
ABSTRACT
The amount of remaining tissue and restoration of endodontically treated teeth markedly affect the survival rate of any tooth subjected to endodontic treatment. In this study, the minimally invasive approach adopted in all stages of root canal treatment from beginning to end was evaluated. An advanced search of the PubMed, Web of Science and Scopus electronic databases was performed, for articles on minimally invasive concepts in endodontics published from 2016 to 2021. A total of 594 articles were identified by the initial electronic search performed by two experts in endodontics. The summaries of the retrieved texts were evaluated in terms of their relevance to the topic of interest; those that were not relevant were eliminated. Based on our literature review, it is not possible to conclude definitively that minimally invasive approaches should always be applied. However, with appropriate case selection, minimally invasive treatment can provide a good prognosis while maintaining the tooth structure.
Introduction
There is a great deal of interest in minimally invasive treatments in the fields of dentistry and endodontics. The amount of remaining tissue and restoration of endodontically treated teeth markedly affect the survival rate of any tooth subjected to endodontic treatment. There have been a number of studies on endodontic biology, innovative diagnostic and treatment methods, and the application of new materials. Minimally invasive endodontic approaches are safe, accurate and efficient, and preserve as much of the healthy tissue as possible. The primary goal of endodontic treatment is to access, shape and clean the complicated anatomy in a way that allows efficient 3 D filling of the root canal system, while leaving the tooth with the strength necessary to maintain function [Citation1]. Prevention of pulpal and periapical disease, along with tooth retention, are the main goals of minimally invasive endodontics. In this framework, it is necessary to protect the tooth structure and supporting tissues, especially for the preservation of coronal and radicular dentin [Citation2].
Newly developed technologies and materials have emerged that allow minimally invasive endodontic procedures. The use of cone-beam computed tomography (CBCT) instead of 2 D radiography provides high-quality 3 D views of the tooth and surrounding structures, providing interrelated images in three orthogonal planes [Citation3,Citation4]. A tooth-specific and unique access design is used with static and dynamic guides based on preoperative CBCT scans [Citation5]. Novel access cavity concepts have also been introduced for use instead of traditional access cavities [Citation6,Citation7]. Rather than overextension of the root canal system, the use of instruments with smaller tapers for mechanical preparation has been proposed to preserve more dentin and reduce stress [Citation8,Citation9] from the planning and diagnosis step until the end of treatment.
Today, many file systems with different taper and cutting efficiency are available. These instruments cause varying levels of removed dentin volume and surface area in the root canals. During mechanical preparation, removing excessive amounts of dentine tissue or leaving behind uninstrumented areas causes failure [Citation10]. The target is to allow effective disinfection by being faithful to the original root canal anatomy. The access cavity design affects the chemomechanical preparation as well as the file system used. For this reason, it is beneficial to evaluate the cavity and canal preparation together. This paper presents minimally invasive concepts in endodontics.
Methods
Study design
In this study, the minimally invasive approach adopted in all stages of root canal treatment from beginning to end was evaluated. For this purpose, experimental studies on the subject in the literature were examined. Three separate databases were selected to provide a wide search.
Research strategy
This systematic review study was performed considering the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement. The clear expression of the research question was: ‘Are minimally invasive approaches more preventive than the traditional method for dental hard tissues in endodontically treated teeth?’ The population, intervention, comparison and outcome (PICO) strategy was used for the structured review question as follows:
P: Endodontically treated teeth
I: Minimally invasive cavities and canal preparations
C: Traditional root canal treatment
O: Preservation of dental hard tissue structure
An advanced search of the PubMed, Web of Science and Scopus electronic databases was performed, for articles on minimally invasive concepts in endodontics published from April 2016 to April 2021.
Keywords
The databases were searched using the following six keywords: minimally invasive access cavity; minimally invasive root canal instrumentation; root canal filling after minimally invasive preparation; restoration of minimally endodontically treated teeth; minimally invasive approach to endodontic retreatment and surgical endodontics; minimally invasive endodontics.
Eligibility evaluation
The eligibility criterion was the application of minimally invasive approaches in endodontic treatment. The target publications were original articles investigating the intraoperative and postoperative effects of the application of minimally invasive approaches in root canal treatment. Although the studies could be in vitro or in vivo, they were all required to be related to endodontic therapy.
Inclusion criteria
The inclusion criteria were articles published in the English language; published within the 5-year period 2017–2021; and full-text articles.
Literature search
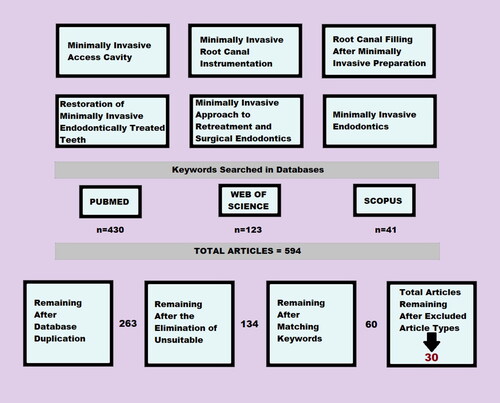
A total of 594 articles were initially retrieved in this study. The titles of the articles were screened by two authors, and only those related to the topic of interest were included. After eliminating 263 duplicate articles and those unrelated to the topic of interest, based on an evaluation of the summaries of the text, 134 papers were included. A further selection process was then applied, and 74 of the 134 articles were excluded based on the keywords.
Disagreements between the evaluators in terms of the relation between an article and a specific keyword were resolved by additional discussions with a third reviewer.
Only original articles were included; case reports, reviews, and editorials were excluded. According to these criteria, 30 full-text articles were included in the final evaluation ().
Figure 1. Database research and screening flow chart.
Nine of the selected articles (Sabeti et al. [Citation11]; Maske et al. [Citation12]; Allen et al. [Citation6]; Saberi et al. [Citation13]; Zhang et al. [Citation14]; Yuan et al. [Citation8]; Isufi et al. [Citation15]; Silva et al. [Citation16]; Jiang et al. [Citation17]) concerned the effects of minimally invasive access cavities on fracture resistance. Fourteen articles (Lin et al. [Citation18]; Rover et al. [Citation19]; Alovisi et al. [Citation20]; Freitas et al. [Citation21]; Vieira et al. [Citation22]; Lima et al. [Citation10]; Silva et al. [Citation23]; Wang et al. [Citation24]; Zogheib et al. [Citation25]; Rover et al. [Citation26]; Plotino et al. [Citation9]; Moore et al. [Citation27]; Cheng et al. [Citation28]; Pérez et al. [Citation29]) were related to the effects of minimally invasive design on root canal shaping, cleaning, and filling. Three articles (Nayak et al. [Citation30]; Jain et al. [Citation31]; Gambarini et al. [Citation32]) described the use of guides in endodontics. Four articles (Özyürek et al. [Citation33]; Silva et al. [Citation34]; Fráter et al. [Citation35]; Belleflamme et al. [Citation36]) were related to restoration of endodontically treated teeth.
Results
A total of 594 articles were identified by the initial electronic search of the PubMed, Web of Science and Scopus databases. All searches and screening were performed by two experts in endodontics. The article search was performed separately for each keyword and database. The summaries of the retrieved texts were evaluated in terms of their relevance to the topic of interest; those that were not relevant were eliminated. In total, 60 articles were saved, including 30 original articles, 21 case reports, 7 review articles, and 2 editorials. The 30 full-text original articles were examined. Nine of the original articles were related to minimally invasive access cavities, the fracture resistance of teeth and the amount of coronal cervical dentin removed. Fourteen studies aimed to evaluate the effectiveness of minimally invasive access cavities in root canal preparation, irrigation and canal filling. The use of guides and navigation systems for minimally invasive treatment was discussed in three of the articles. The characteristics of restorations for endodontically treated teeth were presented in another seven original articles ().
Table 1. Results of studies with minimally invasive approach.
Discussion
New types of cavity preparations are presented as alternatives to traditional endodontic cavities (TECs). Conservative access cavities (CACs), ultraconservative access cavities (UCACs) and truss access cavities (TRACs) have been described in the literature as a means of minimizing weakening of the structure [Citation7] ( and ). Different results were obtained in studies examining various cavity designs. Isufi et al. [Citation15] compared the rate of hard tissue removal among various types of access cavities. The results showed that the volume of dentin and enamel removed increased in order from UCAC to CAC, and finally to TAC. The authors suggested standardization using CBCT to distinguish between different endodontic cavities in subsequent studies [Citation15]. This could help to identify cavities and avoid confusion among researchers.
Figure 2. Occlusal view in lower molar tooth: (a) traditional endodontic access cavity illustration; (b) conservative endodontic access cavity; (c) ultraconservative endodontic access cavity; (d) truss endodontic access cavity.
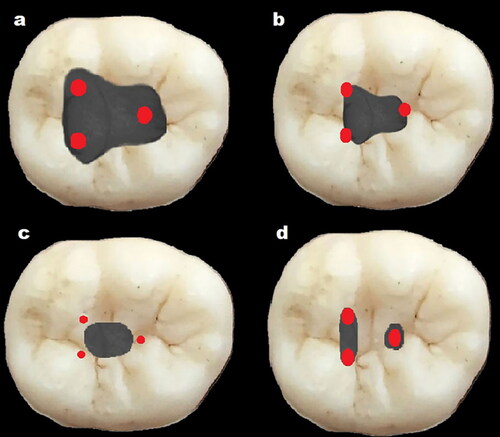
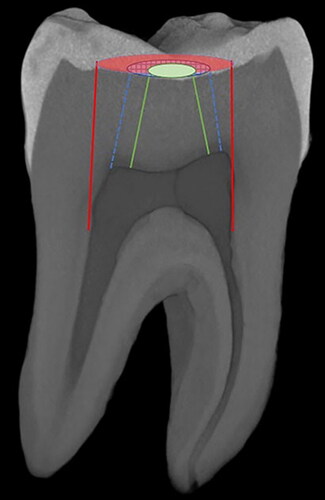
Figure 3. Micro-ct image of lower molar tooth from lateral view. Red area and lines indicate border of traditional endodontic access cavity. Blue area and lines indicate border of conservative endodontic access cavity. Green area and lines indicate border of ultraconservative endodontic access cavity.
Dental fractures are serious because they can necessitate tooth extraction [Citation11]. Minimally invasive approaches reduce the risk of fracture in teeth with filled root canals. Removal of decayed tissue and creation of an access cavity are important in root canal treatment. Allen et al. [Citation6] reported that a TEC may make the tooth more susceptible to fracture than a minimally invasive design. It has been suggested that root fracture may occur depending on the amount of tissue removed from the pericervical area during preparation of the access cavity. Previous studies indicated that the cervical area is exposed to greater stress as the cavity volume increases. Yuan et al. [Citation8] reported that the use of a minimally invasive approach reduced the stress distribution in the crown and cervical areas.
On the other hand, Silva et al. [Citation16] reported that UCACs were not associated with resistance to fracture. Consistent with this view, Sabeti et al. [Citation11] reported that there was no significant difference in fracture resistance between TACs and CACs. Maske et al. [Citation12] showed that the cavity type does not affect the fracture resistance of endodontically treated teeth. Despite the results of the above studies, the authors acknowledged the contribution of preservation of the tooth structure around the pulp chamber and pericervical region to durability.
Saberi et al. [Citation13] examined thermal stresses in teeth using a device that simulates temperature changes in the oral cavity. In their study comparing TRACs and TACs, the TRAC design increased the fracture resistance of endodontically treated teeth under thermal loads [Citation13].
The occlusal surface of the crown of the maxillary first molar teeth has grooves and cristae that extend between the mesiopalatal and distobuccal tubercles. Zhang et al. [Citation14] reported that the mesial groove is the beginning point of fracture in first molar teeth with the application of force. The same study indicated that stress in the cervical region was higher in TAC and modified cavity teeth than in CAC. In addition, it was emphasized that removing less hard tissue during preparation increases the fracture resistance of the teeth [Citation14]. In another study performed in the maxillary first molar, a similar stress distribution was observed on the occlusal surface in different types of cavities, but the stress on the pericervical dentin was more evident in large cavities [Citation17].
Effective shaping, cleaning, and filling are important for successful root canal treatment. Many instruments varying in flexibility and metallurgical properties have been produced for canal preparation. Performing canal instrumentation by removing less tissue with a minimally invasive technique is a new approach. Using smaller tapered files supports preservation of root dentin and reduces stress, especially in the coronal third of the tooth [Citation10]. However, removal of less dentin from the canal has disadvantages, such as inadequate disinfection of necrotic pulp. Effective irrigation is essential for cleaning the root canals from microorganisms. If root canals are not cleaned sufficiently, apical periodontitis cannot heal in infected teeth [Citation22]. Therefore, clinicians must decide whether a given case is suitable for minimally invasive treatment. Wang et al. [Citation24] reported that while a small tapered canal preparation reduces stress on teeth, the design of the access cavity is more important.
Mechanical instrumentation and disinfection play major roles in the success of root canal treatment. At this stage, elimination of the residual debris and smear layer is an important consideration. The amount of debris produced from the canal wall varies among files with different designs and tapers. Plotino et al. [Citation9] observed that a 25-size instrument created a cleaner canal surface than a 20-size one in the apical third of the root canal. Moreover, apical enlargement should be sufficient to achieve strong antimicrobial efficacy, even if the irrigation solution is activated with a sonic device [Citation9]. Perez et al.’s study [Citation29] highlighted another point that unprepared canal area was observed after each increase in preparation size.
After preparation, the canal diameter can affect the resistance of the root to forces generated during function. However, in another study, decreasing the taper to 4% did not statistically increase the fracture resistance of maxillary premolars treated endodontically compared to the 6% taper [Citation25].
The endodontic access cavity affects the operator’s ability to manipulate and shape the root canal with a suitable file system. According to Moore et al. [Citation27], CACs in maxillary molars did not seem to affect the instrumentation efficacy and biomechanical responses compared with TACs. On the other hand, Alovisi et al. [Citation20] reported that TACs may supply a better protection of the original canal anatomy during shaping compared with CACs, especially the apical third. If the instrument works more inner surface of the canal, apical transportation can occur [Citation20]. Unfortunately, this can be observed in minimally accessed teeth. Interestingly, in the study of Freitas et al. [Citation21], there was no difference between cavity designs in the operation of the instrument in curved root canals.
Another important consideration is that the quality of root canal filling depends on its resistance to leakage and the tightness of the fit. Rover et al. [Citation19] observed more voids in the canal fillings of teeth prepared with minimally invasive access cavities. This suggests that a small access cavity is inadequate for entry to the canal to fill the oval-shaped canal of the mandibular incisors.
Endodontic treatment of teeth with a calcified pulp chamber and root canal is difficult. New technologies, such as use of endodontic operation microscopes, guides, and superior imaging techniques, allow the detection of calcified canals. The use of a guide enables minimally invasive treatment that prevents undesirable tissue loss and perforations by simulating the 3 D structure of the root canal anatomy [Citation30]. Moreover, dynamic navigation systems create only small cavities and facilitate access to obliterated canal pulp via drills operating at high speeds [Citation31].
After the root canal treatment is completed, permanent restoration of the teeth should be done. Different restorations can be considered depending on the amount of hard tissue loss. An endocrown design for the restoration of endodontically treated teeth with large amounts of structural material loss can be applied if there is retention of at least 2 mm of the material in the pulp chamber. Endocrown restorations are less invasive compared to post and core restorations, which have a negative effect on the root [Citation36]. In cases that can be restored with bonded composite resins, the shape and size of the cavity are important in terms of the durability of the material. With the developing adhesive technology, there are various alternative applications. In a study on this topic, there was no difference in fracture resistance between TAC and CAC in the groups using the same composite material [Citation33].
Conclusions
Minimally invasive treatments have been widely adopted in endodontics recently. Generally, this type of treatment is intended to reduce hard tissue loss. Based on our literature review, it is not possible to conclude definitively that minimally invasive approaches should always be applied. However, with appropriate case selection, minimally invasive treatment can provide a good prognosis while maintaining the tooth structure.
Acknowledgments
The authors deny any conflicts of interest related to this study.
Data availability statement
The data supporting the findings of this study are available at: https://doi.org/10.17632/tbvb5t4xh6.1.
Disclosure statement
No potential conflict of interest was reported by the authors.
Funding
The author(s) reported there is no funding associated with the work featured in this article.
References
- Mukherjee P, Patel A, Chandak M, et al. Minimally invasive endodontics a promising. Future concept: A review article. Int J Sci Study. 2015:2015.
- Gutmann JL. Minimally invasive dentistry (endodontics). J Conserv Dent. 2013;16(4):282–283.
- Patel S, Brown J, Pimentel T, et al. Cone beam computed tomography in endodontics – a review of the literature. Int Endod J. 2019;52(8):1138–1152.
- Parker J, Mol A, Rivera E, et al . CBCT uses in clinical endodontics: the effect of CBCT on the ability to locate MB2 canals in maxillary molars. Int Endod J. 2017;50(12):1109–1115.
- Connert T, Krug R, Eggmann F, et al. Guided endodontics versus conventional access cavity preparation: a comparative study on substance loss using 3-dimensional-printed teeth. J Endod. 2019;45(3):327–331.
- Allen C, Meyer CA, Yoo E, et al. Stress distribution in a tooth treated through minimally invasive access compared to one treated through traditional access: a finite element analysis study. J Conserv Dent. 2018;21(5):505–509.
- Silva E, Pinto KP, Ferreira CM, et al. Current status on minimal access cavity preparations: a critical analysis and a proposal for a universal nomenclature. Int Endod J. 2020;53(12):1618–1635.
- Yuan K, Niu C, Xie Q, et al. Comparative evaluation of the impact of minimally invasive preparation vs. conventional straight-line preparation on tooth biomechanics: a finite element analysis. Eur J Oral Sci. 2016;124(6):591–596.
- Plotino G, Özyürek T, Grande NM, et al. Influence of size and taper of basic root canal preparation on root canal cleanliness: a scanning electron microscopy study. Int Endod J. 2019;52(3):343–351.
- Lima C, Barbosa A, Ferreira C, et al. The impact of minimally invasive root canal preparation strategies on the ability to shape root canals of mandibular molars. Int Endod J. 2020;53(12):1680–1688.
- Sabeti M, Kazem M, Dianat O, et al . Impact of access cavity design and root canal taper on fracture resistance of endodontically treated teeth: an ex vivo investigation. J Endod. 2018;44(9):1402–1406.
- Maske A, Weschenfelder VM, Soares Grecca Vilella F, et al. Influence of access cavity design on fracture strength of endodontically treated lower molars. Aust Endod J. 2021;47(1):5–10.
- Saberi EA, Pirhaji A, Zabetiyan F. Effects of endodontic access cavity design and thermocycling on fracture strength of endodontically treated teeth. CCIDE. 2020;Volume 12:149–156.
- Zhang Y, Liu Y, She Y, et al. The effect of endodontic access cavities on fracture resistance of first maxillary molar using the extended finite element method. J Endod. 2019;45(3):316–321.
- Isufi A, Plotino G, Grande NM, et al. Standardization of endodontic access cavities based on 3-dimensional quantitative analysis of dentin and enamel removed. J Endod. 2020;46(10):1495–1500.
- Silva E, Lima C, Barbosa A, et al. Preserving dentine in minimally invasive access cavities does not strength fracture resistance of restored mandibular molars. Int Endod J. 2021;54(6):966–974.
- Jiang Q, Huang Y, Tu X, et al. Biomechanical properties of first maxillary molars with different endodontic cavities: a finite element analysis. J Endod. 2018;44(8):1283–1288.
- Lin C-Y, Lin D, He W-H. Impacts of 3 different endodontic access cavity designs on dentin removal and point of entry in 3-dimensional digital models. J Endod. 2020;46(4):524–530.
- Rover G, Lima CO, Belladonna FG, et al. Influence of minimally invasive endodontic access cavities on root canal shaping and filling ability, pulp chamber cleaning and fracture resistance of extracted human mandibular incisors. Int Endod J. 2020;53(11):1530–1539.
- Alovisi M, Pasqualini D, Musso E, et al . Influence of contracted endodontic access on root canal geometry: an in vitro study. J Endod. 2018;44(4):614–620.
- Freitas GR, Ribeiro TM, Vilella FSG, et al. Influence of endodontic cavity access on curved root canal preparation with ProDesign logic rotary instruments. Clin Oral Investig. 2021;25(2):469–475.
- Vieira GC, Pérez AR, Alves FR, et al. Impact of contracted endodontic cavities on root canal disinfection and shaping. J Endod. 2020;46(5):655–661.
- Silva EJNL, Attademo RS, da Silva MCD, et al. Does the type of endodontic access influence in the cyclic fatigue resistance of reciprocating instruments? Clin Oral Invest. 2021;25(6):3691–3698.
- Wang Q, Liu Y, Wang Z, et al. Effect of access cavities and canal enlargement on biomechanics of endodontically treated teeth: a finite element analysis. J Endod. 2020;46(10):1501–1507.
- Zogheib C, Sfeir G, Plotino G, et al. Impact of minimal root canal taper on the fracture resistance of endodontically treated bicuspids. J Int Soc Prev Community Dent. 2018;8(2):179–183.
- Rover G, Belladonna FG, Bortoluzzi EA, et al. Influence of access cavity design on root canal detection, instrumentation efficacy, and fracture resistance assessed in maxillary molars. J Endod. 2017;43(10):1657–1662.
- Moore B, Verdelis K, Kishen A, et al. Impacts of contracted endodontic cavities on instrumentation efficacy and biomechanical responses in maxillary molars. J Endod. 2016;42(12):1779–1783.
- Cheng X, Tian T, Tian Y, et al . Erbium:yttrium aluminum garnet laser-activated sodium hypochlorite irrigation: a promising procedure for minimally invasive endodontics . Photomed Laser Surg. 2017;35(12):695–701.
- Pérez A, Alves F, Marceliano-Alves M, et al. Effects of increased apical enlargement on the amount of unprepared areas and coronal dentine removal: a micro-computed tomography study. Int Endod J. 2018;51(6):684–690.
- Nayak A, Jain PK, Kankar P, et al . Computer-aided design-based guided endodontic: A novel approach for root canal access cavity preparation. Proc Inst Mech Eng H. 2018;232(8):787–795.
- Jain SD, Carrico CK, Bermanis I. 3-Dimensional accuracy of dynamic navigation technology in locating calcified canals. J Endod. 2020;46(6):839–845.
- Gambarini G, Galli M, Morese A, et al. Precision of dynamic navigation to perform endodontic ultraconservative access cavities: a preliminary in vitro analysis. J Endod. 2020;46(9):1286–1290.
- Özyürek T, Ülker Ö, Demiryürek EÖ, et al. The effects of endodontic access cavity preparation design on the fracture strength of endodontically treated teeth: traditional versus conservative preparation. J Endod. 2018;44(5):800–805.
- Silva EJNL, Oliveira V, Silva A, et al. Effect of access cavity design on gaps and void formation in resin composite restorations following root canal treatment on extracted teeth. Int Endod J. 2020;53(11):1540–1548.
- Fráter M, Forster A, Jantyik Á, et al . In vitro fracture resistance of premolar teeth restored with fibre-reinforced composite posts using a single or a multi-post technique . Aust Endod J. 2017;43(1):16–22.
- Belleflamme MM, Geerts SO, Louwette MM, et al. No post-no core approach to restore severely damaged posterior teeth: an up to 10-year retrospective study of documented endocrown cases. J Dent. 2017;63:1–7.