
Abstract
The aim of this study is to develop a model describing the interactions and interdependence between the obstacles to effective implementation of a collaborative model of pandemic preparedness and response. A comprehensive review of the relevant literature highlighted 15 key variables. The contextual interactions between these barrier variables were identified based on the opinions of experts with COVID-19 pandemic experience and analyzed to determine their driving and dependence powers using interpretive structural modeling. The findings indicate that the lack of guidelines and procedures for coordinated actions, differences in organizational culture (working habits) and funding constraints are the most critical barriers to effective multi-stakeholder collaboration. Managers of collaborative programmes, policymakers and researchers should carefully focus on these hindrances because any improvement in them can significantly affect the overall system.
1. Introduction
The recent coronavirus pandemic event has aptly demonstrated the intricate interconnectedness and interdependence of humans globally. This global crisis is a reminder of the shared vulnerability of people and of the need for countries to pursue a multi-sectoral collaboration for the planning and coordination of an effective response to pandemics (McClelland Citation2017). One trend involves the increased cooperation between various actors such as policymakers, public health workers, civil society organizations, private sector, veterinarians, academics, and religious and community leaders to build community resilience for withstanding and recovering from the pandemic situation. This approach is often referred to as collaborative health emergency preparedness (Shoaf et al. Citation2014). Any effective preparation and response strategy for the COVID-19 pandemic requires a committed political will (Nkengasong and Mankoula Citation2020), and multi-sector organizations need to collaborate to boost the national pandemic preparedness and response capability.
Lasker, Weiss, and Miller (Citation2001), Green and Johnson (Citation2015) contend that collaboration is highly effective in achieving health outcomes. Nonetheless, collaboration has a high potential to fail when leadership challenges are present (Bauer, AbouAssi, and Johnston Citation2020) and resources are minimal, as is the case in many parts of Africa (Okwen et al. Citation2018). The process of exploring collaboration in many African contexts can be frustratingly slow and ineffective due to the aforementioned barriers. Recent works (e.g., Cruz Citation2014; Bennett and Carney Citation2011; Bevc et al. Citation2014; Goering et al. Citation2003; Mac McCullough, Eisen-Cohen, and Lott Citation2020; Swaan et al. Citation2018; Paige et al. Citation2010; Bevc et al. Citation2014; Nick et al. Citation2009; Santibañez et al. Citation2017; Pratt et al. Citation2018) have extensively identified the common barriers to successful multi-stakeholder collaboration in the public health emergency context. Nonetheless, most of these studies have highlighted restrictions without examining their contextual relationships or degree of influence on one another. Understanding the interactions among the different barriers can help policymakers to develop pandemic preparedness strategies and consequently strengthen their response capabilities in different pandemic scenarios. Several studies have identified common generic obstacles to effective collaboration in health emergencies and pandemic situations; however, the effects of those barriers in developed and developing countries differ.
Multiple studies on the obstacles to effective collaboration have focused on the milieu of developed countries; for example, Pollack, Amin, and Talan (Citation2012) concentrated on the United States, whereas Hansson et al. (Citation2018) emphasized Sweden. Developed-country contexts are quite different from developing ones, and they have been relatively under-researched by academic scholars who have published in top journals, particularly in the areas of examining the barriers to effective collaboration in health emergencies and pandemic situations. Therefore, empirical work needs to address this gap in the literature.
Developing countries, especially the ones in Sub-Saharan Africa (SSA), encounter unique challenges in their capacity to develop practical response actions toward the COVID-19 crisis. Loembé et al. (Citation2020) suggested that Africa could become the next epicenter of the pandemic because of the current trends in incidence and underlying vulnerabilities in healthcare systems. As the pandemic transitions continue to intensify in the continent, and a multi-stakeholder collaboration is considered essential to effectively respond to such situations (Schwartz and Yen Citation2017), increasing the contextual understanding of the barriers and their interaction with each other is a critical step for healthcare leaders and policymakers. Knowledge of the obstacles is crucial as these hindrances could prevent different actors from the public and private sectors as well as civil society and non-governmental organizations (NGOs) from collaborating on the effective preparation and response to the COVID-19 pandemic and planning for future health emergencies.
The interpretive structural modeling (ISM) technique helps to “impose order and direction on the complexity of the relationships among the variables of a system” (Janssen et al. Citation2018:648). Given the importance of making sense of the complicated contextual realities of most of Africa (e.g., weak institutions, limited infrastructure and huge informal sector), which could affect the ability of key stakeholders to collaborate in their bid to address health emergencies such as the pandemic in Africa, ISM is well suited to help structure the current research. Therefore, the aim of this research is to adopt ISM to develop a theory detailing the barriers to effective multi-stakeholder collaboration in pandemic preparedness and response. The following research question is consequently formulated and addressed: Which factors act as barriers to successful collaborative work between multiple stakeholders in response to the COVID-19 pandemic, and how are they related to each other from an SSA perspective? First, 15 different barriers were identified in this study through a literature review. The contextual interactions among these barriers were subsequently analyzed from the perspectives of experts from four SSA countries (i.e., Nigeria, Kenya, Cameroon and Zambia) that represent three major regions of the African continent (west, east and southern regions). Group discussions were used as the data collection method. The experts included members of the multi-stakeholder COVID-19 Task Force that works toward preparedness and response to the coronavirus pandemic.
The ISM approach utilized in this research was informed by professional views (Janssen et al. Citation2018; Khan et al. Citation2020); it was adopted because “it helps to transform unclear and poorly articulated mental models of systems into visible, well-defined models” (Sushil Citation2012:87). Through this approach, we determined that the driving and dependence powers of the obstacles would merit attention.
The findings of this study are expected to provide policymakers and healthcare professionals with new insights and guidance for ensuring successful collaborations in future cases of pandemic response preparation. The contribution of this research is twofold. First, it is one of the first studies to analyze the interactions of barriers to collaborative working in the crisis management of public health emergencies. Through the developed ISM-based model, the study helps to enhance the understanding of the specific barriers that require focus and attention in a future collaboration model of public preparedness for a pandemic.
Second, the research contributes to the literature by addressing the observation that in uncertain and rapidly changing situations, “outbreaks demand a multi-sectoral preparedness and response that is challenging for healthcare institutions [to effectively coordinate and manage]” (de Vries et al. Citation2019:52). By boosting the understanding of contextual interactions among the barriers, policymakers can develop interventions to strengthen intersectoral collaboration in public health emergency preparedness, particularly in developing countries.
2. Literature review
The literature review comprises two sections. The first section deals with stakeholder theory as the point of departure in this study. The second section presents a review of the literature on the barriers to a multi-stakeholder collaboration for pandemic (and other health emergencies) preparedness and response.
2.1. Stakeholder theory
Stakeholders have been defined in various ways. They may pertain to “any group or individual who can affect or is affected by the achievement of the organization’s objectives” (Freeman Citation1984:46). Stakeholders are also depicted as “all parties who will be affected by or will affect the organization’s strategy” (Nutt and Backoff Citation1993:439). Furthermore, a stakeholder may refer to “any person group or organization that can place a claim on the organization’s attention, resources, or output, or is affected by that output” (Bryson Citation2004). Stakeholders are also those “individuals or groups who depend on the organization to fulfill their own goals and on whom, in turn, the organization depends” (Johnson and Scholes Citation2002:206). All these definitions of stakeholders portray the interdependence of the firm and these entities.
Stakeholder theory has its roots in the work of Edward Freeman (Citation1984). The theory states that the choices of an organization are influenced by the desires and perceptions of multiple stakeholders (Kannan Citation2018). Therefore, organizations should create value for all stakeholders, not merely for investors or shareholders. Stakeholder theory has been widely used in different research areas, including the examination of sustainable shipping barriers (Yuen et al. Citation2017), nature of inter-organizations in social partnerships (Savage et al. Citation2010: Leach, Pelkey, and Sabatier Citation2002), stakeholder management strategies in supply chain collaboration (Co and Barro Citation2009) and university–industry collaboration (Abidin et al. Citation2016).
van der Wal (Citation2020) recently identified three essential competencies for public managers during a pandemic, namely managing stakeholders, dealing with political masters and engaging in collaborative networks. Beech and Anseel (Citation2020) highlighted the importance of developing partnerships with multiple stakeholders to succeed during a pandemic. However, research using stakeholder theory to examine collaboration in responding to global pandemics and other public health emergencies such as the COVID-19 crisis is scarce. Stakeholder theory is particularly suitable for exploring collaboration in crisis situations such as pandemics because it allows the interests of diverse stakeholders to be suppoted. We define multi-stakeholder partnership (alliance) in this context as the interactive process in which stakeholders or actors from different sectors or industries and with varied opinions team up to collectively plan and implement actions and share resources and risks with responsibility for an effective pandemic response (Wood and Gray Citation1991; Gray and Stites Citation2013; Ayala-Orozco et al. Citation2018).
In this study, we focus on multi-stakeholder collaborative initiatives for responding to the COVID-19 crisis across four African countries, as well as the obstacles to the effectiveness of such collective work. Stakeholder theory is appropriate in our study because it allows us to explore the stakeholders’ experiences with the 15 barriers (listed in ) and to examine the contextual interactions between these barriers regarding a collaborative response to the coronavirus pandemic.
Table 1. Identification and classification of barriers to successful collaboration.
Collaborative organizations are increasingly viewed as an effective means of tackling complex health challenges; however, research has underscored the significant difficulty of leveraging the diverse knowledge and skills of members from different industry sectors to address local healthcare problems (Hearld and Alexander Citation2020). Such difficulty is perhaps due to the prevalent belief that only the clinicians in health organizations have answers to healthcare problems. By contrast, less importance is given to non-clinical stakeholders in the health system. Alliance members are more likely to see their cooperation as sustainable when they have a common goal and notice that the collaboration worked in the past (D’Aunno, Hearld, and Alexander Citation2019). For politicians to work together with NGOs, as well as for the private sector and other healthcare stakeholders to deliver effective pandemic preparedness and response, they need to be conscious of the factors that impede successful collaborative work. Collaboration between stakeholders from different industry sectors can create mutual competitive advantage and value (Cao and Zhang Citation2011). However, the constituent members may also have competing self-interests. Hence, leaders who champion diverse stakeholder collaboration require an understanding of the complexities of balancing personal and group interests to achieve sustainable outcomes from multi-sector healthcare alliances (Hearld and Alexander Citation2020).
In this study, we aim to improve our understanding of the factors that constrain successful collaborative preparedness and response to pandemics from the SSA perspective. Specifically, we analyze in more detail the relational influence and interdependence among different barriers and highlight the important areas of focus for achieving effective collaboration in response to pandemics and other public health emergencies.
2.2. Barriers to successful collaboration in the health emergency context
Partnership in health emergency preparedness and response situations tend to be ineffective when concerns about the ownership of results and differences in organizational culture and working practices emerge (Dunlop et al. Citation2016; Ryu and Johansen Citation2017). Furthermore, collaborative efforts typically do not yield the expected outcomes without any clarity about the roles and responsibilities of the partners (de Vries et al. Citation2019). Shoaf et al. (Citation2014) explored the factors influencing collaborative efforts for emergency preparedness between local health departments and school districts in the US. They revealed that the lack of direction from the leadership, staff pressurized for additional commitment (overwork) and perceived loss of individual organization autonomy inhibit collaborative preparedness efforts. In a study examining cross-border health governance between institutions in the US and Mexico, Cruz (Citation2014) identified several challenges to collaboration. These challenges include legal impediments between the representatives of the two countries, the cumbersome task of accessing information, the overlap and duplication of inter-agency coordination, insufficient funding, mistrust and misalignment of interests.
Santibañez et al. (Citation2017) identified fluctuating healthcare funding priorities as a critical barrier to engaging community and faith-based organizations in responding to the Zika virus epidemic. In the same manner, matters relating to resource limitation, unethical priority setting and less confidence in the adopted surveillance technology were identified as issues requiring strategic legal intervention to ensure effective pandemic preparedness in Asia (Bennett and Carney Citation2011). Using available resources in the most efficient and equitable way is an essential consideration for countries seeking to meet the enormous financial requirements to respond to the coronavirus crisis. Additionally, the importance of strong coordination and leadership in achieving this goal in a collaborative activity cannot be overemphasized (Sullivan, Williams, and Jeffares Citation2012). However, similar to the observation of Mays and Scutchfield (Citation2010), a leader’s inability to equitably incentivise team members and high opportunity costs affect collaboration performance. This result is linked to the finding that managers struggle to make effective decisions when responding to the slow-growing incident because of the lack of clarity in information transferred between collaborating agencies and gaps in awareness of the chain of command (Dalnoki-Veress, McKallagat, and Klebesadal Citation2014).
In attempting to improve response services to public health preparedness planning, Bevc et al. (Citation2014) conducted a multilevel evaluation study on the North Carolina preparedness and emergency response. The primary concerns identified include the lack of resources to train partners, high turnover of staff, potential disconnects between planning priorities and the evidence-based vulnerability risk population, inadequate directive (guidance) and variation in the planning process. However, earlier research conducted in Ontario, Canada by Goering et al. (Citation2003) recognized some of the drawbacks of the initiatives for promoting collaboration between a research unit and the mental health policy office. The issues constituting implicit or explicit obstacles to effective linkage in policy development processes include the partners’ lack of commitment and loyalty, non-supportive collaborative environment, absence of clarity about mutual expectations, nonexistence of a quality control mechanism, absence of shared decision-making, informal interactive style of communication and limited resource commitment over time. Even though this article was published years ago, the evidence remains relevant for evaluating potential barriers to successful collaboration in preparing for a public health emergency.
In addition to the issues concerning communication, data sharing and constrained or lack of prioritization of resources, several barriers relate to divergent organizational cultures and priorities of the collaborating entities (Pratt et al. Citation2018; Christensen and Laegreid Citation2020), which reflect in the multiple stakeholders’ experience with collaboration in healthcare emergency response. Drawing lessons from the Hurricane Katrina event, Koliba, Mills, and Zia (Citation2011) developed a model for analyzing complex accountability challenges in collaborative networks. Their study highlighted some factors that constituted challenges to emergency management planners, such as a breakdown in administrative accountability and prevalent confusion over tradeoffs between different types of liabilities emanating from emergencies. Similarly, the lessons derived from Ebola preparedness in the Netherlands have indicated the need for coordination and collaboration in response planning and execution (Swaan et al. Citation2018). The study evaluated the experiences of stakeholders from the public health and the curative sectors while identifying opportunities for improving preparedness practices. The findings implied that the lack of guidelines or blueprints for regional and national coordinated preparedness actions can delay patient management in emerging infectious diseases.
Meanwhile, Lai (Citation2012) used learning network theory to demonstrate the factors that influence the success of collaboration in fighting pandemic crises in the Asia-Pacific region. They concluded that learning networks predict the effectiveness of mobilization and swift response, but the lack of networking capabilities may be viewed as a weakness for collaboration effectiveness. Networking capability is indeed critical to achieving success in collaborative projects; nonetheless, failures in leadership style, information transfer and communication are underscored in a wide range of literature. For example, in attempting to identify gaps in pandemic influenza response plan and explore opportunities to improve future preparedness for healthcare delivery, Paige et al. (Citation2010) identified three key barriers. These barriers include the absence of clarity in the governance and decision-making structure around surveillance and case reporting, lack of communication, inconsistencies of procedures and legal issues.
With regard to facilitating the emergency response for vulnerable populations (e.g., people with special healthcare needs), Nick et al. (Citation2009) underscored significant concerns relating to the lack of regular consultation with public health officials, poor coordination among emergency medical services, inability to locate vulnerable populations and a gap in the integration of data into broader, region- or nationwide emergency planning. However, a surprising aspect is that similar issues remain to date, as recent evidence (e.g., Mac McCullough et al. Citation2020) revealed that people’s propensity to share information is restricted by raised expectations about the benefits of collaboration, resource slack or low availability of resources, absence of trust and members’ self-interest.
Fifteen barriers were recognized from the preceding literature discussion and summarized in ; hence, they address the first research objective of this study. Notably, these barriers were reported in prior research in the general context of health emergency preparedness and response. Some of these barriers may possibly be more important for responding to the COVID-19 pandemic than the broader context of a health emergency. Further analysis of the barriers is therefore necessary.
To our knowledge, this work is the first study to analyze the relationships and interdependence of barriers to a multi-stakeholder collaborative approach to pandemic preparedness and response. Such research is urgently required to contribute to knowledge and literature on the critical obstacles that inhibit the use of collaboration for effectively responding to pandemics and other public health emergencies. The establishment of the interactions and interdependence of these barriers is also necessary. Thus, the aim of this research is to identify and examine the mutual influences of the different obstacles to a multi-stakeholder collaborative response to the COVID-19 pandemic. The key barriers to collaboration are identified in previous studies and subsequently evaluated using expert feedback, thereby improving the understanding of the contextual interactions of the identified barriers.
3. Methodology
3.1. ISM methodology: Analyzing the contextual relationships among the barriers
The second research objective of this study is to determine the contextual relationships among the barriers listed in , in such a way that we can ascertain their dominance in the implementation of a collaborative model of pandemic preparedness and response. This objective is addressed using the well-established ISM methodology, a technique developed by Warfield (Citation1974) and Sage (Citation1977). ISM is a decision-making tool in which a set of variables is evaluated and modified into a more manageable, straightforward and meaningful framework. Through the ISM method, researchers can impose order on the complexity of variables and present them in a structured manner (Cherrafi et al. Citation2017; Jharkharia and Shankar Citation2005). Researchers have used the concept of ISM for analyzing the interactions among variables in implementing total quality management (Talib, Rahman, and Qureshi Citation2011), green supply chain management (Mathiyazhagan et al. Citation2013), lean manufacturing practices (Cherrafi et al. Citation2017; Vasanthakumar, Vinodh, and Ramesh Citation2016) and success factors in the apparel supply chain (Chowdhury et al. Citation2020).
However, to our knowledge, this method is apparently not being employed in the analysis of the barriers to collaborations for healthcare emergency preparedness. According to Vinodh, Ramesh, and Arun (Citation2016), ISM is useful for constructing a multilevel structural model to emphasize the dominant factors that affect the implementation of a system. Such is the case with the various barriers to the success of collaboration in pandemic preparedness and response. The attributes of the ISM method include the application of experts’ practical knowledge and judgements to analytically review and revise a set of variables (Thakkar et al. Citation2005). A series of distinct steps of the ISM application in the current study is presented in ; these steps are later discussed in more detail (Cherrafi et al. Citation2017; Vinodh et al. Citation2016).
Figure 1. Stages of the application of the ISM methodology.
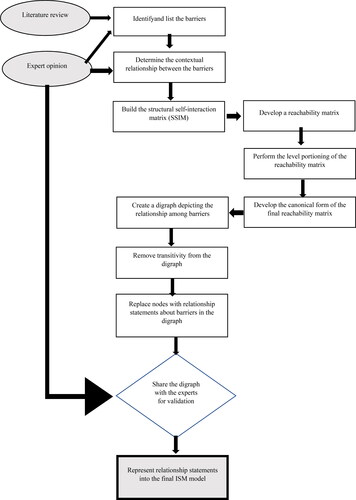
Step 1: Identify the variables under consideration in the study. In this paper, the barriers to the implementation of successful collaboration in healthcare preparedness and response were identified with the aid of a literature review and brainstorming sessions involving experts and academics.
Step 2: Establish the contextual association among the identified variables. The contextual relationships among the barriers (identified in Step 1) were established through the continuous appraisal of the team of experts.
Step 3: Create the structural self-interaction matrix (SSIM) that implies pairwise relationships among the barriers to collaboration success (from Step 2).
Step 4: Develop an initial reachability matrix from the SSIM matrix and check the transitivity. The results of this process are used for conducting the level partitioning of the barriers (obtained from Step 3) to determine the reachability and antecedent sets.
Step 5: Develop the final reachability matrix after applying the transitivity rule. The rule of transitivity suggests that if barrier A is related to barrier B and barrier B is related to barrier C, then barrier A is certainly related to barrier C.
Step 6: Formulate the various levels of the partition table from the final reachability matrix.
Step 7: Create a digraph that completely depicts the relationships among the barrier variables assigned in the final reachability matrix, and then remove the transitivity links.
Step 8: Develop the ISM-based model by replacing variable nodes with statements. The MICMAC analysis is also used at this stage to group the various barriers involved in the categories (i.e., driving variables, dependence variables, autonomous variables and linkage variables).
Step 9: Review the ISM model developed in Step 8 to check for inconsistencies and make the necessary adjustments.
3.2. Data collection
To analyze the identified 15 barriers to effective collaborative preparedness for health emergencies (see ), 32 experts from four SSA countries were initially contacted through emails and phone calls. These communication modes allowed us to discuss the study objectives with potential participants and to solicit their interest. After regular correspondences with the selected experts, 10 accepted our invitation to participate in the study. We also contacted three academics who volunteered to participate in this investigation. A decision team of 13 members was subsequently formed to further examine the barriers to successful collaboration in preparedness and response to a public health emergency (i.e., pandemic). The team consisted of two public health policymakers, two clinicians (a doctor and a nurse), two senior managers of NGOs, two officers from security services, one supplier of health products, two university professors specializing in public health and two researchers specializing in stakeholder collaboration. All the expert panel members were part of the COVID-19 Task Force in their respective African countries (i.e., a multi-stakeholder platform that works toward preparedness and response to the coronavirus pandemic). One of the key challenges encountered in this study concerned the identification and persuasion of these experts to spend their valuable time in participating in the research. Hence, this process took over three months to implement (i.e., from April to June 2020). Brief profiles of the selected experts are provided in .
Table 2. Profiles of the selected experts.
The ISM methodology requires the opinion and judgment of experts to establish the contextual relationships between factors previously identified in the literature. The experts, who are usually assembled in a small group to build contextual relationships, utilize focus group discussion methods (Shukla, Todorov, and Kapletia Citation2018). The results of the literature survey revealed that most studies adopting the ISM approach use a small group of experts (ranging from two to 13) from the industry and the academia for developing the contextual relationships (e.g., Chowdhury et al. Citation2020; Haleem et al. Citation2012; Purohit et al. Citation2016; Cherrafi et al. Citation2017; Panahifar, Byrne, and Heavey Citation2015; Mathiyazhagan et al. Citation2013). Therefore, our team of experts was considered appropriate for this study and adequate for building the proposed ISM model.
We sequentially organized two meetings with a team of experts to identify the contextual relationships among the variables (see ) considered to be barriers to successful collaboration in pandemic preparedness and response. The meetings occurred virtually via a free online conferencing tool (i.e., Zoom). Cherrafi et al. (Citation2017) have recommended this two-stage approach as one that supports the robust process of developing an ISM model. In the first meeting, experts were required to accomplish two activities. First, they needed to quantify the importance of the 15 barriers identified through the literature review on a low–moderate–high scale. Second, they needed to describe how these barriers had been encountered in the reality of the COVID-19 pandemic. The results of this initial evaluation are presented in .
Table 3. Experience of the barriers in the context of the COVID-19 pandemic.
A second meeting was convened to enable the team of experts to assess and discuss the barriers in more detail and to ascertain the contextual relationships among them. The experts were asked to indicate whether one barrier leads to another and if so, in what way. From this process, the contextual relationships among the barriers to successful collaboration in pandemic preparedness and response were developed.
3.3. Structural self-interaction matrix development
After the establishment of the “leads to” type of contextual relationship, the next phase involved the development of an SSIM to reveal the pairwise interactions between two barrier variables (i and j). Instead of the generic binary rating scale, this research employed a differential rating scale proposed by Sushil (Citation2012) to estimate the strength of the inter-relationships more precisely. Furthermore, to depict the direction of relationships, the current research adopted the color-coded differential rating scale developed by Vishnu, Sridharan, and Kumar (Citation2019). This differential rating is described in .
Table 4. Differential rating scale.
Four color codes were used to denote the direction of relationships among the barriers. Black indicates the direct link from the barrier listed in each row to the barrier in the corresponding column, whereas sandal denotes the reverse relationship; moreover, red implies a mutual relationship and blue signifies the lack of any relationships among the barriers. Based on the contextual relationship, the SSIM for the barriers to successful collaboration in pandemic preparedness and response was developed (see ).
Table 5. Structural self-interaction matrix.
3.4. Initial reachability matrix development
This stage involved the transformation of the relationship matrix into an initial reachability matrix by converting the information in each entry of SSIM into a numerical matrix (Vishnu et al. Citation2019). The initial reachability matrix was formed after substituting the alpha code with its corresponding numerical value as tabulated in . This initial reachability matrix later needed to be checked for the transitivity of the contextual relationship, which is the fundamental assumption of ISM (Cherrafi et al. Citation2017; Chowdhury et al. Citation2020). The reachability matrix also uncovered the driving and dependence powers of the barriers. The driving power of a specific barrier was computed by calculating the quantity of barriers that it could impact. The dependence power of a specific barrier was established by totaling the number of barriers through which it was influenced (Chowdhury et al. Citation2020).
3.5. Final reachability matrix
Following the development of the initial reachability matrix and the performance of the necessary adjustments, the final reachability matrix was produced using a transitivity rule (Cherrafi et al. Citation2017; Kannan et al. Citation2008). In the final reachability matrix, values with an asterisk (*) mark were entered to register transitivity and possible variations. The transitivity rule explained earlier was employed in the initial reachability matrix in to develop the final reachability matrix for the barriers to successful collaboration in pandemic preparedness and response (see ).
Table 6. Initial reachability matrix.
Table 7. Final reachability matrix.
3.6. Level partitions
The reachability and antecedent sets (Warfield Citation1974) for every barrier were uncovered from the final reachability matrix depicted in . The reachability set comprised the barrier itself and the other barriers that they might help to influence. By contrast, the antecedent set included the barrier itself and all the barriers that might influence it. The barriers common to the reachability and antecedent sets were subsequently fit into an intersection set, thereby signifying that both impacted each other. The barrier with the same reachability and intersection sets was labeled “top-level attribute” or the top-level barrier in the ISM hierarchy (Cherrafi et al. Citation2017). After its identification, the top-level barrier was removed from the other reachability, antecedent and intersection sets. The iteration was repeated until the levels of each barrier were discovered, as summarized in . The continuous procedure (i.e., iterative level partitioning) helped in creating the digraph and the final interpretative structural model. The further computation of the iteration levels for determining the levels of ISM is presented in the Supplementary material (Tables 1–4).
Table 8. Level partitions for the barriers.
3.7. Canonical form of the final reachability matrix
Finally, we developed the canonical form of the final reachability matrix by arranging the barriers in the order of their levels (see ). It was consequently used for constructing the ISM model.
Table 9. Canonical form of the final reachability matrix.
3.8. Micmac analysis
The MICMAC analysis, otherwise known as Matrice d'Impacts Croisés-Multiplication Appliquée á un Classement, was performed in this study to enhance the understanding of the degree of dependence of the barriers on one another, beyond the visual depiction of their hierarchical relationship. In other words, the MICMAC analysis helped to establish the driving and dependence powers of the barriers under study. The diagram of driving and dependence powers is illustrated in . The barriers were then classified into four categories based on their driving and dependence powers (Vinodh et al. Citation2016), namely driving barriers, dependence barriers, autonomous barriers and linkage barriers.
Figure 2. Diagram of driving power and dependence.
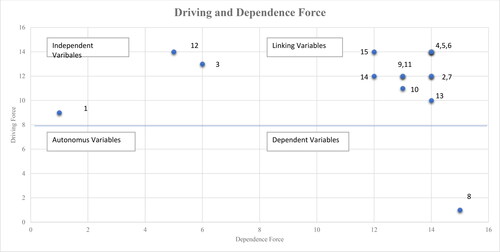
The barriers with a very weak driving force and a weak dependence force are categorized as autonomous barriers, as depicted in Quadrant I. This classification suggests that these barriers are not related to other barriers; therefore, they need to be tackled independently to achieve collaboration success. The barriers with a weak driving force but a high dependence force are categorized as dependent barriers, as presented in Quadrant II. This classification signifies that several other barriers may cause the barrier to occur. Furthermore, the barriers with a high driving force and a high dependence force are categorized as linkage barriers, as depicted in Quadrant III. These barriers have a strong and dynamic influence, implying that any intervention developed to mitigate them will also influence other barriers. Finally, Quadrant IV includes barriers with a high driving force but a low dependence force, and they are classified as independent barriers.
In summary, the dependent barriers are influenced by the independent barriers that hinder the success of collaboration in pandemic preparation and response initiatives. However, this relationship is mediated by the linkage barriers. Hence, the analysis results presented in enabled us to design a classification system for the 15 barriers to the success of collaboration in response to the COVID-19 pandemic in Africa. The classification represents an important initial step to help public leaders and policymakers (particularly those responsible for leading the multi-stakeholder response to pandemic situations) to identify the interaction of various barriers that impede the success of collaborative efforts. The ISM analysis results provide insights into the role of each barrier to help in understanding the specific types of barriers that impact or are impacted by other types.
3.9. Development of the ISM-based model
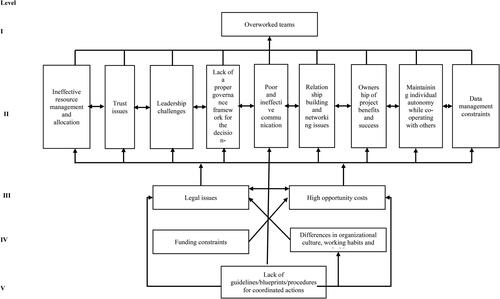
From the level partitioning of the final reachability matrix, we developed a hierarchical model; in this model, the nodes denote the barriers, and the links represent the interactions. For example, if a relationship exists between the barriers j and i, then it is depicted with an arrow pointing from i to j. The graphical model emerging from this process is referred to as a directed graph or digraph (Cherrafi et al. Citation2017; Chowdhury et al. Citation2020). After the removal of the transitivity links and the replacement of the nodes with barrier statements, the diagram was finally transformed into the ISM model. The diagram was shared with experts to validate its contents and structure (as described in ). It was consequently converted into the ISM-based model, as illustrated in .
Figure 3. ISM model for barriers.
4. Results and discussion
A collaborative model of pandemic preparedness and response involves the exchange of information and the sharing of resources and responsibilities as well as benefits between multi-stakeholder organizations. An example is the U.N. Inter-Agency Task Force that harnesses the collective resources of member states to respond to the challenges of the COVID-19 pandemic (World Health Organization, n. d). In developing countries, the joint efforts of the public and private sectors, together with civil society organizations, have been leveraged for the same purpose (Rajan et al. Citation2020). Such collaboration provides several benefits. The collaborating agencies or organizations can pool their resources and capabilities to accomplish objectives that individual entities may struggle to achieve on their own. These objectives can include increasing the recognition and visibility for the institutional stakeholders (Shoaf et al. Citation2014), raising awareness of the disease and advocating health prevention behaviors such as social distancing and hand washing. Furthermore, collaboration prevents the duplication of efforts, promotes the efficient use of resources, encourages team building and fosters a sense of ownership among members of the partnering organizations (Rinehart, Laszlo, and Briscoe Citation2001; Shoaf et al. Citation2014).
Although evidence (e.g., Mays and Scutchfield Citation2010; Green and Johnson Citation2015) has indicated that partnerships on public health issues produce improved outcomes for patients and the wider population, success is uncertain because it is often hampered by barriers. Similarly, recent media coverage of the government’s coronavirus response in African countries has focused on building partnerships between different stakeholders (Green Citation2020). Nonetheless, the lessons learned have not been widely identified, recorded and analyzed. Such a situation is the principal concern of this research. From a relational perspective, many barriers impede collaboration, such as lack of trust, absence of an effective governance structure, communication-related issues, resource limitations/capability issues and power differences (Walker et al. Citation2013). For example, institutions providing financial support for countries during the COVID-19 pandemic may have diverse priorities for managing the crisis. Frictions might arise if these NGOs attempt to coerce African public health leaders to tailor the country’s specific COVID-19 spending plans to their funder’s priorities.
The ensuing need relates to the analysis and overcoming of the barriers to successful collaboration between multiple organizations that implement joint preparedness and response activities for public health emergencies in the African context. In this regard, we reviewed the literature to identify the barriers to successful collaboration in pandemic preparedness and response and then validated those barriers using the opinions of experts. Additionally, we evaluated the contextual interaction among the barriers using the ISM technique. The results informed the development of the ISM (in ), which provides structural relationships between different barriers based on their driving power and dependence across five different levels. This study revealed that the lack of guidelines and procedures for coordinated actions (at Level V of the ISM model) is the most critical barrier to focus on because it can influence the remaining 14 barriers in direct and indirect ways. This barrier has a direct effect on the differences in organizational culture, working habits and priorities (at Level IV) as well as on the high opportunity costs and legal issues (both at Level III). Our participants further explained how these barriers interact, particularly in terms of the procurement of personal protective equipment (PPE), engagement with the private sector and issues concerning data sharing, thereby hindering successful collaboration in COVID-19 preparedness and response:
Most governments are talking about inter-agency coordination. However, a structure or a procedure to guide actions is lacking, especially with regard to working with local supply chain actors. This [factor]reduces our capacity to quickly respond because we spend time creating such templates or procedures. Some organisations we are collaborating with are not very keen on having open-access data. For example, in [tapping] the private sector to perform services such as data analysis, you look at the specific provisions that allow the public sector to invite the private sector to examine such data. (Participant 3)
Public procurement regulations restrict the freedom of collaborating partners that want to get PPE/kits from their preferred supplier, especially when there is matched funding and [a need to] follow government procurement. [However,] collaborators have their [own] interests. (Participant 7)
The initial response was like, “Let us continue to do things the way we do them by simply following that conventional option rather than saying we have products that can be distributed across the country by engaging the private sector.” It took a while for people to [realise] that they have additional resources that could be tapped. The public health supply chain system is so inflexible and challenging to the extent that people are not thinking of alternatives such as the military and other players that can be deployed to make [the management and delivery of] supplies more efficient. (Participant 8)
Therefore, the first and most crucial step in facilitating successful collaboration for pandemic preparedness and response is to develop procedures and templates for guiding the coordinated actions of multiple stakeholders. With such guidelines, members within a collaborative relationship can become proactive in managing differences in the organizational culture and reduce the potential of legal infractions and the high opportunity cost of regulatory compliance. Additionally, this approach would create the possibility to prevent the emergence of many other barriers (at Level II), including ineffective resource management and allocation, trust issues, leadership issues and lack of a proper governance framework for the decision-making process. The other obstacles are relationship-building and networking issues, poor and ineffective communication, ownership of project benefits and success, maintenance of individual autonomy while co-operating with others and data management constraints. The above-mentioned barriers have mutual relationships.
An unsurprising yet worthy point to mention is that the existential problems of leadership and resource management in Africa (Afegbua and Adejuwon Citation2012) hamper the trust and confidence of partners that provide financial support for healthcare systems in the continent. One participant’s comment reflects this premise:
An existing challenge concerns the trust from partners that support healthcare systems in Africa. When a country has a history of misuse of funds and fiscal mismanagement, [such record] continues to play out. Funders want assurance from the government on how the money for COVID-19 will be spent. Hence, donors are now selective in terms of the countries to which to channel the resources. You do not know whether you have more money to give to these countries, or if politicians will find things to divert. (Participant 1)
Furthermore, the effects of mutual interactions between the various barriers at Level II of the ISM model can result in another barrier, namely overworked teams. For example, this barrier implies that in the case where effective leadership is present to facilitate equity in resource distribution and encourage collaborators to communicate better (network, share data) to build trust, people involved in a multi-stakeholder collaboration project will feel less overworked. However, the barrier of overworked teams does not produce other obstacles. One participant substantiated this finding:
I would say people are overworked… but the impact [of this situation] on collaboration has not been reported. People often complain about being stressed, and even resources must be stretched. People must dig deeper than they normally would, but that [action] should be expected in the COVID-19 situation. (Participant 13)
Additionally, the MICMAC analysis offered useful insights into the interdependencies of the individual barriers, as illustrated in the driving force and dependence diagram (see ). The results from this analysis indicated funding constraints as the only barrier that falls under (autonomous) Quadrant I, and such barrier can be considered as disconnected from the whole system. The largest number of barriers have a low driving force and a high dependence force; dependent variables as presented in Quadrant II. The barriers include ineffective resource management and allocation, poor and ineffective communication, overworked teams, relationship-building and networking issues, ownership of project benefits and success, maintenance of individual (organizational) autonomy while co-operating with others, data management constraints, legal issues and high opportunity costs. These are weak drivers but strong dependent variables, which are influenced by other independent and linkage variables in the system.
Therefore, a challenging undertaking would be the direct eradication of these barriers, and managers of a collaborative project must find the driving factors to appropriately address them. For example, in the present scenario of a multi-stakeholder collaboration for the COVID-19 crisis, the establishment of a proper governance framework for the decision-making process with guidelines for coordinated actions and effective data management can help in tackling the challenges concerning resource allocation and an overworked team. Thus, project-related stress (team burnout) is reduced and the chances of a successful collaboration are increased.
Meanwhile, Quadrant III () includes three linkage barriers that managers must pay close attention to because of their high driving force and high dependence force. The linkage barriers include trust issues, leadership challenges and lack of a proper governance framework for the decision-making process. These significant barriers have a substantial impact on the entire ISM model because they influence and are influenced by many other factors (barriers) in the system. The linkage barriers are unstable, indicating that if they are not improved, then they will affect the different barriers in the system and thus hinder the success of the collaborative response to a pandemic situation.
As depicted in , differences in organizational culture, working habits and priorities as well as lack of guidelines, blueprints or procedures for coordinated actions have a high driving force with a low dependence force (see Quadrant IV). The two barriers in this group are denoted as independent factors because they have a strong influence over the other barriers, hence rendering them a threat to successful collaboration in pandemic preparedness and response from the perspective of health systems in Africa. Therefore, managers of the multi-stakeholder collaboration, policymakers and researchers should thoroughly focus on these barriers because any improvement in them can significantly affect the overall system.
Interestingly, our experts ranked the two independent barriers high in importance in terms of collaborative actions in response to the COVID-19 pandemic in SSA countries. Hence, our results agreed with the findings of previous studies about key factors hindering effective collaboration in the context of healthcare emergency and pandemic response. For example, the most critical barriers identified in studies conducted on the collaborative response to the Zika virus epidemic in France (Santibañez et al. Citation2017) and the management of pandemic influenza in Asia (Bennett and Carney Citation2011) included funding constraints, inefficient use of resources and differences in organizational culture.
However, other studies reported different results, particularly considering the collaboration between biomedical and complementary and alternative care providers in the Netherlands (van der Watt et al. Citation2017) and the collaboration between community mental health and juvenile justice systems in the US (Kapp et al. Citation2013). The highest-ranked barriers in these studies were distrust within and between groups and lack of informal relationships, respectively. This finding implies that significant barriers to effective collaboration are context-specific, and the obstacles that are important for a multi-stakeholder collaborative pandemic preparedness and response in SSA may not be critical hindrances for other sectors and in other countries.
4.1. Theoretical, practical and policy implications
The findings of this study have theoretical, practical and policy implications. In terms of theoretical implications, the results from our analysis show the ranking of the key barriers to successful collaboration in pandemic preparedness and response using data from developing countries, particularly the ones in SSA. Contribution to knowledge is made through the classification and description of the barriers that impede the success of a collaborative model of pandemic preparedness and response, and the ensuing interactions and interdependence that are inherent to them. In this regard, implications for practice are considered as an essential part of the theoretical conceptualisations (Walker et al. Citation2013). Hence, the ISM model developed from our findings is presented in a manner that informs both theory and practice. Appropriate mitigation strategies can be developed by unraveling the complex interactions between different barriers.
The ISM and MICMAC analyses offered useful insights into the hindrances to collaboration, drawing lessons from the preparedness and response of SSA to the COVID-19 pandemic. The lack of guidelines, blueprints or procedures for coordinated actions was found to be the most critical barrier in our study. This finding suggested that once a decision has been made to collaborate with a diverse range of stakeholders to strengthen national or regional pandemic preparedness and response, the government must establish a clear, appropriate and coherent set of procedures and rules to guide the coordinated actions. Our analysis also signified that the above-mentioned barriers constitute an independent variable with a very high driving force and a direct impact on the other barriers in the system (at Level V of the ISM model), such as poor and ineffective communication, differences in organizational culture, working habits and priorities, and overworked teams. These obstacles, coupled with legal issues and high opportunity costs, render the procurement outcomes inefficient. For example, when a decision is made to go with a funder for the procurement of PPE and testing kits, a realization later occurs regarding the alternative collaborators’ potential to offer more advantages in terms of what should have been procured. The implementations down the line consequently become unrealistic compared to the promises made. A notable solution to this problem emerged during a discussion with an expert, that is, to set aside or excuse those regulatory encumbrances to ensure a more effective response.
Differences in organizational culture, working habits and priorities constituted the second most crucial obstacle, and they were identified as another independent barrier with a high driving force on other linkage barriers. Coupled with legal issues, this barrier has a direct impact on other linkage barriers (at Level V of the ISM) such as trust issues, inadequate and ineffective communication, maintenance of individual autonomy while co-operating with others, and relationship-building and networking issues. This finding revealed the notion of collaborative inertia, which frequently relates to the challenges of inter-firm relationships, such as differences in aspirations, resource commitment and cultural experiences of the partners (Vangen and Huxham Citation2010). For example, an expert indicated that the government’s bureaucratic operational system prevents public policymakers from engaging with the private sector. Notably, some public bodies in Africa lack structures or policies for engaging the private sector in this situation.
The reduction or removal of unnecessary policies and administrative hindrances in public sector operations is therefore essential to improve the multi-stakeholder collaboration. For example, as governments prepare for the future responsibility for the COVID-19 vaccination programme, they can plan to outsource the cold chain and storage functions to third-party operators rather than relying on the underperforming (Yadav Citation2015) existing supply chain facilities for health products. As suggested by other researchers, managers often provide partnering entities with incentive packages (Esteve, Van Witteloostuijn, and Boyne Citation2015; Fuller and Vu Citation2011; Shoaf et al. Citation2014; Mays and Scutchfield Citation2010) to encourage the unrestricted flow of information and knowledge sharing in collaborative initiatives; furthermore, the expectation is that the rewarding process should be clear. Concomitantly, the sharing or exchange of information can also be facilitated by the natural networking disposition of collaborating organizations and continuance of relationships (Sweeney et al. Citation2010). These factors have been determined to contribute to organizational relational capacity (individually and collectively) in a collaborative model for pandemic preparedness.
For example, in their case study of pandemic influenza preparedness and response in Israel, Kohn et al. (Citation2010) revealed that the preexisting relational history between the partner organizations and a similarity in organizational cultures predict the success of collaborations. This crucial point should be considered in African countries when multiple stakeholders from diverse sectors and distinct backgrounds work together in responding to healthcare emergencies, as adverse actions could derail the achievement of collaborative advantage (Vangen and Huxham Citation2010). Therefore, managers and policymakers in public sector organizations need to implement an appropriate governance framework within which project decisions are made by the right people and at the right time to enhance the realization of the benefits of collaborative working (Schotanus, Telgen, and de Boer Citation2010; Walker et al. Citation2013).
5. Conclusions, limitations, and future research
In times of pandemic, multi-stakeholder collaboration initiatives have become a popular technique for strengthening the preparedness capacity of various countries. The key benefits and drivers of collaboration have become widely recognized across sectors or industries. However, the barriers encountered in a collaborative model of pandemic preparedness and responses have not been analyzed in an exhaustive manner. Scant research has been conducted in this area, particularly in developing countries such as the ones in SSA. Furthermore, the capacity to implement a successful multi-stakeholder collaborative response to public health emergencies (e.g., pandemic) in African countries has yet to be comprehensively evaluated. The challenges of high-density population, soaring incidences of infectious diseases, poor healthcare infrastructure and low GDP per capita (Umviligihozo et al. Citation2020) have prompted the need for SSA to strengthen the response to the COVID-19 crisis. As collaboration has been confirmed as an effective preparedness and response strategy for a public health emergency, it requires more attention from policymakers, managers and researchers to help improve their preparedness and response to future outbreaks.
A literature review was conducted in this study to identify the key barriers to successful collaboration for pandemic preparedness and response. The results of the literature review were shared with experts for examination, validation and finalization. We determined the perceived level of importance of these barriers based on the opinions of experts who participated in collaborative programmes for COVID-19 response in four SSA countries, namely Nigeria, Kenya, Cameroon and Zambia. These experts subsequently established the mutual interactions and degree of influence of the barriers to develop a hierarchical ISM model. The MICMAC analysis was also performed on the obstacles to categorize them in terms of driving and dependence influence (force). The findings can guide policymakers and managers who seek to promote fruitful collaboration among multiple stakeholders in responding to health emergencies or pandemic situations. They are also beneficial for researchers to deepen their insights into the contextual interactions of barriers to collaboration, which they can use for formulating propositions to help guide future research, for example in the conceptualization of stakeholder theory.
5.1. Limitations
This study has some limitations that must be addressed in future research. The ISM approach was used for developing an initial model based on data obtained from the literature and the analysis of expert opinions from four SSA countries regarding the barriers to successful collaboration in pandemic preparedness and response. Future studies should utilize a more randomized larger dataset from other African countries to minimize sample bias and improve the replicability of the findings. Furthermore, the proposed ISM model has not been empirically validated with a large sample of participants; thus, other methods should be used in future studies to further test the robustness and efficacy of the model, such as fuzzy Delphi method, fuzzy MICMAC and structural equation modeling (SEM).
Assigning a single crisp score for rating the relationship between the barriers is sometimes difficult for experts due to uncertainty or lack of complete knowledge. In this case, fuzzy methodologies may help in incorporating uncertainties. In fact, through this methodology rather than the use of a single crisp score, the experts may be asked to rate the relationship using fuzzy numbers (i.e., triangular fuzzy number, trapezoidal fuzzy number and bell-shaped fuzzy number, among others) based on a probability-based membership function. This scale can depict the relationship more realistically than single-valued numbers.
Furthermore, as ISM is an exploratory subjective model, the results may vary when new expert opinions are incorporated. However, the results of ISM provide an interesting hypothesis regarding the inter-relationships among the barriers that can be tested for statistical significance. In this direction, an extensive questionnaire-based survey can be conducted. Using the survey data, SEM can be developed and tested based on the hypothesis defined from the ISM results. Being a combination of path analysis, factor analysis and regression, such an SEM model can validate the findings of ISM and offer proof of the robustness of the results. Future research could also investigate practical solutions for addressing the barriers identified in this study.
Supplemental Material
Download MS Word (20.2 KB)Additional information
Notes on contributors
Temidayo O. Akenroye
Temidayo O. Akenroye holds a PhD from the Salford Business School, University of Salford, UK. He is a supply chain management scholar and published in leading management journals on health innovation, healthcare supply chains, public procurement, and sustainability. He is currently a Senior Lecturer at Liverpool Business School, UK.
Alim Abubakre
Alim Abubakre holds a PhD from Southampton Business School, University of Southampton, UK. His primary research focuses on stakeholder management theory, corporate social responsibility, and strategy. He is currently a lecturer at Coventry Business School, Coventry University, Coventry, UK.
Jamal Elbaz
Jamal Elbaz is an Associate Professor at Ibn Zohr University, Agadir, Morocco. He is an author and expert in logistics, SCM and operations management. His research areas cover sustainable supply chain management, corporate social responsibility, entrepreneurship, and supply chain risk management. He has published many books and papers and communicated several oral presentations in international conferences.
C. R. Vishnu
C. R. Vishnu is an Assistant Professor of Production & Operations Management at Xavier Institute of Management and Entrepreneurship (XIME) Kochi, Kerala, India. His research interests include supply chain risk management, decision making in operations management and network design for supply chains. He holds a PhD degree in Operations Management and Supply Chains and has published research papers in high-ranking scientific journals.
Jean-Noël Beka Be Nguema
Jean-Noël Beka Be Nguema is a Postdoctoral Researcher and Lecturer at School of Management, he received his PhD degree in Management Science & Engineering from University of Science and Technology of China (USTC). His research interest covers Supply Chain Finance, performance management and operation management.
Gaurav Rana
Gaurav Rana is a Director at Tourism Edu Federation and Assistant Professor at Shri Ram College of Commerce, University of Delhi. He is a recipient of the Dewang Mehta National Award for Best Professor in Strategic Management Studies.
Ugwushi Bellema Ihua
Ugwushi Bellema Ihua is the Executive Director at Africa Polling Institute (API), an independent, nonprofit and nonpartizan public opinion think-tank, which conducts opinion polls, surveys, social research and evaluation studies at the intersection of democracy, governance. He holds a PhD in Business Management from the University of Kent, UK.
Hellen Kalili
Hellen Kalili is a Senior Strategic Advisor at LiveGene, University of Leicester, UK. She was the Regional Coordinator for Africa Resource Center (ARC) - an independent strategic advisor, promoting collaboration to help countries achieve their health goals. She holds an MSc in Procurement and Supply Chain Management from the University of Salford, UK.
Oyindamola Falode
Oyindamola Falode is the Managing Director of Panda Consultant Limited, Lagos, Nigeria. She is a project management expert and has worked with governments and civil society organizations in implementing the Sustainable Development Goals in Nigeria.
References
- Abidin, I., A. A. Rani, M. R. Ab Hamid, and Y. Zainuddin. 2016. “University-Industry Collaboration, Firm Performance and Stakeholder Theory.” Selangor Business Review 1(1):51–63.
- Afegbua, S. I., and K. D. Adejuwon. 2012. “The Challenges of Leadership and Governance in Africa.” International Journal of Academic Research in Business and Social Sciences 2(9):141.
- Ayala-Orozco, B., J. A. Rosell, J. Merçon, I. Bueno, G. Alatorre-Frenk, A. Langle-Flores, and A. Lobato. 2018. “Challenges and Strategies in Place-Based Multi-Stakeholder Collaboration for Sustainability: Learning from Experiences in the Global South.” Sustainability 10(9):3217. doi: https://doi.org/10.3390/su10093217.
- Bauer, Z., K. AbouAssi, and J. Johnston. 2020. “Cross-Sector Collaboration Formality: The Effects of Institutions and Organizational Leaders.” Public Management Review, 1–23. doi: https://doi.org/10.1080/14719037.2020.1798709.
- Beech, N., and F. Anseel. 2020. “COVID‐19 and Its Impact on Management Research and Education: Threats, Opportunities and a Manifesto.” British Journal of Management 31(3):447–9. doi: https://doi.org/10.1111/1467-8551.12421.
- Bennett, B., and T. Carney. 2011. “Pandemic Preparedness in Asia: A Role for Law and Ethics?” Asia-Pacific Journal of Public Health 23(3):419–30. doi: https://doi.org/10.1177/1010539511408411.
- Bevc, C. A., M. C. Simon, T. A. Montoya, and J. A. Horney. 2014. “Institutional Facilitators and Barriers to Local Public Health Preparedness Planning for Vulnerable and at-Risk Populations.” Public Health Reports 129 Suppl 4(6):35–41. doi: https://doi.org/10.1177/00333549141296S406.
- Bryson, J. M. 2004. “What to Do When Stakeholders Matter: Stakeholder Identification and Analysis Techniques.” Public Management Review 6(1):21–53. doi: https://doi.org/10.1080/14719030410001675722.
- Burby, R. J. 2003. “Making Plans That Matter: Citizen Involvement and Government Action.” Journal of the American Planning Association 69(1):33–49. doi: https://doi.org/10.1080/01944360308976292.
- Cao, M., and Q. Zhang. 2011. “Supply Chain Collaboration: Impact on Collaborative Advantage and Firm Performance.” Journal of Operations Management 29(3):163–80. doi: https://doi.org/10.1016/j.jom.2010.12.008.
- Cherrafi, A., S. Elfezazi, J. A. Garza-Reyes, K. Benhida, and A. Mokhlis. 2017. “Barriers in Green Lean Implementation: A Combined Systematic Literature Review and Interpretive Structural Modelling Approach.” Production Planning & Control 28(10):829–42. doi: https://doi.org/10.1080/09537287.2017.1324184.
- Christensen, T., and P. Laegreid. 2020. “The Coronavirus Crisis—Crisis Communication, Meaning-Making, and Reputation Management.” International Public Management Journal, 23(5):713–29.
- Chowdhury, N. A., S. M. Ali, S. K. Paul, Z. Mahtab, and G. Kabir. 2020. “A Hierarchical Model for Critical Success Factors in Apparel Supply Chain.” Business Process Management Journal 26(7):1761–88. doi: https://doi.org/10.1108/BPMJ-08-2019-0323.
- Cicmil, S., and D. Marshall. 2005. “Insights into Collaboration at the Project Level: Complexity, Social Interaction and Procurement Mechanisms.” Building Research & Information 33(6):523–35. doi: https://doi.org/10.1080/09613210500288886.
- Co, H. C., and F. Barro. 2009. “Stakeholder Theory and Dynamics in Supply Chain Collaboration.” International Journal of Operations & Production Management 29 (6):591–611. doi: https://doi.org/10.1108/01443570910957573.
- Cruz, P. L. 2014. “Cross-Border Governance on the U.S.–Mexico Border: Institutional Challenges and Developments in Health Collaboration.” Regions and Cohesion 4(1):53–71. doi: https://doi.org/10.3167/reco.2014.040104.
- D’Aunno, T., L. Hearld, and J. A. Alexander. 2019. “Sustaining Multistakeholder Alliances.” Health Care Management Review 44(2):183–94. doi: https://doi.org/10.1097/HMR.0000000000000175.
- Dalnoki-Veress, F., C. McKallagat, and A. Klebesadal. 2014. “Local Health Department Planning for a Radiological Emergency: An Application of the AHP2 Tool to Emergency Preparedness Prioritization.” Public Health Reports 129(6_suppl4):136–44. doi: https://doi.org/10.1177/00333549141296S418.
- de Vries, M., P. Kenis, M. Kraaij-Dirkzwager, E. J. Ruitenberg, J. Raab, and A. Timen. 2019. “Collaborative Emergency Preparedness and Response to Cross-Institutional Outbreaks of Multidrug-Resistant Organisms: A Scenario-Based Approach in Two Regions of The Netherlands.” BMC Public Health 19(1):52. doi: https://doi.org/10.1186/s12889-018-6376-7.
- Dunlop, A. L., K. M. Logue, L. Vaidyanathan, and A. P. Isakov. 2016. “Facilitators and Barriers for Effective Academic-Community Collaboration for Disaster Preparedness and Response.” Journal of Public Health Management and Practice 22(3):E20–28. doi: https://doi.org/10.1097/PHH.0b013e3182205087.
- Esteve, M., A. Van Witteloostuijn, and G. Boyne. 2015. “The Effects of Public Service Motivation on Collaborative Behavior: Evidence from Three Experimental Games.” International Public Management Journal 18(2):171–89.
- Freeman, R. 1984. Strategic Management: A Stakeholder Approach. Boston: Pitman.
- Fuller, B. W., and K. M. Vu. 2011. “Exploring the Dynamics of Policy Interaction: Feedback among and Impacts from Multiple, Concurrently Applied Policy Approaches for Promoting Collaboration.” Journal of Policy Analysis and Management 30(2):359–80. doi: https://doi.org/10.1002/pam.20572.
- Goering, P., D. Butterill, N. Jacobson, and D. Sturtevant. 2003. “Linkage and Exchange at the Organizational Level: A Model of Collaboration between Research and Policy.” Journal of Health Services Research & Policy 8 Suppl 2(2):14–9. doi: https://doi.org/10.1258/135581903322405126.
- Gray, B., and J. P. Stites. 2013. Sustainability through Partnerships: Capitalising on Collaboration. London, ON, Canada: Network for Business Sustainability.
- Green, B. N., and C. D. Johnson. 2015. “Interprofessional Collaboration in Research, Education, and Clinical Practice: working Together for a Better Future.” The Journal of Chiropractic Education 29(1):1–10. doi: https://doi.org/10.7899/JCE-14-36.
- Green, D. 2020. “Is Africa Winning the War Against COVID? We Don’t Know Yet and Here’s Why.” https://medium.com/@CooperSmithOrg/is-africa-winning-the-war-against-covid-we-dont-know-yet-and-here-s-why-a38fa1dcb99d
- Haleem, A., Sushil, M. A. Qadri, and S. Kumar. 2012. “Analysis of Critical Success Factors of World-Class Manufacturing Practices: An Application of Interpretative Structural Modelling and Interpretative Ranking Process.” Production Planning and Control 23(10-11):722–34. doi: https://doi.org/10.1080/09537287.2011.642134.
- Hansson, A., A. Svensson, B. H. Ahlström, L. G. Larsson, B. Forsman, and P. Alsén. 2018. “Flawed Communications: Health Professionals' Experience of Collaboration in the Care of Frail Elderly Patients.” Scandinavian Journal of Public Health 46(7):680–9. doi: https://doi.org/10.1177/1403494817716001.
- Hearld, L. R., and J. A. Alexander. 2020. “Sustaining Participation in Multisector Health Care Alliances: The Role of Personal and Stakeholder Group Influence.” Health Care Management Review 45(3):196–206. doi: https://doi.org/10.1097/HMR.0000000000000216.
- Jharkharia, S., and R. Shankar. 2005. “IT‐Enablement of Supply Chains: Understanding the Barriers.” Journal of Enterprise Information Management 18(1):11–27. doi: https://doi.org/10.1108/17410390510571466.
- Johnson, G., and K. Scholes. 2002. Exploring Corporate Strategy. 6th ed. Harlow: Peason Education.
- Janssen, M., N. P. Rana, E. L. Slade, and Y. K. Dwivedi. 2018. “Trustworthiness of Digital Government Services: Deriving a Comprehensive Theory through Interpretive Structural Modelling.” Public Management Review 20(5):647–71. doi: https://doi.org/10.1080/14719037.2017.1305689.
- Kannan, D. 2018. “Role of Multiple Stakeholders and the Critical Success Factor Theory for the Sustainable Supplier Selection Process.” International Journal of Production Economics 195:391–418. doi: https://doi.org/10.1016/j.ijpe.2017.02.020.
- Kannan, G., A. N. Haq, P. Sasikumar, and S. Arunachalam. 2008. “Analysis and Selection of Green Suppliers Using Interpretative Structural Modelling and Analytic Hierarchy Process.” International Journal of Management and Decision Making 9(2):163–82. doi: https://doi.org/10.1504/IJMDM.2008.017198.
- Kapp, S. A., C. G. Petr, M. L. Robbins, and J. J. Choi. 2013. “Collaboration between Community Mental Health and Juvenile Justice Systems: Barriers and Facilitators.” Child and Adolescent Social Work Journal 30(6):505–17. doi: https://doi.org/10.1007/s10560-013-0300-x.
- Khan, W., A. Akhtar, S. A. Ansari, and A. Dhamija. 2020. “Enablers of Halal Food Purchase among Muslim Consumers in an Emerging Economy: An Interpretive Structural Modeling Approach.” British Food Journal 122(7):2273–87. doi: https://doi.org/10.1108/BFJ-08-2018-0528.
- Kohn, S., D. J. Barnett, A. Leventhal, S. Reznikovich, M. Oren, D. Laor, I. Grotto, and R. D. Balicer. 2010. “Pandemic Influenza Preparedness and Response in Israel: A Unique Model of Civilian-Defense Collaboration.” Journal of Public Health Policy 31(2):256–69. doi: https://doi.org/10.1057/jphp.2010.17.
- Koliba, C. J., R. M. Mills, and A. Zia. 2011. “Accountability in Governance Networks: An Assessment of Public, Private, and Nonprofit Emergency Management Practices following Hurricane Katrina.” Public Administration Review 71(2):210–20. doi: https://doi.org/10.1111/j.1540-6210.2011.02332.x.
- Lai, A. Y. 2012. “Organizational Collaborative Capacity in Fighting Pandemic Crises: A Literature Review from the Public Management Perspective.” Asia-Pacific Journal of Public Health 24(1):7–20. doi: https://doi.org/10.1177/1010539511429592.
- Lasker, R. D., E. S. Weiss, and R. Miller. 2001. “Partnership Synergy: A Practical Framework for Studying and Strengthening the Collaborative Advantage.” The Milbank Quarterly 79(2):179–205. doi: https://doi.org/10.1111/1468-0009.00203.
- Leach, W. D., N. W. Pelkey, and P. A. Sabatier. 2002. “Stakeholder Partnerships as Collaborative Policymaking: Evaluation Criteria Applied to Watershed Management in California and Washington.” Journal of Policy Analysis and Management 21(4):645–70. doi: https://doi.org/10.1002/pam.10079.
- Loembé, M. M., A. Tshangela, S. J. Salyer, J. K. Varma, A. E. O. Ouma, and J. N. Nkengasong. 2020. “COVID-19 in Africa: The Spread and Response.” Nature Medicine 26(7):999–1003.
- Mathiyazhagan, K., K. Govindan, A. NoorulHaq, and Y. Geng. 2013. “An ISM Approach for the Barrier Analysis in Implementing Green Supply Chain Management.” Journal of Cleaner Production 47:283–97. doi: https://doi.org/10.1016/j.jclepro.2012.10.042.
- McClelland, A. 2017. “The Centrality of Communities and Civil Society in Epidemic and Pandemic Prevention. A Framework for Improved Preparedness and Response.” Prehospital and Disaster Medicine 32(S1):S205–S6. doi: https://doi.org/10.1017/S1049023X17005362.
- Mac McCullough, J., E. Eisen-Cohen, and B. Lott. 2020. “Barriers and Facilitators to Intraorganizational Collaboration in Public Health: Relational Coordination across Public Health Services Targeting Individuals and Populations.” Health Care Management Review 45(1):60–72. doi: https://doi.org/10.1097/HMR.0000000000000203.
- Mays, G. P., and F. D. Scutchfield. 2010. “Improving Public Health System Performance through Multi-Organisational Partnerships.” Preventing Chronic Disease 7(6).
- Nick, G. A., E. Savoia, L. Elqura, M. S. Crowther, B. Cohen, M. Leary, T. Wright, J. Auerbach, and H. K. Koh. 2009. “Emergency Preparedness for Vulnerable Populations: People with Special Health-Care Needs.” Public Health Reports 124(2):338–43. doi: https://doi.org/10.1177/003335490912400225.
- Nkengasong, J. N., and W. Mankoula. 2020. “Looming Threat of COVID-19 Infection in Africa: act Collectively, and Fast.” The Lancet 395(10227):841–2. doi: https://doi.org/10.1016/S0140-6736(20)30464-5.
- Nutt, P. C., and R. W. Backoff. 1993. “Organizational Publicness and Its Implications for Strategic Management.” Journal of Public Administration Research and Theory 3(2):209–31.
- Okwen, M., J. Signe, S. M. Macpella, L. Mbibeh, and L. Cockburn. 2018. “Professional Collaboration for Vision and Healthcare in Cameroon: Case Report.” African Vision and Eye Health 77(1):1–10. doi: https://doi.org/10.4102/aveh.v77i1.434.
- Paige, S., M. Jones, L. D’Ambrosio, W. Taylor, D. Bonne, M. Loehr, and A. Stergachis. 2010. “Strengthening Community Partnerships with Local Public Health through Regional Pandemic Influenza Exercises.” Public Health Reports 125 (3):488–93. doi: https://doi.org/10.1177/003335491012500318.
- Panahifar, F., P. J. Byrne, and C. Heavey. 2015. “A Hybrid Approach to the Study of CPFR Implementation Enablers.” Production Planning & Control 26(13):1090–109. doi: https://doi.org/10.1080/09537287.2015.1011725.
- Pollack, C. V., Jr., A. Amin, and D. A. Talan. 2012. “Emergency Medicine and Hospital Medicine: A Call for Collaboration.” The American Journal of Medicine 125(8):826.e1–e6. doi: https://doi.org/10.1016/j.amjmed.2011.12.005.
- Pratt, R., B. Gyllstrom, K. Gearin, C. Lange, D. Hahn, L.-M. Baldwin, L. VanRaemdonck, D. Nease, and S. Zahner. 2018. “Identifying Barriers to Collaboration between Primary Care and Public Health: Experiences at the Local Level.” Public Health Reports 133(3):311–7. doi: https://doi.org/10.1177/0033354918764391.
- Purohit, J. K., M. L. Mittal, S. Mittal, and M. K. Sharma. 2016. “Interpretive Structural Modeling-Based Framework for Mass Customisation Enablers: An Indian Footwear Case.” Production Planning & Control 27(9):774–86. doi: https://doi.org/10.1080/09537287.2016.1166275.
- Rajan, D., K. Koch, K. Rohrer, C. Bajnoczki, A. Socha, M. Voss, M. Nicod, V. Ridde, and J. Koonin. 2020. “Governance of the Covid-19 Response: A Call for More Inclusive and Transparent Decision-Making.” BMJ Global Health 5(5):e002655. doi: https://doi.org/10.1136/bmjgh-2020-002655.
- Rinehart, T. A., A. T. Laszlo, and G. O. Briscoe. 2001. Collaboration Toolkit: How to Build, Fix, and Sustain Productive Partnerships. Washington, DC: US Department of Justice, Office of Community Oriented Policing Services.
- Ryu, S., and M. S. Johansen. 2017. “Collaborative Networking, Environmental Shocks, and Organizational Performance: Evidence from Hurricane Rita.” International Public Management Journal 20(2):206–25. doi: https://doi.org/10.1080/10967494.2015.1059915.
- Sage, A. 1977. Methodology for Large Scale Systems. New York: McGraw-Hill.
- Santibañez, S., J. Lynch, Y. P. Paye, H. McCalla, J. Gaines, K. Konkel, L. J. O. Torres, W. A. North, A. Likos, and K. L. Daniel. 2017. “Engaging Community and Faith-Based Organisations in the Zika Response, United States.” Public Health Reports 132(4):436–42. doi: https://doi.org/10.1177/0033354917710212.
- Savage, G. T., M. D. Bunn, B. Gray, Q. Xiao, S. Wang, E. J. Wilson, and E. S. Williams. 2010. “Stakeholder Collaboration: Implications for Stakeholder Theory and Practice.” Journal of Business Ethics 96(S1):21–6. doi: https://doi.org/10.1007/s10551-011-0939-1.
- Schotanus, F., J. Telgen, and L. de Boer. 2010. “Critical Success Factors for Managing Purchasing Groups.” Journal of Purchasing and Supply Management 16(1):51–60. doi: https://doi.org/10.1016/j.pursup.2009.10.002.
- Schwartz, J., and M. Y. Yen. 2017. “Toward a Collaborative Model of Pandemic Preparedness and Response: Taiwan's Changing Approach to Pandemics.” Journal of Microbiology, Immunology and Infection 50(2):125–32. doi: https://doi.org/10.1016/j.jmii.2016.08.010.
- Shoaf, K. I., M. M. Kelley, K. O’Keefe, K. D. Arrington, and M. L. Prelip. 2014. “Enhancing Emergency Preparedness and Response Systems: Correlates of Collaboration between Local Health Departments and School Districts.” Public Health Reports 129 Suppl 4(6):107–13. doi: https://doi.org/10.1177/00333549141296S414.
- Shukla, M., I. Todorov, and D. Kapletia. 2018. “Application of Additive Manufacturing for Mass Customisation: Understanding the Interaction of Critical Barriers.” Production Planning & Control 29(10):814–25. doi: https://doi.org/10.1080/09537287.2018.1474395.
- Sullivan, H., P. Williams, and S. Jeffares. 2012. “Leadership for Collaboration: Situated Agency in Practice.” Public Management Review 14(1):41–66. doi: https://doi.org/10.1080/14719037.2011.589617.
- Sushil, S. 2012. “Interpreting the Interpretive Structural Model.” Global Journal of Flexible Systems Management 13(2):87–106. doi: https://doi.org/10.1007/s40171-012-0008-3.
- Swaan, C. M., A. V. Öry, L. G. C. Schol, A. Jacobi, J. H. Richardus, and A. Timen. 2018. “Research Full Report: Ebola Preparedness in The Netherlands: The Need for Coordination between the Public Health and the Curative Sector.” Journal of Public Health Management and Practice 24(1):18–25. doi: https://doi.org/10.1097/PHH.0000000000000573.
- Sweeney, P. M., S. Stebbins, D. D. Stier, and Z. Pines. 2010. “State Courts and Public Health: Building Partnerships to Enhance Preparedness.” Public Health Reports 125 Suppl 5(5):87–91. doi: https://doi.org/10.1177/00333549101250S512.
- Talib, F., Z. Rahman, and M. N. Qureshi. 2011. “Analysis of Interaction among the Barriers to Total Quality Management Implementation Using Interpretive Structural Modeling Approach.” Benchmarking: An International Journal 18(4):563–87. doi: https://doi.org/10.1108/14635771111147641.
- Thakkar, J., S. G. Deshmukh, A. D. Gupta, and R. Shankar. 2005. “Selection of Third-Party Logistics (3PL): A Hybrid Approach Using Interpretive Structural Modeling (ISM) and Analytic Network Process (ANP).” Supply Chain Forum: An International Journal 6(1):32–46. doi: https://doi.org/10.1080/16258312.2005.11517137.
- Umviligihozo, G., L. Mupfumi, N. Sonela, D. Naicker, E. A. Obuku, C. Koofhethile, T. Mogashoa, A. Kapaata, G. Ombati, C. M. Michelo, et al. 2020. “Sub-Saharan Africa Preparedness and Response to the COVID-19 Pandemic: A Perspective of Early Career African Scientists.” Wellcome Open Research 5:163. doi: https://doi.org/10.12688/wellcomeopenres.16070.2.
- van der Wal, Z. 2020. “Being a Public manager in times of Crisis: The Art of Managing Stakeholders, Political Masters, and Collaborative Networks.” Public Administration Review. 80(5):759–764.
- van der Watt, A. S. J., G. Nortje, L. Kola, J. Appiah-Poku, C. Othieno, B. Harris, B. D. Oladeji, O. Esan, V. Makanjuola, L. N. Price, et al. 2017. “Collaboration between Biomedical and Complementary and Alternative Care Providers: Barriers and Pathways.” Qualitative Health Research 27(14):2177–88. doi: https://doi.org/10.1177/1049732317729342.
- Vangen, S., and C. Huxham. 2010. “Introducing the Theory of Collaborative Advantage.” In The New Public Govenance? Emerging Perspectives on the Theory and Practice of Public Governance, edited by Osborne Stephen P. London: Routledge.
- Vasanthakumar, C., S. Vinodh, and K. Ramesh. 2016. “Application of Interpretive Structural Modelling for Analysis of Factors Influencing Lean Remanufacturing Practices.” International Journal of Production Research 54(24):7439–52. doi: https://doi.org/10.1080/00207543.2016.1192300.
- Vinodh, S., K. Ramesh, and C. S. Arun. 2016. “Application of Interpretive Structural Modelling for Analysing the Factors Influencing Integrated Lean Sustainable System.” Clean Technologies and Environmental Policy 18(2):413–28. doi: https://doi.org/10.1007/s10098-015-1025-7.
- Vishnu, C. R., R. Sridharan, and P. R. Kumar. 2019. “Supply Chain Risk Inter-Relationships and Mitigation in Indian Scenario: An ISM-AHP Integrated Approach.” International Journal of Logistics Systems and Management 32(3/4):548–78. doi: https://doi.org/10.1504/IJLSM.2019.098335.
- Walker, H., F. Schotanus, E. Bakker, and C. Harland. 2013. “Collaborative Procurement: A Relational View of Buyer–Buyer Relationships.” Public Administration Review 73(4):588–98. doi: https://doi.org/10.1111/puar.12048.
- Warfield, J. N. 1974. “Developing Interconnection Matrices in Structural Modeling.” IEEE Transactions on Systems, Man, and Cybernetics SMC-4(1):81–7. doi: https://doi.org/10.1109/TSMC.1974.5408524.
- Wood, D. J., and B. Gray. 1991. “Toward a Comprehensive Theory of Collaboration.” The Journal of Applied Behavioral Science 27(2):139–62. doi: https://doi.org/10.1177/0021886391272001.
- World Health Organisation. n.d. “U.N. Inter-Agency Task Force on NCDs and COVID-19.” https://www.who.int/teams/ncds/covid-19/unitaf
- Yadav, P. 2015. “Health Product Supply Chains in Developing Countries: Diagnosis of the Root Causes of Underperformance and an Agenda for Reform.” Health Systems and Reform 1(2):142–54. doi: https://doi.org/10.4161/23288604.2014.968005.
- Yuen, K. F., X. Wang, Y. D. Wong, and Q. Zhou. 2017. “Antecedents and Outcomes of Sustainable Shipping Practices: The Integration of Stakeholder and Behavioural Theories.” Transportation Research Part E: Logistics and Transportation Review 108:18–35. doi: https://doi.org/10.1016/j.tre.2017.10.002.