
Abstract
Background: There is no known risk-free level of alcohol use in pregnancy. Despite this, many still believe that occasional drinking is safe. To-date, there is limited evidence of the influences on women’s decisions about low to moderate alcohol use in pregnancy. The aim of this study was to explore alcohol use intentions during pregnancy, using variables from the theory of planned behavior, the prototype/willingness model and personality variables. The study also investigated whether priming participants with exposure to prototypes describing different alcohol use behaviors had an impact on intentions.
Methods: Participants, 746 women aged 20 to 45 years, were randomized to be prompted to think of one of two different “types” of behaviors, i.e., small level of alcohol use in pregnancy and ambiguous level of alcohol use in pregnancy. They then completed measures of theoretical variables, impulsivity, venturesomeness, and self-efficacy. Participants then answered whether they intended to use alcohol during a future pregnancy.
Results: Over half of the variance in intentions to consume alcohol while pregnant were predicted by the final model (R2= .527, F (1, 438) = 13.201, p < .001). Positive attitudes toward alcohol use in pregnancy, from the theory of planned behavior, were the most significant predictor of intentions and intentions did not differ between groups according to prototype exposure.
Conclusions: Future research should aim to explore the efficacy of interventions to reduce low to moderate alcohol use in pregnancy that utilize both the theory of planned behavior and prototype/willingness model to target determinants of intentions.
Introduction
Alcohol use during pregnancy
Alcohol exposure in utero can impact on a child’s development in many ways (Khalid et al., Citation2014), including adversely impacting brain development (Ornoy & Ergaz, Citation2010). In particular, evidence suggests that, for 1 in 13 children, prenatal exposure to alcohol develops into Fetal Alcohol Spectrum Disorder, a disorder characterized by severe impairments in multiple domains of cognitive and physical functioning (Popova et al., Citation2017). As there is no known safe level of prenatal alcohol exposure, it is commonly recommended that no alcohol use during pregnancy is safest (Department of Health, Citation2016; National Health & Medical Research Council, Citation2020). However, the evidence for harm associated with low levels of alcohol use during pregnancy is mixed (Comasco et al., Citation2018), in part due to methodological issues, including a lack of consistency in how alcohol use in pregnancy is measured.
Importantly, the mixed evidence for low to moderate alcohol use during pregnancy, does not mean that there is evidence of limited harm (Mamluk et al., Citation2017) or that there is a level at which drinking alcohol while pregnant can be considered risk-free. Nonetheless, prior research into determinants has largely focused on heavy alcohol use, with little evidence for determinants of low to moderate alcohol use in pregnancy (Roozen et al., Citation2017). In addition to perceived risk, the importance of social context is increasingly being recognized in relation to alcohol use decisions during pregnancy. In particular, prior research has documented that women experience peer pressure to drink alcohol while pregnant (Meurk et al., Citation2014), and that friends and family are influential in their decision making (Gouilhers et al., Citation2019). Additionally, a recent study found that of those who reported drinking alcohol during pregnancy over half drank on “special occasions” only (Tsang et al., Citation2021), suggesting that social environments may be particularly conducive to alcohol use in pregnancy.
The theory of planned behavior
The theory of planned behavior (TPB), which has been used extensively to predict individuals’ alcohol use (Cooke et al., Citation2016), states that an individual’s behavior is predicted by their behavioral intention which is predicted by attitudes, subjective norms, and perceived behavioral control (Ajzen, Citation1991). Attitude is the overall positive or negative evaluation an individual makes about the behavior. Subjective norms reflect the extent of social pressure experienced, while perceived behavioral control is the overall evaluation about capacity to adopt the behavior. Abraham (Citation2015) notes that the theory is best applied to behaviors where motivation is important (e.g., lack of motivation to abstain from alcohol in pregnancy). Hence, the theory of planned behavior may be particularly useful for understanding low to moderate alcohol use that appears to be a product of decision-making impacted by motivation (Corrales-Gutierrez et al., Citation2020).
The prototype/willingness model
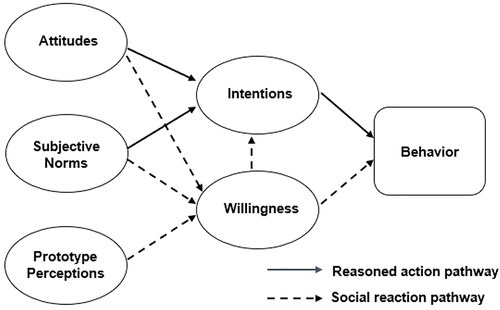
The TPB has been criticized for its underlying presumption that behavior is planned and rational (Sheeran et al., Citation2013) and that it may not adequately account for reactive or momentary influences on behavior (Rivis et al., Citation2006). Given the importance of the social context of risk behaviors such as alcohol use in pregnancy, the applicability of the TPB to alcohol use in pregnancy may be limited in this aspect. One model that does incorporate the socially reactive aspect of planned and unplanned behavior is the prototype/willingness model (PWM) (See ). The PWM was initially developed to explore the decisionmaking of adolescents in regards to health-risk behaviors (Gibbons & Gerrard, Citation1995) by including not only intentions, but also including willingness, i.e., an individual’s willingness to engage in a behavior under certain circumstances. Willingness is different from intention because it is situationally specific such that despite having the intention to behave a certain way someone may act in opposition to that intention when provided the opportunity (e.g., accepting a glass of champagne at a wedding while pregnant despite previously intending to abstain during pregnancy). The model further incorporates the social aspect of decision-making by proposing that an individual holds an image of the prototypical person who engages in the behavior and expects that their peers share this same image. It is then assumed that if a prototype is seen favorably, then the individual would be motivated to behave in a similar way, such that they are also seen favorably. Additionally, the more similar one feels they are to a prototypical person they view favorably, the more likely they are to feel that they would be viewed favorably if they were to do the same behavior.
Figure 1. Prototype/willingness model. Adapted from (Gerrard et al., 2008).
In fact, previous research has found that perceptions of likeability, similarity and responsibility differed according to the amount of alcohol prototypes were said to consume in pregnancy (Fletcher et al., Citation2022). That is, those who were said to drink a “small” amount of alcohol in pregnancy were rated more positively than those who were said to drink an ambiguous amount in pregnancy. Despite this more positive view of the behavior of low to moderate alcohol use in pregnancy, there was no associated increase in individual willingness to use a small amount of alcohol while pregnant. The authors speculated that although momentary willingness was not affected by perceptions, alcohol use intentions may be (Fletcher et al., Citation2022).
Impulsivity, venturesomeness and Self-Efficacy
In addition to social influences, research has found a relationship between personality and alcohol use in pregnancy (Lupattelli et al., Citation2021). Openness to experience (Beijers et al., Citation2014; Lupattelli et al., Citation2021), extraversion (Lupattelli et al., Citation2021; Ystrom et al., Citation2012) and novelty-seeking (Magnusson et al., Citation2007) have all been linked to increased alcohol use during pregnancy, suggesting that those high in these traits may more willingly engage in the behavior (Lupattelli et al., Citation2021). Further, these traits are broadly captured by the concepts of venturesomeness and impulsivity. That is, an individual’s level of venturesomeness is their appetite for risk and sensation seeking (e.g., skydiving) (Cross et al., Citation2011). In addition to how venturesome someone may be individuals also have a level of impulsivity in regard to decision making. In particular, decisions that are made hastily, with little to no forethought or consideration of consequences can be described as impulsive (Moeller et al., Citation2001). High impulsivity has been found to be related to both social alcohol use (Lannoy et al., Citation2017) and problem drinking (Haeny et al., Citation2020).
Although Ajzen (Citation2002) considers perceived behavioral control to be a combination of self-efficacy (i.e., one’s perception of their ability to engage in a behavior) and perceived control (i.e., the level of control individual’s feel they have over a behavior), many studies operationalize those aspects separately and have found that they have varying relationships with intentions. For example, a meta-analysis of studies exploring the TPB and general alcohol use found that, when examined separately, self-efficacy had a strong relationship with alcohol use intentions whereas perceived control over alcohol use had an insignificant, negative relationship with intention (Cooke et al., Citation2016). In addition to behavior-specific self-efficacy, general self-efficacy has been found to be predictive of intentions to engage in a variety of behaviors such that higher levels of general self-efficacy are associated with stronger intentions to engage in desired behaviors (Luszczynska et al., Citation2005).
Overview and hypotheses
The present study sought to provide more insight into influences on women’s decisions about low to moderate alcohol use in pregnancy. We sought to explore both the general and socially reactive (i.e., contextspecific) pathways that may contribute to alcohol use in pregnancy using a theory-based approach. Therefore, the TPB and the PWM were applied to the prediction of intention to use low to moderate amounts of alcohol while pregnant. Additionally, we used an experimental methodology to examine whether there were differences in perceptions of low to moderate alcohol use during pregnancy (“small use” prototype condition) compared to an undefined level of alcohol use during pregnancy (“ambiguous use” prototype condition). Scores on the outcome measures according to prototype exposure were compared.
Specifically, it was hypothesized that:
H1: Attitudes, subjective norms and perceived behavioral control would be predictive of intention to use low-moderate amounts of alcohol in pregnancy after controlling for impulsivity, venturesomeness, and self-efficacy.
H2: The addition of PWM variables to the TPB would increase the amount of variance explained in intentions to use low-moderate amounts of alcohol in pregnancy after controlling for impulsivity, venturesomeness, and self-efficacy.
H3: An “ambiguous use” prototype would be rated less favorably than a “small use” prototype.
Method
Participants and procedure
Ethical approval was obtained by the Curtin University Human Research Ethics Committee (HREC number HRE2019-0339). Participants were 746 women aged 20 to 45 years who had previously had a drink containing alcohol and were either currently pregnant, had previously been pregnant or intended to become pregnant in the future. Firstly, 461 participants were recruited via posts made on local community Facebook pages as well as on online parenting forums in Australia. These posts provided a brief overview of the study and included a link to the survey where the study was outlined in full, participants were provided with a copy of the participant information sheet and were entered into a random draw for one of three $100 vouchers. An additional 285 UK participants completed the study via the paid recruitment platform Prolific and were paid AUD$16.81/GBP£9.60 per hour for their time. Data collection took place between January and April 2021.
Participants provided informed consent and were then randomized to one of two conditions and were presented with the following definition of a prototype:
“The following questions concern your images of people. What we are interested in here are your ideas about typical members of different groups. For example, we all have ideas about what typical movie stars are like or what the typical grandmother is like. When asked, we could describe one of these images- we might say that the typical movie star is pretty or rich, or that the typical grandmother is sweet and frail. We are not saying that all movie stars or all grandmothers are exactly alike, but rather that many of them share certain characteristics” (Gibbons et al., Citation1995, p. 85).
Participants were also presented with a prompt to consider either the “typical person who drinks alcohol in pregnancy” (“ambiguous use” prototype) or the “typical person who drinks a small amount of alcohol in pregnancy” (“small use” prototype).
Measures
Demographics
Included age, marital status, education, employment status and pregnancy history.
Recent alcohol use
To determine how recently participants had consumed alcohol participants were asked when, if ever, they had last consumed alcohol ranging from never to over 3 months ago.
Pregnancy history and intentions
Participants were asked whether they were currently pregnant, whether they had previously been pregnant, whether they had biological children and whether they intended to become pregnant in the future.
Previous alcohol use during pregnancy
Participants with a biological child were asked to indicate whether they changed their alcohol drinking habits around the time of their most recent pregnancy by selecting one of 6 options (i.e., didn’t drink even before pregnancy, stopped drinking while trying to get pregnant, stopped drinking when they found out they were pregnant, stopped drinking at some point after finding out they were pregnant, reduced the amount they drank when pregnant, or did not stop or reduce drinking when pregnant). Those who indicated that they stopped drinking at some point after finding out they were pregnant, reduced the amount they drank when pregnant, or did not stop or reduce drinking when pregnant were recorded as having consumed alcohol during a past pregnancy.
Impulsivity and venturesomeness
The Eysenck Impulsivity and Venturesomeness Scale was used (Eysenck et al., Citation1985). The 35-item scale asks Yes/No questions about whether respondents would engage in a series of “risky” experiences (e.g., Would you enjoy parachute jumping?) or behave impulsively (e.g., Do you generally do and say things without stopping to think?). There were 19 items on the impulsivity subscale (α = .811) and 16 on the venturesomeness subscale (α = .779).
Self-Efficacy
Self-efficacy was measured using the General Self-Efficacy Scale (Schwarzer & Jerusalem, Citation1995). Respondents were presented with 10 statements expressing an ability to achieve goals even under difficult situations (e.g., “I can always manage to solve difficult problems if I try hard enough”) and asked to identify how true each statement was for them on a 4-point scale ranging from “not true at all” to “completely true” (α = .843).
Prototype measurement
Dependant on randomization, participants were asked to describe, in three to five words, the kind of person who would drink either a small or an ambiguous amount of alcohol in pregnancy. Describing the prototype in their own words was meant to produce a clear image in the participants’ minds about the characteristics of the prototype. Participants were then asked to assign a rating on a 5-point Likert scale of how likable/unlikable they thought the individual was, how responsible/irresponsible they believed they were and how similar/dissimilar they felt they were to them.
Subjective measure of alcohol use in pregnancy
To determine what behavior each participant was considering when responding to questions about alcohol use in pregnancy, they were asked to specify how much the person they were considering in the previous question would drink. Participants randomized to the “ambiguous use” condition were also asked to specify how much they thought someone who drank a small amount while pregnant would have.
Willingness to consume low to moderate amounts of alcohol in pregnancy
Six items assessing willingness to consume low to moderate amounts of alcohol in pregnancy under particular circumstances were included (α = .796). Three different hypothetical situations were presented, that asked participants to suppose that they were pregnant and that they had the opportunity to have a drink containing alcohol (e.g., at a wedding, at home with their partner, at a friend’s house). These particular situations to reflect previous situations from the literature (McBride et al., Citation2012; Tsang et al., Citation2021). Participants first rated on a 7-point Likert scale how willing they would be to accept and finish the drink in each scenario (from not at all willing to very willing). They were then asked to respond to the three scenarios in the same way but to indicate how willing they would be to say no and refuse the drink. Refusal responses were reverse scored.
Intention to consume low to moderate amounts of alcohol in pregnancy
Participants were told that the following questions were about drinking “small” amounts of alcohol in pregnancy and were prompted to consider the amount that they specified when responding to the question assessing a subjective measure of low to moderate amounts of alcohol. Only those participants who previously stated that they intended to become pregnant in the future were then asked to indicate their agreement with the statement “I intend to drink alcohol at some point during any future pregnancy” along a 7-point Likert scale ranging from “strongly agree” to “strongly disagree.”
TPB direct measures
Adapted items from the TPB Alcohol Questionnaire (Duncan et al., Citation2012) were used were used as direct measures of the TPB constructs. All items were adapted to specify that the behavior being considered was “small” levels of alcohol use. An item on the attitude scale was also adapted to ask about whether the participant felt that drinking a small amount of alcohol while pregnant would be “safe” for them instead of whether it would be “useful” (four items, α = .87). An additional item was included on the subjective norm scale (i.e., “If I were pregnant and drank a small amount of alcohol most people who are important to me would think that was safe”) resulting in four items (α = .811). The perceived behavioral control items had low reliability (α = .385). Removing one item which did not correlate very highly with the other three items (corrected item − total correlation = .046) increased the reliability to a more acceptable level, thus resulting in a three item scale (α = .583).
Data analysis
Apart from perceived behavioral control, all other variables had acceptable reliability coefficients. A series of independent samples t-tests were then used to compare the ratings for all the outcome measures reported by those in the “ambiguous use” condition (N = 381) to the ratings reported by those in the “small use” condition (N = 365).
Although the Shapiro-Wilk statistic was significant for all variables, upon examination of the histograms and QQ plots the data appeared to be normally distributed. Additionally, given that large and relatively equal sample sizes (N > 30-40) are robust against violations of the assumption of normality (Pallant, Citation2011) the results were interpreted as having satisfied the assumption. Levene’s test was significant for responsibility, similarity, perceived behavioral control and willingness to accept a drink while pregnant so the t-test for equal variances not assumed are reported.
An a priori power analysis was conducted using G*Power version 3.1.9.7 (Faul et al., Citation2007) to determine the minimum sample size required. Results indicated the required sample size to achieve 80% power for detecting a medium effect, at a significance criterion of α = .05, was N = 189.
Findings
Demographics
Of the whole sample, 57.1% were aged 25 to 35 years old (M = 31, SD = 5.8). The majority (73.7%) had completed either an undergraduate or a postgraduate degree and 80.7% were employed either part-time or full-time. Additionally, 77.9% drank alcohol within the last month and 68.5% of participants intended to become pregnant in the future. Just over half of the participants had previously been pregnant (53.1%) with 45.6% of participants currently had a biological child and 13% were currently pregnant. Fewer than 2% of participants had never been and did not ever intend to become pregnant. Additional demographics are outlined in and Electronic Supplementary Material 1.
Table 1. Previous alcohol use, pregnancy history, and intention (N = 746).
Alcohol use intentions and behavior in pregnancy
This study found that 30.72% of participants reported that they intended to drink a “small” amount of alcohol while trying to get pregnant whereas 7.63% intended to drink at some point while pregnant. In comparison, Australian data from 2003 found that 31.6% of women intended to drink an ambiguous amount of alcohol when planning to get pregnant while 23.7% intended to drink during a future pregnancy (Peadon et al., Citation2011). Although the percentage of participants intending to drink alcohol while trying to get pregnant was similar between studies, significantly fewer participants intended to drink while pregnant in this study. This may be reflective of health promotion efforts in recent years focusing on preventing alcohol use while pregnant.
Reporting on their most recent pregnancy, of those in this study who had previously had a child (N = 340), 62.7% stopped drinking when they found out they were pregnant while 11.6% continued to drink after they became aware they were pregnant. In comparison, recent Australian data collected between 2017-2018 found that of 935 women who drank pre-pregnancy, 18% continued to drink alcohol once they knew they were pregnant, a third of which reported drinking on special occasions only (Tsang et al., Citation2021). However, differences in the reporting of alcohol use during pregnancy, particularly in terms of specific time points and amounts, means it is difficult to compare rates between studies. For example, data collected in 2006 found that 34.1% of participants reported consuming alcohol at some point during their previous pregnancy however, they did not distinguish between consumption prior to and after awareness of pregnancy (Peadon et al., Citation2011).
Descriptive findings
Correlations between variables of interest are outlined in .
Table 2. Correlations between the study variables.
Group differences
Independent t-tests demonstrated that there were significant differences related to prototype exposure for likability, responsibility, similarity, perceived behavioral control and willingness to accept a drink while pregnant. Specifically, those exposed to the “small use” prototype rated its likability, level of responsibility and degree of similarity to themselves as higher. Those exposed to “small use” prototype also had a greater level of perceived behavioral control and a greater overall willingness to accept and finish a drink while pregnant. However, there was less than a 1.5-point difference in the means between groups for each of the variables.
Predicting intentions to drink while pregnant
For those participants who intended to become pregnant in the future (N = 511), stepwise hierarchical regression was used to predict their intentions to drink alcohol at any point while pregnant. Prototype exposure was entered in the first step, followed by age, and having a biological child in the second step, impulsivity, venturesomeness, and self-efficacy in the third step, subjective norms, attitudes, and perceived behavioral control in the fourth step, likability, similarity, and responsibility in the fifth step, and willingness in the final step (see ). The model accounted for 52.7% of variance in intentions to drink alcohol while pregnant (R2= .527, F(1, 438) = 13.201, p < .001). The following were all significant predictors of variance in intentions to drink alcohol at any point in a future pregnancy; venturesomeness, which predicted 0.8% of variance; subjective norms, which predicted 0.6% of variance; attitudes, which predicted 8.9% of variance; perceived similarity, which predicted 5.0% of variance; and, willingness to drink while pregnant; which predicted 1.4% of variance. Those who were more venturesome, felt that they were similar to someone who would drink alcohol while pregnant, had a greater situational willingness to drink while pregnant and/or held more positive subjective norms and attitudes toward drinking alcohol while pregnant were more likely to intend to drink alcohol while pregnant. As willingness is proposed to have a direct relationship with behavior steps 1 to 5 were also run as an additional analysis with willingness as the dependent variable. This model accounted for 38% of the variance in willingness (R2= .38, F(1, 645) = 5.023, p < .05).
Table 3. Summary of hierarchical regression analysis for variables predicting alcohol use intentions during pregnancy (N = 511).
Discussion
The aim of this research was to explore women’s intentions to consume alcohol when pregnant. Additionally, this study used concepts from the prototype/willingness model to determine whether prototype perceptions and situationally specific willingness to drink alcohol while pregnant added to the prediction of alcohol use intentions.
Predictive utility of the TPB and the PWM
In this study, over half the variance in low to moderate alcohol use intentions was accounted for by the final model. In combination with impulsiveness, venturesomeness, and self-efficacy, variables from the TPB explained 39% of variance in intentions, with the addition of variables from the PWM, a further 8% of variance was explained. In comparison, a study of pregnant women found that 59% of the variance in intentions to consume alcohol while pregnant was predicted by the TPB alone (Duncan et al., Citation2012).
Although the TPB had greater predictive utility in the study by Duncan et al. (Citation2012) than the model used in this study, it is important to note the differences in the two populations, namely, currently pregnant women as opposed to women intending a future pregnancy. These differences may indicate that, despite thinking that exposure to guidelines for alcohol use in pregnancy can act as an opportunity for planning future behavior, actual decisions about alcohol use intentions may not be made until one becomes pregnant. However, in this study, of those who intended a future pregnancy and were included in the regression analysis (N = 511), 11.4% were also currently pregnant, further exploration of this sub-sample may provide greater insight into this possible distinction. Mixed acceptance of alcohol use at different periods during pregnancy, e.g., different trimesters, may also extend the intentionbuilding period such that there are many opportunities to revise intentions throughout the different stages of pregnancy meaning that intention is not necessarily stable.
Predictors of intentions to use alcohol in pregnancy
In this study venturesomeness, subjective norms, and situational willingness to drink while pregnant each predicted 0.6, 0.8 and 1.4% of variance in alcohol use intentions respectively. Attitudes and perceived prototype similarity predicted 8.9% and 5% of the unique variance in intentions. The remaining variables (i.e., self-efficacy, impulsivity, perceived behavioral control, perceived prototype likability, and responsibility) were all non-significant in the final model. Because impulsivity likely has more influence in-the-moment than on planned decisions, the influence of trait impulsivity on alcohol use decisions may have been difficult to establish through the proxy of intentions. Future research may look at the intention-behavior relationship as moderated by impulsivity to determine how this trait influences planned behavior. Although both self-efficacy and venturesomeness were significant predictors at step 3 of the model, only venturesomeness was still significant at steps 4 and 5. These findings suggest that trait levels of venturesomeness have more influence on intentions to drink alcohol in pregnancy than self-efficacy does on intentions to abstain. These findings also align with prior work demonstrating that risk-taking (of which venturesomeness is one facet) increases the odds of binge-drinking among women (de Haan et al., Citation2015). However, the results for this study may have differed if a more specific measure of self-efficacy was used, such as drink refusal self-efficacy which assesses whether individuals feel that they are able to resist drinking alcohol under specific circumstances (Oei et al., Citation2005).
Intentions to drink while pregnant have been found to be significantly associated with neutral or positive attitudes to alcohol use during pregnancy (Peadon et al., Citation2011). The current study also found that a positive attitude was a significant predictor of intention, however, despite the shared finding, it is important to note that Peadon et al. (Citation2011) did not use a theoretical framework in their study and direct comparisons on attitude measures between studies are not possible. The finding that perceived behavioral control was not a significant predictor of intentions in this study is unsurprising, given that scores on the perceived behavioral control measure were relatively high overall, (x = 6.61, SD = .748) with over 86% of the respondents agreeing or strongly agreeing with each item. Additionally, a meta-analysis of the predictive utility of the theory of planned behavior in relation to alcohol and dietary behaviors found that perceived behavioral control had minimal effect on intention and that attitude was the strongest predictor overall (Hagger et al., Citation2016).
In concordance with the findings of this study, Duncan et al. (Citation2012) also found that attitudes and subjective norms were significant predictors of intention in the final model while perceived behavioral control was not. In comparison, Vézina-Im and Godin (Citation2011) examined non-pregnant women’s intentions to abstain from alcohol during a future pregnancy and found that although attitude and perceived behavioral control were significant predictors of intentions to abstain, subjective norms were not. Despite the apparent contradictions, these differences in results are not unusual given that the study by Vézina-Im and Godin (Citation2011) was conducted with a population that consisted primarily of university students and that although the authors were addressing the same health behavior as the current study (alcohol use in pregnancy), it was framed as abstinence from alcohol during a future pregnancy as opposed to intentions to drink low to moderate amounts during a future pregnancy. The level of control needed to completely abstain from alcohol in pregnancy may be higher than that needed to limit drinking to a small or moderate amount. This may explain why perceived behavioral control was relevant when examining intentions to abstain as opposed to intentions to drink even though they are two different sides of the same coin.
The hypothesis that the addition of PWM variables to the TPB would increase the amount of variance explained in intentions to use low-moderate amounts of alcohol in pregnancy was partially supported. Perceived similarity of the prototype and willingness to consume alcohol were the only predictors from the PWM that were significant in the final model. Interestingly, perceived similarity contributed to the model above and beyond willingness which is inconsistent with the PWM. However, this finding is not uncommon, in fact a meta-analysis of predictive studies using the PWM found that intention was better predicted by prototype similarity (.47) than willingness (.41) (Todd et al., Citation2016). The extent to which willingness contributed to the model in this study was minimal compared to that found by the meta-analysis, that is 1.4% of variance in intention as opposed to 21.6% respectively. However, this is not unexpected given that willingness-intention and similarity-intention relationships are moderated by behavior type (Todd et al., Citation2016). Furthermore, the meta-analysis found that in relation to alcohol use specifically, willingness accounted for 56.4% of variance in alcohol use intentions, however, this finding was in regard to the PWM only and did not include variables from the TPB.
Prototype exposure and perceptions
The experimental use of different prototype exposures had mixed results. Although there was a significant effect of exposure to prototypes on the resulting prototype perceptions, such that exposure to the “ambiguous use” prototype was associated with less positive ratings of the perceived likeability, similarity and responsibility of the prototype, the means for each condition only differed by less than 1.5 scale points each. Additionally, prototype exposure had no significant relationship with any variable other than PWM ratings; thus, the hypothesis that prototype exposure would be associated with intentions to drink alcohol while pregnant was not supported.
Strengths and limitations
The main strategy for reducing low to moderate alcohol use during pregnancy is public health messaging, with a reliance on communicating health guidelines. Therefore, this study aimed to explore determinants of intentions to consume low to moderate amounts of alcohol while pregnant in order to better inform such messaging. Although we were unable to measure actual alcohol use behavior during pregnancy, by including women who had previously had children as well as those who intended to in the future, we were able to explore the planned aspects of alcohol use in pregnancy that health promotion messaging often targets.
It is important to note that while the validity of the TPB as a predictive model of intentions is well accepted, the link between intentions and behavior is less established (Sniehotta et al., Citation2015). Accordingly, there are limitations in the extent to which the current findings can provide insight into predictors of actual alcohol use behavior during pregnancy. However, pre-pregnancy intentions have been shown in previous research to be predictive of alcohol use behavior in pregnancy (Zammit et al., Citation2008), and a meta-analysis of experimental studies across a wide range of behaviors found that medium/large changes in intention led to small/medium changes in behavior (Webb & Sheeran, Citation2006). Therefore, targeting the determinants of intentions to use alcohol while pregnant may be useful for promoting behavior change.
Although a strength in some ways, another key limitation of this work was the inclusion of participants with a wide range of pregnancy histories and intentions. Although effort was made to ensure the sample would include those for whom this research would be relevant, the research may have benefited from using quotas when recruiting such that the sample could be stratified according to key characteristics, for example pregnancy history. This would allow for the detection of any sub-group differences.
A strength of this study was the choice to prompt partcipants to be specific about the behavior they were considering when answering the questions. That is, when asked about alcohol use intentions, participants were instructed to identify what they considered a “small” amount of alcohol to be. This was done to avoid asking about intentions to drink neither an ambiguous amount of alcohol nor a specific, possibly irrelevant/hard to understand amount of alcohol during pregnancy. Additionally, we allowed participants to self-identify a “small” amount of alcohol use as it would not have been appropriate to specify exactly what was meant by a “small” amount as that could have been conflated by participants as a “safe” amount. Furthermore, specifying amounts of alcohol use may create additional complexities if participants are not familiar with what a standard drink is, especially considering that our sample included those from both Australia and the UK. However, there is the possibility that participants may have had intentions to consume alcohol at lower levels than what they perceived to be the typical “small” amount and this was unable to be determined through the methods used in this study. Overall, further validation of the scales used in this study would have also provided more robust evidence that the measures were relevant for our population of women aged 20-45 years in Australia.
Conclusion
The findings of this study indicate that the theory of planned behavior and the prototype willingness model are useful theoretical frameworks with which to explore determinants of alcohol use intentions and possibly behavior in pregnancy. In particular, future behavior change interventions should focus on changing the attitudes of women toward low to moderate alcohol use during pregnancy. Additional factors that could be targeted by interventions to reduce low to moderate alcohol use in pregnancy include, the perception of those who drink alcohol during pregnancy, the subjective norms people hold in relation to alcohol use in pregnancy and individual’s willingness to drink alcohol in particular social situations.
Electronic Supplementary Material 1.docx
Download MS Word (17.2 KB)Disclosure statement
The authors report there are no competing interests to declare.
Data availability statement
The data that support the findings of this study are openly available in Open Science Framework at https://osf.io/h4rmz/
Additional information
Funding
References
- Abraham, C. (2015). Mapping modifiable mechanisms in health promotion research: A commentary on Sniehotta, Presseau, and Araújo-Soares. Health Psychology Review, 9(2), 160–164. https://doi.org/10.1080/17437199.2014.905967
- Ajzen, I. (1991). The theory of planned behavior. Organizational Behavior and Human Decision Processes, 50(2), 179–211. https://doi.org/10.1016/0749-5978(91)90020-T
- Ajzen, I. (2002). Perceived behavioral control, self-efficacy, locus of control, and the theory of planned behavior. Journal of Applied Social Psychology, 32(4), 665–683. https://doi.org/10.1111/j.1559-1816.2002.tb00236.x
- Beijers, C., Burger, H., Verbeek, T., Bockting, C. L., & Ormel, J. (2014). Continued smoking and continued alcohol consumption during early pregnancy distinctively associated with personality. Addictive Behaviors, 39(5), 980–986. https://doi.org/10.1016/j.addbeh.2014.01.022
- Comasco, E., Rangmar, J., Eriksson, U. J., & Oreland, L. (2018). Neurological and neuropsychological effects of low and moderate prenatal alcohol exposure. Acta Physiologica, 222(1), e12892. https://doi.org/10.1111/apha.12892
- Cooke, R., Dahdah, M., Norman, P., & French, D. P. (2016). How well does the theory of planned behaviour predict alcohol consumption? A systematic review and meta-analysis. Health Psychology Review, 10(2), 148–167. https://doi.org/10.1080/17437199.2014.947547
- Corrales-Gutierrez, I., Mendoza, R., Gomez-Baya, D., & Leon-Larios, F. (2020). Understanding the relationship between predictors of alcohol consumption in pregnancy: Towards effective prevention of FASD. International Journal of Environmental Research and Public Health, 17(4), 1388. https://doi.org/10.3390/ijerph17041388
- Cross, C. P., Copping, L. T., & Campbell, A. (2011). Sex differences in impulsivity: A meta-analysis. Psychological Bulletin, 137(1), 97–130. https://doi.org/10.1037/a0021591
- de Haan, L., Egberts, A. C. G., & Heerdink, E. R. (2015). The relation between risk-taking behavior and alcohol use in young adults is different for men and women. Drug and Alcohol Dependence, 155, 222–227. https://doi.org/10.1016/j.drugalcdep.2015.07.013
- Department of Health. (2016). Alcohol guidelines review: Report from the guidelines development group to the UK chief medical officers. https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/545739/GDG_report-Jan2016.pdf
- Duncan, E. M., Forbes-McKay, K. E., & Henderson, S. E. (2012). Alcohol use during pregnancy: An application of the theory of planned behavior. Journal of Applied Social Psychology, 42(8), 1887–1903. https://doi.org/10.1111/j.1559-1816.2012.00923.x
- Eysenck, S. B. G., Pearson, P. R., Easting, G., & Allsopp, J. F. (1985). Age norms for impulsiveness, venturesomeness and empathy in adults. Personality and Individual Differences, 6(5), 613–619. https://doi.org/10.1016/0191-8869(85)90011-X
- Faul, F., Erdfelder, E., Lang, A.-G., & Buchner, A. (2007). G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behavior Research Methods, 39(2), 175–191. https://doi.org/10.3758/BF03193146
- Fletcher, T., Mullan, B., & Finlay-Jones, A. (2022). Perceptions of two different alcohol use behaviours in pregnancy: An application of the prototype/willingness model. Health Psychology and Behavioral Medicine, 10(1), 1071–1085. https://doi.org/10.1080/21642850.2022.2143362
- Gerrard, M., Gibbons, F. X., Houlihan, A. E., Stock, M. L., & Pomery, E. A. (2008). A dual-process approach to health risk decision making: The prototype willingness model. Developmental Review, 28(1), 29–61.
- Gibbons, F., & Gerrard, M. (1995). Predicting young adults’ health risk behavior. Journal of Personality and Social Psychology, 69(3), 505–517. https://doi.org/10.1037//0022-3514.69.3.505
- Gibbons, F., Gerrard, M., & Boney-McCoy, S. (1995). Prototype perception predicts (lack of) pregnancy prevention. Personality and Social Psychology Bulletin, 21(1), 85–93. https://doi.org/10.1177/0146167295211009
- Gouilhers, S., Meyer, Y., Inglin, S., Pfister Boulenaz, S., Schnegg, C., & Hammer, R. (2019). Pregnancy as a transition: First-time expectant couples′ experience with alcohol consumption. Drug and Alcohol Review, 38(7), 758–765. https://doi.org/10.1111/dar.12973
- Haeny, A. M., Gueorguieva, R., Morean, M. E., Krishnan-Sarin, S., DeMartini, K. S., Pearlson, G. D., Anticevic, A., Krystal, J. H., & O’Malley, S. S. (2020). The association of impulsivity and family history of alcohol use disorder on alcohol use and consequences. Alcoholism: Clinical and Experimental Research, 44(1), 159–167. https://doi.org/10.1111/acer.14230
- Hagger, M. S., Chan, D. K., Protogerou, C., & Chatzisarantis, N. L. (2016). Using meta-analytic path analysis to test theoretical predictions in health behavior: An illustration based on meta-analyses of the theory of planned behavior. Preventive Medicine, 89, 154–161. https://doi.org/10.1016/j.ypmed.2016.05.020
- Khalid, O., Kim, J. J., Kim, H.-S., Hoang, M., Tu, T. G., Elie, O., Lee, C., Vu, C., Horvath, S., Spigelman, I., & Kim, Y. (2014). Gene expression signatures affected by alcohol-induced DNA methylomic deregulation in human embryonic stem cells. Stem Cell Research, 12(3), 791–806. https://doi.org/10.1016/j.scr.2014.03.009
- Lannoy, S., Billieux, J., Poncin, M., & Maurage, P. (2017). Binging at the campus: Motivations and impulsivity influence binge drinking profiles in university students. Psychiatry Research, 250, 146–154. https://doi.org/10.1016/j.psychres.2017.01.068
- Lupattelli, A., Ronningen, E., Krogsrud, S. K., Nordeng, H., & Ystrom, E. (2021). Personality and its relation to the use of alcohol and cigarettes during pregnancy: A multinational study. Journal of Health Psychology, 26(9), 1293–1306. https://doi.org/10.1177/1359105318775194
- Luszczynska, A., Scholz, U., & Schwarzer, R. (2005). The general self-efficacy scale: Multicultural validation studies. The Journal of Psychology, 139(5), 439–457. https://doi.org/10.3200/JRLP.139.5.439-457
- Magnusson, Å., Göransson, M., & Heilig, M. (2007). Hazardous alcohol users during pregnancy: Psychiatric health and personality traits. Drug and Alcohol Dependence, 89(2-3), 275–281. https://doi.org/10.1016/j.drugalcdep.2007.01.015
- Mamluk, L., Edwards, H. B., Savović, J., Leach, V., Jones, T., Moore, T. H. M., Ijaz, S., Lewis, S. J., Donovan, J. L., Lawlor, D., Smith, G. D., Fraser, A., & Zuccolo, L. (2017). Low alcohol consumption and pregnancy and childhood outcomes: Time to change guidelines indicating apparently ‘safe’ levels of alcohol during pregnancy? A systematic review and meta-analyses. BMJ Open, 7(7), e015410. https://doi.org/10.1136/bmjopen-2016-015410
- McBride, N., Carruthers, S., & Hutchinson, D. (2012). Reducing alcohol use during pregnancy: Listening to women who drink as an intervention starting point. Global Health Promotion, 19(2), 6–18. https://doi.org/10.1177/1757975912441225
- Meurk, C. S., Broom, A., Adams, J., Hall, W., & Lucke, J. (2014). Factors influencing women’s decisions to drink alcohol during pregnancy: Findings of a qualitative study with implications for health communication. BMC Pregnancy and Childbirth, 14(1), 246. https://doi.org/10.1186/1471-2393-14-246
- Moeller, F. G., Barratt, E. S., Dougherty, D. M., Schmitz, J. M., & Swann, A. C. (2001). Psychiatric aspects of impulsivity. The American Journal of Psychiatry, 158(11), 1783–1793. https://doi.org/10.1176/appi.ajp.158.11.1783
- National Health and Medical Research Council. (2020). Australian guidelines to reduce health risks from drinking alcohol. https://www.nhmrc.gov.au/file/15923/download?token=t0Hrxdvq
- Oei, T. P., Hasking, P. A., & Young, R. M. (2005). Drinking refusal self-efficacy questionnaire-revised (DRSEQ-R): A new factor structure with confirmatory factor analysis. Drug and Alcohol Dependence, 78(3), 297–307. https://doi.org/10.1016/j.drugalcdep.2004.11.010
- Ornoy, A., & Ergaz, Z. (2010). Alcohol abuse in pregnant women: Effects on the fetus and newborn, mode of action and maternal treatment. International Journal of Environmental Research and Public Health, 7(2), 364–379. https://doi.org/10.3390/ijerph7020364
- Pallant, J. (2011). SP SS Survival Manual: A Step by Step to Data Analysis. Allen and Unwin Berkshire Publishers, Berkshire, Australia.
- Peadon, E., Payne, J., Henley, N., D’antoine, H., Bartu, A., O’Leary, C., Bower, C., & Elliott, E. J. (2011). Attitudes and behaviour predict women’s intention to drink alcohol during pregnancy: The challenge for health professionals. BMC Public Health, 11(1), 584. https://doi.org/10.1186/1471-2458-11-584
- Popova, S., Lange, S., Probst, C., Gmel, G., & Rehm, J. (2017). Estimation of national, regional, and global prevalence of alcohol use during pregnancy and fetal alcohol syndrome: A systematic review and meta-analysis. The Lancet Global Health, 5(3), e290–e299. https://doi.org/10.1016/S2214-109X(17)30021-9
- Rivis, A., Sheeran, P., & Armitage, C. J. (2006). Augmenting the theory of planned behaviour with the prototype/willingness model: Predictive validity of actor versus abstainer prototypes for adolescents’ health-protective and health-risk intentions. British Journal of Health Psychology, 11(Pt 3), 483–500. https://doi.org/10.1348/135910705X70327
- Roozen, S., Kok, G., & Curfs, L. (2017). Fetal alcohol spectrum disorders: Knowledge synthesis. https://cris.maastrichtuniversity.nl/portal/files/16028548/eBook_Fetal_Alcohol_Spectrum_Disorders_Knowledge_Synthesis.pdf
- Schwarzer, R., & Jerusalem, M. (1995). Generalized self-efficacy scale. In J. Weinman, S. Wright, & M. Johnston (Eds.), Measures in health psychology: A user’s portfolio. Causal and control beliefs. NFER-Nelson. (pp. 35–37).
- Sheeran, P., Gollwitzer, P. M., & Bargh, J. A. (2013). Nonconscious processes and health. Health Psychology: Official Journal of the Division of Health Psychology, American Psychological Association, 32(5), 460–473. https://doi.org/10.1037/a0029203
- Sniehotta, F. F., Presseau, J., & Araújo-Soares, V. (2015). On the development, evaluation and evolution of health behaviour theory. Health Psychology Review, 9(2), 176–189. https://doi.org/10.1080/17437199.2015.1022902
- Todd, J., Kothe, E., Mullan, B., & Monds, L. (2016). Reasoned versus reactive prediction of behaviour: A meta-analysis of the prototype willingness model. Health Psychology Review, 10(1), 1–24. https://doi.org/10.1080/17437199.2014.922895
- Tsang, T. W., Kingsland, M., Doherty, E., Anderson, A. E., Tully, B., Crooks, K., Symonds, I., Tremain, D., Dunlop, A. J., Wiggers, J., & Elliott, E. J. (2022). Predictors of alcohol use during pregnancy in Australian women. Drug and Alcohol Review, 41(1), 171–181.
- Vézina-Im, L.-A., & Godin, G. (2011). Psychosocial determinants of intention to abstain from drinking alcohol while pregnant among a sample of women of childbearing age. Addiction Research & Theory, 19(2), 128–137. https://doi.org/10.3109/16066359.2010.512107
- Webb, T. L., & Sheeran, P. (2006). Does changing behavioral intentions engender behavior change? A meta-analysis of the experimental evidence. Psychological Bulletin, 132(2), 249–268. https://doi.org/10.1037/0033-2909.132.2.249
- Ystrom, E., Vollrath, M. E., & Nordeng, H. (2012). Effects of personality on use of medications, alcohol, and cigarettes during pregnancy. European Journal of Clinical Pharmacology, 68(5), 845–851. https://doi.org/10.1007/s00228-011-1197-y
- Zammit, S. L., Skouteris, H., Wertheim, E. H., Paxton, S. J., & Milgrom, J. (2008). Pregnant women’s alcohol consumption: The predictive utility of intention to drink and pre-pregnancy drinking behavior. Journal of Women’s Health (2002), 17(9), 1513–1522. https://doi.org/10.1089/jwh.2007.0595