
Abstract
The ways in which the decisions we make for others differ from the ones we make for ourselves has received much attention in the literature, although less is known about their relationship to our predictions of the recipient’s preferences. The latter question is of particular importance given real-world occurrences of surrogate decision-making which require surrogates to consider the recipient’s preferences. We conducted three experiments which explore this relationship in the medical and financial domains. Although there were mean discrepancies between surrogate predictions and choices, we identified a predictive relationship between the two. Moreover, when participants took high risks for themselves, it seems that they were not willing to do so for others, even when they believed that the recipient’s preferences were similar to their own. We discuss these findings relative to current theories and real-world instances of surrogate decision-making.
Introduction
Background
Making a decision is often difficult given that the way it fulfils the decision-maker’s goal can only be known in hindsight. Making the right decisions for other people, which we term surrogate decisions, can be even more difficult due to the fact that they are often made in the absence of knowledge of the recipient’s wishes and values. Uncertainty concerning another’s utilities is thereby added to the uncertainty of the decision-making process itself. Does that degree of uncertainty impact the way people make surrogate decisions or are we capable of predicting a recipient’s wishes and preferences and making decisions accordingly? Do surrogates take into account these factors or do they take a different approach to making such decisions? These questions are essential to understanding how we make surrogate decisions, which is important given that a significant proportion of the decisions we make are for other people. We aim to address the latter question in this paper where we present three experiments which explore the relationship between decision-makers’ predictions of a recipient’s utility and the choices they make for the recipient. We present findings from two domains involving risk in order to assess how that relationship might change according to the content and context of the decision. We investigate the financial domain, where self-other differences are not yet clearly accounted for, and the medical domain, where the relationship between choices and predictions is highly relevant to real world medical decisions.
Although many surrogate decisions are relatively trivial, such as choosing a present, others involve life and death medical decisions. It is important to understand how surrogate decision-makers integrate the recipient’s wishes and preferences into their decision process in these situations with high risks and stakes. When a patient is deemed to have lost their decision-making capacity due to illness or injury, a surrogate (often next-of-kin) is asked to make a decision on their behalf. These surrogates are usually instructed to make a decision that is in the recipient’s best interest whilst also following the substituted judgment standard, that is, making the decision the recipient would have made if they were able to do so. A twofold question therefore arises: can surrogates accurately predict the recipient’s wishes and preferences, and if they can, are they guided by these predictions when formulating their decision? Concerning surrogate accuracy, Shalowitz, Garrett-Mayer, and Wendler (Citation2006) showed in a systematic review that surrogates’ predictions of patients’ treatment preferences in hypothetical scenarios were accurate only 68% of the timeFootnote1. In terms of whether surrogates take into account these preferences, qualitative research suggests that surrogates experience a conflict between wanting to make a decision in accordance with the patient’s values and factors such as preserving the patient’s life or the family’s well-being (Dionne-Odom, Willis, Bakitas, Crandall, & Grace, Citation2015; Schenker et al., Citation2012). These findings suggest that the substituted judgment standard may have unrealistic expectations of surrogates’ decision-making, adding to the debate concerning its suitability (Torke, Alexander, & Lantos, Citation2008).
Theories and models of surrogate decision-making
Tunney and Ziegler's (2015) domain-general model of surrogate decision-making proposes that surrogate decisions are the result of perspective taking that varies according to the features of the decision. These features are expected to affect whether the decision maker is likely to engage in a simulated perspective (predicting what the recipient would do), a benevolent perspective (what the recipient should do), a projected perspective (what the decision-maker would do if they were the recipient), and/or an egocentric perspective (what the decision maker wants to do). In situations where the quality of the decision is largely determined by the recipient’s own preferences (buying a present for example), if the decision maker knows the recipient well, a simulated decision is likely to be taken. However, if the decision maker possesses little information about the recipient, they might rely on a projected perspective. In situations where a high level of responsibility is placed on the decision maker, they might be inclined to take as much risk as they think is reasonable rather than how much risk they think the recipient would take: a benevolent rather than a simulated decision. Medical professionals for example are expected to adopt a more benevolent or egocentric perspective if they fear the professional or legal consequences of making the wrong decision, even if that means going against what the patient would want, whereas a surrogate for a next-of-kin may put more emphasis on a simulated perspective.
Theories specific to surrogate risk-taking do not speak of the relationship between surrogate predictions and decisions but can offer an account of their outcome. The Risk-as-Feelings hypothesis proposes that our subjective risk preferences are the result of emotional reactions to the risk rather than a purely cognitive evaluation of it (Loewenstein, Weber, Hsee, & Welch, Citation2001). In the context of surrogacy, the decision-maker is not the recipient of the outcome of the decision, thereby introducing psychological distance between the decision-maker and the outcome (Trope & Liberman, Citation2010). There is what is termed a self-other empathy gap (Loewenstein, Citation1996) which reduces the emotional involvement of the decision maker in the decision process. The decision-maker’s emotional reactions to the prospect of a risk would therefore be reduced when making a surrogate decision compared to their own. It would follow, therefore, that surrogate decisions are closer to risk neutrality. Although such a hypothesis can help us understand how surrogate decisions differ from people’s own decisions, it does not admit the possibility that surrogate decisions could be in fact based on surrogate predictions which may themselves be closer to risk neutrality. Finally, Social Values Theory (Stone & Allgaier, Citation2008) proposes that self-other differences in decisions involving risk will arise because surrogate decisions are largely based on the social value placed on the risk, thereby acting as a norm. It is plausible that surrogates take into account whether risk-taking is socially valued or not, particularly when being held accountable or when making a decision for a stranger, but again this does not allow for the possibility that surrogates may take an approach that is largely based on a simulated perspective.
Surrogate decisions and predictions involving risk
In the financial domain, the literature on self-other differences is rather contradictory. There are findings suggesting that people are less risk averse for others than for themselves (Batteux et al., Citation2017; Mengarelli, Moretti, Faralla, Vindras, & Sirigu, Citation2014; Pollmann, Potters, & Trautmann, Citation2014; Polman, Citation2012), while others showing that people are more risk-averse for others (Eriksen & Kval⊘y, Citation2010; Fernandez-Duque & Wifall, Citation2007; Zaleska & Kogan, Citation1971), as well as findings reporting no self-other differences (Benjamin & Robbins, Citation2007; Stone, Yates, & Caruthers, Citation2002). These findings concerning surrogate choices have been discussed relative to the Risk-as-Feelings hypothesis (Batteux et al., Citation2017; Fernandez-Duque & Wifall, Citation2007), reduced loss aversion (Mengarelli et al., Citation2014; Polman, Citation2012), increased caution due to responsibility (Zaleska & Kogan, Citation1971), and Social Values Theory (Stone & Allgaier, Citation2008). However, there has been little mention of the interplay between surrogate predictions and surrogate choices.
The question concerning the relationship between surrogate predictions and choices in financial decisions is one that can be posed given the similarities between predictions and choices. It has been found that people’s surrogate predictions are closer to risk neutrality than the decisions they make for themselves, both in the domain of gains where people were risk averse but predicted someone else to be less risk averse as well as in the domain of losses where people were risk seeking and predicted that someone else would be less risk seeking (Faro & Rottenstreich, Citation2006; Hadar & Fischer, Citation2008; Hsee & Weber, Citation1997; Krishnamurthy & Kumar, Citation2002). Research has also shown that people’s surrogate choices are closer to risk neutrality than the decisions they make for themselves in both gain and loss frames (Batteux, Ferguson, & Tunney, Citation2017; Sun, Liu, Zhang, & Lu, Citation2016; Zhang, Liu, Chen, Shang, & Liu, Citation2017; Ziegler & Tunney, Citation2015). Such findings suggest that perhaps in a financial context people make surrogate decisions in accordance with their predictions of what that person would do: they predict that person’s risk preferences and choose accordingly. However, it is difficult to establish whether similarities between predictions and choices can tell us anything about whether surrogates engage in simulated perspective-taking. In fact, Pahlke, Strasser, and Vieider (Citation2015) show that in some instances, people make more risk-averse choices when choosing for themselves and someone else, as opposed to for themselves only, but report that they believe others are more risk-seeking than them. In the following paper, we add to this evidence by presenting an alternative way of investigating the relationship between surrogate choices and predictions which allows us to directly compare them.
When faced with hypothetical treatment scenarios, research indicates that decision-makers accept less risk for someone else than for themselves. This has been shown when doctors make decisions or recommendations for their patients (Garcia-Retamero & Galesic, Citation2012; Ubel, Angott, & Zikmund-Fisher, Citation2011). These differences might arise due to an effect of accountability whereby physicians feel the need to be able to justify their choices to others (Ubel et al., Citation2011) and fear the legal consequences of their decisions (Garcia-Retamero & Galesic, Citation2012), thereby reducing the risk they are prepared to take for a patient relative to themselves. This has also been found when people from the general population make decisions for a hypothetical patient or a family member (Dore, Stone, & Buchanan, Citation2014; Oliver, Citation2013; Petrova, Garcia-Retamero, & Van Der Pligt, Citation2016; Zikmund-Fisher, Sarr, Fagerlin, & Ubel, Citation2006), which has been discussed as the result of employing greater caution when making a decision for someone else (Oliver, Citation2013) and the need to justify one’s decisions (Zikmund-Fisher et al., Citation2006), in which case maximising survival chances is easier to defend.
Concerning predictions, Garcia-Retamero and Galesic (Citation2012) report that general practitioners predict their patients to either be more risk-seeking than themselves or have similar risk preferences but make more risk-averse choices for them than for themselves. They also find a positive correlation between doctors’ own preferences and their predictions of patients’, but none between their predictions of patients’ preferences and the choices they make for them. This suggests on the one hand that there is a discrepancy between doctors’ surrogate predictions and surrogate choices, and on the other that their predictions of a patient’s risk preferences are related to their own preferences, which is a common finding across the medical literature (Fagerlin, Danks, Ditto, & Houts, Citation2001; Raymark, Citation2000). Similar results have been reported in a study where participants made more risk-averse vaccination decisions for a younger sister they were responsible for than for themselves, irrespective of the sister’s preferences (Petrova et al., Citation2016). Our aim in this paper is to further explore the relationship between surrogate predictions and choices of ordinary decision-makers in order to understand how self-other differences arise in the medical domain when making decisions for a stranger, whilst setting aside the professional and legal constraints felt by doctors when making such decisions.
There is also evidence that in relationship scenarios, young adults take more risks for others than themselves but believe that others would take the same level of risk as them (Stone & Allgaier, Citation2008). However, we believe that the scenarios described in each domain are different enough that findings from one domain cannot be assumed to translate to other domains. Indeed, individuals’ risk preferences are not constant across domains (Zou & Scholer, Citation2016), nor do they attend to probabilities in the same way (Pachur, Hertwig, & Wolkewitz, Citation2014) or perceive the ratio between gains and losses to be equivalent (Zou & Scholer, Citation2016). Furthermore, Tunney and Ziegler’s (Citation2015) model of surrogate decision-making predicts that different features of the decision will impact perspective-taking. Different levels of accountability might be held against a medical and a financial decision-maker. The fact that self-other differences have been more consistent in the medical than the financial domain also suggests that there may be important differences between the two which should not be disregarded.
The present research
We present three experiments which explore the relationship between surrogate predictions and choices in both medical and financial domains when ordinary people make decisions on behalf of strangers. The way we investigate this is different from the literature in that we use a within-subjects design. This allows us to assess whether participants’ surrogate predictions are predictive of their surrogate choices, instead of comparing choices and predictions in a between-subjects design. In doing so, we can infer whether surrogates might compute a simulated perspective when making their decisions, rather than inferring that they do not in light of discrepancies between choices and predictions. We can then compare decisions across domains in order to draw conclusions regarding whether surrogates are more likely to take a simulated approach in a particular domain.
We have two research questions which require different analyses. The first is whether surrogate predictions are predictive of surrogate choices. To answer it, we will conduct partial correlations between surrogate predictions and choices, controlling for choices for the self. We will also conduct multiple linear regressions with surrogate choices as an outcome variable and surrogate predictions and choices for the self as predictor variables. The second question is whether any self-other differences in choices can be accounted for by a perceived difference in participants’ own choices and the recipient’s choices. To answer it, we will conduct linear regressions with the self-other difference in choices as an outcome variable and the self-other difference in predictions as a predictor variable.
Experiment 1
In Experiment 1, we examine surrogate risk-taking in the financial domain. A number of potential explanations as to why self-other differences in decisions involving risk may arise in financial decisions have been proposed. The Risk-as-Feelings hypothesis suggests that the decisions we make for others will be closer to risk neutrality than our own. However, if surrogate decisions are based on surrogate predictions, we would again expect these to be closer to risk neutrality than our own decisions given the evidence mentioned above. Given that both suggested explanations would lead to similar outcomes, we need to investigate them in a way that can assess their relative contribution. We assessed self-other differences by asking participants to make a series of choices between two gambles, one with a high probability of winning a small amount and the other with a low probability of winning a large amount. Participants also completed a task where they were are asked to give a rating to each bet. The key manipulation is that participants are asked to predict the recipient’s utility of each bet in order to identify whether surrogates’ choices are coherent with their perception of the recipient’s utility of the bets. In other words, do participants predict someone else’s ratings of the bets to differ from their own? Moreover, is there a relationship between participants’ predictions of someone else’s ratings and the choices they make for them?
Method
Design
A 2 (Recipient) x 2 (Task) within-subjects design was used where participants complete a choice task and a rating task for themselves and for another participant.
Participants
Participants (n = 36) were recruited from the University of Nottingham. The age group ranged from 18 to 34 (M = 21.97, SD = 3.57). There were 12 males and 24 females. Ethics approval was obtained from the ethics committee at the University of Nottingham.
Stimuli
The stimuli were 27 pairs of bets, each made up of a P-bet and a £-bet. P-bets consisted of a high probability of winning a modest amount of money and a low probability of losing a modest amount of money. £-bets consisted of a low probability of winning a large amount of money and a high probability of losing a modest amount of money. The stimuli were those used by Tunney (Citation2006), with the only difference being that all amounts were multiplied by a factor of 10. Each pair had a very similar expected value, the highest difference being £3.75. Expected values varied between £11.70 and £43. The amounts that could be won varied between £15 and £500. The amounts that could be lost varied between £1.50 and £80. The amount to win in £-bets was always larger than in P-bets. In all bets, the amount that could be won was always higher or equal to the amount that could be lost.
Procedure
The experiment consisted of two sessions which were completed by participants 3-7 days apart. Participants made decisions for themselves in one session and for another participant in the other. The order in which participants completed the sessions was counterbalanced across participants. Each session was composed of two stages which were both completed on a computer using PsychoPy (Peirce, Citation2007). The first stage was the choice phase where participants made choices between the paired P-bets and £-bets. The second stage was the rating phaseFootnote2. When making decisions for themselves, participants were asked to imagine that the bets were in the form of a lottery ticket and indicate the minimum selling price they would be prepared to sell the bet for, such that they would be indifferent to whether they played the bet or received the selling price instead. When making decisions for someone else, participants were asked to predict the minimum price they think that person would be prepared to sell the bet for. Bets were rated individually and presented in random order. The 6 bets which served as practice trials in the choice phase were also used as practice trials in the rating phase. To reiterate, participants were asked to make choices for another participant in the choice phase but predict what the recipient would do in the rating phase.
Participant compensation
Participants were told that the amount of money they would get as compensation would vary according to decisions made in the choice phase. For every participant, one of the bets they chose for themselves and one of the bets the previous participant had chosen for them was played for real money. A small proportion of the amounts that were won (or lost) were added (or subtracted) to (or from) their initial inconvenience allowance of £4. The proportion of the amounts was adjusted so that participants would obtain on average £5. The bets that were played for real money were selected at random and participants were not told which ones they were.
Results
There were no differences between the proportion of P-bet choices for self (M = 0.76, SD = 0.24, CI [0.68, 0.84]) and for other (M = 0.76, SD = 0.24, CI [0.70, 0.82]) (t35=0.093, p=.926). To assess whether participants predicted the other participant’s ratings to be different to their own, we computed the mean rating for each type of bet in each condition (see ). Participants’ own ratings and their predictions of another person’s ratings were entered into a 2 (Recipient) x 2 (Type of Bet) repeated-measures ANOVA. There was no main effect of recipient (F1,35=1.243, MSe=108.047, p=.273). There was a main effect of type of bet (F1,35=8.153, MSe=845.808, p=.007, ηp2=0.189): participants rated the £-bet higher than the P-bet. There was no interaction between recipient and type of bet (F1,35=1.017, MSe=66.617, p=.320).
Figure 1. Means of participants’ own ratings and their predictions of another’s person’s ratings of the £-bet and the-P bet (Experiment 1). Error bars represent the standard error of the mean.
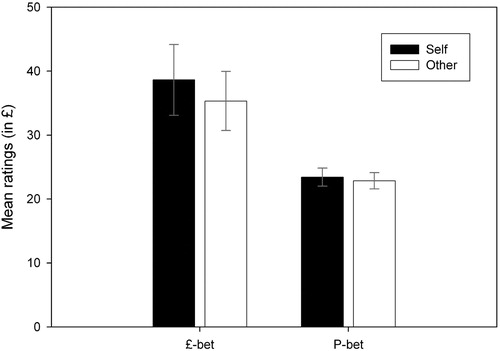
We identified whether there was a relation between participants’ predictions of other people’s ratings of the bets and the choices they made for them using Pearson’s correlations. We used the difference between ratings of the £-bet and ratings of the P-bet as a measure of ratings of the bets by subtracting P-bet ratings from £-bet ratings. There was no association between the proportion of P-bet choices for other and ratings of the bets (r = 0.077 [-0.266, 0.360]Footnote3, p=.657). We compared this to the relation between participants’ own ratings and choices, where there was a negative correlation between the proportion of P-bet choices for self and ratings of the bets (r=-0.660 [-0.867, -0.251], p<.001). This means that the higher participants rated the £-bets relative to the P-bets, the more likely they were to choose them for themselves.
We then assessed whether surrogate predictions of ratings had a relationship with choices independently of participants’ own ratings and choices. We performed a partial correlation between P-bet choices for other and ratings for other, controlling for P-bet choices and ratings for self, which was not significant (r = 0.232, p=.187). We also conducted a multiple linear regression, with surrogate P-bet choices as the outcome variable and ratings for other, ratings for self and P-bet choices for self as predictor variables. We found that the model was significant (F2,32=4.477, p=.010) and accounted for 29.6% of the variance in surrogate choices. Surrogate predictions did not predict surrogate choices (B = 0.003, SE = 0.002, p=.187), nor did participants’ own ratings (B < 0.001, SE = 0.002, p=.885). However, participants’ own choices did (B = 0.442, SE = 0.150, p=.006). Participants’ likelihood of choosing the P-bet for another person increases as their likelihood of choosing the P-bet for themselves increases.
Discussion
There were no self-other differences in choices and no differences between people’s own ratings and their predicted surrogate ratings, suggesting that they predicted another person’s utility of the bets to be similar to their own. The absence of self-other differences could be due to the fact that participants do not perceive the recipient’s utility of the bets to be different to their own. We did not find a relationship between participants’ surrogate ratings and choices. When participants predicted that another person would rate the £-bet highly, they did not show a preference for the £-bet when choosing on their behalf. This suggests that, in financial decisions, surrogates either do not compute the other person’s utilities when making a decision on their behalf, or may not heavily rely on them, if at all. On the other hand, it could be that the two different modes of preference elicitation lead to decisions that are not related, rather than surrogate predictions and choices not being related. This is coherent with literature on preference reversals, which shows that, like we found here, people favour the P-bet in the choice task but the £-bet in the rating task (Lichtenstein & Slovic, Citation1971). However, there was a relationship between participants’ own ratings and choices. Rating the £-bet highly increased the likelihood of choosing it over the P-bet when making a decision for oneself, which means that the two modes of preference elicitation were related when participants decided for themselves. Therefore, our finding that they were not for others is indicative of the relationship between surrogate predictions and decisions.
Experiment 2
In Experiment 2, we examine the relationship between surrogate choices and predictions in medical scenarios. Participants were recruited from the general population in order to assess whether self-other differences observed in doctors for their patients also arise when ordinary people make decisions for others. We included both scenarios which depicted moderate and severe conditions. The decisions we presented in Experiment 1 had outcomes which were relatively small, and much smaller than scenarios in the medical literature. The health literature cited above includes scenarios of varying significance, from resulting in mild symptoms to death, but has not yet looked at whether less significant scenarios alters self-other differences. In the interpersonal domain, self-other differences have been found for low-impact but not high-impact scenarios (Beisswanger, Stone, Hupp, & Allgaier, Citation2003; Stone & Allgaier, Citation2008), suggesting that outcome significance might affect self-other differences in the medical domain.
We investigate self-other differences using the QALY (quality-adjusted life years) standard gamble (SG) task commonly used to measure the utility of health outcomes (Whitehead & Ali, Citation2010). The SG task is designed to measure utility under risk for a particular medical condition by presenting a choice between a safe option (staying in that condition) and a risky option (taking a risky treatment). We investigate predictions by adding a measure of utility without a risk component using the time trade-off (TTO) QALY task which elicits an expression of the participant’s value of a particular medical condition. Surrogates are asked to predict the recipient’s utilities in the TTO task and make choices for the recipient in the SG task. This allows for a comparison between surrogates’ decisions under risk and their predictions of the recipient’s value of the medical condition in order to evaluate whether surrogate choices can be accounted for by the surrogate’s perception of the recipient’s value of the condition.
The reason we use the TTO task, rather than eliciting surrogate predictions in the SG gamble task, is to avoid interpretation difficulties if we find that surrogate choices and predictions are congruent, as in the financial literature, which could mean that surrogates are making a simulated decision, but it could also be the result of an attenuation of the participant’s own risk preference in both cases or the participant’s motivation for consistency. Using the TTO task does not eliminate all alternative explanations, but it does place the participant in a slightly different context when predicting the recipient’s utilities, which can tell us something informative about surrogate predictions, independently from the surrogate choices made in the SG task. Given the literature, we do not anticipate self-other differences in surrogate predictions, but we do expect differences in surrogate choices, and therefore hypothesise that surrogate predictions cannot account for surrogate choices.
Method
Design. A 2 (Recipient) x 2 (Magnitude) x 2 (Task) repeated-measures design was used. The first factor ‘Recipient’ was a within-subjects factor where participants made decisions for themselves (self) and for another participant (other). The second factor ‘Magnitude’ was a within-subjects factor relating to the severity of the health state. The third factor ‘Task’ was a within-subjects factor, which refers to whether utilities were elicited via the SG or the TTO task.
Participants. Participants (n = 36) were recruited from the University of Nottingham. The age group ranged from 20 to 47 (M = 25.40, SD = 5.66). There were 10 males and 26 females. Ethics approval was obtained from the ethics committee at the University of Nottingham.
Materials and Procedure. Participants completed the experiment on a computer using PsychoPy (Peirce, 2007). They completed two different tasks which were designed to measure their utilities of each illness. Utilities were taken as measures of value or preference for health states and were bounded by 0 (prefer to die rather than live with condition) and 1 (indifferent between condition and full health). In both tasks, participants were presented with six scenarios (three moderate and three severe conditions, see Appendix). Two of the severe conditions (paraplegia and Broca’s aphasia) were adapted from Rosen, Tsai, and Downs (Citation2003) because they elicited low utilities, to which we added a vegetative state scenario. Angina was used as a moderate condition because it elicited high utilities in Read, Quinn, Berwick, Fineberg, and Weinstein (Citation1984), to which we added a headache and a nausea scenario. In all scenarios, it is specified that without treatment there is no chance of recovery. Participants completed each task twice: once for themselves and once for another unknown participant who they were told was also a student. The SG task measures how much risk participants are willing to take to recover, whereas the TTO task measures how many years of their life participants are willing to sacrifice to recover. The SG task measures risk preferences whereas the TTO task does not.
In the SG task, participants were given the choice between a safe option: remaining in a condition (paraplegia, Broca’s aphasia, vegetative state, angina, headache, nausea) and a risky option: a treatment with a probability p of complete recovery and a probability 1-p of death. The probability p in the risky option was presented in descending order (100%, 95%, 90%, 80%, 70%, 60%, 50%, 40%, 30%, 20%, 10%, 5%, 0%) until respondents switched from choosing the risky option to the safe option. They made these choices once for themselves and once on behalf of another participants. In the TTO task, participants were asked to indicate how many years in full health were for them equivalent to 50 years with the disease. In other words, how many years of their life would they trade-off or sacrifice to live in full health. The years they would rather live in perfect health divided by 50 years was taken as the measure of utility. Crucially, when completing the task for another participant, they were asked to predict what the participant would do: in other words, how many years in full health would be equivalent for that participant to 50 years with the disease.
Half the participants completed both tasks for themselves first whereas half the participants completed both tasks for another participant first. Half the participants completed the SG task first in each block of recipient and half the participants completed the TTO task first in each block of recipient. In the SG task participants were asked to make choices on behalf of the participant, whereas in the TTO task participants were asked to predict what they think the participant would do.
Results
For responses in the SG task, we computed participants’ utilities of the medical scenarios for each recipient by taking their indifference point between taking the risky option and the safe option. The indifference point is the average of the two probabilities either side of the crossover point from the risky to the safe option. Utilities varied between 0 and 1 where 0 indicates that they always chose the risky option and 1 indicates that they always chose the sure option. We then averaged utilities for moderate and severe conditions to have an overall utility for each magnitude. We converted responses on the TTO task to a utility that varied between 0 and 1, where 0 indicates that they would rather die than live at all with the condition and 1 indicates that they are not willing to sacrifice any life years to live in full health.
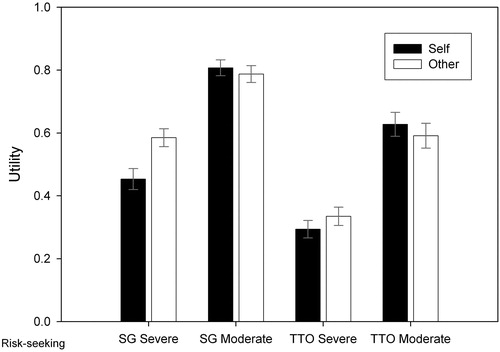
We entered these utilities in a 2 (Recipient) x 2 (Magnitude) x 2 (Task) repeated measures ANOVA (see ). There was a main effect of task (F1,35=37.818, MSE = 0.075, p<.001, ηp2=0.519), a main effect of magnitude (F1,35=98.241, MSE = 0.062, p<.001, ηp2=0.737). The main effect of recipient was not significant (F1,35=2.986, MSE = 0.022, p=.093, ηp2=0.079). Of primary interest, there was an interaction between recipient and task (F1,35=6.044, MSE = 0.016, p=.019, ηp2=0.147). According to a simple effects analysis, participants’ utilities were higher for someone else than for themselves in the SG task (mean difference=-0.06, p=.025), but there were no differences on the TTO task (mean difference=-0.004, p=.804). There was also an interaction between recipient and magnitude (F1,35=38.179, MSE = 0.007, p<.001, ηp2=0.522). According to a simple effects analysis, participants’ utilities were higher for someone else than for themselves for severe conditions (mean difference=-0.09, p=.001), but slightly lower for someone else for moderate conditions (mean difference = 0.03, p=.050). The interaction between recipient, task and magnitude was not significant (F1,35=3.499, MSE = 0.005, p=.070, ηp2=0.091).
Figure 2. Average utility for each recipient, magnitude and utility estimation task with error bars representing the standard error of the mean (Experiment 2). Higher utilities indicate less risk-taking in the SG task and less life years sacrificed in the TTO task.
To explore whether surrogate choices and predictions were related, we conducted Pearson’s correlations between utilities in the SG and the TTO task. Surrogate choices in the SG task were positively correlated to surrogate predictions in the TTO task for severe conditions (r = 0.503 [0.272, 0.688], p=.002) but not for moderate conditions (r = 0.061 [-0.253, 0.388], p=.725). Similarly, for themselves, participants’ utilities in both tasks were positively correlated for severe conditions (r = 0.534 [0.215, 0.763], p=.001) but not for moderate conditions (r=-0.127 [-0.431, 0.289], p=.461).
We then assessed whether surrogate predictions in the TTO task predicted surrogate choices in the SG task independently of participants’ own choices in the SG task and ratings in the TTO task. Partial correlations between surrogate predictions and choices, controlling for self ratings and choices, were significant for severe conditions (r = 0.606, p<.001) but not moderate conditions (r = 0.192, p=.269). We also conducted a multiple linear regression with surrogate choices as the outcome variable and ratings for other, ratings for self and choices for self as predictor variables. For severe conditions, the model was significant (F2,32=13.555, p<.001) and accounted for 56.0% of the variance in surrogate choices. Surrogate predictions positively predicted surrogate choices (B = 0.668, SE = 0.155, p<.001) and so did participants’ own choices (B = 0.551, SE = 0.119, p<.001). On the other hand, participants’ own ratings negatively predicted surrogate choices (B=-0.563, SE = 0.183, p=.004). For moderate conditions, the model was significant (F2,32=8.677, p<.001) and accounted for 44.9% of the variance in surrogate choices. Surrogate predictions did not predict surrogate choices (B = 0.021, SE = 0.178, p=.908), nor did participants’ own ratings (B = 0.094, SE = 0.184, p=.611), but their own choices did (B = 0.714, SE = 0.141, p<.001).
The fact that we used a within-subjects design suggests there might be contamination between the SG task and the TTO task. Participants who completed the TTO task first were asked to take the recipient’s perspective before making a choice on their behalf. To evaluate whether the order in which participants completed both tasks affected the relationship between predictions and choices, we added the order in which participants completed the tasks as a predictor into the regression model with severe conditions. The model remained significant (F4,31=9.858, p<.001) and accounted for 56.0% of the variance, but order was not a significant predictor (B=-0.006, SE = 0.045, p=.898). However, surrogate predictions (B = 0.666, SE = 0.158, p<.001), participants’ own choices (B = 0.544, SE = 0.132, p<.001) and participants’ own ratings (B=-0.562, SE = 0.186, p=.005) predicted surrogate choices. We also checked whether order was a predictor of the difference between surrogate predictions and choices for severe conditions. The model was not significant (F1,34=0.347, p=.559).
Finally, we assessed whether participants’ perceived difference between their own and the recipient’s values in the TTO task could account for the self-other differences we found in the SG task. We conducted a linear regression with the difference between self and other on the SG task as the outcome variable and the difference between self and other on the TTO task as the predictor variable. Given that the relationship between predictions and choices differed by outcome magnitude, we ran two separate analyses. For severe conditions, we found that the model was significant (F1,34=21.985, p<.001) and accounted for 39.3% of the variance in self-other differences in choices. The self-other difference in ratings was a significant predictor of the self-other difference in choices (B = 0.798, SE = 0.170, p<.001). For moderate conditions, the model was not significant (F1,34=0.011, p=.916).
Discussion
In terms of surrogate decisions, they were more risk-averse than people’s own decisions for severe medical conditions, which supports the hypothesis that medical scenarios elicit a more cautious approach to surrogate decision-making. However, they were slightly more risk-seeking than participants’ own decisions for moderate conditions. This could be due to the fact that people were more risk-seeking for severe than moderate conditions and were not prepared to take that level of risk on behalf of the recipient. In terms of surrogate predictions, participants perceived the recipient’s utilities of the medical conditions to be slightly lower than their own, indicating that there is a discrepancy between surrogate predictions and choices. For both severe and moderate conditions, we found that participants’ own choices predicted their surrogate choices. Crucially, for severe conditions, surrogate predictions predicted surrogate choices independently of participants’ own utilities. This suggests that predictions inform choices, even if they cannot fully account for the variance in choices. In other words, surrogates take into account their predictions of the recipient’s utilities, but there are other factors driving the reduction in risk-taking. Other possibilities remain, however, such as it is in fact choices that inform predictions, or that they are both influenced by a common underlying mechanism. For moderate conditions, we did not find a relationship between predictions and choices for either self or other. It is therefore unclear whether surrogate predictions are not related to decisions for moderate conditions, or whether the SG and TTO tasks are more strongly related for severe than moderate conditions.
Experiment 3
Experiment 1 and 2 show that the relationship between surrogate choices and predictions differs between domains. In financial decisions, although we did not find self-other differences in either choices or ratings, surrogate ratings did not predict surrogate choices. In medical decisions, although we found conflicting self-other differences in choices and ratings, surrogate ratings did predict surrogate choices in the case of severe illnesses. This suggests that participants are integrating a simulated approach when making medical decisions but not financial decisions. We therefore conducted a third experiment with a larger sample size to directly compare the relationship between surrogate choices and predictions in both domains.
Although the specific choice trials were taken from Experiments 1 and 2, we had to make a number of amendments to their designs in order to conduct a feasible experiment. Firstly, we needed to ensure that we used a unique dependent variable that we could then enter in an analysis of variance. It was therefore difficult to use the ratings task from Experiment 1. Instead, we compared surrogate choices with surrogate predictions on the same task, meaning that participants completed the same task three times (self, other, predictions) in each domain, with preference for the safer option as the dependent variable. This also eliminates the interpretation difficulties that arise from using two different tasks to compare choices and predictions. Secondly, we wanted to make sure that the experiment was not too long in order to sustain participants’ attention throughout and preserve the quality of the data. To this end, we selected particular trials from Experiment 1 (16 of the 24 choice trials) and Experiment 2 (severe conditions). The fact that participants completed three tasks per domain rather than four also contributed to shortening the experiment.
Method
Design
A 3 (Recipient) x 2 (Domain) within-subjects design was used where participants made choices for themselves, for another participant, and predicted what another participant would do. They made choices in the financial and medical domains.
Participants
Participants (n = 80) were recruited via Prolific. The age group ranged from 18 to 35 (M = 27.51, SD = 5.11). There were 23 males and 57 females with varying levels of education. All participants resided in the United Kingdom to ensure that the currency used (£) in the task was relevant to all. Ethical approval was obtained from the ethics committee at the University of Nottingham.
Choice task
The financial choices consisted of 16 pairs of bets, each made up of a P-bet and a £-bet, taken from Experiment 1. We chose the bets that had the largest difference between the probabilities of the P-bet and of the £-bet, in order to further validate the P-bet as the safest option. The only difference was that all amounts were multiplied by a factor 10 in order to make the scenarios more significant to participants. The medical choices were identical to the SG task with severe conditions (paraplegia, Broca’s aphasia, vegetative state) in Experiment 2.
Procedure
Participants completed each choice task three times: once for themselves, once for another participant, and once where they had to predict what the other participant would do. They were told to imagine that the other participant was of a similar age and situation to them. The order in which they completed each task (self-financial, other-financial, predict-financial, self-medical, other-medical, predict-medical) was randomised. The order in which they completed the trials within each task was randomised.
Results
Data pre-processing
In the financial domain, we took the proportion of P-bet choices as a measure of risk-taking. In the medical domain, we computed participants’ utilities of the medical scenarios for each recipient by taking their indifference point between taking the risky option and the safe option. The indifference point is the average of the two probabilities either side of the crossover point from the risky to the safe option. Utilities varied between 0 and 1 where 0 indicates that they always chose the risky option and 1 indicates that they always chose the sure option. We then averaged utilities across medical conditions to have an overall utility. 5 participants were excluded from the analysis as an indifference point could not be computed from the choices they made because they were inconsistent (for example, choosing a treatment which has a 50% chance of working but not one which has a 70% chance of working). 75 participants remained in the analysis.
Analysis of variance
We conducted our analysis with a 3 (recipient) x 2 (domain) repeated-measures ANOVA (see ). We did not expect to find an effect of recipient in the financial domain, given that we did not find self-other differences in Experiment 1. However, we did expect to find an effect of recipient in the medical domain whereby choices for the self and predictions of the recipient’s choices are more risk-taking than surrogate choices. We therefore predicted a 2-way interaction between recipient and domain and use simple effects analyses to further analyse our results.
Figure 3. Participants’ choices for each recipient by domain with error bars representing the standard error of the mean (Experiment 3). In the financial domain, higher values indicate a higher preference for the P-bet. In the medical domain, higher values indicate a higher preference for staying in the medical condition as opposed to taking the treatment.
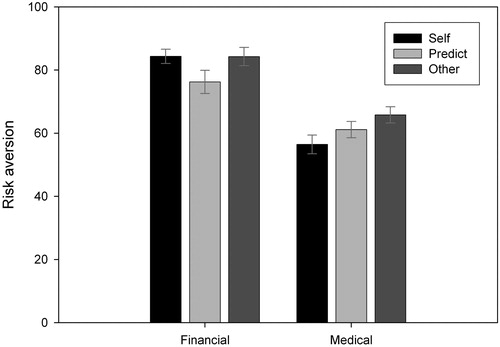
We found a main effect of recipient (F2,148=5.100, MSe=315.434, p=.007, ηp2=0.064). Surrogate choices were more risk-averse than participants’ own choices (mean difference = 4.628, p=.014) and surrogate predictions (mean difference = 6.328, p=.005), but there were no differences between participants’ own choices and surrogate predictions (mean difference = 1.699, p=.417). We found a main effect of domain (F1,74=47.921, MSe=983.228, p<.001, ηp2=0.393) whereby choices in the financial domain were more risk-averse than in the medical domain (mean difference = 20.465, p<.001). Crucially, we found an interaction between recipient and domain (F2,148=5.390, MSe=304.990, p=.006, ηp2=0.068). In the financial domain, participants predicted that the recipient would be more risk-seeking than them (mean difference = 8.083, p=.022, d = 0.31), yet were not significantly more risk-taking for the recipient than for themselves (mean difference = 0.083, p=.981, d = 0.004). Consequently, their surrogate choices and predictions were significantly different (mean difference = 8.000, p=.044, d = 0.28). In the medical domain, participants predicted that the recipient would be more risk-averse than them (mean difference = 4.684, p=.023, d = 0.19) and made more risk-averse choices for the recipient than for themselves (mean difference = 9.340, p<.001, d = 0.38). Surrogate choices were also more risk-averse than surrogate predictions (mean difference = 4.656, p=.016, d = 0.21).
We did not find self-other differences in the financial domain, but we did find that participants expect others to be more risk-taking than them. However, they seem to make similar decisions for them than they would for themselves. In the medical domain on the other hand, participants expect others to be more risk-averse than them and make more risk-averse decisions for them. Nevertheless, their surrogate decisions are more risk-averse than what they would predict the recipient’s to be. We can conclude that there are discrepancies between surrogate choices and predictions, but that surrogate choices are more in line with surrogate predictions in the medical domain than they are in the financial domain.
Regression analyses
We performed Pearson’s correlations to explore the relationship between surrogate choices and predictions. Surrogate choices and predictions were positively correlated in the financial (r = 0.316 [0.062, 0.562], p=.006) and the medical domain (r = 0.732 [0.586, 0.839], p<.001), although that relationship was much stronger in the medical domain. Partial correlations between surrogate choices and predictions, controlling for participants’ own choices, were significant in the financial domain (r = 0.292, p=.012) and in the medical domain (r = 0.333, p=.004).
We then performed regression analyses to assess whether surrogate predictions were predictive of surrogate choices, independently of participants’ own choices. In the financial domain, we found that the model was significant (F2,72=4.002, p=.022) and accounted for 10% of the variance in surrogate choices. Surrogate predictions significantly predicted surrogate choices (B = 0.249, SE = 0.096, p=.012), but participants’ own choices did not (B=-0.001, SE = 0.158, p=.996). In the medical domain, we found that the model was significant (F2,72=80.337, p<.001) and accounted for 69.1% of the variance in surrogate choices. Surrogate predictions significantly predicted surrogate choices (B = 0.292, SE = 0.098, p=.004), but so did participants’ own choices (B = 0.513, SE = 0.085, p<.001). The model accounted for more variance in surrogate choices in the medical domain than it did in the financial domain.
We assessed whether participants’ perceived difference between their own and the recipient’s ratings could account for self-other differences in choices for each domain using a linear regression. In the financial domain, the model was significant (F1,73=10.605, p=.002) and accounted for 12.7% of the variance in surrogate choices. Differences between surrogate choices and predictions were predictive of self-other differences in choices (B = 0.355, SE = 0.109, p=.002). In the medical domain, the model was significant (F1,73=24.958, p<.001) and accounted for 25.5% of the variance in surrogate choices. Differences between surrogate choices and predictions were predictive of self-other differences in choices (B = 0.440, SE = 0.088, p<.001). Again, the model accounted for more variance in surrogate choices in the medical domain than it did in the financial domain.
Finally, we checked whether the order in which participants completed surrogate predictions and decisions was a predictor of the difference between the two. For each domain, we ran a 2 (Condition) x 2 (Order) ANOVA where condition had two levels (surrogate predictions and surrogate choices) and order had two levels (predictions first and predictions second). In the financial domain, there was a main effect of condition whereby choices were more risk-averse than predictions (F1,73=4.342, MSe=536.037, p=.041, ηp2=0.056). We also found an interaction between condition and order (F1,73=4.342, MSe=536.037, p=.019, ηp2=0.073). A simple effects analysis indicated that there were no differences between predictions and choices when predictions were completed first (mean difference=-1.182, p=.827), but there were when they were completed second (mean difference = 16.941, p=.001). Predictions were more risk-seeking than choices only when they were completed after choices by participants. On the other hand, the predictive relationship between predictions and choices appeared in both groups as shown by regression analyses. The model was significant for those that completed predictions first (F1,36=6.454, p=.016) and those that completed predictions second (F1,36=6.123, p=.017). In the medical domain, there was a main effect of condition whereby choices were more risk-averse than predictions (F1,73=4.342, MSe=135.084, p=.016, ηp2=0.077), but there was no interaction between condition and order (F1,73=0.951, MSe=135.084, p=.333, ηp2=0.013).
General discussion
Summary of findings
Across all three experiments, we generally found discrepancies between surrogate choices and predictions. Either self-other differences in choices and predictions did not manifest themselves in the same way (i.e. same direction or magnitude), or we found a self-other difference in one but not the other. These discrepancies in mean values across participants are in line with findings from previous studies (Garcia-Retamero & Galesic, Citation2012; Stone & Allgaier, Citation2008; Stone, Choi, de Bruin, & Mandel, Citation2013). On the other hand, we were able to examine whether surrogate predictions are related to choices, which paints a different picture of their predictive relationship. Indeed, even in cases which presented these mean discrepancies, we found that surrogate predictions were predictive of surrogate choices. Interestingly, the only case in which we did not find such a relationship was in Experiment 1 where self-other differences in choices and predictions were similar.
This shows that concluding that surrogate choices are not informed by surrogate predictions from a mean difference might be misleading. The crucial difference here was that we used a within-subjects designFootnote4 which allowed us to directly compare participants’ predictions and choices. Without these analyses, we would not have been able to see the relationship between the two, and instead would have concluded that predictions and choices were at odds with one another. It is possible that this design encouraged participants to consider predictions in their choices, although we did not find order effects in Experiment 2. However, it is in fact more relevant to real-world occurrences of surrogate decision-making where surrogates are instructed to make a simulated decision and therefore do consider them.
Comparing surrogate decisions across domains
In the financial domain, we did not find any self-other differences. Although surrogates did not believe others would value each option offered by the choice differently (Experiment 1), they perceived others’ choices to be more risk-seeking than their own (Experiment 3). Given that participants were risk-averse for both themselves and the recipient, our findings are consistent with previous studies that show that surrogates believe others make more risk-neutral choices than them (Faro & Rottenstreich, Citation2006; Hadar & Fischer, Citation2008; Hsee & Weber, Citation1997; Krishnamurthy & Kumar, Citation2002). Furthermore, we failed to find a relationship between surrogate choices and predictions in Experiment 1, but we did in Experiment 3. The difference between the two experiments was that predictions were elicited using different tasks. This suggests that surrogates are integrating their perception of the recipient’s risk preference in their decision-making (Experiment 3), but not their perception of the recipient’s utility for each option of the choice separately (Experiment 1). Moreover, although there was no overall self-other difference in choices, we did find that the difference between participants’ own choices and their predictions of someone else’s was predictive of the self-other difference. Interestingly, we only found discrepancies between choices and predictions when participants completed predictions after choices in Experiment 3. This suggests that participants might have conformed their choices to their predictions when made after, but not the other way around. Nevertheless, this did not affect the relationship between surrogate predictions and choices.
In the medical domain, we found that the severity of the condition had an impact on self-other differences. Contrary to the interpersonal domain (Beisswanger et al., Citation2003; Stone & Allgaier, Citation2008), self-other differences were more pronounced for severe than moderate conditions, again suggesting that surrogate decisions are not directly comparable across domains. Our finding that decision-makers take fewer risks for someone else than for themselves when making decisions about severe conditions are consistent with the literature. We have also shown that ordinary decision-makers are more risk-averse for strangers. It could therefore be the case that surrogates tend to take fewer risks for others in the medical domain regardless of their role, but that doctors have additional responsibility and professional obligations which warrant a further reduction in risk-takingFootnote5. This shows that surrogates are more risk-averse for others regardless of whether they are a stranger or a close other (Zikmund-Fisher et al., Citation2006).
We found a clear relationship between surrogate predictions and choices for severe illnesses. Nevertheless, we still found differences between surrogate choices and predictions, which shows that surrogate choices are not completely accounted for. As with financial decisions, we find that participants’ own choices have a strong relationship with their surrogate choices. However, there is still variability in surrogate choices that is unaccounted for. Given that surrogate choices were more risk-averse than surrogate predictions and people’s own choices, we suggest that participants did not want to be accountable for taking a risk that would harm the recipient and therefore preferred to take a safer option; an account that has been explored with medical professionals (Garcia-Retamero & Galesic, Citation2012). Similarly, Petrova et al. (Citation2016) found that participants made risk-averse choices for a hypothetical sibling irrespective of whether the sibling would have done so too, thereby suggesting that the predictive relationship between surrogate choices and predictions might have been weaker if there had been wider discrepancies between the two.
The relationship between surrogate choices and predictions was more consistent in medical decisions than in financial ones. However, the choices made in the financial domain were far less significant and life-changing, indicating that perhaps surrogates are more likely to incorporate a simulated approach when the significance of the decision is high. Indeed, surrogate predictions did not predict surrogate choices in financial decisions with small amounts (Experiment 1), but they did predict financial decisions with higher amounts or decisions for severe illnesses (Experiment 3). The interaction between the significance of the decision and the likelihood of making a simulated decision is therefore worth investigating.
Finally, across both domains, it does seem to be the case that surrogates are not willing to accept large risks on behalf of someone else, even when they would do so themselves and expect the recipient’s utilities to be similar to their own. This is consistent with accounts of self-other differences based on caution when making decisions on behalf of someone else, due to the responsibility placed on the decision-maker and the uncertainty contained in making a decision in the absence of knowledge of the recipient’s preferences. Nevertheless, we did not find that surrogates reduced their risk-taking for others when making financial decisions or decisions concerning moderate illnesses. This could mean that important decisions elicit a precautionary approach, but that less significant ones might not evoke a feeling of responsibility on the part of the decision-maker, who might put less thought into the decision process and therefore be more inclined to making a similar decision to their own. On the other hand, individuals may not be willing to take a high level of risk for someone else to avoid making a decision that risks causing harm to the recipient, either to avoid bearing that responsibility or due to moral and social values steering them in that direction. These accounts would benefit from being investigating in future research to better understand the domain differences we report here.
Theoretical implications
The present findings are best understood within the framework of Tunney and Ziegler’s (Citation2015) model of surrogate decision-making. The accountability held against the decision-maker and the significance of the decision are both factors that are taken into account by the model and expected to alter surrogates’ perspective-taking. In terms of perspective-taking, we found evidence suggesting that, when making decisions for a stranger, participants relied on a projected perspective. This follows from the model’s prediction that surrogates would default to reproducing their own choices in the absence of knowledge about the recipient’s preferences. Nevertheless, participants also seemed to take a simulated approach for financial and medical decisions of higher significance. Notably, the projected and simulated perspectives combined accounted for a much higher proportion of the variance in medical choices (69%) than in financial ones (10%), thereby indicating that the latter would benefit from further investigation. Alternatively, it is possible that the relationships we identified between surrogate choices and predictions or participants’ own choices are the result of a common underlying mechanism, rather than reflecting participants’ perspective-taking. Although our findings are consistent with the latter, more work is needed to ascertain that this is the case.
When participants accept more risk for themselves but lower risk for others, this could be interpreted as them taking a more benevolent approach – whereby they do not judge taking such a level of risk to be in the best interest of the recipient, or a more egocentric approach – where they do not want to be responsible for taking that risk. It is conceivable that the higher the significance of the decision and accountability of the decision-maker, the more likely it is that decision-makers take a cautious approach, thereby focusing on a more benevolent or egocentric perspective. The model also predicts that individuals who are higher in empathy will attribute more weight to a simulated perspective, which is supported by findings by Petrova et al. (Citation2016). Moreover, when surrogates are familiar with the recipient’s preferences, they are expected to be more likely to take a simulated decision. Future work should aim to address how individual differences and the identity of the recipient might affect the relationship between predictions and choices.
The Social Values Theory of surrogate risk-taking (Stone & Allgaier, Citation2008) emphasises the influence that social values can have on the decision process. It would make sense for high risk-taking to not be socially valued in a medical context, particularly amongst health professionals, which could account for why participants took fewer risks for others when making important treatment decisions. In fact, Stone et al. (Citation2013) report that people take less risk for a friend in physical safety scenarios, even when they predict their friend to take the same level of risk as them. These results mirror ours and suggest that social values might be similar across physical safety and medical treatment scenarios. However, given our findings it seems unlikely that all surrogate decisions are driven solely by social values.
Conclusions and future directions
In this paper, we sought to investigate the relationship between surrogates’ predictions of a recipient’s utilities and the choices they make on their behalf. We did find support for a predictive relationship between surrogate predictions and choices. However, our findings indicate that self-other differences in decision-making cannot be solely accounted for by a perceived self-other difference in utilities. It would be interesting to examine whether this is also the case when surrogates are explicitly asked to make a decision based on the recipient’s wishes and preferences. This would strengthen the conclusion that making a surrogate decision is a difficult task due to the responsibility placed on the decision-maker and the higher level of uncertainty relative to making one’s own decisions, making it unlikely that they can accurately represent the recipient’s wishes and preferences. Additionally, gaining more insight into the decision process through confidence measures and thought-listing techniques would further elucidate the decision process.
In order to develop a better understanding of how our study can speak to real-world scenarios, future research should build on it by using more realistic scenarios and investigating whether the present findings change when people make decisions for someone they are familiar with. Our findings can nonetheless speak to the wider research concerning surrogate decision-makers which shows that surrogates have a difficult time trying to reconcile the patient’s wishes with a multitude of other perspectives and responsibilities (Dionne-Odom et al., Citation2015; Schenker et al., Citation2012), and that the substituted judgment standard is limited in helping surrogates make the right decision (Torke et al., Citation2008). On the other hand, it presents a more hopeful picture than previous research which indicated that decisions are not made in line with their predictions of the recipient’s preferences.
Declaration of interest statement
The authors declare no conflicts of interest.
Acknowledgement
This work was supported by the Economic and Social Research Council [grant number ES/J500100/1], an ESRC post-graduate studentship to Eleonore Batteux.
Data availability statement
The data that supports the findings of this study are available from https://osf.io/tp8sg/.
Notes
1 There are many other literatures that show that our predictions of others’ preferences are often inaccurate, for example in gift giving (Galak, Givi, & Williams, Citation2016), willingness to pay (Frederick, Citation2012), the false-consensus effect (Ross, Greene, & House, Citation1977) and the egocentric anchoring and adjustment heuristic (Epley, Keysar, Van Boven, & Gilovich, Citation2004).
2 We call this task a rating task to differentiate it from the choice task. However, both tasks can be conceptualised as two different decision questions.
3 95% confidence intervals were obtained via 1000 bootstrapped samples.
4 The studies we presented here also manipulated the recipient as a within-subjects factor, which raises the possibility that self-other differences may be contingent on that manipulation. However, similar findings have also been reported using between-subjects designs in both the medical (Zikmund-Fisher et al., Citation2006; Ubel et al., Citation2011) and financial domain (Polman, Citation2012; Pollmann et al., Citation2014; Sun et al., Citation2016).
5 Indeed, Garcia-Retamero, Okan, and Maldonado (Citation2015) conducted a study with a student sample and found that they were more risk-seeking for a classmate than for themselves, which contradicts their previous findings with doctors using the same scenarios (Garcia-Retamero & Galesic, Citation2012). Notably, the severity of the illness depicted in the scenario they used was akin to that of our moderate conditions which slightly increased risk-taking.
6 The scenarios presented are worded as in the self condition. In the other condition, it was made clear that the other was another participant and all pronouns were changed accordingly.
References
- Batteux, E., Ferguson, E., & Tunney, R. J. (2017). Risk Preferences in Surrogate Decision Making. Experimental Psychology, 64(4), 290–297. doi:10.1027/1618-3169/a000371
- Beisswanger, A. H., Stone, E. R., Hupp, J. M., & Allgaier, L. (2003). Risk Taking in Relationships: Differences in Deciding for Oneself Versus for a Friend. Basic and Applied Social Psychology, 25(2), 137–143. https://doi.org/10.1207/S15324834BASP2502
- Benjamin, A. M., & Robbins, S. J. (2007). The role of framing effects in performance on the Balloon Analogue Risk Task (BART). Personality and Individual Differences, 43(2), 221–230. doi:10.1016/j.paid.2006.11.026
- Dionne-Odom, J. N., Willis, D. G., Bakitas, M., Crandall, B., & Grace, P. J. (2015). Conceptualizing surrogate decision making at end of life in the intensive care unit using cognitive task analysis. Nursing Outlook, 63(3), 331–340. doi:10.1016/j.outlook.2014.10.004
- Dore, R. A., Stone, E. R., & Buchanan, C. M. (2014). A Social Values Analysis of Parental Decision Making. The Journal of Psychology, 148(4), 477–504. doi:10.1080/00223980.2013.808603
- Epley, N., Keysar, B., Van Boven, L., & Gilovich, T. (2004). Perspective taking as egocentric anchoring and adjustment. Journal of Personality and Social Psychology, 87(3), 327–339. doi:10.1037/0022-3514.87.3.327
- Eriksen, K. W., & Kval⊘y, O. (2010). Myopic investment management. Review of Finance, 14(3), 521–542. doi:10.1093/rof/rfp019
- Fagerlin, A., Danks, J. H., Ditto, P. H., & Houts, R. M. (2001). Projection in Surrogate Decisions About Life-Sustaining Medical Treatments. Health Psychology, 20(3), 166–175. doi:10.1037/0278-6133.20.3.166
- Faro, D., & Rottenstreich, Y. (2006). Affect, Empathy, and Regressive Mispredictions of Others’ Preferences Under Risk. Management Science, 52(4), 529–541. doi:10.1287/mnsc.1050.0490
- Fernandez-Duque, D., & Wifall, T. (2007). Actor/observer asymmetry in risky decision making. Judgment and Decision Making, 2(1), 1–8. Retrieved from http://journal.sjdm.org/06134/jdm06134.htm
- Frederick, S. (2012). Overestimating Others ’ Willingness to Pay. Journal of Consumer Research 39(1), 1–21. doi:10.1086/662060
- Galak, J., Givi, J., & Williams, E. F. (2016). Why Certain Gifts Are Great to Give but Not to Get: A Framework for Understanding Errors in Gift Giving Errors in Gift Giving. Current Directions in Psychological Science, 25(6), 380–385. doi:10.1177/0963721416656937
- Garcia-Retamero, R., & Galesic, M. (2012). Doc, What Would You Do If You Were Me? On Self-Other Discrepancies in Medical Decision Making. Journal of Experimental Psychology-Applied, 18(1), 38–51. doi:10.1037/a0026018
- Garcia-Retamero, R., Okan, Y., & Maldonado, A. (2015). The Impact of Depression on Self-Other Discrepancies in Decision Making. Journal of Behavioral Decision Making, 28(1), 89–100. doi:10.1002/bdm.1833
- Hadar, L., & Fischer, I. (2008). Giving advice under uncertainty: What you do, what you should do, and what others think you do. Journal of Economic Psychology, 29(5), 667–683. doi:10.1016/j.joep.2007.12.007
- Hsee, C. K., & Weber, E. U. (1997). A fundamental prediction error: self-other discrepancies in risk preference. Journal of Experimental Psychology: General, 126(1), 45–53. doi:10.1037//0096-3445.126.1.45
- Krishnamurthy, P., & Kumar, P. (2002). Self–Other Discrepancies in Waiting Time Decisions. Organizational Behavior & Human Decision Processes, 87(2), 207–226. doi:10.1006/obhd.2001.2980
- Lichtenstein, S., & Slovic, P. (1971). Reversals of preference between bids and choices in gambling decisions. Journal of Experimental Psychology, 89(1), 46–55. doi:10.1037/h0031207
- Loewenstein, G. (1996). Out of Control: Visceral Influences on Behavior. Organizational Behavior and Human Decision Processes, 65(3), 272–292. doi:10.1006/obhd.1996.0028
- Loewenstein, G. F., Weber, E. U., Hsee, C. K., & Welch, N. (2001). Risks as Feelings. Psychological Bulletin, 127(2), 267-286. doi:10.1037/0033-2909.127.2.267
- Mengarelli, F., Moretti, L., Faralla, V., Vindras, P., & Sirigu, A. (2014). Economic decisions for others: An exception to loss aversion law. PLoS ONE, 9(1), 1–6. https://doi.org/10.1371/journal.pone.0085042
- Oliver, A. (2013). Testing the rate of preference reversal in personal and social decision-making. Journal of Health Economics, 32(6), 1250–1257. doi:10.1016/j.jhealeco.2013.10.003
- Pachur, T., Hertwig, R., & Wolkewitz, R. (2014). The affect gap in risky choice: Affect-rich outcomes attenuate attention to probability information. Decision, 1(1), 64–78. doi:10.1037/dec0000006
- Pahlke, J., Strasser, S., & Vieider, F. M. (2015). Responsibility effects in decision making under risk. Journal of Risk and Uncertainty, 51(2), 125–146. doi:10.1007/s11166-015-9223-6
- Peirce, J. W. (2007). PsychoPy—psychophysics software in Python. Journal of neuroscience methods, 162(1), 8–13. doi:10.1016/j.jneumeth.2006.11.017
- Petrova, D., Garcia-Retamero, R., & Van Der Pligt, J. (2016). What Factors Moderate Self-Other Discrepancies in Decision Making? Results from a Vaccination Scenario. Spanish Journal of Psychology, 19(2016), 1–11. https://doi.org/10.1017/sjp.2016.50
- Pollmann, M. M. H., Potters, J., & Trautmann, S. T. (2014). Risk taking by agents: The role of ex-ante and ex-post accountability. Economics Letters, 123(3), 387–390. doi:10.1016/j.econlet.2014.04.004
- Polman, E. (2012). Self-other decision making and loss aversion. Organizational Behavior and Human Decision Processes, 119(2), 141–150. doi:10.1016/j.obhdp.2012.06.005
- Raymark, P. H. (2000). Accepting or rejecting medical treatment: A comparison of decisions made for self versus those made for a significant other. Journal of Applied Social Psychology, 30(11), 2409–2436. doi:10.1111/j.1559-1816.2000.tb02443.x
- Read, J. L., Quinn, R. J., Berwick, D. M., Fineberg, H. V., & Weinstein, M. C. (1984). Preferences for health outcomes. Comparison of assessment methods. Medical Decision Making, 4(3), 315–329. doi:10.1177/0272989X8400400307
- Rosen, A. B., Tsai, J. S., & Downs, S. M. (2003). Variations in risk attitude across race, gender, and education. Medical Decision Making, 23(6), 511–517. doi:10.1177/0272989X03258431
- Ross, L., Greene, D., & House, P. (1977). The “false consensus effect”: An egocentric bias in social perception and attribution processes. Journal of Experimental Social Psychology, 13(3), 279–301. doi:10.1016/0022-1031(77)90049-X
- Schenker, Y., Crowley-Matoka, M., Dohan, D., Tiver, G. A., Arnold, R. M., & White, D. B. (2012). I Don’t Want to Be the One Saying ‘We Should Just Let Him Die’: Intrapersonal Tensions Experienced by Surrogate Decision Makers in the ICU. Journal of General Internal Medicine, 27(12), 1657–1665. doi:10.1007/s11606-012-2129-y
- Shalowitz, D. I., Garrett-Mayer, E., & Wendler, D. (2006). The accuracy of surrogate decision makers: a systematic review. Archives of Internal Medicine, 166(5), 493–497. doi:10.1001/archinte.166.5.493
- Stone, E. R., & Allgaier, L. (2008). A Social Values Analysis of Self-Other Differences in Decision Making Involving Risk. Basic & Applied Social Psychology, 30(2), 114–129. doi:10.1080/01973530802208832
- Stone, E. R., Choi, Y., de Bruin, W. B., & Mandel, D. R. (2013). I can take the risk, but you should be safe: Self-other differences in situations involving physical safety. Judgment and Decision Making, 8(3), 250–267. Retrieved from http://journal.sjdm.org/10/10907/jdm10907.html
- Stone, E. R., Yates, A. J., & Caruthers, A. S. (2002). Risk taking in decision making for others versus the self. Journal of Applied Social Psychology, 32(9), 1797–1824. doi:10.1111/j.1559-1816.2002.tb00260.x
- Sun, Q., Liu, Y., Zhang, H., & Lu, J. (2016). Increased Social Distance Makes People More Risk Neutral. The Journal of Social Psychology, 157(4), 502–512. doi:10.1080/00224545.2016.1242471
- Torke, A. M., Alexander, G. C., & Lantos, J. (2008). Substituted judgment: The limitations of autonomy in surrogate decision making. Journal of General Internal Medicine, 23(9), 1514–1517. doi:10.1007/s11606-008-0688-8
- Trope, Y., & Liberman, N. (2010). Constual-level theory of psychological distance. Psychology Review, 117(2), 440–463. doi:10.1037/a0018963
- Tunney, R. J. (2006). Preference reversals are diminished when gambles are presented as relative frequencies. Quarterly Journal of Experimental Psychology (2006), 59(9), 1516–1523. doi:10.1080/17470210600750509
- Tunney, R., & Ziegler, F. (2015). Toward a Psychology of Surrogate Decision-Making. Perspectives on Psychological Science, 10(6), 880–885. doi:10.1177/1745691615598508
- Ubel, P. A., Angott, A. M., & Zikmund-Fisher, B. J. (2011). Physicians recommend different treatments for patients than they would choose for themselves. Archives of Internal Medicine, 171(7), 630–634. https://doi.org/10.1001/archinternmed.2011.457
- Whitehead, S. J., & Ali, S. (2010). Health outcomes in economic evaluation: The QALY and utilities. British Medical Bulletin, 96(1), 5–21. doi:10.1093/bmb/ldq033
- Zaleska, M., & Kogan, N. (1971). Level of Risk Selected by Individuals and Groups When Deciding for Self and for Others. Sociometry, 34(2), 198–213. doi:10.2307/2786410
- Zhang, X., Liu, Y., Chen, X., Shang, X., & Liu, Y. (2017). Decisions for others are less risk-averse in the gain frame and less risk-seeking in the loss frame than decisions for the self. Frontiers in Psychology, 8(SEP), 1601–1610. doi:10.3389/fpsyg.2017.01601
- Ziegler, F. V., & Tunney, R. J. (2015). Who's been framed? Framing effects are reduced in financial gambles made for others. BMC Psychology, 3(1), 9 doi:10.1186/s40359-015-0067-2
- Zikmund-Fisher, B. J., Sarr, B., Fagerlin, A., & Ubel, P. A. (2006). A matter of perspective: Choosing for others differs from choosing for yourself in making treatment decisions. Journal of General Internal Medicine, 21(6), 618–622. doi:10.1111/j.1525-1497.2006.00410.x
- Zou, X., & Scholer, A. A. (2016). Motivational Affordance and Risk-Taking Across Decision Domains. Personality and Social Psychology Bulletin, 42(3), 275–289. doi:10.1177/0146167215626706
Appendix: Medical scenarios6
Severe conditions
Paraplegia: Imagine you suddenly develop paraplegia. You suffer from a complete loss of sensation and movement from the waist down, meaning that your legs are paralysed. You are wheelchair-bound and you lose control of your bladder and your bowel. You require some assistance with self-care. Without treatment, there is no chance of recovery.
Broca’s Aphasia: Imagine that you suddenly develop Broca’s aphasia (a type of stroke). You will have a very difficult time speaking and writing. Nobody can understand you except for maybe the one or two people closest to you. This is very frustrating because you can understand other people but they don’t understand you. You can speak a little but you have to work hard at it and most of the words you say will not make sense. Without treatment, there is no chance of recovery.
Vegetative State: Imagine you are the victim of an accident which leaves you in a vegetative state. You are bed-bound and need to be fed through a tube. You have almost lost all consciousness. You are unable to see, speak, and can barely think. You can hear and understand some of the things that are going on around you. You can slightly move your fingers meaning that you can occasionally communicate. There is no pain with this condition and without treatment, there is no chance of recovery.
Moderate conditions
Angina: Imagine that you suddenly develop an angina. You have pain or discomfort in mainly in your chest but also in your upper body. You suffer from fatigue and occasional dizziness. You find breathing more difficult than usual. You can take medication to alleviate the symptoms but these are persistent and without treatment, there is no chance of recovery.
Headache: Imagine that you suddenly develop a persistent headache. You suffer from an aching head pain and a sensation of tightness or pressure across your forehead. You struggle to concentrate and the pain can render you unable to take part in your daily activities. Medication does not entirely relieve the pain and without treatment, there is no chance of recovery.
Nausea: Imagine that you develop an illness with symptoms of nausea. You often feel discomfort in your stomach and you are occasionally sick. This makes it more difficult for you to eat and get on with your day. You may be unable to work if the discomfort is too high. You can take medication to reduce the symptoms and without treatment, there is no chance of recovery.