
ABSTRACT
The aim of this study was to compare the reliability of both linear and angular measurements conducted on two-dimensional (2D) lateral cephalometric images and three-dimensional (3D) cone-beam computed tomography-generated cephalograms derived from various rendering software. Pre-treatment cephalometric digital radiographs of 15 patients and their corresponding cone beam computed tomographic images were randomly selected. Vista Dent OC as 2D, In vivo 5.1.2, Maxilim and Romexis software were used to generate cephalograms from the CBCT scans (NewTom 3G, QR Verona, Italy). In total, 19 cephalometric landmarks were identified and 18 widely used (11 linear, 7 angular) measurements were performed by an independent observer. Mann–Whitney and Kruskall–Wallis H tests were also used to compare the four methods (p < 0.05). Intra-class correlation coefficients (ICCs) were used to examine the intra-observer reliability. Intra-observer examinations showed various unreliable ICCs, which was an indication of poor reproducibility for condylion-gnathion (Co-Gn), gonion-mentum (Go-Me), anterior nasal spina-mentum (ANS-Me), Wits for all 2D and 3D rendering software (p > 0.05). The ICCs for Vista Dent OC (2D) measurements indicated high reproducibility (p < 0.05). The 2D and 3D generated cephalograms from various rendering software were found to be similar; however, measurements on curved surfaces are not easily reproducible for 3D software.
Introduction
Since 1931, two-dimensional (2D) planar images, especially lateral cephalometric X-rays made with standardized projection geometrics, have been used to identify specific anatomic maxillofacial landmarks. These anatomical landmarks anatomy are the basis of a simple methodology to determine well-known linear and angular measurements also known as conventional cephalometry that has become one of the standard diagnostic tools for analyzing maxillofacial deformities and orthodontic problems and evaluating growth and/or treatment changes.[Citation1,Citation2] However, conventional or digital 2D lateral cephalometric radiographs (LCRs) that project three-dimensional (3D) structures onto a 2D plane can cause magnification problems.[Citation3–5] Moreover, errors in the patient's head position and magnification make landmark identification difficult and can cause reduced measurement reliability.[Citation3,Citation4,Citation6,Citation7] Additionally, one of the most common insufficiencies of 2D methods with lateral cephalometric radiography and cephalometric analysis is double imaging of the lower borders of the mandible. Therefore, observer identification errors are also common in orthodontic anatomical landmarks.[Citation3–5] Since 3D technology provides a more realistic representation of the head of the patient and has expanded the diagnostic possibilities,[Citation8] its popularity has increased rapidly. Multislice computed tomography (MSCT) has been used for evaluating 3D structures; however, because of the high radiation risk of this technique, its use is restricted to selected cases.[Citation9]
Cone-beam computed tomography (CBCT) is a technique that has been proposed for maxillofacial imaging [Citation2,Citation9,Citation10–15] during the last decade and was first reported in medical literature by Mozzo et al. [Citation16]. CBCT is used increasingly for certain categories of patients because of the distinct advantage of a lower radiation dose than MSCT, as well as the possibility of importing and exporting individualized, overlap-free reconstructions and DICOM data to/from other applications. CBCT is now used for orofacial clefts, orthognathic issues and severe maxillofacial deformities.[Citation2,Citation9] These possibilities added to increased access to CBCT imaging for orthodontics are enabling the movement from 2D cephalometric analysis to 3D analysis.[Citation4] With the increasing use of 3D measurements in orthodontics, various 3D rendering software programs have been introduced to orthodontists for linear and angular measurements.
Even though studies have concluded that 2D and 3D measurements have shown similar reproducibility and are both reliable methods to use clinically, they still face some obstacles such as unreliability in identifying certain anatomical areas and points with 3D imaging.[Citation4,Citation5,Citation17] Although the accuracy [Citation1,Citation13,Citation17–20] and reliability [Citation21–23] of cephalometric landmark identification and measurements have been widely studied in vitro and in vivo for CBCT and 2D cephalometric radiographs, there is still the need for studying and comparing the reliability and reproducibility of 3D generated cephalograms vs. 2D conventional radiographs for different cephalometric landmarks.
Technological developments have provided us with quicker and more effective results in order to improve life quality and clinical approaches. However, such technological advances still generate various errors that need to be identified. As a result, the aim of this study was to compare the reliability of both linear and angular measurements that were conducted on 2D direct digital cephalometric radiographs (Vista Dent OC, 4.2.44, GAC International, Inc., Bohemia, NY, USA) and 3D CBCT generated cephalograms derived from various 3D rendering (In vivo 5.1.2, Maxilim, Romexis) software programs.
Materials and methods
Using retrospective data from our faculty, power analysis (Power and Precision software, Biostat, Englewood, NJ, USA) was conducted by using one-way ANOVA which indicated that the detection of differences between 2D and 3D cephalometric measurements could be obtained with at least 11 patients at a power of 0.8 (alpha = 0.05). Thus, this study was conducted using 15 (10 females, 5 males) randomly selected good-quality lateral cephalometric images and their corresponding CBCT images.
The study protocol was carried out according to the principles of the Helsinki Declaration, including all amendments and revisions. Collected data was only accessible to the researchers. Patients or their legal guardians gave their informed consent prior to radiography and the study was reviewed and approved by the institutional ethical board of the faculty (YDU/2014/24-142). Subjects with evidence of existing orthodontic treatment, missing permanent incisors or first molars, supernumerary teeth that were erupted or overlying incisor apices, gross skeletal asymmetries or bone disease were excluded from the study.
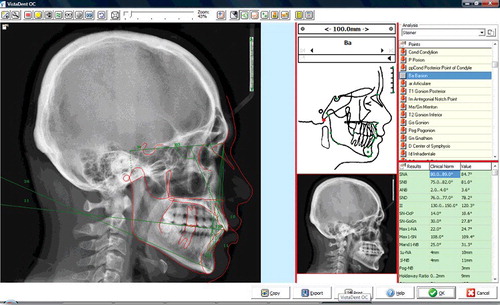
For generating 2D images, Planmeca 2002 cc Proline (Planmeca, Helsinki, Finland) was used to obtain digital cephalometric radiographs. The head rotation can affect the linear and angular measurements.[Citation24,Citation25] Therefore, radiographs were acquired according to the strictly standardized protocol, with the natural head position stabilized by ear rods, a focus-to-median plane distance of 152 cm and a detector-to-mid-sagittal distance of 12 cm as recommended by the manufacturer. Images were exposed at 73 kvp, 14 mA for 0.64s each at magnification of 1.25. Digital images were stored in a computer database using the manufacturer's own software (Romexis, version 3.2, Planmeca, Helsinki, Finland), corrected for magnification and imported to Vista Dent OC (2D), 4.2.44 (GAC International, Inc., Bohemia, NY, USA). Observers were permitted to adjust the image using the enhancement functions for brightness and contrast. The images were calibrated by digitizing two points on the ruler within the digital image using the manufacturer's software. Following digitization of the landmarks, measurements were automatically generated by the Vista Dent program ().
Figure 1. General layout of the Vista Dent OC software showing the cephalometric analysis.
For CBCT generated cephalograms, scans were obtained using a NewTom 3G CBCT scanner (Quantitative radiology s.r.l., Verona, Italy). Recent studies indicate that small variations in head position do not influence the reliability of measurements from 3D CBCT,[Citation26] but all CBCT scans were obtained according to the strict standardized scanning protocol. Patients were placed in a horizontal position, checked to ensure that their mouths were closed in a normal, natural occlusive position and instructed to lie still throughout the duration of the scan. Images were obtained using a 12 inch (∼30 cm) field of view (FOV) to ensure inclusion of the entire facial anatomy, with 0.3-mm-thick axial slices and isotropic voxels. Axial images were exported in a DICOM file format with a 512 × 512 matrix and were imported to In vivo 5.1.2 (Anatomage Inc., San Jose, CA, USA), Maxilim version 2.3.0. (Medicim, Sint-Niklass, Belgium) and Romexis (Romexis 3.2, Planmeca, Helsinki, Finland). All images were reconstructed on a 21.3-inch flat-panel colour active matrix TFT medical display (Nio Color 3MP, Barco, France) with a resolution of 76 Hz 0.2115 mm pitch 10 bit. The examiners were also permitted to use enhancements and orientation tools such as magnification, brightness and contrast to improve visualization of the landmarks.
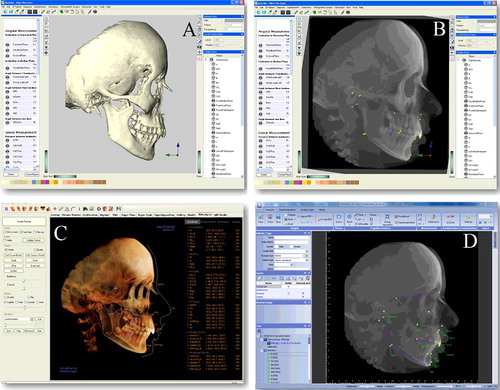
Linear and angular measurements of the 3D CBCT-generated images were performed by using landmarks that were identified by a pointer-driven cursor. All of the landmarks were firstly traced on the CBCT-generated cephalograms using 3D rendering software ().
Figure 2. Image showing (a) 3D generated skull representation, and (b) generated cephalograms measurements in Maxilim software, (c) cephalometric measurements in In vivo and (d) Romexis software packages.
Landmark identification and measurement for 2D and 3D cephalometric analyses were performed by an orthodontist with 4 years of experience (UK). In total, 19 cephalometric landmarks () were identified and 18 widely used measurements (11 linear and 7 angular) were recorded.
Table 1. The list of landmarks and cephalometric measurements that were used in the study.
An error analysis exercise was carried out using all of the data from the four different methodologies on the radiographs, which were retraced a second time after an interval of two weeks. Systematic bias was examined using SPSS software reliability analysis and interclass correlation coefficients (ICCs) were assessed ( and ).
Table 2. Intra-observer reliability for all tracing methods.
Table 3. Intra-class correlation coefficients for all tracings.
Statistical analysis
The SPSS 17.0.1 (SPSS, Chicago, IL) software program was used to carry out the statistical analysis. Mann–Whitney U and Kruskall–Wallis H tests were used to compare the tracing methods. A p value of less than or equal to 0.05 was considered statistically significant.
Results and discussion
Intra-observer reproducibility
In order to reveal the reliability of the methodologies, every single measurement was collected second time after a time period. Those results were used to expose reliability within each method individually (); and also among methodologies (). Overall intra-observer reproducibility ranged from 0.428 to 0.998. This result indicated that there were certain measurements that had low reproducibility. Detailed examination showed that only Vista Dent OC (2D) ICC values demonstrated a reliable reproducibility and ranged from 0.797 to 0.998 separately. However, the other three 3D rendering software ICC values demonstrated low reproducibility. Therefore, the reliability of the measurements of Co-Gn, ANS-ME and WIT'S Appraisal was found to be much less with the 3D – Maxilim, In vivo 5.1 and Romexis methods (). Additionally, Co-Gn and ANS-ME measurements were also calculated to be longer with 3D methods than 2D ().
Table 4. Analysis of mean differences for 2D and 3D measurements according all tracing methods.
Differences between the cephalometric measurements for all methods are provided in . The measurements of Co-Gn, Ar-Go, Go-Me and ANS-ME were statistically different between the 2D and 3D and also within the 3D results (p < 0.05). Therefore, the mean Co-Gn measurement for Vista Dent was 99.8 compared to 110.1 for Maxilim, 109.9 for In vivo and 182.1 for Romexis in CBCT-generated cephalograms. The Ar-Go measurements in the different programs were 47.8 for Vista Dent, 47.8 for Maxilim, 48.2 for In vivo, whereas Romexis was 79.4. Meanwhile, Go-Me and ASN-ME and Vista Dent OC were also significantly different in the Romexis software. All these measurements were significantly longer when compared to 2D Vista Dent and CBCT Generated Romexis software (p = 0.001) (). The other parameters showed no statistical differences between the 2D and 3D methods.
The aim of this study was to compare the reliability of both linear and angular measurements conducted on 2D lateral cephalometric images and 3D CBCT-generated cephalograms derived from various rendering software programs.
Cephalometric radiography is one of the most valuable diagnostic tools for evaluating skeletal growth, treatment response and long-term follow-up after orthodontic treatment. Lateral and frontal cephalograms are the most used projections for this purpose.[Citation27] However, these projections are prone to 2D radiographic limitations such as superimposition of the anatomic structures, difficulties in landmark identification, magnification and distortion. Therefore, imaging modality with 3D capabilities allows for evaluating and tracing anatomy more accurately.[Citation28–30]
In order to compensate for the shortcomings of 2D imaging methods, new technologies have been adapted to evaluate maxillofacial structures, such as multislice CT (MDCT) and cone beam CT (CBCT). Evaluating the reliability of measurements obtained with cephalometric images generated or reconstructed from 3D CT and CBCT data is important for orthodontists. Several studies have examined the reliability of linear and 3D measurements using CBCT.[Citation5,Citation10,Citation27] Most of these studies have reported that both CBCT and CT techniques can be used to obtain dimensionally accurate linear and angular measurements.[Citation5,Citation10,Citation27,Citation31–33] However, few studies have used CBCT-generated cephalograms using rendering programs in vivo.[Citation5,Citation6,Citation14,Citation27,Citation34]
The current study evaluated the reliability of linear and angular measurements in four rendering software programs; either in 2D or 3D generated cephalograms. According to the results, most of the cephalometric parameters used in this study showed no statistical differences between the measurements obtained by 2D Vista Dent tracing method and those obtained from CBCT-generated cephalograms (p > 0.05). However, the Co-Gn, Ar-Go, Go-Me and ANS-ME parameters showed significant differences between the 2D and 3D methods. Previous studies have demonstrated difficulties in locating landmarks, especially gonion (Go) and Menthon (Me), using computerized tracing methods.[Citation5,Citation35–37]
A previous study by Oz et al. [Citation4] also indicated an absolute difference between Go-Me and Co-Gn, which is similar to our results. Another study by Farranato et al. [Citation38] also evaluated 2D and 3D generated cephalograms using Mimicks software and found that Go-Me measurements were statistically different. They stated that 2D techniques determine the projections of these anatomical landmarks, which in reality are placed on different planes in 3D generated images. Moreover, in a previous study it was stated that conventional cephalograms may rely on the construction of multiple reference planes to assist in identifying the Co, Go, Po and Me and this may not be possible with on-screen digitalization.[Citation35]
A recent study by Michele et al. [Citation39] also evaluated 2D and 3D CBCT-generated cephalograms’ reliability in terms of linear and angular measurements. In terms of the study's intra- and inter-observer reliability, they found no statistically significant correlation between all 2D and 3D measurements. However, in their study, they did find differences for the interincisor angle, the IMPA angle and also in the intra-observer reliability of 3D cephalometric measurements. The results are also similar to our results in terms of their measurements for Wits appraisal.
Shokri et al. [Citation40] also performed a similar study with 2D and 3D generated cephalograms and concluded that several landmark measurements were different, in particular the Pog-Go.
Olszewski et al. [Citation41] researched the comparison of inter- and intra-observer reproducibility of the cephalometric measurements performed in 2D on 3D CT surface renderings on dry skulls and indicated that the reproducibility was significantly better for the measurements based on direct identification of the landmarks on 3D CT surface renderings. Nalcaci et al. [Citation6] evaluated 3D cephalometric images and traditional 2D images in terms of angular measurements. They also used a third-party software program (Mimics 9.0, Leuven, Belgium). They investigated 14 cephalometric angular measurements and showed significant differences only in the U1-NA and U1-SN measurements. Pittayapat et al. [Citation42] also evaluated the linear measurement accuracy using 2D cephalometric images and 3D generated cephalograms using Maxilim software. Overall, they found that N-A, N-Me, Go-Me, Co-Go and SmN-Go were significantly different between the tracing methods.
Another study by Zamora et al. [Citation3] evaluated whether the angular and linear measurements of 3D reconstructions obtained from CBCT are equal to those of 2D images obtained from the cephalograms using two different software packages (Beta Nemoceph 3D, Software Nemotec, SL, Madrid, Spain, and In vivo 5 Anatomage, San Jose, CA). In this study, no statistically significant differences were found for 2D and 3D generated cephalograms. There were also no statistically significant differences for any of the angular and linear measurements between the two software packages of the CBCT (NemoStudio and In vivo 5). Our study also found no statistically significant difference between 2D cephalograms (Vista Dent OC) and 3D Maxilim and In vivo software packages in most of landmarks. However, significant differences were found for the landmarks Co, Go and Me in particular. Moreover, in this study a significant difference was found between Romexis software and Maxilim and In vivo software packages. The difference between these software programs may be due to the generation technique of the cephalograms. However, it should be stated that there are difficulties in locating the landmarks Go and Me when using both manual and computerized tracing methods. Previous studies have also demonstrated low rates of reproducibility of measurements involving the points Co, Go, Me and Po.[Citation4,Citation5,Citation17,Citation37] These results are in line with our findings, which can be interpreted as meaning that the 2D conventional tracings rely on the construction of multiple reference planes to assist in identifying the Co, Go, Po and Me, which may not be possible with on-screen digitalization.[Citation4]
The 3D generated cephalograms are able to analyze actual anatomical structures rather than the 2D projections. The 3D cephalograms cannot make use of certain non-existent constructed landmarks (e.g. articulare) that are used in conventional cephalometric analysis. Recent studies have indicated that there is a need for additional new anatomical landmarks for 3D generated cephalograms. Recently, Van Vlijmen et al. [Citation2] concluded that there is a need to develop and test new 3D cephalometric systems that use 3D representations of the skull. For this purpose, Pittayapat et al. [Citation43] proposed a sella turcica landmark and evaluated the reproducibility of this landmark using CBCT data and the Maxilim software package. There is still a lack of data available for use as reference values for 3D cephalometric measurements, which should be investigated and also developed with further studies that can be applicable for different software packages.
Conclusions
In conclusion, measurements from conventional 2D digital radiographs and CBCT-generated cephalograms by a rendering software program yielded similar results with good reproducibility. However, some discrepancies still exist; especially in the identification and measurement of curved surfaces in 3D generated cephalograms. 3D imaging is essential to visualize anatomic landmarks in the maxillofacial imaging. For now all landmarks, especially for orthodontic analysis were established for 2D imaging. With the progress of 3D imaging new landmarks and analysis systems should be designed as a future attempt in this particular area.
Acknowledgments
The authors wish to thank Mr. Simon Thompson for language editing and proofreading of the manuscript.
Disclosure statement
No potential conflict of interest was reported by the authors.
Related Research Data
References
- Moshiri M, Scarfe WC, Hilgers ML, et al. Accuracy of linear measurements from imaging plate and lateral cephalometric images derived from cone-beam computed tomography. Am J Orthod Dentofacial Orthop. 2007;132:550–560.
- van Vlijmen OJ, Maal T, Bergé SJ, et al. A comparison between 2-D and 3-D cephalometry on CBCT scans of human skulls. Int J Oral Maxillofac Surg. 2010;39:156–160.
- Zamora N, Llamas JM, Cibrián R, et al. Cephalometric measurements from 3-D reconstructed images compared with conventional 2-D images. Angle Orthod. 2011;81:856–864.
- Oz U, Orhan K, Abe N. Comparison of linear and angular measurements using two-dimensional conventional methods and three-dimensional cone beam CT images reconstructed from a volumetric rendering program in vivo. Dentomaxillofac Radiol. 2011;40:492–500.
- Chien PC, Parks ET, Eraso F, et al. Comparison of reliability in anatomical landmark identification using two-dimensional digital cephalometrics and three-dimensional cone beam computed tomography in vivo. Dentomaxillofac Radiol. 2009;38:262–273.
- Nalçaci R, Oztürk F, Sökücü O. A comparison of two-dimensional radiography and three-dimensional computed tomography in angular cephalometric measurements. Dentomaxillofac Radiol. 2010;39:100–106.
- Baumrind S, Frantz RC. The reliability of head film measurements. 1. Landmark identification. Am J Orthod. 1971;60:111–127.
- Swennen GR, Schutyser F. Three-dimensional virtual approach to diagnosis and treatment planning of maxilla-facial deformity. In: Bell W, editor. Distraction osteogenesis of the facial skeleton. Hamilton, Ontario: BC Decker, Inc.; 2007. p. 55.
- van Vlijmen OJ, Bergé SJ, Swennen GR, et al. Comparison of cephalometric radiographs obtained from cone-beam computed tomography scans and conventional radiographs. J Oral Maxillofac Surg. 2009;67:92–97.
- Moreira CR, Sales MA, Lopes PM, et al. Assessment of linear and angular measurements on three-dimensional cone beam computed tomographic images. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2009;108:430–436.
- Farman AG, Scarfe WC. Development of imaging selection criteria and procedures should precede cephalometric assessment with cone beam computed tomography. Am J Orthod Dentofacial Orthop. 2006;130:257–265.
- Scarfe WC, Farman AG, Sukovic P. Clinical applications of cone beam computed tomography in dental practice. J Can Dent Assoc. 2006;72:75–80.
- Periago DR, Scarfe WC, Moshiri M, et al. Linear accuracy and reliability of cone beam CT derived three-dimensional images constructed using an orthodontic volumetric rendering program. Angle Orthod. 2008;78:387–395.
- Ludlow JB, Gubler M, Cevidanes L, et al. Precision of cephalometric landmark identification: cone beam computed tomography vs conventional cephalometric views. Am J Orthod Dentofacial Orthop. 2009;136:312–313.
- Brown AA, Scarfe WC, Scheetz JP, et al. Linear accuracy of cone beam CT derived 3-D images. Angle Orthod. 2009;79:150–157.
- Mozzo P, Procacci C, Tacconi A, et al. A new volumetric CT machine for dental imaging based on the cone beam technique: preliminary results. Eur Radiol. 1998;8:1558–1564.
- Lascala CA, Panella J, Marques MM. Analysis of the accuracy of linear measurements obtained by cone beam computed tomography (CBCT-NewTom). Dentomaxillofac Radiol. 2004;33:291–294.
- Moerenhout BA, Gelaude F, Swennen GR, et al. Accuracy and repeatability of cone-beam computed tomography (CBCT) measurements used in the determination of facial indices in the laboratory setup. J Craniomaxillofac Surg. 2009;37:18–23.
- Pinsky HM, Dyda S, Pinsky RW, et al. Accuracy of three-dimensional measurements using cone-beam CT. Dentomaxillofac Radiol. 2006;35:410–416.
- Lagravère MO, Carey J, Toogood RW, et al. Three-dimensional accuracy of measurements made with software on cone-beam computed tomography images. Am J Orthod Dentofacial Orthop. 2008;134:112–116.
- de Oliveira AE, Cevidanes LH, Phillips C, et al. Observer reliability of three-dimensional cephalometric landmark identification on cone-beam computerized tomography. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2009;107:256–265.
- Naji P, Alsufyani NA, Lagravère MO. Reliability of anatomic structures as landmarks in three-dimensional cephalometric analysis using CBCT. Angle Orthod. 2014;84:762–772.
- Sawchuk D, Alhadlaq A, Alkhadra T, et al. Comparison of two three-dimensional cephalometric analysis computer software. J Orthod Sci. 2014;3:111–117.
- Yoon YJ, Kim DH, Yu PS, et al. Effect of head rotation on posteroanterior cephalometric radiographs. Angle Orthod. 2002;72:36–42.
- Malkoc S, Sari Z, Usumez S, et al. The effect of head rotation on cephalometric radiographs. Eur J Orthod. 2005;27:315–321.
- Hassan B, van der Stelt P, Sanderink G. Accuracy of three-dimensional measurements obtained from cone beam computed tomography surface-rendered images for cephalometric analysis: influence of patient scanning position. Eur J Orthod. 2009;31:129–134.
- Kumar V, Ludlow J, Soares Cevidanes LH, et al. In vivo comparison of conventional and cone beam CT synthesized cephalograms. Angle Orthod. 2008;78:873–879.
- Harrell WE Jr. 3-D Diagnosis and treatment planning in orthodontics. Semin Orthod. 2009;15:35–41.
- Harrell WE Jr., Hatcher DC, Bolt RL. In search of anatomic truth: 3-dimensional digital modeling and the future of orthodontics. Am J Orthod Dentofacial Orthop. 2002;122:325–330.
- Harrell WE Jr., Stanford S, Bralower P. ADA initiates development of orthodontic informatics standards. Am J Orthod Dentofacial Orthop. 2005;128:153–156.
- Tepper G, Hofschneider UB, Gahleitner A, et al. Computed tomographic diagnosis and localization of bone canals in the mandibular interforaminal region for prevention of bleeding complications during implant surgery. Int J Oral Maxillofac Implants. 2001;16:68–72.
- Jacobs R, Mraiwa N, vanSteenberghe D, et al. Appearance, location, course, and morphology of the mandibular incisive canal: an assessment on spiral CT scan. Dentomaxillofac Radiol. 2002;31:322–327.
- Longoni S, Sartori M, Braun M, et al. Lingual vascular canals of the mandible: the risk of bleeding complications during implant procedures. Implant Dent. 2007;16:131–138.
- Lagravère MO, Gordon JM, Guedes IH, et al. Reliability of traditional cephalometric landmarks as seen in three-dimensional analysis in maxillary expansion treatments. Angle Orthod. 2009;79:1047–1056.
- Polat-Ozsoy O, Gokcelik A, ToygarMemikoglu TU. Differences in cephalometric measurements: a comparison of digital versus hand-tracing methods. Eur J Orthod. 2009;31:254–259.
- Santoro M, Jarjoura K, Cangialosi TJ. Accuracy of digital and analogue cephalometric measurements assessed with the sandwich technique. Am J Orthod Dentofacial Orthop. 2006;129:345–351.
- Lopes PM, Moreira CR, Perrella A, et al. 3-D volume rendering maxillofacial analysis of angular measurements by multislice CT. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2008;105:224–230.
- Farronato G, Salvadori S, Nolet F, et al. Assessment of inter- and intra-operator cephalometric tracings on cone beam CT radiographs: comparison of the precision of the cone beam CT versus the latero-lateral radiograph tracing. Prog Orthod. 2014;15:1.
- Michele C, Federica A, Roberto DG, et al. Two-dimensional and three-dimensional cephalometry using cone beam computed tomography scans. J Craniofac Surg. 2015;26:e311–e315.
- Shokri A, Khajeh S, Khavid A. Evaluation of the accuracy of linear measurements on lateral cephalograms obtained from cone-beam computed tomography scans with digital lateral cephalometric radiography: an in vitro study. J Craniofac Surg. 2014;25:1710–1713.
- Olszewski R, Zech F, Cosnard G, et al. Three-dimensional computed tomography cephalometric craniofacial analysis: experimental validation in vitro. Int J Oral Maxillofac Surg. 2007;36:828–833.
- Pittayapat P, Bornstein MM, Imada TS, et al. Accuracy of linear measurements using three imaging modalities: two lateral cephalograms and one 3-D model from CBCT data. Eur J Orthod. 2015;37:202–208.
- Pittayapat P, Jacobs R, Odri GA, et al. Reproducibility of the sella turcica landmark in three dimensions using a sella turcica-specific reference system. Imaging Sci Dent. 2015;45:15–22.