
ABSTRACT
Tactile, motor and cognitive capacities decline with age, but little is known about how this relates to braille reading outcomes. This study investigated correlates of braille reading speed among working-age and older adults. Texts were read in two modes (oral/silent) and two media (paper/electronic braille display) by 46 blind adults (age range 23–88) who learned braille between the ages of 4 and 63. Participants completed demographic questionnaires and tests of tactile acuity, fine-motor dexterity and working-memory. A relationship between decreased performance in tactile sensitivity and increased age was observed, but no relationship between increased age and braille reading speed was found. Active tactile acuity, reading frequency and braille learning age were significantly correlated with braille reading speed. No significant difference based on medium was observed, though silent reading was significantly faster than reading aloud. Findings underscore the importance of providing opportunities for older braille learners to secure training and to have frequent opportunities to practice braille between sessions. Findings also challenge the suggestion that increased age alone will impede braille learning. The most significant barrier faced by older braille learners is not their age, but challenges that could instead be addressed through policy and practice changes.
Introduction
Although the prevalence of acquired visual impairment continues to increase, research on braille, adulthood and aging remains minimal (Varma, Vajaranant, & Burkemper, Citation2016). While tactile sensitivity, finger and hand dexterity, and cognitive functions are crucial components of efficient braille reading (Wormsley & D’Andrea, Citation1997), research is needed to understand the physiological and cognitive characteristics of older braille readers, and to explore the potential role of age-related declines on braille reading outcomes (Cryer & Home, Citation2011). This study examined the relationship between tactile, motor and cognitive measures and braille reading performance within a sample of working-age and older adults.
Braille provides access to vital information including personal communication, leisure reading, and professional correspondence (Huebner, Citation1989). The ability to read braille, like print literacy for the sighted, is associated with higher levels of education, income and employment for individuals who are blind (Bell, Citation2010; Martiniello & Wittich, Citation2019; Ryles, Citation1996). Today, braille is read on paper or using electronic displays which instantly convert electronic information into braille (Nadeem, Aziz, Sajjad, Aziz, & Shaikh, Citation2016) and which have slightly higher and more pronounced dots than on paper (Tiresias, Citation2009). The braille code consists of six dots organized in a 3 × 2 matrix. Different combinations of these dots form the letters, numbers and punctuation symbols needed for over 133 languages (UNESCO, Citation2013). Braille can either be represented in uncontracted or contracted form. In uncontracted braille, a one-to-one correspondence exists, where each print letter has a braille equivalent. In contracted braille, common words or frequently occurring groups of letters are represented using shortforms or abbreviations, as a space-saving mechanism (for example, in English contracted braille, the letters “ab” standing alone represent the word “about”).
Braille reading requires tactile sensitivity in the fingertips (Foulke, Citation1982), which has been shown to decline at a rate of approximately 1% per year (Bruns et al., Citation2014; Legge, Madison, Vaughn, Cheong, & Miller, Citation2008; Stevens, Foulke, & Patterson, Citation1996), effectively more than halved between ages 20 and 80. Notably, braille readers maintain higher tactile acuity thresholds in the reading fingers across all ages by 15% compared to age-matched sighted counterparts (Bruns et al., Citation2014; Stevens et al., Citation1996).
Proficient braille reading also requires effective finger and hand coordination, to follow a line of text and to transition between lines (Kusajima, Citation1974). Though braille can be read with one hand, two-handed reading is associated with higher reading speeds, particularly when the hands are used cooperatively (Wright, Wormsley, & Kamei-Hannan, Citation2009). However, declines in fine motor dexterity between those in their early 20s and those in their 80s of up to 35% have been reported (Agnew, Bolla‐Wilson, Kawas, & Bleecker, Citation1988; Tiffin & Asher, Citation1948; Yeudall, Fromm, Reddon, & Stefanyk, Citation1986).
Unlike print reading where multiple words are perceived during a single saccadic pause, braille is read sequentially as the fingers fluidly move to perceive each symbol, potentially placing greater demands on working-memory for less proficient readers (Perea, Jiménez, Martín-Suesta, & Gómez, Citation2015). Conversely, proficient braille readers draw on contextual cues and are able to predict words based on the first two or three symbols to facilitate reading (Wormsley & D’Andrea, Citation1997), contributing to speed increases of 30% or more (Krueger, Citation1982; Legge, Madison, & Mansfield, Citation1999; Mousty & Bertelson, Citation1985; Nolan & Kederis, Citation1969). However, working memory, vital for rapidly recalling text that is read, is shown to decline especially after age 60 (Nyberg, Lövdén, Riklund, Lindenberger, & Bäckman, Citation2012).
Despite knowledge of these age-related changes, little is known about the extent to which these measures correlate with braille reading outcomes as individuals age. A recent scoping review revealed that research in this domain is sparse and highly inconsistent (Martiniello & Wittich, Citation2020). More than 60% of the reviewed studies examined braille reading performance in relation to only one physiological or cognitive domain, potentially overlooking the effects of confounding variables. Additionally, the use of a variety of often novel measures of tactile, motor, and cognitive functioning calls into question the validity, reliability, and comparability of the assessments. No previous studies have directly explored the relationship between fine-motor or working-memory declines and braille reading outcomes. However, Mousty and Bertelson (Citation1985) reported that readers who benefit most from two-handed reading are those whose slower hand is not significantly inferior to the faster hand, suggesting that when both hands are utilized, a cooperative element is in play. Finally, the existing literature focuses on children, with fewer than one-third of prior studies including any participants over the age of 60 (Martiniello & Wittich, Citation2020).
In adult braille rehabilitation, at least two categories of clients are encountered: those with congenital visual impairments who learned braille early in life but who seek rehabilitation for changing needs as they age, and those who experience vision loss later in life and who require braille training to regain independence (Ponchillia & Ponchillia, Citation1996). Understanding the characteristics of proficient adult braille readers would aid in supporting the unique needs of older braille learners (Cryer & Home, Citation2011). This study therefore explored the relationship between tactile, motor and cognitive capacities and braille reading performance within a single sample of braille readers, with attention devoted to the role of age within this context. The research questions were as follows:
What is the correlation between chronological age and tactile, motor, and cognitive capacities among working-age and older adult braille readers?
What variables correlate strongly with braille reading speed?
What is the influence of reading media (paper vs. braille display) and reading mode (oral vs. silent reading) on braille reading speed?
Materials and methods
Eligibility and recruitment
Data were collected between May 2019 and January 2020. The protocol received ethical approval from the Center for Interdisciplinary Research in Rehabilitation of Greater-Montreal (CRIR #1326-0418), and Vision Loss Rehabilitation Canada. Participants were required to be at least 18 years of age, self-identify as meeting the legal definition of blindness (a visual acuity of 20/200 with best correction in the better eye or a visual field of less than 20 degrees: see Corn & Lusk, Citation2010), and have completed English or French braille training at least one year prior to study participation. Participants were also asked to describe their level of vision, in line with the definitions outlined by the World Health Organization (Citation1993). The invitation to participate was circulated to rehabilitation centers and blindness consumer agencies across Canada, on social media platforms geared toward blind Canadians, and through snowball sampling (Goodman, Citation1961).
Materials and procedure
In all cases, consent forms, study instructions and reading passages were provided in either English or French depending on the language of participants. Informed written or audio-recorded verbal consent was obtained in accordance with the Declaration of Helsinki and Public Health (World Medical Association,Citation2013) prior to their inclusion in the study. The battery of tests, summarized in , were presented in a randomized order, except for the cognitive screening test, which was administered first to minimize the potential influence of cognitive fatigue (Ackerman & Kanfer, Citation2009). Participants had the option of completing all tests at their home or at an approved research site, either within a single session of two hours or over two one-hour sessions.
Table 1. Assessments included in this study.
Mild Cognitive Impairment (MCI) screening
Participants were assessed for mild cognitive impairment using the Montreal Cognitive Assessment, adapted for use with blind participants (Wittich, Phillips, Nasreddine, & Chertkow, Citation2010). In this verbal performance-based assessment, participants were asked a short series of questions to assess factors deemed relevant to reading, including their memory, attention, logical reasoning, language, abstract thought, and orientation. A score of 18 or higher of 22 is considered a “pass,” with lower score indicating a possible risk for a mild cognitive impairment.
Handedness
The Edinburgh Handedness Inventory (EHI) is a short verbal questionnaire to quickly ascertain an individual’s handedness (Oldfield, Citation1971). A mathematical formula provides a handedness score (negative = left bias, positive = right bias). While the preferred braille reading hand is not determined by handedness and there is considerable evidence that handedness has no influence on braille reading speed (Bradshaw, Nettleton, & Speir, Citation1982; Fertsch, Citation1947; Foulke, Citation1964; Legge et al., Citation1999; Millar, Citation1984; Sampaio & Philip, Citation1995; Wilkinson & Carr, Citation1987), this information determined the “dominant” hand to be used for the Purdue Pegboard Test.
Fine-motor dexterity
The Purdue Pegboard Test is a measure of hand and finger dexterity and coordination (Buddenberg & Davis, Citation2000; Tiffin & Asher, Citation1948). A participant’s score was determined as the number of metal pegs successfully placed in 30 seconds into vertical rows of holes in a board placed before the participant. The task was repeated three times (and averaged), first with their dominant hand (as determined by the EHI score), then with the non-dominant hand, and then with both hands together. Very limited data are available to establish “norms” for blind participants assessed with the Purdue Pegboard, and comparisons to what has been reported are problematic because of differences in methodology and reporting (Wittich & Nadon, Citation2015). However, Tobin and Greenhalgh (Citation1987) reported mean scores (averaged across men and women) for the right/left/hands together of 8.23/7.53/6.71.
Tactile working-memory
Participants completed a tactile working-memory test developed by Papagno et al. (Citation2017). This working-memory assessment was utilized because performance was independent of braille competency, unlike previous measures such as “reading span” (Daneman, Citation1988). Participants first tactually explored (with their preferred braille reading hand) checkerboard matrix patterns of squares, half of which were smooth and half rough, and then re-constructed the pattern from memory. Patterns grew larger until a participant was unable to complete at least two out of three patterns successfully. A “tactile span” score was calculated as the average number of rough blocks in the three largest patterns successfully reconstructed (range 0–15).
Tactile acuity
Four measures of tactile acuity were obtained, two passive (Two-Point Discrimination Test and Grating Orientation Task) and two active (Legge “Dot” and “C” Tactile Acuity Charts), each yielding a tactile acuity threshold (in mm) representing the smallest separation between two stimuli that a participant was able to reliably detect. Consistent with prior studies, testing was performed on the index finger of the preferred braille reading hand (Bruns et al., Citation2014; Legge et al., Citation2008; Stevens et al., Citation1996).
Two-point discrimination
The Two-Point Discrimination Test measures the minimum distance at which two points of a caliper can be discerned on the skin (Weber, Citation1996). In each trial, using the Touch-Test Discriminator® (Fabricated Enterprises Inc., White Plains, NY), two small (<0.5 mm) rounded points were briefly applied to the distal pad of the stationary index finger with a defined separation (ranging from 2 to 7 mm). Based on prior studies, 64 presentations were administered in a pseudorandomized sequence: 8 at each of the defined gap sizes, and 8 control “single point” presentations (Bruns et al., Citation2014; Dinse et al., Citation2006). Correct and incorrect results were plotted and a logistic regression line fitted to ascertain the midpoint, defined as the threshold at which results surpassed chance.
Grating Orientation Task (GOT)
The GOT utilizes a set of small, plastic grating domes (JVP Domes, Stoetling Co.) with equidistant groove and ridge widths to measure the minimum grating width at which a participant can discern the orientation of the stimulus (Remblay, Backman, Cuenco, Vant, & Wassef, Citation2000; Van Boven & Johnson, Citation1994). The domes were placed on the pad of the immobile index finger in one of two orientations (laterally or longitudinally) for 1 second and participants verbally reported the perceived orientation (Bleyenheuft & Thonnard, Citation2007; Bruns et al., Citation2014; Van Boven & Johnson, Citation1994). At each groove width, 20 trials were presented, half in each orientation based on pseudorandomized sequences counterbalanced across participants. The smallest grating widths whose orientations were reliably reported (75% correct) represent a threshold estimate of the spatial resolution.
Legge “dot” and “C” charts
Two charts which measure active tactile acuity, which more closely resembles the braille reading process than static measurements, were administered (Bruns et al., Citation2014; Legge et al., Citation2008; Oshima, Arai, Ichihara, & Nakano, Citation2014). The images used to produce the tactile charts were constructed using a custom software tool (Tibbs, Citation2018), printed onto heat-sensitive Swell Touch Paper (American Thermoform: La Verne, CA), and fused with a PIAF Picture in a Flash Tactile Graphic Maker (Piaf Tactile: Poznan, Poland). Participants read the charts at their own pace and reported the braille letters read or the position of the gap in the letter “C,” as appropriate. The tactile acuity threshold was calculated in logMAR units as the minimum size attainable on each chart plus 0.0125 logMAR for each incorrect response. The final scores were converted to millimeters (mm = 2.28 x 10logMAR) for comparison with other measures.
Reading assessments
Participants read four passages from the International Reading Speed Test (IReST) (Hahn et al., Citation2006), a standardized multilingual, validated reading assessment utilizing paragraphs of approximately 132 words of encyclopedic text (Morrice, Hughes, Wittich, & Johnson, Citation2018; Trauzettel-Klosinski & Dietz, Citation2012): two in hard copy braille (one read aloud, one silently) and two on an electronic braille display (one read aloud, one silently). As described in the online supplemental materials, these passages have similar word-length characteristics as those used in prior braille reading assessments, such as the MNREAD (Legge et al., Citation1999). The paper reading samples were produced using a Juliet Classic embosser (Enabling Technologies Inc., Jensen Beach, Florida, USA), and a BrailleNote Touch Plus 32 (Humanware Technologies, Drummondville, QC, Canada) was utilized for presenting the electronic braille. Given that the IReST is a multilingual standardized reading measure, passages were available in either English or French depending on the language of participants, and in both uncontracted and contracted braille, depending on their braille reading preference. In all cases, the language (English or French) and braille level (uncontracted or contracted braille) was the same for all four passages that a given participant read.
Participants were asked to read as quickly as possible without stopping to correct errors, and were advised that a multiple-choice comprehension question (included as part of the IReST assessment) would be asked when they completed reading the passage (Morrice et al., Citation2018). However, as described in the Limitations section below, analysis focused on reading speed, given that the average comprehension error rate among participants was very low (<10%). A 3-minute time limit for each passage was imposed to minimize fatigue. Reading rate in characters per minute (cpm) and general information about hand movements during braille reading was noted in accordance with the categorization scheme used by Garcia (Citation2004): one-handed, two-handed (conjoint), two-handed (disjointed), indeterminate/unknown.
Data cleaning
Prior to analysis, the data were cleaned and verified. To remove outliers, all response variables were converted to z-scores. A total of 8 raw data points with an associated |z| > 3 were then replaced with the most extreme raw value from within the “normal range” for that variable (|z| ≤ 3). No response variables were observed to be severely non-normal, demonstrating a skew >3 or a kurtosis >10 (Kline, Citation2011). Nine participants did not complete the full testing protocol, eight of whom were missing one assessment and one of whom was missing two assessments; however, the randomized order of the evaluations minimized any clustering effects with respect to this missing data.
Results
Demographics
Overall, 46 participants between the ages of 23 and 88 (M= 52.3, SD = 14.9) from British Columbia (n = 13), Ontario (n = 8), and Québec (n = 23) participated, including 31 women (67.4%) and 15 men (32.6%). In total, 80.4% (n = 37) participants were English-speaking and 19.6% (n = 9) were French-speaking. On the Montreal Cognitive Assessment, scores ranged between 15 and 22 (M= 19.83, SD = 1.91). summarizes demographic characteristics.
Table 2. Demographic characteristics of participants.
Characteristics of visual diagnoses
Most participants (n= 36) self-reported a congenital visual impairment at birth (age of onset of blindness: range 0–23, M = 2.6, SD = 5.8). Based on the WHO definitions, the vast majority (n = 44, 95.6%) self-reported a profound visual impairment (<20/400 acuity), while one participant (2.2%) reported a severe loss (<20/200 but >20/400) and one (2.2%) had only a moderate loss (<20/70 but >20/200). The most common causes of blindness included retinitis pigmentosa (n = 14, 30.4%), glaucoma (n = 9, 19.6%), retinitis of prematurity (n = 9, 19.6%), and cataracts (n = 7, 15.2%).
Braille learning and usage
outlines the braille history and reading frequency for participants and indicates the language and braille code used. Thirty participants learned braille before the age of 12 (range 4–63, M = 11.75, SD = 9.46). Approximately 78% of participants reported using braille at least weekly. provides an overview of the tasks for which braille is used. Reading speeds were highly variable between subjects, ranging from 34 cpm to 600 cpm (approximately 6.4 words per minute (wpm) to 113 wpm), with an average of 245.31 cpm (SD = 157.85 cpm), or approximately 46.2wpm (SD = 29.8 wpm). As the configuration of the braille alphabet is the same in both English and French, no statistically significant differences based on language were predicted or observed between English and French speaking participants.
Table 3. Braille learning and reading characteristics of participants.
Figure 1. Percentage of participants who utilize braille for the indicated activities in their daily living.
Correlation between age and tactile, motor, and cognitive capacities
The means, standard deviations, and Pearson correlations among the measured variables were computed (summarized in ).
Table 4. Descriptive statistics and correlations among measure variables.
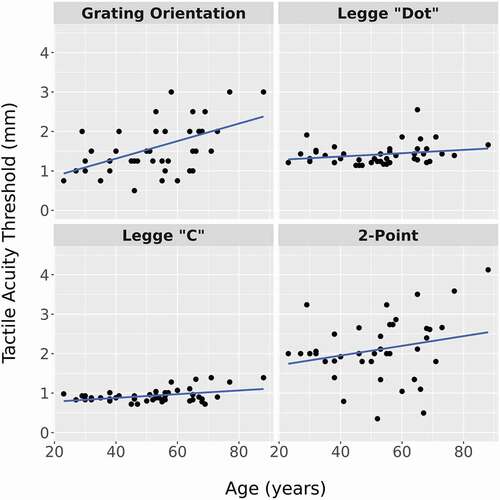
This revealed an apparent trend toward decreased performance on all measures with increasing age. Consistent with prior research (Legge et al., Citation2008; Stevens et al., Citation1996), as shown in , acuity thresholds on the four tactile acuity measures (GOT, 2-Point Discrimination, Legge “Dot” Chart, and Legge “C” Chart) rose with age, although only the correlations for GOT (r= .532, p < .001) and Legge “C” Chart (r= .417, p = .004) were statistically significant.
Figure 2. Tactile acuity thresholds for each participant (by age) for each of the four acuity measures.
Correlates of braille reading speed
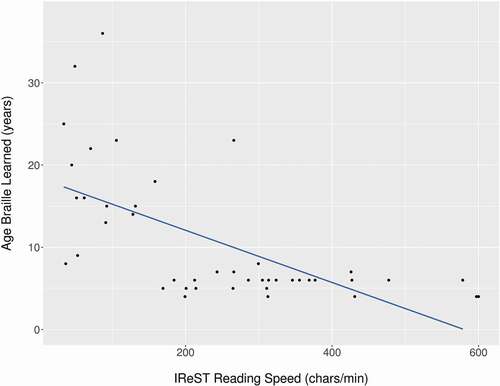
Based on Pearson correlations, active tactile acuity as measured using the Legge “Dot” (r= −.349, p = .022) and Legge “C” (r= −.307, p = .045) Charts and frequency of braille usage (r= .424, p = .005) emerged as significant correlates of braille reading speed. Frequency of braille usage was strongly correlated with reading speed irrespective of when braille was learned (before age 12: r = .421, p= .023; after age 12: r= .382, p= .041). However, the most significant association with reading speed, as demonstrated in , was the age at which braille was learned (r = −.623, p< .001).
Figure 3. Depiction of the relationship between IReST reading speed (characters per minute) and the age at which braille was first learned (years).
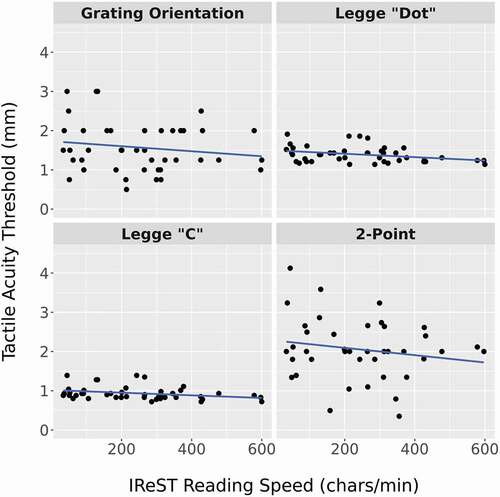
As shown in , for each of the four measures of tactile acuity, decreased acuity (i.e. an increased tactile sensitivity threshold) was associated with declines in braille reading speed. These correlations were statistically significant for the Legge “Dot” Chart (r = −.349, p = .022) and Legge “C” Charts (r= −.307, p = .045), but not for the GOT or 2-Point Discrimination Test.
Figure 4. Depiction of the relationship between each of the tactile acuity measures and IReST reading speed (characters per minute).
To determine whether these correlates explained unique variation in braille reading speed, a multiple linear regression was conducted. For this analysis, all identified significant correlates were entered (age braille was learned, frequency of braille usage, and the Legge tactile acuity) simultaneously. As Legge “Dot” and Legge “C” measure the same underlying construct and a high correlation among them was observed (r= .619, p< .001), only Legge “Dot” (which had the highest r value) was retained for this analysis. The results revealed that the overall model was significant: F(3, 41) = 9.589, p < .001, adj. R2 = .369. Further, as shown in , each of (1) the age at which braille was learned, (2) frequency of braille use, and (3) Legge “Dot” tactile acuity were significant predictors in the model.
Table 5. Multiple linear regression results for correlated factors on reading speed.
Influence of mode and medium
presents descriptive statistics regarding speed for reading on paper and for reading on a braille display in both aloud and silent modes. Each participant underwent all four conditions (paper-aloud, paper-silent, display-aloud, display-silent). To examine mean differences in reading speed between conditions while accounting for dependency in the data, a 2 (medium) x 2 (mode) repeated measures ANOVA was conducted. The ANOVA revealed no significant main effect of medium on reading speed: F(1,42) = 1.683, p > .05, ηp2 = .039. Participants performed similarly whether they were reading on paper (M= 249.43cpm, SD = 164.31cpm) or on a display (M= 241.19cpm, SD = 157.71cpm). There was, however, a significant effect of mode on reading speed (F(1,42) = 27.10, p < .001, ηp2 = .392), with participants reading more quickly in the silent mode (M= 262.21cpm, SD = 175.09cpm) than in the aloud mode (M = 228.41cpm, SD = 143.77cpm).
Table 6. Descriptive statistics for reading speed by medium and mode.
To assess the impact of potential covariates on these mean differences, a series of sequential 2 (medium) x 2 (mode) ANCOVAs controlling for each potential covariate were conducted, revealing significant effects of the age at which braille was learned and the Purdue bimanual score. More specifically, separate two-way ANCOVAs revealed a significant effect of Purdue “both hands” (F(1,39) = 4.773, p = .035, ηp2 = .109) and the age braille was learned (F(1,41) = 6.716, p = .013, ηp2 = .141) on the impact that mode had on reading speed. To explore these effects further, participants were divided into four groups on two dimensions: whether they learned braille early or late (divided based on the mean age of braille learning: 11.61); and whether they were in the stronger or poorer group for the Purdue Pegboard Test (mean Purdue score for both hands: 4.44), and a 2 × 2 within ANOVA predicting speed by mode and medium separately for each group was performed. These results revealed that reading silently was faster than aloud, a difference that was more pronounced in those that learned earlier (ηp2 = .490) versus later (ηp2 = .381). The silent advantage was likewise more pronounced in those with high Purdue (Both) scores (ηp2 = .472) versus those with low scores (ηp2 = .342).
Discussion
Given that physiological and cognitive capacities are known to decline with age, previous researchers have questioned whether assessments for these measures could be used to estimate braille reading ability in aging braille readers or as remedial activities for older learners of braille (Cryer & Home, Citation2011). As expected, a steady, linear decline in tactile acuity and fine-motor dexterity with increasing age was observed, though only the tactile sensitivity measures were associated with significant age-related declines. Tactile working memory only marginally decreased with increasing age. This is consistent with research on working-memory in the sighted, where longitudinal evidence indicates that significant declines are unlikely to be observed until after age 60 (Nyberg et al., Citation2012).
Only the age at which braille was learned, frequency of braille usage, and active tactile acuity emerged as significant correlates of braille reading speed. Consistent with previous findings (see, among others, Davidson, Appelle, & Haber, Citation1992; Fertsch, Citation1947; Garcia, Citation2004; Wright et al., Citation2009), advanced two-handed reading correlated with greater braille reading speed. Silent reading was associated with greater braille reading rates than reading aloud. Finally, no differences in speed between reading on paper and reading on a braille display were observed.
Although previous studies have explored tactile, motor and cognitive capacities in isolation (Daneman, Citation1988; Holland, Citation1934; Loomis, Citation1985; Stevens et al., Citation1996), this is the first study to explore these measures within a single sample of working-age and older adult braille readers. This is noteworthy given that declines in one age-related capacity could inadvertently effect performance in another (Heller & Gentaz, Citation2013). For example, a significant negative correlation between tactile sensitivity and fine-motor dexterity has been reported in numerous studies (Murata et al., Citation2010). Tremblay, Wong, Sanderson, and Coté (Citation2003) measured tactile spatial acuity (using the GOT) and fine-motor dexterity (using the Purdue Pegboard Test) in 30 elderly participants between the ages of 60 and 95, and found that impaired tactile spatial acuity at the fingertips was strongly correlated with hand dysfunction in older adults. This close relationship between tactile perception and hand movements is especially relevant to braille reading, where ineffective hand reading patterns can affect tactile perception and vice versa (Wormsley, Citation1981). In our sample, moderate negative correlations between active tactile acuity measures and fine-motor dexterity were observed, in that particitants with greater active tactile acuity were more likely to achieve higher scores on the Purdue Pegboard Test. Only tactile acuity was ultimately found to be related to braille reading speed; however, the association between motor function and tactile acuity should serve as a reminder that because of potential confounding variables, clinical decision-making must be based on a comprehensive global evaluation without unduly relying on the outcome of a single assessment. While it may seem appealing to some to seek a single “test” to foresee braille reading potential in older learners, possible overlapping relationships between these underlying capacities highlight the limitations in doing so (Martiniello, Haririsanati, & Wittich, Citation2020). While specific correlates emerge as especially important, these findings reinforce the multifaceted nature of reading potential.
Relationship between age and capacities
Consistent with previous research (Murman, Citation2015), age was associated with declines in tactile, motor and cognitive ability. Importantly, however, these findings suggest that getting older on its own should not negatively affect braille reading. In this sample, chronological age did not correlate with braille reading speed. Four previous studies explored the relationship between the age of participants and braille reading speed (Bola et al., Citation2016; Daneman, Citation1988; Legge et al., Citation2008; Olson, Harlow, & Williams, Citation1975). However, these investigations resulted in inconsistent findings and not all studies provided ample information about the age distribution of participants. Among those that did, only one (Legge et al., Citation2008) included participants above the age of 60. The present study adds to this body of work, with 46 participants ranging between the ages of 23 and 88, 30% of whom fall above the age of 60. Notably, our study replicates the findings of Legge (Legge et al., Citation2008), who also included participants above the age of 60 and did not observe a relationship between age and braille reading speed.
These findings suggest that, as experienced braille readers age, they do not exhibit significant changes in their braille reading speed due to age alone. This is somewhat inconsistent with research on print reading and aging. The average print reading rate as measured by the IReST is 228 words per minute for healthy sighted adults between the ages of 18–35, though this is reduced by a factor of 19% (185 wpm) for those within the 65–80 age range (Hahn et al., Citation2006). Research illustrates that tactile ability is highly experience-dependent (Goldreich & Kanics, Citation2003; Wong, Peters, & Goldreich, Citation2013). As will be discussed further below, this study suggests that the accumulated tactile experience of participants may play a significant role in both enhancing and maintaining braille reading skills as individuals age.
Correlates of braille reading speed
Among the examined variables, the age at which braille was learned, frequency of braille usage, and active tactile acuity emerged as the only significant correlates of braille reading speed. Similarly, and consistent with previous findings (see, among others, Davidson et al., Citation1992; Fertsch, Citation1947; Garcia, Citation2004; Wright et al., Citation2009), two-handed reading was associated with greater reading speed, with the advanced two-handed technique correlating with the highest reading rates. These findings heighten the importance of having ample opportunities to enhance tactile sensitivity and proper hand reading patterns both between sessions and once formal instruction concludes, especially for those who learn braille later in life. This places an emphasis on developing proper hand movement techniques among older braille learners, rather than focusing on fine-motor declines which do not appear to influence reading outcomes within this sample.
Despite the correlation between active tactile acuity and reading speed, it is worth noting that this correlation was not found in a prior study using the Legge Dot Chart (Legge et al., Citation2008). However, the braille readers in Legge and colleagues (Citation2008) had marginally lower tactile acuity thresholds (by 0.07 logMAR or .18 mm) and were significantly faster readers, achieving average speeds of 109.5 wpm compared to 46.2wpm in the present study. Moreover, the range of tactile acuity scores in the present study is greater and includes one participant whose acuity was above the standard braille size of 2.28 mm, whereas the worst tactile acuity observed in Legge among blind participants was approximately 1.5 mm (see Figures A3 and A5 in Legge et al., Citation2008). As Legge et al. (Citation2008) and Millar (Citation2003) have argued, if acuity is below the braille spacing of 2.28 mm, reading speed may become independent of acuity and mediated by other factors, just as with sighted readers (Legge, Citation2007, chap. 3). Consequently, it may be that, for our comparatively slower readers with comparatively poorer acuity measures, differences in tactile acuity had a more pronounced effect on reading performance.
Although researchers have explored the correlation between passive and active tactile acuity and braille reading outcomes separately (Bola et al., Citation2016; Legge et al., Citation2008; Nolan & Morris, Citation1965; Stevens et al., Citation1996), this is the first study that explores the contribution of both measures within a single sample. These findings confirm that while passive tactile acuity tests may be reliable measures of static tactile acuity (Bruns et al., Citation2014), these passive measures are not representative of the dynamic process of braille reading. While readers may exhibit low thresholds on a passive tactile acuity test, they may nonetheless struggle with braille reading if they lack proper haptic movements. From a clinical perspective, the use of a measure such as the Legge “Dot” Chart may be helpful as a diagnostic tool to detect potentially undiagnosed neuropathy or tactile acuity limitations. However, as tactile acuities have been shown to improve with practice (Wong et al., Citation2013), and even those with comparatively poorer acuities have demonstrated the ability to read (Bernbaum, Albert, & McGarry, Citation1989), a reasonable time for familiarization with braille reading must be afforded. We thus underscore that these evaluations should not be used as a definitive screening tool to determine eligibility for braille instruction, but rather that an emphasis in enhancing active tactile acuity through practice should be provided.
The significance of frequency of braille usage in this study cannot be over-emphasized. Frequency of braille usage is a vital correlate of braille reading outcomes, irrespective of the age at which braille was learned. Participants who learned braille at an older age but who use braille frequently in their daily lives demonstrated greater braille reading performance than those who learn braille at the same age but who use it less frequently. On the surface, this finding is logical. Active tactile perception, also a significant correlate of braille reading speed, is shown to improve with intensive practice (Wong et al., Citation2013). While it is true that reading frequency is associated with greater educational achievement among the sighted (National Center for Education Statistics, Citation2013), print readers have far greater opportunities to encounter visual reading in the environment. Practitioners have long emphasized the importance of maintaining braille literacy rich environments for blind children, as important determinants of reading achievement (Wormsley & D’Andrea, Citation1997). This study underscores that these consistent opportunities to use braille are equally vital for adults, and that it is frequency of braille usage, and not simply age, that influences braille reading outcomes. This is noteworthy given that referral rates for braille instruction in adulthood remain low (Bernbaum et al., Citation1989; Harley, Pichert, & Morrison, Citation1985), due in part to beliefs held by some clinicians that older clients will be unable to learn braille (Martiniello et al., Citation2020). It thus becomes imperative to ensure that adult braille programs incorporate supports to supplement the training provided during sessions.
Differences based on mode and medium
Consistent with prior research (Chen, Liang, Lu, Potměšil, & Zhong, Citation2019; Fertsch, Citation1946; Knowlton & Wetzel, Citation1996; Laroche, Boulé, & Wittich, Citation2012; Wetzel & Knowlton, Citation2000), a clear and statistically significant difference was found between oral and silent reading, with silent reading being approximately 15% faster. Silent reading has also been correlated with greater reading speeds among the sighted (Van den Boer, van Bergen, & de Jong, Citation2014). Fertsch (Citation1946) hypothesized that the slower reading rates are a consequence of readers feeling self-conscious about mispronouncing a word that, when reading silently, they might predict through context. It has also been suggested that the time and cognitive effort required to decode and work out not only the meaning but also the pronunciation of each word leads to a slowing of reading speed (Chen et al., Citation2019; Van den Boer et al., Citation2014). These findings reinforce the importance of considering both reading task and reading mode when assessing older clients. While performance when reading aloud may be markedly poorer than when reading silently, careful attention should be paid to how braille will be used in daily life when assessing client progress.
The age at which braille was learned and bimanual Purdue performance emerged as especially significant to silent reading speeds. This distinction is likely due to the greater cognitive load associated with reading aloud and the inherent multitasking of such a task, rather than as a direct consequence of the difference in fine motor performance. Proud and Morris (Citation2010), for example, have previously demonstrated decreased performance on the Purdue Pegboard when participants are simultaneously tasked with a verbal serial-7 subtraction exercise.
Finally, no differences in reading speed were observed when comparing reading on paper (M= 249.43cpm, SD = 164.31cpm) and on a braille display (M = 241.19cpm, SD = 157.71cpm). Most participants were already experienced braille readers, and the overwhelming majority (95%) had active tactile acuity scores (on the Legge “Dot” Chart) below the 2.28 mm threshold required for braille reading. It is possible, as suggested by Douglas et al. (Citation2009), that the increased dot height of a display (.63 mm-.8 mm for display (Tiresias, Citation2009) and .46 mm-.48 mm for paper braille (Douglas et al., Citation2009; Gardner, Citation2005; Tiresias, Citation2009)) may be especially beneficial for novice braille learners or for those with reduced tactile sensitivity due to age. In a study focusing on novice braille learners, Martiniello and Wittich (Citation2021) found that, although all participants could learn braille on paper and on braille display, participants with reduced tactile sensitivity achieved greater accuracy and speed on the display condition.
Limitations and future research
This study is the first to explore the role of multiple capacities and age-related factors on the braille reading performance of working-age and older adults; however, several limitations should be noted. First, while we focus on speed, even participants with slower reading rates indicated using braille for functional tasks such as identifying elevator buttons. In this way, reading rate is not the only or best indication of whether a client can successfully use braille to meet their specific needs. While data on reading accuracy were collected, the rate of errors, as a percentage of characters read, was exceptionally low (<0.7%) and thus no meaningful analysis could be conducted. Similarly, the error rate for comprehension questions was less than 10%, and 70% of those errors resulted from a single IReST passage, which at least one author utilizing the IReST in a Canadian sample has previously suggested “reflects the poor quality of content of the question as opposed to participants not understanding the content of the text” (Morrice, Citation2017, p. 21). Future research is needed to explore accuracy and comprehension among older braille learners in greater depth.
Second, while some prior studies have observed distinct categories of reading proficiency (see, for example, in Legge et al., Citation1999), reading speeds were, save for a few of the fastest readers, relatively evenly distributed across the range of observed speeds. As such, dividing the sample to identify differences between “poor” and “good” readers based on mean reading speeds, as has been done in prior studies, was not possible.
Third, this is a cross-sectional study and observed correlations are neither predictive nor evidence of a causal relationship (Bowen & Wiersema, Citation1999). Longitudinal studies that track these measures over time would help to better understand the impact of aging (rather than age) on braille reading outcomes.
Conclusion
This study advances research on braille and aging by clarifying previous work and demonstrating that although tactile, motor and cognitive capacities decline with age, age alone does not correlate with braille reading speed. Instead, a focus should be placed on introducing braille early in vision loss and on providing older braille clients with frequent opportunities to use braille to enhance tactile skills. As the population continues to age, further research is needed to develop programs and policies designed to meet the unique needs of older braille learners, including those with reduced tactile sensitivity.
Declaration of Conflicting Interests
The authors declare that there are no conflicts of interest.
Acknowledgments
The authors would like to thank Humanware for providing the BrailleNote Touch Plus, and Dr Mahadeo Sukhai, Sara Brennan, Charles André-Labbé, Chantal Robillard, Chantal Nicole, Norman Robert Boie, Karine Elalouf, Eleanor Diamond and Emilia Milheiro for their support.
Additional information
Funding
References
- Ackerman, P. L., & Kanfer, R. (2009). Test length and cognitive fatigue: An empirical examination of effects on performance and test-taker reactions. Journal of Experimental Psychology. Applied, 15(2), 163.
- Agnew, J., Bolla‐Wilson, K., Kawas, C. H., & Bleecker, M. L. (1988). Purdue pegboard age and sex norms for people 40 years old and older. Developmental Neuropsychology, 4(1), 29–35. doi:https://doi.org/10.1080/87565648809540388
- Bell, E. C. (2010). Competitive employment for consumers who are legally blind: A 10-year retrospective study. Journal of Rehabilitation Research and Development, 47(2), 109–116. doi:https://doi.org/10.1682/JRRD.2009.08.0120
- Bernbaum, M., Albert, S. G., & McGarry, J. D. (1989). Diabetic neuropathy and braille ability. Archives of Neruology, 46(11), 1179–1181. doi:https://doi.org/10.1001/archneur.1989.00520470033022
- Bleyenheuft, Y., & Thonnard, J.-L. (2007). Tactile spatial resolution measured manually: A validation study. Somatosensory & Motor Research, 24(3), 111–114. doi:https://doi.org/10.1080/08990220701496639
- Bola, L., Siuda-Krzywicka, K., Paplinska, M., Sumera, E., Hanczur, P., & Szwed, M. (2016). Braille in the sighted: Teaching tactile reading to sighted adults. PloS One, 11(5), e0153394.
- Bowen, H. P., & Wiersema, M. F. (1999). Matching method to paradigm in strategy research: Limitations of cross-sectional analysis and some methodological alternatives. Strategic Management Journal, 20(7), 625–636. doi:https://doi.org/10.1002/(SICI)1097-0266(199907)20:7<625::AID-SMJ45>3.0.CO;2-V
- Bradshaw, J. L., Nettleton, N. C., & Speir, K. (1982). Braille reading and left and right hemispace. Neuropsychologia, 20(4), 493–500. doi:https://doi.org/10.1016/0028-3932(82)90048-3
- Bruns, P., Camargo, C. J., Campanella, H., Esteve, J., Dinse, H. R., & Röder, B. (2014). Tactile acuity charts: A reliable measure of spatial acuity. PloS One, 9(2), e87384. doi:https://doi.org/10.1371/journal.pone.0087384
- Buddenberg, L. A., & Davis, C. (2000). Test–retest reliability of the purdue pegboard test. American Journal of Occupational Therapy, 54(5), 555–558. doi:https://doi.org/10.5014/ajot.54.5.555
- Chen, X., Liang, L., Lu, M., Potměšil, M., & Zhong, J. (2019). The effects of reading mode and braille reading patterns on braille reading speed and comprehension: A study of students with visual impairments in China. Research in Developmental Disabilities, 91, 103424. doi:https://doi.org/10.1016/j.ridd.2019.05.003
- Corn, A. L., & Lusk, K. E. (2010). Perspectives on low vision (chapter 1). In Foundations of low vision: Clinical and functional perspectives (pp. 3–34). New York, N.Y.: American Foundation for the Blind
- Cryer, H., & Home, S. (2011). Final report: Feasibility of developing a diagnostic touch test to determine braille reading potential. Birmingham, UK: RNIB Centre for Accessible Information.
- Daneman, M. (1988). How reading braille is both like and unlike reading print. Memory & Cognition, 16(6), 497–504. doi:https://doi.org/10.3758/BF03197051
- Davidson, P. W., Appelle, S., & Haber, R. N. (1992). Haptic scanning of braille cells by low-and high-proficiency blind readers. Research in Developmental Disabilities, 13(2), 99–111. doi:https://doi.org/10.1016/0891-4222(92)90018-2
- Dinse, H. R., Kleibel, N., Kalisch, T., Ragert, P., Wilimzig, C., & Tegenthoff, M. (2006). Tactile coactivation resets age-related decline of human tactile discrimination. Annals of Neurology, 60(1), 88–94. doi:https://doi.org/10.1002/ana.20862
- Douglas, G., Weston, A., Whittaker, J., Wilkins, S. M., & Robinson, D. (2009). An investigation of the height of embossed braille dots for labels on pharmaceutical products. Journal of Visual Impairment & Blindness, 103(10), 662–667. doi:https://doi.org/10.1177/0145482X0910301009
- Fertsch, P. (1946). An analysis of braille reading. Outlook for the Blind and the Teachers Forum, 40, 128–131.
- Fertsch, P. (1947). Hand dominance in reading braille. The American Journal of Psychology, 60(3), 335–349. doi:https://doi.org/10.2307/1416915
- Foulke, E. (1964). Transfer of a complex perceptual skill. Perceptual and Motor Skills, 18(3), 733–740. doi:https://doi.org/10.2466/pms.1964.18.3.733
- Foulke, E. (1982). Reading braille (tactual perception: A sourcebook (pp. 168–208). New York, N.Y.: Cambridge University Press.
- Fuchs, L. S., Fuchs, D., Hosp, M. K., & Jenkins, J. R. (2001). Oral reading fluency as an indicator of reading competence: A theoretical, empirical, and historical analysis. Scientific Studies of Reading, 5(3), 239–256. doi:https://doi.org/10.1207/S1532799XSSR0503_3
- Garcia, L. G. (2004). Assessment of text reading comprehension by Spanish-speaking blind persons. The British Journal of Visual Impairment, 22(1), 4–12. doi:https://doi.org/10.1177/026461960402200102
- Gardner, J. A. (2005). Braille, innovations, and over-specified standards. In Proceedings of GOTHI’05 (guidelines on tactile and haptic interactions) Carter, J. & Fourney, D., Eds. (pp. 26). Saskatoon: USERLab, University of Saskatchewan.
- Goldreich, D., & Kanics, I. M. (2003). Tactile acuity is enhanced in blindness. The Journal of Neuroscience, 23(8), 3439–3445. doi:https://doi.org/10.1523/JNEUROSCI.23-08-03439.2003
- Goodman, L. A. (1961). Snowball sampling. The Annals of Mathematical Statistics, 32(1), 148–170. doi:https://doi.org/10.1214/aoms/1177705148
- Hahn, G., Penka, D., Gehrlich, C., Messias, A., Weismann, M., Hyvärinen, L., … Dauxerre, C. (2006). New standardised texts for assessing reading performance in four European languages. British Journal of Ophthalmology, 90(4), 480–484. doi:https://doi.org/10.1136/bjo.2005.087379
- Harley, R. K., Pichert, J. W., & Morrison, M. (1985). Braille instruction for blind diabetic adults with decreased tactile sensitivity. Journal of Visual Impairment & Blindness, 79(1), 12–17. doi:https://doi.org/10.1177/0145482X8507900103
- Heller, M. A., & Gentaz, E. (2013). Psychology of Touch and Blindness. New York, N.Y.: Psychology Press.
- Holland, B. F. (1934). Speed and pressure factors in braille reading. Journal of Visual Impairment & Blindness, 28(1b), 13–17. doi:https://doi.org/10.1177/0145482x3400700104
- Huebner, K. M. (1989). Daily uses of braille as told by 4 adult braille users. Journal of Visual Impairment & Blindness, 83(6), 308–309. doi:https://doi.org/10.1177/0145482X8908300612
- Juel, C., & Holmes, B. (1981). Oral and silent reading of sentences. Reading Research Quarterly, 16(4), 545–568. doi:https://doi.org/10.2307/747315
- Kline, R. B. (2011). Principles and practice of structured equation modeling. New York, N.Y., USA: Guilford Press.
- Knowlton, M., & Wetzel, R. (1996). Braille reading rates as a function of reading tasks. Journal of Visual Impairment & Blindness, 90(3), 3. doi:https://doi.org/10.1177/0145482X9609000312
- Krueger, L. E. (1982). A word-superiority effect with print and braille characters. Perception & Psychophysics, 31(4), 345–352. doi:https://doi.org/10.3758/BF03202658
- Kusajima, T. (1974). Visual reading and braille reading: An experimental investigation of the physiology and psychology of visual and tactual reading. New York, N.Y., USA: American Foundation of the Blind.
- Laroche, L., Boulé, J., & Wittich, W. (2012). Reading speed of contracted French braille. Journal of Visual Impairment & Blindness, 106(1), 37–42. doi:https://doi.org/10.1177/0145482X1210600105
- Legge, G. E. (2007). Psychophysics of reading in normal and low vision. Boca Raton, FL: CRC Press. doi:https://doi.org/10.1201/9781482269482
- Legge, G. E., Madison, C. M., & Mansfield, J. S. (1999). Measuring braille reading speed with the MNREAD test. Visual Impairment Research, 1(3), 131–145. doi:https://doi.org/10.1076/vimr.1.3.131.4438
- Legge, G. E., Madison, C. M., Vaughn, B. N., Cheong, A. M. Y., & Miller, J. C. (2008). Retention of high tactile acuity throughout the lifespan in blindness. Perception & Psychophysics, 70(8), 1471–1488. doi:https://doi.org/10.3758/PP.70.8.1471
- Loomis, J. M. (1985). Tactile recognition of raised characters: A parametric study. Bulletin of the Psychonomic Society, 23(1), 18–20. doi:https://doi.org/10.3758/BF03329767
- Martiniello, N., & Wittich, W. (2019). Employment and visual impairment: Issues in adulthood. In J. Ravenscraft (Ed.), Routledge handbook of visual impairment (pp. 415–437). London, England: Routledge Taylor & Francis Group.
- Martiniello, N., Haririsanati, L., & Wittich, W. (2020). Enablers and barriers encountered by working-age and older adults who pursue braille training. Disability and Rehabilitation, 1–16. doi:https://doi.org/10.1080/09638288.2020.1833253
- Martiniello, N., & Wittich, W. (2020). The association between tactile, motor and cognitive capacities and braille reading performance: A scoping review of primary evidence to advance research on braille and aging. Disability and Rehabilitation. doi:https://doi.org/10.1080/09638288.2020.1839972
- Martiniello, N., & Wittich, W. (2021). Exploring the influence of reading medium on braille learning outcomes: A case series of 6 working-age and older adults. British Journal of Visual Impairment, 026461962199070. doi:https://doi.org/10.1177/0264619621990702
- Millar, S. (1984). Is there a “best hand” for braille? Cortex, 20(1), 75–87. doi:https://doi.org/10.1016/S0010-9452(84)80025-8
- Millar, S. (2003). Reading by touch. London, Englland: Routledge.
- Morrice, E. (2017). Validation of the international reading speed texts in a Canadian sample. [Master’s Thesis, Concordia University]. https://spectrum.library.concordia.ca/982587/
- Morrice, E., Hughes, J., Wittich, W., & Johnson, A. (2018). Validation of the international reading speed texts in a Canadian sample. Annals of Eye Science, 3(AB104), AB104–AB104. doi:https://doi.org/10.21037/aes.2018.AB104
- Mousty, P., & Bertelson, P. (1985). 1. A study of braille reading: Reading speed as a function of hand usage and context. The Quarterly Journal of Experimental Psychology, 37A(2), 217–233. doi:https://doi.org/10.1080/14640748508400931
- Murata, J., Murata, S., Hiroshige, J., Ohtao, H., Horie, J., & Kai, Y. (2010). The influence of age-related changes in tactile sensibility and muscular strength on hand function in older adult females. International Journal of Gerontology, 4(4), 180–183. doi:https://doi.org/10.1016/j.ijge.2010.11.004
- Murman, D. L. (2015). The impact of age on cognition. Seminars in Hearing, 36(3), 111–121. doi:https://doi.org/10.1055/s-0035-1555115
- Nadeem, M., Aziz, N., Sajjad, U., Aziz, F., & Shaikh, H. (2016). A comparative analysis of Braille generation technologies. In 2016 International Conference on Advanced Robotics and Mechatronics (ICARM) (pp. 294–299). Macau, China: IEEE.
- National Center for Education Statistics. (2013). Average National Assessment of Educational Progress (NAEP) reading scale score and percentage distribution of students, by age, amount of reading for school and for fun, and time spent on homework and watching TV/video: Selected years, 1984 through 2012. NAEP Trends in Academic Progress, 1996 and 1999; and 2008 and 2012 NAEP Long-Term Trend Reading Assessments. Retrieved from https://nces.ed.gov/programs/digest/d19/tables/dt19_221.30.asp
- Nolan, C. Y., & Kederis, J. C. (1969). Perceptual factors in braille word recognition (research series no. 20). New York, N.Y., USA: American Foundation for the Blind.
- Nolan, C. Y., & Morris, J. E. (1965). Development and validation of the roughness discrimination test. The International Journal for the Education of the Blind, 15(1), 1–6.
- Nyberg, L., Lövdén, M., Riklund, K., Lindenberger, U., & Bäckman, L. (2012). Memory aging and brain maintenance. Trends in Cognitive Sciences, 16(5), 292–305. doi:https://doi.org/10.1016/j.tics.2012.04.005
- Oldfield, R. C. (1971). The assessment and analysis of handedness: The Edinburgh inventory. Neuropsychologia, 9(1), 97–113. doi:https://doi.org/10.1016/0028-3932(71)90067-4
- Olson, M., Harlow, S. D., & Williams, J. (1975). Rapid reading in braille and large print: An examination of mcbride’s procedures. Journal of Visual Impairment & Blindness, 69(9), 392–395. doi:https://doi.org/10.1177/0145482x7506900902
- Oshima, K., Arai, T., Ichihara, S., & Nakano, Y. (2014). Tactile sensitivity and braille reading in people with early blindness and late blindness. Journal of Visual Impairment & Blindness, 108(2), 122–131. doi:https://doi.org/10.1177/0145482X1410800204
- Papagno, C., Minniti, G., Mattavelli, G. C., Manatovan, L., & Cecchetto, C. (2017). Tactile short-term memory in sensory-deprived individuals. Experimental Brain Research, 235(2), 471–480. doi:https://doi.org/10.1007/s00221-016-4808-0
- Perea, M., Jiménez, M., Martín-Suesta, M., & Gómez, P. (2015). Letter position coding across modalities: Braille and sighted reading of sentences with jumbled words. Psychonomic Bulletin & Review, 22(2), 531–536. doi:https://doi.org/10.3758/s13423-014-0680-8
- Ponchillia, P. E., & Ponchillia, S. V. (1996). Foundations of rehabilitation teaching with persons who are blind or visually impaired. New York, N.Y., USA: American Foundation for the Blind.
- Proud, E. L., & Morris, M. E. (2010). Skilled hand dexterity in Parkinson’s disease: Effects of adding a concurrent task. Archives of Physical Medicine and Rehabilitation, 91(5), 794–799. doi:https://doi.org/10.1016/j.apmr.2010.01.008
- Ramalu, P. Y., Swenor, B. K., Jefferys, J. L., & Rubin, G. S. (2013). Description and validation of a test to evaluate sustained silent reading. Invetigative Ophthalmology & VIsual Science, 54(1), 673–680. doi:https://doi.org/10.1167/iovs.12-10617
- Remblay, F., Backman, A., Cuenco, A., Vant, K., & Wassef, M. A. (2000). Assessment of spatial acuity at the fingertip with grating (JVP) domes: Validity for use in an elderly population. Somatosensory & Motor Research, 17(1), 61–66. doi:https://doi.org/10.1080/08990220070300
- Ryles, R. (1996). The impact of braille reading skills on employment, income, education, and reading habits. Journal of Visual Impairment & Blindness, 90(3), 219–226. doi:https://doi.org/10.1177/0145482X9609000311
- Sampaio, E., & Philip, J. (1995). Influences of age at onset of blindness on braille reading performances with left and right hands. Perceptual and Motor Skills, 81(1), 131–141. doi:https://doi.org/10.2466/pms.1995.81.1.131
- Stevens, J. C., Foulke, E., & Patterson, M. Q. (1996). Tactile acuity, aging, and braille reading in long-term blindness. Journal of Experimental Psychology. Applied, 2(2), 91–106. doi:https://doi.org/10.1037/1076-898X.2.2.91
- Tibbs, A. (2018). Tactile Acuity Chart Generators. [Source code]. https://github.com/tibbsa/tac
- Tiffin, J., & Asher, E. J. (1948). The Purdue Pegboard: Norms and studies of reliability and validity. Journal of Applied Psychology, 32(3), 234–247. doi:https://doi.org/10.1037/h0061266
- Tiresias. (2009). Braille cell dimensions. Retrieved October 19, 2020 from http://www.arch.mcgill.ca/prof/klopp/arch678/fall2008/3%20Student%20exchange/Team%20Surface/Connexion%20Surface%20Folder/MA%20files/Braille%20cell%20dimensions.pdf
- Tobin, M., & Greenhalgh, R. (1987). Normative data for assessing the manual dexterity of visually handicapped adults in vocational rehabilitation. Journal of Occupational Psychology, 60(1), 73–80. doi:https://doi.org/10.1111/j.2044-8325.1987.tb00242.x
- Trauzettel-Klosinski, S., & Dietz, K. (2012). Standardized assessment of reading performance: The New International Reading Speed Texts IReST. Investigative Ophthalmology & Visual Science, 53(9), 5452–5461. doi:https://doi.org/10.1167/iovs.11-8284
- Tremblay, F., Wong, K., Sanderson, R., & Coté, L. (2003). Tactile spatial acuity in elderly persons: Assessment with grating domes and relationship with manual dexterity. Somatosensory & Motor Research, 20(2), 127–132. doi:https://doi.org/10.1080/0899022031000105154
- UNESCO. (2013). World braille usage. Paris, France; Washington, DC: Perkins, the International Council on English Braille, and the National Library Service for the Blind and Physically Handicapped.
- Van Boven, R. W., & Johnson, K. O. (1994). The limit of tactile spatial resolution in humans: Grating orientation discrimination at the lip, tongue, and finger. Neurology, 44(12), 2361. doi:https://doi.org/10.1212/WNL.44.12.2361
- Van den Boer, M., van Bergen, E., & de Jong, P. F. (2014). Underlying skills of oral and silent reading. Journal of Experimental Child Psychology, 128, 138–151. doi:https://doi.org/10.1016/j.jecp.2014.07.008
- Varma, R., Vajaranant, T., & Burkemper, B. (2016). Visual impairment and blindness in adults in the United States: Demographic and geographic variations from 2015 to 2050. Journal of the American Medical Association: Opthalmology, 134(7), 802–809.
- Weber, E. H. (1996). E. H. Weber on the tactile senses (2nd ed.). Erlbaum (Uk): Taylor & Francis, Publ.
- Wetzel, R., & Knowlton, M. (2000). A comparison of print and braille reading rates on three reading tasks. Journal of Visual Impairment & Blindness, 94(3), 146–154. doi:https://doi.org/10.1177/0145482X0009400303
- Wilkinson, J. M., & Carr, T. H. (1987). Strategic hand use preferences and hemispheric specialization in tactual reading: Impact of the demands of perceptual encoding. Brain and Language, 32(1), 97–123. doi:https://doi.org/10.1016/0093-934X(87)90119-2
- Wittich, W., & Nadon, C. (2015). The Purdue Pegboard test: Normative data for older adults with low vision. Disability and Rehabilitation. Assistive Technology, 12(3), 272–279.
- Wittich, W., Phillips, N., Nasreddine, Z. S., & Chertkow, H. (2010). Sensitivity and specificity of the Montreal cognitive assessment modified for individuals who are visually impaired. Journal of Visual Impairment & Blindness, 104(6), 360. doi:https://doi.org/10.1177/0145482X1010400606
- Wong, M., Peters, R. M., & Goldreich, D. (2013). A physical constraint on perceptual learning: Tactile spatial acuity improves with training to a limit set by finger size. Journal of Neuroscience, 33(22), 9345–9352. doi:https://doi.org/10.1523/JNEUROSCI.0514-13.2013
- World Health Organization. (1993). The ICD-10 classification of mental and behavioural disorders: Diagnostic criteria for research (Vol. 2). Geneva, Switzerland; Author.
- World Medical Association (2013). Declaration of Helsinki: Ethical principles for medical research involving human subjects. Journal of the American Medical Association, 310(20), 2191–2194. doi:https://doi.org/10.1001/jama.2013.281053
- Wormsley, D. P. (1981). Hand movement training in Braille reading. Journal of Visual Impairment & Blindness, 75(8), 327–331. doi:https://doi.org/10.1177/0145482X8107500804
- Wormsley, D. P., & D’Andrea, F. M. (1997). Instructional strategies for braille literacy. New York, N.Y., USA: American Foundation for the Blind.
- Wright, T., Wormsley, D. P., & Kamei-Hannan, C. (2009). Hand movements and braille reading efficiency: Data from the alphabetic Braille and contracted Braille study. Journal of Visual Impairment & Blindness, 103(10), 649–661. doi:https://doi.org/10.1177/0145482X0910301008
- Yeudall, L. T., Fromm, D., Reddon, J. R., & Stefanyk, W. O. (1986). Normative data stratified by age and sex for 12 neuropsychological tests. Journal of Clinical Psychology, 42(6), 918–946. doi:https://doi.org/10.1002/1097-4679(198611)42:6<918::AID-JCLP2270420617>3.0.CO;2-Y