
Abstract
Ischemic stroke (IS) is a multifaceted, complicated illness resulting from a confluence of genetic, environmental and vascular risk factors. Many genes that may contribute to ischemic stroke have been discovered in humans. The genetic contribution appears to be greater in IS patients with hypertension. There is conflicting evidence about a positive correlation between the AGT M235T polymorphism and ischemic stroke. The aim of this study was to examine the possible association of the AGT M235T gene polymorphism with the risk of ischemic stroke. A hospital-based case-control study was carried out in 36 ischemic stroke patient cases and 36 age- and sex-matched healthy controls. Clinical parameters were measured to assess the associated risk factors. DNA was isolated from blood samples, and the AGT M235T genotypes were identified using polymerase chain reaction (PCR) and analyzed by agarose gel electrophoresis. The AGT-TT genotype (OR = 4.64, 95% CL = 1.23–17.4; p = 0.023 and T allele (OR = 2.54, 95% CL = 1.28–5.02; p = 0.003) were significantly more common in patients than in controls, indicating that it may be a major risk factor for the development of ischemic stroke. The results suggest that there may be a significant correlation between the AGT M235T gene polymorphism and the development of ischemic stroke in the studied Ethiopian population.
Introduction
Ischemic stroke (IS) is the loss of brain tissue caused by a cessation of blood supply to a region of the brain caused by a blockage of a carotid or vertebral artery, and it has become the world’s second leading cause of disability and death [Citation1]. Age, sex, body mass index (BMI), type 2 diabetes (T2DM), hyperlipidemia, smoking and hypertension (HTN) are all risk factors for IS [Citation2]. The occurrence of IS has also been linked to genetic variables, either directly or via modulating the effects of the above-mentioned risk factors [Citation3]. HTN raises the relative risk 3.1 times for men and 2.9 times for women, making it the most important modifiable risk factor for IS, where the incidence of stroke rises proportionately with both systolic and diastolic blood pressure [Citation2]. The decrease in IS mortality over the past ten years can be partly accredited to the intensive management of HTN and dyslipidemia which is prevalent in the group of stroke victims [Citation4].
A vital component of the rennin-angiotensin-aldosterone system (RAAS), angiotensinogen (AGT) interacts with renin to produce angiotensin I, a precursor to angiotensin II, and is crucial for maintaining fluid homeostasis and controlling blood pressure [Citation5]. AGT is a 12 kb long gene on chromosome 1 (1q42–q43) that belongs to the serpin gene superfamily and has 5 exons and 4 introns. This gene’s M235T polymorphism (rs699), which is caused by a thymine to cytosine substitution at nucleotide 704, causes the methionine (M) residue to be replaced by a threonine (T) residue at amino acid position 235 [Citation6]. When compared to those with the MM genotype, those with the TT genotype have higher blood pressure and plasma AGT levels because of the AGT-M235T polymorphism [Citation7].
The AGT gene is a significant contributor to the aetiology of atherosclerosis and HTN-induced IS, as well as vascular homeostasis [Citation8]. Even though the AGT M235T gene polymorphism has been widely studied in cardiovascular and cerebrovascular diseases, the findings of research on the role of this polymorphism in IS are contradictory and provide conflicting data [Citation9,Citation10]. Furthermore, although a number of studies have estimated the prevalence, risk factors and outcome of IS in the Ethiopian population [Citation11], there are no reported data about the effect of the AGT gene polymorphism on the occurrence and progression of IS. Therefore, this study aimed to assess the possible relationship between the AGT M235T gene polymorphism and the risk of IS in the Ethiopian population.
Subjects and methods
Ethics statement
The study protocol was approved by the University of Gondar Institutional Review Board (Ref. VP/RTT/05/1016/2022). All study participants gave written informed consent. All the data were obtained anonymously and treated confidentially.
Study participants
This hospital-based matched case control study was conducted at Debre Tabor Referral Hospital (Debre Tabor, North-West Ethiopia) from May to August 2022. It has a follow-up medical referral clinic (MRC) for major chronic conditions like IS, where treatment and follow-up for those patients take place. The IS patients that had been confirmed by computed tomography (CT) scans and magnetic resonance imaging (MRI), were recruited into this study. The study included patients who had been receiving follow-up care at MRC for at least one year. Controls were age- and sex-matched healthy volunteers who were available during the study period. They were healthy individuals with normal brain imaging from the same geographical location and social status. Patients who are diagnosed with hemorrhagic stroke, transient ischemic attack, hepatic and renal disease, cardiac source of embolization, secondary HTN, or chronic bacterial or viral infection were excluded. Patients who are unable to respond or are not willing to sign informed consent were also excluded from this study. The study included a total of 72 participants of both sexes, consisting of 36 IS patients and 36 healthy control groups. Participants were selected by simple random sampling methods, using a table of random numbers (TRN), from all the registered patients.
Data collection methods
By analogy to our previous work [Citation12], the socio-demographic characteristics of both patients and healthy control subjects were taken through a semi-structured questionnaire. Portable digital scales and portable stadiometers were used to determine body weight and height, respectively. Body mass index (BMI) was calculated by dividing weight (in kilograms) by height (in meters squared). Participants were classified as underweight (BMI < 18.5 kg/m2), healthy (18.5 - 25 kg/m2), overweight (25.0–29.9 kg/m2) or obese (≥ 30 kg/m2) based on their BMI [Citation13]. A digital instrument was used to measure blood pressure in the sitting stance after 5 min of rest, and the mean of three readings was used to compute SBP and DBP. Participants were categorized as hypertensive, if mean SBP ≥ 140 mmHg and mean DBP ≥90 mmHg or if they used antihypertensive medication; pre-hypertension, SBP 120–139 mmHg or DBP 80–89 mmHg; normal blood pressure, SBP <120 mmHg and DBP <80 mmHg [Citation14].
Sample collection and laboratory methods
All participants, including patients and healthy controls, had a blood sample of 5 mL taken from the median cubital vein by laboratory staff under safety procedures, as described in our previous work [Citation12]. From the 5-mL sample, 3 mL was retained in the test tube without anticoagulants to allow the blood to clot. The tubes were then centrifuged to extract the serum, which was then collected into new tubes for biochemical tests. Enzymatic analyses of TC, TG, LDL, HDL, creatinine, and glucose were performed on each test in the Debre Tabor Referral Hospital diagnostic laboratory using the Dimension EXL 200 fully automated analyzer. Results were then scored by an investigator blinded to the sample withdrawal condition and experimental groups. If the fasting plasma glucose level was more than 110 mg/dL, diabetes mellitus was identified [Citation15]. Dyslipidemia can be defined if TC, TG and LDL levels are above 200 mg/dL, 150 mg/dL and 130 mg/dL, respectively, and the HDL level is below 60 mg/dL [Citation13]. Kidney disease was diagnosed if the blood creatinine concentration is >1.3 mg/dL [Citation16].
Genomic DNA extraction and genotyping
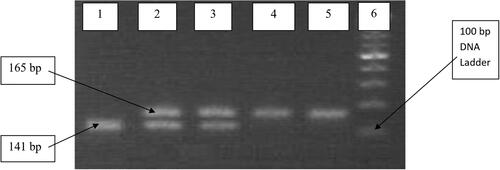
Genomic DNA was extracted from the remaining 2 mL samples collected in EDTA (anticoagulant) containing tubes of each participant at the University of Gondar Molecular Biology Laboratory. A non-enzymatic salting-out technique was carried out for DNA extraction as described by Suguna et al. with little modification [Citation17]. The quality of isolated genomic DNA was verified utilizing 1% agarose gel electrophoresis () and the sample was kept at −20 °C until it was needed [Citation18]. The AGT M235T genotypes were identified using forward primer, 5’CAG GGT GCT GTC CAC ACT GGA CCC C-3′ and reverse primer, 5′-CCG TTT GTG CAG GGC CTG GCT CTC T-3′[Citation19]. Amplification was performed in 25-μL reaction mixture: 12.5 μL of 5 x FIREPol master mix (Solis BioDyne, Tartu, Estonia), constituting MgCl2, dNTPs, PCR buffer and Taq polymerase, 1 μL forward primer, 1 μL reverse primer, 2 μL of each sample and 8.5 μL PCR grade water were added to complete the total volume. A TC-412 PCR thermocycler was used. The initial denaturation stage of the amplification was set at 10 min at 95 °C, and it was then followed by 35 cycles of amplification with denaturation steps of 10 s at 94 °C, primer hybridization steps of 30 s at 64 °C, elongation steps of 20 s at 72 °C, and a final elongation step of 5 min at 72 °C. In a 10 μL mixture containing 5 U of the restriction enzyme PsyI (Tth111I, #ER1331, Thermo Fisher Scientific, Waltham, Massachusetts, U.S.), the amplified fragment of 165 bp was exposed to enzymatic digestion for 3 h at 65 °C. The mutant T235 allele splits into two pieces that are 141 and 24 bp, but the normal M235 allele is not digested [Citation20]. Finally, AGT M235T genotypes 165 bp band (MM), 141 bp band (TT), and both 165 and 141 bp band (MT) PCR products were separated electrophoretically for 50 min at 120 V in a 2% agarose gel ().
Figure 1. Agarose gel (1%) electrophoresis showing the quality of isolated genomic DNA. Lane 1: 100 bp DNA ladder (Ready to Load, Solis BioDyne, Tartu, Estonia); Lanes 2 – 13: isolated genomic DNA.
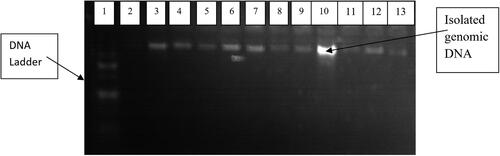
Figure 2. Representative 2% agarose gel electrophoresis showing PCR products of the AGT M235T gene. Lane 1: homozygous MM genotype; Lanes 2 and 3: heterozygous MT genotypes; Lanes 4 and 5: homozygous TT genotypes; Lane 6: 100 bp DNA ladder.
Statistical analysis
The data were analyzed using STATA version 14. Mean and standard deviation (x + s) were used to show quantitative data. A t-test for independent samples was applied to compare continuous variables between IS patients and healthy controls. The chi-square test was used to compare the distribution of genotype and allele frequencies. With a 95% confidence interval (CI), logistic regression was used to evaluate the risk correlations of the AGT gene M235T polymorphisms with IS. One-way analysis of variance (ANOVA) was used to compare how the AGT genotypes and clinical factors were related. Differences were considered statistically significant at the p < 0.05 level.
Results
The IS cases and healthy control groups had similar distribution by sex and age. Of the IS participants (n = 36), 19 (52.8%) were males and 17 (47.2%) were females; and in the group of healthy control subjects (n = 36), 18 (50%) were males and the remaining 18 (50%) were females. The mean ages of the study groups were 59.4 ± 12.1 and 58.2 ± 6.9 for cases and controls, respectively. When compared to the control group values, the systolic blood pressure (SBP), diastolic blood pressure (DBP), total cholesterol (TC), triglycerol (TG) and LDL-cholesterol levels were significantly higher in patients, but HDL-cholesterol levels were lower (p < 0.001). However, there were no significant differences in body mass index (BMI), fasting blood glucose (FBG), or blood creatinine level between the two groups ().
Table 1. General characteristics of the study participants in Debre Tabor Referral Hospital, Northwest Ethiopia, 2022.
The frequencies of the TT, MT and MM genotypes among the patients group were 52.78%, 33.34% and 13.89%, respectively, whereas in the control group the same were found to be 25.00%, 44.44% and 30.56%, respectively (). The genotype distributions were consistent with the Hardy-Weinberg equilibrium (p > 0.05) in both the patient and control groups. The T and M allele frequencies in patients were 0.69 and 0.31, respectively, while they were 0.47 and 0.53 in controls (). There was a significant difference (p < 0.05) in the distribution of the AGT genotype polymorphism between the two groups. Furthermore, the frequency of homozygous TT genotype was higher among the patients than in the control group (OR: 4.64; 95% CI: 1.23–17.41; p = 0.023). Similarly, the frequency of the T allele was 2.5 times higher than the M allele in IS patients (OR: 2.54; 95% CI: 1.28–5.02; p = 0.003) compared to healthy controls. However, the frequency of the AGT genotype MM was lower in the patients than in the healthy controls ().
Figure 3. Distribution of the AGT M235T genotype in cases and controls.
Note: * Statistically significant differences at P < 0.05.
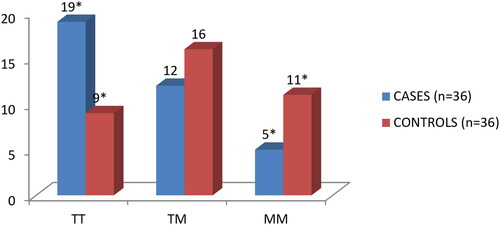
Table 2. Distribution of AGT M235T genotypes and allele frequencies of the study participants in Debre Tabor Referral Hospital, Northwest Ethiopia, 2022.
shows the association of AGT M235T genotype with clinical parameters of IS patients and healthy controls. The fasting blood glucose, blood pressure, and lipid profiles were compared with the AGT genotypes (TT, MT, and MM) in the study groups. The above clinical variables are relatively higher in the TT genotype than in MT and MM genotypes. However, those clinical parameters were not found to be significant with the genotypes in the study groups (p > 0.05).
Table 3. Association of AGT M235T genotype with clinical characteristics in Debre Tabor Referral Hospital, Northwest Ethiopia, 2022.
Discussion
Ischemic stroke is a complex and heterogeneous condition with multiple etiologies and significant clinical symptoms [Citation21]. Even though conventional risk factors like smoking, HTN, DM and dyslipidemia were thought to be more common than inherited risk factors, recent case-control studies and meta-analyses have shown that genetic risk factors and genetic background have a significant impact on IS susceptibility [Citation22]. Extracellular volume and the homeostasis of the vascular wall are mediated by AGT, a circulating substrate in the RAAS, which is converted to angiotensin I by renin and then generates angiotensin II [Citation23]. Numerous studies have shown that angiotensin II influences atherosclerotic changes and plaque rupture through a variety of mechanisms, including vasoconstriction and the expansion of vascular smooth muscle cells, which promote peripheral resistance of blood vessels [Citation24]. It has been shown that human RAAS activation worsens ischemia-induced brain injury mainly via stimulating atherosclerosis, reducing cerebral blood flow, and increasing oxidative stress, which results in a hypertension-induced IS complication [Citation25].
Although contradictory results have been reported, the AGT gene M235T polymorphism has been found to be highly related to a higher prevalence of IS in some ethnic populations [Citation23,Citation26,Citation27]. In the present study, the AGT gene polymorphisms and associated risk factors were examined in IS patients and healthy controls. When compared to the MM genotype and M allele, the TT genotype and T allele had a significantly higher frequency in cases than in controls (, ). This finding is consistent with a meta-analysis conducted in East Asia that included six eligible studies containing 891 IS patients and 727 healthy controls and discovered that patients with the TT genotype were significantly more at risk of IS than those with the MM genotypes (OR = 2.24, 95%CI = 1.37–3.66; p < 0.05) [Citation26]. A second meta-analysis involved 17 studies and 16,030 subjects in total; 3,842 of them were IS patients and 12,188 were controls. Twelve of these studies focused on Asian people, while 5 dealt with Caucasian populations; 7 studies were based on a healthy population, whereas 10 employed hospital-based populations as controls. The results of the cumulative analysis found that Asians but not Caucasians had a significant correlation between the AGT M235T polymorphism and IS (OR = 1.447, 95% CI = 1.207–1.735: p < 0.05) [Citation23]. A third meta-analysis conducted in the Chinese population, containing 21 studies, showed a significant association between angiotensinogen M235T polymorphism and IS risk (OR = 1.69; 95% CI, 1.35–2.11; p < 0.001). In the stratified analysis by ethnicity, the study found that this polymorphism was significantly associated with ischemic stroke in Asians (OR = 1.85; 95% CI, 1.45–2.35; p < 0.001) [Citation10]. A fourth meta-analysis, which was also carried out in the Chinese population, included eight studies (1,636 cases and 1,433 controls) and showed a significant correlation (OR = 2.60, 95% CI = 1.77–3.83; p < 0.001) between the AGT M235T gene polymorphism and the incidence of ischemic stroke [Citation27].
On the other hand, the findings of this study disagree with a case-control study conducted in Japan [Citation28], which included 147 consecutive IS patients and 133 healthy age-matched controls. Based on the allele and its genotype, there was no significant correlation between the AGT gene polymorphism and HTN in Japanese IS patients; and the M allele of the AGT gene polymorphism was more dominant than the T allele in IS patients, independent of hypertension [Citation28]. Another study conducted in populations from Mongolia included a total of 164 participants (68 cases and 96 controls), and the AGT M235T genotypes and allele frequencies were not significantly different between the groups (OR = 1.05, 95% CI = 0.18–6.14; p = 0.955) [Citation29]. A study conducted in the Korean population involved 260 subjects and also revealed no significant difference in the distribution of angiotensinogen M235T genotypes among the study groups (OR = 1.02, 95% CI = 0.44–2.41; p > 0.05) [Citation30]. The varying distribution frequencies of the AGT M235T polymorphism, which are impacted by regional and ethnic variances, may be the reason for the controversial findings among the various ethnic communities [Citation31]. Additional variables might be at play, including various study methodologies, bias in selection, various matching criteria, or the kind of stroke [Citation32].
There are some limitations to this study. First, the relatively small sample size, due to low patient flow to the medical referral clinic (MRC) follow-up, may lead to a bias in identifying the AGT M235T genotype in IS patients. Second, there are no measurements of plasma angiotensinogen levels or other genes of RAAS that correlate directly with the genetic polymorphisms investigated in this study. Third, all subjects included in this study were Ethiopians. As previously discussed [Citation28], the distribution of the AGT gene M235T polymorphism varies with race, and hence, the effect on the pathogenesis of IS in different ethnic groups requires further investigation. To the best of our knowledge, this is the first investigation into the relationship between genetic variations of AGT and IS in the Ethiopian population. The findings of this study will serve as a baseline for these locations, but further research must be done to find other gene polymorphisms that could be reliable indicators of IS in this population. Finally, the very high incidence of this polymorphism in the African population may affect the results of the study. However, the participants in our study are of homogeneous genetic background; and thus, such effects are unlikely since both patients and controls are from the same ethnic populations.
Conclusions
This study found that the AGT M235T gene of the TT genotype and the T allele have association with a high risk of IS development. As a result, although more research is required to support this hypothesis, the obtained results indicate that the AGT gene M235T polymorphism may be used as a biomarker for the early diagnosis and detection of IS. Further studies with a larger sample size are needed to understand the correlation between the AGT gene and ischemic stroke.
Authors’ contributions
All authors made a significant contribution to the work reported, whether that was in the conception, study design, execution, acquisition of data, analysis, or interpretation. A.M. prepared the final draft of the manuscript. M.A. and N.B. critically reviewed the article and gave final approval of the version to be published. All authors agreed on the journal to which the article has been submitted.
Ethics approval and consent to participate
The study protocol was approved by the University of Gondar institutional review board (Ref. VP/RTT/05/1016/2022). Study participants were recruited only after written informed consent was obtained from each of them. All the data were obtained anonymously and treated confidentially.
Competing interests
The authors declare to have no conflicts of interest.
Abbreviations:
| AGT | = | angiotensinogen |
| BMI | = | body mass index |
| DBP | = | diastolic blood pressure |
| EDTA | = | ethylenediaminetetraacetic acid |
| FBG | = | fasting blood glucose |
| HDL | = | high density lipoprotein |
| HTN | = | hypertension |
| IS | = | ischemic stroke |
| LDL | = | low density lipoprotein |
| PCR | = | polymerase chain reaction |
| RAAS | = | renin-angiotensin-aldosterone system |
| SBP | = | systolic blood pressure |
| TC | = | total cholesterol |
| TG | = | triglycerol |
Acknowledgments
We would like to give our heartfelt thanks to the Debre Tabor Referral Hospital diagnostic laboratory staff for their support during sample collection and laboratory analysis.
Availability of data
The anonymized data used and/or analyzed in this are available from the corresponding author upon reasonable request.
Disclosure statement
No potential conflict of interest was reported by the authors.
Correction Statement
This article has been republished with minor changes. These changes do not impact the academic content of the article.
Additional information
Funding
References
- Wang J, et al. Association of laboratory parameters and genetic polymorphisms with ischemic stroke in Chinese Han population. Exp Ther Med. 2021;21(5):1–9.
- Yu J, Zhou R, Cai G. From hypertension to stroke: mechanisms and potential prevention strategies mechanisms involved in the pathogenesis of hypertension-Induced stroke. CNS Neurosci Ther. 2011;17(5):577–584.
- Malueka RG, Dwianingsih EK, Sutarni S, et al. The D allele of the angiotensin-converting enzyme (ACE) insertion/deletion (I/D) polymorphism is associated with worse functional outcome of ischaemic stroke. Int J Neurosci. 2018;128(8):697–704.
- Cipolla MJ, Liebeskind DS, Chan SL. The importance of comorbidities in ischemic stroke: impact of hypertension on the cerebral circulation. J Cereb Blood Flow Metab. 2018;38(12):2129–2149.
- Isordia-Salas I, Santiago-Germán D, Cerda-Mancillas MC, et al. Gene polymorphisms of angiotensin-converting enzyme and angiotensinogen and risk of idiopathic ischemic stroke. Gene. 2019;688:163–170.
- Shahid M, Rehman K, Akash MSH, et al. Genetic polymorphism in angiotensinogen and its association with cardiometabolic diseases. Metabolites. 2022;12(12):1291.
- Wang B, Guo Q, Peng Y, et al. Association of AGT M235T and ACE I/D polymorphisms with the risk of ischemic stroke : meta-analysis in Han Chinese population. J Neurol Sci. 2012;320(1–2):79–84.
- Gorgui J, Gorshkov M, Khan N, et al. Hypertension as a risk factor for ischemic stroke in women. Can J Cardiol. 2014;30(7):774–782.
- Zhai CN, Cong HL, Zhang H, et al. M235T polymorphism in the angiotensinogen gene and cardiovascular disease: an updated meta-analysis of 39 case-control comparisons. Anatol J Cardiol. 2019;21(4):222–232.
- Bao H, et al. Angiotensinogen polymorphism and ischemic stroke risk. Int J Clin Exp Med. 2015;8(8):12914–12920.
- Abate TW, Zeleke B, Genanew A, et al. The burden of stroke and modifiable risk factors in Ethiopia: a systemic review and meta-analysis. PLoS One. 2021;16:1–19. pp.
- Melake A, Nega B. Association between ACE I/D gene polymorphism and dyslipidemia in hypertensive patients with ischemic heart disease complication among Ethiopian population. Res Rep Clin Cardiol. 2023;14:1–8.
- Gadekar T, Dudeja P, Basu I, et al. Correlation of visceral body fat with waist–hip ratio, waist circumference and body mass index in healthy adults: a cross sectional study. Med J Armed Forces India. 2020;76(1):41–46.
- Flynn JT, et al. Clinical practice guideline for screening and management of high blood pressure in children and adolescents. Pediatrics. 2017;140(3):1–74.
- Keutmann S, Zylla S, Dahl M, et al. Measurement uncertainty impacts diagnosis of diabetes mellitus: reliable minimal difference of plasma glucose results. Diabetes Ther. 2020;11(1):293–303.
- Helmersson-Karlqvist J, Ridefelt P, Boija EE, et al. Lower creatinine concentration values and lower inter-laboratory variation among Swedish hospital laboratories in 2014 compared to 1996: results from the equalis external quality assessment program. Clin Chem Lab Med. 2019;57(6):838–844.
- Suguna S, Nandal DH, Kamble S, et al. Genomic DNA isolation from human whole blood samples by non enzymatic salting out method. Int J Pharm Pharm Sci. 2014;6(6):198–199.
- Al-Hassani OMH. Detection of AGT gene polymorphism in patient with hypertension in Mosul city. Iraqi J Biotechnol. 2019;18(2):64–69.
- Kooffreh ME, Anumudu CI, Akpan EE, et al. A study of the M235T variant of the angiotensinogen gene and hypertension in a sample population of Calabar and Uyo, Nigeria. Egypt J Med Hum Genet. 2013;14(1):13–19.
- Mocan O, Radulescu DAN, Buzdugan E, et al. Association between M235T -AGT and I/D -ACE polymorphisms and carotid atheromatosis in hypertensive patients : a cross-sectional study. In Vivo. 2020;2819:2811–2819.
- Della-Morte D, Guadagni F, Palmirotta R, et al. Genetics of ischemic stroke, stroke-related risk factors, stroke precursors and treatments. Pharmacogenomics. 2012;13:595–613.
- Salem GM, Gab-Allah GK. Angiotensin converting enzyme polymorphism and ischemic stroke. Neurosciences (Riyadh). 2020;25(3):176–181.
- Liang B, Qin L, Wei H, et al. AGT M235T polymorphisms and ischemic stroke risk : a meta-analysis. J Neurol Sci. 2013;331(1–2):118–125.
- Tascilar N, Dursun A, Ankarali H, et al. Angiotensin-converting enzyme insertion/deletion polymorphism has no effect on the risk of atherosclerotic stroke or hypertension. J Neurol Sci. 2009;285(1-2):137–141.
- Schelleman H, Klungel OH, Witteman JCM, et al. Angiotensinogen M235T polymorphism and the risk of myocardial infarction and stroke among hypertensive patients on ACE-inhibitors or b -blockers. Eur J Hum Genet. 2007;15(4):478–484.
- Wang S, Zeng R, Lei L, et al. Angiotensinogen gene polymorphism and ischemic stroke in East Asians: a meta-analysis⋆. Neural Regen Res. 2013;8(13):1228–1235.
- Gao T, Huang L, Fu Q, et al. Association of polymorphisms in the AGT gene (M235T, T174M) with ischemic stroke in the Chinese population. J Renin Angiotensin Aldosterone Syst. 2015;16(3):681–686.
- Nakase T, Mizuno T, Harada S, et al. Angiotensinogen gene polymorphism as a risk factor for ischemic stroke. J Clin Neurosci. 2007;14(10):943–947.
- Huriletemuer H, Zhang C, Niu G, et al. Gene polymorphisms and related risk factors in Mongolian hypertensive stroke patients. Neurosciences. 2010;15(3):184–189.
- Jea J, Bang C, Lee T, et al. Lack of association between angiotensinogen M235T gene polymorphism and ischemic stroke in Korean. J Korean Neurol Assoc. 2001;19(1):24–28.
- Rong C, Xing Y, Jiang X, et al. Angiotensin-converting enzyme gene polymorphism and Middle cerebral artery stenosis in a Chinese Han population. Neural Regen Res. 2013;8(15):1410–1417.
- Yadav S, et al. Detailed analysis of gene polymorphisms associated with ischemic stroke in South Asians. PLoS One. 2013;8(3):1–8.