
Abstract
This study aimed to characterize the morphology of the first permanent molars affected by molar-incisor hypomineralization (MIH) using a light microscope (LM) and scanning electronic microscope (SEM). A total of 8 teeth were divided into two groups: experimental group − 4 first permanent molars being clinically diagnosed as MIH, and control group − 4 sound and healthy first permanent molars. The free surfaces of each tooth were split in half across in a buccolingual direction and then were examined using SEM and LM. Under LM observation the hypomineralized enamel appeared opaquer and demonstrated areas of porosity. The SEM observation of enamel with MIH revealed superficial defects which embedded numerous colonies of microorganisms as well as disorganized prisms and loosely packed crystallites. Our results support the idea that there is a significant distinction between the structure of MIH-affected and sound unaffected enamel. The clinical appearance of MIH-affected enamel correlated with the severity of enamel changes.
Introduction
Molar-Incisor Hypomineralization (MIH), firstly introduced by Weerheijm et al., was approved by the dental scientific community worldwide [Citation1]. Generally, MIH is defined as a qualitative morphological defect of the enamel involving the occlusal and/or incisal third of one or more permanent molars and/or incisors due to ‘hypomineralisation of systemic origin’ [Citation2–4]. An analysis conducted by Jalevik et al. indicated that the systemic factors during the first age of childhood played a profound role concerning MIH disturbance [Citation5]. The immature structure of these teeth is the reason for rough and opaque lesions which result in rapid caries development and post-eruptive breakdown [Citation6].
As reviewed by [Citation7], despite the lack of certain evidence, the most likely reason for MIH was the disturbance of the secretory function of the ameloblasts resulting in restriction of crystal elongation and information of hypomineralized enamel [Citation5,Citation7–9]. In contrast, Xie et al., Crombie et al., and Bozal et al. found defects that were most likely to occur during the enamel maturation, especially during the early mineralization stage, consistent with the retention of enamel matrix, i.e. ameloblastin [Citation3,Citation10,Citation11].
Some authors found that there was a difference in the physical, chemical, and mechanical properties of the enamel between MIH-affected teeth and the healthy and sound ones [Citation12]. However, the total number of all morphologically studied teeth with MIH is still limited. Recent investigations which focused on the ultrastructure and mineral composition of the enamel surface of teeth affected by MIH demonstrated an increased amount of carbon resulting in increased organic content as well as decreased proportions of Ca and P and the ratio Ca/P [Citation3,Citation5,Citation10,Citation11]. Bozal et al. reported higher proportions of Ca and P on the enamel surface which were not packed and could not be included in the formation of prismatic structures, however [Citation10]. In addition, significantly lower hardness values in the hypomineralized enamel were found in comparison with the normal enamel, varying according to the chemical properties and morphology [Citation8,Citation13].
Polarized light microscopy (LM), scanning electron microscopy (SEM) and transmission electron microscopy (TEM) were used for the microstructural investigation of hard dental tissues to observe the changes associated with hypomineralization [Citation3,Citation8,Citation10]. The most significant clinical problems deriving from MIH microstructure include poor aesthetics, high caries susceptibility, hypersensitivity, anesthetic failure, and difficulty in adhesion related to the adhesive restoration of the lesions. Knowledge of the specific structural abnormalities associated with MIH will provide dental practitioners, especially paediatric dentists, with fundamental benefits in the early prevention and successful treatment of such teeth [Citation7].
Aim
The study is aimed to characterize the morphology of the first permanent molars affected by Molar-Incisor Hypomineralization (MIH) using a LM and SEM.
Material and methods
Ethics statement
The parents gave written informed consent.
Tooth extraction
After obtaining the parents’ written informed consent, a total of 8 teeth were extracted from 8 patients aged from 8 to 17 years (mean age 12.00 ± 3.85) divided into two groups: experimental group: 4 first permanent molars being clinically diagnosed as MIH according to the Judgement Criteria for MIH of the European Academy of Paediatric Dentistry [Citation14]; and control group: 4 sound and healthy first permanent molars.
Reasons for tooth extraction of the investigated teeth were as follows:
in the experimental group – history of dental pain, followed by failure of the endodontic treatment in combination with incomplete root development of teeth with severe MIH defects (level of severity of the defects according to EAPD criteria [Citation14])
in the control group – orthodontic treatment (reasons unrelated to the study).
After extraction, each tooth was stored in 0.1% thymol in an individual container with a unique ID code at 4 °C in the refrigerator.
Experimental design
The free surfaces of each tooth were split in half across in buccolingual direction.
Eight of the halves (four from the experimental group and four from the control group) were thoroughly rinsed with distilled water and gently dried, then they were mounted and sputter-coated with gold nanoparticles (ELMI Sputter) for observation under a SEM (JEOL 6390, USA). Various magnifications were used.
The other eight halves (four from the experimental group and four from the control group) were divided into two groups:
Group 1 - Ground sections of 100 µm thickness were made using hard tissue microtome. A self-cure acrylic resin was used as the embedding medium. After making the sections of desired thickness, the sections (MIH and control) were studied under LM for histological changes.
Group 2 - Four halves were fixed in 10% neutral buffered formalin for 7 days before being demineralized in 10% formic acid containing 2% formalin for 7 days. Samples were then dehydrated (70% IMS-denatured alcohol ×2, 90% IMS ×2, 100% IMS ×3, xylene ×3, paraffin wax ×3) before being blocked in wax. Ten transverse sections, 6 mm thick were cut from each sample, mounted on poly-lysine slides, and heat-fixed prior to staining using the Brown and Brenn method. Penetration of bacteria into dentine was visualized by LM at ×400 magnification.
Data analysis
The obtained data were processed and analyzed using SPSS (Statistical Package for Social Science software) version 21.0 (IBM, the USA). Spearman correlation coefficient was used. Differences were considered statistically at the p˂0.05 level.
Results
The enamel of the control group (teeth without MIH) had a normal appearance. Clinically, the MIH affected teeth represent mild (cream-white colored) and moderate (brown-yellow) hypomineralization lesions. Similar to previous reports [Citation5], the present results indicated pore size variations in the structure of the enamel of MIH-affected teeth. A great number of porous defects throughout the entire width of the enamel were observed in the yellowish/brownish zones. In contrast, a limited number of pores were found only in the inner layer of enamel in the opaque-white zones.
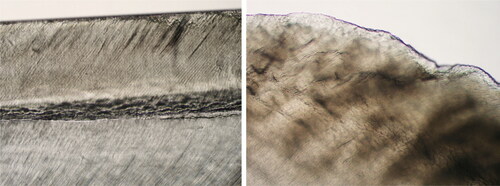
Under LM observation, the ground sections of the normal enamel revealed homogenously mineralized enamel that gave a translucent appearance while the hypomineralized enamel (MIH) appeared opaquer in incident light. () The colour of the hypomineralized enamel varied from white to beige.
Figure 1. Light microscopic view of a ground section of normal and hypomineralized enamel. Normal mineralized enamel gave a translucent appearance. (×10 magnification) Hypomineralized enamel appeared more opaque than normal in incident light (the colour was white to beige). (×40 magnification).
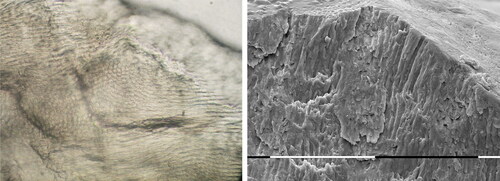
The SEM observation of the hypomineralized enamel (MIH) revealed minimal loss of substance due to mechanical abrasion (). The current results demonstrated that mild hypomineralization of the enamel surface was associated with porous occasional cracks with concavities and the presence of different planes, giving the surface a staggered/layered appearance. Higher porosity, bigger concavities, larger cracks, and a large quantity of scale-like lesions were found in the zones of moderate hypomineralization. The superficial defects embedded numerous colonies of microorganisms organized in biofilm (). The enamel with hypomineralization (MIH) had no typical features of prismatic enamel. The cross-section view showed that the apatite crystals had more rounded ends than in the control group specimens. The enamel exhibited disorganized enamel prisms, a porous structure, and loosely packed crystallites. () The enamel on the control group (teeth without MIH) had a prismatic surface without structural alterations.
Figure 2. Scale-like lesions and loss of structure with trasological evidence for mechanical abrasion ×150 and ×6000.
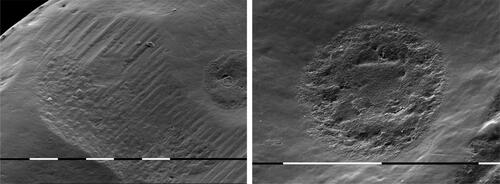
Figure 3. The concavities of the porous hypomineralized enamel embedded bacterial colonies. ×1500 and ×3000.
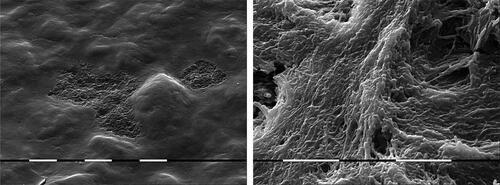
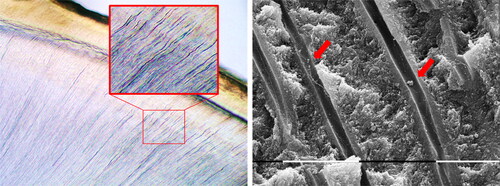
Figure 4. Light microscopic view of a ground section of enamel affected by MIH (×40 magnification) and SEM microphotography of enamel affected by MIH. The enamel exhibits disorganized enamel prisms, a porous structure, and loosely packed crystallites. (×40 magnification and ×500).
There was a significantly positive correlation between the clinical appearance and the severity of the structural changes found in the enamel of MIH-affected teeth (r = 0.437, p ≤ 0.001). Such a difference was not observed when sound unaffected enamel was investigated (p > 0.05).
The stained sections from the cuspal areas, below the hypomineralized enamel, demonstrated the presence of bacteria in the dentinal tubules. In some areas, many tubules were positive for bacterial penetration. The SEM analyses showed dentinal tubules without any odontoblast but filled with bacteria ().
Figure 5. Bacterial invasion in dentinal tubules under intact but hypomineralized enamel. In sections near the cuspal parts of the hypomineralized enamel, the dentinal tubules showed bluish staining, indicating the presence of Gram-positive bacteria. The SEM observation revealed severely contaminated dentinal tubules. (×40 magnification and ×4000).
Discussion
There are few morphological studies on MIH with controversial conclusions [Citation3,Citation8,Citation11]. The results from our study confirmed that the morphological characteristics of the enamel in teeth with MIH differ considerably from what is found in normal enamel [Citation3,Citation5,Citation8,Citation10]. In line with previous SEM studies, the present findings demonstrated a porous surface of the MIH-affected teeth that entirely corresponded with the chemical, mechanical and physical properties of the tissue [Citation3,Citation5,Citation10].
In agreement with previous observations [Citation7], the microstructural analysis demonstrated that there are two major structural abnormalities of MIH-affected teeth. On the one hand, the mean size of the enamel rod sheath regions was larger compared to the normal one [Citation15]. On the other hand, there was lower density in combination with loosely packed apatite crystals.
Jalevik et al. reported more or less blurred borders of the rods and undistinguishable interrod zones varying according to the degree of hypomineralization and structural decomposition pattern [Citation5]. In our study, a bad organization, as well as less tight packing of the apatite crystals, were found which were similar to the results reported in recent studies [Citation16,Citation17]. The borders of the enamel rods were indistinct and the interrod zones hardly visible, or the rods were very thin with wide interrod zones like described by Jalevik et al., Fagrell et al., and Xie et al. [Citation3,Citation5,Citation8]. In line with several studies, the current SEM investigation described porous enamel composed of prisms with more rounded ends than in the normal healthy enamel [Citation8,Citation10]. Moreover, the prisms were ‘coated’ by a structureless layer due to the increased amount of organic compound found in MIH specimens [Citation8]. However, the borderline between the affected and healthy enamel was distinct [Citation5]. These findings raise the question of the effectiveness of the current adhesive strategies in teeth with MIH. Thus, some authors recommended the removal of all affected enamel surrounding the cavity, whereas others tried a pretreatment with 5% NaClO [Citation18].
Fagrell et al. examined in histological and SEM study the presence of bacteria in the dentinal tubules beneath apparently intact, but hypomineralized enamel in MIH-affected permanent molars [Citation8]. The authors found that the stained sections from the coronal areas, below the hypomineralized enamel, indicated the presence of bacteria in the dentinal tubules close to the DEJ. In a recent study, the presence of bacteria under the intact enamel layer was also confirmed [Citation11]. The authors reported the extremely porous enamel as a possible explanation of the bacterial penetration [Citation8]. In 2020, Krishnan et al. assesses the enamel permeability of MIH-affected enamel using SEM [Citation19]. The investigators found a high presence of droplets resulting in high permeability in comparison with the healthy tooth surface, which appeared to be an important risk factor for dental caries [Citation11]. As previously emphasized by Fagrell et al. [Citation20], these findings have significant clinical importance demonstrating possible bacterial penetration from hypomineralized enamel towards dentin resulting in hypersensitivity of MIH-affected teeth. In this situation, the applications of different protective strategies (remineralization, coating with fluoride varnish, etc.) are reasonable.
The main contribution of this study is to enrich the world database on MIH with new morphological evidence and to emphasize the necessity of new preventive and treatment strategies. However, the limitations of the study, such as the small sample size, emphasize the need for future studies to investigate these structural abnormalities in permanent teeth to obtain more reliable results.
Conclusions
Our results support the idea that there is a significant distinction between the structure of MIH-affected and sound unaffected enamel. There is a correlation between the clinical appearance of MIH-affected enamel and the severity of enamel changes. The presence of bacteria in the dentinal tubules under the intact enamel layer with MIH requires preventive strategies to arrest the spreading of the infection in depth. Extensive research is warranted to enhance further the effectiveness of common attempts for remineralization on enamel affected by MIH.
Acknowledgments
We would like to thank the managing director of the Institute of Mineralogy and Crystallography of the Bulgarian Academy of Science, for valuable comments and support during this project.
Disclosure statement
No potential conflict of interest was reported by the authors.
Data availability statement
The data supporting the findings of this study are available from the authors upon reasonable request.
Funding
The author(s) reported there is no funding associated with the work featured in this article.
References
- Weerheijm KL, Jälevik B, Alaluusua S. Molar-incisor hypomineralisation. Caries Res. 2001;35(5):390–391.
- Weerheijm KL. Molar incisor hypomineralization (MIH): clinical presentation, aetiology and management. Dent Update. 2004;31(1):9–12.
- Xie Z, Kilpatrick NM, Swain MV, et al. Transmission electron microscope characterisation of molar-incisor-hypomineralisation. J Mater Sci Mater Med. 2008;19(10):3187–3192.
- Glodkowska N, Emerich K. Molar incisor hypomineralization: prevalence and severity among children from nothern Poland. Eur J Paediatr Dent. 2019;20(1):59–66.
- Jälevik B, Dietz W, Norén JG. Scanning electron micrograph analysis of hypomineralized enamel in permanent first molars. Int J Paediatr Dent. 2005;15(4):233–240.
- Raposo F, de Carvalho Rodrigues AC, Lia ÉN, et al. Prevalence of hypersensitivity in teeth affected by Molar-Incisor hypomineralization (MIH). Caries Res. 2019;53(4):424–430.
- Dos Santos MA, Cople Maia L. 2012. Molar incisor hypomineralization: morphological, aetiological, epidemiological and clinical considerations, contemporary approach to dental caries, Ming-yu Li, IntechOpen, Available from: https://www.intechopen.com/chapters/32183.
- Fagrell TG, Dietz W, Jälevik B, et al. Chemical, mechanical and morphological properties of hypomineralized enamel of permanent first molars. Acta Odontol Scand. 2010;68(4):215–222.
- Li M. 2012. Contemporary approach to dental caries. Croatia: InTech.
- Bozal CB, Kaplan A, Ortolani A, et al. Ultrastructure of the surface of dental enamel with molar incisor hypomineralization (MIH) with and without acid etching. Acta Odontol Latinoam. 2015;28(2):192–198. https://doi.org/10.1590/S1852-48342015000200016.
- Crombie FA, Manton DJ, Palamara JE, et al. Characterisation of developmentally hypomineralised human enamel. J Dentist. 2013;41(7):611–618.
- Elhennawy K, Manton DJ, Crombie F, et al. Structural, mechanical and chemical evaluation of molar-incisor hypomineralization-affected enamel: a systematic review. Arch Oral Biol. 2017;83:272–281.
- Noor M. 2014. Phenotypic properties of enamel in molarincisor hypomineralisation (MIH) and amelogenesis imperfecta (AI) teeth [Doctoral dissertation]. Eastman Dental Institute, University of College London. Available from: https://discovery.ucl.ac.uk/id/eprint/1448706/1/Mohd_Noor_Final_Thesis.pdf.redacted.pdf.
- Weerheijm KL, Duggal M, Mejare I, et al. Judgement criteria for molar-incisor-hypomineralisation (MIH) in epidemiologic studies: a summary of the european meeting on MIH held in athens. Eur J Pediatr Dent. 2003;4:110–113.
- Salvati E, Besnard C, Harper RA, et al. Finite element modelling and experimental validation of the enamel demineralisation process at the rod level. J Adv Res. 2021;29:167–177.
- Almuallem Z, Busuttil-Naudi A. Molar incisor hypomineralisation (MIH) – an overview. Br Dent J. 2018;225(7):601–609.
- Dos Santos MPA, Cople L. Molar incisor hypomineralization: Morphological, aetiological, epidemiological and clinical considerations. In: Li M-Y, editor. Contemporary approach to dental caries. Rijeka (Croatia): InTech; 2012. p. 423–446.
- Venezie RD, Vadiakas G, Christensen JR, et al. Enamel pretreatment with sodium hypochlorite to enhance bonding in hypocalcified amelogenesis imperfecta: case report and SEM analysis. Pediatr Dent. 1994;16(6):433–436.
- Krishnan R, Al Wadei MM, Al Qahthani MT, et al. Assessment of enamel permeability using scanning electron microscopy in permanent teeth with and without molar incisor Hypomineralisation-An in vivo study. J Clin Diagn Res. 2020;14(2):ZC18–ZC22.
- Fagrell TG, Lingström P, Olsson S, et al. Bacterial invasion of dentinal tubules beneath apparently intact but hypomineralized enamel in molar teeth with molar incisor hypomineralization. Int J Paediatr Dent. 2008;18(5):333–340.
- Lygidakis NA, Dimou G, Briseniou E. Molar-Incisor-Hypomineralisation (MIH). retrospective clinical study in greek children. I. Prevalence and defect characteristics. Eur Arch Paediatr Dent. 2008;9(4):200–206.