
Abstract
The aim of this paper is to identify preferred Central and Eastern Europe (CEE) medical tourism destinations (MTD) and medical services in the context of socio-demographic determinants. The computer-assisted web interviewing (CAWI) method was used. A total of 282 completed self-administered questionnaires were collected from Britons and Germans, who constitute a large segment of medical tourists in CEE. Subsequently, the responses were analysed using the chi-square test and the method of logistic regression function. The results indicated that the chosen destinations and medical services vary depending on gender, age and nationality. The survey results have implications for scholars, allowing them to understand the way Britons and Germans evaluate MTDs and medical services in CEE, as well as for medical tourism facilitators/brokers and destination management organisations engaged in the process of creating a medical tourism product. The obtained results have also implications for further research related to the development of medical tourism in CEE.
1. Introduction and background
Medical tourism should be perceived as a phenomenon in which patients travel outside their permanent place of residence in order to use medical services, including tourism packages (Connell, Citation2013). The scope of these services is wide, because medical needs and consumer expectations are becoming more individualised (Cohen & Prall, Citation2015; Holliday et al., Citation2015; Lunt et al., Citation2014). Medical tourism is beneficial for both the patients (lower cost, avoiding queues in the home country), as well as the entire industry (economic development of enterprises, countries/regions). Given the above, it can be seen that medical tourism is a complex process (Runnels & Carrera, Citation2012), resulting from the demands of the modern market, particularly the demand side. The term ‘medical tourism’ can be quite peculiar to researchers representing various fields of science. Nonetheless, it is a rapidly growing phenomenon spurred on by an increasingly empowered patient base searching for quality, affordability, availability, accessibility in healthcare, perceived quality, satisfaction, and trust in the staff and clinic (Choi, Citation2015), including access to treatments that are not legally allowed in their place of residence (Connell, Citation2013). The reasons why patients undertake medical trips also include a feeling of overall dissatisfaction with the national health system in their country (Cameron et al., Citation2014), or even the need to preserve confidentiality for some people seeking medical treatment (Andrei, Ţigu, Drăgoescu, & Sinescu, Citation2014).
In the field of science and social life medical tourism is still not fully recognised and clearly defined (Lunt & Horsfall, Citation2014). In the literature there are various approaches explaining this phenomenon. On the one hand, medical tourism is perceived as an obligatory type of tourist trip program (linked to leisure tourism, visits to friends and relatives); on the other hand, as a phenomenon of global (including cross-border) health care (The European Parliament, Citation2011; Lunt & Carrera, Citation2010). According to Connell (Citation2013, p. 10) all movements of cross-border health care should be referred to as medical travel, ‘but it should also be noted that “medical tourism” will continue to be used for many components of that mobility’.
There are various types of medical services offered by medical tourism enterprises (clinics, hospitals) located in MTDs. Medical tourism destinations can be found on all continents and are especially popular in relatively poor, developing countries. What differentiates medical tourism destinations from therapeutic and wellness and wellbeing tourism destinations to the greatest extent is that there is no need for the presence of natural setting and natural healing resources. This is due to the fact that the existence of medical tourism destinations is determined only by relevant political and legal regulations (e.g., provisions on abortion or transplantation) (Dryglas & Salamaga, Citation2018). Over the previous two decades, medical tourism literature presented large numbers of ever-new services in this industry such as stem cell therapy, cosmetic surgery (e.g., Lasik surgery in Colombia), dental services (e.g., teeth whitening in Poland), invasive medical interventions (e.g., sex reassignment surgery in Thailand), ‘death’ services (e.g., euthanasia (‘suicide’) in Switzerland, abortion in Spain and Sweden), transplant services (e.g., kidney transplant in Philippines, xenotransplantation), reproductive services (e.g., surrogate parenthood in India). In medical tourism services there is a need for: (1) consultation with, and approval of, a medical specialist to perform a medical procedure, (2) performance of services by qualified medical personnel, (3) medical care, and (4) usually, payment for the total cost of the service by the patient. The last element points to the difference between a tourist and a mobile medical patient, where in the case of the latter the national health fund or an insurance company from the patient’s country of origin covers the costs. Connell (Citation2013, p. 3) doubts whether undergoing invasive and painful medical procedures can be considered as an appropriate criterion to use the term medical tourism. Using this approach, medical tourism is a ‘conscious activity in which a traveller (a medical tourist) aims to receive health-care services in his/her own country or abroad to maintain (or improve) their health condition and/or aesthetic appearance of their body, which is sometimes combined with relaxation, regeneration of physical and mental strengths, sightseeing and entertainment’ (Lubowiecki-Vikuk, Citation2016, p. 31). Lunt et al. (Citation2014) point out that tourism plays a peripheral role in the decision-making process of ‘medical tourists’, but their final decisions are taken primarily for health reasons. However, some of those people might engage in tourism activities as well. This proves again that the phenomenon of medical tourism is multidimensional and the research on it should be continued.
Halecki (Citation1952) introduced CEE as a term referring to the geopolitical, historical and cultural setting of the region in question. The different classifications of CEE countries are most often based on a historical criterion and the standardisation of geographical names (United Nations Group of Experts on Geographical Names, Citation2016), as well as interpretations by representatives of various research centers (Kłoczowski, Citation1995). Thus, there are different CEE region systemisations in the subject literature. The present paper assumes, in line with Kłoczowski’s study (Citation1995), that CEE includes: Albania, Belarus, Bosnia and Herzegovina, Bulgaria, Croatia, the Czech Republic, Estonia, Hungary, Latvia, Lithuania, Macedonia, Moldova, Montenegro, Poland, Romania, Serbia, Slovakia, Slovenia and Ukraine. It is clear that the CEE region encompasses not only the Visegrád Group countries (the Czech Republic, Hungary, Poland, Slovakia), but also EU Member States, including members of the North Atlantic Treaty Organisation (all the countries listed above except for Belarus, Bosnia and Herzegovina, Macedonia, Moldova, Serbia and Ukraine). According to Smith, Puczkó, Michalkó, Kiss, and Sziva (Citation2016), the CEE region has a rich tradition of providing a variety of health-related services: medical, therapeutic and wellness. These authors reported that the market potential in this part of Europe is high and that more agencies will specialise in medical tourism in the future. This stems from the fact that the region boasts a convenient location on the map of Europe and offers a favorable climate, and a beautiful and often pristine natural environment, and competitive prices for international tourists. The CEE countries are not only attractive for tourists, but also innovative as regards their access to technological medical specialisations (Wisla & Sierotowicz, Citation2016). Apart from the listed drivers for development of services and MTDs, a thorough review of the relevant literature also revealed several barriers which, depending on the socio-economic condition of a given country, include a negative or unknown image, mistrust and lack of cooperation between health care and tourism systems, and the specificity of legislation (Bušelić & Pavlović, Citation2003; Karmowska & Marciniak, Citation2015; Kesar & Rimac, Citation2011; Kiss, Citation2015; Lubowiecki-Vikuk & Kurkowiak, Citation2017). Migrations of medical professionals to the European Union countries are becoming a serious problem (Beladi, Chao, Ee, & Hollas, Citation2015). All these problems require government support, an innovative approach to eliminate defects, and the use of the opportunities and observations of contemporary trends on the market.
The analysis of theoretical and conceptual studies and of works from the analytical and research-based category in the field of medical tourism confirms the thesis of a cognitive gap in theoretical and empirical research on MTDs and medical services in CEE. Hence, in response to the gap mentioned, the authors propose a study which aims to analyse the market potential of medical tourism in CEE based on the opinions of Britons and Germans to complement the assessment of medical tourist demand for CEE MTDs.
Therefore, this study aims to identify preferred CEE MTDs and medical services in the context of socio-demographic determinants. In-depth analysis of the literature on medical tourism, especially on issues relating to MTDs and medical services in CEE, made it possible to develop the following research questions (RQ) used in the empirical study conducted:
RQ1: In which of CEE MTDs have Britons and Germans used medical services and how do their choices differ in terms of socio-demographic factors?
RQ2: In which of CEE MTDs would Britons and Germans like to use medical services and how do their choices differ in terms of socio-demographic factors?
RQ3: What is the level of customer satisfaction with the medical services in CEE MTDs?
RQ4: Which medical services in CEE MTDs would Britons and Germans like to use the most and how do their choices differ in terms of socio-demographic factors?
RQ5: How do socio-demographic factors affect the likelihood of Britons and Germans choosing medical services in CEE MTDs?
2. Methods
The CAWI method was used. The method is based on the technique of computer-assisted data collection because websites are frequently the first contact point with potential international service providers (Maguire et al., Citation2016). Next, following the recommendations of the Medical Tourism Association and the International Medical Travel Journal, organisations and associations operating in the medical tourism services sector in the UK and Germany were selected and sent the questionnaire via e-mail. An invitation to participate in the survey was also made available on dedicated online forums and social networking sites. In this way, the questionnaire was targeted at a clearly defined group of people, i.e., those who visit selected websites related to medical tourism in the CEE countries. A total of 282 completed self-administered questionnaires were collected from Britons and Germans, who constitute a large segment of medical tourists in CEE (Lunt et al., Citation2014). An original electronic questionnaire in two languages, English and German, was developed and translated by two independent translators. The study was conducted from 1 to 30 September 2015, just after the end of the tourist season.
Descriptive analysis of the sample showed that both Britons and Germans completed randomly the same number of surveys (141) in which the number of female and male participants was almost equal (71 vs. 70). Similarly to the analysis of gender characteristics, the analysis of the age of the respondents, stratified into five age groups (18–29, 30–39, 40–49, 50–59, ≥60), showed a balanced representation of German respondents in all age groups (20.6%, 17.7%, 22.0%, 17.0% and 22.7%, respectively). As for the British respondents, the following age groups dominated: 50–59, 40–49 and 30–39 (26.2%, 24.1% and 23.4% respectively). The youngest group, aged 18–29, accounted for 14.2% of the British respondents, whereas the oldest group (≥60) for 12.1%.
The questionnaire consisted of six questions. Four of them were single answer questions where the respondents had to pick just one from predetermined lists of countries. The other two questions were multiple choice questions. Respondents were asked (1) to name the CEE countries in which they had already been the so-called medical tourist, (2) to name the CEE countries in which they would like to be a medical tourist (or recommend them), (3) to name their preferences (suggestions) as concerns the choice of CEE in which to use the following services: dental; in vitro, infertility treatment; body sculpting (liposuction), aesthetic medicine, plastic surgery; ophthalmology. Additionally, apart from answering the questions regarding the nationality and gender, respondents chose one of the five given age groups.
Subsequently, the responses were analysed using the chi-square test proposed by Satorra and Bentler (Citation1994) and the method of logistic regression function (Freedman, Citation2009, p. 128). The chi-square test and the test for probability were conducted to find out if the respondents differed by nationality, age and gender as concerned their interest in medical tourism. In order to use the method of logistic regression the answers (dependent variable) were coded as dichotomous variables, depending on whether or not Poland was chosen as the answer in single answer question. In order to examine the association between demographic factors and choosing Poland as the answer the odds ratio was calculated with the confidence intervals (CI) which allows one to determine whether this association is statistically significant. If the 95% confidence interval for the odds ratio does not contain 1.0 we can conclude that there is a statistically significant (at the 0.05 significance level) association between variables. If the 95% confidence interval for the odds ratio contains 1.0, the association is not significant. All statistical analyses were conducted using the data analysis software system - Statistica ver. 12.0. The significance level was set as p-value ≤ 0.05.
3. Results
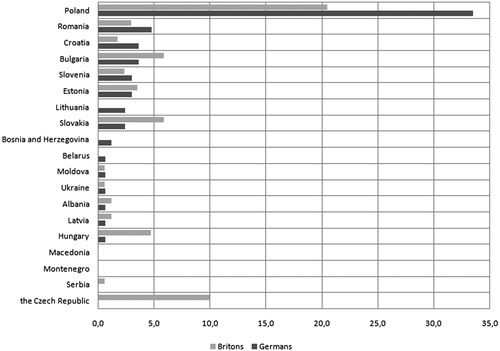
The data in show the experience of the respondents as regards the use of medical services outside their home country. The order of the countries depends on the frequency of the respondents’ answers. Both for Germans (33.5%) and for Britons (20.5%) Poland is the country where they have used medical services most frequently. As regards other CEE MTDs, none of the respondents from Germany has used medical services in the Czech Republic or Serbia and, similarly to Britons, in Montenegro or Macedonia. Moreover, Britons have never used medical tourism services in Belarus, Bosnia and Herzegovina or Lithuania, either. The surveyed subjects declared to have been medical tourists in the following proportions: in Poland there were 26.9% (especially Germans 61.5%; males 51.6%; aged 60 + 36.2% and aged 30–39 28.6%), the Czech Republic 5.0% (especially the British 100.0% and males 58.8%), Bulgaria 4.7%, Slovakia 4.1%, Romania 3.9% (mostly females 76.9%), Estonia 3.3%, and the rest 13.3%. A total of 38.8% of the respondents had never been medical tourists, whereas 2.7% of the responses to the question about the choice of the country where the respondent would like to get medical services, indicated a country outside CEE.
Figure 1. CEE MTD where Britons and Germans used medical services.
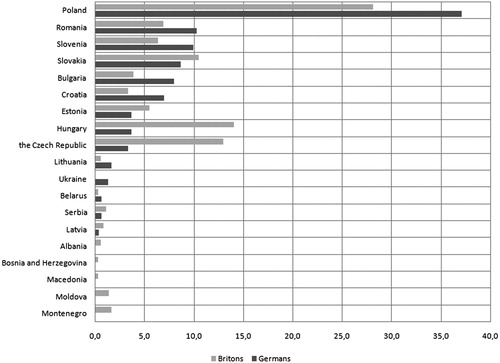
British (28.1%) as well as German (37.1%) respondents more often chose Poland (32.6%) as the preferred CEE MTD (). Of the CEE countries, also Slovakia (9.5%), Hungary (8.8%), Romania (8.6%), the Czech Republic (8.1%), Slovenia (8.1%) and other countries (21.4%) were opted for. The least likely choice of the surveyed people would be a trip to Bosnia and Herzegovina and Macedonia (0.1%, respectively). Male respondents would choose Poland less frequently than women (48.1% vs. 51.9%), and more of them would undertake the treatment in Hungary (58.1% vs. 41.9%), Slovakia (51.6% vs. 48.4%), Slovenia (60.4% vs. 39.6%) and Romania (55.4% vs. 44.6%). The Czech Republic was chosen more willingly by the surveyed women (56.1%) than men (43.9%). Referring to the age categories, it was observed that the respondents aged 18–29 more often than others declared their willingness to participate in medical tourism in Poland (39.2%) and Slovakia (12.8%). The surveyed persons aged 30–39 outside Poland (32.4%) would choose treatment in the Czech Republic or Hungary (11.5%, respectively). Apart from Poland (28.8%), Slovakia would be preferred by the persons aged 40–49 (11.0%). The 50- and 59-year-olds declared that apart from Poland (28.1%), they would also opt for Hungary (14.4%), the Czech Republic (8.9%), Romania (8.2%), as well as Bulgaria, Croatia and Slovenia (7.5%, respectively). The surveyed 60+ respondents would most willingly undergo medical treatment outside their own country in Poland (35.7%), Slovenia (11.3%) or Romania (10.4%).
Figure 2. CEE MTD where Britons and Germans would like to use medical services.
In order to analyse customer satisfaction with medical services in CEE MTDs, with respect to the first two items of the questionnaire ( and ), the data was pre-filtered and two variables were delineated:
PARC – Poland amongst the recommended countries. Number of countries indicated by respondent. A larger number (observed max = 3) may indicate a larger propensity to acquiring med services in the CEE countries.
PAVC – Poland amongst countries visited in order to acquire medical services. Number of countries indicated by respondent. A larger number (observed max = 3) suggests an experienced customer. Also, and similarly to PARC, larger PAVC value may indicate a larger propensity to acquiring medical services in the CEE countries. Interestingly, there was a rather small correlation between PARC and PAVC (0.157). Therefore, both variables could enter the model without increasing the danger of co-linearity.
The subsample consisted of respondents, who have already acquired medical services in Poland. Satisfied customers were identified as those who (1) had acquired the services, and (2) have selected Poland at least as one of the destination countries in Q2 (satisfied customers, i.e., Q1 = Poland & Q2 = Poland: 89%; not satisfied, i.e., Q1 = Poland & Q2 ≠ Poland: 11%). It turned out that it was a very balanced sample [share of female (50.6%) and male (49.4%) customers amongst the satisfied customers; share of British (37%) and German (63%) customers amongst the satisfied customers].
Since there was an overlap for Q2 = Poland and PAVC, the latter variable has been removed from further inquiries. Re-estimations of the basic model for the subsample of respondents already acquiring medical services in Poland resulted in:
statistically significant variables: intercept (0.107), age cluster (0.015), and PARC (0.042),
statistically insignificant variables: gender (0.312), nationality (0.548).
The second attempt to capture the importance of factors explaining satisfaction is illustrated in .
Table 1. Model re-estimated for the statistically significant variables.
McFadden R^2 = 0.223, Log-likelihood = −24.496. The model predicted correctly 79 out of 81 positive answers, but over-performed when predicting negative answers (only 2 out of 8). Bearing in mind that the vast majority of respondents indicated a positive answer (89%), this result is not surprising.
Both estimated coefficients were positive, which meant that probability of choosing Poland would increase with increasing age and with the increasing number of countries indicated as place where the respondents would like to acquire medical services. The magnitude of marginal effects, however, was very small (0.051 and 0.037, respectively). Comparing MEAMs (marginal effect at mean), there was a slightly greater impact of age than PARC. Older respondents simulated probabilities for age () and PARC clusters () were as follows:
Figure 3. Probability of satisfied customer for age.
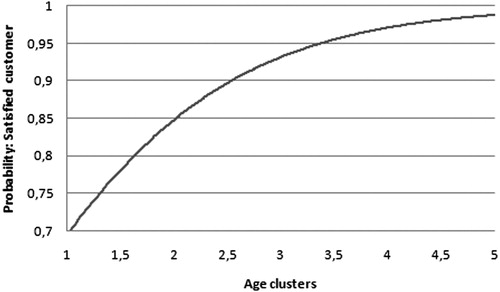
Figure 4. Probability of satisfied customer for PARC.

probability of satisfied customer increased alongside the increasing age. But even for the youngest respondents, the estimated probability was equal to 0.7,
similar situation observed for PARC – probability of satisfied customer increased alongside the number of recommended countries.
Based on the estimated marginal effects () and the simulated probabilities ( and ), the following can be concluded: the share of not-satisfied customers was small, a most-satisfied customer belonged to the oldest cluster and indicated three various countries in which she or he would like to acquire medical services, and even for the youngest and less experienced customers the probability of indicating Poland was still remarkably large.
More German and British respondents opted for dental services in Poland (74.1%) than in other CEE countries (). Thus, Germans (83.7%) opted for this country more often (p = 0.0001) than the British (64.5%). It is worth noting that the second most frequently chosen country was Hungary (9.6%). In this case, the situation is reversed, i.e., the test used for the index structure showed that the proportion of such responses among the British (14.9%) was significantly higher than among Germans (4.3%) (p = 0.0012). Similar results were observed with regard to the gender of the respondents. In comparison to women, men less frequently travelled to Poland for this purpose (67.9% vs. 80.3%; p = 0.0087) and more often to Hungary (13.6% vs. 5.6%; p = 0.0118).
Table 2. Preferred medical services in CEE among the respondents (%).
As regards the preferred destinations for in vitro services and infertility treatment, it was observed that Poland was the most frequently chosen country. As regards the declared trips to Estonia (9.2%), the British (12.1%) more often (p = 0.049) than Germans (6.4%) opted for this destination. The Czech Republic is also known for in vitro and infertility treatment especially considering Germans. The respondents who chose Poland (77.0%) or the Czech Republic (6.0%) cited the acquisition of body sculpting services (liposuction), aesthetic medicine and plastic surgery as the purpose of their trips to those countries. It should be noted that the consumption of such services was the most common purpose of medical trips among the respondents. Poland (72.0%) was also the most frequently chosen CEE country among the respondents using ophthalmological services. The test used for structure ratio showed that the proportion of such responses among Germans (82.3%) was statistically significantly higher (p = 0.0001) than among the British (61.7%). The second most frequently chosen destination was the Czech Republic (12.4%), which was chosen less frequently by Germans (2.1%) than the British (22.7%).
The nationality of the respondents proved to be a significant predictor of response to the questions about dental and ophthalmological services. The chance that Germans would indicate Poland in response to those questions was almost three times greater than the chance that such an answer would be chosen by the British. The odds ratios for the respective questions are as follows: 2.8 [95% CI (1.6, 5.0)], 2.9 [95% CI (1.7, 5.0)] and 3.0 [95% CI (1.8, 4.5)]. Gender, however, was a significant predictor only in response to the question regarding dental services. The chance that women would indicate Poland in response to that question was almost twice higher [the odds ratio = 1.9, 95% CI (1.1, 3.3)] than the chance that this option would be selected by men. Age proved significant only in the case of answers to questions about ophthalmological services. In comparison with a group of 40- and 49-year-olds (the most numerous group), the odds that the youngest people would opt for Poland were three times greater. For ophthalmological services the odds ratio was 2.8 [95% CI (1.2, 6.7)].
In order to incorporate the contingency tables, a logistic binary-choice model has been estimated. Since the application of the logistic model allows for various combinations of the right-hand variables, the binary-choice logistic regression offers larger explanatory power and answers more complex questions. Also, the analysis covers a larger scope of problems including significance analysis, marginal effects, probability estimation and simulations.
The explaining variable has been constructed as a binary dummy set to 1 for every answer indicating Poland as a country in which the respondent would like to purchase medical service, and 0 otherwise. The estimations are summarised in the .
Table 3. The logistic binary-choice model.
Gender turned out to be boarder-line insignificant, but with p-value of 0.155 it might be added to the set of explanatory variables (other coefficients were highly statistically significant). Goodness-of-fit was rather poor, with McFadden R^2 = 0.162 and log-likelihood = −130.480. A relatively poor goodness-of-fit is, however, not surprising as the sample was highly heterogeneous. In terms of correctly predicted explaining variable, the model performs rather well. The model correctly predicted 80.5% of all cases, but over-performed when predicting negative answers (only 23 out of 68). Modeling the cases in which respondents would chose Poland, the model achieved a remarkable 95.3% of correctly predicted answers.
The marginal effects estimated at the averages showed that PAVC had the greatest impact on probability of indicating Poland as a country where medical services could be acquired. It means that there was a strong pattern between respondent’s personal experience and the country of choice. Interestingly, geographical factors influenced the choice of Poland as the coefficient for British citizenship was negative with second largest MEAM. It seems that the distance might be an important factor in evaluating a country’s attractiveness for acquiring medical services.
presents probabilities simulated for various citizenships and experience with medical services in Poland. Comparing the first column, the probability for Germans with no experience with Polish medical services is greater by approximately 17 pps. The gap shrinks considerably for respondents who have already gained experience with the Polish medical sector.
Table 4. Probabilities simulated for various citizenship and PAVC.
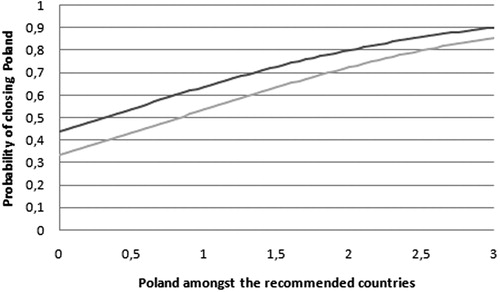
The probability of choosing Poland increases for female respondents. and depict the probabilities for age clusters and PARC for female and male respondents.
Figure 5. Probability of choosing Poland, gender, and age clusters.
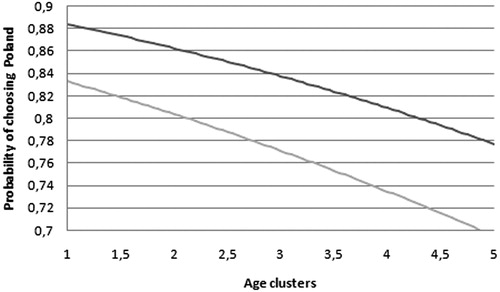
Figure 6. Probability of choosing Poland, PARC and gender.
Interestingly, the sign of the age coefficient is negative [compare it with the positive sign obtained for customer satisfaction model (), where it was positive]. It means that the younger respondents are more willing to acquire medical services in Poland. The graph also depicts the probability response for gender: the black line shows the probability simulated for female respondents, whilst the grey one indicates it for males. It is therefore more likely that a young woman would choose Poland than an aged male respondent.
A similar exercise is performed for the PARC and gender variables (). Again, the black line depicts the probability simulated across the PARC variables for female respondents. The dependence on PARC is easy to recognise, as for the lowest number of recommended countries the probability merely exceeds 0.3 and 0.4 for males and females, respectively. There’s a sharp and almost linear increase for PARC ranging between 0 and 2 countries. For the largest PARC and female respondents the probability of choosing Poland is slightly greater than 0.9.
presents the marginal effects for various medical services estimated at the average values of explanatory variables and shows standard errors and p-values for estimated coefficients. Insignificant variables have been removed from columns. For instance, modeling the demand for dental services age cluster turned out to be insignificant. The probability of choosing Poland decreased when a respondent was British. PARC variable had very little impact on the probability of choosing Poland.
Table 5. Marginal effects at means for various medical services.
Table 6. Standard errors and p-values for estimated coefficients.
The PAVC variable affects the demand for medical services most. It has appeared in all estimated models (i.e., it was statistically significant in all models). Importantly, the fit (McFadden R^2) has dropped for all estimated models. Hence, the results for specific medical services should be interpreted with necessary caution.
presents the predicted answers. The entries have the following interpretation: (0,0) correctly predicted answers ‘Poland not indicated’, (0,1) answer ‘Poland indicated’ predicted as ‘Poland not indicated’, (1,0) answer ‘Poland not indicated’ as ‘Poland indicated’, and (1,1) correctly predicted answer ‘Poland indicated’. For instance, the McFadden R^2 for the model of aesthetic services is 0.07. The model correctly predicted only 6.1% (4 out of 61) of answers not indicating Poland, but was perfectly precise when predicting answers indicating Poland. The model fitted the data extremely poorly when modeling Poland as a country in which fertility treatment could be acquired. All answers have been predicted as indicated Poland, whilst 88 respondents stated otherwise.
Table 7. Goodness-of-Fit.
4. Discussion
The probability of going abroad for medical treatment usually applies to the consumption of services in the field of dentistry (83.7%), ophthalmology (82.3%) and aesthetic medicine (Medizintourismus IUBH Touristic-Radar, Citation2016), as confirmed by the present study. The findings of this study clearly show that both British and German respondents expressed interest in the consumption of specific medical services (dental services, in vitro services, ophthalmological services and body sculpting (liposuction), aesthetic medicine, plastic surgery) located in CEE, where Poland is the leading MTD – also with regard to the respondents’ previous experience. Interest can also be observed in medical tourism to Hungary, the Czech Republic and Estonia. However, due to lower costs and quality of treatment in comparison with the home country, the Germans declare that they would most willingly opt for medical services available in Estonia, Lithuania or Latvia (Melsheimer & Weiß, Citation2014), but no such trends emerge from the results of the research presented herein. In turn, the British travel for the purposes of medical tourism not only to the Czech Republic and Ukraine, where such medical services are the cheapest (Lunt et al., Citation2014), but also to Estonia and Poland. Melsheimer and Weiß (Citation2014) indicate that slightly more than 5% of Germans decide to seek medical treatment outside their home country. Their decision is influenced, among other things, by being members of a particular insurance fund that could finance or subsidise the medical service. German tourists, especially men, are interested in a specific product of medical tourism, adapted to their needs, financial capability and other factors resulting from past experience (Medizintourismus IUBH Touristic-Radar, Citation2016).
Compared to Britons, German respondents are more likely to decide to get dental treatment in Poland (Medizintourismus IUBH Touristic-Radar, Citation2016), as confirmed by the present study. This applies to both men and women. German patients are confronted with high cost-sharing for dental care as certain services are only partially covered in the benefit basket. Complementary private health insurance packages for dental services are most common in the case of voluntary health insurance policies (Panteli et al., Citation2015). Therefore, if planning dental treatment abroad, medical tourists choose neighbouring countries or countries which can be reached without major problems (in the Schengen Area) where the cost of care is lower (Lubowiecki-Vikuk, Citation2018). Thus, the present study confirms the previous findings by Connell (Citation2013) and Lunt et al. (Citation2014) that medical tourists usually use medical services in neighbouring countries. This might suggest that planning treatment abroad and taking account of the risk related thereto, potential medical tourists consider foreign destinations which are the closest to their home country. Additionally, as pointed out by Main (Citation2014), the reasons for dental travel are often combined – women use the services of Polish dentists during shopping trips, visits to relatives/friends, holidays or visits to the hairdresser/beautician. The British respondents – men mainly – stated that, apart from Poland, they were more likely than Germans to use dental services in Hungary. Rab-Przybyłowicz (Citation2014, p. 110) points out that Hungarian dental clinics were the first in Europe to encourage foreigners to come to them for treatment, which contributed to the creation of a positive image of a dental tourism destination.
The study demonstrated that, compared to Germans, the British show particular interest in travelling to Estonia for the purpose of in vitro treatment. This kind of tourist flow can mainly be observed from the north to the south, but it can take place in any direction depending on legislation (Messinis, Messini, Daponte, Garas, & Mahmood, Citation2016, p. 202). The main reason for such trips is the desire for timely and affordable treatment with donor gametes. Culley et al. (Citation2011) also mention the treatment cost in the UK, the higher success rates and less stressful environment abroad, as well as dissatisfaction with treatment in the UK.
The findings related to consumption of ophthalmological services are worth highlighting. In this case, German respondents are much more likely to undertake treatment in Poland than the British. This also concerns people under 40. This relationship is explained on the example of refractive surgery by Lockington, Johnson, Patel, and McGhee (Citation2014, p. 372), who claim that the service ‘is one of the main reasons for medical tourism due to high patient satisfaction and perceived low complication rates’. The British willingly undergo ophthalmological treatment (e.g., cataract surgery) both in Poland and in the Czech Republic, which was previously analysed by Lunt et al. (Citation2014). They also use plastic surgery services, especially liposuction. The study also proves that the trips of British respondents to Poland and the Czech Republic were related to the acquisition of body sculpting services. The investigations of Holliday et al. (Citation2015) confirm that the Czech Republic is one of the most popular cosmetic surgery tourism destinations across the UK. The cost and the distance are the main reasons for undergoing this kind of treatment outside the UK.
5. Conclusion and implications
The example of the British and German respondents shows that depending on the gender, age and nationality, they most frequently opt for consumption of medical services that are considered non-invasive. As for invasive procedures, their behaviour is undoubtedly affected by easy access (close proximity) to the country of destination, and supposedly the quality and high standard of medical care. The selection of Poland or other CEE countries, including those situated close to the UK or Germany, is not surprising. The majority of medical staff in those countries speak English and/or German. Moreover, there are no significant culture barriers. Therefore, it seems that the CEE region is a sustainable medical tourism destination choice for the citizens of Western Europe.
It should be noted that Poland was included in the Medical Tourism Index, as the only country in the CEE region (Fetscherin & Stephano, Citation2016). This is a country-based performance measure, including only the countries which in the comprehensive assessment of standards and quality of services are most often regarded as the most favorable ones to undergo medical treatment in. It should be emphasised that medical tourism in Poland is related in particular to private providers of medical services. Thus, overall assessment of the quality of the health-care system published periodically by the WHO and the OECD, which regards the dominant public sector in Poland, may not reflect better quality and standards of care provided by private health centers which are used by foreign patients (Borek, Citation2013). It should also be taken into account that the rankings of the quality and accessibility of health care which are widely available for foreign patients are unfavorable for Poland. Apart from that, the collective analysis of data on the quality, efficiency and availability of medical care provided by private centers has not been available so far.
It was noted (Health at a Glance: Europe 2014, 2014; OECD and European Union, Citation2014) that medical tourism has a chance to become a Polish export product. Estimates for 2009 indicate that foreign patients spent approx. US $200 million on medical tourism services in Poland. Two years later, there was an increase by almost 20.0%. In Poland, health-care costs are often lower than in the countries of Western Europe. Dental treatment and plastic surgery may serve as an example here. The average prices of dental implants in Poland, in comparison with the prices in the UK and Germany, are lower by over 65%. In the case of breast enlargement, a patient can save almost 49% (Treatment Abroad, Citation2015). The standard of these services is also considered to be high (Health and Wellness Tourism in Poland, Citation2014). The development of medical tourism in Poland is particularly evident through the prism of inbound tourism (Borek, Citation2013). The number of medical tourists in Poland is still not fully recognised. Most frequently the numbers are just rough estimates, and sometimes speculation from industry reports (Ruka & Garel, Citation2015). Nevertheless, these indicators were observed, and at the government level medical tourism was included in the strategy for the development of tourism in Poland, as a tourist product with high competitiveness and a priority for expansion. Currently, the medical tourism market in Poland is in its initial phase, and the relations on this market are not homogeneous. They constitute a reflection of numerous links between network entities: both medical and tourist, and also medical and tourist related (Lubowiecki-Vikuk & Rab-Przybyłowicz, Citation2015).
In 2011–2014, the medical tourism market in Polish urban areas was dominated by domestic tourists. Britons accounted for one-third and Germans for one-fifth of foreign tourists (Lubowiecki-Vikuk & Rab-Przybyłowicz, Citation2015). Among the British, Poland is the most frequently chosen medical tourism destination (preceding Hungary, Thailand, Turkey and Spain) (2015 Medical Travel Trends: United Kingdom, Citation2015). This is particularly evident in the choice by patients undergoing dental treatment, among which crowns and veneers are very common. Poland’s competitors are primarily Hungary, and also Croatia and Lithuania (Felkai, Citation2008; Jónás-Berki, Csapó, Pálfi, & Aubert, Citation2015). Lunt et al. (Citation2014) proved that this is due to the factors such as availability, cost, tourism, negative experience of National Health Service care, and dissatisfaction with UK private options. It is striking that Hungary, in the long term, can become a strong competitor to the Polish market.
The added value of the present work, which contributes to the development of marketing management in medical tourism, encompasses the cognitive and applied dimensions. As regards the empirical part, the results of this study contribute to the scholarly understanding of the way Britons and Germans evaluate MTDs and medical services in CEE. Given the high credibility of data collection, measurement and analysis, this pioneering research within the medical tourism studies may serve as a solid and reliable basis for further studies. The findings of the current research also extend the medical tourism theory, which served as the theoretical basis for the study. The survey results indicate also managerial implications for medical tourism facilitators/brokers and destination management organisations as they suggest that in the process of creating a medical tourism product, special attention should be given to the medical tourists’ nationality, and then to their age and gender, to make the specific medical service match those factors.
The limitations of the study may offer opportunities for future research. Due to time and cost constraints of the project, only empirical studies among Britons and Germans were carried out, whereas the other Western countries were omitted. Future research with a broader scope, including the other countries, would offer a fuller, more holistic perspective on MTDs and medical services in CEE.
Disclosure statement
No potential conflict of interest was reported by the authors.
References
- 2015 Medical Travel Trends: United Kingdom. (2015). Report. MEDIGO. Retrieved from https://www.medigo.com/blog/featured-articles/2015-medical-travel-trends-united-kingdom/
- Andrei, C. L., Ţigu, G., Drăgoescu, R. M., & Sinescu, C. J. (2014). Analysis of medical tourism for cardiovascular diseases. Amfiteatru Economic, 16(8), 1136–1150.
- Beladi, H., Chao, C.-C., Ee, M. S., & Hollas, D. (2015). Medical tourism and health worker migration in developing countries. Economic Modelling, 46, 391–396. doi:10.1016/j.econmod.2014.12.045
- Borek, E. (2013). Medical tourism in Europe and in Poland—Present status, development bariers, perspectives and recemendations concerning the development of medical tourism in Poland. Zdrowie Publiczne i Zarządzanie, 11(4), 333–348. doi:10.4467/20842627OZ.14.033.2172
- Bušelić, M., & Pavlović, D. K. (2003). Communication—A factor for improving the access to and quality of healthcare services. In Management and organization development (pp. 139–146). Kranj: Modern Organization.
- Cameron, K., Crooks, V. A., Chouinard, V., Snyder, J., Johnston, R., & Casey, V. (2014). Motivation, justification, normalization: Talk strategies used by Canadian medical tourists regarding their choices to go abroad for hip and knee surgeries. Social Science & Medicine, 106, 93–100. doi:10.1016/j.socscimed.2014.01.047
- Choi, H. (2015). Medical tourism. In J. Jafari & X. Hiao (Eds.), Encyclopedia in tourism (pp. 1–2). Switzerland. Springer International Publishing. doi:10.1007/978-3-319-01669-6_129-1
- Cohen, I. G., & Prall, E. (2015). Medical tourism. In T. Cook & J. M. Ryan (Eds.), The Wiley Blackwell encyclopedia of consumption and consumer studies (p. 168). Chichester. Wiley-Blackwell. doi:10.1002/9781118989463.wbeccs168
- Connell, J. (2013). Contemporary medical tourism: Conceptualisation, culture and commodification. Tourism Management, 34, 1–13. doi:10.1016/j.tourman.2012.05.009
- Culley, L., Hudson, N., Rapport, F., Blyth, E., Norton, W., & Pacey, A. A. (2011). Crossing borders for fertility treatment: Motivations, destinations and outcomes of UK fertility travelers. Human Reproduction, 26(9), 2373–2381. doi:10.1093/humrep/der191
- The European Parliament. (2011). Directive 2011/24/EU of the European Parliament and of the Council of 9 March 2011 on the application of patients’ rights in cross-border healthcare. Official Journal of the European Union, 50(88), 45–65.
- Dryglas, D., & Salamaga, M. (2018). Segmentation by push motives in health tourism destinations: A case study of Polish spa resorts. Journal of Destination Marketing & Management, 9, 234–246. doi:10.1016/j.jdmm.2018.01.008
- Felkai, P. (2008). Travel medicine in Eastern Europe—The Hungarian way. Travel Medicine and Infectious Disease, 6(4), 195–200. doi:10.1016/j.tmaid.2008.04.002
- Fetscherin, M., & Stephano, R. M. (2016). The medical tourism index: Scale development and validation. Tourism Management, 52, 539–556. doi:10.1016/j.tourman.2015.08.010
- Freedman, D. A. (2009). Statistical models: Theory and practice. Berkeley, CA: Cambridge University Press.
- Halecki, O. (1952). Borderlands of Western civilization. A history of East Central Europe. New York, NY: The Ronald Press Company.
- Health and Wellness Tourism in Poland. (2014). Report. Euromonitor International. Retrieved from http://www.euromonitor.com/health-and-wellness-tourism-in-poland/report
- OECD and European Union. (2014). Health at a Glance: Europe 2014. OECD Publishing. doi:10.1787/health_glace_eur-2014-en
- Holliday, R., Bell, D., Hardy, K., Hunter, E., Jones, M., Probyn, E., & Sanchez-Taylor, J. (2015). Beautiful face, beautiful place: Relational geographies and gender in cosmetic surgery tourism websites. Gender, Place & Culture, 22(1), 90–106. doi:10.1080/0966369X.2013.832655
- Jónás-Berki, M., Csapó, J., Pálfi, A., & Aubert, A. (2015). A market and spatial perspective of health tourism destinations: The Hungarian experience. International Journal of Tourism Research, 17(6), 602–612. doi:10.1002/jtr.2027
- Karmowska, G., & Marciniak, M. (2015). Spatial diversification of living standards in the former communist countries of Central and Eastern Europe and the Balkans. Comparative Economic Research, 18(4), 123–138. doi:10.1515/cer-2015-0032
- Kesar, O., & Rimac, K. (2011). Medical tourism development in Croatia. Zagreb International Review of Economics & Business, 14(2), 107–134.
- Kiss, K. (2015). The challenges of developing health tourism in the Balkans. Tourism, 63(1), 97–110.
- Kłoczowski, J. (1995). East Central Europe in the historiography of the countries of the region. Lublin: Institute of East Central Europe.
- Lockington, D., Johnson, R., Patel, D. V., & McGhee, C. N. J. (2014). Healthcare and a holiday: The risks of LASIK tourism. Clinical and Experimental Optometry, 97(4), 370–372. doi:10.1111/cxo.12121
- Lubowiecki-Vikuk, A. (2016). Participation in medical tourism versus physical activity of patients after liposuction: What are the concerns about health and quality of life? Physical Culture and Sport. Studies and Research, 69(1), 29–42. doi:10.1515/pcssr-2015-0027
- Lubowiecki-Vikuk, A. (2018). Consumption of dental services: Medical tourism in CEE. European Journal of Service Management, 27/1(3), 135–142. doi:10.18276/ejsm.2018.27/1-16
- Lubowiecki-Vikuk, A., & Kurkowiak, J. (2017). Medical tourism potential of Central and Eastern Europe: Attempt at classification. CBU International Conference Proceedings, 5, 286–293. doi:10.12955/cbup.v5.940
- Lubowiecki-Vikuk, A., & Rab-Przybyłowicz, J. (2015). Wybrane aspekty funkcjonowania rynku turystyki medycznej w Polsce. Folia Turistica, 34, 85–107.
- Lunt, N., & Carrera, P. (2010). Medical tourism: Assessing the evidence on treatment abroad. Maturitas, 66(1), 27–32. doi:10.1016/j.maturitas.2010.01.017
- Lunt, N., & Horsfall, D. (2014). Medical tourism. Encyclopedia of Health Economics, 3, 263–270. doi:10.1016/B978-0-12-375678-7.00615-5
- Lunt, N., Smith, R. D., Mannion, R., Green, S. T., Exworthy, M., Hanefeld, J., … King, H. &. (2014). Implications for the NHS of inward and outward medical tourism: A policy and economic analysis using literature review and mixed-methods approaches. Health Services and Delivery Research, 2(2), 1–234. doi:10.3310/hsdr02020
- Maguire, A., Bussmann, S., Meier zu Köcker, C., Verra, S. E., Giurgi, L. A., & Ruggeri, K. (2016). Raising concern about the information provided on medical travel agency websites: A place for policy. Health Policy and Technology, 5(4), 414–422. doi:10.1016/j.hlpt.2016.07.001
- Main, I. (2014). Medical travels of Polish female migrants in Europe. Czech Sociological Review, 50(6), 897–918. doi:10.13060/00380288.2014.50.6.147
- Medizintourismus IUBH Touristic-Radar. (2016). Retrieved from http://www.iubh.de/files/Medizintourismus/IUBH_Themenmappe_Medizintourismus_rz.pdf
- Melsheimer, N., & Weiß, W. (2014). Medizintourismus. In German: Auftrag der ERGO Direkt Versicherungen, März 2014. Retrieved from http://www.stifo.de/publikationen/studienreihe-2014/studie-1-medizintourism.html
- Messinis, I. E., Messini, C. I., Daponte, A., Garas, A., & Mahmood, T. (2016). The current situation of infertility services provision in Europe. European Journal of Obstetrics & Gynecology and Reproductive Biology, 207, 200–204. doi:10.1016/j.ejogrb.2016.10.004
- Panteli, D., Augustin, U., Röttger, J., Struckmann, V., Verheyen, F., Wagner, C., & Busse, R. &. (2015). Informed consumer or unlucky visitor? A profile of German patients who received dental services abroad. Community Dentistry and Oral Epidemiology, 43(5), 415–423. doi:10.1111/cdoe.12164
- Rab-Przybyłowicz, J. (2014). Produkt turystyki medycznej. Warszawa: Difin.
- Ruka, E., & Garel, P. (2015). Medical tourism. Report, September 2015. Brussels: HOPE – European Hospital and Healthcare Federation. Retrieved from http://www.hope.be/05eventsandpublications/docpublications/98_medical_tourism/98_HOPE_Medical-Tourism_September_2015.pdf
- Runnels, V., & Carrera, P. M. (2012). Why do patients engage in medical tourism? Maturitas, 73(4), 300–304. doi:10.1016/j.maturitas.2012.08.011
- Satorra, A., & Bentler, P. M. (1994). Corrections to test statistics and standard errors in covariance structure analysis. In A. Von Eye & C. C. Clogg (Eds.), Latent variables analysis: Applications for developmental research (pp. 399–419). Thousand Oaks, CA: Sage.
- Smith, M., Puczkó, L., Michalkó, G., Kiss, K., & Sziva, I. (2016). Balkan wellbeing and health tourism study. Final Report. Budapest: Metropolitan University. Retrieved from http://infota.org/wp-content/uploads/2016/03/BalkanWellbeingFINALREPORT.pdf
- Treatment Abroad. (2015). Compare the cost of treatment abroad. Retrieved from http://www.treatmentabroad.com/costs
- United Nations Group of Experts on Geographical Names. (2016). East Central and South-East Europe division. Retrieved from http://ecseed.zrc-sazu.si/
- Wisla, R., & Sierotowicz, T. (2016). Medical technological specializations of Central and Eastern European regions. Economics & Sociology, 9(3), 195–209. doi:10.14254/2071-789X.2016/9-3/17