
Nearly 3 billion people rely on solid fuel combustion to meet basic domestic energy needs (Rehfuess, Mehta, & Pruss-Ustun, Citation2006). Many households use traditional cookstoves to meet these energy needs, resulting in extremely high indoor air pollution concentrations. Household air pollution from biomass and coal combustion accounts for an estimated 3.9 million premature deaths per year, representing about 4.8% of the global disease burden (Smith et al., Citation2014). Improved, cleaner-burning stove designs have the potential to substantially reduce household air pollution exposures and improve health (Albalak, Bruce, McCracken, Smith, & De Gallardo, Citation2001; Bruce et al., Citation2004; Ezzati & Kammen, Citation2002; Smith, Citation2002). However, there are few randomized intervention trials, and previous stove intervention studies focused on health impacts have been plagued by low improved stove adoption and sustained use (Perez-Padilla, Schilmann, & Riojas-Rodriguez, Citation2010; Romieu et al., Citation2009), severely limiting interpretations of these studies. Without addressing the ongoing social and behavioral process of adoption and stove use, the full benefits of stove dissemination programs cannot be realized or estimated (Pine et al., Citation2011; Rehfuess, Puzzolo, Stanistreet, Pope, & Bruce, Citation2014; Ruiz-Mercado, Masera, Zamora, & Smith, Citation2011; Troncoso, Castillo, Masera, & Merino, Citation2007).
Several excellent reviews have compiled detailed descriptions of enablers and barriers to stove adoption across a wide variety of cultural and geographical scenarios (Lewis & Pattanayak, Citation2012; Puzzolo, Stanistreet, Pope, Bruce, & Rehfuess, 2013; Rehfuess et al., Citation2014). Furthermore, Puzzolo and colleagues (Citation2013) clearly outlined the complexity involved with promoting the use of improved fuels or stoves and the need to consider a broad range of factors, or constructs, influencing the likelihood of sustained adoption (i.e., fuel and technology characteristics; household and setting characteristics; knowledge and perceptions; financial, tax and subsidy aspects; market development; regulation, legislation, and standards; and programmatic and policy mechanisms). Keeping in mind that the behavior change process is dynamic, it is important to note that these enablers and barriers may interact at multiple levels (e.g., at the individual and community level) as well as at various stages of change (e.g., intent to change behavior, initial behavior change, and/or sustained behavior change; Rehfuess et al., Citation2014; Ruiz-Mercado et al., Citation2011). Given these recent contributions to the literature, this commentary is not meant to be a comprehensive review of behavior change theory, even within the cookstove research arena. Building on this emerging body of work, the objective of this commentary is to propose that behavior change methods and theory also need to have a central role in epidemiologic intervention studies evaluating the health effects of cleaner-burning cookstoves—in the promotion of behavioral change to maximize the health benefit and in the accurate evaluation of the health impact of the intervention.
Given the immense public health impact and the recent increase in efforts to fund large-scale dissemination programs of cleaner-burning cookstoves (Martin, Glass, Balbus, & Collins, Citation2011), the current research paradigms need to be challenged. It is clear that behavior change is a critical piece of the puzzle. Much of the focus has been placed on developing methods to achieve complete and sustained behavior change with respect to stove use, often with the goal of reaching a target guideline for pollutant concentrations (e.g., World Health Organization air quality guidelines). However, our current knowledge regarding the health benefits of cleaner-burning cookstove programs is severely limited, and the answers are inherently dependent on our ability to describe behavior. Exposure-response is a complex continuum with much uncertainty; we essentially ask the question, “Where do we expect people to land on the exposure-response curve after a new stove is introduced?” To understand expected health benefits for a particular stove program we need to accurately predict reductions in exposure, which will vary depending on behaviors surrounding the use of the stove.
Proposed Research Agenda for Health-Related Interventions
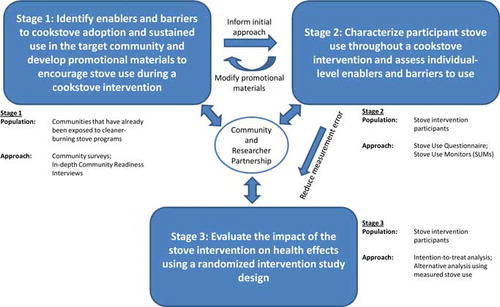
To change the paradigm of health-related cookstove research, a proposed agenda to augment traditional health-based interventions is outlined in Figure . Individual- and community-level barriers to and enablers of initial improved stove adoption and sustained use can be characterized among families that have already participated in stove dissemination programs and that represent the target population for the intervention study (Stage 1). Community-specific promotional strategies can then be developed to encourage sustained adoption for the proposed intervention, thus maximizing its impact. Once the intervention has begun (Stages 2 and 3), it is imperative to systematically evaluate behavior change to explain the valid relationship between stove use and changes in health. Figure provides a schematic of an agenda for an intervention that represents the interconnected relationships between methodological approaches typically used in behavior change science as well as environmental epidemiology, all in a community-engaged approach. The framework is intentionally broad in scope (i.e., a generic representation with examples of various methodological approaches) to provide a roadmap to systematically describe enablers/barriers of stove use and provide a knowledge base from which to compare health impact results across studies, populations, and improved stove types.
Fig. 1 Proposed community-engaged research agenda to augment typical health-related cookstove interventions with the systematic evaluation of enablers and barriers of stove use in order to promote and accurately measure changes in behavior.
Community-engaged approaches provide promising solutions to enhance scientifically valid intervention methods by building community and researcher partnerships (Horowitz, Robinson, & Seifer, Citation2009; O'Fallon & Dearry, Citation2001). For example, a community and researcher partnership can help to inform all stages of the given project, from identifying study participants and developing relevant questions regarding stove use and cooking preferences, to informing and creating promotional materials to promote sustained behavior change, as well as participating in the dissemination of results. These partnerships may be an especially useful approach for working with underserved communities that have typically not been involved in determining how community interventions are likely to be most effective (Israel et al., Citation2005; Schulz et al., Citation2005).
Although several approaches may be deemed appropriate, a few examples are now presented to help add clarity to the broadly defined agenda. In Stage 1, a community-based survey may be used to assess enablers and barriers to stove use among local families that have already received (or have had the opportunity to receive) improved stoves through previous projects disseminating a similar style of stove (as proposed for the intervention). These households likely will be at different stages of the behavior change process (e.g., initial acceptance after receipt of the new stove but has returned to using a traditional stove, or sustained adoption of the new stove). The advantage to this survey approach is that it is hypothesis generating (i.e., specific constructs of the behavior change process may be identified that can then be incorporated into the intervention study), and it is a relatively efficient way to collect information from a large group of people. These surveys should typially collect information on demographics, hypothesized predictors of stove adoption (i.e., age, family size, education), preferences for cooking with new and traditional stoves, and should incorporate questions to account for the multiple levels of stove use observed across individuals in the community (e.g., Stages of Change theory; Prochaska, Diclemente, & Norcross, Citation1992). Alternatively, in-depth interviews designed to gain information regarding community-level enablers and barriers to stove use provide a complementary tool to the individual-level surveys. For example, the Community Readiness Model was developed at Colorado State University to give researchers a tool to address and describe a community's interest and willingness to try new prevention strategies (Edwards, Jumper-Thurman, Plested, Oetting, & Swanson, 2000; Kakefuda, Stallones, & Gibbs, Citation2008; Oetting et al., Citation1995; Stallones, Gibbs-Long, Gabella, & Kakefuda, Citation2008). The model combines an individual-level readiness model for health-related behavior change with community development theory (Prochaska et al., Citation1992) and it relies on interviews with a few key informants who know about the community and the target issue (Edwards et al., Citation2000). The Community Readiness Model can be applied specifically to a cookstove intervention by assigning one of the nine levels of readiness (no awareness, denial/resistance, vague awareness, preplanning, preparation, initiation, stabilization, confirmation and expansion, and high level of community ownership) to six community readiness dimensions: (a) existing efforts for the community to achieve widespread improved cookstove use, (b) the number of people aware of the improved stove option, (c) the groups that may provide key leadership involving decisions to adopt an improved stove, (d) the community climate to support the research, (e) the level of understanding concerning potential health risks associated with traditional cookstove use, and (f) the resources available at the community and household level to adopt the improved stoves. The use of a tool such as the Community Readiness Model is an ideal fit within this framework; the model provides a formal evaluation for identifying specific community-level barriers to new stove adoption as well as the community's readiness for the proposed intervention (Oetting, Jumper-Thurman, Plested, & Edwards, Citation2001). The goal is then to inform promotional materials and communication strategies specific to the community that will enhance the acceptance of the cleaner-burning stove technology for the intervention study.
Stages 2 and 3 are conducted among the actual intervention study participants (typically a smaller sample size than that involved in Stage 1). In Stage 2, individual-level enablers and barriers to stove use can be assessed by incorporating subjective (e.g., surveys, similar to those previously described) and objective measures of stove use. Because the use of questionnaires can be subject to bias (e.g., rely on participant memory and/or the participant's desire to respond as she thinks she should), the recent development of low-cost, reliable monitors (i.e., stove use monitors, SUMs) to measure continuous stove temperature provides an ideal tool to objectively evaluate stove adoption patterns (Ruiz-Mercado, Lam, Canuz, Davila, & Smith, Citation2008). It is important to integrate stove use questions (accuracy may be limited but information gleaned will provide more nuanced information and may be representative of a longer time period) and quantitative stove use monitoring (high accuracy during the relatively short period of measure but without information describing the user's behavioral choices) to develop a more accurate picture of the stove adoption process among intervention participants. In Stage 3, the intent-to-treat analysis typically conducted in randomized controlled trials is valuable because it provides the overall public health impact of an intervention program. However, the detailed stove use information (collected in Stage 2) can be incorporated as the independent variables in epidemiologic health models in order to give the researcher the ability to calculate valid estimates of the relationship between behavior (i.e., cookstove use) and changes in health resulting from the intervention. This framework allows participants to be described along the continuum of behavior change that minimizes the misclassification created when those receiving the intervention do not adopt the technology.
Conclusions
The solution to the massive global health problem surrounding traditional cookstove use is not just more efficient, cleaner-burning stoves; it is clear that advanced technology will not have an impact if the stoves are not sustainably used. Because sustained improved stove use over time drives all of the expected benefits of an intervention, the development of a community-engaged, systematic and generalizable framework to better understand the complex issues surrounding individual- and community-level enablers and barriers to sustained cookstove adoption is paramount. A broad principle of data collection relevant to community-engaged approaches is the use of multiple methods (qualitative and quantitative) to increase the types of information collected and enhance the validity of the conclusions by revealing areas of convergence and areas needing further investigation (Creswell, Klassen, Plano Clark, Clegg Smith, & the Specially Appointed Working Group, 2011; Ivankova, Creswell, & Stick, Citation2006). The combination of community surveys (quantitative and qualitative data), in-depth interviews (qualitative data, Community Readiness Model), and stove use monitors (quantitative data) provide a promising solution to assess and overcome barriers to sustained adoption (Ruiz-Mercado et al., Citation2011). Intentionally integrating these approaches, using rigorous quantitative research to assess the magnitude and frequency of constructs and rigorous qualitative research to explore the meaning and understanding of the constructs, is ideal for questions that call for real-life contextual understandings and multilevel perspectives (Creswell et al., Citation2011; Ivankova et al., Citation2006). Incorporating this agenda could equip epidemiologists with the tools to accurately describe health effects from intervention programs in terms that allow the exposure–response relationships to be defined based on actual stove use patterns. The ability to provide valid estimates of potential health improvements given known variability in stove use and adoption is necessary to inform policy makers and to enact change. This framework, which calls for the integration of behavior change communication and measurement with methods typically used in environmental epidemiology, provides a promising solution to impact the epidemiologic cookstove research field where other approaches, to date, have failed.
Related Research Data
References
- Albalak, R., Bruce, N., McCracken, J. P., Smith, K. R. & De Gallardo, T. (2001). Indoor respirable particulate matter concentrations from an open fire, improved cookstove, and LPG/open fire combination in a rural Guatemalan community. Environmental Science & Technology, 35, 2650–2655.
- Bruce, N., McCracken, J., Albalak, R., Schei, M. A., Smith, K. R., Lopez, V. & West, C. (2004). Impact of improved stoves, house construction and child location on levels of indoor air pollution exposure in young Guatemalan children. Journal of Exposure Analysis and Environmental Epidemiology, 14(Suppl 1), S26–S33.
- Creswell, J. W., Klassen, A. C., Plano Clark, V. L., Clegg Smith, K. & the Specially Appointed Working Group. (2011). Best practices for mixed methods research in the health sciences. Bethesda, MD: Office of Behavioral and Social Sciences Research, National Institutes of Health.
- Edwards, R. W., Jumper-Thurman, P., Plested, B. A., Oetting, E. R. & Swanson, L. (2000). Community readiness: Research to practice. Journal of Community Psychology, 28, 291–307.
- Ezzati, M. & Kammen, D. M. (2002). The health impacts of exposure to indoor air pollution from solid fuels in developing countries: Knowledge, gaps, and data needs. Environmental Health Perspectives, 110, 1057–1068.
- Horowitz, C. R., Robinson, M. & Seifer, S. (2009). Community-based participatory research from the margin to the mainstream: Are researchers prepared? Circulation, 119, 2633–2642.
- Israel, B. A., Parker, E. A., Rowe, Z., Salvatore, A., Minkler, M., Lopez, J., … Halstead, S. (2005). Community-based participatory research: Lessons learned from the Centers for Children's Environmental Health and Disease Prevention Research. Environmental Health Perspectives, 113, 1463–1471.
- Ivankova, N. V., Creswell, J. W. & Stick, S. L. (2006). Using mixed-methods sequential explanatory design: From theory to practice. Field Methods, 18, 3–20.
- Kakefuda, I., Stallones, L. & Gibbs, J. (2008). Readiness for community-based bicycle helmet use programs: A study using community-and individual-level readiness models. Journal of Health Psychology, 13, 639–643.
- Lewis, J. J. & Pattanayak, S. K. (2012). Who adopts improved fuels and cookstoves? A systematic review. Environmental Health Perspectives, 120, 637–645.
- Martin, W. J. 2nd, Glass, R. I., Balbus, J. M. & Collins, F. S. (2011). Public health. A major environmental cause of death. Science, 334, 180–181.
- O'Fallon, L. R. & Dearry, A. (2001). Commitment of the National Institute of Environmental Health Sciences to community-based participatory research for rural health. Environmental Health Perspectives, 109(Suppl 3), 469–473.
- Oetting, E. R., Donnermeyer, J. F., Plested, B. A., Edwards, R. W., Kelly, K. & Beauvais, F. (1995). Assessing community readiness for prevention. International Journal of the Addictions, 30, 659–683.
- Oetting, E. R., Jumper-Thurman, P., Plested, B. & Edwards, R. W. (2001). Community readiness and health services. Substance Use & Misuse, 36, 825–843.
- Perez-Padilla, R., Schilmann, A. & Riojas-Rodriguez, H. (2010). Respiratory health effects of indoor air pollution. International Journal of Tuberculosis and Lung Diseases, 14, 1079–1086.
- Pine, K., Edwards, R., Masera, O., Schilmann, A., Marron-Mares, A. & Riojas-Rodriguez, H. (2011). Adoption and use of improved biomass stoves in Rural Mexico. Energy for Sustainable Development, 15, 176–183.
- Prochaska, J. O., Diclemente, C. C. & Norcross, J. C. (1992). In search of how people change: Applications to addictive behaviors. American Psychologist, 47, 1102–1114.
- Puzzolo, E., Stanistreet, D., Pope, D., Bruce, N. & Rehfuess, E. (2013). Factors influencing the large-scale uptake by households of cleaner and more efficient household energy technologies. London, England: EPPI-Center, Social Science Research Unit, Institute of Education, University of London.
- Rehfuess, E., Mehta, S. & Pruss-Ustun, A. (2006). Assessing household solid fuel use: Multiple implications for the Millennium Development Goals. Environmental Health Perspectives, 114, 373–378.
- Rehfuess, E., Puzzolo, E., Stanistreet, D., Pope, D. & Bruce, N. G. (2014). Enablers and barriers to large-scale uptake of improved solid fuel stoves: A systematic review. Environmental Health Perspectives, 122, 120–130.
- Romieu, I., Riojas-Rodriguez, H., Marron-Mares, A. T., Schilmann, A., Perez-Padilla, R. & Masera, O. (2009). Improved biomass stove intervention in rural Mexico: Impact on the respiratory health of women. American Journal of Respiratory & Critical Care Medicine, 180, 649–656.
- Ruiz-Mercado, I., Lam, N., Canuz, E., Davila, G. & Smith, K. (2008). Low-cost temperature loggers as stove use monitors (SUMs). Boiling Point, 55, 16–18.
- Ruiz-Mercado, I., Masera, O., Zamora, H. & Smith, K. R. (2011). Adoption and sustained use of improved cookstoves. Energy Policy, 39, 7557–7566.
- Schulz, A. J., Kannan, S., Dvonch, J. T., Israel, B. A., Allen, A. 3rd, James, S. A., … Lepkowski, J. (2005). Social and physical environments and disparities in risk for cardiovascular disease: The healthy environments partnership conceptual model. Environmental Health Perspectives, 113, 1817–1825.
- Smith, K. R. (2002). Indoor air pollution in developing countries: Recommendations for research. Indoor Air, 12, 198–207.
- Smith, K. R., Bruce, N., Balakrishnan, K., Adair-Rohani, H., Balmes, J., Chafe, Z., … Rehfuess, E. (2014). Millions dead: How do we know and what does it mean? Methods used in the comparative risk assessment of household air pollution. Annual Review of Public Health, 35, 185–206.
- Stallones, L., Gibbs-Long, J., Gabella, B. & Kakefuda, I. (2008). Community readiness and prevention of traumatic brain injury. Brain Injury, 22, 555–564.
- Troncoso, K., Castillo, A., Masera, O. & Merino, L. (2007). Social perceptions about a technological innovation for fuelwood cooking: Case study in rural Mexico. Energy Policy, 35, 2799–2810.