
Abstract
Background
Alcohol use is a gendered behavior and motherhood is a life stage which may influence drinking motives. However, there are no drinking motive scales uniquely tailored to maternal populations. This work developed a new maternal drinking motives scale (M-DMS) and determined associations between the M-DMS and alcohol-related behavior.
Methods
An online observational survey (n = 534) and online test–retest survey (n = 164) were conducted with adult, UK mothers. From the observational study, data on drinking motives was extracted to determine M-DMS items and factor loading. This was split into two data sets for exploratory and confirmatory factor analyses. Alcohol Use Disorders Identification Test (AUDIT) and Timeline Follow back data, taken from both surveys, were combined to determine the M-DMS’s predictive validity.
Results
Following a parallel analysis and exploratory factor analysis, a two-factor model (positive reinforcement motives, negative reinforcement motives) was deemed the best fit. Probability functional analysis identified items with problematic responses. These were removed before confirmatory factor analysis (on the second dataset) demonstrated a good fit for the two-factor model. All factor loadings were significant and positive (βs > 0.56). Reliability of the two subscales was excellent: negative reinforcement (ωT = 0.95), positive reinforcement (ωT = 0.89). Test–retest reliability was good for both negative (ICC = 0.84, 95%CI = 0.80–0.88) and positive (ICC = 0.77, 95% CI = 0.71–0.82) subscales. Both subscales predicted AUDIT and quantity of alcohol consumption (ps < 0.001).
Conclusion
The first tailored Maternal Drinking Motives Scale (M-DMS) provides a more valid research tool for assessing psychological mechanisms of alcohol use in mothers.
Introduction
Alcohol is the leading risk factor for ill health and early mortality in women aged 15–49 years, covering typical childbearing age (Griswold et al., Citation2018). Risk of harm can occur across levels of alcohol use, with substantial harm attributable to non-dependent drinking in women (O’Dwyer et al., Citation2019). This is partly because women are vulnerable to a wide range of harms, including mental ill-health, self-harm and suicide, cancers, liver disease, and violence (Graziani et al., Citation2014; McCarty et al., Citation2009; Wilsnack et al., Citation2013; World Health Organization, 2019) at lower consumption levels than men (Erol & Karpyak, Citation2015).
When considering maternal drinking, most research has focused on alcohol exposed pregnancy because prenatal alcohol use is the dominant preventable cause of costly birth defects and intellectual disabilities (Baer et al., Citation2003). Yet, alcohol use in motherhood (beyond pregnancy) is also important. In addition to the alcohol-related harms outlined above regarding women’s health, substance use (including alcohol) is a leading cause of mortality in UK mothers between 6 weeks and 12 months postpartum (Knight et al., Citation2023). In terms of child-related harms, non-dependent hazardous (15–35 units p/week) and harmful (>35 units p/week) maternal drinking is associated with increased risk of sudden infant death syndrome and numerous adverse child/adulthood experiences [e.g., hospitalization, accidental medicinal poisoning, mental ill-health, alcohol problems (McGovern et al., Citation2018; Raitasalo et al., Citation2019; Rossow et al., Citation2016)]. Major UK birth cohorts show prevalence of hazardous maternal drinking increases up to offspring adolescence (McGovern et al., Citation2018).
Therefore, maternal drinking, beyond pregnancy, is clearly a significant public health issue. The relative lack of research in this area may reflect several factors, including maternal stereotypes that mothers don’t drink, or a lack of visibility of maternal drinking and its potential harms. Yet women’s alcohol use is changing; the gender gap in drinking is decreasing and this is being driven by increased female alcohol use (Institute of Alcohol Studies, Citation2017; Slade et al., Citation2016). Within UK mothers, up to 18% are hazardous or harmful drinkers (Syed et al., Citation2018) and, internationally, evidence suggests mothers were a particularly vulnerable group to increased drinking during COVID-19 (Ahlers-Schmidt et al., Citation2020; Freisthler & Price Wolf, Citation2022). Greater female and maternal alcohol use is likely a result of multiple factors, including women’s increasing financial independence and access to drinking spaces (Atkinson et al., Citation2019). Additionally, two-thirds of UK alcohol is purchased from off-licensed premises and drinking at home is common (Public Health England, Citation2017). Therefore, alcohol is increasingly affordable for, and available to, women. Furthermore, mothers are also exposed to a narrative of needing alcohol to cope with stress or as a reward (Harding et al., Citation2021), meaning that drinking can be seen as an acceptable activity both for negative and positive reinforcing reasons. Together, these factors may help explain why any reduction in alcohol use because of pregnancy is not maintained by 12-month postpartum (Borschmann et al., Citation2019).
Women’s alcohol research has lagged behind that of men’s (Hunt et al., Citation2016), and there are growing calls for women-specific health interventions, including those aimed at reducing alcohol-related harm (Department Health and Social Care, 2022). Given the gendered nature of drinking (Atkinson et al., Citation2019), it is not surprising that drinking motives can differ between females and males across life stages (Holmila & Raitasalo, Citation2005; Kuntsche et al., Citation2006). The unique risks associated with maternal drinking, means that it is important that any alcohol intervention tailored to mothers addresses maternal drinking motives. Drinking motives are a key proximal factor in determining alcohol use (Marino et al., Citation2018), and are often measured using the Drinking Motives Questionnaire (DMQ). The revised DMQ (DMQ-R) has 20 items and was developed within a reinforcement framework of alcohol use; people drink for positive reinforcement (e.g., enjoying time with friends) or negative reinforcement (e.g., to feel less stressed) (Cooper, Citation1994). This scale further categorizes positive and negative reinforcement motives as internally (e.g., enhancement/coping) or externally (e.g., social/conformity) generated. The DMQ follows the motivational model of alcohol use (Cox & Klinger, Citation1988) and was originally developed in adolescent populations and has since been used in young adult and older adult (60+ y) samples (Gilson et al., Citation2013; van Gils et al., Citation2021). A short form (DMQ-R SF) (12 items) has also been validated in adolescents (Cronbach α 0.70–0.83 across the 4 motive factors) (Kuntsche & Kuntsche, Citation2009), and the coping and conformity subscales have been used in one study assessing associations between parental (Cronbach α 0.94, 0.91) and child (Cronbach α 0.94, 0.95) drinking (Marino et al., Citation2018), and one study used an older version of the DMQ covering three motive domains (coping, enhancement, social) (Doherty & Hunt, Citation2022). Recently, a drinking motives questionnaire has been validated on an adult sample, with motives addressing domains of confidence, social, coping, taste, and enhancement (D'Aquino et al., Citation2023).
Despite these uses, it is possible that existing DMQs do not adequately capture the range of drinking motives most relevant to mothers. Indeed, a recent study showed that mothers were likely to report a change in drinking motives from before, to during and after, pregnancy (Fleming et al., Citation2023). Existing evidence highlights maternal drinking motives as stress reduction, coping, using alcohol as a reward, as a way to retain some aspect of self-identity away from being a parent, and to aid sleep (Fleming et al., Citation2023; Harding et al., Citation2021; Ujhelyi Gomez et al., Citation2022). COVID-19 highlighted motives around boredom relief (Grossman et al., Citation2020) and maternal stress, which may have been associated with mothers of dependent children taking on more of childcare/household chores (Basch et al., Citation2021; Sánchez et al., Citation2021). Existing DMQs do not cover all these potential motives. The public health issue posed by maternal drinking and the growing calls for women-specific alcohol interventions, makes it necessary to develop valid tools for assessing maternal drinking motives. Since substantial evidence has demonstrated good psychometric properties for the revised and short form versions of Cooper’s DMQ, it is reasonable to use these as a basis to develop drinking motive scales tailored to specific populations. The current study used the DMQ-R as a base with several motives amended/added based on existing evidence with maternal samples to produce a maternal drinking motives scale.
Materials and method
Participants
Aged 18 or over, living in the UK, and could speak fluent English. Mothers who were not currently pregnant but who had experienced any form of childbirth, and had at least one dependent child (defined as under 18 years of age, living at home).
Measures
Demographics: Age, ethnicity, sexuality, relationship status, highest level of education, current occupation, average household income (before tax), number of children, UK area of residence.
Alcohol Use Disorders Identification Test (AUDIT: Babor et al., Citation2001): 10 items, assessing alcohol use and potentially harmful drinking behavior. Scores indicate 0–7: low risk drinking, 8–15: increasing risk, 16–19: higher risk, 20+ possible dependence. For women it is recommended that low risk drinking is scored 0–6.
Timeline Followback (TLFB: Sobell, Citation1993): using a diary format, participants were asked to record how many and what type of drink (e.g., large/small glass of wine, pint of beer) they had consumed over the past 7 days. Drinks were converted to UK units (UK unit = 8 g alcohol) and weekly alcohol unit consumption calculated.
Maternal Drinking Motives Scale (M-DMS): Consisted of 24 motive items, including items from the DMQ-R and new items chosen to best match the existing evidence base on maternal drinking motives (e.g., boredom, reward, self-identify, sleep) (Fleming et al., Citation2023; Grossman et al., Citation2020; Harding et al., Citation2021; Ujhelyi Gomez et al., Citation2022). These items also matched the motives identified through public engagement activities with groups of mothers run by the research team. Where appropriate, we used the wording typically used by these attendees. For example, we included “to feel like the old you” as a way of assessing self-identity motives, we included pressure from “family/partner” in addition to friends. As the M-DMS is focused on maternal drinking, respondents were asked “Since being a mother, how often have you drunk alcohol…” followed by the 24 motives (e.g., “to celebrate”). Possible responses were “Always/Almost always” (score 1), “Often” (2), “Sometimes” (3), “Rarely” (4), “Never/Almost never” (5). Scoring was reversed, so that higher scores are indicative of stronger endorsement of the motives.
Procedure
Two studies were completed in the development of this scale.
1. An online survey (N = 534) measuring demographics, alcohol use, health, and well-being in mothers. This survey was posted through social media sites (e.g., Twitter, Facebook) and Prolific (an online research recruitment platform). Just the drinking motives, AUDIT and TLFB data were extracted for the development of the M-DMS.
2. A test–retest survey (N = 164) measuring the AUDIT, TLFB, and drinking motive items. Participants were recruited through Prolific (Palan & Schitter, Citation2018). Test re-test data sets were linked through Prolific email addresses, with the re-test sent out approximately 2 week after the test survey. On the re-test survey, a question was included which asked whether the participant’s motives for drinking had changed since the previous survey.
Data analysis
The full data set for the online survey (N = 534) was randomly split into two samples (barring participants with any missing data on the motives scales, N = 31), to produce an exploratory factor analysis data set (N = 240) and a confirmatory factor analysis data set (N = 263).
Exploratory analysis
A parallel analysis was conducted to ascertain the upper limit of the number of factors to be tested in the exploratory factor analysis. Following this, we conducted an exploratory factor analysis using a minimum residual method (minres) as there was not multivariate normality and the sample sizes were relatively small (<300) (Cudeck, Citation2000). An oblique (Oblimin) rotation was used as past research has shown correlations between drinking motives (Grant et al., Citation2007). Items were considered to load onto a factor if the loading was more than 0.4 and no greater than 0.3 on another factor.
Following this, we conducted polytomous item response theory analysis using a graded response model to further explore responses on specific items. This was to ensure all items had dispersed responses and to allow reduction of the number of items. We did this separately for each subscale identified. Specifically, we explored probability functions for responses on each item to ensure dispersal of responses across all levels of the latent variable. Items were removed when there was poor dispersal of responses (some responses not being the most common across any levels of the latent variable) or where extreme items (1 and 5) were not selected. Internal reliability analysis was conducted on the subscales using McDonalds omega (ωT; see (Revelle & Zinbarg, Citation2009).
Confirmatory analysis
We conducted a confirmatory factor analysis on the second data set, based on the structure identified in the parallel factor analysis. As data were ordinal and responses largely had non-normal distribution, we used a diagonally weighted least square estimator. Several fit indices were produced to evaluate the factor structure. Firstly, the standardized root mean residual (SRMR) absolute fit index with values under 0.08 considered a good fit (Hu & Bentler, Citation1999). The comparative fit index (CFI) baseline comparison test was used and were deemed acceptable at >0.90 and good at >0.95 (Hu & Bentler, Citation1999). In addition, the root mean square error of approximation RMSEA parsimony adjusted measure was calculated with values <0.06 indicative of good fit and values >0.06 but <0.08 being acceptable (Hu & Bentler, Citation1999; MacCallum et al., Citation1996). The Chi-square test statistic along with its degrees of freedom is also reported although not used for assessing model fit (see for example (Babyak & Green, Citation2010)). Modification indices after the initial fit were inspected to identify correlated residuals, and if high and theoretically plausible we allowed these to correlate before refitting the model, Akaike’s information criterion (AIC) are reported to allow model comparison.
Predictive validity
Pearson’s correlations determined associations between drinking motive subscales and key alcohol use measures: AUDIT (alcohol harm) and TLFB (quantity of alcohol consumption).
Test re-test reliability
Assessed using intraclass correlations (ICC): 164 participants had complete data for the initial test and the re-test sample (Median 14 days after the initial sample). Values between 0.50 and 0.75 indicate acceptable reliability, between 0.75 and.9 being good reliability, with over 0.9 being excellent (see Koo & Li, Citation2016).
Results
Demographics
From the original online survey, median age of participants was 35 (±6.31) years and number of children was 2 (±1.01). Participants were predominantly white British (85.2%), married/cohabitating (86.9%), heterosexual (88.4%), with a bachelor’s degree education (35.6%), working full (34.7%) or part (35.2%) time, with median income of £52k (±34.0). Most participants lived in the North West of England (20.2%) followed by the South East of England (16.3%) with a distribution of 2.1–9.4% for other UK areas.
For the test–retest sample, median age of participants was 44 (±12.02) years and number of children were 2 (±0.90). Participants were predominantly white British (85.4%), married/cohabitating (85.4%), heterosexual (97%), with a bachelor’s degree education (36%), working full (32.9%) or part (25%) time, with median income of £44k (±33.5). Most participants lived in the South East of England (15.9%) followed by London (15.2%) with a distribution of 1.2–13.4% for other UK areas.
Parallel analysis and EFA
Initial parallel analysis suggested that there was up to four factors in the data. We therefore ran exploratory analysis exploring four, three, and two factor structures. The four-factor solution was discounted as it contained a single-item factor. The three-factor solution (see supplemental) was discounted because although the third factor had four loadings above the cutoff, three of these also loaded onto another factor.
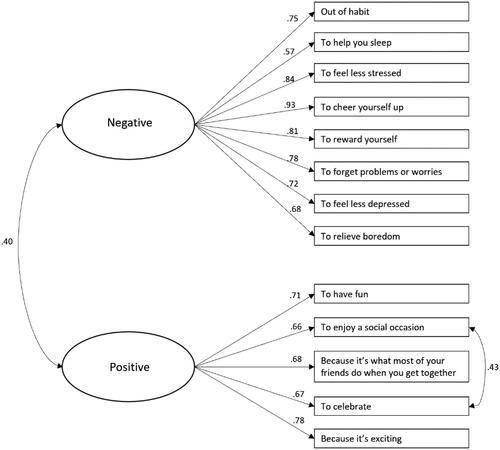
The two-factor model was the best fit (see ). Two items were dropped from the scale for having no loading in excess of 0.4 (“because you felt pressured by family/friends/partner”, “to fit in with a group of people”) and these fit around negative reinforcement (specifically, conformity). Three were dropped because of cross loading in excess of 0.3 (“because it makes you feel good”, “because you like the feeling”, “to relax”) all of which are quite general reinforcement and could be construed as positive or negative reinforcement thereby producing the cross loadings. The two factors were named “positive reinforcement” and “negative reinforcement”.
Table 1. Factor loadings.
Probability function analysis
Although item discrimination parameters were generally high (positive subscale a ≥ 1.55; negative subscale a ≥ 1.92) exploration of the probability functions for each item revealed some problematic items. Exploration of the probability function for “to help get through the daily chores” found that responses of “Often” or “Sometimes” were never the most likely response across any value of the latent variable. Next, there were no endorsements of “Always/Almost always” on “to overcome fatigue”, and a score of “Often” was never the most likely option across any value of the latent variable. On “to get high”, no participants gave a response of “Always/Almost always”, and a response of “Sometimes” was never the most likely response across the latent variable. Three other items had similar issue to this latter problem, responses of “Rarely” on “because you feel more self-confident or sure of yourself”, “to feel like the old you” and “to feel less anxious or nervous” were never the most likely responses across any level of the latent variable. These items were therefore removed from the scale. There were no problematic items on the positive subscale. The final scale can be seen in .
Figure 1. Factor structure of the Maternal Drinking Motives Scale
Internal reliability
The negative (ωT = 0.94) and positive (ωT = 0.95) subscales both had excellent internal reliability.
Confirmatory factor analysis (see )
The confirmatory factor analysis on the second data set demonstrated a good fit (χ2(64) = 95.65, p = 0.006, SRMR = 0.077 CFI = 0.99 RMSEA = 0.044), with modification indices suggesting the residual between “to enjoy a social occasion” and “to celebrate” (MI = 16.31) was relatively high. We, therefore, allowed these residuals to correlate. The amended model was a moderately better fit to the data (χ2(63) = 79.03, p = 0.084, SRMR = 0.070 CFI = 0.99, RMSEA = 0.032). All factor loadings were significant and positive (βs > 0.57). Reliability of the subscales in this sample were also excellent for negative (ωT = 0.95) and positive (ωT = 0.89).
Predictive validity
All complete data was combined (n = 611) to compute Pearson’s correlations between drinking motive subscales and indices of alcohol use. Both had a significant association with AUDIT scores and units consumed (TLFB), the stronger the motives the higher the AUDIT and alcohol use (see ).
Table 2. Pearson’s correlations between variables.
Post hoc analysis (reporting two-tailed significance values) assessed whether positive or negative reinforcement motives were more strongly associated with alcohol measures. The associations between negative motives were greater than positive motives for both AUDIT (z = 4.56, p < 0.001) and TLFB (z = 5.97, p < 0.001) (Lee & Preacher, Citation2013).
Test re-test reliability
Test re-test reliability for the negative subscale was good (ICC = 0.84, 95%CI = 0.80–0.88), as was the positive subscale albeit not as good as the former (ICC = 0.77, 95%CI = 0.71–0.82).
Child’s age
Given that maternal drinking behavior may change as the child ages (e.g., due to changing parental responsibilities and general changes in drinking behavior as adults age: NHS Digital, Citation2022), post hoc analysis investigated whether the negative or positive drinking motive subscales were related to the age of the youngest child. Using the main survey data (which measured child age), we found associations between negative reinforcement motives and the youngest child’s age, r(507) = 0.181, p < 0.001, and positive reinforcement motives and youngest child’s age, r(507) = 0.108, p = .015. In both cases, endorsement of negative and positive drinking motives was positively associated with the mother’s youngest child being older.
Discussion
The aim of this research was to produce a validated tool to assess drinking motives in mothers (maternal drinking motives scale: M-DMS). The original items, used across two studies, were based on a combination of the well-validated DMQ-R items (Cooper, Citation1994) and drinking motives identified through existing evidence on maternal alcohol use (e.g., coping with aspects of motherhood, sleep, boredom, self-identity away from being a parent (Basch et al., Citation2021; Grossman et al., Citation2020; Harding et al., Citation2021; Sánchez et al., Citation2021; Ujhelyi Gomez et al., Citation2022)) and those highlighted through public engagement activities with mothers. The final scale comprises 13 items, loading on to two factors: positive reinforcement motives (5 items) and negative reinforcement motives (8 items).
The most often used drinking motives scale is arguably the DMQ-R (Cooper, Citation1994) which has resulted in revised and short form versions (e.g., Grant et al., Citation2007; Kuntsche & Kuntsche, Citation2009). For the DMQ-R, motives fall into one of four subscales: enhancement (internal positive), coping (internal negative), social (external positive) and conformity (external negative). The original DMQ was developed in adolescents and young adults, and evidence suggests that external factors (e.g., those relating to “social” such as drinking with friends at the weekend, and “conformity” such as peer pressure and fear of missing out) are important in determining alcohol use in this age group (Crawford et al., Citation2022; Sjödin et al., Citation2021; Thrul & Kuntsche, Citation2016). More recently, a DMQ has been developed for use in adults (D’Aquino et al., Citation2023). This was not available when the current study was being conducted but motives fell across 5 sub-factors (social, coping, confidence, taste, enhancement). It is possible that as we enter specific life stages (e.g., motherhood) we may become less influenced by external factors and more motivated by internal drivers, e.g., the desire to enjoy celebrations and/or to feel less stressed. Additionally, existing evidence suggests men are more motivated to drink via external factors relative to women (Thrul & Kuntsche, Citation2016). This may help explain why the two-factor model was the best fit in the current population of adult mothers, but future research is needed to determine how the current M-DMS compares with more recent DMQs developed for general adult populations.
Various studies have employed versions of, or sub-factors from, the DMQ in older samples (Gilson et al., Citation2013), parents (Marino et al., Citation2018), and mothers (Doherty & Hunt, Citation2022). However, the existing evidence suggests that the DMQ (including the DMQ-R, DMQ-R-SF) items may not be the most relevant for maternal populations. For instance, existing evidence identifies mothers use alcohol to manage stress (Basch et al., Citation2021; Pelham & Lang, Citation1999), relieve boredom (Grossman et al., Citation2020), to reward themselves and to reflect aspects of non-maternal self-identify (Harding et al., Citation2021), to aid sleep (Ujhelyi Gomez et al., Citation2022), and to manage childcare/household chores (Basch et al., Citation2021; Sánchez et al., Citation2021). With the exception of managing stress, none of these motives are reflected in existing DMQs. The final version of the M-DMS includes motive items which may reflect specific needs and issues which are relevant to maternal populations, e.g., sleep, habitual drinking, reward, stress, and boredom (Hunter et al., Citation2009; Ujhelyi Gomez et al., Citation2022).
Overall, the M-DMS shows excellent internal reliability, good test re-test reliability, and demonstrates predictive validity. Both the positive and negative reinforcement subscales were positively associated with AUDIT score, a measure of alcohol behavior and harm, and the TLFB, a measure of quantity of alcohol consumption (weekly units). The associations between AUDIT and motives, and TLFB and motives were greater for negative relative to positive motives. This fits with existing literature which suggests negative reinforcement motives are associated with higher levels of alcohol use and, even when controlling for level of consumption, drinking to cope is related to greater alcohol harm (Anderson et al., Citation2013; Irizar et al., Citation2021; Wicki et al., Citation2017). It is important to note, that existing evidence has not focused on maternal populations but rather the general population or specific age groups (e.g., adolescents and young adults). Therefore, future research utilizing measurement invariance testing is needed to see if our findings are replicated and whether these two motive factors (positive and negative reinforcement) differentially predict alcohol use and/or harm in specific sub-groups of maternal populations. For instance, future work should investigate maternal drinking following trauma (e.g., miscarriage, still birth, infant death, psychological birth trauma) and maternal use of health services (e.g., ante/postnatal mental health and/or alcohol and substance services). Given the direct and indirect potential harms to the mother and child (and wider family) of maternal drinking (Foster & Brown, Citation2017; McGovern et al., Citation2018), understanding which drinking motives are associated with higher alcohol use and harm in mothers is an important area of research.
This work has delivered a unique scale for assessing an important public health issue, but there are several limitations. Although the dispersal of participants across UK regions was fairly high, this is a convenience sample and demographics largely consisted of white British mothers, in heterosexual relationships, with a high level of education and income. Although evidence suggests these demographics are associated with greater alcohol use in mothers (Vicario et al., Citation2023), it will be important for future research to determine the validity of the M-DMS in other populations through measurement invariance testing, including non-UK mothers and those from more marginalized populations. Additionally, we only recorded age of children in the main survey. Our analysis showed that endorsement of negative and positive drinking motives increased the older the youngest child was. This suggests that drinking motives may change during motherhood, perhaps dues to the changing maternal role (e.g., decreased/changing parental responsibilities over time) and changes in drinking behavior as individuals become older (national UK data shows alcohol use increases with age; NHS Digital, Citation2022). However, future research is needed to understand this finding properly.
This work has produced the first drinking motives scale developed solely with maternal drinkers. By providing a validated M-DMS, this work contributes to the growing awareness that maternal drinking (and women’s alcohol use in general) is an important area of research, deserving of tailored research tools. In turn this will improve the strength of research in this area, to meet the growing calls for female-specific health research, interventions, and treatments (Department of Health and Social Care, Citation2022).
Data deposition
Data and analysis script will be deposited on acceptance of manuscript.
Declaration of interest
The authors report there are no competing interests to declare.
Additional information
Funding
Notes on contributors
Paul Christiansen
Dr Paul Christiansen An expert statistian, investigating research integrity and accurate measurement of psychological constructs.
Sally Hunt
Dr Sally Hunt A clinical psychologist, researching associations between substance use and mental health. Her work drives innovative new alcohol prevention programs and interventions in Australia, with a focus on women’s health.
Andrew Jones
Dr Andew Jones An experimental psychologist researching heath behaviors with a focus on stigma and discrimination of addictive behaviors. Expert in complex statistical analysis and open science approaches.
Abigail K. Rose
Dr Abi Rose An experimental psychologist with expertise on girls’ and women’s alcohol use. Her work focuses on the relationships between female drinking, health and wellbeing, and the development of evidence-based alcohol harm reduction interventions and treatment.
References
- Ahlers-Schmidt, C. R., Hervey, A. M., Neil, T., Kuhlmann, S., & Kuhlmann, Z. (2020). Concerns of women regarding pregnancy and childbirth during the COVID-19 pandemic. Patient Education & Counseling, 103(12), 2578–2582. https://doi.org/10.1016/j.pec.2020.09.031
- Anderson, K. G., Briggs, K. E. L., & White, H. R. (2013). Motives to drink or not to drink: Longitudinal relations among personality, motives, and alcohol use across adolescence and early adulthood. Alcoholism, Clinical & Experimental Research, 37(5), 860–867. https://doi.org/10.1111/acer.12030
- Atkinson, A., Sumnall, H., Begley, E., & Jones, L. (2019). A rapid narrative review of literature on gendered alcohol marketing and its effects. Institute of Alcohol Studies.
- Babor, T., Higgins-Biddle, J. C., Saunders, J., & Monteiro, M. (2001). AUDIT: The alcohol use disorders identification test (2nd ed.). Guidelines for Use in Primary Care.
- Babyak, M. A., & Green, S. B. (2010). Confirmatory factor analysis: An introduction for psychosomatic medicine researchers. Psychosomatic Medicine, 72(6), 587–597. https://doi.org/10.1097/PSY.0b013e3181de3f8a
- Baer, J. S., Sampson, P. D., Barr, H. M., Connor, P. D., & Streissguth, A. P. (2003). A 21-year longitudinal analysis of the effects of prenatal alcohol exposure on young adult drinking. Archives of General Psychiatry, 60(4), 377–385. https://doi.org/10.1001/archpsyc.60.4.377
- Basch, C. H., Meleo-Erwin, Z. C., Mohlman, J., Fera, J., & Quinones, N. (2021). Use of the Instagram hashtags #winemom and #momjuice among mothers during the COVID-19 pandemic: Descriptive, cross-sectional study. JMIR Pediatrics & Parenting, 4(2), e28991. https://doi.org/10.2196/28991
- Borschmann, R., Becker, D., Spry, E., Youssef, G. J., Olsson, C. A., Hutchinson, D. M., Silins, E., Boden, J. M., Moreno-Betancur, M., Najman, J. M., Degenhardt, L., Mattick, R. P., Romaniuk, H., Horwood, L. J., & Patton, G. C, Cannabis Cohorts Research Consortium. (2019). Alcohol and parenthood: An integrative analysis of the effects of transition to parenthood in three Australasian cohorts. Drug & Alcohol Dependence, 197, 326–334. https://doi.org/10.1016/j.drugalcdep.2019.02.004
- Cooper, M. (1994). Motivations for alcohol use among adolescents: Development and validation of a four-factor model. Psychological Assessment, 6(2), 117–128. https://doi.org/10.1037/1040-3590.6.2.117
- Cox, W. M., & Klinger, E. (1988). A motivational model of alcohol use. Journal of Abnormal Psychology, 97(2), 168–180. https://doi.org/10.1037/0021-843x.97.2.168
- Crawford, J., Jones, A., Rose, A., & Cooke, R. (2022). ‘You see the pictures the morning after and you’re like I wish I was in them’: An interpretative phenomenological analysis of university student’s alcohol-related regrets. Psychology & Health, 37(4), 490–506. https://doi.org/10.1080/08870446.2020.1867728
- Cudeck, R. (2000). Exploratory factor analysis. In Handbook of applied multivariate statistics and mathematical modelling (pp. 265–296). Academic Press.
- D'Aquino, S., Callinan, S., Smit, K., Mojica-Perez, Y., & Kuntsche, E. (2023). Why do adults drink alcohol? Development and validation of a drinking motives questionnaire for adults. Psychology of Addictive Behaviors: Journal of the Society of Psychologists in Addictive Behaviors, 37(3), 402–415. https://doi.org/10.1037/adb0000877
- Department of Health and Social Care. (2022). Women’s health strategy for England.
- Doherty, M., & Hunt, S. A. (2022). An association between psychological childbirth trauma and hazardous alcohol use. International Journal of Mental Health & Addiction, 21(5), 3185–3198. https://doi.org/10.1007/s11469-022-00784-3
- Erol, A., & Karpyak, V. M. (2015). Sex and gender-related differences in alcohol use and its consequences: Contemporary knowledge and future research considerations. Drug & Alcohol Dependence, 156, 1–13. https://doi.org/10.1016/j.drugalcdep.2015.08.023
- Fleming, K. M., Gomez, K. U., Goodwin, L., & Rose, A. K. (2023). Identifying the motives for and against drinking during pregnancy and motherhood, and factors associated with increased maternal alcohol use. Journal of Public Health, https://doi.org/10.1007/s10389-023-02141-7
- Foster, J., & Brown, K. (2017). Like sugar for adults”: The effects of non-dependent parental drinking on children and families. Institute of Alcohol Studies.
- Freisthler, B., & Price Wolf, J. (2022). Longitudinal changes in self-reported alcohol consumption by mothers’ during the COVID-19 pandemic. Alcohol & Alcoholism (Oxford, Oxfordshire), 58(3), 235–237. https://doi.org/10.1093/alcalc/agac064
- Gilson, K. M., Bryant, C., Bei, B., Komiti, A., Jackson, H., & Judd, F. (2013). Validation of the drinking motives questionnaire (DMQ) in older adults. Addictive Behaviors, 38(5), 2196–2202. https://doi.org/10.1016/j.addbeh.2013.01.021
- Grant, V. V., Stewart, S. H., O'Connor, R. M., Blackwell, E., & Conrod, P. J. (2007). Psychometric evaluation of the five-factor modified drinking motives questionnaire-revised in undergraduates. Addictive Behaviors, 32(11), 2611–2632. https://doi.org/10.1016/j.addbeh.2007.07.004
- Graziani, M., Nencini, P., & Nisticò, R. (2014). Genders and the concurrent use of cocaine and alcohol: Pharmacological aspects. Pharmacological Research, 87, 60–70. https://doi.org/10.1016/j.phrs.2014.06.009
- Griswold, M. G., Fullman, N., Hawley, C., Arian, N., Zimsen, S. R. M., & Tymeson, H. D, GBD 2016 Alcohol Collaborators. (2018). Alcohol use and burden for 195 countries and territories, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet (London, England), 392(10152), 1015–1035. https://doi.org/10.1016/S0140-6736(18)31310-2
- Grossman, E. R., Benjamin-Neelon, S. E., & Sonnenschein, S. (2020). Alcohol consumption during the COVID-19 pandemic: A cross-sectional survey of US adults. International Journal of Environmental Research & Public Health, 17(24), 9189. https://doi.org/10.3390/ijerph17249189
- Harding, K. D., Whittingham, L., & McGannon, K. R. (2021). #sendwine: An analysis of motherhood, alcohol use and #winemom culture on Instagram. Substance Abuse, 15, 11782218211015195.
- Holmila, M., & Raitasalo, K. (2005). Gender differences in drinking: Why do they still exist? Addiction (Abingdon, England), 100(12), 1763–1769. https://doi.org/10.1111/j.1360-0443.2005.01249.x
- Hu, L., & Bentler, P. M. (1999). Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Structural Equation Modeling: A Multidisciplinary Journal, 6(1), 1–55. https://doi.org/10.1080/10705519909540118
- Hunt, G., Antin, T., Bjønness, J., & Ettorre, E. (2016). The increasing visibility of gender in the alcohol and drug fields. In Kolind T, Thom B, Hunt G (Eds.), Handbook of drug and alcohol studies: Social science approaches. SAGE.
- Hunter, L. P., Rychnovsky, J. D., & Yount, S. M. (2009). A selective review of maternal sleep characteristics in the postpartum period. Journal of Obstetrics, Gynecology, & Neonatal Nursery, 38(1), 60–68. https://doi.org/10.1111/j.1552-6909.2008.00309.x
- Institute of Alcohol Studies (2017). Women and alcohol.
- Irizar, P., Jones, A., Christiansen, P., Goodwin, L., Gage, S. H., Roberts, C., Knibb, G., Cooke, R., & Rose, A. K. (2021). Longitudinal associations with alcohol consumption during the first COVID-19 lockdown: Associations with mood, drinking motives, context of drinking, and mental health. Drug & Alcohol Dependence, 226, 108913. https://doi.org/10.1016/j.drugalcdep.2021.108913
- Knight, M., Bunch, K., Felker, A., Patel, R., Kotnis, R., Kenyon, S., & Kurinczuk, J. J., On Behalf of MBRRACE-UK. (2023). (Eds.), Saving lives, improving Mothers’ care core report – Lessons learned to inform maternity care from the UK and Ireland Confidential Enquiries into Maternal Deaths and Morbidity 2019–21. National Perinatal Epidemiology Unit, University of Oxford.
- Koo, T. K., & Li, M. Y. (2016). A guideline of selecting and reporting intraclass correlation coefficients for reliability research. Journal of Chiropractic Medicine, 15(2), 155–163. https://doi.org/10.1016/j.jcm.2016.02.012
- Kuntsche, E., Knibbe, R., Gmel, G., & Engels, R. (2006). Who drinks and why? A review of socio-demographic, personality, and contextual issues behind the drinking motives in young people. Addictive Behaviors, 31(10), 1844–1857. https://doi.org/10.1016/j.addbeh.2005.12.028
- Kuntsche, E., & Kuntsche, S. (2009). Development and validation of the drinking motive questionnaire revised short form (DMQ–R SF). Journal of Clinical Child & Adolescent Psychology: The Official Journal for the Society of Clinical Child and Adolescent Psychology, American Psychological Association, Division 53, 38(6), 899–908. https://doi.org/10.1080/15374410903258967
- Lee, I. A., & Preacher, K. J. (2013). Calculation for the test of the difference between two dependent correlations with one variable in common [Computer software] [Available from: http://quantpsy.org].
- MacCallum, R. C., Browne, M. W., & Sugawara, H. M. (1996). Power analysis and determination of sample size for covariance structure modeling. Psychological Methods, 1(2), 130–149. https://doi.org/10.1037/1082-989X.1.2.130
- Marino, C., Moss, A. C., Vieno, A., Albery, I. P., Frings, D., & Spada, M. M. (2018). Parents’ drinking motives and problem drinking predict their children’s drinking motives, alcohol use and substance misuse. Addictive Behaviors, 84, 40–44. https://doi.org/10.1016/j.addbeh.2018.03.028
- McCarty, C. A., Kosterman, R., Mason, W. A., McCauley, E., Hawkins, J. D., Herrenkohl, T. I., & Lengua, L. J. (2009). Longitudinal associations among depression, obesity and alcohol use disorders in young adulthood. General Hospital Psychiatry, 31(5), 442–450. https://doi.org/10.1016/j.genhosppsych.2009.05.013
- McGovern, R., Gilvarry, E., Addison, M., Alderson, H., Carr, L., Geijer-Simpson, E., et al. (2018). Addressing the impact of nondependent parental substance misuse upon children. A rapid review of the evidence of prevalence, impact and effective interventions.
- NHS Digital (2022). Health survey for England, 2021 Part 1.
- O'Dwyer, C., Mongan, D., Millar, S. R., Rackard, M., Galvin, B., Long, J., & Barry, J. (2019). Drinking patterns and the distribution of alcohol-related harms in Ireland: Evidence for the prevention paradox. BMC Public Health, 19(1), 1323. https://doi.org/10.1186/s12889-019-7666-4
- Palan, S., & Schitter, C. (2018). Prolific.ac: A subject pool for online experiments. Journal of Behavioral & Experimental Finance, 17, 22–27. https://doi.org/10.1016/j.jbef.2017.12.004
- Pelham, W. E., Jr., & Lang, A. R. (1999). Can your children drive you to drink? Stress and parenting in adults interacting with children with ADHD. Alcohol Research & Health: The Journal of the National Institute on Alcohol Abuse & Alcoholism, 23(4), 292–298.
- Public Health England (2017). Alcohol sales in England in 2014: Analysis to assess suitability for inclusion as an indicator in the Local Alcohol Profiles for England.
- Raitasalo, K., Holmila, M., Jääskeläinen, M., & Santalahti, P. (2019). The effect of the severity of parental alcohol abuse on mental and behavioural disorders in children. European Child & Adolescent Psychiatry, 28(7), 913–922. https://doi.org/10.1007/s00787-018-1253-6
- Revelle, W., & Zinbarg, R. E. (2009). Coefficients alpha, beta, omega, and the glb: Comments on Sijtsma. Psychometrika, 74(1), 145–154. https://doi.org/10.1007/s11336-008-9102-z
- Rossow, I., Felix, L., Keating, P., & McCambridge, J. (2016). Parental drinking and adverse outcomes in children: A scoping review of cohort studies. Drug & Alcohol Review, 35(4), 397–405. https://doi.org/10.1111/dar.12319
- Sánchez, A., Fasang, A., & Harkness, S. (2021). Gender division of housework during the COVID-19 pandemic: Temporary shocks or durable change? Demographic Research, 45, 1297–1316. https://doi.org/10.4054/DemRes.2021.45.43
- Sjödin, L., Larm, P., Karlsson, P., Livingston, M., & Raninen, J. (2021). Drinking motives and their associations with alcohol use among adolescents in Sweden. Nordisk Alkohol & Narkotikatidskrift: NAT, 38(3), 256–269. https://doi.org/10.1177/1455072520985974
- Slade, T., Chapman, C., Swift, W., Keyes, K., Tonks, Z., & Teesson, M. (2016). Birth cohort trends in the global epidemiology of alcohol use and alcohol-related harms in men and women: Systematic review and metaregression. BMJ Open, 6(10), e011827. https://doi.org/10.1136/bmjopen-2016-011827
- Sobell, L. C., & Sobell M.B. S. (1993). Timeline followback: A technique for assessing self-reported alcohol consumption. In: R.Z., Litten & J. A. Allen, editors. Measuring alcohol consumption: Psychosocial and biological methods. Humana Press.
- Syed, S., & Gr Wolpert, M. (2018). Parental alcohol misuse and the impact on children: A rapid evidence review of service presentations and interventions. Children’s Policy Research Unit.
- Thrul, J., & Kuntsche, E. (2016). Interactions between drinking motives and friends in predicting young adults’ alcohol use. Prevention Science: The Official Journal of the Society for Prevention Research, 17(5), 626–635. https://doi.org/10.1007/s11121-016-0660-5
- Ujhelyi Gomez, K., Goodwin, L., Chisholm, A., & Rose, A. K. (2022). Alcohol use during pregnancy and motherhood: Attitudes and experiences of pregnant women, mothers, and healthcare professionals. PloS One, 17(12), e0275609. https://doi.org/10.1371/journal.pone.0275609
- van Gils, Y., Franck, E., Dierckx, E., van Alphen, S. P. J., & Dom, G. (2021). The role of psychological distress in the relationship between drinking motives and hazardous drinking in older adults. European Addiction Research, 27(1), 33–41. https://doi.org/10.1159/000507664
- Vicario, S., Buykx, P., Peacock, M., Hardie, I., De Freitas, L., Bissell, P., & Meier, P. S. (2023). Women’s alcohol consumption in the early parenting period and influences of socio-demographic and domestic circumstances: A scoping review and narrative synthesis. Drug & Alcohol Review, 42(5), 1165–1194. https://doi.org/10.1111/dar.13643
- Wicki, M., Kuntsche, E., Eichenberger, Y., Aasvee, K., Bendtsen, P., Dankulincová Veselská, Z., Demetrovics, Z., Dzielska, A., Farkas, J., de Matos, M. G., Roberts, C., Tynjälä, J., Välimaa, R., & Vieno, A. (2017). Different drinking motives, different adverse consequences? Evidence among adolescents from 10 European countries. Drug & Alcohol Review, 36(6), 731–741. https://doi.org/10.1111/dar.12572
- Wilsnack, S. C., Wilsnack, R. W., & Kantor, L. W. (2013). Focus on: Women and the costs of alcohol use. Alcohol Reserach: Current Review, 35(2), 219–228.
- World Health Organisation. (2019). Status report on alcohol consumption, harm and policy responses in 30 European countries.