
Abstract
Despite differential uptake of COVID-19 vaccination between Black and non-Hispanic White Americans early in the pandemic, the gap narrowed over time. We tested five hypotheses that could explain the reduction in the disparity. Using a national probability panel of over 1800 individuals surveyed from April 2021 to July 2022, we assessed receipt of recommended doses of COVID-19 vaccines along with (a) reported exposure to deaths due to COVID-19, (b) trust in US health authorities, such as the CDC, (c) knowledge about the safety and efficacy of COVID-19 vaccination, (d) media use as a source of information, and (e) access to COVID-19 vaccines. Only increases in knowledge about the safety and efficacy of COVID-19 vaccines uniquely mediated the increase in vaccination uptake among non-Hispanic Black compared to White, Asian and Hispanic panelists. While trust in CDC and exposure to COVID-19 deaths were related to vaccination acceptance at baseline, those factors were not associated with change in reported vaccination coverage. In addition, neither differential access nor media use explained the increase. Enhanced knowledge about the safety and efficacy of COVID-19 vaccination transmitted from within the Black community likely helped to increase vaccination relative to other racial-ethnic groups.
In the pandemic’s first year, non-Hispanic Black Americans reported lower intentions to receive an eventual COVID-19 vaccine than other racial-ethnic groups (Jamieson et al., Citation2021), a hesitancy that persisted when the vaccines first became available (CDC, Citation2023; Huang et al., Citation2023; Kriss et al., Citation2022; Nguyen, Nguyen, Corlin, Allen, & Chung, Citation2021). The disparity was consistent with longstanding differences in health outcomes between Black and White residents (Brondolo, Kaur, & Flores, Citation2023; Cope, Garrett, & McMorrow, Citation2023; Penner, Albrecht, Coleman, & Norton, Citation2007). These differences have been attributed to unequal access to and treatment by the healthcare system as well as to the psychological effects of racism on the wellbeing of Black individuals (Decoteau & Sweet, Citation2023; Quinn et al., Citation2017). Nevertheless, the primary-series vaccination gap between Black and White non-Hispanic Americans narrowed over time (Kriss et al., Citation2022; Ndugga, Hill, Artiga, & Halder, Citation2022).Footnote1
Although access to vaccination, especially differences in access rooted in socio-economic disparities, was a potential explanation, studies of economic differences between Black and White Americans suggested that factors beyond access were responsible for the disparities (Kriss et al., Citation2022; Mody et al., Citation2022). A national survey conducted late in 2021 also found no evidence of access as a barrier to COVID-19 vaccination by that time (Bonner et al., Citation2023). A panel study from December 2020 to June 2021 observed a steady increase in intentions to vaccinate for COVID-19 among Black respondents to the point where there was no longer a disparity with White respondents (Padamsee et al., Citation2022). Those authors attributed the change to greater perceived importance of receiving the vaccines. However, Black respondents in that panel continued to express concerns about the safety and efficacy of COVID-19 vaccines. Other panel studies during the first months of vaccine availability found that trust in the government’s process of ensuring the safety of vaccines in general and the COVID-19 vaccine in particular was weaker among Black respondents (Na, Banks, & Wang, Citation2023; Nguyen, Nguyen, Corlin, Allen, & Chung, Citation2021).
In line with recommendations for studying vaccination disparities (Cope, Garrett, & McMorrow, Citation2023), identifying the factors that led to the subsequent reduction in the Black-White vaccination gap could help to refine strategies for future efforts either to encourage vaccination against a novel pathogen or a long-standing one, such as seasonal influenza. In this research, we used a national probability panel of American adults to assess one unregistered and four pre-registered hypotheses (https://osf.io/jkzg2/) that could account for the reduction in the COVID vaccination disparity that occurred through July 2022.
Alternative Hypotheses
Awareness of COVID-19 inflicted-death among those one knew: One possible mechanism accounting for increased willingness to vaccinate against COVID-19 was experience with the ill effects of the disease. Black Americans were disproportionately exposed to those risks (American Public Media Research Lab, Citation2023), and this differential exposure could have increased the perceived need for protection provided by vaccination (Padamsee et al., Citation2022; Piltch-Loeb et al., Citation2021; Romer, Winneg, Jamieson, Brensinger, & Jamieson, Citation2022). If this were the case, we would expect greater vaccination to be associated with an increase over time in reported exposure to deaths of persons known to the respondent (Death Hypothesis). We tested this hypothesis by asking about personal exposure to deaths caused by COVID-19.
Lower confidence in public health officials to provide trustworthy information about COVID-19: A second possibility focused on lower levels of perceived trustworthiness of the public health system, especially the Centers for Disease Control and Prevention or CDC. Both historical and actual experience with those authorities have circumscribed such trust among Black Americans (Decoteau & Sweet, Citation2023; Quinn et al., Citation2017; Zelaya, Francis, & Williams, Citation2023). Less trust in the safety of COVID-19 vaccines among Black Americans was also reported in studies early in the vaccination rollout (Huang et al., Citation2023; Nguyen, Nguyen, Corlin, Allen, & Chung, Citation2021). These concerns were explicitly addressed in an op-ed in the New York Times (LaVeist & Benjamin, Citation2021) and in a PSA (National Academy of Medicine, Citationn.d.), in which Black members of the National Academy of Medicine stated that they shared concerns about historic injustices but had examined the evidence and concluded that the vaccines were safe and necessary. Consistent with the Death Hypothesis, these medical experts noted that the virus was disproportionately killing Black Americans. Their messages were placed to reach persons of color in outlets that included Black Entertainment Television (BET), iHeart radio, and Facebook. We tested the hypothesis directly by determining whether respondents’ trust in the advice of the CDC and other health experts increased as the vaccine disparity declined (Trust Hypothesis).
Increase in knowledge about COVID-19 vaccination: Our third possibility focused on knowledge about the safety and efficacy of COVID vaccines. Our measures included both knowledge about the benefits of vaccination (e.g., COVID-19 vaccines are effective in preventing hospitalizations) and rejection of claims unwarranted by existing evidence or cast as false by CDC (Citation2022), typically termed misinformation (e.g., COVID vaccination changes one’s DNA or causes infertility). Lower levels of vaccination knowledge have been associated with resistance to COVID-19 vaccination across the world (Latkin, Dayton, Yi, Konstantopoulos, & Boodram, Citation2021; Loomba, de Figueiredo, Piatek, de Graaf, & Larson, Citation2021; Piltch-Loeb et al., Citation2022). Other studies (Huang et al., Citation2023; Na, Banks, & Wang, Citation2023; Nguyen, Nguyen, Corlin, Allen, & Chung, Citation2021) suggesting that Black Americans had less trust in governmental assurances of vaccine safety did not assess whether this lack of trust was associated with less knowledge about the vaccines. Even if trust in the CDC increased over time, it would be important to know whether this was associated with increased knowledge. We tested the Vaccine Knowledge Hypothesis by assessing respondents’ knowledge about the safety and efficacy of COVID-19 vaccines.
Exposure to pro-vaccination messages in media: A fourth possibility was that Black Americans had increased exposure to media that supported vaccination, such as broadcast national TV news, than to sources such as conservative media outlets that were more likely to cultivate conspiracy beliefs and carry misinformation about vaccination (Motta, Stecula, & Farhart, Citation2020; Motta and Stecula, Citation2023; Romer & Jamieson, Citation2023) (Media Exposure Hypothesis). Media directed to Black audiences (e.g., BET) which carried pro-vaccination content (Roberts, Citation2022) also might have motivated greater acceptance of vaccination. We tested this hypothesis by assessing use of major sources of information in the media that differed in their support for vaccination.
Increased access to COVID-19 vaccines: Because researchers at CDC suggested that “programmatic efforts to provide equitable access to COVID-19 vaccines might have contributed to closing the coverage gap” (Kriss et al., Citation2022), we assessed this possibility in addition to our pre-registered hypotheses (Access Hypothesis).
To test these hypotheses, we examined changes in reported coverage with the primary COVID-19 vaccination series (two mRNA vaccinations or one Johnson & Johnson shot) from June 2021 to July 2022, by which time disparities between Black and White adults had narrowed. Comparing time-trends in vaccination with measures relevant to our various hypotheses enabled us to assess each hypothesis.
Methods
Sample
To test our hypotheses, we relied on data from the Annenberg Science and Public Health (ASAPH) survey collected from April 2021 to July 2022. As previously described (Romer, Winneg, Jamieson, Brensinger, & Jamieson, Citation2022), these data were collected from a nationally representative probability panel drawn randomly from the SSRS Opinion Panel of U.S adults (including Hawaii and Alaska). Additionally, hard-to-reach demographic groups were recruited via an SSRS nationally representative (including Hawaii and Alaska) bilingual telephone survey.
Of the 3,476 U.S. adult panelists invited to participate in wave 1 of the survey, 1,941 completed the first wave of the survey (56% completion rate). The majority completed it online (96%) rather than by telephone (4%) and in English (98%) rather than Spanish (2%). The original 1,941 panelists were re-contacted at each subsequent wave. Post-wave 1 panelist completion rates were high, averaging 85% at each wave and have remained high in subsequent waves 2 through 7. Supplementary Table A shows the fielding dates at each wave and the sample sizes.
During this time, the panel members were not selected for any other studies conducted by SSRS and are considered proprietary. Panelists were compensated the equivalent of $15 for their time at each survey wave. The median length of the surveys was 20 minutes. The survey was deemed exempt from review by the Institutional Review Board of the University of Pennsylvania.
Sample Demographics. displays the distribution of the racial-ethnic groups and other demographic characteristics of the sample at each of the seven waves of the panel, confirming that this distribution was stable over the course of the study. Supplementary Table B shows the demographic distributions of the five racial-ethnic groups. Black respondents tended to be younger, more female, to have lower income, and to identify more with the Democratic party and with Evangelical Christians than White respondents.
Table 1. Percentage of sample by demographics by panel wave (unweighted)
Measures
COVID-19 Vaccination: Our main dependent variable was whether a respondent reported receiving the primary series of CDC-approved COVID-19 vaccinations. At each wave, respondents were asked (a) if they had been vaccinated, (b) if so, which vaccine had they received, and (c), if the Moderna or Pfizer vaccine, whether they had received the second dose. Individuals were coded as having completed the primary series if they received the single dose of the Johnson & Johnson vaccine or both primary series doses of either mRNA vaccines (Moderna or Pfizer). For mRNA vaccines, we coded receipt of the first dose as 1, the second dose as 2 and not having received either as 0. For Johnson & Johnson, a single dose was coded as 2.
Exposure to COVID-19 death: The survey asked respondents “How many, if any, people have you known personally who died from COVID-19.” This variable was collapsed to a binary indicating whether respondents knew a person who died from COVID-19. The survey also asked how worried respondents were about the virus infecting their family (from “not at all” to “very much”).
Trust in Health Authorities: For the trust hypothesis, the survey asked respondents “how confident, if at all, you are that the CDC is providing the public with trustworthy information about means of preventing and treating COVID-19.” Respondents reported confidence on a four-point scale (from “Not at all confident” to “Very confident”). These ratings were highly correlated across time (r’s ranged from .69 to .82) and were highly related to confidence in the FDA (.70 to .86) and in Dr. Anthony Fauci of the NIH (.78 to .84).
Vaccination knowledge Hypothesis: Knowledge concerning the safety and efficacy of COVID-19 and other vaccines was derived from a battery of items scored for accuracy based on alignment with statements by the CDC (Citation2022). The survey asked many different items across waves, but the ones on which we focus here were the 5–11 that have been found to predict resistance to vaccination for COVID-19 (Jamieson et al., Citation2021; Loomba, de Figueiredo, Piatek, de Graaf, & Larson, Citation2021; Romer, Winneg, Jamieson, Brensinger, & Jamieson, Citation2022). The items and waves in which those questions were asked are reported in . Endorsing statements that were true or failing to endorse ones that were false was categorized as higher level of knowledge. With one exception, each item was presented as a statement to which respondents responded on a 4-point scale (from ``Definitely false’“to ``Definitely true”’). Those reporting that they were not sure were coded in the middle of the resulting 5-point scale.
Table 2. Measures of knowledge, wave of assessment, and truth status
Exploratory analysis confirmed that all items loaded primarily on the first principal component at each wave, supporting their use as a measure of knowledge (alpha’s ranged from .83 to .93). We used standardized scores derived from those analyses at each wave because raw scores could change due to changes in the items assessed at each wave. We were primarily interested in relative changes in knowledge across time and groups, which would be evident by standardizing at each wave.
Media use: The survey measured self-reported media use on a five-point scale (from “Never” to “All the time”), where respondents were asked if they get information from different media sources, such as [a] Fox News (i.e, conservative news and opinion); [b] Newsmax, One America News, Gateway Pundit, Parler or Telegram (i.e., “ultra-conservative” news and opinion); [c] CBS, NBC, or ABC News (i.e., national broadcast TV news); [d] the Associated Press, The Wall Street Journal, or The New York Times (i.e., mainstream national newspapers); [e] Facebook, Instagram, or Twitter (i.e., social media); [f] Univision; and [g] Black Entertainment Television (BET), OWN, TV One, Bounce, or the Root (media directed to non-White audiences).
For the access hypothesis, the survey asked whether unvaccinated respondents reported having the opportunity to get a COVID-19 vaccine (yes or no) over the first four waves of the study.
Analysis
To simplify the analysis, we focused on the period from June 2021 to July 2022 (waves 2 to 7) since the changes that occurred in vaccination for Black and White respondents over that time span shown in were largely linear in form and changes after July 2022 were small. We defined a latent growth curve model using structural equation modeling as implemented in Mplus that allowed us to examine changes in the intercepts and slopes of vaccination as a function of differences in intercepts and slopes of deaths due to the pandemic, trust in the CDC, and knowledge about COVID-19 vaccination. Predictors also included differential media use as related to each of four racial-ethnic groups. As we show below, reported access did not differ between the groups and was not included in the model.
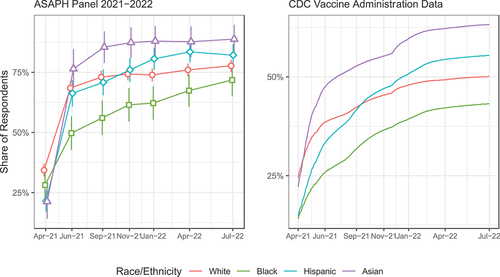
Figure 1. Estimates of COVID-19 primary series vaccination by racial-ethnic identity: (a) as measured by the ASAPH panel; and (b) as reported by CDC administrative data (CDC, Citation2023).
We employed full-information likelihood imputation as implemented in Mplus for missing scores across waves under the assumption that the data were missing at random. We also employed bootstrapping with 1000 samples to determine confidence intervals (CIs) for all parameters in the model. We retained parameters in the final model that reached at least 90% confidence, and we report 99% and where relevant 95% CIs for all parameters. For ease of interpretation, we report standardized parameters for all paths in the model.
Data Availability. A replication dataset is available at https://osf.io/jkzg2/
Results
As seen in , both our national panel and the tracking by CDC show a narrowing in the gap in vaccination by Black and White individuals from June 2021 to July 2022. We first present the overall trends for each hypothesis and then conduct the growth curve analysis to formally test each hypothesis.
Death Hypothesis
As would be expected, there were increases in reported exposure to COVID-19- caused deaths over time (). These increases did not differ by race or ethnicity. However, Black and Hispanic respondents reported more exposure to deaths overall than did White respondents, reflecting disparities in impact of the pandemic along racial and ethnic lines. Changes in reported worry were not differentially elevated among Black respondents (see Supplementary Table C).
Table 3. Percentage of respondents knowing someone who died as a result of COVID-19 with significant differences compared to non-Hispanic White respondents by racial-ethnic group and wave
Trust Hypothesis
As seen in , Black and White respondents did not differ in trust at the outset of the survey, and there was no differential change in trust as a function of race or ethnicity. We also examined reported discussion with a personal care provider at waves 4 and 5, and while this was related to greater experience of deaths (r’s of about .12), it was unrelated to any other factors in our model.
Table 4. Reported trust in the Centers for Disease Control and Prevention (CDC) by wave and racial-ethnic group (1–4 scale)
Knowledge Hypothesis
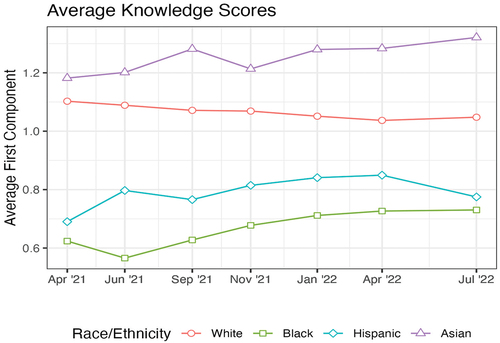
provides the average value of the knowledge scores by racial-ethnic group across the seven waves of our panel. The slopes of these scores were different for Black versus White respondents, with Black respondents increasing in knowledge (p < .001) and White respondents showing a small statistically insignificant decrease (p > .1). The rise in knowledge among Asian respondents was not statistically reliable apart from demographic controls.
Figure 2. Knowledge scores by race-ethnicity and wave.
Media Use
Tests of differences in media use are displayed in . Black respondents tended to use national broadcast TV news, social media, CNN and media directed to Black audiences to a greater degree than did White respondents. This pattern was largely similar for Hispanic respondents, with the exception that they were even more likely to use Univision. Asian respondents were distinguished by greater use of national newspapers.
Table 5. Means for media use by racial-ethnic groups with significant differences from White respondents (0 to 4 scale)
Access Hypothesis
We tested for racial disparities in self-reported access to COVID-19 vaccines. As shown in , at no point during the first year of COVID-19 vaccine availability were unvaccinated Black or Hispanic respondents less likely to report having the opportunity to get vaccinated.
Table 6. Percentage reporting availability of COVID-19 vaccination across the first four waves among those still not vaccinated at each wave with significant differences from White respondents
Growth Curve Model
Our growth curve analysis is based on the 1861 respondents who completed at least two waves of the survey. The final model after dropping paths that did not reach 90% confidence is shown in . The model provided an excellent fit to data as indicated by low RMSEA (.043, 90% CI = .042, .045), high CFI (.953) and low SRMR (.038). Further details about the parameters in the final model are in .
Figure 3. Structural model of standardized weights for factors underlying changes in vaccination between Black and White respondents over time.
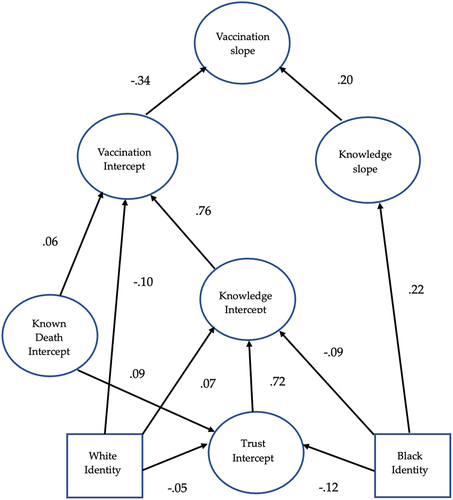
Table 7. Direct predictors of latent variables in Figure 3 with 99% confidence intervals
We first examine differences in vaccination at intercept. Vaccination intercepts were negatively related to vaccination slopes (−.34, 99% CI = −.62, −.25), reflecting the limits imposed by ceiling effects. There were several direct predictors of vaccination intercepts. Consistent with the Knowledge Hypothesis, the strongest predictor was intercepts in knowledge, which were positively related to vaccination intercepts (.76, 99% CI = .70, .79). In addition, Black respondents were less knowledgeable (−.086, 99% CI = −.141, −.026,) while White respondents were more so (.065, 99% CI = .028, .107). Consistent with the Death Hypothesis, reported exposure to deaths was directly and positively related to vaccination at intercept (.055, 99% CI = .006, .101). Aside from these factors, differences in age, use of media such as Fox News, and being White also were related to vaccination intercepts (see ).
Notably, with differences in knowledge and reported exposure to deaths controlled, Black respondents were not less likely to be vaccinated at intercept than others, while White respondents were less likely to be vaccinated. In addition, controlling for age and White identity as well as knowledge, users of media outlets such as Fox News were more likely to be vaccinated.
Differences in knowledge were also strongly and positively related to trust at intercept (.72, 99% CI = .66, .76). However, controlling for other factors, such as education, gender, age, political identity, and use of various sources of information, both Black and White respondents reported less trust in the CDC. Nevertheless, the relation was more than twice as strong for Black respondents. Trust was also directly related to reported exposure to COVID-19 deaths (.087, 99% CI = .035, .135), with those reporting more exposure also being more trusting of the CDC.
The only direct demographic predictors of differences in reports of death at intercept were identification as an Evangelical or as a woman, with each of those reporting more COVID-19 deaths of persons known to them.
Consistent with the Media Use Hypothesis, users of ultra-conservative outlets such as Newsmax reported both less knowledge and less trust in the CDC, while users of national newspapers reported the opposite. Consumers of national broadcast TV tended to be more trusting, while users of Fox News were less so. Users of BET and other outlets that focus on non-White audiences as defined above also reported less knowledge but more trust in CDC. Nevertheless, the correlations between race-ethnicity and media use in show the largest difference in media use between Black and White respondents was for BET and other outlets directed at nonwhite audiences. But the relation of these media to either trust or knowledge was too small to affect disparities in vaccination. The same was the case for differences in use of national TV news, which tended to be used more by Black than White respondents.
Table 8. Correlations between racial-ethnic groups and variables in the model that exceeded 99% confidence intervals
Regarding change in vaccination status, the only direct predictor was the slope of knowledge (.20, 99% CI = .04, .61), supporting the hypothesis that changes in this factor were predictive of changes in vaccination. In support of the Knowledge Hypothesis, Black respondents tended to endorse greater knowledge over time than did other racial-ethnic groups. This change led to a significant indirect positive relation with vaccination slopes (.043, 99% CI = .003, .196). Because intercepts of vaccination were negatively related to slopes of vaccination, negative predictors of vaccination intercept were also positively related to vaccination slopes. Two of these indirect paths going from Black identity to trust and knowledge produced an additional indirect relation of .033. However, these paths also were associated with increases in vaccination among White respondents (.024, 99% CI = .003, .052). Thus, the disparity attributable to intercepts was small. In total, the sum of the indirect relations for Black respondents (.076, 99% CI = .025, .243) was significant, with about 57% of the change in slope attributable to change in knowledge. These indirect relations contrast with those attributable to White identity, which were only mediated by differences in vaccination intercepts and were less than a third as large in total (.024 vs. .076).
Changes in vaccination for Asian and Hispanic groups were driven by differences in vaccination intercepts, which tended to be inversely related to increases in vaccination and reflected the overall increase in vaccination that occurred during the study period.
The model accounted for 59% of the variation in vaccination intercepts and 16% of the variation in vaccination slopes. Thus, the factors in the model did much better in accounting for vaccination differences in June of 2021 than they did for changes over the following year. Nevertheless, the model did account for changes between Black versus White group vaccination over time.
We also tested the model with only Black and White panel members to ensure that the findings were robust when only those two groups were compared. In that case, the relation between the slopes of knowledge and vaccination was even stronger (.273) and the indirect relation with Black identity also stronger (.08). Thus, the findings cannot be attributed to the inclusion of other racial-ethnic groups in the analysis.
Discussion
We tested four preregistered hypotheses and one that was not that could explain the decline in the disparity in vaccination between Black and White Americans from June 2021 to July 2022. While both trust in the CDC and exposure to COVID-19-related deaths were related to vaccination uptake at baseline, changes in these factors over the study period did not predict changes in vaccination for any of the racial-ethnic groups. Nor was there evidence to indicate that Black respondents gained access to vaccination at a greater rate. Although we found evidence for differential media use, it did not predict differential vaccination uptake. Differential increase in knowledge was the strongest predictor.
We tested the knowledge hypothesis by examining changes in items that have been shown previously to correlate highly with COVID-19 vaccination (Loomba, de Figueiredo, Piatek, de Graaf, & Larson, Citation2021, Jamieson et al., Citation2021; Romer, Winneg, Jamieson, Brensinger, & Jamieson, Citation2022). The increased convergence in Black and White individuals’ vaccination status for the primary COVID-19 series over the period from June 2021 to July 2022 was attributable to the differential increase in specific CDC-consistent knowledge about the safety and efficacy of COVID-19 and other vaccines. As a result of this change, the total relation between Black identity and change in vaccination was more than 3 times larger than for White respondents.
Although we did not oversample Black respondents, our findings are consistent with other national surveys and especially CDC (Citation2023) tracking of vaccination rates shown in . Our findings are also consistent with surveys by Padamsee et al. (Citation2022) and Na, Banks, and Wang (Citation2023), which found disparities in global beliefs about the safety and efficacy of COVID-19 vaccines earlier in the rollout when racial-ethnic differences in vaccine receipt were larger. However, our trend analyses showed that the change in belief about vaccines was attributable to change in knowledge about the vaccines rather than to changes in trust in the CDC. As we discuss below, our findings suggest that efforts within local Black communities that bolstered greater knowledge about COVID vaccines were likely to be responsible for the changes in vaccine uptake.
Other sources of change in vaccination were mediated by baseline differences in vaccination which tended to be inversely related to later increases. For example, Black respondents were more likely to have less knowledge at baseline which was also related to lower vaccination levels at baseline. However, lower vaccination at baseline was positively related to change in vaccination owing to the greater opportunity for increases and the general rise in vaccination over time. The general uptake of vaccination across groups tended to benefit those who lagged at the early part of the vaccine rollout. Therefore, most of the racial-ethnic differences in the uptake over time were attributable to those early differences. Nevertheless, for Black panel members, subsequent change in vaccination also was linked to increased knowledge over time.
Black respondents benefited as well from greater exposure to national TV news while the opposite was the case for White respondents. This finding is consistent with a panel study that found greater confidence in COVID vaccination associated with increasing exposure to the national government-sponsored vaccination campaign (Kranzler et al., Citation2023). While exposure to the national campaign on social media was also associated with greater vaccination (Williams et al., Citation2023), neither this media use or any other was strong enough to produce reported vaccination differences between Black and White respondents. For example, even though Black respondents were more likely to use BET and other outlets directed to non-White audiences, the relation between BET use and knowledge was too small to make much difference. The same was true for use of national TV and social media. One media influence not assessed was exposure to local Black-owned newspapers which may have played a role in reducing misinformation about vaccination (Upshaw & Davis, Citation2022; Upshaw, Davis, Love, & Almalki, Citation2023)
Although we lack the survey items needed to assess their role, clergy and medical providers within the Black community may well have had influence. Previous research has found that when Black men are advised to obtain a flu shot from a racially congruent medical provider, they are more likely to accept the advice (Alsan, Garrick, & Graziani, Citation2019). In addition, when Black persons were advised about the importance of vaccination for COVID from a Black physician, they were more likely to report seeking further information about the vaccine (Alsan et al., Citation2021). We did not find that respondents’ primary care providers had much influence in increasing vaccination, but local medical professionals in combination with clergy may have helped to dispel misinformation about the safety of Covid vaccines. A Pew survey found that Black church attenders had the highest rates of vaccination among church goers in the US (Kramer, Citation2021). A case study of Black clergy in South Carolina detailed the ways in which the ministry counteracted distrust of the medical system and promoted acceptance of COVID-19 vaccination (Moore et al., Citation2022). A review of efforts to increase vaccination among Black people worldwide suggested that communication from within trusted members of the community was the most successful strategy (Adeagbo et al., Citation2022).
Other Sources of Disparity
It is likely that some of the reduction in disparity was the result of greater resistance to vaccination among some segments of the White population. A study of differences in state vaccination rates across time found that vaccination hesitancy and overt resistance decreased over time for states with greater proportions of Black residents but remained unchanged in states with greater proportions of White residents (Morales & Paat, Citation2022).
Belief in conspiracy theories also has been associated with skepticism toward vaccination and resistance to vaccination for COVID (Romer & Jamieson, Citation2022). Republicans and White Evangelical Christians have tended to be more exposed to conservative media that promoted conspiracy theories and misinformation about the pandemic (Motta, Stecula, & Farhart, Citation2020; Romer & Jamieson, Citation2022). Black Americans are also less likely to endorse moral values that are more common among the politically conservative (e.g., respect for authority and body purity), which are also linked to greater hesitancy (Nan et al., Citation2022). Consistent with these patterns, White Americans in this study identified more with the Republican party and were less exposed to mainstream media that tended not to promote conspiracy theories and misinformation to the same degree as conservative media (). We also observed a slight but statistically nonsignificant decrease in knowledge among White respondents over the course of the study ().
Limitations
While we present results addressing our pre-registered hypotheses, we deviated from the initial analysis plan by using a growth curve model that allowed us to identify mediators of change in vaccination coverage. This analysis used change in a three-point outcome, which resembles a count score. We used bootstrapping to estimate confidence intervals for all model parameters, a procedure that overcomes deviations from normally distributed outcomes (Efron, Ragosa, & Tibshirani, Citation2004). We also conducted the analysis using a survival model which replicated the finding that knowledge predicted differences in vaccination between Black and other groups over time (see Supplementary Table D).
Finally, although we showed that changes in knowledge uniquely explained changes in vaccination, we cannot know conclusively that this factor was responsible for the change. There could be other factors that actually produced the vaccination change, with knowledge serving to rationalize the true reason for increased reported vaccination. However, we were able to control for the general rise in vaccination that occurred for all groups, which could be a source of such rationalization. These controls along with a wide range of demographic and experience-based measures suggest that knowledge did play a role.
Conclusions
Greater specific knowledge about the safety and efficacy of COVID-19 vaccines authorized for use in the US was associated with greater uptake of those vaccines among Black respondents, paralleling the reduction in Black-White vaccination disparities as the rollout proceeded. Efforts to increase confidence in COVID-19 vaccination within the Black community may have facilitated this increased acceptance resulting in a modest success for the COVID-19 vaccination campaign in the US. The findings suggest that exposure to knowledge about vaccine safety and efficacy from trusted sources may have overcome at least some of the effects of mistrust of governmental health authorities in the Black community historically linked to lower vaccination confidence.
Supplemental Material
Download MS Word (31.6 KB)Supplementary material
Supplemental data for this article can be accessed online at https://doi.org/10.1080/10810730.2024.2354360.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Correction Statement
This article has been republished with minor changes. These changes do not impact the academic content of the article.
Additional information
Funding
Notes
1 From this point onward, we refer to White, Black, Asian, and other racial groups as non-Hispanic in identity and recognize that these designations combine many different ethnic and cultural subgroups (cf. Agyemang, Citation2005; Hunt, Schneider, & Akdağ, Citation2004). We also use Black-White differences in vaccination as the primary measure of vaccination disparity as is traditional in studies of disparities in population health (Cope, Garrett, & McMorrow, Citation2023; Nguyen, Nguyen, Corlin, Allen, & Chung, Citation2021).
References
- Adeagbo, M., Olukotun, M., Musa, S., Alaazi, D., Allen, U. … Salami, B. (2022). Improving COVID-19 vaccine uptake among black populations: A systematic review of strategies. International Journal of Environmental Research and Public Health, 19(19), 11971. doi:10.3390/ijerph191911971
- Agyemang, C. (2005). Negro, Black, Black African, African Caribbean, African American or what? Labelling African origin populations in the health arena in the 21st century. Journal of Epidemiology & Community Health, 59(12), 1014–1018. doi:10.1136/jech.2005.035964
- Alsan, M., Garrick, O., & Graziani, G. (2019). Does diversity matter for health? Experimental evidence from Oakland. American Economic Review, 109(12), 4071–4111. doi:10.1257/aer.20181446
- Alsan, M., Stanford, F. C., Banerjee, A., Breza, E., Chandrasekhar, A. G. & Duflo, E. (2021). Comparison of knowledge and information-seeking behavior after general COVID-19 public health messages and messages tailored for black and latinx communities: A randomized controlled trial. Annals of Internal Medicine, 174(4), 484–492. doi:10.7326/M20-6141
- American Public Media Research Lab. (2023). The color of coronavirus: COVID-19 deaths by race and ethnicity in the U.S. American Public Media. Retrieved from https://www.apmresearchlab.org/covid/deaths-by-race
- Bonner, K. E., Vashist, K., Abad, N. S., Kriss, J. L., Meng, L. … Singleton, J. A. (2023). Behavioral and Social Drivers of COVID-19 Vaccination in the United States, August–November 2021. American Journal of Preventive Medicine, 64(6), 865–876. doi:10.1016/j.amepre.2023.01.014
- Brondolo, E., Kaur, A., & Flores, M. (2023). Structural racism and health in the age of COVID-19: A selective review with policy implications. Social Issues and Policy Review, 17(1), 34–61. doi:10.1111/sipr.12095
- CDC. (2022, July 20). Myths and facts about COVID-19 vaccines. Retrieved from https://www.cdc.gov/coronavirus/2019-ncov/vaccines/facts.html#:~:text=MYTH%3A%20A%20COVID%2D19%20vaccine,you%20sick%20with%20COVID%2D19
- Centers for Disease Control and Prevention. (2023). COVID-19 vaccination demographics in the United States. Department of Health Education and Welfare. Retrieved from https://covid.cdc.gov/covid-data-tracker/#vaccination-demographics-trends
- Cope, L. C., Garrett, B., & McMorrow, S. (2023). How should we measure and interpret racial and ethnic disparities in health care?. Washington, DC: Urban Institute.
- Decoteau, C. L., & Sweet, P. L. (2023). Vaccine hesitancy and the accumulation of distrust. Social Problems. doi:10.1093/socpro/spad006
- Efron, B., Ragosa, D., & Tibshirani, R. (2004). Resampling methods of estimation. In N. J. Smelser & P. B. Baltes (Eds.), International encyclopedia of the social and behavioral sciences (13216–13220). Pergamon Press, Oxford, UK: Elsevier.
- Huang, Q., Abad, N., Bonner, K. E., Baack, B., Petrin, R., & Brewer, N. T. (2023). Explaining demographic differences in COVID-19 vaccination stage in the United States--April-May 2021. Preventive medicine, 166, 107341. doi:10.1016/j.ypmed.2022.107341
- Hunt, L. M., Schneider, S., & Akdağ, B. (2004). Should “acculturation” be a variable in health research? A critical review of research on US hispanics. Social Science and Medicine, 59(5), 973–986. doi:10.1016/j.socscimed.2003.12.009
- Jamieson, K. H., Romer, D., Jamieson, P. E., Winneg, K. M., & Pasek, J. (2021). The role of non-COVID and COVID-specific factors in predicting a shift in willingness to vaccinate: A panel study. Proceedings of the National Academy of Science, 118(52), e2112266118. doi:10.1073/pnas.2112266118
- Kramer, S. (2021). In historically Black protestant churches, regular attenders more likely to have received COVID-19 shot. Pew Research Center. Retrieved from https://www.pewresearch.org/fact-tank/2021/10/15/in-historically-black-protestant-churches-regular-attenders-more-likely-to-have-received-covid-19-shot/
- Kranzler, E. C., Luchman, J. N., Williams, C. J., Model, T. A., Ostby, R. & Peck, J. (2023). Recalled exposure to COVID-19 public education campaign advertisements predicts COVID-19 vaccine confidence. Journal of Health Communication, 28(3), 144–155. doi:10.1080/10810730.2023.2181891
- Kriss, J. L., Hung, M.-C., Srivastav, A., Black, C. L., Lindley, M. C. … Singleton, J. A. (2022). COVID-19 vaccination coverage, by race and ethnicity — National Immunization Survey Adult COVID Module, United States, December 2020–November 2021. MMWR: Morbidity and Mortality Weekly Report, 71(23), 757–763. doi:10.15585/mmwr.mm7123a2
- Latkin, C. A., Dayton, L., Yi, G., Konstantopoulos, A., & Boodram, B. (2021). Trust in a COVID-19 vaccine in the U.S.: A social-ecological perspective. Social Science & Medicine, 270, 113684. doi:10.1016/j.socscimed.2021.113684
- LaVeist, T. A., & Benjamin, G. C. (2021, February 7). 60 black health experts urge black Americans to get vaccinated. New York Times. https://www.nytimes.com/2021/02/07/opinion/covid-black-americans.html
- Loomba, S., de Figueiredo, A., Piatek, S. J., de Graaf, K., & Larson, H. J. (2021). Measuring the impact of COVID-19 vaccine misinformation on vaccination in the UK and USA. Nature Human Behavior, 5(3), 337–348. doi:10.1038/s41562-021-01056-1
- Mody, A., Bradley, C., Redkar, S., Fox, B., Eshun-Wilson, I. … Geng, E. H. (2022). Quantifying inequities in COVID-19 vaccine distribution over time by social vulnerability, race and ethnicity, and location: A population-level analysis in St. Louis and Kansas City, Missouri. PloS Medicine, 19(8), e1004048. doi:10.1371/journal.pmed.1004048
- Moore, D. Mansfield, L. N. Onsomu, E. O. & Caviness-Ashe, N.(2022). The role of black pastors in disseminating COVID-19 vaccination information in black communities in South Carolina. International Journal of Environmental Research Public Health, 19, 8926. doi:10.3390/ijerph19158926
- Morales, D. X., & Paat, Y.-F. (2022). Hesitancy or resistance? Differential changes in COVID-19 vaccination intention between Black and White Americans. Journal of Racial and Ethnic Health Disparities, 11(1), 23–35. doi:10.1007/s40615-022-01494-1
- Motta, M., & Stecula, D. A. (2023). The effects of partisan media in the face of global pandemic: How news shaped COVID-19 vaccine hesitancy. Political Communication, 40(5), 505–526. doi:10.1080/10584609.2023.2187496
- Motta, M., Stecula, D. A., & Farhart, C. (2020). How right-leaning media coverage of COVID-19 facilitated the spread of misinformation in the early stages of the pandemic in the U.S. Canadian Journal of Political Science, 53(2), 335–342. doi:10.1017/S0008423920000396
- Na, L., Banks, S., & Wang, P. (2023). Racial and ethnic disparities in COVID-19 vaccine uptake: A mediation framework. Vaccine, 41(14), 2404–2411. doi:10.1016/j.vaccine.2023.02.079
- Nan, X., Wang, Y., Thier, K., Adebmowo, C., Quinn, S., & Ntiri, S. O. (2022). Moral foundations predict COVID-19 vaccine hesitancy: Evidence from a national survey of Black Americans. Journal of Health Communication, 27(11–12), 801–811. doi:10.1080/10810730.2022.2160526
- National Academy of Medicine. (n.d.). Promoting COVID-19 vaccination uptake in communities of color. Retrieved from https://nam.edu/promoting-vaccination-uptake-english/
- Ndugga, N., Hill, L., Artiga, S., & Halder, S. (2022). Latest data on COVID-19 vaccinations by race/ethnicity. Kaiser Family Foundation. Retrieved from https://www.kff.org/coronavirus-covid-19/issue-brief/latest-data-on-covid-19-vaccinations-by-race-ethnicity/
- Nguyen, K. H., Nguyen, K., Corlin, L., Allen, J. D., & Chung, M. (2021). Changes in COVID-19 vaccination receipt and intention to vaccinate by socioeconomic characteristics and geographic area, United States, January 6—March 29, 2021. Annals of Medicine, 53(1), 1419–1428. doi:10.1080/07853890.2021.1957998
- Padamsee, T. J., Bond, R. M., Dixon, G. N., Hovick, S. R., Na, K. & Garrett, R. K. (2022). Changes in COVID-19 vaccine hesitancy among black and white individuals in the US. JAMA Network Open, 5(1), e2144470. doi:10.1001/jamanetworkopen.2021.44470
- Penner, L. A., Albrecht, T. L., Coleman, D. K., & Norton, W. E. (2007). Interpersonal perspectives on black-white health disparities: Social policy implications. Social Issues and Policy Review, 1(1), 63–98. doi:10.1111/j.1751-2409.2007.00004.x
- Piltch-Loeb, R., Savoia, E., Goldberg, B., Hughes, B., Verhey, T. & Gesser-Edelsburg, A. (2021). Examining the effect of information channel on COVID-19 vaccine acceptance. Public Library of Science ONE, 16(5), e9251095. doi:10.1371/journal.pone.0251095
- Piltch-Loeb, R., Su, M., Bonetti, M., Testa, M., Stanton, E., Toffolutti, V., & Savoia, E. (2022). Cross-national vaccine concerns and predictors of vaccine hesitancy in not-fully vaccinated individuals: Findings from USA, Canada, Sweden, and Italy. Vaccines, 10(1652), 1–19. doi:10.3390/vaccines10101652
- Quinn, S. C., Jamison, A., Freimuth, V. S., An, J., Hancock, G. R., & Musa, D. (2017). Exploring racial influences on flu vaccine attitudes and behavior: Results of a national survey of white and African American adults. Vaccine, 35(8), 1167–1174. doi:10.1016/j.vaccine.2016.12.046
- Roberts, N. (2022, April 28). Give your community a boost: CDC makes a push to end COVID-19 and get us back to a new normal. Retrieved from https://www.bet.com/article/3hq0ev/cdc-promotes-covid-19-vaccines-boosters-in-black-community
- Romer, D., & Jamieson, K. H. (2022). Conspiratorial thinking as a precursor to opposition to COVID-19 vaccination in the US: A multi-year study from 2018 to 2021. Scientific Reports, 12(1), 18632. doi:10.1038/s41598-022-22014-5
- Romer, D., & Jamieson, K. H. (2023). The role of conspiracy mindset in reducing support for child vaccination for COVID-19 in the United States. Frontiers in Psychology, 14(1175571). doi:10.3389/fpsyg.2023.1175571
- Romer, D., Winneg, K. M., Jamieson, P. E., Brensinger, C., & Jamieson, K. H. (2022). Misinformation about vaccine safety and uptake of COVID-19 vaccines among adults and 5-11-year-olds in the United States. Vaccine, 40(45), 6463–6470. doi:10.1016/j.vaccine.2022.09.046
- Upshaw, S. J., & Davis, O. I. (2022). Centering survival as cultural strategy: Black newspapers’ cultural descriptions of the coronavirus pandemic. Journal of Applied Communication Research, 50(5), 478–496. doi:10.1080/00909882.2022.2120367
- Upshaw, S. J., Davis, O. I., Love, B., & Almalki, S. (2023). Using cultural variance framework to promote vaccine confidence among African Americans: A qualitative content analysis of “we can do this” COVID-19 campaign. Howard Journal of Communication. doi:10.1080/10646175.2023.2263211
- Williams, C. J., Kranzler, E. C., Luchman, J. N., Denison, B., Fisher, S. … Peck, J. F. A. (2023). The initial relationship between the United States Department of Health and Human Services’ digital COVID-19 public education campaign and vaccine uptake: Campaign effectiveness evaluation. Journal of Medical Internet Research, 25, e43873. doi:10.2196/43873
- Zelaya, C. M., Francis, D. B., & Williams, L. B. (2023). Understanding COVID-19 vaccine knowledge, beliefs, and trusted information sources among black women in Kentucky: Implications for vaccine uptake. Journal of Health Communication, 28(10), 680–688. doi:10.1080/10810730.2023.2252367
