
Abstract
The aim of the article is fourfold: (1) to identify the level of health consciousness during the pandemic in Slovakia and Croatia, and to point out the possible influence of selected demographic factors on this rate, (2) to identify the degree of consumer ethnocentrism during the pandemic in Slovakia and Croatia and to examine the impact of selected demographic factors to this extent, (3) to examine the link between health consciousness as a factor affecting consumer ethnocentrism and (4) to identify differences in the studied variables of Croatia and Slovakia. The article is supported by a primary survey based on 459 respondents in Croatia and 429 respondents in Slovakia. Whilst referring to our aims, we formulated research questions and hypotheses, in order to answer and verify them we chose ANOVA test and regression analysis. The results point to a high level of respondents' health awareness and an average (in the case of Slovakia) and above-average (in the case of Croatia) rate of consumer ethnocentrism. The results indicate a low relationship between the variables examined. Results can be applied both in theory and in practice in various fields.
1. Introduction
In addition to its impact on public health, coronavirus disease 2019 (Covid-19) caused a huge economic shock (Bartik et al., Citation2020) with significant economic consequences (OECD, Citation2020; Fornaro & Wolf, Citation2020). The authors of the Chaudhary leadership (Chaudhary et al., Citation2020) state that the outbreak of coronavirus resulted in the cessation of social and economic life. The team of authors led by Albu et al. (Citation2020) anticipate that the pandemic expansion of Covid-19 will result in a huge global crisis in all humanitarian, social and economic areas. An increase in the coronavirus pandemic results in a decrease in economic activity (Barro et al., Citation2020), including an increase in unemployment (International Labour Organization (ILO),),), Citation2020) all around the world (Gil-Alana & Poza, Citation2022; McKibbin & Roshen, Citation2020). According to The Economist (Citation2020), the negative impact of the pandemic on business is very strong. The COVID-19 pandemic has had a significant impact not only on the economy as a whole, but also on a significant deterioration in asset quality across different institutional types and sizes, or countries' profiles (Yarovaya et al., Citation2020; Rizvi et al., Citation2020a) as well as a crucial impact on human capital efficiency (Mirza et al., Citation2020). At the same time, the effect of the pandemic can also be identified on the revenues of non-financial firms within the European Union (Rizvi et al., Citation2020b). Rubeo and Baroud (Citation2020) state that it is creating opportunities for fundamental changes because of the global crisis caused by the new pandemic. Williams (Citation2020) pointed out the huge influence of the pandemic on the physical, mental, and social well-being of the population. Such critical situation pushes human behaviour in different directions (Mehta et al., Citation2020) and according to Pandelică et al. (Citation2012) shows new trends in consumer behaviour during this period. Which, for example, according to Kantar (Citation2020) can be reflected in a change in consumer attitudes, behaviour and expectations. However, Flatters and Willmott (Citation2009) found that it is possible to predict how customers will behave after a recession by just by conducting ex post analyses of their previous behavioural tendencies during such recessions. Many authors also point to the importance of health regarding consumer behaviour, whether in the form of health awareness, patients' rights, consumer policy or in the context of economic prosperity. Such a change in a way consumers act can also lead to consumer ethnocentrism (Lesáková, Citation2016). Several studies have found that ethnocentric consumers prefer to buy domestic products over foreign ones (Areiza-Padilla et al., Citation2020; Lee et al., Citation2020). Based on what Akdogan et al. (Citation2012) suggest, the negative attitudes of these consumers towards foreign products may be influenced by several factors, such as the political or economic situation, military or diplomatic events.
The origin of ethnocentrism can be found in social psychology in the context of the study of ethnicities (groups of nations). William Graham Sumner (Citation1906) was the first American psychologist to describe the idea of ethnocentrism in his work Folkways: A Study of the Sociological Importance of Usages, Manners, Customs, Mores, and Morals in 1906. Sumner (Citation1906) characterized ethnocentrism as “the technical name for this view of things in which onés own group (referred to as in-group) is the centre of everything, and all others (referred to as out-group) are scaled and rated with reference to it” (Sumner, Citation2007). The positive aspect of the definition is its versatility, which creates opportunities for various applications. The limits of the definition can be considered to be just the naming of the phenomenon. Depending on the subject, which is characteristic for the given group, it can be linguistic, racial, regional, but also consumer ethnocentrism. According to Baylor (Citation2016), from a marketing point of view, this refers to consumers who prefer goods produced on the domestic market and at the same time those who assume their own cultural superiority (Baylor, Citation2016).
2. Literature review and development of hypothesis and research questions
2.1. Health-conscious consumer behaviour
As a basis, it is necessary to understand where this concept derives from and thus to understand what health represents. The World Health Organization (WHO) defines health as "a state of complete physical, mental and social well-being and not merely the absence of disease or infirmity"(WHO, Citation2020). Health consciousness refers to the extent to which an individual tends to perform health actions (Gould, Citation1988). Gould (Citation1990) defined health consciousness as the inner state of man in terms of health. Health consciousness can be understood as a type of stimulation that encourages consumers to take action to promote health and prevent diseases (Jayanti & Burns, Citation1998; Michaelidou & Hassan, Citation2008). According to Lockie et al. (Citation2002) and Hartman and Wright (Citation1999) the level of health consciousness also influences consumers' shopping behaviour. The level of consumer health consciousness can be measured with the help of Health Consciousness Scale (HCS) (Gould,Citation1988). Čvirik (Citation2020) has already pointed out the significance of this tool in the fight against COVID-19.
RQ1: What is the general level of health consciousness?
There is a presumption that different levels of HCS will be influenced by various factors. We decided to focus on examining the impact of demographic factors, specifically age, gender and education (Gould, Citation1988; Čvirik, Citation2020). Coronavirus should be seen in the context of health, with consumers over the age of 65 being the most vulnerable segment (Adler, Citation2020) and consumers under the age of 18 being the least vulnerable segment, with only about 1% of cases identified in consumers under 10 (Wu & McGoogan, Citation2020). It is therefore logical that some age groups will achieve a different level of health consciousness in the context of the current pandemic situation.
H1: There is a relationship between the age of the respondents and their health consciousness.
H2: There is a relationship between the gender of the respondents and their health consciousness.
H3: There is a relationship between the educations of the respondents and their health consciousness.
2.2. Consumer ethnocentrism
Shimp and Sharma (Citation1987) have been called the creators of the theory of consumer ethnocentrism in the scientific field. They consider consumer ethnocentrism to be a belief, i.e. a strong internal belief that the purchase of foreign products is wrong. These experts are also looking for a reason why it is wrong for ethnocentric consumers to buy imported products. They cite as the main reasons that the purchase of foreign products damages the domestic economy, causes unemployment and is considered to be rather unpatriotic. Due to the internal beliefs of the ethnocentric consumer, it is unacceptable for him to support the out-group (abroad) and thus damage his in-group (domestic). The positive aspect of the definition is the clear identification of in-group and out-group groups, as well as the classification of the reasons for refusing out-group for the ethnocentric consumer.
The measurement of consumer ethnocentrism is possible thanks to the tool - Consumer Ethnocentrism Tendencies Scale (CETSCALE), which includes seventeen elements. It is also important to update and modify CETSCALE with respect to the object's specifications.
RQ2: What is the degree of consumer ethnocentrism?
The creators of the phenomenon of consumer ethnocentrism, Shimp and Sharma (Citation1987), have already observed differences in the degree of ethnocentrism based on age. They concluded that younger consumers are less ethnocentric than the older ones. Caruana and Magri (Citation1996), and Klein and Ettensoe (Citation1999) agree with this statement, and they have reached the same results based on empirical research. Newer studies such as Grundey and Bakowska (Citation2008) and Lesáková (Citation2016) have also shown the tendency of older consumers to be more ethnocentric. However, some authors consider this conclusion to be ambiguous. Sharma et al. (Citation1995) did not show a significant statistical link between age and consumer ethnocentrism. Based on qualitative research, Schooler (Citation1971) concluded that age has a negative attitude towards ethnocentrism. The age limits of the segments are different for different authors, often undefined, which may be the reason for the differentiation of the results.
H4: There is a relationship between age and the level of consumer ethnocentrism.
Gender as a second factor in consumer behaviour has been studied by many experts. Sharma et al. (Citation1995) concluded that women are more ethnocentric than men. The authors Bruning (Citation1997) and Lesáková (Citation2016) also ended up with a similar research result. Caruana and Magri (Citation1996) and Balabanis (Balabanis et al., Citation2001) did not show a link between gender and ethnocentrism based on quantitative research. A study by Bannister and Saunders (Citation1978) shows, based on qualitative research, that men in Britain achieve a higher degree of ethnocentrism than women.
H5: There is a relationship between gender and the level of consumer ethnocentrism.
The study of the difference in the level of formal education obtained and the degree of consumer ethnocentrism has been the subject of research in several studies. Sharma et al. (Citation1995) concluded in a sample of American consumers that consumers with higher education are less ethnocentric. The author team Kaynak and Kara (Citation2002) came to similar conclusions. Balabanis et al. (Citation2001) did not show a link between the factor and consumer ethnocentrism.
H6: There is a relationship between education and the level of consumer ethnocentrism.
2.3. Theoretical connection between health consciousness and consumer ethnocentrism
Based on quantitative research, Klein and Ettensoe (Citation1999) have shown that if consumers are convinced that the national economy is improving, they show a lower level of ethnocentrism and, conversely, if the state of the domestic economy is bad, the level of ethnocentrism increases to improve the situation. Many other studies show (Good & Huddleston, Citation1995; Durvasula et al., Citation1997) that the rate of ethnocentrism may increase as conditions worsen in the country. Considering the current pandemic situation, it is likely that consumers will achieve a higher degree of consumer ethnocentrism. However, it can be assumed that this situation will arise only for consumers who have a higher level of health consciousness (health perception). The available literature has never examined this relationship.
RQ3: What is the intensity and trend of the effect of health consciousness on consumer ethnocentrism?
2.4. International character
In this work we examine two important concepts (health awareness and consumer ethnocentrism). Many studies recommend examining these theories in different countries, as there is a number of factors that can affect the level of consumer ethnocentrism and health awareness, such as degree of patriotism (Sharma et al., Citation1995), the economic system of the country (Rosenblatt, Citation1964), the political history of the nation (Good & Huddleston, Citation1995), culture (Suh & Kwon, Citation2002), the state-led system of measures against COVID-19 and many others. Research suggests that the subjects of the article need to be examined at the international level. Therefore, we decided to conduct research in two countries - Slovakia and Croatia.
RQ4: How can the differences between Slovakia and Croatia be characterized?
3. Methods and methodology
The aim of the article is fourfold: (1) to identify the level of health consciousness during the pandemic in Slovakia and Croatia, and to point out the possible influence of selected demographic factors on this rate, (2) to identify the degree of consumer ethnocentrism during the pandemic in Slovakia and Croatia and to examine the impact of selected demographic factors to this extent, (3) to examine the link between health consciousness as a factor affecting consumer ethnocentrism and (4) to identify differences in the studied variables (health awareness and consumer ethnocentrism) in the conditions of Croatia and Slovakia.
Based on the stated aims, we formulated four research questions and six hypotheses. We examined hypotheses and research questions in the conditions of two countries - Croatia and Slovakia.
In this work we use a number of general philosophical methods (analysis, synthesis, abstraction, induction, deduction), mathematical-statistical methods (descriptive statistics, inductive statistics, estimates of reliability, simple modelling) as well as scientific research methods (qualitative methods, query methods).
3.1. Sample
The article is based on secondary data from the available literature, but in order to meet the set aims, it was necessary to conduct primary research as well. The primary research was in the nature of a quantitative survey, which was based on a questionnaire survey. The survey was conducted in two countries, namely in Croatia and Slovakia. In both cases, the samples were non-probable, which considerably limits their explanatory power.
The basic population for Croatia was characterized as: consumers of Croatian nationality over 15 years of age. The reason for choosing the element of nationality was crucial with regard to the identification of consumer ethnocentrism. The age limit was defined due to the fact that from the age of about 15 consumers make their purchases, have some income and create decision-making and shopping behaviour. A total of 476 respondents took part in the survey, but due to the characteristics of the basic population, we had to adjust the sample (eliminating respondents who had a different nationality or did not reach a defined age). The final sample represented 459 respondents.
The basic population for Slovakia was defined as: consumers of Slovak nationality over 15 years of age. The limits for defining the generic population were the same as in Croatia, specifically nationality and age. A total of 461 respondents took part in the survey, but due to the characteristics of the basic population, we had to filter the sample and the final outcome represented 429 respondents.
We recorded the basic characteristics of the samples in in terms of the examined (selected) demographic variables as well as their individual values.
Table 1. Characteristics of samples.
It should be noted that the demographic characteristics of the sample do not reflect the demographic parameters of the basic population. For a sample of 459 and 429 respondents, the maximum statistical error (with a 95% confidence probability) is at most 5%.
Health consciousness measurements were performed using the Health Consciousness Scale (HCS) (Gould, Citation1988). The tool consists of nine scale questions, to which the respondent expresses the degree of his (dis)agreement, so it can be stated that it is a response to a statement based on the Likert scale. We use a five-point Likert scale, with 1 representing strongly disagreement and 5 representing strongly agreement. From the above, it can be stated that the rate of HCS will range from 9 points to 45 points (the middle value of the scale is 27 points). We recorded the interpretation of individual statements as well as the mean values, standard deviations, and the value of the Cronbach's alpha in .
Table 2. Basic parameters of HCS in Croatia and Slovakia.
As this is an adaptation of a foreign research tool (HCS), it was necessary to verify its internal consistency as well as its reliability. Cronbach's alpha was chosen for this purpose. As we can see, the overall reliability of the tool reached a high value in the conditions of Croatia as well as in Slovakia. Experts recommend interpreting a Cronbach's alpha value below 0.600 as acceptable for the initial stage of research, but a minimum value of 0.700 is recommended for the advanced stage. Tavakol and Dennick (Citation2011) state that the acceptable value of Cronbach's alpha is above 0.700, but for high quality and reliable results the ideal value is above 0.800. As can be seen from , we achieve high reliability in both countries (Croatia 8.867 and Slovakia 0.856). From a practical voice, it is important to examine not only the overall reliability of the tool, but also its elements. As we can see, excluding any statement would not increase the reliability of the research tool, so we consider the tool to be put together correctly in both countries. As can be seen from , the standard deviation is relatively low, indicating similarity of response to individual statements.
The degree of consumer ethnocentrism was measured based on the research tool CETSCALE (Shimp & Sharma, Citation1987). The tool in the original version contains 17 statements, to which the respondent responds with consent, respectively disagreement, the intensity of which is distributed on a five-point Likert scale, with strong agreement representing a value of 5 and strong disagreement representing a value of 1. From the above it can be stated that the measured values will be in the range of 17-85 points (mean value of the tool is 51 points). The average value for the individual statements, as well as the standard deviation and Cronbach's alpha for both countries studied, were recorded in . As an example, we present the original range published by Shimp and Sharma (Citation1987), which was created for American consumers. Of course, the statements were adapted to the conditions of individual countries, and thus to the consumers of the individual countries studied.
Table 3. Basic parameters of CETSCALE in Croatia and Slovakia.
As we can see, based on Cronbach's alpha, we can state the high reliability of the tool in both countries. From the point of view of individual statements, it is clear that we could have further increased the reliability of the instrument in the case of Croatia, if we omitted statement no. 5. In the case of Slovakia, it is obvious that the statements are set correctly, but removing statement no. 3 and no. 13, we would have an equally reliable tool. We recorded the greatest difference in the statements of the respondents in both countries in the statements no. 16. (st. dev. 1.33).
4. Results
In this part of the paper, we will focus on answering research questions and verifying the hypotheses.
RQ1: What is the general level of health consciousness?
Based on measurements performed with HCS. The average measured value under Croatian conditions is 34.91 points with a standard deviation of 5.75 points. The median is 36 points, and the mode is 36 points. From the above, we can conclude that Croatian respondents currently achieve a high above-average health consciousness (approximately 71.98%).
In the case of Slovakia, an average value of 33.16 points was measured with a standard deviation of 5.93 points. The mode and median are at the level of 33 points. Based on the above, it can be concluded that the sample achieves an above-average level of health consciousness (approximately 67.12%).
H1: There is a relationship between the age of the respondents and their health consciousness.
H2: There is a relationship between the gender of the respondents and their health consciousness.
H3: There is a relationship between the level of educations of the respondents and their health consciousness.
Hypotheses H1, H2 and H3 examine the relationship between demographic factors and the level of health consciousness. We tested the hypotheses based on a one-way ANOVA test. Selected (essential) results of the ANOVA test were recorded in . We verified the above-mentioned hypotheses in the conditions of Croatia and Slovakia.
Table 4. Results of the one-way ANOVA test for hypotheses H1, H2 and H3.
As shown in , the confidence level was set to the default value of 95%. At the level of the given value of reliability we can confirm that only H2 is true in case of Croatia, so there is a relationship between the level of health consciousness and gender (alpha > P-value; F-value > F-value crit.). Since the average value of health consciousness in the sample for women was slightly higher than for men, it can be stated that women in the Croatian sample were statistically significantly more health conscious than men. Hypothesis 1 (H1) in both conditions, Hypothesis 2 (H2) in the conditions of the Slovak sample, and Hypothesis 3 (H3) in both investigated conditions are to be rejected.
RQ2: What is the degree of consumer ethnocentrism?
The level of consumer ethnocentrism was measured based on CETSCALE.
The average measured value in the Croatian sample was 58.15 points with a standard deviation of 14.06 points. The mode was 62 points, and the median was 60 points. Based on the above-mentioned parameters, we evaluate the rate of consumer ethnocentrism to be above average (approximately 60.51%).
The average measured value in the Slovak sample was 49.28 points (st. dev. 13.67). The mode was at the level of 37 points and the median was 49. Overall, we rate consumer ethnocentrism as average - to below average (approximately 47.48%).
H4: There is a relationship between age and the level of consumer ethnocentrism.
H5: There is a relationship between gender and the level of consumer ethnocentrism.
H6: There is a relationship between education and the level of consumer ethnocentrism.
Hypotheses H4, H5 and H6 examine the relationship between selected demographic factors and consumer ethnocentrism. Hypothesis verification was performed based on a one-way ANOVA test. Selected values (indicators) of the test were recorded in for both examined samples.
Table 5. Results of the one-way ANOVA test for hypotheses H4, H5 and H6.
As can be seen from the , we can state the confirmation of H4, H5 and H6 in the conditions of both examined samples at the level of reliability of 95% (alpha > P-value; F-value > F-value crit.).
RQ3: What is the intensity and trend of the effect of health consciousness on consumer ethnocentrism?
To determine the trend and the extent of the action of two quantities, we chose a linear regression analysis. The ANOVA test was used to evaluate the model selection. We can state its suitability in both examined samples.
In the case of the Croatian Multiple R, the value is 0.317, which can be interpreted as a weak dependence. The regression line explains about 10% of the variability between the variables. The straight line has a positive character. In general, we can state a low dependence rate.
In case of Slovakia, Multiple R represents 0.119, which indicates a very low dependence (almost none). About 98.6% of the variability is not explained by the regression line, which demonstrates a very low level of dependence. The straight line has a positive character. In general, we can state a very low dependence.
RQ4: How can the differences between Slovakia and Croatia be characterized?
Given the scale of the research, we need to answer the question on three levels - the level of health awareness, the level of consumer ethnocentrism and the level of exploring the interconnection of these two concepts.
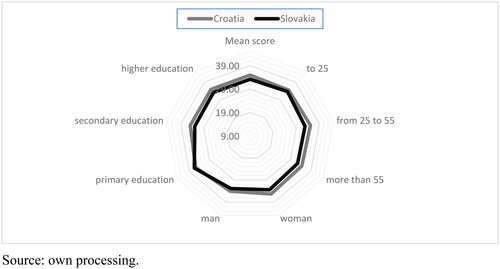
For better clarity, we have constructed based on the level of health awareness, which also points to the differences in individual segments. As we can see, the Croatian sample is very balanced in all examined segments in terms of average value of segments. The situation is similar for the Slovak sample, which, however, contains slight fluctuations. In general, it can be stated that the sample from Croatia achieves a higher overall level of health awareness.
Graph 1. Health awareness rate based on examined segment.
Source: own processing.
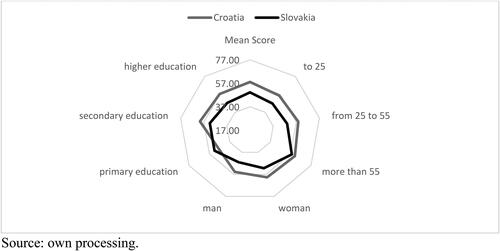
illustrates the situation regarding consumer ethnocentrism. As we can see, the line is considerably deformed in both cases, which indicates a strong influence of the investigated factors. We can also notice that the Croatian sample line surrounds Slovakian in all cases, except for the segment with basic education, where the Slovak sample is more consumer ethnocentric. Overall, it can be stated that the Croatian sample achieves a higher degree of consumer ethnocentrism.
Graph 2. The degree of consumer ethnocentrism within the examined segments.
Source: own processing.
In the case of both Croatia and Slovakia, it can be argued that older respondents are more consumer ethnocentric than younger ones (H4). In the case of Croatia and Slovakia, it can be stated that women achieve a higher level of health consciousness than men (H5). In the case of Slovakia, it can be stated that less educated consumers achieve a higher degree of consumer ethnocentrism, while in the case of the Croatian sample it is quite the opposite - more educated consumers achieve a higher degree of consumer ethnocentrism (H6).
It can also be noted that to a certain (low) extent, consumer ethnocentrism in the Croatian sample is influenced by health awareness. The Slovak sample does not show a relationship between consumer ethnocentrism and health-conscious consumer behaviour.
5. Discussion
The measured value of health-conscious consumer behaviour appears to be highly above average in both examined samples. The reason may be the ongoing emergency situation regarding COVID-19, which appeals to the health awareness of citizens, high prevention and hygiene education. Of course, in the future it would be appropriate to verify whether this rate will increase or decrease due to the improving/deteriorating situation. The minimal influence of demographic factors (apart from gender in the Croatian sample) on the level of health awareness is surprising. The reason may be the high level of vigilance due to COVID-19, which concerns everyone. Of course, we have segments that are more vulnerable, but the behaviour of young respondents also proves their high level of awareness.
The rate of consumer ethnocentrism is significantly higher in the Croatian sample (about 13%). There may be several reasons for the outcome again. It would be useful to examine more closely all the measures that work in each country to increase the level of consumer ethnocentrism. The topic is very relevant also with regard to COVID-19, which, as it limits human lives, also obscures the economy of individual states. It is consumer ethnocentrism that could be the key to restarting the domestic economy and prosperity. We can indicate a strong influence of selected demographic factors on consumer ethnocentrism, however we can also see in the case of education that the influence is the opposite in case of Croatia, compared to Slovakia. We can therefore state that it is necessary to examine in more detail not only the existence of the relationship between demographic factors and consumer ethnocentrism, but also a thorough study of the effects of these factors and subsequent international comparison, which we believe will yield interesting results.
We have not been able to demonstrate the effect of health awareness on consumer ethnocentrism. However, it should be noted that in the Croatian sample this connection was significantly stronger than in the Slovak sample. There may be several reasons. The measures that individual countries are implementing in the fight against COVID-19 may not be fully accepted by the population, which may lead to a reduction in the level of consumer ethnocentrism. It should also be noted that health awareness does not copy the situation and the development of COVID-19. The situation regarding COVID-19 is constantly changing and requires careful scrutiny. We must realize that even if the pandemic is averted, it will be necessary to diagnose and treat the economic consequences it will leave behind.
6. Conclusion
The aim of the article was fourfold: (1) to identify the level of health consciousness during the pandemic in Slovakia and Croatia, and to point out the possible influence of selected demographic factors on this level, (2) to identify the degree of consumer ethnocentrism during the pandemic in Slovakia and Croatia and to examine the impact of selected demographic factors to this extent, (3) to examine the link between health consciousness as a factor affecting consumer ethnocentrism and (4) identify differences in the studied variables (health awareness and consumer ethnocentrism) in the conditions of Croatia and Slovakia.
We managed to meet the goals to complete extent.
We measured the level of health consciousness in both examined samples (both Croatian and Slovak), to be above the average. Considering the demographic factors, the influence of gender was confirmed, but only in the Croatian sample. Other selected demographic factors (age and education) did not show statistical significance. The rate of consumer ethnocentrism was above average in the Croatian sample, but in the Slovak sample it was at the level of the average - even below average. The influence of selected demographic factors (age, sex, education) was confirmed as statistically significant in both examined samples. On a theoretical level, the impact of health consciousness on consumer ethnocentrism is observed, but in terms of actual outcomes, only a tiny dependency is found in Croatia, and much lower results are seen in case of Slovakia. Therefore, it cannot be confirmed that health consciousness has an impact on the level of consumer ethnocentrism.
Research also has some limitations. Due to the selection of the sample, the results cannot be fully generalized. As this is a questionnaire survey, it is not possible to verify the veracity of individual statements of respondents. In the future, we would recommend extending the survey to other countries, looking for possible effects on consumer ethnocentrism, as well as specifying the factors affecting health consciousness. It is health consciousness that can act as an effective means of prevention during a pandemic.
The benefits of the article can be characterized from both theoretical and practical points of view. The universality of health consciousness measurement at the time of the pandemic was demonstrated in both countries studied. In the case of using CETSCALE, it is necessary to consider certain modifications that could lead to a higher reliability of the research tool. At the same time, we contributed and expanded the body of knowledge related to both examined variables (health consciousness and consumer ethnocentrism).
Acknowledgments
We thank the editor and anonymous reviewers for their comments, which contributed to the improvement of the submitted article. The article was adapted under the project “I-22-104-00 Ethnocentrism and its influence on consumer behaviour: measurement, determinants, strategic and intervention options.”
Disclosure statement
In accordance with Taylor & Francis policy and our ethical obligation as researchers, we are reporting that we have not a financial and/or business interests in a company that may be affected by the research reported in the enclosed paper.
References
- Adler, S. E. (2020). Why coronaviruses hit older adults hardest. https://www.aarp.org/health/conditions-treatments/info-2020/coronavirus-severe-seniors.html
- Akdogan, M. S., Ozgener, S., Kaplan, M., & Coskun, A. (2012). The effects of consumer ethnocentrism and consumer animosity on the re-purchase intent: The moderating role of consumer loyalty. EMAJ: Emerging Markets Journal, 2(1), 1–12. https://doi.org/10.5195/EMAJ.2012.15
- Albu, L. L., Preda, C., Lupu, R., Dobrotă, C. E., Călin, G. M., & Boghicevici, C. M. (2020). Estimates of dynamics of the covid19 pandemic and of its impact on the economy. Romanian Journal for Economic Forecasting, 0(2), 5–17. https://ideas.repec.org/a/rjr/romjef/vy2020i2p5-17.html
- Areiza-Padilla, J. A., Cervera-Taulet, A., & Manzi Puertas, M. A. (2020). Ethnocentrism at the coffee shop industry: A study of starbucks in developing countries. Journal of Open Innovation: Technology, Market, and Complexity, 6(4), 164. https://doi.org/10.3390/joitmc6040164
- Balabanis, G., Diamantopoulos, A., Mueller, R. D., & Melewar, T. C. (2001). The impact of nationalism, patriotism and internationalism on consumer ethnocentric tendencies. Journal of International Business Studies, 32(1), 157–175. https://doi.org/10.1057/palgrave.jibs.8490943
- Bannister, J. P., & Saunders, J. A. (1978). UK consumers’ attitudes towards imports: the measurement of national stereotype image. European Journal of Marketing, 12(8), 562–570. https://doi.org/10.1108/EUM0000000004982
- Barro, R. J., Ursúa, J., & Weng, F. J. (2020). The coronavirus and the great influenza pandemic: Lessons from the “Spanish flu” for the coronavirus’s potential effects on mortality and economic activity. NBER Working Paper No. National Bureau of Economic Research. https://doi.org/10.3386/w26866
- Bartik, A. W., Bertrand, M., Cullen, Z., Glaeser, E. L., Luca, M., & Stanton, C. (2020). The impact of COVID-19 on small business outcomes and expectations. Proceedings of the National Academy of Sciences of the United States of America, 117(30), 17656–17666. https://doi.org/10.1073/pnas.2006991117
- Baylor, E. (2016). Ethnocentrism. Oxford Biblografies, https://doi.org/10.1093/OBO/9780199766567-0045
- Bruning, E. (1997). Country of origin, national loyalty and product choice: case of international air travel. International Marketing Review, 14(1), 59–74. https://doi.org/10.1108/02651339710159215
- Caruana, A., & Magri, E. (1996). The effects of dogmatism and social class variables on consumer ethnocentrism in Malta. Marketing Intelligence & Planning, 14(4), 39–44. https://doi.org/10.1108/02634509610121569
- Chaudhary, M., Sodani, P. R., & Das, S. (2020). Effect of COVID-19 on economy in India: Some reflections for policy and programme. Journal of Health Management, 22(2), 169–180. https://doi.org/10.1177/0972063420935541
- Čvirik, M. (2020). Health conscious consumer behaviour: The impact of a pandemic on the case of Slovakia. Central European Business Review, 9(4), 45–58. https://doi.org/10.18267/j.cebr.249
- Durvasula, S., Andrews, J. C., & Netemeyer, R. G. (1997). A cross-cultural comparison ofconsumer ethnocentrism in the United States and Russia. Journal of International Consumer Marketing, 9(4), 73–93. https://doi.org/10.1300/J046v09n04_05
- Flatters, P., & Willmott, M. (2009). Understanding the post-recession consumer. Harvard Business Review, july–august 2009. https://ogur.org/154716.pdf
- Fornaro, L., & Wolf, M. (2020). Covid-19 coronavirus and macroeconomic policy. Economics Working Papers 1713. Department of Economics and Business, Universitat Pompeu Fabra. https://www.barcelonagse.eu/sites/default/files/working_paper_pdfs/1168.pdf
- Gil-Alana, L. A., & Poza, C. (2022). The impact of COVID-19 on the Spanish tourism sector. Tourism Economics, 28(3), 646–653. https://doi.org/10.1177/1354816620959914
- Good, L. K., & Huddleston, P. (1995). Ethnocentrism of Polish and Russian consumers: are feelings and intentions related? International Marketing Review, 12(5), 35–48. https://doi.org/10.1108/02651339510103047
- Gould, S. J. (1988). Consumer attitudes toward health and health care: A differential perspective. Journal of Consumer Affairs, 22(1), 96–118. https://doi.org/10.1111/j.1745-6606.1988.tb00215.x
- Gould, S. J. (1990). Health consciousness and health behaviour: The application of a new health consciousness scale. American Journal of Preventive Medicine, 6(4), 228–237. https://doi.org/10.1016/S0749-3797(18)31009-2
- Grundey, D., & Bakowska, S. (2008). Consumer economics: Brand awareness among Polish consumers. Transformations in Business & Economics, 7(2), 186–199. https://www.researchgate.net/publication/286063373_Consumer_economics_Brand_awareness_among_Polish_consumers
- Hartman, H., & Wright, D. (1999). Marketing to the new natural consumer: Consumer trends forming the wellness category 0th. The Hartman Group, 267. ISBN-10: 1929027001.
- International Labour Organization (ILO). (2020). Almost 25 million jobs could be lost worldwide as a result of COVID-19, says ILO. https://www.ilo.org/global/about-the-ilo/newsroom/news/WCMS_738742/lang–en/index.htm
- Jayanti, R. K., & Burns, A. C. (1998). The antecedents of preventive health care behaviour: an empirical study. Journal of the Academy of Marketing Science, 26(1), 6–15. https://doi.org/10.1177/0092070398261002
- Kantar. (2020). COVID-19 Barometer. The leading syndicated study on how COVID-19 is influencing consumer behaviour, attitudes and expectations, covering over 60 markets. https://www.kantar.com/Campaigns/Covid-19-Barometer
- Kaynak, E., & Kara, A. (2002). Consumer perceptions of foreign products: An analysis of product-country images and ethnocentrism. European Journal of Marketing, 36(7/8), 928–949. https://doi.org/10.1108/03090560210430881
- Klein, J. G., & Ettensoe, R. (1999). Consumer animosity and consumer ethnocentrism: ananalysis of unique antecedents. Journal of International Consumer Marketing, 11(4), 5–24. https://doi.org/10.1300/J046v11n04_02
- Lee, H.-M., Chen, T., Chen, Y.-S., Lo, W.-Y., & Hsu, Y.-H. (2020). The effects of consumer ethnocentrism and consumer animosity on perceived betrayal and negative word-of-mouth. Asia Pacific Journal of Marketing and Logistics, 33(3), 712–730. https://doi.org/10.1108/APJML-08-2019-0518
- Lesáková, D. (2016). Ethnocentric behaviour in the Slovak population: do Slovaks purchase Slovak dairy products? Ekonomický Časopis, 64(8), 795–807.
- Lockie, S., Lyons, K., Lawrence, G., & Mummery, K. (2002). Eating 'green': motivations behind organic food consumption in Australia. Sociologia Ruralis, 42(1), 23–40. https://doi.org/10.1111/1467-9523.00200
- McKibbin, W. J., & Roshen, F. (2020). The global macroeconomic impacts of COVID-19: Seven scenarios. CAMA Working Paper No. 19/2020. SSRN. https://doi.org/10.2139/ssrn.3547729
- Mehta, S., Saxena, T., & Purohit, N. (2020). The new consumer behaviour paradigm amid COVID-19: Permanent or transient? Journal of Health Management, 22(2), 291–301. https://doi.org/10.1177/0972063420940834
- Michaelidou, N., & Hassan, L. M. (2008). The role of health consciousness, food safety concern and ethical identity on attitudes and intentions towards organic food. International Journal of Consumer Studies, 32(2), 163–170. https://doi.org/10.1111/j.1470-6431.2007.00619.x
- Mirza, N., Hasnaoui, J. A., Naqvi, B., & Rizvi, S. K. A. (2020). The impact of human capital efficiency on Latin American mutual funds during Covid-19 outbreak. Swiss Journal of Economics and Statistics, 156(1), 16. https://doi.org/10.1186/s41937-020-00066-6
- OECD. (2020). Interim economic assessment coronavirus: The world economy at risk. https://www.oecd.org/berlin/publikationen/Interim-Economic-Assessment-2-March-2020.pdf
- Pandelică, A., Diaconu, M., & Pandelică, I. (2012). From market orientation to the community orientation for an open public administration: A conceptual framework. Procedia - Social & Behavioural Sciences, 62, 871–875. https://doi.org/10.1016/j.sbspro.2012.09.146
- Rizvi, S. K. A., Mirza, N., Naqvi, B., & Rahat, B. (2020a). Covid-19 and asset management in EU: a preliminary assessment of performance and investment styles. Journal of Asset Management, 21(4), 281–291. https://doi.org/10.1057/s41260-020-00172-3
- Rizvi, S. K. A., Yarovaya, L., Mirza, N., & Naqvi, B. (2020b). The impact of COVID-19 on valuations of non-financial European firms. SSRNhttps://doi.org/10.2139/ssrn.3705462
- Rosenblatt, P. C. (1964). Origins and effects of group ethnocentrism and nationalism. Journal of Conflict Resolution, 8(2), 131–146. https://doi.org/10.1177/002200276400800204
- Rubeo, R., & Baroud, R. (2020). Will the coronavirus change the world? On Gramsci’s ‘Interregnum’ & Zizek’s ethnocentric philosophy. https://www.scoop.co.nz/stories/HL2004/S00159/will-the-coronavirus-change-the-world-on-gramsci-s-interregnum-zizek-s-ethnocentric-philosophy.htm
- Schooler, R. D. (1971). Bias phenomena attendant to the marketing of foreign goods in the US. Journal of International Business Studies, 2(1), 71–81. Retrieved December 30, 2020, from http://www.jstor.org/stable/154727 https://doi.org/10.1057/palgrave.jibs.8490732
- Sharma, S., Shimp, T. A., & Shin, J. (1995). Consumer ethnocentrism: a test of antecedents and moderators. Journal of the Academy of Marketing Science, 23(1), 26–37. https://doi.org/10.1007/BF02894609
- Shimp, A. T., & Sharma, S. (1987). Consumer ethnocentrism: Construction and validation of the CETSCALE. Journal of Marketing Research, 24(3), 280–289. https://doi.org/10.2307/3151638
- Suh, T., & Kwon, I. G. (2002). Globalization and reluctant buyers. International Marketing Review, 19(6), 663–680. https://doi.org/10.1108/02651330210451962
- Sumner, W. G. (1906). Folkways: A study of the sociological importance of usages, manners, customs, mores and morals (pp. 692). Ginn and company.
- Sumner, W. G. (2007). Folkway: A study of the sociological importance of usages, manners, customs, mores, and morals. Cosimo Classics, 704.
- Tavakol, M., & Dennick, R. (2011). Making sense of Cronbach's alpha. International Journal of Medical Education, 2(1), 53–55. https://doi.org/10.5116/ijme.4dfb.8dfd
- The Economist. (2020). The new coronavirus could have a lasting impact on global supply chains. https://www.economist.com/international/2020/02/15/the-new-coronavirus-could-have-a-lasting-impact-on-global-supply-chains?cid1=cust/ednew/n/bl/n/2020/02/29n/owned/n/n/nwl/n/n/AP/415278/n
- WHO. (2020). Constitution. https://www.who.int/about/who-we-are/constitution
- Williams, T. (2020). The impact of COVID-19. Journal of Perioperative Practice, 30(5), 114–115. https://doi.org/10.1177/1750458920919642
- Wu, Z., & McGoogan, J. M. (2020). Characteristics of and important lessons from the coronavirus disease 2019 (COVID-19) outbreak in China: summary of a report of 72, 314 cases from the Chinese Center for Disease Control and Prevention. JAMA, 323(13), 1239–1242. https://doi.org/10.1001/jama.2020.2648
- Yarovaya, L., Mirza, N., Rizvi, S. K. A., & Naqvi, B. (2020). COVID-19 pandemic and stress testing the eurozone credit portfolios. SSRN, Preprint, (October 5, 2020). https://doi.org/10.2139/ssrn.3705474