
 ?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.
?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.Abstract
Healthy China is a crucial policy for advancing global health, addressing inequality between rural and urban health education, and helping the domestic markets recover after the COVID-19 outbreak. This study combines life cycle mechanisms and safety beliefs to evaluate the long-lasting values of health education. We employed data from the China Migration Dynamic Surveys to examine the economic behaviours of 720,900 immigrants using a robust empirical approach combining an Extended Regression Model (E.R.M.), Average Treatment Effects (A.T.E.), and heterogeneous treatment effects. We find that health education increases participation in social medical insurance and the likelihood of purchasing a house. In contrast, the relationship between health education and saving rates is non-linear effects. Empirically robust heterogeneous treatment effects account for heterogeneity in the previous and the younger generations, as well as urban and rural citizens’ long-run effects of health education. This study’s findings suggest that health education stimulates immigrants’ consumption behaviours; however, extra health education is not desirable. Rural-urban citizenship acquisition bias is found to significantly affect health education.
1. Introduction
COVID-19 has disrupted international investment and exports. As a result, the global industry chain is reconstructing itself. Stimulating consumption is essential to improve the current economic slowdown. In particular, improving the potential consumption of immigrants is crucial for boosting China’s future economic growth (ESPAS, Citation2018).
Previous studies have confirmed that immigration has contributed to production and economic development (Alesina & Stantcheva, Citation2020; Borjas, Citation2009; Mazzolari & Neumark, Citation2012). Bodvarsson’s (Citation2008) analysis of the effects of the inflow of Cuban immigrants on production suggest that immigration has a positive impact on retail sales per capita and consumer demand. Borjas’ (Citation2019) study on the effects of immigrants on production found that immigrants is a key contributor to economic growth; however, this is dependent on several variables, including the skill of immigrants, rate of assimilation, distributional labour market consequences, immigration surplus, potential human capital externalities, and long-term consumption impact.
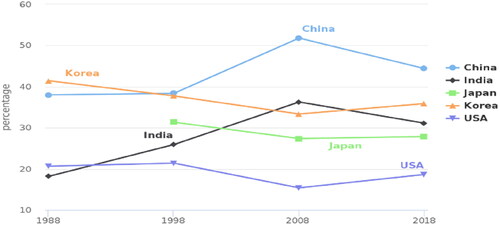
Despite the relatively scarce research on the link between immigration and economic growth, there is no doubt that immigrants contribute significantly to the aggregate output through consumption demand. reports the proportion of savings rates to the gross domestic product (GDP) from 1988 to 2018. Compared with other countries, China has accounted for the highest savings rates during this period. Korea ranked second, while the USA had low savings rates. However, from 2018 to 2019, China and India’s rates declined, while that of Korea, Japan, and the USA increased by 35.85%, 27.84% and 18.62%, respectively, indicating that increased consumption incentivises labour productivity and economic development. In China, immigrants have substantially contributed to urbanisation since 1984; in this study, immigration refers to inner migration.
Figure 1. Proportion of saving rates to G.D.P.Footnote8
Source: the world bank.
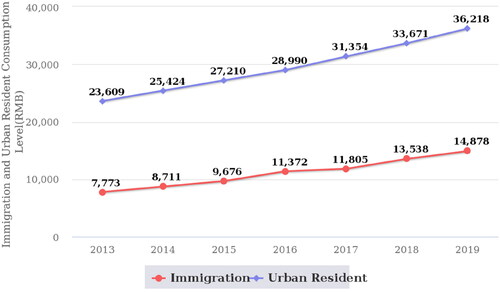
However, the consumption inequality between immigrants and urban residents is obviously phenomenon across China (Carlos Citation2020; Midrigan & Xu, Citation2014). illustrates the consumption elasticity of immigrants and urban residents in China. Significant consumption gaps are observed between the two groups. Therefore, understanding how immigrants’ consumption potential may be increased is the key to expanding domestic demand (Li et al., Citation2018).
Figure 2. Consumption levels of immigrants and urban residents.Footnote9
Source: China Migration Dynamic Survey evaluated by author.
Recent studies have emphasised on the association between health inequality and consumer demand (Stait & Calnan, Citation2016; Sweet, Citation2011). Good health increases individual productivity and human capital returns, which reduce income inequality and increase opportunities of securing a job at a higher wage rate (Aguayo-Rico et al., Citation2005; Ray & Linden, Citation2018). Good health education can help prevent certain illnesses and increase individual productivity; however, health education inequalities and the economic burden of illness increases an individual’s propensity to save (Raghupathi & Raghupathi, Citation2020). China has improved its health education by introducing the Healthy China initiative in 2017. The country has advocated that the residents’ health education coverageFootnote1 would reach 45% in 2019, and pro-health behaviours would achieve 30% by 2030.Footnote2 Although China has gradually spread the reach of its retirement insurance system and boosted health awareness, significant discrepancies are still observed between rural and urban health education. This often leads to a decrease in consumption and an increase in savings among immigrants for facing possible future illnesses; thus, the relationship between health education inequality and consumption need to be analysed through a framework where consumption gaps between urban residents and immigrants are filled.
There is, however, a lack of studies exploring the causal impact of health education on immigrants’ economic behaviours in developing countries. This study addresses the research gap regarding the impact of health education on economic behaviours, particularly on immigrants.
This study contributes to the existing literature through the following. First, using microeconomic data from China Migrants Dynamic Surveys (C.M.D.S.), we show that health education positively influences immigrants’ behaviours, stimulating consumption, involvement in social health insurance, and house purchase. Second, using a large sample of 720,900 immigrants, we show that migration from urban to urban areas generate more benefits from health education than that from rural to rural areas. Third, we suggest that health education affects an individual’s future and attitudes towards savings, social health insurance, and house purchase. Hence, the World Health Organization (W.H.O.) and United Nations commissions should be aware of the importance of health education for economic recovery and prosperity.
The remainder of this article is organised as follows. Section 2 reviews the related literature on the impact of health education on economic behaviour. Section 3 presents the empirical methods and data. Section 4 describes the causal effects of health education. Section 5 discusses the study’s findings and contributions.
2. Literature review and research hypotheses
2.1. Health education and outcomes
The literature on the relationship between health education and economic behaviours is scant but increasing. It mainly focuses on the effectiveness of health education on individual health outcomes, addressing the use of condoms, medical care, obesity, and daily intake of fruits and vegetables (Cingano, Citation2014; Civitelli et al., Citation2020; Hurley, 2020; Miguel 2016; Weathers & Stegman, Citation2012). For example, Dursun et al. (Citation2018) used nationally representative health data from Turkey to show that health education has positive effects on the body mass index (B.M.I.) and obesity in men. However, they did not find any significant effects of health education on the daily consumption of fruits. Similarly, Duflo et al. (Citation2015) estimated that the H.I.V. education programmes on early fertility effectively reduced the school for international training (S.I.T.) in Kenya. Regarding the relationship between health and individual economic behaviours, one potential view is that lack of health insurance prompts higher precautionary savings, especially for immigrants, in line with Chamon and Prasad (Citation2010), who empirically analysed developing countries. Wagstaff and Pradhan (Citation2005) focused on Vietnam and found that health education positively affected household consumption. Some studies have focused on the correlation between health education and welfare, taking distribution effectiveness into account. For instance, Goldin (Citation2020) claimed that Italy's global health education reduced health inequality and social justice. Dupas and Miguel (Citation2016) showed that improved health education in low-income countries increased well-being and promoted economic development. However, some studies reported that education had little or no effect on health behaviours and welfare. For example, Janke et al. (Citation2020) used Quarterly Labour Force Survey (Q.L.F.S.) data to explore the relationship between education and chronic health in the U.K., finding that extra education had no impact on the prevalence of chronic illnesses. Zajacova and Lawrence (Citation2018) showed that health education reproduced inequality across generations.
The role of health education in economic behaviours was analysed using two perspectives based on current literature (Costa-Font & Cowell, Citation2019; Dupas & Miguel, Citation2017; Dursun et al., Citation2018; Finlay, Citation2007; Mukong et al., Citation2017), namely, the direct human capital effect and the indirect incentive effect. The human capital effect asserts that individuals who had better health education had higher wages and consumption demand (Borjas, Citation2019; Ding & He, Citation2018). The incentive effect argues that individuals who had better health education had a higher probability of a greater life expectancy, which the incentive to purchase a house and social insurance (Stait & Calnan, Citation2016). Thus, health education played an indirect role in economic behaviours.
The above-mentioned studies suggest that the effects of health education inequality on economic behaviours could be substantial but diverse (Engleman & Forbes, Citation1986; Heckman et al., Citation2018; Jie & Xi, Citation2020; Piketty, Citation2014). Since health education inequality, whether urban or rural, has a major impact on consumption demand and medical insurance, attention must be paid to the relationship between health education inequality and economic behaviours of immigrants.
We explore how health education affects economic outcomes based on the life cycle hypothesis (Boone, Citation2019; Komenaka et al., Citation2015; Lee et al., Citation2020). The life cycle hypothesis is used to examine two mechanisms concerning health education-induced bias in time perception. The first mechanism involves the direct influence of health education on increasing income and consumption demand (Mazzolari & Neumark, Citation2012; Wagstaff et al., Citation2009; Weathers, Citation2012). The second is the incentive effect of expectation utility among immigrants about having an uncertain future.
Under Boone’s (Citation2019) life cycle model, suppose an immigrant needs to decide whether to save now in exchange for securityFootnote3 in the future. If the immigrant does not worry about having a safety network, they will prefer to consume. Suppose that the immigrant’ expectation utility at time t is defined as the consumption is represented by
is the immigrant’s income,
is uncertain about future income growth, and
represents interest rates. If future security’s discount rates is
then, the immigrant prefers to consume only if:
(1)
(1)
(2)
(2)
Various studies provided evidence of the direct effects of health education on economic behaviours. Weil (Citation2009) and Madrian (Citation2014) showed that there was a link between poverty reduction and long-term economic growth that was impacted by health. Muller (Citation2017) further suggested that health education in the USA had a significant effect on income and savings, which means that residents might prefer consumption in the present as they have better health education.
Health education indirectly affects economic behaviour by changing an individual’s perspective towards distant, future safety-related events. For example, it seems plausible that health education increases confidence, decreasing the pressure of future illness and thoughts on retirement, and thereby decreasing worry about a future safety net (Xue et al., Citation2020; Zajacova & Lawrence, Citation2018). Hoynes et al. (Citation2006) proved that healthcare utilisation and health status impacted immigrants’ income and savings since welfare reforms resulted in significant effects on family health awareness, inducing the decision to save. One potential caveat is that it is not possible to directly predict the effects of health education on saving and consumption. Health education, as a relief from the life cycle, could potentially affect economic behaviours (Goldin, Citation2020). Considering health security in the future, immigrants decide to save, thus feeling as if the possible illness was more distant.
In a precautions savings model, this effect can be represented by security rates. Suppose that weak or strong health education leads immigrants to derive utility from security rates generating a different willingness to save:
(3)
(3)
This expression indicates how health education affects savings and consumption decisions. Therefore, we propose the following proposition:
Proposition 1. Health education has a negative impact on savings rates.
2.2. Health education and consumption behaviours
Ray and Linden (Citation2018) showed that health education may affect future choices by guiding immigrants to have more or less confidence about their future, such as by having pension or living security. Confidence increases attention towards one’s life conditions. Recent studies have investigated the relation between health education and life expectations. Several individuals expect to live longer than their actuarial life expectancy (Pentek, Citation2014; Rappange et al., Citation2016). Immigrants who receive more health education may improve their living conditions and live longer. For example, Health awareness positively affected self-reported well-being but do not influence health outcomes. Cutler and Lleras-Muney (Citation2010) suggested that health education helps an individual gain more resources, including better housing, food, quality of care, and living environment.
Other studies focus on the relation between health education and health insurance. Feinstein (Citation2006) claimed that health education helps promote and sustain healthy lifestyles and positive choices. Ro (2016) further suggest that low health educational attainment is related with self-reported poor health, shorter life expectancy, and shorter survival when sick. Felder (2020) showed that increased health education induced an insurance effect, increasing awareness and making investments on living conditions more critical. However, some studies have pointed out that health education negatively affects economic behaviours too (Cutler & Lleras-Muney, Citation2006). Health education may result in increased attention to preventive care and health medical insurance, which, though beneficial in the long term, raises healthcare costs in the short term (Zimmerman, Citation2014).
Where and
are the respective confidence beliefs related to lower and higher health education in immigrants; the
and
represent consumption demand from lower and higher health education in immigrants; decision-maker with confidence beliefs
would devote less attention to future security than one who holds beliefs
(4)
(4)
In other words, since the discount on health education implies that the value of future rewards is a strictly convex function of time, uncertainty about the pension security payoffs makes saving more attractive. Note that EquationEquation 3(3)
(3) implies that immigrants with lower health education would save, plan more, and consume less (i.e., purchasing a house and worrying about health security). Therefore, we propose the following propositions:
Proposition 2: Health education induces participation in social medical insurance.
Proposition 3: Health education has a positive effect on the likelihood to purchase a house.
3. Empirical strategy
3.1. Data collection
To investigate the relationship between immigrants’ health education and future economic behaviour at the micro-level, we employed data from the C.M.D.S., an annual longitudinal survey of Chinese immigrant communities, families, and individuals launched in 2009 by the Institute of National Health Commission. A multistage, random cluster, proportion to the scale sampling method is applied in each province. The survey collects information such as the scope of migration, immigrants’ employment, social security, income and expenditure, basic public health services within the community, social integration and other health services. This data set covers 31 provinces and the Xinjian production and construction corps of China. There were approximately 200,000 households in the annual survey, with a representative sample of approximately 209.37 million individuals in 2014. The panel data set included information from 500,000 immigrants, the total sample in 2016 accounted for approximately 169,000 observations, with 450,000 immigrating families. The sample in 2017 included 170,000 family observations, with 450,000 individuals. The rural-level sample comprised 10,000, 10,000, 8500 and 85,000 observations in 2014, 2015, 2016 and 2017, respectively.
3.2. Measures
3.2.1. Health education decisions
The essential elements of sequential decision models are decision nodes. At each node, agents consider the benefits and costs to make the next investment decision. The sequential decision models are as follows:
(5)
(5)
EquationEquation (5)(5)
(5) presents a general sequential decision model, where
is the perceived cost for agents at node
;
represents the possibility sets of agent node transitions. We assume
meaning that agents never make decision at nodes
means that agents make the least node transition from
or
shows the node transition
Figure 3. Health education choice.
Source: China Migration Dynamic Survey evaluated by author.
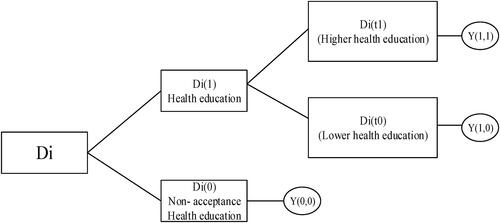
Where j = 2, T2=represents agents receiving health education in j = 1, while T2=
represents agent’s health education node transition in j = 1 and j = 2, respectively. According to Heckman (Citation2017), all decision nodes are:
(6)
(6)
where
and
are the observed and continuous choice outcomes in the sequential choice model, respectively. To estimate the health education returns at each choice node from we use the Average Treatment Effects (A.T.E.)Footnote4 and analyse agents’ two transition nodes (Callaway & Sant'Anna, Citation2019). Likewise, heterogeneous treatment effects are used to estimate the intergeneration transmission and resident-type continuous values (long-lasting values) at two transition nodes (Ben Jann et al., Citation2015).
3.2.2. Economic behaviours
Each immigrant family is asked about their monthly income and expenditure, these strategies allows us to calculate the savings rates of different cross-sections. The study’s sample has a unique advantage in that it reflects immigrants’ future economic behaviour allowing a cross-provincial comparison. Based on the first mechanism of the life cycle hypothesis, the following model is used to explore our propositions:
(7)
(7)
where
indicates family’s monthly saving rates, social health medical insurance, and house purchase;
represents an individual’s health education level;
comprises an individual’s control variables, and
is a random disturbance term. We estimate probit models to assess the propensity to save or consume; we then estimate the effect of an individual’s health education on future economic outcomes controlling for individual characteristics, as well as country and year fixed effects. Doing so, we examine the effect of health education on savings by assessing the extent to which an immigrant participates in health education. To a limited extent, this approach helps us investigate Proposition 1. In addition, we use a probit model to analyse the impact of health education on social health medical insurance and house purchase. Together, these results allow us to investigate Proposition 2.
3.2.3. Health education among immigrants
W.H.O. defines health education as the awareness of a precautious illness and the ability to make a correct judgement to improve future health (Simonds, Citation1974). In this study, we adopt the C.M.D.S. survey measurement (whether an individual in a community has received health education in the past year). The detailed method is as follows: First, considering health education may include various topics, such as occupational disease prevention, H.I.V., reproductive health and contraception, tuberculosis prevention, smoking control, mental health, chronic disease prevention, and maternal and child health care/eugenics. All answers are rated using a seven-point Likert scale (Berens et al., Citation2016; Toçi et al., Citation2014) to objectively assess immigrants’ health education. Second, as long as immigrants participate in health education, we assign one point. The score for non-reception of health education is zero, while reception of health education ranges from 1 to 9. Third, we divide the scores into lower and higher health education based on the median score. Therefore, differences in the acquisition of health education and health education levels may be considered the most direct tests of the three proposed research propositions.
4. Results
4.1. Descriptive statistics
The descriptive statistics of the study’s sample are presented in . After adopting the above-mentioned selection criteria, the final sample comprises 720,900 observations. Columns 1, 4 and 5 of report the number of observations of the base sample for the independent, dependent, and control variables. Column 2 presents the means of the variables used in the regression analysis, and Column 3 reports the standard deviations in parentheses.
Table 1. Descriptive statistics.
4.2. Evaluation of economic behaviours
We first present the Ordinary Least Squares (O.L.S.) and probit estimation results for health education returns. Next, we address the endogeneity of health education and economic behaviours using Extended Regression Models (E.R.M.), and finally, we evaluate the health education continuous variable using the A.T.E. and heterogeneous treatment effects in a sequential choice frame.
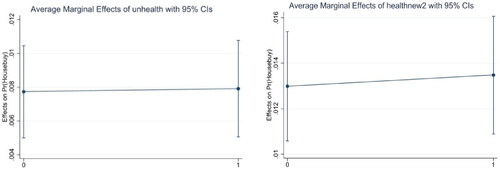
present the Average Marginal Effects (A.M.E.) in all health education sequential choice frames. shows that A.M.E. are −0.1343 and 0.049 in the first and second choice nodes, respectively. The marginal effects indicate indifference regarding the acquisition of health education and the health education levels. Compared with and , the continuous marginal effects of health education diminish for social medical insurance. This finding is consistent with current studies showing the positive impact of health education. Positive impact on participating in social medical insurance is more likely for lower health education groups (Cutler & Lleras-Muney, Citation2010; Heckman, Citation2017). However, we also find that the continuous values of marginal health effects increase the likelihood of purchasing a house.
Figure 4. Average marginal effects of health education on saving rates.
Source: China Migration Dynamic Survey evaluated by author.
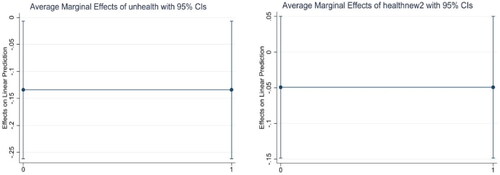
Figure 5. Average marginal effects of health education on social medical insurance.
Source: China Migration Dynamic Survey evaluated by author.
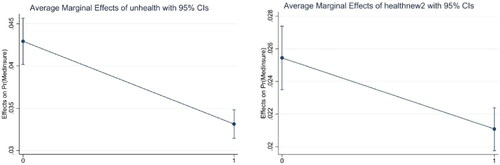
Figure 6. Average Marginal Effects of Health education on house purchasing.
Source: China Migration Dynamic Survey evaluated by author.
4.3. Casual effects of health education on economic behaviours
4.3.1. Interpreting instrumental variables
We address the potential endogeneity between health education and economic behaviours using the E.R.M. model and the ‘whether health documents are established in a village’ condition as an instrument. The presence of health documents in a village reflects the village’s and individuals’ health education level; however, it does not directly affect individual economic behaviours.
In terms of savings rates, we alleviate endogeneity using the E.R.M. model. presents the results of the instrumental variables (I.V.) estimation. Model (1) refers to the first-choice node, and Model (2) to the second choice node. The evaluation of the correlation error implies that health education and saving rates are endogenously determined; the Wald chi-square test for identifying weak instruments show significant critical values at the 10% level, meaning that the proposed instruments are effective. The I.V. coefficients are significant and negative in all samples, and Model (2) further implies that continuous health education values have significant effects on accepting health education.
Table 2. E.R.M. model of health education and saving rates (O.L.S.).
presents the I.V. estimation for social medical insurance and house purchase. Models (1) and (2) include a social medical insurance instrument, while Models (3) and (4) include a house purchase IV. The correlation error is significant at the 10% level, meaning that the ERM model effectively mitigates endogeneity. The weak instrument test significantly rejects the null hypothesis, proving that the instruments used in this study are valid.
Table 3. E.R.M. model returns to health education on Social Medical Insurance and purchasing house (eoprobit).
4.3.2. Average treatment effect of health education decision
We now move beyond the O.L.S. and probit methods to analyse the causal effects of health education returns on economic behaviours. reports evidence of A.T.E. through the health education choice. The estimated average casual effects are lower than the O.L.S. and probit regressions results in . The reason is that the average casual effect considering the sample selection bias and endogenous relationship between none-health education, accept health education and economic behaviours; lower health education, higher health education and economic behaviours (Imai et al., Citation2008).
Table 4. Decomposing treatment effects of health education.
In terms of A.T.E. of saving rates, we find that the returns to health education on saving rates have an inverted U shape, with larger negative effects on those who acquired health education in their first choice. We find no significant relationships between lower health education and higher health education. For social medical insurance, the A.T.E. are more likely to have positive effects on the first-choice node, by 3.97%. Last, we note that the A.T.E. of house purchase increase significantly as health education increases, by 2.97%.
4.4. Heterogeneous treatment effects
4.4.1. Intergenerational heterogeneity
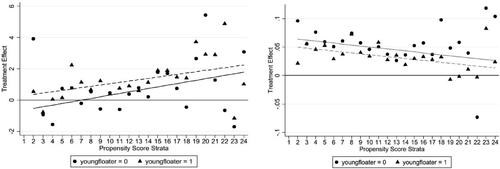
We also account for heterogeneity regarding health educational choices in the previous generation and younger generation.Footnote5 Generation was divided into previous and younger based on birth year. Heterogeneity treatment effects are used to further evaluate the three research propositions (Xie et al., Citation2012). and report the results of intergenerational heterogeneity treatment effects obtained by the Stratification-Multilevel (S.M.) Method, including first health educational choice nodes and second health educational choice nodes, respectively. presents the propensity score strata between the acceptance of health education in the previous generation and the younger generation.
Table 5. Heterogeneous treatment effects of intergeneration on first-choice nodes (S.M.).
Table 6. Heterogeneous treatments effects of intergeneration on second choice nodes (S.M.).
We find that the frequency count increases with the propensity score for those who receive health education in the previous generation. In contrast, the direction of the frequency count is opposite to the propensity score for the younger generation. A possible explanation is that the younger generation prefers to enjoy their life and leave safety beliefs for the future (Currie, 2003). However, the previous generation mostly needs to spend on family life and children's education, which makes them more unsafe in future life. The new generation shows a more significant effect of health education on participating in social medical insurance. One possible explanation is that the new generation of immigrants has a higher demand for public services such as medical care, is relatively more knowledgeable in health education, and has a higher awareness of insurance participation than the previous generation of immigrants. Similar results are obtained regarding house purchases. One possible explanation is that previous generations saved a lot but did not purchase houses. Hence, they are inclined towards a relatively stable investment. reports the propensity score strata between the previous higher health education generation and the younger generation. The younger higher health education generation is more willing to save and participate in social medical insurance than the previous generation. This result implies that the younger generation has awareness and pressure due to social ageing. Hence, they seem healthy as a result of their continuous health investments.
report the health educational heterogeneity outcomes. We find that improving health education to stimulate domestic consumption is not wise for younger generations with higher health education.
Figure 7. Health education heterogeneous effects on intergeneration transmission (Saving Rates).Footnote10
Source: China Migration Dynamic Survey evaluated by author.
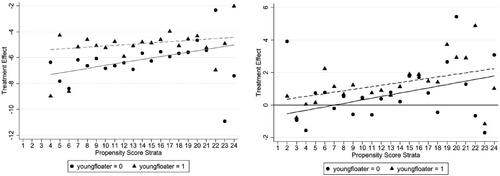
Figure 8. Health education heterogeneous effects on intergeneration transmission (Social Medical Insurance).
Source: China Migration Dynamic Survey evaluated by author.
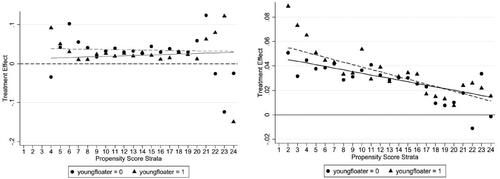
Figure 9. Health education heterogeneous effects on intergeneration transmission (House Purchasing).
Source: China Migration Dynamic Survey evaluated by author.
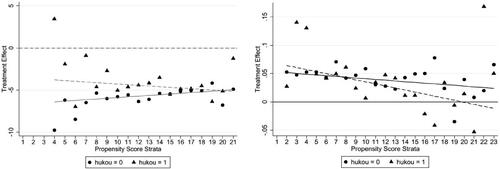
4.4.2. Urban citizenship acquisition
Urban citizenship determines one's level of wages and one's rights to access public services in Chinese cities. Although urbanisation almost equalised essential public health services in China, high-quality education and medical services are still distributed in the eastern coastal areas. This phenomenon implies that the different impacts of health education on the economic behaviour of immigrants are reflected in their urban citizenship acquisition, reflecting the type of HukouFootnote6 and the regional distribution of immigrants. Therefore, urban citizenship plays an essential role in the economic behaviour of immigrants. In this study, we further explore heterogeneity across urban and rural citizens.
and present the results for urban and rural citizenship heterogeneous treatment effects on health education. We find that the frequency count increases with the propensity score for rural citizens who receive health education. A possible explanation is that rural citizenship is typically acquired for work/business. Rural citizens have no long-term stable income or work. Hence, they rely on precautionary savings for facing future uncertainties. In terms of participating in medical insurance, the positive impact of health education on the probability of participating in social health insurance is more significant for rural citizens relative to urban citizens. One possible explanation is that the public health service gap between rural and urban areas is reduced; rural citizens have gradually gained awareness, participating in social health insurance. Furthermore, health education significantly stimulates rural citizens to buy a house in an inflow cityFootnote7 because purchasing a house represents urban residence Hukou and the rights to enjoy equality in medical public services. Further, a house means enjoying better public services and receive better children’s schooling; hence, rural citizens have a relatively higher willingness to purchase a house than urban citizens.
Table 7. Heterogeneous treatments effects of citizenship identification on first choice nodes (SM).
Table 8. Heterogeneous treatments effects of urban citizenship acquisition on second choice nodes (S.M.).
reports the higher health education heterogeneous effects between rural and urban citizens. Higher health education is beneficial for urban citizens, as rural immigrants have a relatively high savings rate and lower willingness to purchase a house.
This tendency is associated with real estate market bubbles and restrictions in the urban household registration system. Higher health education rural citizens do not significantly benefit from purchasing a house.
Consistent with some previous studies saying that health status affects purchasing house and well-being (Yamada et al., Citation2020), we also find that rural citizens with health education are more likely to purchase a house, participate in social medical insurance, and resort to saving (). Suppose they do not own a house in the city, they may not enjoy the same incentives as the local population in terms of medical care and education due to household registration policies; so, they need to own a house. However, higher health education has no positive effects on rural citizens; one possible reason is that real estate bubbles restrict them from purchasing a house, and the retirement issue leads them to limit consumption.
Figure 10. Health education heterogeneous effects on urban residents (Saving Rates).
Source: China Migration Dynamic Survey evaluated by author.
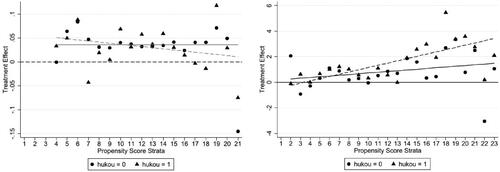
Figure 11. Health education heterogeneous effects on urban residents (Social Medical Insurance).Footnote11
Source: China Migration Dynamic Survey evaluated by author.
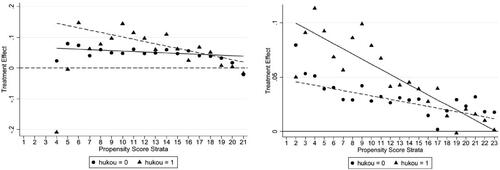
Figure 12. Health education heterogeneous effects on urban residents (House Purchasing).
Source: China Migration Dynamic Survey evaluated by author.
5. Discussion and conclusions
Most research on the economic behaviour of immigrants focuses on whether immigrants’ health education increases wages (Buck et al., Citation2016; George, Citation2019). In this article, we divide immigrants’ health education into two groups (accept health education and none-acceptance; lower health education and higher health education) to evaluate the impact of health education on immigrants’ economic behaviours using a sequential choice model.
Compared with some previous literature that suggests that health education positively affects economic outcome among immigrants (Kim et al., Citation2019; Stephen, 1986), we find robust evidence of the influence of health education on economic behaviours. First, an aggregate 1% increase in health education decreases saving rates by 13.4%, improves by 22.1% the probability of participating in social medical insurance, and rises by 3.61% the probability of purchasing a house in the first health educational nodes. Importantly, all the results support our three research hypotheses. However, an aggregate 1% increase in health education increases savings rates, improves by 9.52% the probability of participating in social medical insurance, and increases by 1.06% the likelihood of purchasing a house in higher health education samples.
We also analyse heterogeneous treatment effects of health education based on two aspects. First, we estimate the relationship between health education and intergeneration, implying that health education positively affects consumption and participation in social health medical insurance and house purchase, especially for the previous generation; however, better health education does not stimulate the younger generation’s consumption. Second, combining these results with However, higher health education does not stimulate urban citizens’ and the younger generation's consumption.
This study focuses more on the relationship between immigration health education and urban citizenship acquisition, finding that health education significantly increases the probability of purchasing a house among rural citizens in all health educational choice nodes, especially in higher education nodes. These results indicate that suitable health education improves economic behaviours. However, extra health education is not desirable.
Our findings support health education benefits of economic growth and consumption (Cesur, 2014; George, Citation2019). However, knowing the effects of health education in the long-run would require a more robust approach and more heterogeneous treatment effects aspects. Therefore, considering the endogenous issues, the importance of creating and spreading health education services must be emphasised, as health education services support individuals’ decision-making, allowing them to enjoy public services’ externalities as equally as possible. However, we have not considered the different effects between inflow and outflow cities due to data limits.
Author contributions
Jinhua Zhang: Data collection. Jialu You: Writing – Original draft; visualisation; writing – reviewing and editing; methodology; empirically analysing.
Competing interests
We declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgements
We acknowledge the research support of central research funds of University (CN) of Shanghai University of Finance and Economics (No. 20200521), and studies suggestions from 2021CES annuls.
Availability of data and materials
http://www.geodata.cn/wjw/#/data/classify/population/yearList. Public data from China Migrants Surveys.
Additional information
Funding
Notes
1 Health education coverage = access health education population/total population.
2 The data from National Health Commission of the people’s republic of China: http://www.nhc.gov.cn/
3 Retirement safety; health safety.
4 ATE(tj)=∫Yi(tj;1)−Yi(tj;0)df(X,θ,ε).
5 Bases on the characteristics of Chinese immigrants, those aged between 15 and 35 years are considered the new generation of immigrants (Young generation = 1), while those aged between 35 and 59 years are defined as the previous generation of immigrants (Young generation = 0).
6 Identification citizenship between rural and urban.
7 Purchasing House means transforming rural citizenship into urban citizenship, implying have the same rights with urban residence to enjoy city service, such as medical, education and public service.
8 The data from World Bank: https://www.worldbank.org/en/home.
9 The data from World Bank: https://www.worldbank.org/en/home. The blue line represents urban residents’ consumption; the red line represents immigrants’ consumption elasticity
10 We compare migrants who choose first nodes (unhealthy education and health education) and second nodes (lower health education and higher health education) same as Figures 9 and 10.
11 Hukou = 1 indicates migrants who are urban citizenship acquisition. Hukou = 0 means migrants who are rural citizenship acquisition.
References
- Aguayo-Rico, A., Guerra-Turrubiates, I. A., & de Oca-Hernández, R. M. (2005). Empirical evidence of the impact of health on economic growth. Issues in Political Economy, 14, 1–17.
- Alesina, A., & Stantcheva, S. (2020). Diversity, immigration, and redistribution. AEA Papers and Proceedings, 110, 329–334. https://doi.org/10.1257/pandp.20201088
- Berens, E. M., Vogt, D., Messer, M., Hurrelmann, K., & Schaeffer, D. (2016). Health literacy among different age groups in Germany: Results of a cross-sectional survey. BMC Public Health, 16, 1151. https://doi.org/10.1186/s12889-016-3810-6
- Bodvarsson, B. (2008). Measuring immigration's effects on labor demand: A reexamination of the Mariel Boatlift. Labour Economics, 15(4), 560–574. https://doi.org/10.1016/j.labeco.2008.04.003
- Boone, J. (2019). Health provider networks with private contracts: Is there under-treatment in narrow networks. Journal of Health Economics, 67(12), 102222. https://doi.org/10.1016/j.jhealeco.2019.102222
- Borjas, G. J. (2019). The wage impact of the marielitos: The role of race. ILR Review, 72(4), 858–870. https://doi.org/10.1177/0019793919825753
- Buck, D., Simpson, M., & Ross, S. (2016). The economics of housing and health – The role of housing associations. The King’s Fund.
- Callaway, B., & Sant'Anna, P. H. C. (2019). Difference-in-differences with multiple time periods. SSRN. https://doi.org/10.2139/ssrn.3148250
- Carlos (2020). Mortality and pulmonary complications in patients undergoing upper extremity surgery at the peak of the SARS-CoV-2 pandemic in the UK: A national cohort study. BMJ Quality & Safety, 30(4), 121–156.
- Chamon, M. D., & Prasad, E. S. (2010). Why are saving rates of urban households in China rising. American Economic Journal: Macroeconomics, 2(1), 93–130. https://doi.org/10.1257/mac.2.1.93
- Cingano, F. (2014). Trends in income inequality and its impact on economic growth [OECD Social, Employment and Migration Working Papers, No. 163]. OECD Publishing.
- Civitelli, G., Tarsitani, G., Rinaldi, A., & Marceca, M. (2020). Medical education: An Italian contribution to the discussion on global health education. Globalization and Health, 16(1), 30. https://doi.org/10.1186/s12992-020-00561-8
- Costa-Font, J., & Cowell, F. (2019). Incorporating inequality aversion in health-care priority setting. Social Justice Research, 32(2), 172–185. https://doi.org/10.1007/s11211-019-00328-6
- Cutler, D. M., & Lleras-Muney, A. (2006). Education and health: Evaluating theories and evidence. [NBER Working Papers, 12352].
- Cutler, D. M., & Lleras-Muney, A. (2010). Understanding differences in health behaviors by education. Journal of Health Economics, 29(1), 1–28. https://doi.org/10.1016/j.jhealeco.2009.10.003
- Ding, H., & He, H. (2018). A tale of transition: An empirical analysis of economic inequality in urban China, 1986–2009. Review of Economic Dynamics, 29, 106–137. https://doi.org/10.1016/j.red.2017.12.007
- Duflo, E., Dupas, P., & Kremer, M. (2015). Education, HIV, and early fertility: Experimental evidence from Kenya. The American Economic Review, 105(9), 2757–2797. https://doi.org/10.1257/aer.20121607
- Dupas, P., & Miguel, E. (2016). Impacts and determinants of health levels in low-income countries [NBER Working Papers 22235]. National Bureau of Economic Research Inc.
- Dupas, P., & Miguel, E. (2017). Impacts and determinants of health levels in low-income countries. In Handbook of economic field experiments (pp. 3–93). North-Holland Press.
- Dursun, B., Cesur, R., & Mocan, N. (2018). The impact of education on health outcomes and behaviors in a middle-income, low-education country. Economics and Human Biology, 31, 94–114. https://doi.org/10.1016/j.ehb.2018.07.004
- Engleman, S. R., & Forbes, J. F. (1986). Economic aspects of health education. Social Science & Medicine, 22(4), 443–458. https://doi.org/10.1016/0277-9536(86)90049-3
- ESPAS. (2018). Global trends to 2030: The future of migration and integration [ESPAS Ideas Paper Series]. European Strategy and Policy Analysis System.
- Feinstein, L. (2006). What are the effects of education on health? OECD Proceedings of the Copenhagen Symposium (pp. 172–184).
- Finlay, J. (2007). The role of health in economic development [PGDA Working Paper Series 21]. Harvard University.
- George, J. (2019). Immigration and economic growth [National Bureau of Economic Research, Working Paper 25836]. “Working Paper Series”. https://doi.org/10.3386/w25836
- Heckman, J. J. (2017). The Non-Market Benefits of Education and Ability (October 2017). NBER Working Paper No. w23896. https://ssrn.com/abstract=3049720
- Heckman, J. J., Humphries, J. E., & Veramendi, G. (2018). Returns to education: The causal effects of education on earnings, health, and smoking. Journal of Political Economy, 126(s1), S197–S246. https://doi.org/10.1086/698760
- Hoynes, H. W., Page, M. E., & Stevens, A. H. (2006). Poverty in America: Trends and explanations. Journal of Economic Perspectives, 20(1), 47–68. https://doi.org/10.1257/089533006776526102
- Imai, K., King, G., & Stuart, E. A. (2008). Misunderstandings between experimentalists and observationalists about causal inference. Journal of the Royal Statistical Society: Series A (Statistics in Society), 171(2), 481–502. https://doi.org/10.1111/j.1467-985X.2007.00527.x
- Goldin, J. (2020). Health insurance and mortality: Experimental evidence from taxpayer outreach. The Quarterly Journal of Economics, 24(9), 1–49.
- Janke, K., Johnston, D. W., Propper, C., & Shields, M. A. (2020). The causal effect of education on chronic health conditions in the UK. Journal of Health Economics, 70, 102252–102296. https://doi.org/10.1016/j.jhealeco.2019.102252
- Jann, B., Brand, J. E., & Xie, Y. (2014). HTE: Stata module to perform heterogeneous treatment effect analysis. Statistical Software Components S457129, Boston College Department of Economics.
- Jie, C., & Xi, Y. (2020). How is the potential consumption of citizenization of migrant population? Based on estimation on income elasticity of consumption of China’s migrant population in the new era. Urban and Environmental Studies, 1, 34–54.
- Kim, D.-H., Wu, Y.-C., & Lin, S.-C. (2019). Education, health, and economic development. Macroeconomic Dynamics, 23(2), 837–869. https://doi.org/10.1017/S1365100517000050
- Komenaka, I. K., Nodora, J. N., Hsu, C.-H., Martinez, M. E., Gandhi, S. G., Bouton, M. E., Klemens, A. E., Wikholm, L. I., & Weiss, B. D. (2015). Association of health literacy with adherence to screening mammography guidelines. Obstetrics & Gynecology, 125(4), 852–859. https://doi.org/10.1097/AOG.0000000000000708
- Lee, H. Y., Zhou, A. Q., Lee, R. M., & Dillon, A. L. (2020). Parents’ functional health literacy is associated with children’s health outcomes: Implications for health practice, policy, and research. Children and Youth Services Review, 110(1), 104801–104887. https://doi.org/10.1016/j.childyouth.2020.104801
- Li, K., Wang, X.-F., Li, D.-Y., Chen, Y.-C., Zhao, L.-J., Liu, X.-G., Guo, Y.-F., Shen, J., Lin, X., Deng, J., Zhou, R., & Deng, H.-W. (2018). The good, the bad, and the ugly of calcium supplementation: A review of calcium intake on human health. Clinical Interventions in Aging, 13, 2443–2452. https://doi.org/10.2147/CIA.S157523
- Madrian, B. C. (2014). Employment-based health insurance and job mobility: Is there evidence of job-lock. The Quarterly Journal of Economics, 109(1), 27–54.
- Mazzolari, F., & Neumark, D. (2012). Immigration and product diversity. Journal of Population Economics, 25(3), 1107–1137. https://doi.org/10.1007/s00148-011-0355-y
- Midrigan, V., & Xu, D. Y. (2014). Finance and misallocation: Evidence from plant-level data. American Economic Review, 104(2), 422–458. https://doi.org/10.1257/aer.104.2.422
- Mukong, A. K., Van Walbeek, C., & Ross, H. (2017). Lifestyle and income-related inequality in health in South Africa. International Journal for Equity in Health, 16(1), 103. https://doi.org/10.1186/s12939-017-0598-7
- Muller, A. (2017). Functional integration of China’s social protection: Recent and long-term trends of institutional change in health and pension insurance. Asian Survey, 57(6), 1110–1134.
- Pentek, M. (2014). Subjective expectations at biological therapy initiation: A survey of rheumatoid arthritis patients and rheumatologists. The European Journal of Health Economics, 15, 83–92.
- Piketty, T. (2014). Capital in the twenty-first century. Harvard University Press.
- Raghupathi, V., & Raghupathi, W. (2020). The influence of education on health: An empirical assessment of OECD countries for the period 1995–2015. Archives of Public Health = Archives Belges de Sante Publique, 78, 20. https://doi.org/10.1186/s13690-020-00402-5
- Rappange, D. R., Brouwer, W. B. F., & van Exel, J. (2016). Rational expectations? An explorative study of subjective survival probabilities and lifestyle across Europe. Health Expectations, 19(1), 121–137. https://doi.org/10.1111/hex.12335
- Ray, D., & Linden, M. (2018). Health, inequality and income: A global study using simultaneous model. Journal of Economic Structures, 7(1), 22. https://doi.org/10.1186/s40008-018-0121-3
- Simonds, S. K. (1974). Health education as social policy. Health Education & Behavior, 2(1_suppl), 1–191. https://doi.org/10.1177/10901981740020S102
- Stait, E., & Calnan, M. (2016). Are differential consumption patterns in health-related behaviours an explanation for persistent and widening social inequalities in health in England? International Journal for Equity in Health, 15(1), 171. https://doi.org/10.1186/s12939-016-0461-2
- Sweet, E. (2011). Symbolic capital, consumption, and health inequality. American Journal of Public Health, 101(2), 260–264. https://doi.org/10.2105/AJPH.2010.193896
- Toçi, E., Burazeri, G., Kamberi, H., Jerliu, N., Sørensen, K., & Brand, H. (2014). Socio-economic correlates of functional health literacy among patients of primary health care in Kosovo. Public Health, 128(9), 842–850. https://doi.org/10.1016/j.puhe.2014.06.009
- Wagstaff, A., Lindelow, M., Jun, G., Ling, X., & Juncheng, Q. (2009). Extending health insurance to the rural population: An impact evaluation of China's New Cooperative Medical Scheme. Journal of Health Economics, 28(1), 1–19. https://doi.org/10.1016/j.jhealeco.2008.10.007
- Wagstaff, A., & Pradhan, M. (2005). Health Insurance Impacts on Health and Nonmedical Consumption in a Developing Country. Policy Research Working Paper No. 3563.
- Weathers, R. R., & Stegman, M. (2012). The effect of expanding access to health insurance on the health and mortality of Social Security Disability Insurance beneficiaries. Journal of Health Economics, 31(6), 863–875. https://doi.org/10.1016/j.jhealeco.2012.08.004
- Weil, D. N. (2009). Economic growth (pp. 1–592). Prentice Hall.
- Xie, Y., Brand, J. E., & Jann, B. (2012). Estimating heterogeneous treatment effects with observational data. Sociological Methodology, 42(1), 314–347. https://doi.org/10.1177/0081175012452652
- Xue, X., Reed, W. R., & Menclova, A. (2020). Social capital and health: A meta-analysis. Journal of Health Economics, 72, 102317. https://doi.org/10.1016/j.jhealeco.2020.102317
- Yamada, I., Asai, A., Shindo, H., Hideaki Takeda, H., & Matsumoto, Y. (2020). LUKE: deep contextualized entity representations with entity-aware self-attention. In Proceedings of the 2020 Conference on Empirical Methods in Natural Language Processing (EMNLP) (pp. 6442–6454). Association for Computational Linguistics.
- Zajacova, A., & Lawrence, E. M. (2018). The relationship between education and health: Reducing disparities through a contextual approach. Annual Review of Public Health, 39(1), 273–289. https://doi.org/10.1146/annurev-publhealth-031816-044628
- Zimmerman, S. D. (2014). The returns to college admission for academically marginal students. Journal of Labor Economics, 32(4), 711–754.