
ABSTRACT
OBJECTIVES: Emergency medical services (EMS) provide health care in situations with limited time and resources. Challenges arise when introducing novel medications, treatments, or technologies or modifying existing practices in these settings. Effective implementation strategies are pivotal for their success. This study aims to identify and categorize potential facilitators and barriers in the implementation of prehospital EMS through a review of relevant research articles.
METHODS: We searched PubMed and EMbase to identify studies published before December 2023, following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines for our search strategy and scoping review. We included original articles written in English that report on the factors that influence the implementation in prehospital settings. We extracted and categorized the factors into different themes.
RESULTS: Out of the 371 retrieved papers, we selected 19 (5%) for inclusion in this review. We extracted 46 influencing factors from the selected articles and categorized them into ten themes: (1) Outer system, (2) Inner system, (3) Practitioner characteristics, (4) Resources, (5) Communication and collaboration, (6) Patient factors, (7) Intervention characteristics, (8) De-implementation of prior practices, (9) Logistical issues, and (10) Quality improvement.
CONCLUSIONS: This study examined the literature on EMS implementation factors and proposed a 10-theme EMS model framework. Key factors include training/education, equipment/tools, communication with hospitals, and practitioners’ attitudes.
Disclaimer
As a service to authors and researchers we are providing this version of an accepted manuscript (AM). Copyediting, typesetting, and review of the resulting proofs will be undertaken on this manuscript before final publication of the Version of Record (VoR). During production and pre-press, errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal relate to these versions also.INTRODUCTION
Implementation science is the systematic integration of research findings and evidence-based practices into existing practice while ensuring their effectiveness [1]. Various theoretical frameworks have been introduced and used in previous research on implementation science, including the behavior change theory, the planned change framework, and the knowledge-to-action framework [2]. When promoting new implementation tasks, these theoretical frameworks can be used to mitigate resistance and enhance implementation efforts. Implementation science has gained recognition in the health care field, and several frameworks have been developed recently for health care applications. Damschroder et al. introduced the comprehensive Consolidated Framework for Implementation Research (CFIR) structure in 2009 by integrating 19 existing theoretical frameworks for implementation science [3]. The CFIR has since become one of the most extensively applied implementation frameworks in the health care field.
Emergency medical services (EMS) refer to the provision of medical treatment in prehospital settings and transportation for patients with acute illnesses or injuries. This service is typically provided by trained health care professionals, such as emergency medical technicians (EMTs) or paramedics. To provide rapid, efficient, and effective care, different EMS systems have established various treatment protocols. Emergency medical service systems in different regions must be tailored according to variations in local resources, training programs, and health care systems. With advancements in emergency medicine, some drugs and technologies may be beneficial for patients in prehospital settings. Moreover, as medical evidence evolves, treatment guidelines are updated accordingly. The implementation of these updates can be challenging in prehospital settings. There are more uncontrollable factors in the prehospital environment and more stakeholders, such as EMS clinicians, patients, hospital health care practitioners, and EMS administrators are involved compared to the hospital setting. These complexities can increase resistance to implementation. Some researchers have attempted to identify potential facilitators and barriers of implementation in EMS field [4-7]. In this study, we reviewed research related to the “implementation science in prehospital EMS” to identify and categorize known facilitators and barriers.
METHODS
Eligibility criteria
Our research question was: “Amongst EMS systems, what variables facilitate or hinder the implementation of specific interventions.” This guided the application of the Population, Exposure, Comparator, Outcome variables, Study design, Time frame (PECOST) framework of this scoping review:
Population: Health care practitioners implementing specific interventions in prehospital settings.
Exposure: Presence of any facilitators or barriers that possibly impact the implementation processes and outcomes.
Comparator: Absence of any specific factor.
Outcome variables: Identification and classification of known facilitators and barriers.
Study designs: We included articles that were: (1) written in English, (2) original articles relevant to the review question (excluding review articles, abstracts, and conference reports) published in peer-reviewed journals, and (3) reported on factors influencing implementation in prehospital settings. We excluded articles that addressed hospital settings and those that solely described the current implementation state. Furthermore, studies that exclusively relied on multiple-choice questions or questionnaires were also excluded, as closed-ended surveys may potentially limit data collection and synthesis.
Time frame: From inception to December 31, 2023.
Information source and search strategy
We employed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) criteria as the foundation for our search strategy and review. The review question posed was “What are the facilitators and the barriers that EMS stakeholders may encounter while implementing new guidelines, tools, or protocols in the prehospital setting?” We conducted a comprehensive search in December 2023 on the PubMed and EMbase databases using combinations of the following keywords: “emergency medical service,” “EMS,” “prehospital,” “implementation science,” “implementation,” “knowledge translation,” “barrier,” “facilitator,” and “enabler”. The titles and abstracts of all identified studies were initially examined by two reviewers, CYC and YCW, who rejected those that did not meet the inclusion criteria. Subsequently, we further reviewed the full articles of potentially relevant studies for inclusion. Any conflicts were resolved through discussion until an agreement was reached. Additionally, we scrutinized the references of the included articles to identify additional articles for potential inclusion.
Study selection, data extraction, and results synthesis
Two reviewers (CYC, CWY) independently screened the titles and abstracts. Discrepancies were resolved through discussion to achieve consensus, with full-text analysis employed where necessary. Two authors (CYC, CWY) extracted the data from the finalized study list, with any disparities addressed through discussion. Extracted data encompassed authorship, publication year, country, theoretical framework, study design, sample size, data collection method, outcome measures, and findings (Table 1).
Following data extraction, we employed a narrative synthesis methodology, entailing the systematic aggregation and summarization of data extracted from the included studies. In adherence to the methodological framework of scoping reviews, we did not perform a meta-analysis. The review adheres to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines, with specific extensions for Scoping Reviews.
RESULTS
Study selection
We obtained a total of 371 studies during our initial database search. After removing duplicates and screening the titles and abstracts, we identified 118 original articles published in peer-reviewed journals relevant to our research topic. We excluded two of the articles that could not be retrieved in full text. Following a comprehensive examination of the remaining 116 articles, we excluded those that were not original, not written in English, did not take place in prehospital settings, focused on reporting implementation outcomes rather than factors influencing implementation, or collected data only through questionnaires. A total of 20 articles were obtained for the analysis. Since two of these articles were published by the same first author using the same database, they were treated as a single entity, and the data extraction results were presented together [8, 9]. Finally, a total of 19 independent studies were included in this review (Figure 1).
Study characteristics
A total of 19 articles were incorporated in this review, spanning 2010 to 2023. An overview of these 19 articles is presented in Table 1. Among the 19 articles, 17 relied on qualitative research methods. Of the remaining 2 that employed mixed-method study designs, we retrieved the qualitative survey portion that mentioned the influencing factors [8, 9]. The data from seven articles were derived from interviews, six came from focus groups, and four used both.
In terms of the implemented interventions, three publications were general protocols, while the remaining 16 papers were associated with specific procedures, examinations, or treatments. The interventions included drawing blood, intravenous thrombolytic therapy, seizure management, pain management, resuscitation protocols, stroke care policies, oral steroid administration, prehospital palliative care, spinal immobilization with vacuum mattresses, remotely supported ultrasonographic examinations, termination of resuscitation efforts, prehospital emergency care system assessment tools, electronic patient care report systems, triage scales, and computerized clinical decision supports.
Among all of the studies we analyzed, only six articles (31.5%) focused exclusively on interviewing EMS clinicians [10-15]. The remaining articles included a broader range of participants, such as EMS clinicians, emergency department staff, medical directors, and policy implementers. Additionally, two studies did not provide the precise number of participants, whereas the number of participants in the remaining studies ranged from 10-66, with the majority being between 15-30.
More than half (10) of the publications did not rely on any theoretical frameworks but employed grounded theory to interpret the collected data. Furthermore, five out of the remaining nine articles that did apply theoretical frameworks used the CFIR research framework. All of these five studies were published in the last five years [5, 7, 16-18].
The factors influencing the implementation process in EMS systems
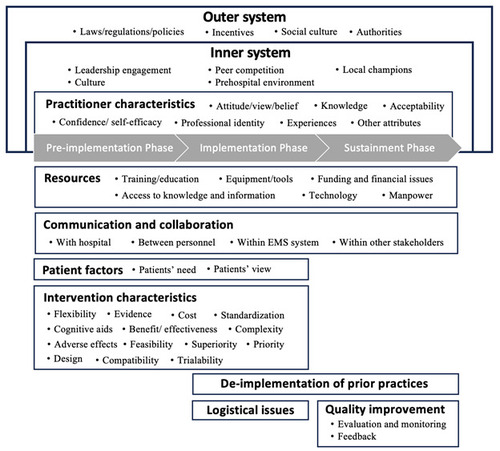
After carefully scrutinizing the 19 publications, we identified and extracted a total of 46 factors, encompassing both barriers and facilitators. We categorized these factors into ten themes, including: (1) Outer system, (2) Inner system, (3) Practitioner characteristics, (4) Resources, (5) Communication and collaboration, (6) Patient factors, (7) Intervention characteristics, (8) De-implementation of prior practices, (9) Logistical issues, and (10) Quality improvement (Table 2, Figure 2).
Outer system: The outer system refers to the broader environment outside of the EMS system. The factors within this theme include laws/regulations/policies, incentives, social culture, and authorities.
Inner system: The inner system encompasses factors within the EMS system. This theme includes leadership engagement, peer competition, local champions, culture, and the prehospital environment.
Practitioner characteristics: The intervention practitioner, mostly EMS clinicians, can affect the implementation. This theme includes factors such as attitudes/views/beliefs, knowledge, acceptability, confidence/self-efficacy, professional identity, experiences, and other traits.
Resources: The resources mentioned in the selected articles included training/education, equipment/tools, technology, access to knowledge and information, funding/financial issues, and manpower.
Communication and collaboration: Communication and collaboration occurs within the EMS system between the practitioner and the hospital, among personnel, and with other stakeholders.
Patient factors: Patient factors, such as patients’ needs and views, can impact implementation.
Intervention characteristics: Factors under this theme encompass flexibility, evidence, cost, cognitive aid, benefit/effectiveness, standardization, complexity, adverse effects, feasibility, superiority, priority, compatibility, design, and trialability. “Flexibility” means how an intervention can be modified, enhanced, or reimagined to align with prehospital needs. Cognitive aids include toolkits and checklists. “Adverse effects” encompass medication side effects and delayed transport to the hospital. “Feasibility” indicates whether the intervention is suitable for the prehospital setting. “Superiority” refers to whether a new approach is more advantageous than the current practice. “Priority” indicates if there are competing clinical priorities. “Compatibility” refers to how an intervention integrates into existing workflows and systems. “Trialability” refers to whether the intervention has been tested or trialed elsewhere.
De-implementation: Prior practices must be gradually phased out while implementing new strategies.
Logistical issues: During implementation, logistical issues such as equipment and drug regulation must be addressed.
Quality improvement: Evaluation and monitoring ensure implementation quality. Providing qualitative and quantitative feedback can help review and correct the implementation process.
We divided the implementation process into three phases: the pre-implementation phase, the implementation phase, and the sustainment phase. The themes that influence all three phases include the Outer system, Inner system, Practitioner characteristics, Communication and collaboration, and Resources. The Patient factors and Intervention characteristics affect the pre-implementation and implementation phases. De-implementation of prior practices is essential during the implementation and sustainment phases. Logistical issues are crucial during the implementation phase, while Quality improvement plays an essential role during the sustainment phase.
The top four factors mentioned most frequently in articles are Training/education (mentioned in 17 articles), Equipment/tools (13 articles), communication and collaboration with hospitals (12 articles), and practitioner’s attitudes/views/beliefs (12 articles).
DISCUSSION
From the selected articles, we extracted 46 factors that influence the implementation in prehospital settings. These factors were divided into 10 themes. Each theme impacts various phases of the implementation process. “Resources” and “Intervention characteristics” were mentioned in every selected articles. For individual factors, training/education, equipment/tools, communication and collaboration with hospitals, and practitioner’s attitude/views/beliefs were the most frequently mentioned across all articles. The present study synthesizes and classifies the existing literature on the factors that influence prehospital implementation, with a focus on identifying the most prominent ones. We hope that the findings of this research will serve as the groundwork for future studies in implementation science within the EMS field.
Systematic review of implementation science in prehospital settings
A systematic review of implementation science in prehospital settings was conducted by Fishe et al. in 2018 [19]. The purpose of the research was to examine the existing evidence regarding the methodologies used to implement evidence-based guidelines (EBGs) in prehospital settings. A total of 41 papers were incorporated into the analysis, with approximately one-third (n = 13) specifically examining implementation barriers. Our study focused on influencing factors and identified 19 relevant articles, which is more than Fishe uncovered. Fishe’s research identified several obstacles to successful implementation, such as difficulties in promoting collaboration among EMS agencies, hospitals, and governmental/regulatory bodies, and financial and resource constraints. In our study, the two most commonly mentioned factors among the selected articles were “Resources” and “Communication and collaboration with the hospital,” which aligns with Fishe’s findings. A detailed discussion of influencing factors is presented in the following section.
Comparison with the existing framework
Among the existing frameworks, we chose the CFIR framework because it is designed for health care settings and offers a comprehensive set of influencing factors. There are two versions of CFIR. The initial one was introduced in 2009 [3]. In 2006, the author surveyed CFIR users’ experiences and subsequently released a second version in 2022 [6, 20]. Version 1 focuses on influencing factors, while version 2 includes processes and implementation roles. Since version 1 is more aligned with our paper, we made the following comparison with CFIR 1. (The CFIR mentioned below refers to CFIR version 1.)
The CFIR framework consists of five domains: intervention characteristics, inner setting, outer setting, individual characteristics, and process. Each domain contains 4 to 12 constructs, for a total of 26 constructs in the framework. To provide more details, the author divides some constructs into several subconstructs. However, this classification may confuse users, as it obscures the difference between constructs and subconstructs. This makes consistent analysis challenging because sometimes certain subconstructs are significant enough to be considered independent constructs. For instance, Guerrier et al. used the CFIR as theoretical framework in their study and treated “implementation climate,” “tension for change,” “compatibility,” “relative priority,” “organizational incentives and rewards,” “goals and feedback,” and “learning climate” as independent constructs for coding. However, according to the CFIR, the latter six are actually subconstructs under “implementation climate” [16].
Additionally, CFIR includes some similar concepts that appear in different domains. For example, “resource” is a subconstruct under the “readiness” construct in the inner setting, and it also appears in the “patient and resource” construct in the outer setting. In this study, we adopted a more detailed classification, to more accurately capture the unique aspects and requirements of our study. Although we proposed more themes (10 themes vs. 5 domains) in our article, the classification hierarchy consists only of themes and factors, making it relatively straightforward.
Although the CFIR provides a comprehensive framework for analyzing the implementation of interventions in the health care field, it may be difficult to apply in a prehospital setting. There are numerous stakeholders within EMS systems, including EMS clinicians, EMS agencies, hospitals, health care practitioners in the hospital, and patients. The interactions between these stakeholders are complicated, making it challenging to classify them strictly as inner or outer settings. In CFIR, communication is named as “cosmopolitanism” in the outer setting and “network and communication” in the inner setting. In our classification, we separated communication and collaboration into a distinct category to emphasize the importance of communication in EMS and highlight the impact of different roles.
Some influencing factors mentioned in CFIR, while reasonable, are not particularly important in the context of EMS. For instance, “intervention source,” which refers to whether the intervention is developed internally or externally, is a construct under the “intervention characteristics” domain. In prehospital care, both general protocols and specific interventions are typically managed by a competent authority rather than being developed and promoted internally. As a result, this construct has little impact on the EMS setting. Another example is “peer pressure,” which CFIR classifies under the “outer setting” domain. This refers to whether other competing organizations or peers have already started implementing the intervention. Since EMS systems are usually public national units with a limited number of competitors, the EMS systems in different countries or regions do not often interact and have distinct operational backgrounds, resulting in fewer comparisons. In our study, we also used the label “peer pressure,” but we classified it under the inner setting, emphasizing competition among practitioners.
Under the “intervention characteristics” domain of CFIR, there are eight constructs: intervention source, evidence strength and quality, relative advantage, adaptability, trialability, complexity, design quality and packaging, and cost. In our study, in the “intervention characteristics” theme, we removed the “intervention source” due to the aforementioned reason and retained the remaining seven constructs. Furthermore, we also identified additional factors specific to EMS. “Cognitive aids,” such as toolkits or checklists, assist practitioners in reducing cognitive load during implementation. Another notable factor is “standardization.” Several articles have mentioned the need for a unified protocol to guide practitioners on what actions are permissible. As some interventions are unsuitable for prehospital environments, “feasibility” is a key consideration. For instance, if a triage scale requires blood test results, it is not suitable for prehospital use. Another important factor not mentioned in the CFIR is adverse effects. Beyond medication side effects, extended transport time can also reduce EMS clinicians' willingness to implement interventions. Additionally, due to the limited time in prehospital settings, the presence of competing tasks (“Priority”) and the degree to which new interventions integrate into the existing workflow (“Compatibility”) can significantly impact implementation.
In CFIR, the “process” domain includes “planning,” “engaging,” “executing,” and “reflecting and evaluating.” In our study, we did not consider the process as an influencing factor. Instead, we framed the implementation process as the core structure, divided into pre-implementation, implementation, and sustainment phases. Our diagram illustrates how each theme impacts different phases of the implementation process.
Factors related to EMS implementation
“Resources” is the theme mentioned in every article. Specifically, training/education is mentioned in 17 articles, while equipment/tools are mentioned in 13 articles. This highlights the pivotal role of a well-designed training program for successful implementation in EMS. Providing necessary and effective equipment is also crucial for program implementation.
The “intervention characteristics” theme is mentioned in every article. Given that EMS practitioners work in a resource- and time-limited environment, an overly complex or infeasible intervention for the prehospital setting may hinder their willingness to execute it. Interventions must be adaptable to the limited resources available in prehospital settings. For example, medications that can be administered intramuscularly are easier to implement than those requiring intravenous administration. Establishing standard protocols and ensuring that practitioners have access to these protocols are both important.
Due to the involvement of multiple entities within the EMS system, communication and collaboration among these entities profoundly influence implementation. Among them, communication with hospitals is particularly emphasized, as most patients are ultimately transferred to the hospital. It includes feedback, support from medical directors, data collection, interaction, mutual understanding between EMS personnel and health care professionals, and the continuum of care. Effective communication with medical facilities and the willingness of hospital medical staff to embrace new interventions could significantly impact the implementation process.
LIMITATIONS
There are several limitations to this study. First, we excluded the studies that collected data by multiple-choice questions or questionnaires, as closed-ended surveys may potentially limit data collection and synthesis. However, this approach might overlook some potential influencing factors and their weights and proportions. Second, we only synthesized and categorized the mentioned influencing factors. Whether each factor is repeatedly mentioned or emphasized in the original article is not reflected in our paper.
CONCLUSIONS
In this study, we examined the existing literature and synthesized and categorized the factors influencing EMS implementation. We also proposed a model framework for EMS implementation. This framework includes 10 themes, each impacting different stages of implementation. The most frequently mentioned among the 46 factors identified are training/education, equipment/tools, communication and collaboration with hospitals, and practitioners' attitudes/views/beliefs. These research findings provide crucial insights for the implementation of protocols and establish a groundwork for future studies of implementation science within the EMS field.
ACKNOWLEDGEMENTS: Not applicable
DECLARATION OF INTEREST STATEMENT: The article was supported by the Taiwan National Science and Technology Council (MOST 111-2628-H-002-011-MY3) and Far Eastern Memorial Hospital (FEMH-2023-C-048). This funding source had no role in study design and execution, data analyses and interpretation, and decision to submit results.
DECLARATION OF GENERATIVE AI IN SCIENTIFIC WRITING: The authors did not use a generative artificial intelligence (AI) tool or service to assist with preparation or editing of this work. The author(s) take full responsibility for the content of this publication.
Funding Sources: The article was supported by the Taiwan National Science and Technology Council (MOST 111-2628-H-002-011-MY3) and Far Eastern Memorial Hospital (FEMH-2023-C-048). This funding source had no role in study design and execution, data analyses and interpretation, and decision to submit results.
Disclosure statement: The authors report there are no competing interests to declare.
Table 1: Summary of included studies
Table 2: The influencing factors in prehospital implementation
Figure 1: PRISMA diagram of study selection
Figure 1 footnotes: * Irrelevant outcome indicated the statement of implementation process, the effectiveness of the implemented intervention rather than the influencing factor. ** Studies collect data by questionnaire were excluded.*** Two articles were written by the same first author using the same database, and were analysed from different perspectives. These two articles were count in one.
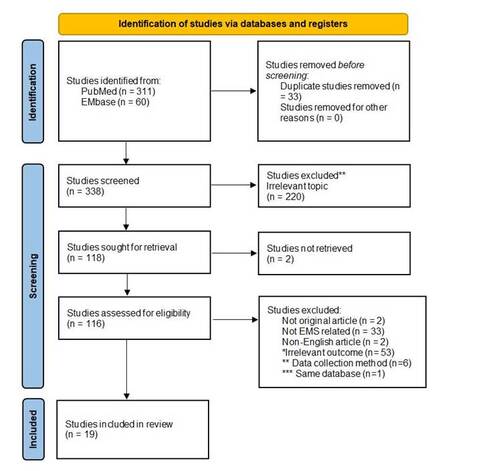
Figure 2: The framework for implementation in EMS
REFERENCES
- Eccles, M.P. and B.S. Mittman, Welcome to Implementation Science. Implementation Science, 2006. 1(1): p. 1.
- Wensing, M., Implementation science in healthcare: Introduction and perspective. Z Evid Fortbild Qual Gesundhwes, 2015. 109(2): p. 97-102.
- Damschroder, L., et al., Fostering Implementation of Health Services Research Findings into Practice: A Consolidated Framework for Advancing Implementation Science. Implementation science: IS, 2009. 4: p. 50.
- Rasool, A., et al., Policy implementation strategies to address rural disparities in access to care for stroke patients. Front Health Serv, 2023. 3: p. 1280250.
- Joiner, A., et al., Barriers and facilitators for developing a prehospital emergency care system evaluation tool (PEC-SET) for low-resource settings: a qualitative analysis. BMJ Open, 2023. 13(12): p. e077378.
- Damschroder, L.J., et al., The updated Consolidated Framework for Implementation Research based on user feedback. Implement Sci, 2022. 17(1): p. 75.
- McManus, K., et al., Implementing Oral Systemic Corticosteroids for Pediatric Asthma into EMS Treatment Guidelines: A Qualitative Study. Prehosp Emerg Care, 2022: p. 1-7.
- Sasson, C., et al., A qualitative study to identify barriers to local implementation of prehospital termination of resuscitation protocols. Circ Cardiovasc Qual Outcomes, 2009. 2(4): p. 361-8.
- Sasson, C., et al., A qualitative study to understand barriers to implementation of national guidelines for prehospital termination of unsuccessful resuscitation efforts. Prehosp Emerg Care, 2010. 14(2): p. 250-8.
- Dixon, J., et al., Using the South African Triage Scale for prehospital triage: a qualitative study. BMC Emerg Med, 2021. 21(1): p. 125.
- Curtis, K., et al., Implementation evaluation of pre-hospital blood collection in regional Australia: a mixed methods study. Australas Emerg Care, 2021. 24(4): p. 255-263.
- Carey, J.M., et al., Paramedic-Identified Enablers of and Barriers to Pediatric Seizure Management: A Multicenter, Qualitative Study. Prehosp Emerg Care, 2019. 23(6): p. 870-881.
- McCaul, M., L. Hendricks, and R. Naidoo, Prehospital providers' perspectives for clinical practice guideline implementation and dissemination: Strengthening guideline uptake in South Africa. PLoS One, 2019. 14(7): p. e0219761.
- Porter, A., et al., Implementation and use of computerised clinical decision support (CCDS) in emergency pre-hospital care: a qualitative study of paramedic views and experience using Strong Structuration Theory. Implement Sci, 2018. 13(1): p. 91.
- Bigham, B.L., et al., Knowledge translation in emergency medical services: a qualitative survey of barriers to guideline implementation. Resuscitation, 2010. 81(7): p. 836-40.
- Guerrier, C., et al., Emergency Medical Services Leadership Perspectives on Implementation of Evidence-Based Guidelines: A Qualitative Study. Prehosp Emerg Care, 2022: p. 1-9.
- Carter, A.J.E., et al., Essential Elements to Implementing a Paramedic Palliative Model of Care: An Application of the Consolidated Framework for Implementation Research. J Palliat Med, 2022. 25(9): p. 1345-1354.
- Lynch, A., S. Sobuwa, and N. Castle, Barriers to the implementation of prehospital thrombolysis in the treatment of ST-segment elevation myocardial infarction in South Africa: An exploratory inquiry. Afr J Emerg Med, 2020. 10(4): p. 243-248.
- Fishe, J.N., et al., Implementing Prehospital Evidence-Based Guidelines: A Systematic Literature Review. Prehosp Emerg Care, 2018. 22(4): p. 511-519.
- Kirk, M.A., et al., A systematic review of the use of the Consolidated Framework for Implementation Research. Implementation Science, 2016. 11(1): p. 72.
