
Abstract
Successful doctor–patient communication relies on appropriate levels of communicative health literacy, the ability to deal with and communicate about health information. This article aims to describe the development of a narrative- and picture-based health literacy intervention intended to support older patients with limited health literacy when communicating during their primary care consultations. We performed a formative evaluation that included a review of the literature and interviews with stakeholders on relevant health literacy issues, qualitative studies with the target group, intervention planning, and a small-scale evaluation. Cocreation with the target group was a major component. Seven photo stories were developed incorporating principles from narrative and social learning theory and covering communication themes and strategies identified during focus group discussions and role-play exercises. The intervention was developed in 3 different formats: 1-page photo stories, narrated video clips using the original photo story pictures, and interactive video clips covering participation and communication during primary care consultations. In our small-scale evaluation, older adults considered the cocreated intervention appealing and comprehensible. The intervention shows promise for improving the health of older adults but needs further evaluation. This study provides a rigorous template for the participatory development of health literacy interventions.
Doctor–patient communication is an important part of personalized health care and influences clinical outcomes, adherence, and patient satisfaction (Hall, Roter, & Katz, Citation1988; Roter, Hall, & Katz, Citation1988; Stewart, Citation1995). Its success depends to a large extent on the patient’s level of health literacy, in particular communicative health literacy. Communicative health literacy refers to the communicative aspects of health literacy and includes the ability to actively seek and exchange information during interactions with health care professionals (Nutbeam, Citation2000; Rubin, Parmer, Freimuth, Kaley, & Okundaye, Citation2011; Williams, Davis, Parker, & Weiss, Citation2002). Higher levels of health literacy are associated with more participatory interaction during medical encounters (Katz, Jacobson, Veledar, & Kripalani, Citation2007).
As older adults relatively frequently suffer from multiple chronic conditions, appropriate doctor–patient communication is even more important for them than for others. Moreover, older adults consider health care providers to be the most trusted and frequent source of health information (National Cancer Institute, Citation2006). However, older adults frequently have limited health literacy and as a consequence experience more difficulties in participating in care consultations, ask fewer questions, and report less patient-centered communication (McCaffery, Smith, & Wolf, Citation2010; Smith, Dixon, Trevena, Nutbeam, & McCaffery, Citation2009; Zamora & Clingerman, Citation2011).
The significance of doctor–patient communication in combination with the often low levels of health literacy of older adults calls for the development of communicative health literacy interventions for these adults. This need for communicative health literacy interventions is recognized, as illustrated in existing interventions such as the Ask Me 3 intervention (National Patient Safety Foundation, Citation2014) and question prompt sheets (Brandes, Linn, Butow, & Van Weert, Citation2015). These interventions have been shown to increase question-asking behavior in cancer patients (Brandes et al., Citation2015). However, interactive health literacy entails more than patients asking questions. It may therefore be beneficial to develop interventions that empower older adults in a broader range of skills, such as expressing their needs and concerns.
A core component of existing interventions is that patients are instructed or advised to act (e.g., ask questions and express possible misunderstandings during interactions with health care professionals). However, persuading patients to actively communicate during health care interactions is not always sufficient. Patients may fail to perform the suggested behaviors because they feel unable to do so or because they lack motivation. Moreover, resistance and associated counterarguing is a common human response to persuasive health communication, especially if recipients feel unable to perform the suggested behavioral strategies (Fransen, Smit, & Verlegh, Citation2015; Moyer-Gusé, Citation2008). Narrative health communication may be an effective strategy for increasing the effectiveness of communicative health literacy interventions and decreasing resistance to messages.
Narrative Health Communication
The potentially positive effects of narrative forms of health communication, like entertainment-education, storytelling, and testimonials, can be explained by a series of mechanisms and theories that have been explored in theoretical and empirical studies (Braddock & Dillard, Citation2016; De Graaf, Hoeken, Sanders, & Beentjes, Citation2012; Green & Brock, Citation2000, Citation2002; Hinyard & Kreuter, Citation2007; Hoeken & Sinkeldam, Citation2013; Slater & Rouner, Citation2002). Narrative communication uses story structures that provide a familiar mode of interaction. A narrative-based intervention could therefore be easier to process (Glaser, Garsoffky, & Schwan, Citation2009; Hinyard & Kreuter, Citation2007; Schank & Abelson, Citation1995; Zabrucky & Moore, Citation1999). Indeed, narrative health information was found to increase comprehensibility for older adults with different levels of health literacy (Koops van ’t Jagt, Hoeks, Jansen, De Winter, & Reijneveld, Citation2015). Furthermore, narratives have the potential to increase personal involvement and provide users with role models and step-by-step scenarios (Hinyard & Kreuter, Citation2007). Narrative communication can thus be viewed as a form of learning through experience (Mar & Oatley, Citation2008; Schank & Abelson, Citation1995). In addition, narratives may increase motivation to accept the included health messages and to act on those messages because of decreased resistance (Fransen et al., Citation2015; Moyer-Gusé, Citation2008). Readers or viewers are transported or absorbed into the story world (i.e., transportation) and perceive similarity and identify with characters, which may enhance self-efficacy to perform suggested behaviors. Taken together, narrative health communication is a promising strategy for improving the effectiveness of health literacy interventions. Recent studies also suggest that photo storybooks or fotonovelas in particular may be effective health communication tools, especially for readers with a low level of literacy (Boyte, Pilisuk, Matiella, & Macario, Citation2014; Duizer, Koops van ’t Jagt, & Jansen, 2014; James et al., Citation2005; Unger, Cabassa, Molina, Contreras, & Baron, Citation2013; Unger, Molina, & Baron, Citation2009).
This study aimed to develop a narrative-based communicative health literacy intervention that supports older adults in communicating with their doctor during care consultations. Because interventions that are tailored to the needs of the target group have proven to be more effective, we used a formative evaluation approach that included older adults’ own topics, barriers, and solutions (see also Cabassa, Molina, & Baron, Citation2012). Formative evaluation uses a set of activities to develop and pretest intervention materials and methods, allowing for a better understanding of the desired outcomes and essential components and contributing to interventions that are relevant and valuable to the target group (Nutbeam & Bauman, Citation2006). Moreover, cocreation with the target group is believed to increase the possibility that readers or viewers perceive similarity and identify with characters.
Our aim was to capture a wide range of health literacy experiences. We therefore performed the study not only in The Netherlands but also in Hungary, a Central European country with lower general health literacy levels. Previous research has shown health literacy levels in Western Europe (e.g., The Netherlands) to be higher than those in Central European countries for which health literacy data are available (HLS-EU Consortium, Citation2012).Footnote1
Methods
The intervention described in this article was developed using a formative evaluation approach based on intervention mapping protocols (e.g., Bartholomew et al., Citation2016; Bartholomew, Parcel, & Kok, Citation1998) within the context of the EU FP7 IROHLA project.Footnote2 Important components of the intervention development process were (a) a literature review and stakeholder analysis to explore relevant communicative health literacy issues; (b) focus group discussions (FGDs) to identify relevant target group barriers, needs, and preferences with regard to doctor–patient communication; and (c) role-play exercises to include older adults’ own solutions and strategies to the barriers identified. It was part of the participatory developmental process to specify with which communicative behaviors older adults from the target group needed support. This process of cocreation was chosen to ensure that the intervention would reflect themes, issues, and strategies that were relevant and authentic to the target group.
presents the activities during the development of the intervention that reflected formative evaluation: Phase 1: literature review and stakeholder analysis to identify relevant health literacy issues; Phase 2: formative evaluation to understand the target population and identify relevant barriers, needs, and preferences for the issue identified in Phase 1; Phase 3: role-play exercises to identify authentic target group solutions and strategies to the barriers identified in Phase 2; Phase 4: intervention planning and development based on the first three phases; and Phase 5: pilot testing of intervention methods and materials as developed in Phase 4. Each of these phases is discussed briefly here.
Fig. 1. Development procedure for the photo story health literacy intervention. NL = The Netherlands; HU = Hungary.
Phase 1: Literature Review and Stakeholder Analysis
A literature review was conducted using search terms related to (interactive) health literacy, older adults, patient–provider communication and participation, and using reference lists. Supplemental Online Appendix 1 provides a list of search terms. The following questions guided our literature review: (a) What are relevant communicative health literacy issues for older adults with limited health literacy? and (b) Which modifiable determinants are important in communicative health literacy interventions for older adults with limited health literacy?
In addition, we performed a stakeholder analysis by interviewing eight health care professionals from The Netherlands who regularly worked with older adults with limited health literacy using a semi-structured interview protocol. The number of interview participants was decided based on reaching thematic content saturation. We interviewed a geriatric specialist trainee, a general practitioner (GP) trainee, a GP, a sports and physical activity consultant for the elderly, a diabetes nurse/nurse practitioner, a sociologist, a former nurse and member of a senior think-tank, a health scientist specializing in vulnerable groups, and a board member of the local department of a Dutch older adults union. The purpose of the interview series was to explore to what extent communicative components of health literacy are recognized and identified as important and modifiable aspects by health professionals. The one-on-one interviews, carried out by the first author, started with an open-ended question asking for themes the interviewees considered relevant for older adults with limited health literacy. The interview outline, presented in Supplemental Online Appendix 2, was informed by health behavior theories, models, and research methods such as the salient belief elicitation, the theory of planned behavior, the health action process approach, and stages of change and included questions about outcome expectancies, efficacy beliefs, and intentions (Ajzen, Citation1991; Fishbein & Ajzen, Citation2010. Prochaska, Citation1994; Prochaska & DiClemente, Citation1983; Schwarzer, Citation2008). The interviews were analyzed by the first author using an open-ended content analysis.
Phase 2: FGDs in Hungary and The Netherlands
In the second phase, four semi-structured FGDs were conducted in The Netherlands (two groups, N = 11) and Hungary (two groups, N = 16) with older adults with low health literacy to assess their barriers, needs, and preferences with regard to the theme that was identified during the first phase. Participants in The Netherlands were recruited via the GP who had been interviewed during the first phase. This GP worked in a relatively disadvantaged village with mostly less educated citizens; most of them had only a primary education. Two FGDs were conducted in a local care home for the elderly. Participants in Hungary were recruited by contacting elderly patients through informal channels, local organizations, and stakeholders. Hungarian recruiters also asked older adults to bring along someone whom they would invite to support them while visiting their GP to collect additional input. FGDs were carried out in the native language of the participants, guided by a discussion leader with experience in qualitative methods (the first author for The Netherlands and a social-psychological researcher for Hungary) who used a semi-structured discussion guide (see Supplemental Online Appendix 3). All discussions were audio recorded and transcribed verbatim, and all identifiers were removed to maintain anonymity.
FGDs were analyzed from the top down using the six functions of medical communication described in the Framework of Endpoints in Medical Communication (De Haes & Bensing, Citation2009) combined with a coding scheme based on the topics covered in the discussion guide. Content analysis was conducted by the first author according to the five main steps identified in the framework analysis method: familiarization with the data: creating a thematic framework; indexing; charting; and mapping and identification (Ritchie, Spencer, & O’Connor, Citation2003).
Phase 3: Role-Play Exercises in Hungary and The Netherlands
In the third phase, we conducted role-play exercises in both countries with older adults with limited health literacy (The Netherlands, N = 9; Hungary, N = 4). The aim of this phase was to elicit patients’ authentic strategies, solutions, and verbalizations of these strategies that were considered possibly effective by older adults themselves for the issues identified during FGDs. Using role play exercises with a skilled actor playing the GP, based on different real life scenarios and involving a facilitator, gave the older participants the chance to safely practice communication strategies and create their own templates for communicative behaviors. Five scenario cards were developed with situations that were described as relevant by the participants during the group discussions. Each scenario was introduced by the researcher, after which one of the participants was invited to play the role of the older adult. Afterward, the other participants were invited to give feedback and propose other possible solutions and strategies. The role-play exercises were tape recorded and transcribed verbatim, and all identifiers were removed to maintain anonymity. For each scenario, participants’ strategies and responses were analyzed by the first author.
Phase 4: Planning and Development
This phase aimed to develop storylines and sketches for each of the themes that were identified during the analysis of the first four phases. Furthermore, we conducted a questionnaire-based expert consultation with both older adults (The Netherlands, N = 3) and health care professionals (Hungary, N = 1; The Netherlands, N = 6). We explored whether there were any suggestions for improvements to the format and content of the intervention. In this phase, we constructed our storylines and sketches based on theories of narrative mechanisms and theories of social and observational learning (e.g., Bandura, Citation1971, Citation1977; Mar & Oatley, Citation2008; Moyer-Gusé, Citation2008).
The final sketches were used as a starting point for producing the intervention. Amateur actors were recruited from a local theater group. The photographs were shot by a professional photo story designer in a local GP practice and in the home of the first author. The photo story designer subsequently edited the photographs and added speech and thought bubbles according to the scripts.
Phase 5: Pretesting the Method and Materials
Phase 5 aimed to evaluate whether older adults with limited health literacy found the intervention appealing, relevant, and recognizable. In order to explore whether readers would recognize the themes present in the intervention, an FGD was organized with five participants from the earlier group discussions in The Netherlands.
We report on outcomes of each phase that provided input for the next phase.
Results
Literature Review and Stakeholder Analysis (Phase 1)
We found some studies on older adults’ preferences for involvement in care in particular (Bastiaens, Van Royen, Rotar Pavlic, Raposo, & Baker, Citation2007; Chiu, Feuz, McMahan, Miao, & Sudore, Citation2015) and on doctor–patient communication in general (Bastiaens et al., Citation2007) but not on the specific needs, barriers, experiences, and preferences of older adults with limited health literacy regarding doctor–patient communication.
A large-scale study with chronic patients (n = 1,314) with varying levels of health literacy found that low health literacy is associated with an increased number of perceived barriers (Henselmans, Heijmans, Rademakers, & Van Dulmen, Citation2014). Patients with low literacy felt less confident and perceived more barriers to communication. The most frequently reported barriers were patients forgetting, professionals taking too little time, and patients wishing not to be bothersome (Henselmans et al., Citation2014). Patients endorsed relatively simple support, such as question prompt sheets (Henselmans et al., Citation2014). Perceived efficacy in patient–provider communication has also been found to be strongly associated with perceived self-management skills (Ten Klooster et al., Citation2011). These findings suggest that if interventions aim to activate patients with lower levels of health literacy, they should both improve communication self-efficacy and address barriers that are considered relevant by the target group (see also Osborn, Paasche-Orlow, & Wolf, Citation2011; Sarkar, Fisher, & Schillinger, Citation2006; Wolf et al., Citation2007, on the mediating role of self-efficacy linking health literacy to other health behaviors and outcomes). Furthermore, a qualitative analysis of two existing patient activation interventions (Ask Share Know and the Smart Health Choices questions; Muscat et al., Citation2015) revealed that adults with limited literacy experienced considerable difficulties with these interventions, such as feeling a lack of confidence, being mostly passive during clinical encounters, and struggling to read and understand several key terms included in both interventions. In addition, a systematic review addressing health literacy in patient decision aids revealed that communication aspects receive little attention in these interventions (McCaffery et al., Citation2013). In sum, the findings of our literature review stress the need for simple interventions that include communication aspects, address patients’ barriers, increase patients’ self-efficacy, and use clear and familiar language.
In the stakeholder analysis, all health professionals highlighted the importance of doctor–patient communication for older adults with limited health literacy. It was confirmed that a lack of self-confidence can be an important barrier to active participation. The interviewees also confirmed the need for interventions that acknowledge older adults’ barriers to active participation and increase their levels of self-efficacy. Barriers may include lacking adequate verbalizations and being unaware of the importance of some information, as represented by the following quotes from stakeholders:
I think that older people find it really difficult at the doctor’s. They are not as assertive as the rest of the population […] So I really do think that daring to ask questions is important.
I think they find it difficult, because, um, well there’s still somewhat of let’s call it a hierarchy […] that they dread going to the doctor, to challenge him … I can well imagine that that is what they feel, or um … that they don’t want to be rude, or if the doctor is pushed for time that they then think, “Oh, I don’t want to bother him.” And if he talks nonstop … Well, when do you interrupt? You have to be quite assertive then, don’t you?
The danger is that I end up discussing the patient with their children […] They are happy to let their children speak for them because they can’t put it into words themselves.
Maybe they don’t know that we need that information. There are still quite a few people who think that if they say they have a headache I will immediately be able to tell from the look on their face why that is.
These outcomes, taken together with the results of the literature review, led to the decision to explore older adults’ experiences, barriers, needs, and preferences in doctor–patient communication in the next phase. Moreover, older adults’ barriers should be incorporated into the intervention development as well as self-efficacy as a core component.
FGDs (Phase 2)
Older adults’ ideas on doctor–patient communication identified during the FGDs were categorized according to the following four recurring categories: GP-related issues, patient-related issues, contextual issues, and issues related to the doctor–patient interaction. Furthermore, we analyzed the transcripts according to four main dimensions based on the Framework of Endpoints in Medical Communication (De Haes & Bensing, Citation2009): the affective or relationship dimension, communicating information (information provision and information gathering), enabling decision making, and supporting disease- and treatment-related behavior. Finally, we distinguished between needs, barriers, and facilitators.
In the FGDs, participants discussed experiences, needs, barriers, and solutions related to all four dimensions described previously. Overall, the affective dimension was stressed in the majority of contributions, whereas decision making was mostly present in the Hungarian discussions with regard to medication.
and present the most important barriers to and facilitators of communicative health literacy that came up during the Dutch and Hungarian FGDs. Barriers to communicative health literacy included contextual factors, such as the doctor’s availability; patient-related factors, such as stress, emotions, and insufficient self-efficacy; GP-related factors, such as incomprehensible or overwhelming information; and interactional factors, such as an absence of mutual trust and asymmetry in expertise and knowledge.
Table 1. Barriers to doctor–patient communication regarding affective communication, information provision and gathering, decision making, and disease- and treatment-related communication
Table 2. Facilitators of doctor–patient communication regarding affective communication, information provision and gathering, decision making, and disease- and treatment-related communication
During the FGDs, the majority of participants mentioned that it could help to ask questions, ask for clarification, or bring something up for discussion but that they often did not know appropriate ways to do this or did not believe in their own abilities.
Role-Play Exercises (Phase 3)
The role-play exercises had the following themes, based on barriers discussed during FGDs: GP’s use of difficult language, GP’s lack of time and/or patient centeredness, difficulties with medication adherence, the GP providing too much or too little information, and feeling stressed or nervous. The following strategies were considered successful solutions to these scenarios by the Hungarian and Dutch participants: (a) asking questions and/or repeating questions, using polite and proper wording; (b) sharing anxieties and insecurities with the doctor; (c) bringing along a companion for support; (d) making a list of questions before the consult; and (e) writing things down during the consult.
Discussing the role-play exercises with participants also revealed several barriers to performing these strategies. Patients often feel impolite if they ask the same question multiple times or if they interrupt their doctor, because “(S)he is the doctor.” Older patients apparently often look up to their doctor, which prevents them from asking questions and speaking up for themselves. In addition, patients sometimes feel dependent on their doctor. Participants confirmed that providing them with proper and polite phrases to do these things may help to lower these barriers and recognized that sharing example strategies during the role-play exercises was helpful. This suggests that scenarios portraying specific examples of such communication strategies may be beneficial.
In order to provide older adults with limited health literacy with solutions and strategies to overcome the barriers they experience during doctor–patient communication, we decided to develop a narrative-based health literacy intervention. The decision to develop a narrative intervention was based on the outcomes of a systematic review of the comprehensibility of health-related documents, advantages of narrative formats reported in the literature, and positive evaluations of examples of narrative-based health information during FGDs.
Planning and Production (Phase 4)
Planning
Emphasis was put on integrating narrative elements that are considered important in narrative theory and were discussed previously, such as transportation, identification, and perceived similarity (Moyer-Gusé, Citation2008) and the use of step-by-step social scenarios (i.e., the use of narratives as a social virtual reality game; Mar & Oatley, Citation2008; Schank & Abelson, Citation1995). We instructed our older actors to display lively facial expressions to portray the character’s emotions because of practice-based indications of the importance of vivid imagery to engage the photo story’s audience. Compared to video imagery, which includes dynamic movement of facial muscles, photographs offer fewer possibilities to portray emotional states. Lively facial expressions help to portray the characters’ emotions and to tell the story. In seven six-frame stories, the main characters experienced barriers similar to those identified during FGDs (titles of stories are in parentheses; see –). These barriers were as follows:
Lack of time or attention (“All Ears”)
Feeling nervous: bringing a companion for social support (“Two Heads Are Better”)
Incomprehensible language (“Double Dutch”)
Medication adherence (“Some List”)
Translating advice or prescriptions into concrete actions (“Salt!”)
Medication management (“Inside the Box”)
Making a list of questions in preparation for the consult (“Piece of Paper”)
Fig. 2. Story 1 about lack of attention from a general practitioner.
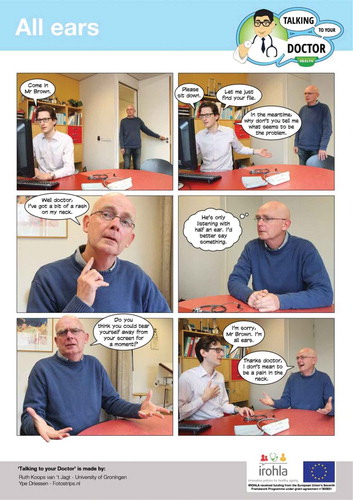
Fig. 3. Story 2 about bringing someone for support.

Fig. 4. Story 3 about incomprehensible medical language.

Through social interaction with peers, family members, or their doctors, the main characters came up with solutions and communication strategies to deal with these barriers. In this way, our photo stories were in line with theories on social learning (Bandura, Citation1971, Citation1977). The solutions and strategies we included in the photo stories were also based on Phases 2 and 3 of the formative evaluation and included phrases that had been articulated during the FGDs and role-play exercises. In case these verbalizations only existed in Dutch, translations were adapted to the target languages in such a way that content was preserved.
In all seven stories, patients’ doubts and worries were explicitly portrayed, aiming to increase recognition, perceived similarity, identification, and self-referent thoughts. Stories have the potential to elicit thoughts and reflections about one’s own experiences and ideas, which make up a potentially powerful process through which stories may achieve effects in readers, listeners, and viewers (De Graaf, Citation2014).
Intervention Production
Three formats for the intervention were developed, all originally in Dutch, taking into account literacy level. First, we developed an A4-paper-size booklet that included the seven photo stories. Next, we developed seven video clips based on the photo stories, now with audio. Finally, we developed interactive video clips in which the stories were interrupted by a question to the viewer (e.g., “What would you do?”). These video clips were developed for the Dutch website www.oefenen.nl, which offers learning modules and exercises for adult language learners. The booklet with the photo stories was translated into English, German, Italian and Hungarian. The video clips were developed in Dutch and English and the interactive video clips in Dutch.
– present three of the seven stories included in the final booklet. A screenshot from an interactive video clip is shown in .
Fig. 5. Screenshot of an interactive video clip on www.oefenen.nl. The question on the right part of the screen asks the user “Have you ever experienced something similar? Were you unable to tell your doctor something?”.

Questions included in the interactive video clips were designed with the purpose to encourage and increase users’ self-referent thoughts (e.g., “Do you recognize this?” “What would you do?” “What would be your advice for this lady?”). The team of experts at www.oefenen.nl also developed questions and exercises for the video clips in which participants are invited to apply related skills.
Small-Scale Evaluation (Phase 5)
In the final phase, the intervention was evaluated with members of the Dutch focus group described in Phase 3. In total, five participants shared their opinions on the newly developed booklets with photo stories. Participants said that the photo stories were recognizable and lively and represented situations they had discussed during the earlier group discussions. They also indicated that the photo stories were about important themes and said that the photo stories should be distributed in waiting rooms and in care facilities. A few quotes from older adults follow:
“Lovely pictures!”
“I’m definitely taking it home with me. Then my wife can read it too.”
“I think a lot of people will take a copy.”
“It’s an interesting booklet. You really have to take the time to let it sink in. You can’t just flick through it.”
“It’s very true to life.”
“Well maybe if people have a booklet like this, they’ll take a look at it before they go to the doctor. That’s my opinion anyway.”
“I think it looks really good. Really good.”
One older adult elaborated as follows:
This is easier for us to understand … Because you’re old and aren’t so flexible in your thinking anymore. There are photos with a story, and because you experience that, um, well not daily, but at least a couple of times per year … You regularly have to deal with illnesses and talking to doctors … Then this appeals to you much more.
Note that participants evaluated the main character in the first photo story (“All Ears”) as being too bold. We therefore adjusted the script. A frame was included in which the patient overthinks whether he should confront the GP with his lack of attention before the patient takes action, making the confrontation “less abrupt and rude.” This confirmed our initial approach in which we aimed to explicitly portray patients’ doubts and worries to make them more similar and recognizable to users.
Discussion
This study aimed to describe the development of a communication intervention for older adults with limited health literacy. We found that older adults with limited health literacy feel less able to apply communication strategies, are less aware of the importance of participatory interaction, and perceive more barriers to communication. Together these may limit their ability to participate actively in doctor–patient communication. Therefore, the intervention we developed not only aimed to increase older adults’ awareness of their barriers and the importance of doctor–patient communication but also aimed to empower them to use strategies to overcome these barriers. This may add to the available tools for empowering older adults in their primary care contacts, such as training programs to enhance doctor–patient communication and shared decision making (Cooper et al., Citation2011; Muscat et al., Citation2015).
A narrative approach was considered to be a promising tool for achieving these aims. We developed seven photo stories, each focusing on one of the identified issues or themes incorporating principles from social learning theory (Bandura, Citation1971, Citation1977; Mar & Oatley, Citation2008) and theories on narratives (Mar & Oatley, Citation2008; Moyer-Gusé, Citation2008; Schank & Abelson, Citation1995). The stories explicitly addressed negative thoughts regarding communicative ability that may hinder individuals with lower health literacy in their interaction with health professionals. It is important to note that the stories also explicitly showed how to handle these problems in order to increase older patients’ awareness, communicative self-efficacy, and intentions.
A stepwise approach in cocreation with stakeholders and the target group resulted in photo stories that the target group considered relevant, recognizable, and appealing. Such a simple intervention could be implemented relatively easily in the communication training of patients and professionals. The positive feedback during our small-scale evaluation suggests that photo stories and fotonovelas may indeed effectively support older adults with a low level of literacy, as has been suggested in the literature (Boyte et al., Citation2014; James et al., Citation2005; Unger et al., Citation2009, Citation2013). Evidently this assumption requires testing in larger scale evaluations.
Compared with other communication health literacy interventions that are currently available, such as patient decision aids (McCaffery et al., Citation2013), the Ask Me 3 intervention, and AskShareKnow and the Smart Health Choices questions (Muscat et al., Citation2015), the current intervention adds to the field with its addressing of a broad range of communication skills and its explicit acknowledgment and narrative representation of older patients’ barriers. The latter has been suggested to add to its effectiveness (Fransen et al., Citation2015; Moyer-Gusé, Citation2008) and was explicitly appreciated in the small-scale evaluation.
The specific stepwise design procedure described here involved the participation of older adults from the target group in almost every step. The FGDs and role-play exercises enabled participants to share valuable information about their ideas and experiences with doctor–patient communication and to safely practice and discuss communication strategies in hypothetical scenarios. This process of cocreation may increase empowerment in older adults with low health literacy, further extending the potential for personal involvement with this type of narrative intervention, which is in itself already a major strength of narratives (Hinyard & Kreuter, Citation2007).
Strengths and Limitations
A major strength of this study is its use of a stepwise, bottom-up development procedure that took into account perspectives from (a) the literature, (b) health care professionals, (c) older adults themselves from Hungary and The Netherlands, and (d) informal caretakers in Hungary. This resulted in a cocreated communication intervention that members of the target group consider relevant, recognizable, and appealing.
Another important strength is that it provides a template for the development of similar interventions for other target groups or on other topics. We incorporated principles from intervention mapping and formative evaluation in a new framework, using a multimethod approach including a broad range of communicative health literacy perspectives. We successfully applied the innovative qualitative methodology of role-play exercises to actively involve the target group in identifying the intervention’s strategies. This framework may be easily adapted for the purpose of other health literacy interventions and contributes to developing interventions that are considered relevant and appealing by the target group.
A limitation of the study may be that we included older adults from only two European regions and professionals from only one European region. Moreover, the photo stories were produced in The Netherlands and depicted only Dutch actors. Ongoing evaluation studies will provide more insight into the applicability of our findings and our intervention in other European countries, for instance by adapting the pictures and texts to other cultures.
Conclusion
Our method led to a cocreated photo story intervention on doctor–patient communication incorporating principles from narrative theory and social learning, following a rigorous phased approach including the participation of health care professionals and older adults with limited health literacy. Next steps include pilot studies to systematically evaluate its appreciation and effectiveness regarding communication self-efficacy and behavioral intentions in The Netherlands, Germany, and Italy. Visual-narrative interventions may be very promising for improving the health of older adults, though this requires further evaluation. This type of intervention may help to achieve adequate diagnosis, enhanced doctor–patient relationships, improved self-management, and medication management and adherence.
UHCM_A_1193918_Appendix_3.docx
Download MS Word (22.2 KB)UHCM_A_1193918_Appendix_2.docx
Download MS Word (16.4 KB)UHCM_A_1193918_Appendix_1.docx
Download MS Word (13.2 KB)Acknowledgments
We are very grateful to Ágnes Novosath, Péter Csizmadia, and Koós Tamás, who organized the focus group discussions and role-play exercises in Hungary. Furthermore, we are very thankful to all of the focus group participants, all of the actors, photo story designer Ype Driessen, and the general practice where we had our photo shoot. Finally, the development of the interactive photo stories was made possible by the team at ETV.nl.
Funding
This review is part of the IROHLA project. IROHLA is coordinated by the University Medical Center Groningen and has received funding from the European Union’s Seventh Framework Programme (FP7/2007-2013) under Grant No. 305831.
Supplemental Material
Supplemental online appendices (Appendix 1: Search Terms Used in Medline and Google Scholar; Appendix 2: Interview Outline for Health Care Professionals; Appendix 3: Focus Group Outline) are available on the publisher’s website at http://dx.doi.org/10.1080/10810730.2016.1193918.
Additional information
Funding
Notes
1 The European Health Literacy Survey was conducted in July 2011 by TNS Opinion in all countries participating in the project, thus Austria, Bulgaria, Germany NRW, Greece, Ireland, The Netherlands, Poland, and Spain. In The Netherlands, 2% of the general population had inadequate health literacy and 27% had problematic health literacy. No data are available for Hungary, but in Bulgaria, 27% had inadequate health literacy and 35% had problematic health literacy. About 12% of all European respondents were found to have inadequate general health literacy, and more than one third (35%) were found to have problematic health literacy.
2 The IROHLA (“Intervention Research on Health Literacy among the Aging Population”) project focused on improving health literacy for older people in Europe. It identified and validated a set of 20 best-evidence interventions, constituting a comprehensive approach to addressing the health literacy needs of the aging population in Europe. These interventions were incorporated into an evidence-based guideline for policy and practice for local, regional, and national government authorities (www.healthliteracy.eu).
Related Research Data
References
- Ajzen, I. (1991). The theory of planned behavior. Organizational Behavior and Human Decision Processes, 50, 179–211. doi:10.1016/0749-5978(91)90020-T
- Bandura, A. (1971). Social learning theory. New York, NY: General Learning Press.
- Bandura, A. (1977). Self-efficacy: Toward a unifying theory of behavioral change. Psychological Review, 84, 191–215. doi:10.1037/0033-295X.84.2.191
- Bartholomew, L. K., Markham, C. M., Ruiter, R. A. C., Fernàndez, M. E., Kok, G., & Parcel, G. S. (2016). Planning health promotion programs: An intervention mapping approach (4th ed.). Hoboken, NJ: Wiley.
- Bartholomew, L. K., Parcel, G. S., & Kok, G. (1998). Intervention mapping: A process for developing theory- and evidence-based health education programs. Health Education & Behavior, 25(5), 545–563. doi:10.1177/109019819802500502
- Bastiaens, H., Van Royen, P., Rotar Pavlic, D., Raposo, V., & Baker, R. (2007). Older people’s preferences for involvement in their own care: A qualitative study in primary health care in 11 European countries. Patient Education and Counseling, 68, 33–42. doi:10.1016/j.pec.2007.03.025
- Boyte, R. M., Pilisuk, T., Matiella, A. C., & Macario, E. (2014). Developing a bilingual fotonovela to encourage human papillomavirus preteen immunization in California: A case study. Californian Journal of Health Promotion, 12(3), 1–13.
- Braddock, K., & Dillard, J. P. (2016). Meta-analytic evidence for the persuasive effect of narratives on beliefs, attitudes, intentions, and behaviors. Communication Monographs. Advance online publication. doi:10.1080/03637751.2015.1128555
- Brandes, K., Linn, A. J., Butow, P. N., & Van Weert, J. C. M. (2015). The characteristics and effectiveness of question prompt list interventions in oncology: A systematic review of the literature. Psycho-Oncology, 24(3), 245–252. doi:10.1002/pon.3637
- Cabassa, L. J., Molina, G. B., & Baron, M. (2012). Depression fotonovela: Development of a depression literacy tool for Latinos with limited English proficiency. Health Promotion Practice, 13(6), 747–754. doi:10.1177/1524839910367578
- Chiu, C., Feuz, M. A., McMahan, R. D., Miao, Y., & Sudore, R. L. (2015). “Doctor, make my decisions”: Decision control preferences, advance care planning, and satisfaction with communication among diverse older adults. Journal of Pain and Symptom Management. Advance online publication. doi:10.1016/j.jpainsymman.2015.07.018
- Cooper, L. A., Roter, D. L., Carson, K. A., Bone, L. R., Larson, S. M., Miller, E. R., … Levine, D. M. (2011). A randomized trial to improve patient-centered care and hypertension control in underserved primary care patients. Journal of General Internal Medicine, 26(11), 1297–1304. doi:10.1007/s11606-011-1794-6
- De Graaf, A. (2014). The effectiveness of adaptation of the protagonist in narrative impact: Similarity influences health beliefs through self-referencing. Human Communication Research, 40, 73–90. doi:10.1111/hcre.2014.40.issue-1
- De Graaf, A., Hoeken, H., Sanders, J., & Beentjes, J. W. J. (2012). Identification as a mechanism of narrative persuasion. Communication Research, 39(6), 802–823. doi:10.1177/0093650211408594
- De Haes, H., & Bensing, J. (2009). Endpoints in medical communication research, proposing a framework of functions and outcomes. Patient Education and Counseling, 74(3), 287–294. doi:10.1016/j.pec.2008.12.006
- Duizer, E., Koops van ’t Jagt, R., & Jansen, C. J. M. (2014). Zoete verleiding: Een onderzoek naar de effecten van een fotoverhaal over diabetes bij laaggeletterden [Sweet Temptations: A study into the effects of a fotonovela about diabetes on low-literates]. Tijdschrift Voor Taalbeheersing, 36(3), 293–330. doi:10.5117/TVT2014.3.DUIZ
- Fishbein, M., & Ajzen, I. (2010). Predicting and changing behavior: The reasoned action approach. New York, NY: Psychology Press.
- Fransen, M. L., Smit, E. G., & Verlegh, P. W. J. (2015). Strategies and motives for resistance to persuasion: An integrative framework. Frontiers in Psychology, 6, 1201–1221. doi:10.3389/fpsyg.2015.01201
- Glaser, M., Garsoffky, B., & Schwan, S. (2009). Narrative-based learning: Possible benefits and problems. Communications-European Journal of Communication Research, 34(4), 429–447.
- Green, M. C., & Brock, T. C. (2000). The role of transportation in the persuasiveness of public narratives. Journal of Personality and Social Psychology, 79(5), 701–721. doi:10.1037/0022-3514.79.5.701
- Green, M. C., & Brock, T. C. (2002). In the mind’s eye: Transportation-imagery model of narrative persuasion. In M. C. Green, J. J. Strange, & T. C. Brock (Eds.), Narrative impact: Social and cognitive foundations (pp. 315–341). Mahwah, NJ: Erlbaum.
- Hall, J. A., Roter, D. L., & Katz, N. R. (1988). Meta-analysis of correlates of provider behavior in medical encounters. Medical Care, 26, 657–675. doi:10.1097/00005650-198807000-00002
- Henselmans, I., Heijmans, M., Rademakers, J., & Van Dulmen, S. (2014). Participation of chronic patients in medical consultations: Patients’ perceived efficacy, barriers and interest in support. Health Expectations, 18, 2375–2388. doi:10.1111/hex.12206
- Hinyard, L. J., & Kreuter, M. W. (2007). Using narrative communication as a tool for health behavior change: A conceptual, theoretical, and empirical overview. Health Education & Behavior, 34(5), 777–792. doi:10.1177/1090198106291963
- HLS-EU Consortium. (2012). Comparative report of health literacy in eight EU member states. Retrieved from http://www.healthliteracyeurope.net
- Hoeken, H., & Sinkeldam, J. (2013). De rol van emoties in narratieve overtuiging [The role of emotions in narrative persuasion]. Tijdschrift Voor Taalbeheersing, 35(3), 226–236. doi:10.5117/TVT2013.3.HOEK
- James, S., Reddy, P. S., Ruiter, R. A. C., Taylor, M., Jinabhai, C. C., Van Empelen, P., & Van Den Borne, B. (2005). The effects of a systematically developed photo-novella on knowledge, attitudes, communication and behavioural intentions with respect to sexually transmitted infections among secondary school learners in South Africa. Health Promotion International, 20(2), 157–165. doi:10.1093/heapro/dah606
- Katz, M., Jacobson, T., Veledar, E., & Kripalani, S. (2007). Patient literacy and question-asking behavior during the medical encounter: A mixed-methods analysis. Journal of General Internal Medicine, 22, 782–786. doi:10.1007/s11606-007-0184-6
- Koops van ’t Jagt, R., Hoeks, J. C. J., Jansen, C. J. M., De Winter, A. F., & Reijneveld, S. A. (2015). Comprehensibility of health related documents for older adults: A systematic review. Journal of Health Communication, 21(2), 159–177. doi:10.1080/10810730.2015.1049306
- Mar, R. A., & Oatley, K. (2008). The function of fiction is the abstraction and simulation of social experience. Perspectives on Psychological Science, 3(3), 173–192. doi:10.1111/j.1745-6924.2008.00073.x
- McCaffery, K. J., Holmes-Rovner, M., Smith, S. K., Rovner, D., Nutbeam, D., Clayman, M. L., … Sheridan, S. L. (2013). Addressing health literacy in patient decision aids. BMC Medical Informatics and Decision, 13(Suppl. 2), S10. doi:10.1186/1472-6947-13-S2-S10
- McCaffery, K. J., Smith, S. K., & Wolf, M. (2010). The challenge of shared decision making among patients with lower literacy: A framework for research and development. Medical Decision Making, 30(1), 35–44. doi:10.1177/0272989X09342279
- Moyer-Gusé, E. (2008). Toward a theory of entertainment persuasion: Explaining the persuasive effects of entertainment-education messages. Communication Theory, 18, 407–425. doi:10.1111/comt.2008.18.issue-3
- Muscat, D. M., Morony, S., Shepherd, H. L., Smith, S. K., Dhillon, H. M., Trevena, L., … McCaffery, K. (2015). Development and field testing of a consumer shared decision-making training program for adults with low literacy. Patient Education and Counseling, 98, 1180–1188. doi:10.1016/j.pec.2015.07.023
- National Cancer Institute. (2006). Health Information National Trends Survey. Retrieved from http://hits.cancer.gov/
- National Patient Safety Foundation. (2014). Ask me 3. Retrieved from http://www.npsf.org/?.page=2015aksme3
- Nutbeam, D. (2000). Health literacy as a public health goal: A challenge for contemporary health education and communication strategies into the 21st century. Health Promotion International, 15, 259–267. doi:10.1093/heapro/15.3.259
- Nutbeam, D., & Bauman, A. (2006). Evaluation in a nutshell: A practical guide to the evaluation of health promotion programs. Sydney, Australia: McGraw-Hill.
- Osborn, C. Y., Paasche-Orlow, M. K., & Wolf, M. S. (2011). The mechanisms linking health literacy to behavior and health status. American Journal of Health Behavior, 35(1), 118–128. doi:10.5993/AJHB.35.1.11
- Prochaska, J. O. (1994). Strong and weak principles for progressing from precontemplation to action on the basis of twelve problem behaviors. Health Psychology, 13, 47–51. doi:10.1037/0278-6133.13.1.47
- Prochaska, J. O., & DiClemente, C. C. (1983). Stages and processes of self change of smoking: Toward an integrative model of change. Journal of Consulting and Clinical Psychology, 51, 390–395. doi:10.1037/0022-006X.51.3.390
- Ritchie, J., Spencer, L., & O’Connor, W. (2003). Carrying out qualitative analysis. In J. Ritchie & J. Lewis (Eds.), Qualitative research practice: A guide for social science students and researchers (pp. 219–262). London, UK: Sage.
- Roter, D. L., Hall, J. A., & Katz, N. R. (1988). Patient-physician communication: A descriptive summary of the literature. Patient Education and Counseling, 12, 99–119. doi:10.1016/0738-3991(88)90057-2
- Rubin, D. L., Parmer, J., Freimuth, V., Kaley, T., & Okundaye, M. (2011). Associations between older adults’ spoken interactive health literacy and selected health care and health communication outcomes. Journal of Health Communication, 16(Suppl. 3), 191–204. doi:10.1080/10810730.2011.604380
- Sarkar, U., Fisher, L., & Schillinger, D. (2006). Is self-efficacy associated with diabetes self-management across race/ethnicity and health literacy? Diabetes Care, 29(4), 823–829. doi:10.2337/diacare.29.04.06.dc05-1615
- Schank, R. C., & Abelson, R. P. (1995). Knowledge and memory: The real story. In R. S. Wyer, Jr. (Ed.), Knowledge and memory: The real story (pp. 1–85). Hillsdale, NJ: Erlbaum.
- Schwarzer, R. (2008). Modeling health behavior change: How to predict and modify the adoption and maintenance of health behaviors. Applied Psychology, 57(1), 1–29.
- Slater, M. D., & Rouner, D. (2002). Entertainment-education and elaboration likelihood: Understanding the processing of narrative persuasion. Communication Theory, 12(2), 173–191.
- Smith, S. K., Dixon, A., Trevena, L., Nutbeam, D., & McCaffery, K. J. (2009). Exploring patient involvement in healthcare decision making across different education and functional health literacy groups. Social Science & Medicine, 69, 1805–1812. doi:10.1016/j.socscimed.2009.09.056
- Stewart, M. A. (1995). Effective physician-patient communication and health outcomes: A review. Canadian Medical Association Journal, 152, 1423–1433.
- Ten Klooster, P. M., Oostveen, J. C., Zandbelt, L. C., Taal, E., Drossaert, C. H., Harmsen, E. J., & Van De Laar, M. A. (2011). Further validation of the 5-item Perceived Efficacy in Patient-Physician Interactions (PEPPI-5) scale in patients with osteoarthritis. Patient Education and Counseling, 87, 125–130. doi:10.1016/j.pec.2011.07.017
- Unger, J. B., Cabassa, L. J., Molina, G. B., Contreras, S., & Baron, M. (2013). Evaluation of a fotonovela to increase depression knowledge and reduce stigma among Hispanic adults. Journal of Immigrant and Minority Health, 15, 398–406. doi:10.1007/s10903-012-9623-5
- Unger, J. B., Molina, G. B., & Baron, M. (2009). Evaluation of Sweet Temptations, a fotonovela for diabetes education. Hispanic Health Care International, 7(3), 145–152. doi:10.1891/1540-4153.7.3.145
- Williams, M. V., Davis, T., Parker, R. M., & Weiss, B. D. (2002). The role of health literacy in patient-physician communication. Family Medicine, 34(5), 383–389.
- Wolf, M. S., Davis, T. C., Osborn, C. Y., Skripkauskas, S., Bennett, C. L., & Makoul, G. (2007). Literacy, self-efficacy, and HIV medication adherence. Patient Education and Counseling, 65(2), 253–260. doi:10.1016/j.pec.2006.08.006
- Zabrucky, K. M., & Moore, D. (1999). Influence of text genre on adults’ monitoring of understanding and recall. Educational Gerontology, 25(8), 691–710. doi:10.1080/036012799267440
- Zamora, H., & Clingerman, E. M. (2011). Health literacy among older adults: A systematic literature review. Journal of Gerontological Nursing, 37(10), 41–51.