
ABSTRACT
Background
eLearning can be an effective tool to achieve learning objectives. It facilitates asynchronous distance learning, increasing flexibility for learners and instructors. In this context, the high educational value of videos provides an invaluable primary component for longitudinal digital curricula, especially for maintaining knowledge on otherwise rarely taught subjects. Although literature concerning eLearning evaluation exists, research comprehensively describing how to design effective educational videos is lacking. In particular, studies on the requirements and design goals of educational videos need to be complemented by qualitative research using grounded theory methodology.
Methods
Due to the paucity of randomized controlled trials in this area, there is an urgent need to generate recommendations based on a broader fundament than a literature search alone. Thus, the authors have employed grounded theory as a guiding framework, augmented by Mayring’s qualitative content analysis and commonly used standards. An adaptive approach was conducted based on a literature search and qualitative semi-structured interviews. Drawing on these results, the authors elaborated a guide for creating effective educational videos.
Results
The authors identified 40 effective or presumedly effective factors fostering the success of video-based eLearning in teaching evidence-based medicine, providing a ready-to-use checklist. The information collected via the interviews supported and enriched much of the advice found in the literature.
Discussion
To the authors’ knowledge, this type of comprehensive guide for video-based eLearning needs has not previously been published. The interviews considerably contributed to the results. Due to the grounded theory-based approach, in particular, consensus was achieved without the presence of a formal expert panel. Although the guide was created with a focus on teaching evidence-based medicine, due to the general study selection process and research approach, the recommendations are applicable to a wide range of subjects in medical education where the teaching aim is to impart conceptual knowledge.
Introduction
Motivation
Despite extensive efforts to establish effective teaching in the fields of medical statistics and epidemiology, we observed the persistent problem of ‘statistical illiteracy,’ that is, the inability to adequately interpret statistical data and test results, which is known to be an issue in medical risk communication and decision-making [Citation1]. Although most medical curricula, as at our institution, address medical statistics and epidemiology quite extensively, leading to satisfactory exam results, the presence of statistical illiteracy in trained doctors points to a lack of long-term retention [Citation1,Citation2].
Longitudinal learning, including spaced learning, promises longer recall of imparted knowledge, especially when active learning techniques (e.g., quizzes) are employed, while the feasibility of longitudinal educational modules is dependent on whether asynchronous learning opportunities are implementable at reasonable costs. With this in mind, we have focused our research on video-based eLearning, which we consider to be a suitable tool for this use case.
In teaching evidence-based medicine, we have experienced an urgent need for the teaching of conceptual knowledge and the communication of ideas, concepts, and techniques for problem solving. This applies even more in our use case as the ‘statistical’ way of thinking is imported into medical school curricula from a different field. To ensure long-term retention of this way of thinking, short, easy-to-understand chunks of knowledge seem to be ideal. This becomes even more important if the statistical way of thinking is not integrated into learners’ daily lives. In particular, the understanding of unaccustomed concepts may depend on opportunities for review. This is another reason for focusing on video-based eLearning to support these curricular components in medical education.
Motivated by the above considerations, we implemented a longitudinal, asynchronous digital curriculum based on educational videos at RWTH Aachen’s faculty of medicine to supplement existing classroom teaching. Educational video is a cornerstone of our longitudinal curriculum and is augmented by several other modalities (e.g., text-based learning materials, e-tests, and player-vs.-player quizzes). Therefore, a substantial need exists for videos that generate concrete learning achievements.
In our search for a comprehensive, ready-to-use guide for creating video-based eLearning offerings in medical education, we were confronted with the absence of such work. For this reason, we decided to conduct a systematic review and interviews to define best practices and to create such a guide.
State of research
Prior to describing the creation of a comprehensive guide on video-based eLearning, a brief overview of the known issues should be helpful.
Studies have shown that eLearning in medical education is effective for imparting knowledge under specified conditions, for example, in teaching evidence-based medicine [Citation3,Citation4]. However, eLearning is not always more effective than other forms of learning [Citation5]. Vaona et al. stated in their Cochrane Review that eLearning interventions cause a large positive effect when compared to no intervention, and only a small positive effect when compared to traditional learning, although these results are not conclusive. They concluded, ‘Even if e‐learning could be more successful than traditional learning in particular medical education settings, general claims of it as inherently more effective than traditional learning may be misleading’ [Citation5].
With regard to videos, the literature shows that they can be useful for their impact on learning [Citation6–8] and are widely used in education [Citation9]. A high educational value is also attributed to videos because of their advanced multimedia level in Mayer’s cognitive theory of multimedia learning [Citation10,Citation11]. This theory is well known and widely respected in the literature for its assumption that different channels process visuals and auditive content in the learner’s mind, with resulting implications that are outlined in more depth below. Consequently, some authors even describe this theory as unique with respect to its impact on multimedia design [Citation12].
Moreover, students’ perceptions of educational videos are often subjectively reported to be positive in various contexts, not just at our institution [Citation13,Citation14], and videos may be more engaging than conventional learning materials (e.g., textbooks) [Citation8]. Nonetheless, Guo et al. have shown that student engagement collapses after a median of six minutes of video [Citation9]; therefore, we assume that there is either a pressing need for short videos or for the improvement of educational video formats.
Furthermore, some studies show that educational video does not robustly lead to better knowledge acquisition or effectiveness compared to other forms of learning [Citation15–17], although, as with eLearning in general, no comprehensive real-world assessment has been provided. This insight might depend on how videos are designed and the context in which they are used [Citation5,Citation17]. Unfortunately, researchers do not always report how the videos or eLearning content used in evaluation trials were created; consequently, the knowledge acquired to develop a best-practice video-based eLearning program is limited [Citation18]. However, since many eLearning modalities include educational videos (e.g., [Citation19]), our focus on best practices for educational video has the potential to make a highly pertinent contribution toward better eLearning.
Instructional design for video-based eLearning
Our search for guidance on effective eLearning design yielded general underlying principles, such as the ADDIE model, which is based on generic analysis, design, development, implementation, and evaluation [Citation20]. Its application helps to establish a structure for creating and maintaining educational interventions but does not answer the question of how exactly the individual domains should be implemented.
Guidelines for instructional design and their possible implementation by leveraging software are found in Overbaugh’s ‘Research-Based Guidelines for Computer-Based Instruction Development,’ published in 1994 [Citation21]; however, this publication neglects the current developments and possibilities of educational videos.
In the design of effective educational videos, Mayer’s cognitive theory of multimedia learning [Citation10,Citation11] represents a milestone publication. According to this theory, the learner’s mind uses different ‘channels’ to process verbal and visual content (‘dual channel’), and each channel is only able to handle a limited amount of information (‘limited capacity’). In addition, learning success hinges on the learner’s cognitive processing during learning (‘active processing’) [Citation10]. This theory is consistent with and incorporates the cognitive load theory of Sweller et al., which assumes that the verbal and visual channels have respective limited capacities [Citation22,Citation23]. Although the principles introduced by Mayer are essential for creating well-designed videos, applying them in isolation does not necessarily lead to perfect results, as other design and instructional aspects remain unaddressed.
Furthermore, various studies on effective educational video design exist [Citation14,Citation24–28], some of which were published only after our project began [Citation29,Citation30]; however, we consider these valuable publications to be insufficient on their own to provide a comprehensive guide to video-based eLearning or to meet our needs in teaching evidence-based medicine due to their focus on specific aspects, different levels of conceptions, or experience-led approaches rather than on a comprehensive, ready-to-use, evidence-based feature set or framework for generating effective educational videos.
As we ourselves would have greatly appreciated evidence-based guidelines for creating instructional videos for our own and other institutions that explained related difficulties (or at least a guiding checklist pointing out important issues traditionally encountered), especially in creating or evaluating eLearning resources [Citation31], we decided to strive for such a guiding document.
To ensure the highest possible quality for this document, a systematic review, which ideally can include several randomized controlled trials per item, suggests itself. To close any gaps in the evidence in a reasonable way, a consensus should then be reached, as in a formal guideline-creation process. However, after a preliminary search, we encountered a paucity of randomized trials in this field. To overcome this literature gap under the given circumstances, an approach along the lines of grounded theory [Citation32–34] was deemed particularly appropriate in view of the topicality and significance of the subject. A grounded theory approach can augment existing evidence from the literature at a higher level than expert opinions alone to achieve categorization, relativization, and consensus for a guiding document. This eliminates the necessity of conducting the multitude of studies required while still achieving high representativity based on a defined methodology.
Objective
In the belief that tailoring an educational program to a target group may be useful to maximize student engagement and achievement, we investigated our learners’ needs by focusing our research on this question: What form should successful video eLearning take, especially in teaching evidence-based medicine?
Materials and methods
To establish requirements for educational video (general criteria for adequate use and specific design requirements), we dovetailed the literature search and interviews after conducting preliminary requirement analysis based on the literature, resulting in the ‘spiral model’ used in this study. Our approach is summarized in .
Figure 1. “Spiral model” – Process model for adapting the requirement analysis to subsequent interviews.

To better interpret, balance, and apply the findings in the literature (which were often obtained under narrow parameters) as well as theories, we employed the following methodology:
We gathered evidenced insights from the literature; however, to consistently interpret and merge the findings, we required qualitative research methods and statements from different stakeholder perspectives. In addition to providing a methodologically independent confirmation of previous findings, this approach allows the discussion of aspects not yet considered in the literature.
To create a defined methodology for our work, we selected grounded theory as the guiding framework and incorporated commonly used standards to strengthen the methodology and meet established reporting standards, as shown in .
Figure 2. Grounded theory approach incorporating different standards of reporting.
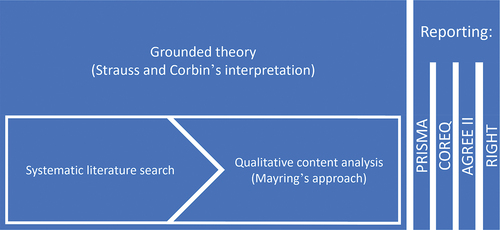
To this end, we used grounded theory methodology per Strauss and Corbin’s interpretation [Citation32–34]. Furthermore, we respected Mayring’s approach to qualitative content analysis [Citation35,Citation36] in planning, performing coding, interpretation, evaluation, and reporting.
Our research approach is based on essential elements of grounded theory. These include the analysis of data obtained, which is directly interwoven with data collection, whereupon the latter is influenced in the sequel. Furthermore, regarding ‘theoretical sampling,’ we decided to make our interview population as diverse as possible to obtain conceptual representativeness for the stakeholders, especially regarding study progress, age, and academic performance. In addition, we anchored the aspect of ‘theoretical saturation’ in our approach, terminating the recruitment of further interview partners once saturation was reached.
However, our objective of creating a comprehensive guide for successful video eLearning involves various aspects that we do not believe, in good conscience, would be limited to a few core categories that are axially related to the remaining categories; therefore, we deviated from the established principles here.
The subsequent development of the interview content by applying grounded theory methodology enabled the achievement of categorization, relativization, and consensus on the part of the interviewees, who represented the respective stakeholders at the end-user level. To achieve the highest possible quality, our work was guided by the characteristics required by the RIGHT statement [Citation37,Citation38] and in AGREE II [Citation39–41], which are commonly used for clinical guideline development and recommended by the EQUATOR network. It should be noted that we are aware that our work does not fully reflect a ‘classical’ guideline development approach with an expert panel.
To comply with established standards in the individual steps of our work, we followed the PRISMA checklist [Citation42] for the literature search underlying our grounded theory approach and the COREQ statement [Citation43] for reporting qualitative characteristics. Since human beings were involved in our study, we consulted the Ethics Committee at University Hospital RWTH Aachen. They approved our protocols, declaring that their vote is not required (ID EK 091/18).
Literature search
We performed a literature search using PubMed due to our focus on medical education. The search began in November 2017 and was intensively conducted from February – March 2018, as well as subsequently (see below) to stay up to date. We chose an explorative approach to generate a basis for semi-structured interviews and fulfill the requirement analysis.
We searched for literature describing concepts and methods for designing eLearning content, especially videos or parts thereof (e.g., animations). We focused our search on studies involving undergraduate students as the primary population and graduate learners as the secondary population, each trained on concepts and theories using different design elements, which were then compared to each other or to traditional design elements, allowing evidence-based principles to be derived. We subsequently defined the eligibility criteria. We included articles that presented theories and studies on how to design video-based learning or eLearning for concept delivery, giving concrete (evidence-based) advice. We included reviews, randomized controlled trials, controlled trials, case reports, and expert opinions. Articles were excluded from this synthesis if they did not primarily focus on asynchronous learning capabilities or mainly discussed concepts for flipped classrooms, virtual seminars, or virtual enriched group work (e.g., problem-oriented learning); if they focused on procedural craft skills as often taught in surgery (the wrong setting); or if they only described the status quo of eLearning applications without offering critical appraisal or deriving advice. Because of our focus on video-based, asynchronous eLearning, we limited the search to the period starting in 2006, the first full year since the emergence of YouTube® as a well-known online tool for making videos available online.
We started our search using ‘((((video OR educational video OR video-based eLearning OR video based learning OR video eLearning OR video learning OR medical video OR video tape recording[MeSH]) AND (online)) AND (medical students[MeSH] OR students[MeSH])) AND (educational technology[MeSH])) AND (guidelines as topic[MeSH])’ as the initial search string. After obtaining only one relevant paper out of two results, we widened our search by varying the search string by combining the terms in the initial search string in different ways. Our search strings can be found in Box 1 in the Appendix.
The titles and abstracts were screened for potentially relevant articles, and then full texts were accessed. presents a graphical summary according to the PRISMA checklist [Citation42].
Figure 3. Graphical summary according to the PRISMA guidelines.
Preliminary requirement analysis
Based on the literature search described, we conducted a preliminary requirement analysis and expanded it according to assumptions arrived at deductively and inductively. User stories were chosen as the requirement analysis format. Based on this analysis, we selected important and controversial points (e.g., style of animations, Khan style [handwritten, step-by-step explanations with voice commentary], examples in explanations [amount and quality], and interactions) to serve as interview topics and developed a semi-structured interview guide. To avoid focusing solely on the points revealed by the literature search, the interview guide included open and broad questions on how eLearning and educational video should be developed in the participant’s opinion.
This interview guide can be found in the Appendix.
Adapting the data elicitation – “spiral model”
To enrich and adapt the preliminary requirement analysis, we immediately took the new aspects mentioned in an interview into consideration for discussion with participants in subsequent interviews.
For this purpose, a literature search followed every interview in which new aspects were mentioned. Based on the results and the interview content itself, we enhanced the preliminary requirement analysis and adapted the interview content for subsequent interviews, as shown in . Furthermore, categorization, relativization, and consensus were achieved via this process, as the points mentioned in previous interviews were thereby discussed with the interviewees. Consequently, interviewees were confronted with either contrasting or similar statements previously made by others, in addition to statements derivedfrom literature, and then provided their statement.
Subsequent search
To stay up to date, we conducted annual literature searches using our initial search string and the first four strings derived therefrom (see Box 1 in the Appendix) to add new articles and aspects. The following outlines our suggested updating procedure:
A renewed literature search should be conducted at least every three years and new findings added. In the event of substantial changes or the emergence of new features considered worthy of discussion, a renewed implementation of the interview-based methodology should be considered at least every 10 years.
COREQ-compliant description of the interview process
To meet the reporting standards in qualitative research, we respected the consolidated criteria for reporting qualitative research (COREQ) by Tong et al. [Citation43].
Study design
As described above, the interview content was defined based on the preliminary requirement analysis; however, performing the interviews successively resulted in the expansion of the preliminary requirement analysis and, therefore, the interview content.
We selected the participants by academic semester. At least one participant from each year was recruited to obtain a cross section of the various potential eLearning needs of students across several years. The main target group of our eLearning curriculum consisted of students for whom the start of research activities and clinical work were assumed to be imminent. In addition, without such eLearning, students in advanced semesters would have had their last training in evidence-based medicine years before. Therefore, we aimed to recruit a disproportionate number of 4th year students (according to the German six-year curriculum) as representatives of the main target group.
Other factors for recruiting participants were cross sections of academic performance and age, the approximate female/male ratio by course of study, and reachability by the interviewer.
Data collection
We provided a semi-structured interview guide for every interview (see the Appendix). We conducted only one interview per participant. After approval, the interviews were audio-recorded using a professional pocket music recorder. No participant disagreed to the recording. In addition, field notes were taken during and immediately after the interviews.
Following the concept of ‘theoretical saturation’ from grounded theory, we planned to cease further interviews when the last interview conducted did not add new relevant information. To ensure a sufficiently large cross-section, the minimum number of participants was set at 11 following the considerations stated above.
The transcripts were not returned to the participants as our research variant was based on Mayring’s qualitative content analysis approach and grounded theory methodology and, thus, complete transcripts were not created.
Analysis
Our analysis was guided by this research question: What form should successful video eLearning take, especially in teaching evidence-based medicine? Due to our preliminary requirement analysis, we documented our preconceptions in our interview guide. We chose a mixed research design incorporating descriptive (deductive category development, top-down process) and explorative (inductive category development, bottom-up process) elements [Citation35] to investigate our learners’ needs and desires and to discuss specific points derived from the literature. As a coding unit of up to three keywords (in the sense of a paraphrase) was defined, the context unit comprised up to several contiguous sentences. The evaluation unit consisted of interviews. Thus, all statements concerning a single category were analyzed consecutively.
To save time and resources, we transcribed the audio-recorded interviews only partly in the spirit of a selective protocol [Citation35]. Due to limited resources, the audio material was transcribed by the researchers themselves. However, this allowed the transcription and coding rules to be applied simultaneously. Whenever a passage met the requirements of the coding guide for deductive categories (available in the Appendix) or our procedure for inductive category development (see below), the entire passage was transcribed and associated with the interview number and the time code that marked the start of the relevant passage in the audio file. Therefore, the partly transcribed interviews nevertheless included relevant information.
To ensure that the inductive category assignment complied with the open questions and possible non-predetermined interview content, we referred to our research question and previous content-analytical units. We established the categories as every implementable feature, design element, or variant of content presentation that could be considered a (potentially) valuable part of a best-practice eLearning implementation. As a level of abstraction, we defined generally applicable statements, comments, and viewpoints from which advice could be derived and which could be enriched with concrete examples and statements, although the latter was not necessary.
After the first run of coding, the categories were controlled, and interrelated categories were joined. During the second instance of listening to all the interviews, the complete category list was accessible. Aspects mentioned regarding each category were allocated and transcribed as before, including the assignment of time stamps. For the analysis, we used transcribed passages. The time stamps ensured that they were reidentifiable in the raw data. We adapted the categories during coding.
Intercoder agreement was ensured by weekly supervision dialogues between the authors, including the presentation, discussion, and reworking of the coding performed by confirming the analysis, as suggested by Mayring for very open material with an explorative research question [Citation35]. In addition, as the project progressed, we discussed the theories and findings of the study at department meetings to obtain surrogate communicative validation from our colleagues as learners and educators.
Formulation of recommendations
To meet our objective of providing comprehensive guidelines for creating educational videos despite the paucity of randomized controlled trials, we have included as recommendations all characteristics shown or assumed to be effective, provided that the following criteria apply:
– the derived recommendation appears relevant for concept delivery to the target group (undergraduate learners);
AND
– the derived recommendation is based on a higher level of evidence than qualified expert opinion, OR, if it is an expert opinion, it was confirmed in discourse with the interviewees AND/OR the authors. Furthermore, we made the decision to allow the formulation of recommendations based on the applicable legal situation and the advice derived therefrom.
Results
Systematic research yielded no paper describing a comprehensive evidence-based best practice approach to educational video creation for teaching evidence-based medicine. However, we found papers describing approaches to creating videos in other fields of medicine [Citation29,Citation44] and scientific education [Citation45] as well as general considerations regarding various aspects of creating videos [Citation30,Citation46] or eLearning/computer-based learning materials and learning platforms [Citation21,Citation47].
Like many previous researchers, we agree that Mayer’s cognitive theory of multimedia learning is an important underpinning concept for creating educational video content. Much advice on creating well-designed educational videos can be traced back to his principles of ‘dual channels,’ ‘limited capacity,’ and ‘active processing’ [Citation29], including achieving the balanced utilization of both channels while avoiding cognitive overload to provide the best possible processing of content as efficiently as feasible. In fact, the appropriate amount of information on each channel is a key factor for well-designed learning materials.
Furthermore, research by de Leeuw et al. describes a model for designing postgraduate digital education, mentioning important points for creating, maintaining, and evaluating eLearning offerings on a conceptual level; however, no concrete advice is given on how to design the educational intervention itself [Citation48].
We also identified many additional points, such as design, administrative, and legal (i.e., data protection, copyright, and personality rights) issues.
presents the detailed results of our spiral model approach, including the literature search and the interviews, while shows the results of the interview analysis.
Table 1. Literature-based requirement analysis for eLearning content and educational videos – User stories.
Table 2. Results of analysis of semi-structured interviews at RWTH Aachen University in 2018 (n = 11).
We interviewed a total of 11 participants (one student from each year [Years 1–6 in the German six-year curriculum], in addition to five students from Year 4). Eight participants were female and three male. This was equivalent to approximately 73% females and nearly coincided with the gender representation at RWTH Aachen’s faculty of medicine (69% male/31% female) [Citation59]. Every potential participant who was asked to participate did so. No one dropped out.
We carried out face-to-face interviews in various locations to suit the participants (six in a social room at the faculty of medicine, four at home, and one in a café). Non-participants were present in the social room and in the café, but they were usually more than three meters away and out of auditory range. All the participants were medical students at RWTH Aachen University and aged 18–30 years. The participants’ academic performance ranged from sufficient to excellent. The average interview duration was 25.36 minutes (SD 7.59 min; median 23.12 min; range 15.58–36.67 min).
Because the last interviews conducted did not deliver new relevant information, we did not recruit more participants than the initially planned 11, following the concept of ‘theoretical saturation’ from grounded theory.
As intended, during the interview process, it was possible to discuss the reported characteristics in the literature as effective or presumably effective, thus achieving categorization, relativization, and consensus on the part of the interviewees as representatives of the respective stakeholders at the end-user level. Additionally, the spiral model enabled reflection on the temporally preceding interview content with the literature research findings and discussion of the results obtained with the subsequent interviewees. Thus, we obtained a broader basis for the development of recommendations than a literature review alone could have provided.
From the interview analysis, 10 deductively formulated categories and eight inductively found categories of content emerged (see ).
Interestingly, various categories came up inductively, although we could have deductively set them because such recommendations appear in the literature. We considered these categories to be so self-evident that they did not need any discussion; however, we would have implemented them without further discourse due to their plausibility (e.g., ‘reduce extraneous processing,’ ‘structuring,’ and ‘chapters’). In our opinion, this underscores the perceived importance of these features and adds valuable focus for the further development of educational content for learners’ needs.
Most advice found in the literature search was confirmed through the interviews, and the students’ comments and clarifications enriched it. ‘Khan style’ (hand-written step-by-step explanations with voice commentary) and ‘talking head’ style (adding the speaker’s head to the visuals) were the only two areas in which the recommendations of the literature and the students’ opinions clearly differed. Our sample preferred subsequent text animations instead of the traditional Khan style.
Furthermore, the importance of take-home messages was outlined in the interviews. To our knowledge, however, this point is not a prominent recommendation in the literature.
Although the interviews mainly supported the previously found recommendations, they provided additional (specific) information about the students’ opinions and examples of what worked well in eLearning at our institution and what might work in various fields and situations. Therefore, the interviews helped accentuate the suggestions found in the literature.
presents our conclusions, condensed into a single checklist for use in producing our videos (our checklist for educational videos for video-based eLearning). We identified 40 important points for well-designed educational videos and enriching techniques with concrete, processable questions to ensure the consideration of relevant design factors before creating content. Due to the various contexts of implementation, not every point must necessarily be respected in every video project.
Table 3. Our checklist for educational videos for video-based eLearning.
Discussion
Although eLearning and educational video are prominent topics in current research and university discourse, we were unable to find a comprehensive paper that considered most of the points relevant to our needs in relation to creating a video-based eLearning course in evidence-based medicine. Most of the recommendations we discussed can be found via a literature search, but to our knowledge, a broad compilation of these is novel.
Our work provides an extensive guide for video-based eLearning to meet the needs of teaching evidence-based medicine. In the context of the interviewed sample (consisting solely of medical students) and our focus on teaching the ‘statistical’ way of thinking (which is an unaccustomed concept for many medical students and is not integrated into the learners’ daily lives), the user value was reported to be highly appropriate for the targeted group. Nonetheless, our results should be applicable to other fields of (medical) education, especially where the aim is teaching conceptual knowledge and communicating ideas, concepts, and techniques for problem solving, as our research focus was applicable to such settings.
However, our work must be compared to articles that describe the development of eLearning offerings on a conceptual level (e.g., de Leeuw et al. [Citation48]). Moreover, approaches such as the ‘Online Nursing Education Best Practices Guide’ by Authement and Dormire [Citation47] should be mentioned. This approach provides an instructor checklist with 33 points focusing mainly on organizational issues for online education, which represents an important support for creating and conducting successful eLearning programs. Choe et al.’s ‘Summary of Best Practices for Creating Engagement in Educational Videos’ [Citation30] is based on a text-based survey of undergraduate students. It describes and compares different video styles based on Mayer’s principles of multimedia learning, as well as students’ perceptions, and it can be a valuable aid for video creation. The aim of their work is close to our own, namely, to assist in quality educational video development, although it focuses on comparing different forms of presentation to derive valuable recommendations. However, the goal of their work was not to develop comprehensive guidelines for creating educational videos, and it included neither a systematic literature review nor consensus developed via interviews. Furthermore, we acknowledge studies such as that by Young et al. [Citation29], who outlined principles for effective educational videos. Although the authors describe how their techniques are used for a specific topic, the beneficial general aspects are clearly identifiable. Moreover, the work of Roshier et al. [Citation14] deserves mention. Based on focus group interviews and the authors’ experiences, it presents valuable suggestions for developing a video-based eLearning offering. Although the authors neither conducted a systematic literature review nor focused on educational theories, they provide orientating guidance that can contribute to the successful implementation of educational videos online.
General underlying models, such as the ADDIE model, which is based on generic analysis, design, development, implementation, and evaluation [Citation20], and dividing video creation into preproduction, production, and postproduction stages [Citation46], should also be mentioned. In the sense of the ADDIE model, our work enriches the design and development component, specifically for educational videos in teaching conceptual knowledge in medicine.
Although some findings overlap, our compilation of the requirements and recommendations in practicable guide form, informed by the available evidence and the findings of our qualitative research approach, enhances the existing literature at a new level by covering a broad spectrum of issues and providing concrete recommendations along with a checklist.
While our work and teaching aim relate to teaching concepts and knowledge but not (surgical) procedures, we excluded guidelines on surgical education videos from our literature search. Nevertheless, considering approaches from surgery might enhance the recommendations, particularly for situations where the teaching aim cannot be categorized as either conceptual knowledge or surgical procedures. Karic et al.’s [Citation60] ‘Ideal Third Year Medical Student Educational Video Checklist’ mentions guidance and describes critical maneuvers, time efficiency, identifying instruments, and trocar placement as key aspects, among others. Apart from time efficiency, the ‘surgical setup’ is also described by Chauvet et al. [Citation61] as a crucial point for creating effective surgical educational videos. Providing all the information necessary to teach vividly is also important in teaching concepts and educational video in general.
In our work, we encourage the enrichment of data collection with interviews to confirm suitability for individual situations. Although our sample size of interviews was modest (n = 11), the different points of view provided general considerations, further fields of interest, and specific comments on the appropriate form of video-based eLearning in our setting that may not have otherwise arisen. In addition, the confirmation and, sometimes, contextual relativization provided were relevant.
Interestingly, one point that was crucial to the interviewed students and, in our opinion, a relevant aspect of effective video design was the use of take-home messages. To our knowledge, this is not prominently recommended in the literature. This aspect certainly calls for further research.
However, given our results, one must keep in mind that good teaching always includes the individual component of the respective teacher, and the context and audience must always be considered. Thus, in some situations, a humorous approach may have a positive effect, whereas in others, it may be inappropriate (e.g., in some medical topics).
Furthermore, the potential gaps between ‘pleasing students,’ ‘perceived beneficial factors by students,’ and ‘fostering learning’ should be noted. Although the aim should be to maximize both learning and student satisfaction, particularly effective features for learning may be unpopular and vice versa. For instructional videos that follow Mayer’s principles, thanks to the data presented by Choe et al. [Citation30], there is at least some indication that ‘pleasing students’ and ‘fostering learning’ need not be mutually exclusive, as evidenced by the similar effectiveness of the video styles examined. Therefore, one could fall back on features perceived by students as positive and satisfying. However, it is a limitation of this work that only characteristics derived from Mayer’s cognitive theory of multimedia learning were considered. Regarding other characteristics, further research, preferably randomized controlled trials, is necessary.
Regarding the evaluation issue, it should be noted that this cannot be concluded with the first review but must be continued on an ongoing basis. In this regard, continuous evaluation systems and measures should be established. If more than sporadic criticism arises, certain elements could be reconsidered and improved if necessary.
Regarding the methodology, the ability to substantiate any guideline recommendation with a clear body of studies is highly desirable. Preferably, a meta-analysis of multiple randomized controlled trials should be conducted, each examining only one feature, and recommendations should be developed from the resulting body of data. However, since the necessary studies do not exist on a sufficiently large scale and cannot be produced with reasonable effort by most research teams, our grounded theory approach is crucial to filling this gap.
It is important to note that the guidelines and checklist were compiled using grounded theory as a guiding framework; thus, the results should be formally considered interpretative and theories in progress, given grounded theory’s inherent methodology. However, we have mitigated this aspect as far as possible by incorporating established standards and applying the resulting defined methodology. Thanks to grounded theory as a guiding framework, we were able to combine, in a meaningful manner, accepted methods that, in themselves, would not be subject of this criticism. Thus, grounded theory fulfills an intermediary role, as this approach integrates existing evidence, classifies it, expands it through interviews, and thereby achieves categorization, relativization, and consensus. Thus, using our approach, we can deliver recommendations of higher value than expert opinions on their own.
Our approach offers creators a guide to designing an educational video set and/or reviewing one using our checklist for educational videos for video-based eLearning. We are aware that not every single point must be implemented in every context, but by referring to the literature in , a creator can check whether a characteristic mentioned applies to a given project. Creators should at least consider all the items and be able to justify why not all have been implemented.
In this context, it should be mentioned again that we elaborated our checklist for the transfer of conceptual knowledge so that for intended applications (e.g., skill transfer), practitioners can check whether all of the recommendations should be applied in a given setting in this way (e.g., the controversy about avoiding background music [Citation50]).
Our guide can also be used as a valuable basis for further evaluation and description of implemented eLearning offerings. Using our checklist, important features can be evaluated to improve outcomes, and reporting gaps can be identified and resolved in the revision process. Thus, whether reported outcomes are influenced by unknown design aspects can be revealed. Practitioners do not always report how the videos used in evaluation trials were created [Citation18], thus, we propose our checklist as a practical tool for reporting relevant design decisions in creating educational videos.
Conclusion
We created a comprehensive guide for creating video-based eLearning offerings for teaching evidence-based medicine using a spiral model approach consisting of grounded theory methodology, a systematic literature search, and student interviews to reach a consensus. The 40-item checklist introduced can be useful for creating, reviewing, and reporting on educational videos, especially if they focus on teaching conceptual knowledge.
Outlook
Based on our guide for educational video creation, we developed a video-based eLearning offering to address the abovementioned statistical illiteracy of medical students. Our procedure, its implementation, how we dealt with problems that arose, and the evaluation trial are planned to be reported in a further publication.
Ethical approval
We consulted the Ethics Committee at University Hospital RWTH Aachen about this study as part of our research project (ID EK 091/18). They approved our protocols, declaring that their vote is not required.
Acknowledgment
The authors wish to thank all students who took part in the interviews.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Additional information
Funding
References
- Gigerenzer G, Gaissmaier W, Kurz-Milcke E, et al. Helping doctors and patients make sense of health statistics. Psychol Sci Public Interest. 2007;8(2):53–21. doi: 10.1111/j.1539-6053.2008.00033.x
- Wegwarth O, Schwartz LM, Woloshin S, et al. Do physicians understand cancer screening statistics? A National Survey of primary care physicians in the United States. Ann internal med. 2012;156(5):340–U152. doi: 10.7326/0003-4819-156-5-201203060-00005
- Ahmadi S-F, Baradaran HR, Ahmadi E. Effectiveness of teaching evidence-based medicine to undergraduate medical students: A BEME systematic review. Med Teach. 2015;37(1):21–30. doi: 10.3109/0142159X.2014.971724
- Weberschock T, Sorinola O, Thangaratinam S, et al. How to confidently teach EBM on foot: development and evaluation of a web-based e-learning course. Evid Based Med. 2013;18(5):170–172. doi: 10.1136/eb-2012-100801
- Vaona A, Banzi R, Kwag KH, et al. E-learning for health professionals. Cochrane Database Syst Rev. 2018;2018(8). CD011736. doi: 10.1002/14651858.CD011736.pub2
- Chi DL, Pickrell JE, Riedy CA. Student learning outcomes associated with video vs. paper cases in a public health dentistry course. J Dent Educ. 2014;78(1):24–30. doi: 10.1002/j.0022-0337.2014.78.1.tb05653.x
- Murthykumar K, Veeraiyan DN, Prasad P. Impact of video based learning on the perfomance of post graduate students in biostatistics: a retrospective study. J Clin Diagn Res. 2015;9(12):ZC51–3. doi: 10.7860/JCDR/2015/15675.7004
- Stockwell BR, Stockwell MS, Cennamo M, et al. Blended learning improves science education. Cell. 2015;162(5):933–936. doi: 10.1016/j.cell.2015.08.009
- Guo PJ, Kim J, Rubin R. How video production affects student engagement, In Proceedings of the first ACM conference on Learning @ scale conference - L@S ’14; Atlanta, Georgia, USA. 2014. p. 41–50.
- Mayer RE. Applying the science of learning: evidence-based principles for the design of multimedia instruction. Am Psychol. 2008;63(8):760–769. doi: 10.1037/0003-066X.63.8.760
- Mayer RE. Applying the science of learning to medical education. Med Educ. 2010;44(6):543–549. doi: 10.1111/j.1365-2923.2010.03624.x
- Yue C, Kim J, Ogawa R, et al. Applying the cognitive theory of multimedia learning: an analysis of medical animations. Med Educ. 2013;47(4):375–387. doi: 10.1111/medu.12090
- Lehmann R, Seitz A, Bosse HM, et al. Student perceptions of a video-based blended learning approach for improving pediatric physical examination skills. Ann Anat. 2016;208:179–182. doi: 10.1016/j.aanat.2016.05.009
- Roshier AL, Foster N, Jones MA. Veterinary students’ usage and perception of video teaching resources. BMC Med Educ. 2011;11(1):1. doi: 10.1186/1472-6920-11-1
- Brockfeld T, Muller B, de Laffolie J. Video versus live lecture courses: a comparative evaluation of lecture types and results. Med Educ Online. 2018;23(1):1555434. doi: 10.1080/10872981.2018.1555434
- Higgins Joyce A, Raman M, Beaumont JL, et al. A survey comparison of educational interventions for teaching pneumatic otoscopy to medical students. BMC Med Educ. 2019;19(1):79. doi: 10.1186/s12909-019-1507-0
- Suppan M, Stuby L, Carrera E, et al. Asynchronous Distance Learning of the National Institutes of Health stroke scale during the COVID-19 pandemic (E-Learning vs video): randomized controlled trial. J Med Internet Res. 2021;23(1):e23594. doi: 10.2196/23594
- Yiu SHM, Spacek AM, Pageau PG, et al. Dissecting the contemporary clerkship: theory-based educational trial of videos versus lectures in medical student education. AEM Educ Train. 2020;4(1):10–17. doi: 10.1002/aet2.10370
- Frankl SE, Joshi A, Onorato S, et al. Preparing future doctors for telemedicine: an asynchronous curriculum for medical students implemented during the COVID-19 pandemic. Acad Med. 2021;96(12):1696–1701. doi: 10.1097/ACM.0000000000004260
- Allen WC. Overview and Evolution of the ADDIE Training System. Adv Dev Hum Resour. 2006;8(4):430–441. doi: 10.1177/1523422306292942
- Overbaugh RC. Research-based guidelines for computer-based instruction development. J Res Comput Educ. 1994;27(1):29–47. doi: 10.1080/08886504.1994.10782114
- Mayer R, Moreno R. Nine ways to reduce cognitive load in multimedia learning. Educ Psychol. 2003;38(1):43–52. doi: 10.1207/S15326985EP3801_6
- Sweller J. Implications of cognitive load theory for multimedia learning. In: Mayer RE, editor The Cambridge handbook of multimedia learning. Cambridge: Cambridge Univ. Press; 2005. pp. 19–30.
- Brame CJ. Effective educational videos: principles and guidelines for maximizing Student learning from video content. CBE Life Sci Educ. 2016;15(4):es6. doi: 10.1187/cbe.16-03-0125
- Dong C, Goh PS. Twelve tips for the effective use of videos in medical education. Med Teach. 2015;37(2):140–145. doi: 10.3109/0142159X.2014.943709
- Norman MK. Twelve tips for reducing production time and increasing long-term usability of instructional video. Med Teach. 2017;39(8):808–812. doi: 10.1080/0142159X.2017.1322190
- Rana J, Besche H, Cockrill B. Twelve tips for the production of digital chalk-talk videos. Med Teach. 2017;39(6):653–659. doi: 10.1080/0142159X.2017.1302081
- Iorio-Morin C, Brisebois S, Becotte A, et al. Improving the pedagogical effectiveness of medical videos. J Vis Commun Med. 2017;40(3):96–100. doi: 10.1080/17453054.2017.1366826
- Young TP, Guptill M, Thomas T, et al. Effective educational videos in emergency medicine. AEM Educ Train. 2018;2(Suppl 1):S17–S24. doi: 10.1002/aet2.10210
- Choe RC, Scuric Z, Eshkol E, et al. Student satisfaction and learning outcomes in asynchronous online lecture videos. CBE Life Sci Educ. 2019;18(4):r55. doi: 10.1187/cbe.18-08-0171
- Raymond M, Iliffe S, Pickett J. Checklists to evaluate an e-learning resource. Educ Prim Care. 2012;23(6):458–459. doi: 10.1080/14739879.2012.11494162
- Corbin JM, Strauss A. Grounded theory research: Procedures, canons, and evaluative criteria. Qual Sociol. 1990;13(1):3–21. doi: 10.1007/BF00988593
- Strauss A, Corbin JM. Grounded theory methodology: an overview. In: Denzin NK, and Lincoln YS, editors. Handbook of qualitative research. Thousand Oaks, USA: Sage Publications; 1994. p. 273–285.
- Strübing J. Grounded Theory. In: Bohnsack R, Flick U, Lüders C, editors. Qualitative Sozialforschung. Wiesbaden: Springer VS; 2014.
- Mayring P. Qualitative content analysis: theoretical foundation, basic procedures and software solution. Klagenfurt, Austria: Klagenfurt; 2014. p. 143.
- Mayring P. Qualitative Inhaltsanalyse: Grundlagen und Techniken. 12th ed. Weinheim, Germany & Basel, Switzerland: Beltz; 2015.
- Chen Y, Yang K, Marušic A, et al. A reporting tool for practice guidelines in health care: the RIGHT statement. Ann Intern Med. 2017;166(2):128–132. doi: 10.7326/M16-1565
- Chen Y, Yang K, Marusic A, et al. RIGHT Explanation and Elaboration: guidance for reporting practice guidelines. 2017.
- Brouwers MC, Kho ME, Browman GP, et al. AGREE II: advancing guideline development, reporting and evaluation in health care. CanMed Assoc J. 2010;182(18):E839–42. doi: 10.1503/cmaj.090449
- Brouwers MC, Kerkvliet K, Spithoff K. The AGREE Reporting Checklist: a tool to improve reporting of clinical practice guidelines. BMJ. 2016;352:i1152. doi: 10.1136/bmj.i1152
- AGREE Next Steps Consortium. The AGREE II Instrument [Electronic version]. 2017.
- Moher D, Liberati A, Tetzlaff J, et al. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. 2009;6(7):e1000097. doi: 10.1371/journal.pmed.1000097
- Tong A, Sainsbury P, Craig J. Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. Int J Qual Health Care. 2007;19(6):349–357. doi: 10.1093/intqhc/mzm042
- Sait S, Tombs M. Teaching medical students how to interpret chest X-Rays: the design and development of an e-Learning Resource. Adv Med Educ Pract. 2021;12:123–132. doi: 10.2147/AMEP.S280941
- Mulcahy RS. Creating effective eLearning to help drive change. ACS Chem Health Saf. 2020;27(6):362–368. doi: 10.1021/acs.chas.0c00091
- Fleming SE, Reynolds J, Wallace B. Lights… camera… action! a guide for creating a DVD/video. Nurse Educ. 2009;34(3):118–121. doi: 10.1097/NNE.0b013e3181a0270e
- Authement RS, Dormire SL. Introduction to the online nursing education best practices guide. Sage Open Nurs. 2020;6:2377960820937290. doi: 10.1177/2377960820937290
- de Leeuw R, Scheele F, Walsh K, et al. A 9-step theory- and evidence-based postgraduate medical digital education development model: empirical development and validation. JMIR Med Educ. 2019;5(2):e13004. doi: 10.2196/13004
- Cross A, Bayyapunedi M, Cutrell E, et al. Combining the benefits of handwriting and typeface in online educational videos. CHI 2013. 2013.
- Wong G, Apthorpe HC, Ruiz K, et al. An innovative educational approach in using instructional videos to teach dental local anaesthetic skills. Eur J Dent Educ. 2019;23(1):28–34. doi: 10.1111/eje.12382
- Maloy J, Fries L, Laski F, et al. Seductive details in the flipped classroom: the impact of interesting but educationally irrelevant information on Student learning and motivation. CBE Life Sci Educ. 2019;18(3):r42. doi: 10.1187/cbe.19-01-0004
- Spreckelsen C, Juenger J. Repeated testing improves achievement in a blended learning approach for risk competence training of medical students: results of a randomized controlled trial. BMC Med Educ. 2017;17(1):177. doi: 10.1186/s12909-017-1016-y
- McCoy L, Lewis JH, Dalton D. Gamification and multimedia for medical education: a landscape review. J Am Osteopath Assoc. 2016;116(1):22–34. doi: 10.7556/jaoa.2016.003
- Adam M, McMahon SA, Prober C, et al. Human-centered design of video-based health education: an iterative, collaborative, community-based approach. J Med Internet Res. 2019;21(1):e12128. doi: 10.2196/12128
- Phelan J. Ten tweaks that can improve your teaching. Am Biol Teach. 2016;78(9):725–732. doi: 10.1525/abt.2016.78.9.725
- Jang HW, Kim KJ. Use of online clinical videos for clinical skills training for medical students: benefits and challenges. BMC Med Educ. 2014;14(1):56. doi: 10.1186/1472-6920-14-56
- Margolis A, Porter A, Pitterle M. Best practices for use of blended learning. Am J Pharm Educ. 2017;81(3):81(3. doi: 10.5688/ajpe81349
- Yavner SD, Pusic MV, Kalet AL, et al. Twelve tips for improving the effectiveness of web-based multimedia instruction for clinical learners. Med Teach. 2015;37(3):239–244. doi: 10.3109/0142159X.2014.933202
- RWTH Aachen University, Zahlenspiegel 2017. 2018.
- Karic B, Moino V, Nolin A, et al. Evaluation of surgical educational videos available for third year medical students. Med Educ Online. 2020;25(1):1714197. doi: 10.1080/10872981.2020.1714197
- Chauvet P, Botchorishvili R, Curinier S, et al. What is a good teaching video? Results of an online international survey. J Minim Invasive Gynecol. 2020;27(3):738–747. doi: 10.1016/j.jmig.2019.05.023
Appendix
Box 1 Search strings used for the initial literature search
Additional Information Regarding the COREQ-Checklist
Research Team and Reflexivity
The first author, a male 4th-year MD student aged 21 years, conducted the interviews. Prior to the interviews, the other author trained him via a supervision dialogue, reflection on the literature, and postprocessing.
All participants were personally known to the interviewer, and at least occasional personal contact between the interviewer and the participants existed independently of this study. The interviewer and the participants were also medical students at the same faculty and, at the very least, were acquainted. The participants knew that the study’s goal was to create a requirement analysis to improve the faculty’s eLearning program for evidence-based medicine (i.e., by implementing educational video).
Interview Guide “Fighting Statistical Illiteracy” – What Form Should Successful Video eLearning Take?
Watch? □ Recorder? □ Writing materials? □
Welcome, gratitude, concern (=> title), consent to recording? Estimated timeframe: 30 minutes. Explaining procedure incl. subjectivity, open-minded; everything may be important!
Your benefit: chance to make an impact on this course; help improve the teaching and learning environment
=> start recording
As a student, you are a member of our target group; therefore, this interview has the sense of customer orientation!
Vision/Warm up:
Appealing & effective eLearning offerings on the topic of fighting statistical illiteracy; here, video-based
‘fighting statistical illiteracy’ particularly means studying comprehension and the correct handling of terms and values => creating the ability to interpret and self-confidently classify studies and results, also with regard to medical risk-communication
But: Not a statistics course (although content may overlap)
Exploration of present situation:
Huge spectrum of knowledge to be acquired with simultaneous danger of bulimia learning.
Nevertheless, evidence-based medicine topics are important for advanced semesters (e.g., research activities, how to write a paper) => our motivation for offering a voluntary evidence-based medicine course
What is your opinion concerning eLearning?
Talking about current eLearning at our institution (key facts): Our institutional eLearning, if any, often consists only of presentations and texts. Only a few videos are available, and they are usually not embedded in the main courses. Generally speaking, there are not many interactions.
=> Does that bother you? Would you like more (comprehensive) eLearning?
Keywords: eLearning in general, effectiveness, convenience, no travel time, …
Exploration of future situation:
What do you expect from successful eLearning? [our goal: crisp and brief, but effective]
Do you consider videos to be advisable for this purpose?
What do you wish for? What are must-haves and nice-to-haves for you? What must not appear?
What videos do you wish for? Let’s talk about animations and Khan style.
What do you think about examples in explanations? How many make it boring; when does it become boring? Do you prefer everyday-life examples or specific (medical) examples?
What do you think about games (like a quiz app for playing against other students) or interactions in general with other course mates in this context? Would you play educational games?
Let’s talk about learning controls, tests, and repeated testing!
What would you prioritize in order to use eLearning effortlessly?
Would you invest 10 to 15 minutes per week in such a course?
Do you think you would learn successfully from such a course?
Let’s talk about motivation. What do you think is more engaging: videos or scripts? Are 2 pages of script too much for one week?
[refer to requirement analysis]
Summary, feedback, gratitude => stop recording! Goodbye, outlook => course offering in summer semester, results of interviews will be available later.
Taking field notes □