action level for wrist velocity are highly consistent.
The main limitation of this study was the small number of assemblers and of sub-cycles. This probably affected the correlation coefficient between assessed hand activity and measured wrist velocity, which was 0.4. With more participants and sub-cycles, the statistical power would be stronger, which may result in a higher correlation coefficient. Despite this, the results showed a statistically significant correlation between assessed hand activity and measured wrist velocity, and an acceptable agreement between the TLV and the proposed action level for wrist velocity. However, additional studies are needed to confirm the results.
There was uneven number of women and men in the current study. However, we do not think this had a negative influence on the results, as the muscular activity during work was normalized to each participant´s own MVE. Also, the self-estimated exertions were analysed independently of each other.
The verbal anchors of the translated HAL 0–10 scale made it easier for the experts to use the scale during assessments in the field. The translation from English to Swedish may have caused a slightly different meaning between the two versions. However, we have no reason to believe that these small differences affected the results.
The ranges of the time for the different sub-cycles were quite wide because of their content of different amount of work and a slightly different work pace and work order among the assemblers. However, we believe that this heterogeneity did not influence the results since the sub-cycles were assessed separately. One of the sub-cycles had a rather short cycle time. Despite this, we considered it to be sufficient for making a reasonable estimate of the hand activity, and it was therefore included in the analysis.
The results of the ACGIH TLV for hand activity is grouped into three categories (green, yellow and red) to classify the risk of developing WMSDs, while the proposed action levels are grouped into two categories (below and above the proposed action level). Classification into green, yellow and red categories is often used to categorize risk levels in observational methods [Citation31,Citation32]. This facilitates the identification of work tasks with lower and higher risks of WMSDs, which is useful when priorities must be made between different measures. A future development of the proposed action levels may be to establish a third category below the proposed action levels, which would correspond to the yellow exposure category of risk levels used in observational methods. This would provide opportunities to further distinguish between lower and higher risks of developing WMSDs for quantitative measures. Despite the difference between the two methods, we believe it is of value to compare these risk assessment methods.
5. Conclusions
The results of the present study indicate that the proposed action level for wrist velocity is highly consistent with the TLV. It is set at a level that agrees well with the TLV and is a useful tool for risk assessment of harmful exposure in the forearm, wrist and hand. Furthermore, the hand activity and recorded wrist velocities showed a statistically significant correlation, while no such correlation was found between self-estimated exertion and recorded muscular load. Both the ACGIH TLV for hand activity and the proposed action level for wrist velocity showed that most of the work tasks in the workplace investigated imply a risk of developing WMSDs in the forearm, wrist and hand.
Acknowledgements
The authors wish to thank the assemblers and the company for agreeing to participate in this study.
Disclosure statement
No potential conflict of interest was reported by the authors.
Data availability statement
The data that support the findings of this study are available from the corresponding author on reasonable request.
Additional information
Funding
References
- Nordander C, Ohlsson K, Åkesson I, et al. Exposure–response relationships in work-related musculoskeletal disorders in elbows and hands – a synthesis of group-level data on exposure and response obtained using uniform methods of data collection. Appl Ergon. 2013;44(2):241–253. doi:10.1016/j.apergo.2012.07.009
- van Rijn RM, Huisstede BM, Koes BW, et al. Associations between work-related factors and the carpal tunnel syndrome – a systematic review. Scand J Work Environ Health. 2009;35(1):19–36. doi:10.5271/sjweh.1306
- ACGIH. TLVs and BEIs. Cincinnati (OH): Signature Publications; 2019.
- Eliasson K, Palm P, Nyman T, et al. Inter- and intra-observer reliability of risk assessment of repetitive work without an explicit method. Appl Ergon. 2017;62:1–8. doi:10.1016/j.apergo.2017.02.004
- Kjellberg K, Lindberg P, Nyman T, et al. Comparisons of six observational methods for risk assessment of repetitive work – results from consensus assessment. In: Lindgaard G, Moore D, editors. Proceedings of 19th Triennial Congress of the IEA; Aug 9–14; Melbourne: International Ergonomics Association; 2015.
- Forsman M. Ergonomic risk assessments – a need for reliable and attractive methods. Kuopio, Finland: Faculty of Health Sciences; 2016. (Reports and Studies in Health Sciences; 22).
- Rislund C, Hemphälä H, Hansson G-Å, et al. Evaluation of three principles for forklift steering: effects on physical workload. Int J Ind Ergon. 2013;43(4):249–256. doi:10.1016/j.ergon.2013.04.011
- Colim A, Pereira D, Lima P, et al. Designing a user-centered inspection device’s handle for the aircraft manufacturing industry. Appl Sci. 2023;13(20):1–18. doi:10.3390/app132011584
- Åkesson I, Balogh I, Hansson GÅ. Physical workload in neck, shoulders and wrists/hands in dental hygienists during a work-day. Appl Ergon. 2012;43(4):803–811. doi:10.1016/j.apergo.2011.12.001
- Nordander C, Hansson G-Å, Ohlsson K, et al. Exposure–response relationships for work-related neck and shoulder musculoskeletal disorders – analyses of pooled uniform data sets. Appl Ergon. 2016;55:70–84. doi:10.1016/j.apergo.2016.01.010
- Balogh I, Arvidsson I, Björk J, et al. Work-related neck and upper limb disorders – quantitative exposure–response relationships adjusted for personal characteristics and psychosocial conditions. BMC Musculoskelet Disord. 2019;20(1):139. doi:10.1186/s12891-019-2491-6
- Arvidsson I, Dahlqvist C, Enquist H, et al. Action levels for the prevention of work-related musculoskeletal disorders in the neck and upper extremities: a proposal. Ann Work Exposures Health. 2021;65(7):741–747. doi:10.1093/annweh/wxab012
- Latko WA, Armstrong TJ, Foulke JA, et al. Development and evaluation of an observational method for assessing repetition in hand tasks. Am Ind Hyg Assoc J. 1997;58(4):278–285. doi:10.1080/15428119791012793
- Gunnarsson A-B, Wersäll M. Hand Arm Risk Assessment Method (HARM) – evaluation of a method for assessment of biomechanical exposure of the upper limbs when performing manual tasks as well as its suitability within work environment inspection [master`s thesis]. Stockholm: KTH Royal Institute of Technology; 2011.
- Gunnar B. Psychophysical scaling with applications in physical work and the perception of exertion. Scand J Work Environ Health. 1990;16:55. doi:10.5271/sjweh.1815
- Yung M, Dale AM, Kapellusch J, et al. Modeling the effect of the 2018 revised ACGIH® hand activity threshold limit value® (TLV) at reducing risk for carpal tunnel syndrome. J Occup Environ Hyg. 2019;16(9):628–633. doi:10.1080/15459624.2019.1640366
- Simonsen JG, Dahlqvist C, Enquist H, et al. Assessments of physical workload in sonography tasks using inclinometry, goniometry, and electromyography. Saf Health Work. 2018;9(3):326–333. doi:10.1016/j.shaw.2017.08.007
- Dahlqvist C, Nordander C, Granqvist L, et al. Comparing two methods to record maximal voluntary contractions and different electrode positions in recordings of forearm extensor muscle activity: refining risk assessments for work-related wrist disorders. Work. 2018;59:231–242. doi:10.3233/WOR-172668
- Hansson G-Å, Asterland P, Skerfving S. Acquisition and analysis of whole-day electromygraphic field recordings. In: Hermens HJ, Hägg G, Freriks B, editors. Proceedings of the Second General SENIAM (Surface EMG for Non-Invasive Assessment of Muscles) Workshop; 1997 Jun 13–14. Stockholm: Roessingh Research and Development; 1997. p. 19–27.
- Jensen C, Vasseljen Jr O, Westgaard RH. Estimating maximal EMG amplitude for the trapezius muscle: on the optimization of experimental procedure and electrode placement for improved reliability and increased signal amplitude. J Electromyogr Kinesiol. 1996;6(1):51–58. doi:10.1016/1050-6411(94)00012-3
- Cohen J. Weighted kappa: nominal scale agreement provision for scaled disagreement or partial credit. Psychol Bull. 1968;70(4):213–220. doi:10.1037/h0026256
- Warrens MJ. Conditional inequalities between Cohen’s kappa and weighted kappas. Stat Methodol. 2013;10(1):14–22. doi:10.1016/j.stamet.2012.05.004
- Graham M, Milanowski A, Miller J. Measuring and promoting inter-rater agreement of teacher and principal performance ratings. Online Submission. 2012:1–33.
- Spielholz P, Silverstein B, Morgan M, et al. Comparison of self-report, video observation and direct measurement methods for upper extremity musculoskeletal disorder physical risk factors. Ergonomics. 2001;44(6):588–613. doi:10.1080/00140130118050
- De Looze MP, Toussaint HM, Ensink J, et al. The validity of visual observation to assess posture in a laboratory-simulated, manual material handling task. Ergonomics. 1994;37(8):1335–1343. doi:10.1080/00140139408964912
- Balogh I, Orbaek P, Ohlsson K, et al. Self-assessed and directly measured occupational physical activities – influence of musculoskeletal complaints, age and gender. Appl Ergon. 2004;35(1):49–56. doi:10.1016/j.apergo.2003.06.001
- Oliv S, Gustafsson E, Baloch AN, et al. The quick exposure check (QEC) – inter-rater reliability in total score and individual items. Appl Ergon. 2019;76:32–37. doi:10.1016/j.apergo.2018.11.005
- Dohyung K. Systematic comparison of OWAS, RULA, and REBA based on a literature review. Int J Environ Res Public Health. 2022;19(595):1–23.
- Tirloni AS, Reis DCD, Borgatto AF, et al. Association between perception of bodily discomfort and individual and work organisational factors in Brazilian slaughterhouse workers: a cross-sectional study. BMJ Open. 2019;9(2):e022824. doi:10.1136/bmjopen-2018-022824
- Singh P, Bhardwaj P, Sharma SK, et al. Association of organisational factors with work-related musculoskeletal disorders and psychological well-being: a job demand control model study. Theor Issues Ergon Sci. 2022: 1–14.
- Rose LM, Eklund J, Nord Nilsson L, et al. The RAMP package for MSD risk management in manual handling – a freely accessible tool, with website and training courses. Appl Ergon. 2020;86:1–11.
- Chiasson M-È, Imbeau D, Aubry K, et al. Comparing the results of eight methods used to evaluate risk factors associated with musculoskeletal disorders. Int J Ind Ergon. 2012;42(5):478–488. doi:10.1016/j.ergon.2012.07.003