
Abstract
Families in the Timor society of Indonesia have customarily used traditional houses, called Ume Kbubu, for confinement practices of a newborn baby and the mother during the first 40 days after birth. The practice, known as Sei (smoke) tradition, involves retaining heat, which is believed to foster healing, inside the house by continuously burning a wood burning stove. Exacerbated by inadequate ventilation in the traditional house, this practice results in poor indoor air quality and negatively affects the health of the mother and baby. Preliminary findings from a baseline study conducted in 2009 identified high levels of indoor air pollution in Ume Kbubu where mothers practiced the Sei tradition. Many respondents expressed that they suffered from respiratory health problems during the practice. On the basis of those results, a follow-up study was conducted in 2011 to develop and test a communication-focused behavior change intervention that would foster conversion of traditional houses into healthy Ume Kbubu and promote changes to traditional practices for better health outcomes. The study suggests that redesigning an Ume Kbubu house could promote better air quality inside the house and involving the community in the health intervention program led to positive changes in the Sei practice (i.e., decreasing the Sei period's length from 40 days to 4 days on average and attempting to reduce household air pollution). The study resulted in several recommendations in relation to sustained transformation to improve health behaviors.
Traditional beliefs and practices are common in various cultures around the world, including Indonesia. Out of 1,331 ethnic groups currently living in Indonesia, around 370 ethnicities are still practicing their local traditions (Agus, Horiuchi, & Porter, Citation2012; Swasono, Citation1998; Wulandari & Klinken, Citation2011). As early as 1961, anthropological studies described how a wide range of cultural ceremonies and traditions were performed by Javanese families in connection with weddings, pregnancy, and childbirth (Geertz, Citation1961).
In the Timor communities of Indonesia, one common postpartum tradition is the Sei or smoke tradition, in which new mothers and their newborn babies sit or lie above embers from biomass fuel (e.g., wood and agricultural crop residue) for up to 40 days (Prasodjo Citation2009, Citation2012). The community believes that childbirth causes a state of excess cold that depletes the mother's heat and blood, leaving her vulnerable to cold, wind, bad spirits, and disease. The Sei tradition is performed to restore the mother to a state of equilibrium. While participating in the Sei tradition, mothers are also encouraged to consume hot food and drinks, and are forbidden from eating particular foods such as seafood that may cause salty breast milk and stomachache. This practice of new mothers restoring their equilibrium and warmth during the postnatal period is similarly found in other Eastern and Southern Asian cultures and countries (e.g., Hoekman et al., Citation2008; Raven et al., Citation2007; Yamashita et al., Citation2014).
Sei, Household Air Pollution, and Health
The Sei tradition in the Timor community frequently takes place inside a traditional house, Ume Kbubu, which means a “rounded house” as reflected by its physical shape (see Figure ). In the past, the Ume Kbubu served as the main dwelling place for people to sleep, cook, store food, and save seeds for the planting season. Today, most people have moved to permanent houses, and the Ume Kbubu is now usually used for domestic activities (e.g., cooking, family gatherings, other social interactions), as a nurturing space for mothers, and for food storage (McWilliam, Citation2002; Windi & Whittaker, Citation2012).
Fig. 1 Ume Kbubu traditional house in Timor community, often called rumah bulat or “round house,” as reflected by its physical shape.
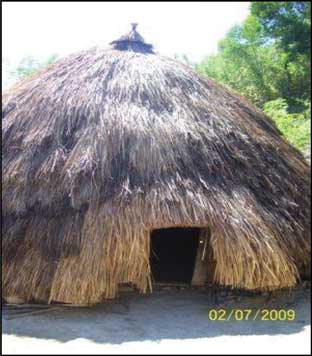
The house is generally made of rattan frames that are bent into a beehive-shape and covered with long, thick dried grasses, which extend to the ground. There is a small, low entrance door through which most people must bend to enter. It has an earthen-based floor, no windows or ventilation, and a central fireplace (Dima, Antariksa, & Nugroho, Citation2013). Owing to these characteristics, the house effectively traps heat from the burning of firewood that is used to provide warmth during cold weather and to protect food stocks (e.g., dry and preserve corns and grains). However, these conditions also lead to high levels of exposure to household air pollution for the mother and newborn baby during the Sei (Prasodjo, Citation2009).
Studies indicate that housing conditions have a significant influence on the health of the occupants (see, for example, Armstrong & Campbell, Citation1991; Bruce et al., Citation2014; Bruce, Perez-Padilla & Albalak, Citation2000; Krieger & Higgins, Citation2002; Lim et al., Citation2012). Furthermore, the effect of high levels of household air pollution on health is much higher among those who spend more time indoors than outdoors. Thus, mothers and young children who are confined indoors after childbirth in dwellings with high levels of household air pollution are a particularly vulnerable group (Smith et al., Citation2011; Warwick & Doig, 2004).
Globally, household air pollution is attributed to 3.5 to 4.3 million deaths annually (Bruce et al., Citation2014; Lim et al., Citation2012; World Health Organization, Citation2014) and accounts for 4% to 6% of the global burden of disease (Smith et al., Citation2011). The levels of household air pollution are usually higher among poor households in developing countries (Martin et al., Citation2013), particularly in rural areas as many of those families still rely on unprocessed biomass fuels for cooking and heating purposes (Smith et al., Citation2011). There is now strong evidence to link an increased risk of diseases such as acute lower respiratory infections in children, chronic obstructive pulmonary disease and cardiovascular disease in adults to exposure to high levels of household air pollution (Barnes, Citation2014; Smith et al., Citation2011).
The high exposure of women and children during postpartum traditions (e.g., Sei tradition in Timor) is likely to result in similar poor health outcomes as those linked to cooking related smoke. Yet, very little is known about the effectiveness and feasibility of programs to reduce household air pollution caused by the Sei. Even less is known about the potential for behavioral change to reduce household air pollution exposure (Barnes, Citation2014). According to Buntoro (Citation2006), the Ume Kbubu design may have contributed to the recent increases in acute lower respiratory infections reported by the Timor Tengah Selatan District Health Office (i.e., acute lower respiratory infections increased from 17.1% in 2002 to 26.1% in 2004). However, the study did not collect any robust evidence on the household air pollution levels inside the traditional house or on the health outcomes of mothers and newborns that performed the Sei practice.
In response to this knowledge gap, the aim of this study was to provide insight into a behavior change communication intervention designed to promote the construction and use of healthy adapted-traditional houses among Timor women in Indonesia following childbirth. The objectives of the study were as follows:
To qualitatively understand knowledge, attitudes and practices about the Sei tradition.
To describe the possible effect of the intervention on levels of household air pollution.
To describe the development of the behavior change communication intervention.
Theoretical Perspective
The Diffusion of Innovation theory (Rogers, Citation2003) provides a theoretical orientation for this study. The Diffusion of Innovation theory focuses on behaviors in terms of innovation rather than the individual as an agent of behavior change. The innovation here can be defined as an idea, practice or object perceived as new. It theorizes four main elements of behavior change, namely innovation, communication channels, time and social system (Rogers, Citation2003).
This study focused on promoting innovative healthy adapted-traditional houses through behavior change communication with the community. In this study, consultations with local institutions (e.g., policymakers, medical staff, community-based leaders, and other stakeholders who have been directly involved in the traditional behavior) were conducted for promotion, socialization, and advocacy. The stakeholders were facilitated and encouraged to discuss the Sei tradition and its implications for health issues. By involving the wider community in such a participatory action program, the prototype of a redesigned traditional house was expected to transform traditional houses into healthy Ume Kbubu, which have more adequate ventilation that will lead to better health.
In line with the Diffusion of Innovation theory, this intervention focused on relationships between people, their environment, and the technology that surrounds them to change behavior. The innovations were designed to be compatible with existing values, experiences and needs of potential adopters; easy to understand; testable by communities; and to have observable results. Rogers (Citation2003) argued that such innovations are evaluated “through the subjective valuations of near peers” (p. 36). Therefore, interpersonal communications played a key role in the intervention. This idea is especially relevant in the context of Timor society and in Indonesia in general, where social networks and a communal environment are particularly strong. Therefore, consultations with different stakeholders who influence and approve changes to cultural practices were necessary for diffusion of innovation to occur.
Method
Study Site
The Timor community is one of the indigenous groups in the eastern part of Indonesia. They are largely situated in the western part of Timor Island in the province of Nusa Tenggara Timur, covering four districts (Belu, Kupang, Timor Tengah Selatan, and Timor Tengah Utara) and one capital city (Kupang). The province of Nusa Tenggara Timur has relatively high poverty, child malnutrition, and maternal and child mortality rates. In 2010, the poverty level was 23% and the maternal mortality rate was 271 per 100,000 live births (Dinas Kesehatan Timor Tengah Selatan, 2010).
The Atoni, also known as the Dawan, make up the majority of the Timorese population, which was estimated at about 61% of the West Timor population (Windi & Whittaker, Citation2012). Many ethnic groups in Timor, especially among rural populations, are still following traditional practices to satisfy cultural patterning. The Sei tradition is largely practiced by rural communities in Timor Tengah Selatanand Timor Tengah Utara districts. The Boti tribe from the Dawan in Timor Tengah Selatan district is one of the groups who continue to routinely practice Sei tradition; families in major urban cities are less likely to participate in this practice.
Using purposive sampling, the district of Timor Tengah Selatan where the proportion of women practicing Sei tradition is high (more than 40%, based on the 2009 health report from Dinkes Nusa Tenggara Timur) was selected as the main study site. On the basis of the availability of time and resources, the subdistricts of Amanuban (Nulle) and Kie (where more than 40% of families had practiced the Sei tradition) were selected.
Study Design
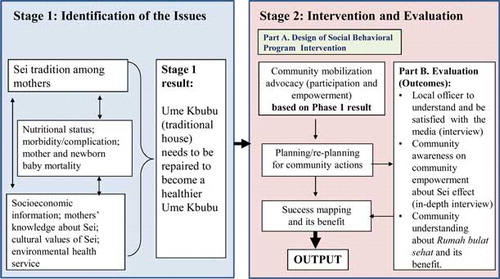
This study was part of a larger research project focused on morbidity and mortality among mothers who practice the Sei tradition. It was conducted in two stages: a baseline study in 2009 and a follow-up study in 2011–2012 (Prasodjo, Citation2009, Citation2012). The baseline study focused on the identification of health issues related to the Sei practice, while the follow-up study focused on evaluating the feasibility and possible effect of the behavior change intervention. A summary of study frameworks applied in the two stages is presented in Figure .
Fig. 2 Study framework in Stage 1 (baseline study) and Stage 2 (follow-up study).
Baseline Study
During the baseline study, a mixed methods approach (Creswell, Citation2003) was used to identify the issues related to Sei tradition. Quantitative structured questionnaires were conducted with 358 mothers who had practiced Sei tradition in the past year. The qualitative in-depth interviews and observation were carried out with 10 randomly selected mothers, of whom 5 were still practicing the Sei tradition at the time of the interview and the other 5 had completed the practice.
Household Air Pollution Monitoring
Household air pollution was monitored in the houses of the 5 mothers still practicing the Sei tradition, by measuring parameters of temperature, humidity, ventilation speed, natural light, dust particle matter (i.e., particulate matter less than 10 microns in aerodynamic diameter [PM10]), sulfur dioxide and nitrogen dioxide levels, and formaldehyde. The levels of PM10, sulfur dioxide, and nitrogen dioxide were measured according to the principals of national standard. For example, gravimetric analysis was used to measure suspended particulate matter (SPM) levels (Badan Standardisasi Nasional, 2005). Over 24 hours, the dust from indoor air was sucked on a preweighed filter with the aid of vacuum pump. The trapped dust in the filter was then analyzed to assess the elemental composition of the dust and the microbial composition. Detail measure principles for sulfur dioxide and nitrogen dioxide levels were evaluated by using pararosaniline and Griess Saltzman methods, respectively (Prasodjo, Citation2009, Citation2012). All collected data on household air pollution were compared with the limit levels as recommended in the national regulation (i.e., 829/Menkes/SK/VII/1999) that was adapted from the World Health Organization's guidelines on the requirements for a healthy house.
Follow-Up Study
The follow-up study included a behavioral change communication campaign through advocate programs in 2011, followed by an evaluation study in 2012.
Advocate Program
The advocate programs were developed by considering findings and recommendations obtained from the baseline study, particularly on the identification of health related issues caused by the Sei traditional practices among the community and the importance of social and cultural factors to the tradition. As reported in Prasodjo (Citation2009), respiratory health issues, household air pollution, and a reluctance to change Sei practices were all identified in the baseline study.
Behavior Change Communication Interventions
On the basis of findings from the baseline study, the follow-up study developed promotional and educational materials to improve community awareness on maternal health and the consequences of Sei traditional practice. Participatory action research was used to develop these behavior change communication materials and approaches. Participatory action research assists researchers and research participants (e.g., the community) to work together during the project to improve or change the condition or situation (Cohen, Greenwood & Harkavay, Citation1992). In this study, community stakeholders were gathered to discuss their understanding about traditional practices (including Sei tradition) and to find strategies for adopting healthier behavior. This involved interpersonal communication, intersectoral meetings, and coordination with local health departments, nongovernmental organizations, and community members (including families). Support was received from Nusa Tenggara Timur provincial health office, Timor Tengah Selatan district health office, women's society club (Sanggar Suara Perempuan), Puskesmas Kie and Puskesmas Nulle, village leaders, traditional births attendances, elders, and families in the study sites.
Consultations with local health staff identified health issues related to the Sei tradition, as well as potential solutions. Families and wider communities were also instrumental in designing the behavior change communication messages and channels, including designing the content and wording of media materials, such as brochures (see Figure ; an English translation is provided in Figure ). The information provided in the brochure aimed to encourage the community to be aware of health issues in relation to Sei tradition, particularly on the issues of respiratory infection, burns and mortality of mothers and newborns, and to promote construction of healthy traditional houses. The brochure contains three parts: (a) general information on short- and long-term effects of Sei (smoke) tradition on health, (b) specific information on the effects of Sei tradition on newborn babies’ health, and (c) specific information on the effects of Sei tradition on mother's health. A culturally appropriate representative picture and short messages in the local language were included to facilitate understanding. The messages included the following content [English translation]:
Fig. 3 A media communication to community about the Sei tradition and its consequences to health-related issues for mothers and children, in the Bahasa Indonesian language: the front (top panel) and back (bottom panel) sides of the brochure.
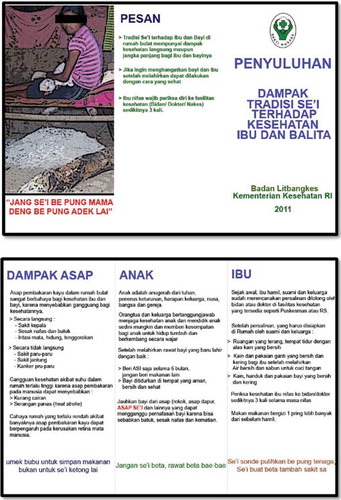
Fig. 4 Media communication to community about the Sei tradition and its consequences to health-related issues for mothers and children, translated from Bahasa Indonesian to English: the front (top panel) and back (bottom panel) sides of the brochure.
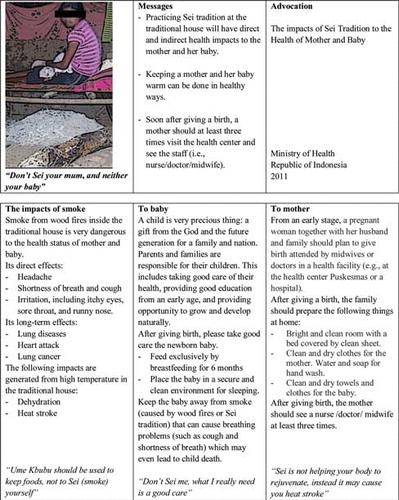
“Don't Sei your mum, and neither your baby.”
“Ume Kbubu should be used to keep foods, not to Sei (smoke) yourself.”
“Don't Sei me; what I really need is a good care.”
“Sei is not helping your body to rejuvenate, instead it may cause you heat stroke.”
After developing the promotional/educational materials, the next step was to identify the optimal channel to deliver the message. In-depth interviews and roundtable discussions with stakeholders revealed that fathers and grandmothers have the most influence over the mother and newborn within the family. Moreover, at the wider level the Timor communities have traditionally high levels of respect and trust for the priests, community leaders and health volunteers. Therefore, those stakeholders were chosen as the most effective channels for communication as a result of their ability to influence and approve changes to cultural practices in the community.
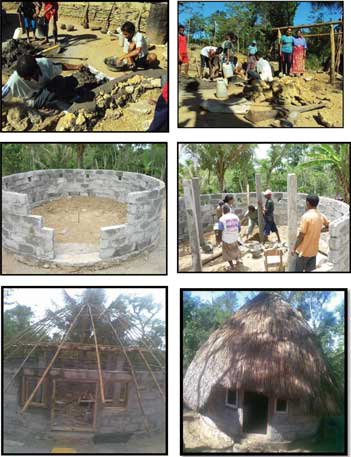
The second phase of the behavior change communication interventions aimed to promote the adoption of a healthy Ume Kbubu house in order to reduce the levels of household air pollution experienced in the traditional Ume Kbubu. The communities also helped design a healthy Ume Kbubu prototype (see Figure ). During a roundtable discussion, the local community decided to redesign the traditional house by building a new house rather than modifying an existing one. This was due to most families being initially reluctant to offer their traditional house to be redesigned. The community actively participated in redesigning this healthy house by taking into account earlier findings and recommendations obtained from the baseline study. In terms of its construction, this redesigned healthy Ume Kbubu has some differences with the old traditional house while at the same time retained several key elements. For example, the redesigned house has a better ventilation system with a proper high entrance door and windows. Yet, the redesigned house retains its main function as a place to protect or preserve food stocks. Families were encouraged to voluntarily accept a healthy Ume Kbubu and after being informed about the household air pollution levels inside their traditional house and the potential detrimental health impacts among mothers and newborns.
Fig. 5 Process of building a healthy Ume Kbubu in Timor Tengah Selatan District, Indonesia.
Evaluation Study
The evaluation was conducted 1 year after implementation in 2012 to assess the effectiveness of the behavior change communication interventions. As with the baseline, a mixed methods approach was used. Structured quantitative surveys were conducted with 202 women who had given birth in the last year. Of these, 81% (n = 163) had practiced Sei tradition and 19% (n = 39) had not. Information was collected on socioeconomic background, knowledge, and public health implications related to the traditional behaviors. For the qualitative study, in-depth interviews were conducted with 10 randomly selected mothers, of whom 5 were still practicing the Sei tradition at the time of interview and the other 5 had completed the practice (Prasodjo, Citation2012).
Similar with the baseline study, the follow-up study also collected information on household air pollution from four traditional houses and one prototype of a redesigned healthy Ume Kbubu for comparison purposes. In this case, the same methods as used in the baseline survey were applied. All houses belonged to mothers who were doing Sei tradition at the time of observation in 2012.
Data Analysis
A descriptive analysis was applied for quantitative data. For the qualitative analysis, this study applied a triangulation approach by using thematic analysis. The data were transcribed and then analyzed using a matrix system (Hansen, Citation2006)
Results
Knowledge, Attitudes, and Practice: Healthy Traditional Ume Kbubu
During the follow-up study, the in-depth interviews conducted with mothers and families showed that the majority of the participants perceived Sei tradition as an important element in Timorese traditional practice. It has been practiced for many generations by mothers after giving birth, and has continued due to the influence of parents and grandparents, and sometimes fear of consequences for not participating such as social stigma. Most participants believed that there are fundamental values attached to this tradition, which form a group symbol and kinship among family.
From the structured quantitative survey, there were some women (19%, n = 39) who had given birth in the past year but did not practice Sei tradition. These women indicated that marriage with other ethnic groups, medical conditions, or perceptions that the Sei tradition had no significant effect were their main reasons for not practicing the behavior.
All respondents who practiced Sei tradition stated that it is believed to speed up the recovery process after giving birth by shrinking swollen tissues, drying up the blood and preventing bleeding. This practice was also recognized as one way to achieve birth spacing, as it involves a separation period between mother and her partner. Moreover, the informants considered childbirth as a state of excess cold that required special treatments such as Sei or smoke and tatobi—hot water massage on the belly—as stated by four respondents:
… a mother who just gave a birth has cold condition, thus she has to do Sei tradition in order to keep her warm, besides the weather here is so cold, so it should be Sei. (Husband of FM1)
… doing Sei will make your body rejuvenate, while tatobi or taking hot water bath will make you feel fresh … (Mother FM2)
Yes Sei tradition is still carried out here, so here most of the hot water bath, the term is tatobi, use hot water that is placed in a large bowl, so that mothers get stronger faster and prevent the white blood not to rise. (Mother FM3)
After my wife giving a birth, I will keep her warm and prepare burning firewood. Here, if we didn't do Sei and tatobi then it will harm a mother's life. She could not use cold water for bathing because it could also harm her and even death, therefore Sei tradition should be done. We believe that cold condition could increase the white blood levels for a mother. (Husband of FM4)
Some health related consequences were reported by mothers who practiced the Sei tradition. Respondents who had practiced the tradition in the last year reported that mothers and their babies suffered from health respiratory problems (i.e., coughing and wheezing) during the practice.
… indeed I often had coughing during Sei practice, and my baby did too. However this is our tradition, so we had to do it anyway. (Mother FM5)
The majority of the interviewed mothers stayed in the traditional house Ume Kbubu for the Sei process. The main reason reported for this was the constant warmth from the fire pit inside the house that created a comfortable place for recovery. Another reason was the significant traditional function of the house in Timorese culture. A few mothers reported using alternative locations and procedures. Alternative locations included the Lopo (another Timorese traditional house) and the main regular house known as rumah besar. The differences between Ume Kbubu and Lopo houses are in their physical structures and functions. The Ume Kbubu has a roof with sides that touch the ground and is the main place where people cook, store food, and save seeds for the planting season. The Lopo has more open space with short walls, and mainly functions as a living room especially to greet and receive guests.
In the follow-up study, there was tentative evidence to suggest that behavior change communication in terms of diffusion of innovation of healthy traditional houses led to behavior change. More mothers practiced the Sei tradition in an alternative place such as rumah besar or Lopo in the follow-up compared to baseline. On average, the practicing mothers had done the Sei tradition for the duration of 21 days compared with 26 days at baseline. A small proportion of mothers (15%, n = 24) have started to do Sei tradition for only 4 days or less.
…since I heard about the dangers of Sei tradition to my baby's health, I did Sei tradition for my second child only for 4 days; I also understand what village midwife had already told me about the danger. (Mother FM5)
…I follow my priest who told us in church about the effect of 40 days Sei/smoke tradition to my baby's health, so for my 3rd child I only did 3 days Sei tradition. (Mother FM1)
… since I live in my healthy traditional house, I feel the difference, my house much brighter, we already have 2 windows, it's not humid anymore, due to this cement floor. (Mother FM4)
In terms of the heat source used inside the traditional house, some families had started to use charcoal embers under the bed instead of burning firewood. As many families now perceived that the main health concern related with their Sei tradition was due to the smoke inside the house, they have attempted to reduce the smoke levels by changing the firewood pit inside the house with charcoal because it is believed to emit less smoke. There was also evidence that the duration of using a hot furnace or burning coal was also reduced. Based on the interviews, instead of a full 24hours per day, the warm condition was only introduced by lighting the fire pits/stoves during the night when the outside weather was cold. The husband usually prepared firewood in the afternoon, and then placed it inside the house before the night came. Such practices may have been associated with a reduction in air pollution as indicated from measured indicators presented in Prasodjo (Citation2012).
The results also show that the wider community benefited from this intervention. For example, the staff from the District Health Office and puskesmas indicated that they have more comprehensive knowledge about the effect of Sei tradition on the health of mothers and babies, as well as its possible effect on indoor air quality.
Household Air Pollution
At baseline, recorded household air pollution levels in traditional houses did not comply with the standard of healthy indoor air quality. The range of concentration levels of PM10 was very variable and was between 155 µg/m3 and 1,370 µg/m3, which was higher than the limited standard level recommended by the Ministry of Health (i.e., 150 µg/m3). Significant variations in factors that contribute to levels of household air pollution were seen at baseline—for example, differences in how long the Sei had been in practice for (i.e., early days or toward the end of 40th day), the size of burning firewood (i.e., small or big), ventilation, floor type, and composition of households.
At follow-up, results indicated that concentration levels of PM10, sulfur dioxide, nitrogen dioxide, and formaldehyde were also variable but with lower median levels as compared with the medians at baseline. For example, the median concentration of PM10 was 122 µg/m3 at follow-up and 315 µg/m3 at baseline. Overall, the concentration levels at follow-up were lower in the prototype healthy-redesigned house as compared with the four traditional houses (Prasodjo, Citation2012). These results are from a very small sample and the large variation in values suggests that the results are indicative only and should be interpreted with caution.
Development of Behavior Change Communication Intervention: Healthy Improved Ume Kbubu
The study originally aimed to introduce five prototypes of healthy-improved Ume Kbubu to the community. Because of some limitations in technical tools, budgetary aspects as well as the number of volunteers, only one healthy Ume Kbubu was introduced. Constructing the new healthy Ume Kbubu cost 5 million Indonesian rupiah (around US$500). This amount is very expensive for the communities, which have an annual provincial gross domestic product of about US$262 (Biro Pusat Statistik, 2010). Despite those challenges, one community supported the process by contributing their time and manual skills. They expressed that the process helped them to understand the community empowerment program, the process of community empowerment, and the advantages of a healthy Ume Kbubu.
Despite evidence of behavior change with regard to length and location of Sei practices, some families were still reluctant to support these interventions. Many families said they were willing to adopt it, yet poor education and low socioeconomic levels were barriers to adoption of a healthy improved house. The families also expressed concern that the new Ume Kbubu would no longer provide warmth during the cold weather, nor protect their crops and food stock.
Feedback from the local communities provided two recommendations for future practice. Many families would like to have more information written in the local language in addition to Indonesian, which is currently used in the brochure. The use of Indonesian language was initially done to ensure understanding by the community leaders who came from different cultural backgrounds. For the healthy Ume Kbubu, the house structure should be redesigned in a way that maintains its original structure and composition because of its significant traditional function as indicated in McWilliam (Citation2002) and Windi and Whittaker (Citation2012). More important, the house should be used to protect the family as well as to preserve their harvests.
Discussion
Preliminary findings from this study identify a range of health concerns relating to high levels of indoor air pollution in the traditional house Ume Kbubu, where mothers practiced the Sei tradition. At the same time, this tradition is still perceived as an important element in Timorese traditional practice. Therefore, a communication-focused behavior change intervention was introduced to foster conversion of traditional houses into healthy Ume Kbubu, and promote changes to traditional practices for better health outcomes.
For many Timorese, leaving Ume Kbubu is considered to omit the essence of the past. Promoting behavior changes in relation to maternal, child and newborn health behavior in relation to entrenched traditional practices is a complex process that requires an awareness and respect of the significance of these practices in the community as well as an understanding of the realities, sociocultural variables and environmental factors. Strategies need to accommodate the existing behavior practiced and acknowledged by the communities. From the baseline study in 2009, we identified and understood the behaviors which were having negative health impacts. Accordingly, the behavior change communication plans were designed by considering the observed risk factors related to the health of the mother and newborn.
Among the Timor population, the Sei tradition was traditionally done for up to 40 days. Because of that, many health services for postnatal mothers and babies, such as childhood immunization, could not be provided effectively. This tradition is still difficult to eliminate in some villages, such as Boti (Timor Tengah Selatan district) and Hauteas (Timor Tengah Utara district) where the communities have retained monarchy and traditional systems in which the heads of village are their leaders. Many mothers from Boti tribe, who prefer to have care from traditional healers, have insisted on following the Sei tradition even though it was discouraged by the village midwives.
The assessments of household air pollution in the existing traditional houses Ume Kbubu suggest that levels of several pollutants are far above the recommendations for a healthy house as stated by the Indonesian Ministry of Health (1999) or the World Health Organization (Citation2014). This is due to the fire pit inside the house that produces unhealthy gases and smoke, as well as poor ventilation. Nevertheless, the extremely variable results were from a very small sample size and so can only be interpreted as indicative and not conclusive evidence of the household air pollution in these traditional houses. These preliminary findings were presented to and discussed with involved stakeholders in the community. It has therefore increased their understanding about traditional practices (i.e., Sei tradition). At the same time, some families started to use an alternative practice of the Sei tradition by using a charcoal ember instead of burning firewood. Such practice requires further investigation to ensure that it is not exposing the mothers and babies to dangerously high levels of carbon monoxide. Further studies are needed to conduct personal exposure monitoring for the woman and child during the Sei tradition, to get robust data on their exposure at baseline and postintervention (which might include shortening the duration, increasing ventilation and making other affordable culturally appropriate changes to the traditional Ume Kbubu).
The participatory action research, which involved the wider community to develop a brochure on the health impacts of Sei tradition and to introduce a prototype of a healthy traditional house Ume Kbubu, demonstrated several important findings. The behavior change strategy successfully engaged the Timorese community, through consultation and involvement, as indicated by their willingness to support and adopt the interventions. Some families have already used healthy traditional houses Ume Kbubu that have more ventilation to help reduce levels of household air pollution, and there has been a shift toward reducing the length of the Sei tradition from the first 40 days after the baby was born to an average of 21 days (Prasodjo, Citation2012).
Some challenges were also identified in this study. The healthy redesigned Ume Kbubu is considered expensive for many rural communities that are dominated by poor families. It is not surprising that some families are still reluctant to adopt this approach. Therefore, a more cost efficient alternative is needed. The study found that some families used alternative places such as rumah besar or Lopo for doing their Sei tradition. Other alternatives would be using simple locally available materials that can be easily found for building the healthy Ume Kbubu, rather than using modern materials such as bricks and cement as was done for the prototype house. As a result, the cost could be reduced while maintaining its traditional function.
Conclusion
This study has shown that traditional behaviors can be changed by using participatory approaches. At the level of prevention, behavior change has been identified as a possible intervention strategy to reduce the effect of household air pollution on the health of mothers and children. In this case, introduction of a healthy traditional house was communicated to the wider community, and early adopters who started to change their traditional practices were identified. The strategy showed preliminary evidence of reducing the duration of Sei tradition from 40 days to only 4 days with a postintervention average of 21 days. It is hoped with continued behavior change communication intervention such changes in practices become more accepted and duration of exposure to high levels of household air pollution are reduced to improve the health status of communities, particularly mothers and newborn babies.
In summary, this current study has implications for further research. The preliminary study highlighted that Timorese women practiced Sei in the traditional house, which has many negative consequences. Some preliminary changes in Sei practice, including shorting the period's length and attempting to reduce household air pollution, have been seen after the behavior change communication intervention. To determine the current extent of traditional Sei practices among women, as well as the effect on household air pollution levels and health, a larger study with more robust household air pollution monitoring is required. This will provide further evidence on the relationship between traditional practices and maternal/children's health and morbidity among the Timorese population. It is also recommended that more collaboration between the government, the community and all related stakeholders is needed to communicate and socialize the implementation of the healthy house.
Acknowledgments
The authors acknowledge the support received from Indonesian Ministry of Health, particularly the Center for Public Health Intervention Technology from the National Institute of Health Research and Development, and the Nusa Tenggara Timur Provincial Health Office as well as the Timor Tengah Selatan District Health Office in conducting the study. Special thanks are also given to the research team, mothers, families, and all stakeholders who participated in and contributed to this study.
References
- Agus, Y., Horiuchi, S. & Porter, S. E. (2012). Rural Indonesia women's traditional beliefs about antenatal care. BMC Research Notes, 5, 589.
- Armstrong, J. R. & Campbell, H. (1991). Indoor air pollution exposure and lower respiratory infections in young Gambian children. International Journal of Epidemiology, 20, 424–429.
- Badan Standardisasi Nasional [The National Standardization Agency of Indonesia]. (2005). Bagian 3: Cara Uji Partikel Tersuspensi Total Menggunakan Peralatan High Volume Air Sampler (HVAS) dengan Metoda Gravimetri [Part 3: Measuring total suspended particle by using gravimetry method with high-volume air sampler (HVAS) equipment). Standar Nasional Indonesia no. 19-7119.3-2005.
- Barnes, B. R. (2014). Behavioural change, indoor air pollution and child respiratory health in developing countries: A review. International Journal of Environmental Research and Public Health, 11, 4607–4618.
- Biro Pusat Statistik [Central Bureau of Statistics]. (2010). Indonesian population census. Jakarta, Indonesia: Author.
- Bruce, N., Perez-Padilla, R. & Albalak, R. (2000). Indoor air pollution in developing countries: a major environmental and public health challenge. Bulletin of the World Health Organization, 78, 1078–1092.
- Bruce, N., Pope, D., Rehfuess, E., Balakrishnan, K., Adair-Rohani, H. & Dora, C. (2014). WHO indoor air quality guidelines on household fuel combustion: Strategy implications of new evidence on interventions and exposure risk functions. Atmospheric Environment. doi:10.1016/j.atmosenv.2014.08.064
- Buntoro, A. (2006). Rumah Bulat jadi sumber penyakit di Nusa Tenggara Timur? [Round house as the source of health problems in NTT Province?]. Retrieved from http://www.ntt-online.org
- Cohen, A. B., Greenwood, D. J. & Harkavay, I. (1992). Social research for social change: Varieties of participatory action research. Collaborative Inquiry, 7, 2–8.
- Creswell, J. W. (2003). Research design: Qualitative, quantitative and mixed methods approaches. Thousand Oaks, CA: Sage.
- Departemen Kesehatan [Indonesian Ministry of Health]. (1999). Keputusan Menteri Kesehatan No.829/MENKES/SK/VII/1999 tentang persyaratan kesehatan perumahan [Ministry of Health regulation on requirement of healthy house]. Jakarta, Indonesia: Author.
- Dima, T. K., Antariksa & Nugroho, A. M. (2013). Konsep ruang Ume Kbubu Desa Kaenbaun Kabupaten Timor Tengah Utara [Spatial concept of Ume Kbubu in Kaenbaun Village, Timor Tengah Utara District]. Jurnal RUAS, 11, 28–36.
- Dinas Kesehatan Kabupaten Timor Tengah Selatan. (2010). Health profile 2010. Soe, Indonesia: Dinkes TTS.
- Geertz, H. (1961). The Javanese family: A study of kinship and socialization. New York, NY: The Free Press of Glencoe.
- Hansen, E. C. (2006). Successful qualitative health research: A practical introduction. Singapore: Allen & Unwin.
- Hoekman, N., Thompson, S. & Mercer, M. A. (2008). Improving maternal and newborn health in East Timor (Timor-Leste). Fourth Annual Report, PVO Child Survival and Health Grants Program USAID/GH/HIDN/NUT. Seattle, WA: Health Alliance International.
- Krieger, J. & Higgins, D. (2002). Housing and health: Time again for public health. American Journal of Public Health, 92, 758–768.
- Lim, S. S., Vos, T., Flaxman, A. D., Danaei, G., Shibuya, K., Adair-Rohani, H., … Ezzati, M. (2012). A comparative risk assessment of burden of disease and injury attributable to 67 risk factors and risk factor clusters in 21 regions, 1990–2010: A systematic analysis for the Global Burden of Disease Study 2010. The Lancet, 380, 2224–2260.
- Martin, W. J., II, Glass, R. I., Araj, H., Balbus, J., Collins, F. S., … Bruce, N. G. (2013). Household air pollution in low- and middle-income countries: Health risks and research priorities. PLoS Med, 10, e1001455.
- McWilliam, A. (2002). Paths of origin, gates of life. Leiden, The Netherlands: Koninklijk Instituut voor Taal-en Volkenkunde [Royal Institute of Linguistic and Anthropology].
- Meyer, J. (2000). Using qualitative methods in health-related action research. British Medical Journal, 320, 178–181.
- Prasodjo, R. (2009). Studi kejadian kesakitan dan kematian pada ibu dan bayi yang melakukan budaya Sei di kabupaten Timor Tengah Selatan, Nusa Tenggara Timur [Study of morbidity and mortality among mothers and babies who practiced Sei tradition in Timor Tengah Selatan District, East Nusa Tenggara] (Unpublished research report). Jakarta, Indonesia: Pusat Penelitian dan Pengembangan Ekologi Kesehatan. Badan Penelitian dan Pengembangan Kesehatan [Research Center and Development of Health Ecology].
- Prasodjo, R. (2012). Studi intervensi tradisi SEI di Kabupaten Timor Tengah Selatan Tahap 3: Evaluasi Model Intervensi, Model Pembuatan Rumah Bulat (Tahap Evaluasi) [Intervention study of SEI tradition in Timor Tengah Selatan District, Stage 3: Evaluation of Intervention Model, Model Making of Rumah Bulat (Phase Evaluation)] (Unpublished research report). Jakarta, Indonesia: Bidang Teknologi Intervensi Kesehatan Masyarakat. Badan Penelitian dan Pengembangan Kesehatan [Research Center and Development of Health Ecology].
- Raven, J., Chen, Q., Tolhurst, R. & Garner, P. (2007). Traditional beliefs and practices in the postpartum period in Fujian Province, China: A qualitative study. BioMed Central Pregnancy and Childbirth, 7, 1–11.
- Rogers, E. M. (2003). Diffusion of innovations (5th ed.). New York, NY: Free Press.
- Smith, K. R., McCracken, J. P., Weber, M. W., Hubbard, A., Jenny, A., Thompson, L. M., … Bruce, N. (2011). Effect of reduction in household air pollution on childhood pneumonia in Guatemala (RESPIRE): A randomised controlled trial. The Lancet, 378, 1717–1726.
- Swasono, M. F. H. (1998). Kehamilan dan kelahiran dalam konteks budaya dan implikasinya terhadap kesehatan bayi dan ibu [Pregnancy and delivery in cultural context and its implication to child's and mother's health]. In Meutia F. Swasono (Ed.), Kehamilan, kelahiran, perawatan ibu dan bayi dalam konteks budaya [Pregnancy, delivery, maternal and neonatal cares in the context of cultural] (pp. 346–353). Jakarta: University of Indonesia Press.
- Windi, Y. K. & Whittaker, A. (2012). Indigenous round houses versus ‘healthy houses': Health, place and identity among the Dawan of West Timor, Indonesia. Health & Place, 18, 1153–1161.
- World Health Organization. (2000). The proceedings of WHO-USAID Global Consultation on the Health Impact of Indoor Air Pollution and Household Energy in Developing Countries, Washington, DC.
- World Health Organization. (2014). Deaths from household air pollution, 2012. Geneva, Switzerland: Author. Retrieved from http://apps.who.int/gho/data/node.main.140?lang1/4en
- Wulandari, L. P. & Klinken, W. A. (2011). Beliefs, attitudes and behavior of pregnant women in Bali. Midwifery, 27, 867–871.
- Yamashita, T., Suplido, S. A., Ladines-Llave, C., Tanaka, Y., Senba, N. & Matsuo, H. (2014). A cross-sectional analytic study of postpartum health care service utilization in the Philippines. PLoS ONE, 9, e85627.