
Abstract
Objectives
Prehospital electrocardiogram (ECG) and administration of aspirin are evidence-based strategies for patients with acute coronary syndrome (ACS). However, emergency medical services (EMS) compliance in patients with suspected ACS varies widely. We sought to understand the barriers to prehospital ECG acquisition and aspirin administration for patients with suspected ACS.
Methods
In this qualitative study, we interviewed EMS clinicians at three geographically diverse United States (U.S.)-based EMS agencies. We interviewed practicing clinicians and quality and operations leaders at these agencies. Based on the Reach, Effectiveness, Adoption, Implementation, and Maintenance (RE-AIM) framework, interviews were recorded, transcribed, and analyzed using a grounded qualitative approach with open coding. The Systems Engineering Initiative for Patient Safety (SEIPS) framework and a constant comparison technique were used to identify and refine themes.
Results
Twenty-five paramedics and 20 additional agency personnel participated. Median age was 41 (IQR: 34–51) years and 13 (29%) were female. Themes were organized using SEIPS and longitudinally through four phases of an EMS call. During the pre-arrival phase, staffing challenges, training quality, and dispatch may anchor EMS clinicians on a diagnosis. During the diagnosis and treatment phase, safety and communication barriers may take priority over care delivery. Additionally, EMS clinicians must allocate assets (e.g. whether to send an advanced life support unit) and financial resources; veteran EMS clinicians identified their experience whereas newer clinicians cited their recent education when making these decisions. Also, diagnostic uncertainty due to increasing patient complexity and atypical presentations contributed to diagnostic errors. During the response and transport phase, the scope of practice limits the use and interpretation of the ECG, with clinicians reporting that liberal use of ECG led to more rapid decision-making. Finally, in the after phase, personnel reported the “psychologically taxing” nature of the job contributing to biases, bad habits, and burnout. Performance feedback was desired for personal development, though currently perceived as infrequent and punitive.
Conclusions
Multiple, interrelated themes underscored the complexities of delivering evidence-based care to prehospital patients with ACS. Education in ECG interpretation, resource allocation, bias, and enhancing feedback may serve as strategies to address the identified barriers.
Introduction
Recognizing that “time is muscle” in cardiac emergencies (Citation1–4), substantial efforts have focused on developing systems of care, like the American Heart Association’s (AHA) Mission: Lifeline initiative (Citation5), to prioritize the safe and efficient management of patients with ST-elevation myocardial infarction (STEMI) from the prehospital setting through coronary reperfusion. Beyond timely care, there are two actions that Emergency Medical Services (EMS) can perform that are evidence-based for the prehospital management of patients with STEMI. The ISIS-2 trial established the mortality benefit of giving aspirin early, and administration of aspirin to patients with suspected Acute Coronary Syndrome (ACS) in the prehospital setting is the standard of care (Citation6). Studies also demonstrated that prehospital electrocardiograms (ECG) are associated with a reduction in door-to-balloon time (Citation7) and mortality (Citation8). Recognizing EMS’s critical role in ACS care, the AHA recommended obtaining prehospital ECGs to improve the chain of survival (Citation9). With increased recognition of the essential role of EMS in the chain or survival, the appropriate administration of aspirin and use of ECG are priorities for prehospital clinicians caring for patients with suspected ACS. However, there is substantial variability in the performance of this care. An ECG is performed in the prehospital setting between 20% and 80% of the time in patients with suspected ACS and aspirin is given only 45% and 58% of the time to patients with acute myocardial ischemia and/or suspected ACS (Citation10–12). Reasons for variability may be due to atypical presentations of ACS, time of day, female sex, younger age, Black, Hispanic, and those with more comorbidities, and rurality of the calls (Citation10,Citation13,Citation14).
Despite the critical role for the care of prehospital patients with suspected ACS, there is limited research examining reasons for this variability, particularly amongst United States (U.S.)-based EMS systems. In an abstract from the United Kingdom about the performance of ECGs, focus groups reported that decision-making was impacted by patient characteristics (e.g., age, sex, ethnicity, privacy), clinician training, and systemic barriers like equipment availability, distance to the percutaneous coronary intervention center, guidelines, and organizational pressures (Citation15). A study of Hong-Kong EMS clinicians examining ECG performance cited patient privacy concerns and patients’ desire to forgo ECG to not further delay transport to the hospital (Citation16). In a Chinese study, interviewees identified a theme of capacity limitations and disjointed care leading to STEMI treatment delay (Citation17). In Sub-Saharan Africa, coronary care networks were identified as fragmented secondary to delayed STEMI recognition, systems delays, and lack of regionalized care (Citation18). In a single qualitative study from the U.S., EMS clinicians identified that communication barriers, lack of supplies, protocol changes, and experience all impact timely prehospital STEMI care (Citation19).
While emerging data paints a complex portrayal of the barriers to ECG use in the prehospital setting, important gaps in understanding this variability in US-based EMS systems of care remain. To address these gaps, we sought to use qualitative methods to understand a diverse set of perspectives on this challenge using EMS clinician and stakeholder (operational leadership, education, and quality assurance leaders) perspectives with the goal of identifying potentially modifiable targets for future intervention studies.
Methods
We used a qualitative approach with semi-structured interviews to understand EMS and stakeholders’ perceptions of barriers to the use of evidence-based guidelines in the prehospital care of patients with suspected ACS.
Setting and Selection of Participants
We partnered with ESO, Inc. as part of a larger National Institutes of Health study on prehospital ACS care to conduct interviews at three heterogenous prehospital agencies. We recruited three EMS agencies from the South, Mid-Atlantic, and Northwest regions of the US to participate via convenience sampling of agencies already using ESO. Their annual call volumes and staffing varied from 25,000–106,000 calls and from 130–600 staff members. Within the selected agencies, EMS clinicians and stakeholders were recruited through local champions, email notifications, and snowball recruiting techniques through other participants.
Study participants included EMS clinicians from each agency. Clinicians were included if they worked at least one clinical shift in the preceding month with at least one EMS call for a patient with chest pain. Additional stakeholders included clinical and operational leaders at the organizations with previous EMS field experience and supervisory roles in feedback and compliance, including local training officers, medical directors, and local administrative leadership. These stakeholders were not required to be from one of the three EMS agencies so that we could enhance broader representation of the stakeholder perspectives. This study was approved by the Vanderbilt University Medical Center Institutional Review Board, as exempt as it was minimal risk.
Data Collection
One-on-one semi-structured interviews were conducted virtually by two study personnel including one coauthor (MR) using an interview guide () based on the Reach, Effectiveness, Adoption, Implementation, and Maintenance (RE-AIM) framework to assess the reach, effectiveness, adoption, implementation, and maintenance of a public health intervention like prehospital ECG and aspirin in suspected ACS (Citation20,Citation21). Interview guides were developed and tailored to each group of respondents. EMS clinicians were asked questions about attitudes, norms, and potential motivators of behavior change, specifically 1) barriers of guideline recommended care; 2) potential incentives to address gaps in care; and 3) context, including EMS workflow and processes in the care of suspected ACS patients. Stakeholders were asked questions about the characteristics of practice setting and environment surrounding feedback and quality review, specifically 1) potential site variability for guideline recommended care and 2) existing approaches to feedback. In addition to planned prompts in the interview guide, participants were asked follow-up questions to clarify responses and elicit further detail.
Table 1. Summary of EMS clinician and stakeholder interview guides.
Interviewers planned to pilot the interview guide with up to 10 participants and these pilot interviews were recorded and reviewed by a qualitative methods expert. All interviews were conducted virtually by a trained interviewer (MR) at a time convenient to the participant to minimize interference with clinical work. Interviews were targeted to last approximately 30 min, recorded using Microsoft Teams (Redmond, WA), transcribed and de-identified by a transcriptionist (Home Row, Inc., Henderson, NV), and stored securely with a unique participant number. Once the interviewer was trained and interview guide finalized, the pilot was completed and we planned to review interview findings after 3–5 interviews to evaluate for thematic and content saturation, the point at which no new information is learned (Citation22). We then reviewed every 3–5 interviews until thematic saturation was reached by consensus with the study team.
Analysis
We used the Systems Engineering Initiative for Patient Safety (SEIPS) model to analyze the interview transcripts. The SEIPS model is a patient safety framework to help explain how system design can impact both patient safety and outcomes of employees, patient, and the organization (Citation23). Applied to the prehospital setting, the SEIPS model facilitates an examination of the patient through their prehospital care journey focusing on how people, environment, tasks, technology, processes, feedback, and outcomes influence health care quality and patient safety. We reasoned that this framework best suited the objective of this research to examine patients with suspected ACS, as they experience multiple phases of care in the prehospital setting that rely on many interrelated factors related to people (patients and clinicians), environments, tasks, and processes.
A hierarchical coding system was developed and refined using an iterative, grounded, inductive qualitative approach guided by the SEIPS model. In developing the coding system, we identified 29 major themes that were further subdivided into subthemes. Transcripts were then coded by an open coding approach using Dedoose (Los Angeles, CA).
After thematic saturation was achieved, we calculated the frequencies of each code to examine the distribution of quotes. The codes were then cross-referenced with quotes to identify themes and to identify representative quotes of potential barriers to evidence-based care. These themes were presented and analyzed by the research team in an iterative process to further refine the themes and subthemes along the EMS continuum of care, beginning at EMS dispatch and ending after the delivery of the patient to the health care facility. Transcripts, quotation, and codes were all managed using Microsoft Teams and Excel (Microsoft Inc., Redmond, WA), and Dedoose (Manhattan Beach, CA). This research adheres to the Consolidated Criteria for Reporting Qualitative Research (COREQ) guidelines for qualitative research (Citation24).
Results
A total of 45 interviews were conducted. Twenty-five paramedics and 20 clinical and operational stakeholders were interviewed. Their demographics are presented in . The median age of EMS clinicians was 34 (interquartile range [IQR] 31.5–48.5) years, the median years of service was 17 (IQR 12–23.5), and 7 (28%) were female. All clinicians were paramedics, and one was also a nurse. Among stakeholders, two were quality officers (10%), six were medical directors (30%), four were EMS/fire chiefs (20%), two were STEMI coordinators (10%), and six were EMS consultants/lawyers/executive directors (30%). The median age of stakeholders was 49 (IQR 38.8–58.8), and 6 (30%) were female.
Table 2. Characteristics of interview participants.
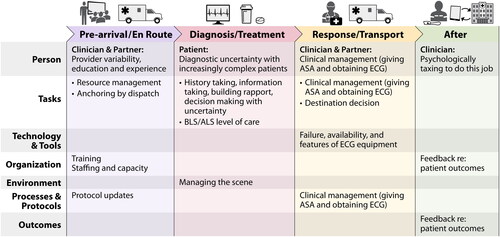
Qualitative results are organized by intervals along the EMS care continuum, with several themes noted during each interval. The discrete time intervals used were 1) pre-arrival/en route to a call, 2) the diagnosis/treatment phase, 3) the response/transport phase, and 4) after the call phase. The pre-arrival/en route phase begins when the patient activates 9-1-1 until EMS arrives on scene. It also includes any education or training that the clinician may have received prior to the call. The diagnosis/treatment phases begins when the clinician encounters the patient and lasts until transport to the hospital begins. The response/transport phase includes the interval between scene departure and handing over care at the hospital. The phase of care after the call includes documentation, emotional response, and feedback/follow-up on patient care. The salient themes are visually represented throughout the course of an EMS call in .
Figure 1. Summary of themes and subthemes from 45 interviews with EMS clinicians and stakeholders organized by phase of the EMS call (x-axis) and the SEIPS framework domains (y-axis).
Pre-Arrival/En Route Phase
Prior to being activated for a potential ACS call, the training, agency protocols, availability of staffing, and type of information provided by telecommunicators impact the delivery of care once upon scene. First, interviewees discussed how variable involvement from their medical directors may delay or outright prevent updates in prehospital protocols.
Some of your younger doctors or more progressive doctors are constantly doing research. So, they might be titrating their protocols regularly […] as new research comes out. Versus your veteran doctor, who – can’t teach an old dog new tricks. […] They don’t like change, and their protocols probably reflect that same demeanor. – Paramedic 24
Additionally, interviewees cited how staffing and capacity issues frequently made it difficult to provide the level of care that they would like to.
Currently we’re struggling with is staffing, which all agencies are struggling with that right now. […] But if we don’t have enough paramedics come to work during the day for our shift, we might have to make those ambulances that would’ve been in advanced life support, a basic life support. – Stakeholder 16, STEMI coordinator
Additionally, some clinicians referenced how dispatch’s communications can potentially anchor a responding team on a diagnosis and its severity, but that when they receive new or conflicting information, they must be able to pivot their decision making and diagnosis.
We have a high amount of stimulant and drug use, also. So, […] you have to be careful about being led down the wrong path and just assuming it’s just a drug overdose. – Stakeholder 10, Assistant Fire Chief
Diagnosis and Treatment Phase
The diagnosis and management of a patient on scene with suspected ACS can be complex, delaying definitive diagnosis and prompt treatment. Interviewees cited multiple challenges including communication barriers, complex and atypical presentations of potentially life-threatening illnesses, how clinician experience impacts care activities performed while on scene and the need to allocate resources while caring for the patient.
First, when on scene, a recurring theme was the challenge of obtaining a history, gathering information, and building a rapport with the patient.
The number one thing would be any kind of communication barrier […] If the patient’s unresponsive already, then obviously it makes it harder to provide care. If the patient speaks different languages, it makes it harder to provide care because we have to go through our language line and […] there’s always some errors in translation and there’s some time barriers. – Stakeholder 4, Medical Director
Communication barriers further compounded prompt care when patients did not comprehend the potential severity of their illness.
Willingness to be helped makes it easier on me. We run into a lot of patients that are not willing to go to the hospital. Even if you’re telling them, "You’re having a heart attack," and they’re like, "No, I don’t want to go.”–Stakeholder 11, Associate Chief Medical Officer
In addition, paramedics and stakeholders frequently referenced how patient presentations have become more complex and it is difficult to deal with making decisions in uncertainty.
Chest pain, or what people think is chest pain, isn’t always chest pain. So, your elderly, female diabetics, they don’t have chest pain all the times when they’re having a heart attack. – Paramedic 24
Increased experience was identified as motivating prompt care while on scene.
When you walk into a bedroom, you look at a person, are they sick or not? […] and it’s until you start running those and get that real world experience that you can literally walk in and go, "They are sick." Like, I don’t even need their vital signs to tell you they’re not good. – Paramedic 5
Clinicians also cited how once they were on scene that they are often tasked with not only caring for the patient, but also the allocation of resources and triaging of assets due to resource limitations. They spoke about the need to make decisions related to whether to transport to a catheterization lab capable center, to use an ALS unit, and whether to drive with the use of lights and sirens.
We were supposed to be dispatched to a patient, care first for that patient and then bring them to the hospital, rather than necessarily having to decide what level of resources are appropriate for their care. But the reality is because of the constraints of resources that we face, we have to make such decisions. – Stakeholder 20, EMS Systems Consultant
Response and Transport Phase
The response and transport phase includes the transportation of the patient to the hospital. Impacting the use of aspirin and ECG were the perceived attitudes about their use, and scope of practice under the clinician’s license. Specifically, interviewees referenced how clinical management varies from patient to patient, but that more liberal use of ECG and aspirin were warranted.
I generally perform 12-leads on just about everybody. If they have an issue going from their belly button all the way up to their head, anything that I think is neurological or cardiac or pulmonary, or if they are nausea or chest pain, I get a 12-lead. Some medics do not. – Stakeholder 8, Quality Assurance Officer
I would say the bar is pretty low if they don’t have an allergy to [aspirin]. We tend to be pretty liberal with it simply because, from what I understand, it’s one of the medications we have that really does show mortality benefit. – Stakeholder 20, EMS Systems Consultant
Additionally, depending on the level of the clinician, some tools, such as ECG, may not be available or they may not be able to interpret the readings based on their scope of practice.
Or they might not even […] have the tools. You know, […] like our BLS providers, they don’t have the capability […] to perform or to interpret 12-lead EKGs. So […] if they just think, oh, this person just has, like, a, you know, like a stomach flu or something like that, they’ll just transport the patient to the closest hospital. – Paramedic 11
After Phase
In the phase following the EMS encounter, the quality and timing of feedback along with the emotional toll of the job were recognized as taxing. These factors impact how EMS clinicians prepare for the next response, their emotional state when they do so, and potential biases that may arise.
Interviewees discussed how they wanted more feedback on their patients’ outcomes at the hospital, and how the quality of feedback that they receive was often lacking. They discussed how feedback is essential for education and growth.
At an agency level, if paramedics don’t hear back that they activated a STEMI alert, and it wasn’t a STEMI, they don’t know that they’re doing something wrong. So, that could lead to differences in care for sure. And I've done some work on that, actually, just showing that the feedback that individual people get in EMS is so poor that there’s no way for them to learn, in essence, right? They can’t learn from their mistakes or their successes because they never hear back. – Paramedic 18
So, for me looking at those reports, it’s really to be able to help the patient, you know, identify if I'm doing good job, if our agency’s doing a good job. And if I see faults in something, I can obviously let my supervisors know and push that up the chain of command and if they identify that I'm right, they would work on fixing it because their goal is just like mine, good patient care. – Stakeholder 16, STEMI Coordinator
In addition, clinicians also discussed how it can be psychologically taxing to do the job of EMS, and how the constant stress of the job wears on clinicians and may lead to biases about the patient population they care for.
We have to be the duck. If you ever see a duck floating on the water, he looks calm and relaxed. But if you look at his feet under the water, those little feet are going a mile a minute to keep him relaxed, you know? And that’s, you know, inside our brain is going a mile a minute, but outside we have to be the duck. We have to be just calm all times. – Paramedic 5
We all have bias of some type. But if we choose to let that bias affect how we deliver our care – and that bias can be something as simple as race. Something as simple as somebody having an accent that you just don’t understand, or just somebody that you may typically run on a lot, even an individual that you know. […] So, not having that bias. I won’t say, "not having it," but not letting it affect you doing a good patient assessment and providing good and competent care, I think is really key – Stakeholder 10, Assistant Fire Chief
Discussion
Interviews of EMS clinicians and stakeholders illustrated how EMS clinicians work in a complex system that is often resource constrained, time-pressured, and mentally challenging. Major themes emerged that impact the use of evidence-based care in suspected ACS patients, including: training, availability of staffing, dispatch anchoring, atypical clinical presentations, communication barriers, the role of experience in recognizing illness severity, triaging resources, attitudes about the use of evidence-based care, scope of practice license, the dearth of quality feedback, and the psychological stress of working in EMS.
The revealed themes regarding challenges of providing evidence-based care to patients with suspected cardiovascular emergencies in the prehospital environment are grounded in prior research. Delivery of evidence-based care is complicated by staffing shortages and hospital capacity issues. This has likely become more prevalent in recent years as greater attention is paid to the high rate of turnover in the EMS workforce (Citation25), and how to address the EMS workforce crisis (Citation26, Citation27). Additionally, participants discussed the important role of medical directors in updating protocols to deliver evidence-based care. Carey et al. (Citation28) interviewed prehospital clinicians and identified similar findings that direct medical oversight facilitates guideline concordant care, while ambiguous protocols hinder evidence-based care.
Once on scene, the environment, patients and their families, and task management create further complexity. In our interviews, paramedics discussed how difficulties in overcoming communication challenges and quickly establishing rapport hindered their ability to deliver evidence-based care. A retrospective analysis quantified language barriers in prehospital care delays in Minnesota, and found that while small, language barriers were identified in 3.3 out of every 1,000 patient encounters (Citation29). Further and consistent with our findings, patients with multiple chronic medical comorbidities did not receive approximately 20% of guideline recommendations (Citation30). Groups that do not present with typical ACS symptoms were also less likely to receive evidence-based care (Citation14,Citation31–33).
Clinicians identified that during the treatment and response phase of care, liberal use of ECGs was necessary to prevent missed cardiac emergencies. They also noted that dispatching the wrong level of ambulance or incorrectly triaging the severity of a patient meant that the EMS clinician transporting the patient may not even have the ability to perform and/or interpret an ECG based on their scope of practice. This is consistent with current recommendations that do not include a monitor capable of obtaining a 12-lead ECG on basic life support ambulances (Citation34).
In the final phase after the EMS call, EMS clinicians in our study often cited their desire for more robust feedback. This is consistent with prior studies that found that more than 97% of EMS clinicians desired more feedback, up to one third did not receive any feedback in the previous thirty days, and that clinicians universally thought that receiving feedback was either “essential” or “beneficial” (Citation35,Citation36). The EMS clinicians also reported in our interviews that the stress of the job contributed to burnout, fatigue, and bad habits in their care of prehospital ACS patients. This is supported by researching highlighting the mental burden of working in EMS, with findings indicating that EMS clinicians have signs of posttraumatic stress syndrome, depression, higher sick day usage, and thoughts about leaving their job or the profession (Citation37–40).
These interviews underscore the relevance and challenges of these systemic factors in the relatively brief time periods for the delivery of prehospital care for patients with suspected ACS. Using the identified themes and representative quotes, we identified two potential interventions to address some of these barriers. First is the use of education and training to mitigate the experience gaps, unique patient populations, communication barriers, and different patient backgrounds that may generate biases. Prior research showed that quality improvement programs that inform continuing education and targeted educational interventions are effective strategies to improve performance (Citation41,Citation42). The second strategy is the delivery of targeted and systemic feedback to clinicians about care processes and patient outcomes. Multiple studies have shown that audit and feedback improve outcomes and guideline adherence (Citation41–45) and may be protective against burnout (Citation40). However, providing feedback effectively and in a sustainable manner is difficult and rarely done well. It should be timely, actionable, non-punitive, and delivered in a non-group setting (Citation44,Citation45). Within large EMS agencies, it can be difficult to scale this type of feedback to enhance adoption effectively. One potential approach to provide this feedback is through information exchange between hospitals and EMS agencies as there is more widespread adoption of electronic health records (Citation46). However, the design, delivery, context, and timeliness of such feedback remain important considerations in any feedback system (Citation47).
While feedback is an essential component of quality improvement and continuing education, a recent systematic review underscored the need for more rigorous study on the impact of EMS clinician feedback (Citation48). In the future, these studies will inform best practices for improving guideline adherence. These findings inform the design of tools and interventions to address the training and feedback gaps identified. However, they will need to be vetted through rigorous effectiveness implementation trials to examine their adoption, use, and effectiveness in real world settings.
Limitations
While our study represents perspectives from three distinct EMS agencies and stakeholders, generalizability beyond these settings is limited. Further, the clinician perspectives were all paramedics, without Basic Life Support (BLS) clinician perspectives represented. Further, these interviews represent perspectives of individuals and while attempts have been made to mitigate potential biases by the qualitative investigators through use of accepted qualitative methods, the potential remains for bias to exist. Finally, since interviewees were informed that they were being interviewed regarding guideline adherence in suspected ACS their responses may have been impacted by recall bias and social desirability bias. As a result, EMS clinician and stakeholder responses may not reflect actual practice nor the relative ranking of these opinions.
Conclusions
There are numerous barriers to use of aspirin and ECG use for patients with suspected ACS in the prehospital setting. Through interviews with EMS clinicians and key stakeholders, this study identified potential barriers to the evidence-based care of prehospital patients with suspected ACS as: staffing and capacity issues, varying medical director involvement, dispatch anchoring, difficulty managing the scene, patient complexity and diagnostic uncertainty, varying levels of experience and training, resource management, clinical decision making, practice scope, lack of high-quality feedback, and clinician burnout. Potential interventions to address these barriers include targeted education and regular use of non-punitive, individualized feedback.
Declaration of Generative AI in Scientific Writing
The authors did not use a generative artificial intelligence (AI) tool or service to assist with preparation or editing of this work. The author(s) take full responsibility for the content of this publication.
Acknowledgments
None.
Disclosure Statement
The authors report there are no competing interests to declare.
Additional information
Funding
References
- Berger PB, Ellis SG, Holmes DRJ, Granger CB, Criger DA, Betriu A, Topol EJ, Califf RM. Relationship between delay in performing direct coronary angioplasty and early clinical outcome in patients with acute myocardial infarction: results from the Global Use of Strategies to Open Occluded Arteries in Acute Coronary Syndromes (GUSTO-IIb) trial. Circulation. 1999;100(1):14–20. doi:10.1161/01.cir.100.1.14.
- Cannon CP, Gibson CM, Lambrew CT, Shoultz DA, Levy D, French WJ, Gore JM, Weaver WD, Rogers WJ, Tiefenbrunn AJ. Relationship of symptom-onset-to-balloon time and door-to-balloon time with mortality in patients undergoing angioplasty for acute myocardial infarction. JAMA. 2000;283(22):2941–7. doi:10.1001/jama.283.22.2941.
- McNamara RL, Wang Y, Herrin J, Curtis JP, Bradley EH, Magid DJ, Peterson ED, Blaney M, Frederick PD, Krumholz HM, NRMI Investigators Effect of door-to-balloon time on mortality in patients with ST-segment elevation myocardial infarction. J Am Coll Cardiol. 2006;47(11):2180–6. doi:10.1016/j.jacc.2005.12.072.
- Rathore SS, Curtis JP, Chen J, Wang Y, Nallamothu BK, Epstein AJ, Krumholz HM, National Cardiovascular Data Registry Association of door-to-balloon time and mortality in patients admitted to hospital with ST elevation myocardial infarction: national cohort study. BMJ. 2009;338(may19 1):b1807–b1807. Cited: in: PMID: 19454739. doi:10.1136/bmj.b1807.
- Zeitouni M, Al-Khalidi HR, Roettig ML, Bolles MM, Doerfler SM, Fordyce CB, Hellkamp AS, Henry TD, Magdon-Ismail Z, Monk L, et al. Catheterization laboratory activation time in patients transferred with ST-segment–elevation myocardial infarction: insights from the mission: lifeline STEMI accelerator-2 project. Circ Cardiovasc Qual Outcomes. 2020;13(7):e006204. doi:10.1161/CIRCOUTCOMES.119.006204.
- Randomised trial of intravenous streptokinase, oral aspirin, both, or neither among 17,187 cases of suspected acute myocardial infarction: ISIS-2. The Lancet. 1988;332(8607):349–60. doi:10.1016/S0140-6736(88)92833-4.
- Bradley EH, Herrin J, Wang Y, Barton BA, Webster TR, Mattera JA, Roumanis SA, Curtis JP, Nallamothu BK, Magid DJ, et al. Strategies for reducing the door-to-balloon time in acute myocardial infarction. N Engl J Med. 2006;355(22):2308–20. doi:10.1056/NEJMsa063117.
- Nam J, Caners K, Bowen JM, Welsford M, O'Reilly D. Systematic review and meta-analysis of the benefits of out-of-hospital 12-lead ECG and advance notification in ST-segment elevation myocardial infarction patients. Ann Emerg Med. 2014;64(2):176–86.e9. doi:10.1016/j.annemergmed.2013.11.016.
- Jacobs AK, Antman EM, Faxon DP, Gregory T, Solis P. Development of systems of care for ST-elevation myocardial infarction patients. Circulation. 2007;116(2):217–30. doi:10.1161/CIRCULATIONAHA.107.184043.
- Zègre-Hemsey JK, Asafu-Adjei J, Fernandez A, Brice J. Characteristics of prehospital electrocardiogram use in North Carolina using a novel linkage of emergency medical services and emergency department data. Prehosp Emerg Care. 2019;23(6):772–9. Cited: in:: PMID: 30885071. doi:10.1080/10903127.2019.1597230.
- Strandmark R, Herlitz J, Axelsson C, Claesson A, Bremer A, Karlsson T, Jimenez-Herrera M, Ravn-Fischer A. Determinants of pre-hospital pharmacological intervention and its association with outcome in acute myocardial infarction. Scand J Trauma Resusc Emerg Med. 2015;23:105. [cited 2023 Aug 18 doi:10.1186/s13049-015-0188-x.
- Tataris KL, Mercer MP, Govindarajan P. Prehospital aspirin administration for acute coronary syndrome (ACS) in the USA: an EMS quality assessment using the NEMSIS 2011 database. Emerg Med J. 2015;32(11):876–81. Cited: in:: PMID: 25678574. doi:10.1136/emermed-2014-204299.
- McDonald N, Little N, Grierson R, Weldon E. Sex and gender equity in prehospital electrocardiogram acquisition. Prehosp Disaster Med. 2022;37(2):1–7. doi:10.1017/S1049023X2200036X.
- Ebben RH, Vloet LC, Verhofstad MH, Meijer S, Groot JAM, van Achterberg T. Adherence to guidelines and protocols in the prehospital and emergency care setting: a systematic review. Scand J Trauma Resusc Emerg Med. 2013;21(1):9. doi:10.1186/1757-7241-21-9.
- Halter M, Calovski V, Davies G, Driscoll T, Gale C, Gavalova L, Hampton C, Quinn T, Snooks H, Watkins A, et al. OP8 What factors do ems clinicians report as influencing their decision to perform a prehospital 12 lead ECG in acute coronary syndromes?: a qualitative study. Emerg Med J. 2020;37(10):e5–e5. doi:10.1136/emermed-2020-999abs.8.
- Cheung KS, Leung LP, Siu YC, Tsang TC, Tsui MS, Tam CC, Chan RH. Prehospital 12-lead electrocardiogram for patients with chest pain: a pilot study. Hong Kong Med J. 2018;24(5):484–91. doi:10.12809/hkmj177135.
- Yin X, He Y, Zhang J, Song F, Liu J, Sun G, Liang Y, Ye J, Hu Y, Song M, et al. Patient-level and system-level barriers associated with treatment delays for ST elevation myocardial infarction in China. Heart. 2020;106(19):1477–82. PMID: 32580976. doi:10.1136/heartjnl-2020-316621.
- Stassen W, Kurland L, Wallis L, Castren M, Vincent-Lambert C. Barriers and facilitators to implementing coronary care networks in South Africa: a qualitative study. Afr Health Sci. 2020;20(1):338–50. Cited: in:: PMID: 33402921. doi:10.4314/ahs.v20i1.39.
- Carpenter R, McWhorter R, Donaldson S, Silberman D, Maffei S. Working against the clock: a model for rural STEMI triage. Health Serv Insights. 2021;14:11786329211037521. doi:10.1177/11786329211037521.
- Glasgow RE, Vogt TM, Boles SM. Evaluating the public health impact of health promotion interventions: the RE-AIM framework. Am J Public Health. 1999;89(9):1322–7. Cited: in:: PMID: 10474547. doi:10.2105/ajph.89.9.1322.
- Glasgow RE, Harden SM, Gaglio B, Rabin B, Smith ML, Porter GC, Ory MG, Estabrooks PA. RE-AIM planning and evaluation framework: adapting to new science and practice with a 20-year review. Front Public Health. 2019;7:64. Cited: in:: PMID: 30984733. doi:10.3389/fpubh.2019.00064.
- Saunders B, Sim J, Kingstone T, Baker S, Waterfield J, Bartlam B, Burroughs H, Jinks C. Saturation in qualitative research: exploring its conceptualization and operationalization. Qual Quant. 2018;52(4):1893–907. Cited: in:: PMID: 29937585. doi:10.1007/s11135-017-0574-8.
- Carayon P, Wooldridge A, Hoonakker P, Hundt AS, Kelly MM. SEIPS 3.0: human-centered design of the patient journey for patient safety. Appl Ergon. 2020;84:103033. doi:10.1016/j.apergo.2019.103033.
- Tong A, Sainsbury P, Craig J. Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. Int J Qual Health Care. 2007;19(6):349–57. doi:10.1093/intqhc/mzm042.
- Kurth JD, Powell JR, Gage CB, Fauvel AD, Crowe RP, Cash RE, Panchal AR. Evaluating changes in the emergency medical services workforce: a preliminary multistate study. J Am Coll Emerg Physicians Open. 2023;4(3):e12975. [cited 2024 Feb 5 doi:10.1002/emp2.12975.
- Baird S, Evans B. Congressional letter on the EMS workforce shortage. Washington (DC): American Ambulance Association; 2021. [accessed 2024 Mar 19]. https://ambulance.org/2021/10/04/workforceshortage/.
- American Ambulance Association. EMS workforce shortage: support initiatives for the hiring, retention and training of paramedics and EMTs. Washington (DC); 2023, May 31. https://www.dropbox.com/s/2si8p2bpsmy79kx/5-31-2023%20EMS%20Shortage%20One-Pager.docx?dl=0.
- Carey JM, Studnek JR, Browne LR, Ostermayer DG, Grawey T, Schroter S, Lerner EB, Shah MI. Paramedic-identified enablers of and barriers to pediatric seizure management: a multicenter, qualitative study. Prehosp Emerg Care. 2019;23(6):870–81. Cited: in:: PMID: 30917730. doi:10.1080/10903127.2019.1595234.
- Grow RW, Sztajnkrycer MD, Moore BR. Language barriers as a reported cause of prehospital care delay in Minnesota. Prehosp Emerg Care. 2008;12(1):76–9. Cited: in:: PMID: 18189182. doi:10.1080/10903120701709878.
- Cohen-Stavi CJ, Key C, Giveon S, Molcho T, Balicer RD, Shadmi E. Assessing guideline-concordant care for patients with multimorbidity treated in a care management setting. Fam Pract. 2020;37(4):479–85. doi:10.1093/fampra/cmaa024.
- Rothrock SG, Brandt P, Godfrey B, Silvestri S, Pagane J. Is there gender bias in the prehispital management of patients with acute chest pain? Prehosp Emerg Care. 2001;5(4):331–4. doi:10.1080/10903120190939454.
- Cannon AR, Lin L, Lytle B, Peterson ED, Cairns CB, Glickman SW. Use of prehospital 12-lead electrocardiography and treatment times among ST-elevation myocardial infarction patients with atypical symptoms. Acad Emerg Med. 2014;21(8):892–8. doi:10.1111/acem.12445.
- Li T, Cushman JT, Shah MN, Kelly AG, Rich DQ, Jones CMC. Barriers to providing prehospital care to ischemic stroke patients: predictors and impact on care. Prehosp Disaster Med. 2018;33(5):501–7. doi:10.1017/S1049023X18000766.
- Lyng J, Adelgais K, Alter R, Beal J, Chung B, Gross T, Minkler M, Moore B, Stebbins T, Vance S, et al. Recommended essential equipment for basic life support and advanced life support ground ambulances 2020: a joint position statement. Prehosp Emerg Care. 2021;25(3):451–9. Cited: in:: PMID: 33557659. doi:10.1080/10903127.2021.1886382.
- Lavoie CF, Plint AC, Clifford TJ, Gaboury I. “I never hear what happens, even if they die”: a survey of emergency physicians about outcome feedback. Can J Emergency Med. 2009;11(6):523–8. doi:10.1017/S1481803500011787.
- Cash RE, Crowe RP, Rodriguez SA, Panchal AR. Disparities in feedback provision to emergency medical services professionals. Prehosp Emerg Care. 2017;21(6):773–81. Cited in:: PMID: 28622074. doi:10.1080/10903127.2017.1328547.
- Crowe RP, Bower JK, Cash RE, Panchal AR, Rodriguez SA, Olivo-Marston SE. Association of burnout with workforce-reducing factors among EMS professionals. Prehosp Emerg Care. 2018;22(2):229–36. Cited: in:: PMID: 28841102. doi:10.1080/10903127.2017.1356411.
- Donnelly E. Work-related stress and posttraumatic stress in emergency medical services. Prehosp Emerg Care. 2012;16(1):76–85. Cited: in:: PMID: 22128908. doi:10.3109/10903127.2011.621044.
- Hruska B, Barduhn MS. Dynamic psychosocial risk and protective factors associated with mental health in Emergency Medical Service (EMS) personnel. J Affect Disord. 2021;282:9–17. doi:10.1016/j.jad.2020.12.130.
- Crowe RP, Fernandez AR, Pepe PE, Cash RE, Rivard MK, Wronski R, Anderson SE, Hogan TH, Andridge RR, Panchal AR, et al. The association of job demands and resources with burnout among emergency medical services professionals. J Am Coll Emerg Physicians Open. 2020;1(1):6–16. Cited: in:: PMID: 33000008. doi:10.1002/emp2.12014.
- Joyce SM, Dutkowski KL, Hynes T. Efficacy of an EMS quality improvement program in improving documentation and performance. Prehosp Emerg Care. 1997;1(3):140–4. Cited: in:: PMID: 9709356. doi:10.1080/10903129708958807.
- Ebben RHA, Siqeca F, Madsen UR, Vloet LCM, Achterberg T v Effectiveness of implementation strategies for the improvement of guideline and protocol adherence in emergency care: a systematic review. BMJ Open. 2018;8(11):e017572. doi:10.1136/bmjopen-2017-017572.
- Choi B, Tsai D, McGillivray CG, Amedee C, Sarafin J-A, Silver B. Hospital-directed feedback to emergency medical services improves prehospital performance. Stroke. 2014;45(7):2137–40. doi:10.1161/STROKEAHA.114.005679.
- Hysong SJ, SoRelle R, Hughes AM. Prevalence of effective audit-and-feedback practices in primary care settings: a qualitative examination within veterans health administration. Hum Factors. 2022;64(1):99–108. doi:10.1177/00187208211005620.
- Hysong SJ, Best RG, Pugh JA. Audit and feedback and clinical practice guideline adherence: making feedback actionable. Implement Sci. 2006;1(1):9. Cited: in:: PMID: 16722539. doi:10.1186/1748-5908-1-9.
- Adler-Milstein J, Holmgren AJ, Kralovec P, Worzala C, Searcy T, Patel V. Electronic health record adoption in US hospitals: the emergence of a digital “advanced use” divide. J Am Med Inform Assoc. 2017;24(6):1142–8. Cited: in:: PMID: 29016973. doi:10.1093/jamia/ocx080.
- Brown B, Gude WT, Blakeman T, Veer SNvd, Ivers N, Francis JJ, Lorencatto F, Presseau J, Peek N, Daker-White G. Clinical Performance Feedback Intervention Theory (CP-FIT): a new theory for designing, implementing, and evaluating feedback in health care based on a systematic review and meta-synthesis of qualitative research. Implement Sci. 2019;14(1):40. [cited 2023 Oct 25 doi:10.1186/s13012-019-0883-5.
- Wilson C, Janes G, Lawton R, Benn J. Types and effects of feedback for emergency ambulance staff: a systematic mixed studies review and meta-analysis. BMJ Qual Saf. 2023;32(10):573–88. Cited: in: PMID: 37028937. doi:10.1136/bmjqs-2022-015634.
