
Abstract
Background: Life quality has become a widely used concept within rehabilitation and occupational therapy practice.
Aim: This study explored child and parent perspectives of life quality of children with physical impairments compared with a group of non-disabled children.
Method: Data were collected with the Icelandic self- and proxy-reported versions of the KIDSCREEN-27. For children with physical impairments, reports from 34 children and 40 parents were included in the analyses, and in control group reports from 429 children and 450 parents were included.
Results: Children with physical impairments evaluated their life quality within the average range on four out of five life quality dimensions. The lowest scores were within the physical well-being dimension. Self-reported scores of children with physical impairments were higher than those of their parents on all dimensions except autonomy and parent relations. Thus, the parents considered more environmental and personal factors to negatively influence their child’s life quality than children did themselves.
Conclusion: Children with physical impairments experience their life quality similarly to non-disabled children.
Significance: Focus on life quality can help occupational therapists to identify what circumstances positively or negatively influence client well-being and to focus more on contextual factors that contribute to disablement.
Introduction
For the last two decades, children’s rehabilitation has made great strides in moving away from ‘medical model’ and impairment-based interventions that focus on changing children’s body functions and structures, to focusing more on contextual factors in disablement [Citation1,Citation2], as well as children’s life quality [Citation3–5]. This important shift is partly related to the advent of the International Classification of Functioning, Disability and Health for children and youth (ICF-CY) [Citation2] and is also in line with the United Nations Convention on the Rights of Persons with Disabilities (UN-CRPD) [Citation6], both of which offer a relational understanding of the multiple mediators of disablement [Citation7,Citation8]. Accordingly, disability is considered to be the result of the dynamic interactions between children with impairments and ‘attitudinal and environmental barriers that hinders their full and effective participation in society’ [Citation6]. Within occupational therapy studies, children’s well-being is said to be impacted by their daily participation and the occupations in which they engage [Citation9], and improving children’s life quality is a pervasively stated goal of occupational therapy programs worldwide [Citation3,Citation10].
Life quality is a multidimensional concept intended to capture children’s own subjective sense of well-being [Citation5,Citation11]. By focusing on circumstances that enable or constrain children’s participation and prosperity – e.g. in regard to health, standard of living, parental guidance, privacy, education, play and leisure – the concept relates closely to children’s rights [Citation6,Citation12]. However, in health research some conceptual confusion abounds in term of relevant domains and how these interact [Citation8], with different measures having different understandings [Citation13]. Also, the concept is ‘subjective’ insofar as it is typically assessed using self-report measures that produce measurable scores across predetermined domains. Nevertheless, judicious use of generic life quality measures like the KIDSCREEN can help identify what circumstances positively or negatively influence children’s well-being and thus provide valuable insights into how best to support their rights as outlined by the UN-CRPD [Citation6] by focusing on contextual factors that contribute to disablement.
Children with physical impairments often report levels of life quality similar to children in the general population [Citation14–17]. Most related studies focus on children with Cerebral Palsy (CP) while a few have included children with different diagnoses (e.g. children with Spina Bifida or neuromuscular disorders) compared with non-disabled children. For children with CP, quantitative studies indicate that type and severity of impairment are seldom associated with perceptions of life quality [Citation14,Citation15,Citation18]. Nevertheless, children having walking difficulties tend to report lower levels of physical well-being [Citation15] and children experiencing frequent pain often report lower scores of overall life quality than other children [Citation14,Citation15,Citation19]. Furthermore, studies provide conflicting evidence about how life quality of children with other types of physical impairments than CP compares with that of children in general [Citation20–22]. Thus, more studies are needed to shed further light on this topic.
This study is part of a larger research project focusing on the life quality, participation and environments of disabled and non-disabled children living in Iceland (LIFE-DCY) [Citation23–27]. Our present objectives are to 1) describe the life quality of children with physical impairments as reported by the children themselves and their parents and 2) compare life quality of children with physical impairments with life quality of children in the Icelandic population.
Methods
Participants
Participants were recruited from the registry of the State Diagnostic and Counselling Centre (SDCC), which keeps diagnostic records of the vast majority of disabled children in Iceland. Eligible for participation were all children with physical impairments and IQ above 80, aged between 8-18 years at the time of the study. The inclusion criteria were set to increase children’s capacity to read and respond to a questionnaire. Altogether 80 children and their parents were invited to participate in the study. Additionally, a random sample of 429 non-disabled children from the national registry (aged 8-18 years) and 450 parents participated in the study (control group).
For children with physical impairments the response rate was 42.5% (n = 34) (self-reports). More parents than children answered the questionnaire and the response rate for parents (proxy-reports) was 50% (n = 40). According to the records of the SDCC, most children had CP, others Spina Bifida (four children) or Neuromuscular disorders (six children). The children with CP were all classified at Level I or II in the Gross Motor Function Classification System (GMFCS) [Citation28], meaning that they were capable of walking in most settings but uneven terrains, inclines and long distances might influence their mobility choices. shows the sample characteristics of the participating children.
Table 1. Characteristics of the participating children and the children of participating parents.
The majority of proxy respondents were mothers (95% for children with physical impairments and 83.8% for control group). The mean age of proxy respondents was 42 (SD =6.7) for children with physical impairments and 44 (SD =6.6) for control group, and most of them held a university degree; 62.5% for parents of children with physical impairments and 69.3% for control group.
Measure
Data were collected with the Icelandic self- and proxy-reported versions of the KIDSCREEN-27 [Citation29]. The measure is a generic health-related life quality instrument for children and adolescents aged 8-18 years. It was developed simultaneously in 13 European countries by appraising views of children and emphasising perception of psychosocial aspects of well-being rather than functioning or symptoms. The measure includes 27 items covering five life quality domains: physical well-being (five items), psychological well-being (seven items), autonomy and parent relations (seven items), social support and peers (four items) and school environment (four items) (see ). Each question or item is rated on a 5-point Likert response scale ranging from ‘not at all’ to ‘extremely’ or from ‘never’ to ‘always’. The recall period is one week [Citation29].
Figure 1. Conception of the KIDSCREEN-27 dimensions [Citation29].
![Figure 1. Conception of the KIDSCREEN-27 dimensions [Citation29].](/cms/asset/d99c8e11-2f9f-405d-a272-0b59ce11dff3/iocc_a_1509371_f0001_b.jpg)
For this study, an electronic version of the KIDSCREEN-27 was used that allowed questions to be presented one at a time. Additionally, the children had the option of listening to pre-recorded questions. Before answering, both children and parents were asked to think about the last week and the parents were also given the instructions to answer how they thought their child felt. These instructions were in concordance with guidelines from the KIDSCREEN manual [Citation29].
The KIDSCREEN measure has been shown to have good psychometric properties [Citation30,Citation31]. In the current study, the internal consistency (Cronbach’s alpha) for self-report measures was in the range of 0.71 (physical well-being) and 0.93 (psychological well-being) for children with physical impairments and 0.79 (social support and peers) and 0.89 (psychological well-being) for children in control group. For the proxy-versions the range was 0.70 (autonomy and parent relations) and 0.92 (social support and peers) for parents of children with physical impairments and 0.79 (autonomy and parent relations) and 0.88 (social support and peers) for parents of children in control group. Hence, all alpha values met or exceeded the threshold of 0.70 that is required for group comparisons [Citation32].
Procedure
A cross-sectional descriptive comparative design was used. Initially, introductory letters were sent by regular mail to prospective participants in an envelope addressed to parents. The letters contained a link to the study website and a password that enabled participants to answer the life quality measure electronically. Approximately one week later all parents received a phone call as a reminder. This also gave them an opportunity to seek more information about the study. It was considered as a consent for participation if the parents responded to the measure and delivered the introductory letter to their child. The child then decided to take part in the study by answering or not. This arrangement was described in the introductory letters to parents and children.
Participation was anonymous, ensuring that no personal information was attached to the electronic measure. A professional with a long experience working with children with physical impairments and their families at the SDCC was responsible for all communication with the research group while professionals at the University of Akureyri Research Centre contacted the control group. The study was approved by the Icelandic National Bioethics Committee (VSN-13-081-V3).
Analyses
All analyses were conducted using IMB SPSS Statistics 24. Total raw scores from each KIDSCREEN-27 dimension were converted into Rasch scores and then into T-values by using SPSS syntaxes provided in the manual [Citation29]. The threshold for classifying life quality scores as ‘within the average range’ or ‘below the average’ was set at a value of the mean life quality score of children in control group, plus or minus half a standard deviation. For example, if the mean of the control group was 50 and SD was 10 the resulting range was 45 to 55 (50 +/− (0.5*10)).
Independent sample t-tests were conducted to compare the means between different groups (95% significance level) and effect sizes (eta (ɳ2)) were calculated and classified as a small effect (ɳ2 = 0.01), moderate effect (ɳ2 = 0.06), or large effect (ɳ2 = 0.14) (Cohen, 1988). Consistent with guidelines from the KIDSCREEN manual [Citation29], the children were divided into younger (8-11 years) and older (12-18 years) age groups. Additionally, in keeping with the guidelines, a dimension score was not calculated if more than one question remained unanswered.
Results
provides mean T-values and SD, along with independent sample t-tests and effect sizes when comparing self- and proxy-reported scores (see also ). The mean self-reported life quality scores of children with physical impairments were within the average range in four out of five life quality dimensions; psychological well-being, autonomy and parent relations, social support and peers, and school environment. On the physical well-being dimension the children’s mean score fell below the average threshold of 53.34 +/− (0.5*10.81) and t-test showed significant difference between the scores of children with physical impairments and children in control group (t(457) = 3.800, p < 0.001) although the effect size was small (ɳ2 = 0.03).
Figure 2. Life quality scores based on self- and proxy-reports in both groups of children.
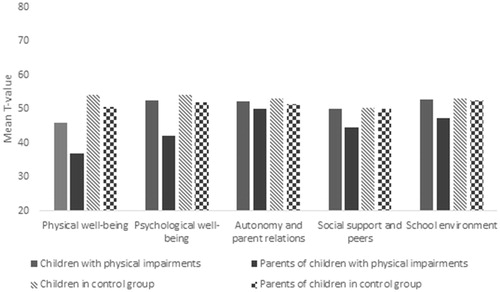
Table 2. Comparison of children’s and parents’ ratings: Independent sample t-tests and effect sizes.
Parents of children with physical impairments evaluated their children’s life quality below the average threshold on two KIDSCREEN dimensions; on physical well-being (50.20 +/− (0.5*10.15)) and psychological well-being (50.85 +/− (0.5*9.90)). On the physical well-being dimension the proxy-mean score fell below one standard deviation from the control group’s mean (<40.05) and t-test showed significant difference (t(48) = 10.190, p < 0.001) with high effect size (ɳ2 = 0.18). For the psychological well-being dimension the difference was also significant (t(470) = 5.201, p < 0.001) but the effect size was small (ɳ2 = 0.05). Additionally, significant differences were found on social support and peers (t(41) = 2.156, p = 0.037, ɳ2 = 0.01) and school environment (t(463) = 2.591, p = 0.010, ɳ2 = 0.01) both with small effect sizes.
The self-reported life quality scores of children with physical impairments were significantly higher than the parent-proxy reported scores on the physical well-being and psychological well-being dimensions with high effect sizes, and on social support and peers and school environment where the effect sizes were moderate. No difference was found between the ratings of children with physical impairments and parents on autonomy and parent relations (see also ).
Differences in age and gender
For children with physical impairments, significant gender differences with moderate effect sizes were found on two life quality dimensions; on psychological well-being (t(31) = 2.086, p = 0.045, ɳ2 = 0.12) and school environment (t(32) = 2.174, p = 0.037, ɳ2 = 0.13), with boys reporting higher levels of life quality than girls. No gender differences were found when analysing the parent-proxy reported scores. Other background factors, like the children’s age and residence did not influence self- or proxy-reported scores among children with physical impairments.
Similar gender differences were not found in self- nor proxy-reported life quality scores among the control group. Nevertheless, girls in the control group reported lower levels of life quality regarding physical well-being than boys (t(332) = 2.882, p = 0.004) but with small effect size (ɳ2 = 0.02). In the control group older children reported lower life quality than younger children on all dimensions except for autonomy and parent relations with small effect sizes (p < 0.01, ɳ2 < 0.06).
Discussion
According to their ratings, children with physical impairments were quite positive about many aspects of their lives. On the KIDSCREEN-27 the children evaluated their life quality within the average range on four out of five life quality dimensions. The results revealed their overall positive emotions and satisfaction with life, fulfilment with their relationships with their parents and friends, and positive feelings about school. In fact, the self-reported scores for both groups of children were quite similar in all dimensions except for physical well-being where the mean score of children with physical impairments was below half a standard deviation from the control group’s average.
In contrast, the ratings of the parents of children with physical impairments were less positive toward their children’s life quality. On two dimensions, physical well-being and psychological well-being, they evaluated their children’s life quality below the average threshold. Thus, the parents were clearly concerned about their child’s physical activity and energy, as well as their self-esteem and happiness.
For children with physical impairments, the self-reported mean scores were higher than those of their parents on four out of five life quality dimensions; on physical well-being, psychological well-being, social support and peers and school environment. Medium to large effect sizes were found in these four dimensions. Despite these differences in ratings, the children with physical impairments and their parents seemed to agree about which area was most problematic, as apparent in the lowest mean scores and high effects sizes for the physical well-being dimension. Similar differences between self- and proxy reported scores were evident between children with autism spectrum disorder and their parents in our larger study [Citation24,Citation27]. These findings are also in concordance with studies showing that parents of children with physical impairments tend to rate their child’s life quality lower than the child’s own ratings, especially in domains that are more subjective than objective (or observable) in nature [Citation33–36].
The study results suggest it is important for occupational therapists and other professionals working with disabled children and their families to recognize that children and parents are likely to have different perspectives of the children´s life quality and consider abilities, constrains and their implications differently when answering measures like the KIDSCREEN [Citation24]. It is not unlikely that parents are concerned with their child’s well-being and future prospects, and that their own normative ideas of what constitutes a good life may affect their answers even though they are asked to answer just as their child would. However, the good news is that the children were generally positive towards their lives as evident on the psychological well-being dimension where the children’s mean scores were relatively high.
Among children with physical impairments, gender differences were found on two life quality dimensions; psychological well-being and school environment with girls reporting lower levels of life quality than boys. These results revealed lower self-esteem, more sadness and more negative feelings about school life among girls than boys. This is noteworthy in light of recent concerns about the effect of the impairment on identity and masculinity of boys with physical impairments, and how it may affect their lives [Citation37]. Nevertheless, little research is available on the intersection of gender and disability with school aged children and the effects of life quality.
For Icelandic children in general, recent findings from the 2015 OECD PISA research about well-being of school-aged children showed higher satisfaction with life among boys than girls [Citation38]. Furthermore, European studies report more decline of life quality of girls than boys with increasing age, especially regarding ‘general moods and feelings about self’ and ‘physical activities and health’ [Citation39,Citation40]. These differences may be due to diverse social expectations, harsh self-criticism (e.g. related to body-image) and puberty being a more significant experience for girls than boys [Citation38,Citation39]. Interestingly, this was not the case in our control group; although girls scored significantly lower than boys on the physical well-being dimensions the effect size was only small and in other life quality dimensions gender differences were not found.
The KIDSCREEN measure has previously been used in several studies to examine life quality of children with physical impairments [Citation15,Citation19,Citation34] and it has been shown to give compatible results with children with CP and in the general population [Citation41]. Most items in the KIDSCREEN-27 concern how the children feel rather than what they do (e.g. ‘have you been happy at school?’) and thus focus on feelings like pleasure and purpose in life, as well as the children’s sense of belonging - reflecting ‘subjective’ well-being which is increasingly considered to be an important strength for life quality measures [Citation11]. The physical well-being dimension perhaps contains the most ‘performance based’ items with questions such as ‘have you been able to run well?’ The study by Erhart et al. [Citation41] shows that children with CP are less likely than children in general to obtain a high score on that item. Nevertheless, it can be argued that children with physical impairments can experience a high level of physical well-being without being able to run, walk or cycle well or the same way as other children do. It also raises the question what it means for them to do things well, which is highly open to individual interpretation, and if the children may instead be responding to an imagined question of ‘can you run?’
It can be argued that life quality measures that offer such set options of what constitutes a good life have major shortcomings, especially since they do not take into account the child’s unique perspective on the relevant significance of each of these options in relation to his or her life [Citation8]. Nonetheless, we suggest that such measures when used judiciously, are still important in enabling the comparison between the ratings of disabled and non-disabled children as well as that of their parents [Citation4], like we have done in this study. Historically, disabled children have been portrayed as incompetent and/or vulnerable in research, and although there is a growing tendency to include children’s perspectives, it is has mainly applied to non-disabled children. Disabled children were, and still are, much less commonly involved, perhaps because of perceived difficulties with access, the need for some accommodations, and/or negative assumptions about their capabilities [Citation42,Citation43]. Therefore, it is important that disabled children are given the opportunity to participate in large-scale studies along with other children. The results of such research can be used to identify specific challenges faced by disabled children compared with other children; to influence public policy decisions in order to support disabled children’s participation and well-being, and ultimately to challenge oppressive social, cultural, legal, institutional, and other barriers that hinder participation and opportunities for disabled children [Citation44].
When children with physical or other types of impairments report that their lives are of diminished quality, there is a cultural assumption – frequently shared by practitioners and researchers – that this is an inevitable consequence of their impairments [Citation44]. Much of our time as occupational therapists is spent on evaluating and classifying children’s bodily structures and function, and consequently we often work towards changing the child’s body so it more closely adheres to valued social norms of wholeness and normalcy. However, the ICF-CY [Citation2] promotes a more expansive view of the role of rehabilitation providers, one that looks more broadly at children’s lives by focusing on the interplay between their social participation and relevant environmental factors. The concept of life quality has the potential to help us identify and address the qualities of meaningful living that are valued contributors to children’s rights and well-being [Citation45]. That is where our focus should be directed.
Strengths and limitations
A strength of this study is the large control group based on population-based sample that allowed us to compare data from children with physical impairments to that of Icelandic children in general. Another strength is that we stressed accessibility issues such as providing the option of listening to pre-recorded questions to children in both groups to enable more children to participate. Also, a professional working at SDCC was in contact with the research group and provided extra information about the study whenever necessary. Not all children with physical impairments living in Iceland are listed in the registry of SDCC and it is a limitation to the study that only 34 children participated. Also, information on background characteristics of non-responders was not available. Another limitation is that mothers constituted a great majority of respondents, with overrepresentation of parents with university degrees, although the latter factor was not found to be associated with differences between child and proxy ratings. No information was gathered about other factors related to the children’s impairment, like possible co-morbidities and services received other than special education services. Also, information was not gathered about financial resources, social-economic status and marital status of the participating families.
Conclusion
This study provides an important understanding of the life quality of children with physical impairments as measured by the KIDSCREEN-27, both from the perspectives of children themselves and from their parents. Our findings indicate that children with physical impairments experience their life quality similarly to non-disabled children. We also know that, as with the general population, some children with physical impairments are at more risk to experience lower life quality than others. Therefore, it is important for occupational therapists and others working with disabled children to understand and identify what factors might influence the children’s well-being e.g. with help from life quality measures like the KIDSCREEN [Citation29]. Nevertheless, further investigation is needed to understand more fully how the key issues of life quality are understood, applied by disabled children and relate to one another – as well as how the constructs of life quality and participation interrelate in the lives of disabled children and youth. The complexities of different interpretations of life quality by disabled children and their parents, and the relations of life quality with other concepts such as participation are the heart of our on-going study LIFE-DCY in Iceland. The findings presented here provide a starting point for further quantitative and qualitative analysis, on which we will report in additional publications.
Acknowledgements
We would like to thank the families who participated in the study. We would also like to thank Professor Barbara E Gibson at the University of Toronto who contributed to the research. The study was supported by the Icelandic Research Fund under Grant number 174299-051; and the Doctoral Grants of The University of Iceland Research Fund.
Disclosure statement
The authors report no conflicts of interest.
Related Research Data
References
- Gibson BE, Darrah J, Cameron D, et al. Revisiting therapy assumptions in children's rehabilitation: clinical and research implications. Disabil Rehabil. 2009;31:1446–1453.
- World Health Organization. International classification of functioning, disability and health: children and youth version. ICF-CY. Geneva: World Health Organization; 2007.
- McDougall J, Wright V, DeWit D, et al. ICF-based functional components and contextual factors as correlates of perceived quality of life for youth with chronic conditions. Disabil Rehabil. 2014;36: 2143–2151.
- Ravens-Sieberer U, Gosch A, Rajmil L, et al. KIDSCREEN-52 quality-of-life measure for children and adolescents. Expert Rev Pharmacoecon Outcomes Res. 2005;5:353–364.
- Colver A. Measuring quality of life in studies of disabled children. Paediatr Child Health. 2008;18:423–426.
- United Nations. Convention on the rights of persons with disabilities. 2007.
- Bickenbach JE. The International classification of functioning, disability and health and its relationship to disability studies. In: Watson N, Roulstone A, Thomas C, editors. Routledge handbook of disability studies. London: Routledge, Taylor & Francis Group; 2012. p. 51–66.
- Gibson BE. Rehabilitation, a post-critical approach. Boca Raton: CRC Press, Taylor & Francis Group; 2016.
- Townsend EA, Polatajko HJ. Enabling occupation II: advancing an occupational therapy vision for health, well-being and justice through occupation. Ottawa, ON: CAOT Publications ACE; 2007.
- King G, Tucker MA, Baldwin P, et al. A life needs model of pediatric service delivery: services to support community participation and quality of life for children and youth with disabilities. Phys Occup Ther Pediatr. 2002;22:53–77.
- Wallander JL, Koot HM. Quality of life in children: a critical examination of concepts, approaches, issues, and future directions. Clin Psychol Rev. 2016;45:131–143.
- United Nations. Convention on the rights of the child. 1989.
- Hemmingsson H, Ólafsdóttir LB, Egilson ST. Agreements and disagreements between children and their parents in health-related assessments. Disabil Rehabil. 2017;39:1059–1072.
- Colver A, Rapp M, Eisemann N, et al. Self-reported quality of life of adolescents with cerebral palsy: a cross-sectional and longitudinal analysis. Lancet. 2015;385:705–716.
- Dickinson HO, Parkinson KN, Ravens-Sieberer U, et al. Self-reported quality of life of 8-12-year-old children with cerebral palsy: a cross-sectional European study. Lancet. 2007;369:2171–2178.
- Chow SM, Lo SK, Cummins RA. Self-perceived quality of life of children and adolescents with physical disabilities in Hong Kong. Qual Life Res. 2005;14:415–423.
- Shikako-Thomas K, Lach L, Majnemer A, et al. Quality of life from the perspective of adolescents with cerebral palsy: "I just think I'm a normal kid, I just happen to have a disability". Qual Life Res. 2009;18:825–832.
- Rosenbaum PL, Livingston MH, Palisano RJ, et al. Quality of life and health-related quality of life of adolescents with cerebral palsy. Dev Med Child Neurol. 2007;49:516–521.
- White-Koning M, Arnaud C, Dickinson HO, et al. Determinants of child-parent agreement in quality-of-life reports: a European study of children with cerebral palsy. Pediatrics. 2007;120:e804–e814.
- Sawin KJ, Bellin MH. Quality of life in individuals with spina bifida: a research update. Dev Disabil Res Rev. 2010;16:47–59.
- Wei Y, Speechley K, Campbell C. Health-related quality of life in children with duchenne muscular dystrophy: a review. J Neuromuscul Dis. 2015;2: 313–324.
- Domellöf E, Hedlund L, Ödman P. Health-related quality of life of children and adolescents with functional disabilities in a northern Swedish county. Qual Life Res. 2014;23:1877–1882.
- Egilson ST, Jakobsdóttir G, Ólafsdóttir LB. Parent perspectives on home participation of high-functioning children with autism spectrum disorder compared with a matched group of children without autism spectrum disorder. Autism. 2018;22:560–570.
- Egilson ST, Ólafsdóttir LB, Leosdottir T, et al. Quality of life of high-functioning children and youth with autism spectrum disorder and typically developing peers: self- and proxy-reports. Autism. 2017;21:133–141.
- Egilson ST, Jakobsdottir G, Olafsson K, et al. Community participation and environment of children with and without autism spectrum disorder: parent perspectives. Scand J Occup Ther. 2017;24: 187–196.
- Jakobsdóttir G, Egilson ST, Ólafsson K. Skólaþátttaka og umhverfi 8-17 ára getumikilla barna með einhverfu: Mat foreldra [School participation and environment of high-functioning children with autism spectrum disorder, aged 8-17 years]. Uppeldi og menntun [Icelandic Journal of Education]. 2015;24:75–97.
- Ólafsdóttir LB, Egilson ST, Ólafsson K. Lífsgaeði 8-17 ára getumikilla barna með einhverfu: Mat barna og foreldra þeirra [Quality of life of high-functioning children with autism spectrum disorders, aged between 8-17 years]. Uppeldi og menntun [Icelandic Journal of Education]. 2014;23:43–63.
- Palisano R, Rosenbaum P, Bartlett D, et al. Gross motor function classification system. Expanded and revised. Hamilton: CanChild; 2007.
- KIDSCREEN Group Europe. The KIDSCREEN questionnaires: quality of life questionnaires for children and adolescents – Handbook. Lengerich: Pabst Science Publishers; 2006.
- Ravens-Sieberer U, Auquier P, Erhart M, et al. The KIDSCREEN-27 quality of life measure for children and adolescents: psychometric results from a cross-cultural survey in 13 European countries. Qual Life Res. 2007;16:1347–1356.
- Robitail S, Ravens-Sieberer U, Simeoni MC, et al. Testing the structural and cross-cultural validity of the KIDSCREEN-27 quality of life questionnaire. Qual Life Res. 2007;16:1335–1345.
- Nunnally JC, Bernstein IR. Psychometric theory. 3rd ed. New York: McGraw-Hill; 1994.
- White-Koning M, Grandjean H, Colver A, et al. Parent and professional reports of the quality of life of children with cerebral palsy and associated intellectual impairment. Dev Med Child Neurol. 2008;50:618–624.
- Longo E, Badia M, Orgaz MB, et al. Comparing parent and child reports of health-related quality of life and their relationship with leisure participation in children and adolescents with Cerebral Palsy. Res Dev Disabil. 2017;71:214–222.
- Lim Y, Velozo C, Bendixen RM. The level of agreement between child self-reports and parent proxy-reports of health-related quality of life in boys with Duchenne muscular dystrophy. Qual Life Res. 2014;23:1945–1952.
- Murray CB, Holmbeck GN, Ros AM, et al. A longitudinal examination of health-related quality of life in children and adolescents with spina bifida. J Pediatr Psychol. 2015;40:419–430.
- Shuttleworth R, Wedgwood N, Wilson NJ. The dilemma of disabled masculinity. Men Masc. 2012; 15:174–194.
- OECD. PISA 2015 Results (Volume III). 2017.
- Bisegger C, Cloetta B, von Rueden U, et al. Health-related quality of life: gender differences in childhood and adolescence. Soz Präventivmed. 2005; 50:281–291.
- Michel G, Bisegger C, Fuhr DC, et al. Age and gender differences in health-related quality of life of children and adolescents in Europe: a multilevel analysis. Qual Life Res. 2009;18:1147–1157.
- Erhart M, Ravens-Sieberer U, Dickinson HO, et al. Rasch measurement properties of the KIDSCREEN quality of life instrument in children with cerebral palsy and differential item functioning between children with and without cerebral palsy. Value Health. 2009;12:782–792.
- Einarsdóttir J, Egilson ST. Embracing diversity in childhood studies: methodological and practical considerations. In: Farrell A, Samuelsson IP, editors. Diversity in the early years: intercultural learning and teaching. Melbourne: Oxford University Press; 2016. p. 35–53.
- Teachman G, Gibson BE. Children and youth with disabilities: innovative methods for single qualitative interviews. Qual Health Res. 2013;23:264–274.
- Hammell KW. Quality of life, participation and occupational rights: a capabilities perspective. Aus Occup Ther J. 2015;62:78–85.
- Hammell KW. Opportunities for well-being: the right to occupational engagement. Can J Occup Ther. 2017;84:209–222.