
ABSTRACT
Introduction: Individuals tend to explore the left side of a face first and for a longer time in comparison to the right side. This left visual field (LVF) bias is suggested to reflect right hemispheric dominance for face processing. Social anxiety disorder (SAD) is associated with maladaptive interpretations of facial expressions, but it is not known whether this is linked to an atypical LVF bias. Previous studies have reported a reduced LVF bias in autism, a condition overlapping with SAD. This pre-registered study examined the LVF bias in adolescents with SAD.
Methods: Eye-tracking was used to investigate the ratio of first fixations to the left on upright and inverted face stimuli in 26 adolescents (13-17 years) with SAD and 23 healthy controls primed to look either between the eyes or at the mouth.
Results: The SAD group showed a smaller LVF bias and an atypical face inversion effect when primed to look at the eyes. Autistic traits predicted a smaller LVF bias, independently of social anxiety level.
Conclusions: Results suggest that SAD is associated with impaired processing of faces at an early stage of visual scanning. The findings contribute to a better understanding of SAD and its overlap with autism.
Introduction
Social anxiety disorder (SAD) is a psychiatric disorder characterised by intense fear of being negatively evaluated in social situations. This fear leads to avoidance, functional impairment and distress for the affected individual (American Psychiatric Association, Citation2013). SAD is associated with maladaptive interpretations of others’ facial expressions and intentions. For example, individuals with high levels of social anxiety display a bias for interpreting ambiguous facial expressions as more threatening in comparison to individuals with lower levels of social anxiety (Yoon & Zinbarg, Citation2008), and tend to misinterpret others as being mocking or critical (Rapee & Heimberg, Citation1997; Weeks et al., Citation2008). These biases may lead to avoidance of social interaction. Consequently, social cognitive biases may function as a maintaining factor, or a causal mechanism contributing to the emergence of SAD (Hofmann, Citation2007; Rapee & Spence, Citation2004). Disrupted processing of facial information could be a factor underlying some of these cognitive biases (NTM Chen & Clarke, Citation2017; Lau & Waters, Citation2017). Previous studies have reported an atypical pattern of visual attention to faces in SAD. Children and adolescents diagnosed with SAD look less at faces with threatening expressions, or eyes with direct gaze than healthy controls (Högström et al., Citation2019; Kleberg et al., Citation2017; Schneier et al., Citation2011; Weeks et al., Citation2013), and tend to view social scenes with atypical visual scanpaths characterised by short, widely distributed fixations (NTM Chen et al., Citation2015). Atypical physiological responses to faces have also been documented by studies using various outcomes and methods, including pupil dilation (Keil et al., Citation2018; Kleberg et al., Citation2019) and functional magnetic resonance imaging (fMRI; Gentili et al., Citation2016; Gingnell et al., Citation2016).
Typically developing individuals tend to explore the left side of a face first (from the viewer's perspective) and for a longer time in comparison to the right side of the face (e.g. Butler et al., Citation2005; Guo et al., Citation2009; Guo et al., Citation2012). Given that the brain’s right hemisphere receives visual input from the left visual field (LVF), it has been commonly assumed that this LVF bias reflects the right hemispheric dominance in face processing (Guo et al., Citation2012; Yovel et al., Citation2008). In contrast, a diminished LVF bias has been found in conditions associated with impaired social interaction, such as autism spectrum disorder (Ashwin et al., Citation2005; Guillon et al., Citation2014). To our knowledge, the LVF bias for faces has not been studied previously in individuals diagnosed with SAD. However, one study found that self-reported social anxiety in a non-clinical sample predicted a reduced bias for the left visual field in perceptual judgements of facial identity (Bourne & Vladeanu, Citation2011; see also Bourne & Vladeanu, Citation2017)
However, autism and SAD are known to be overlapping conditions, both categorically and dimensionally. SAD is one of the most prevalent comorbid conditions found in individuals with ASD (Simonoff et al., Citation2008; Van Steensel, Bögels & Perrin, Citation2011), and elevated levels of autistic traits are often seen in individuals with SAD (Cholemkery et al., Citation2014; Kleberg et al., Citation2017). Both autism and SAD are linked to atypical face perception (Chita-Tegmark, Citation2016; Kleberg et al., Citation2019). A small number of studies have suggested that the two symptom dimensions may map onto different aspects of face perception (Capriola-Hall et al., Citation2018; Kleberg et al., Citation2017) but again, no studies exist in relation to the LVF bias.
Eye-tracking studies have demonstrated that the LVF bias is most pronounced during the earliest stages of visual scanning, i.e. for the first fixation (Dundas et al., Citation2012; Guo et al., Citation2009; Leonards & Scott-Samuel, Citation2005). In contrast, an LVF bias was not found in other scanpath measures such as the average fixation duration during two seconds (Butler et al., Citation2005). The LVF bias has therefore been interpreted as reflecting a rapid and automatic process (Guillon et al., Citation2014; Leonards & Scott-Samuel, Citation2005).
The LVF is typically reduced when faces are inverted (Coolican et al., Citation2008; Luh, Citation1998). This is in line with a large body of research documenting that specialised face processing mechanisms are disrupted by inversion (Rossion, Citation2009; Yovel & Kanwisher, Citation2005). An atypical effect of inversion could therefore provide additional evidence for disrupted face processing in SAD.
The primary aim of the present study was to investigate LVF bias for faces on the first fixation in adolescents with SAD and healthy controls. We focused on this measure rather than other aspects of the scan path in light of previous studies which have documented that the LVF bias is most consistent for this measure. As a secondary aim, we examined the relation between the LVF bias and symptoms of both social anxiety and autistic traits in a dimensional analysis.
As SAD commonly develops in early adolescence or young adulthood (Stein et al., Citation2017), studies on young samples are of particular importance. Faces were presented either upright or inverted and in light of previous research, the SAD group was hypothesized to show a less expressed LVF bias for upright faces compared to controls. In addition, inversion of the face stimuli was expected to affect the LVF bias less in adolescents with SAD than in controls. As an exploratory manipulation, individuals were primed to look first at either the mouth or the eyes, which are typically the two regions that are most salient in face perception.
Pre-registration
The analysis plan and hypotheses were pre-registered in the Open Science Framework (link removed for anonymization). According to the original plan, an additional control group with autism spectrum disorder would be included. This part of the study was dropped, since we only managed to recruit nine individuals with autism.
Method
Participants
The final sample included 49 adolescents (26 with SAD), all residing in the Stockholm region. Demographic information and clinical features are presented in . Participants in the control group were recruited from the Swedish population register, from which adolescents aged 13–17 were randomly selected based on age and gender to match the SAD group. Legal guardians were contacted by mail inviting their adolescent to partake in the study. Initially, 25 individuals agreed to participate in the control group. Of these, one was excluded due to invalid data (see Data Reduction), one because of suspected SAD, and two because they were left-handed according to self-report. Individuals with SAD were recruited from an ongoing clinical trial evaluating cognitive behavioral therapy (CBT) for SAD (Nordh et al., Citation2017). The experimental procedure of this study took place approximately one week before the initiation of CBT treatment. Out of an initial sample of 30 participants in the clinical study, 27 volunteered to participate in the current study. Two of these were excluded because they were left-handed according to self-report.
Table 1. Demographics and Clinical Test Scores
Clinical assessment
Prior to the experiment, all participants were assessed by a clinical psychologist using the Mini-International Neuropsychiatric Interview for Children (MINI-KID) (Sheehan et al., Citation2010). Exclusion criteria for individuals with SAD were a comorbid diagnosis within the autism spectrum disorder, bipolar disorder, psychosis, severe eating disorder, substance abuse and exposure to domestic violence. Exclusion criteria for controls were presence of a psychiatric disorder according to the clinical assessment. Participating individuals completed the Social Phobia and Anxiety Inventory for Children (SPAI-C), a validated self-report measure of social anxiety (Beidel et al., Citation1995). As expected, the SAD group had higher SPAI-C scores than controls (see ), and no individual in the control group scored above the cut off for SAD (Beidel et al., Citation1995). IQ was assessed using the General Ability Index (GAI), from the Wechsler Intelligence Scale for Children 4th. Ed (Wechsler, Citation2003) or the Wechsler Adult Intelligence Scale 4th. Ed (Wechsler, Citation2008) depending on the child’s age. All participants in the SAD group were invited to take the cognitive assessment test within six months after the experiment, and individuals in the control group completed the cognitive assessment at the day of the experiment. IQ was available from 17 individuals with SAD and all individuals in the control group. Parents of all participants completed the Social Responsiveness Scale (SRS) (Constantino & Gruber, Citation2012), a well-validated dimensional measure of autistic traits. As can be seen in , the SAD group had higher scores on the SRS than controls, although lower than what is typically seen in autism (Bölte et al., Citation2008).
Informed consent and ethical approval
Legal guardians and adolescents aged 15–17 gave their written informed consent prior to the study. Adolescents aged 13 and 14 old gave their consent verbally prior to the study. Participants in both the SAD and the control group were compensated with a gift certificate with a value of 21 USD. Ethical approval was obtained from the regional ethical review board in Stockholm (dnr 2015/1383-31 and amendment 2016/1183-32).
Experimental stimuli
Stimuli were images of still faces collected from the Karolinska Directed Emotional Faces (KDEF) dataset (Flykt et al., Citation1998). The stimuli consisted of actors (50% male and 50% female) expressing emotional and neutral faces (equally divided between happy, angry and neutral). The facial images were cropped to show only the inner region of the face in order to reduce the risk that participants attention would be drawn to external features such as the hair. (see –)
Figure 1. Example of upright stimuli displaying primed region between the eyes (a) and primed region on the mouth (b). Blue dot indicates how the position of the face stimuli varied in relation to the initial fixation cross.
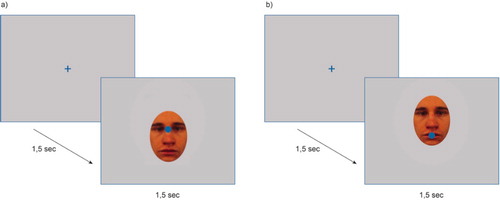
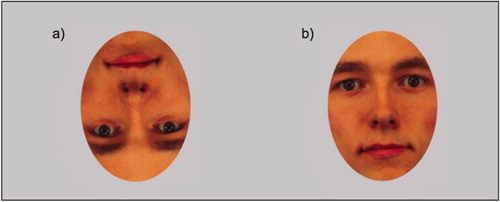
Figure 2. Example of inverted face stimuli (a) and upright face stimuli (b).
Experimental procedure
Participants were positioned approximately 60 cm from a computer screen. Prior to the experiment, a nine-point calibration procedure was completed. Participants were instructed to sit still and attend to the screen, but no further instructions were given. In each trial, participants initially fixated on a central cross appearing on a light grey screen for 1500 ms. This was followed by presentation of the face stimuli for 1500 ms. The location of the face varied in relation to the initial fixation cross so that the participant was primed to look at the vertical midline of the face either at a point between the eyes (50% of trials) or at the mouth (50% of trials; see ). The trials were equally distributed between upright (50%) and inverted faces (50%; see .). In total, each participant completed 120 trials. The position of the initial fixation cross at the screen was kept constant between trials to exclude the possibility to predict the location of the upcoming face. As a consequence of the experimental design, the amount of information presented in the upper and lower visual hemifield differed between conditions. The largest part of the face was presented in the upper hemifield when faces were upright and the mouth was primed, or when faces were inverted and the eyes were primed. In contrast, faces were to the largest part visible in the lower hemifield when the eyes were primed in the upright condition, or the mouth was primed in the inverted condition (see –). Potential implications of this are brought up in the discussion.
Recording and processing of gaze data
Data were collected using a near infrared corneal reflection eye tracker (Tobii T120, Tobii Inc, Danderyd, Sweden) at a sample rate of 120 HZ. Gaze data were filtered using a dispersion-based fixation filter (Tobii fixation filter) with duration and velocity thresholds set to 35 pixels. The analysis was conducted using custom scripts written in MATLAB (Mathworks, Inc, USA). A subset of recordings was visualised and coded manually by two observers blind to group membership as an additional validation check. Trials were included if, (1) a fixation was detected within the primed region at stimulus onset, and (2) a valid fixation (to the left or right) was detected after 80 ms or more. Gaze shifts with latencies < 80 ms were considered anticipatory and if an anticipatory gaze shift was discovered, the whole trial was discarded.
Data reduction and Statistical analyses
First fixation location (left or right of the vertical midline of the face) was coded for each trial. For each individual and condition, the ratio of first fixations to the left of the total number of valid fixations was computed. Thus, a value above 0.5 indicates a higher proportion of fixations to the left. This measure was used as the dependent variable and is referred to as the LVF ratio. In a first set of analyses, we compared the LVF ratio to chance level in each group and condition using one-sample t-tests. In a second step, data were analysed using linear mixed effects models (LMM). The LMMs were fitted with random intercept for individual to account for the fact that trials were nested at the level of the individual (i.e. were repeated measures). Data were analysed with Orientation (upright or inverted face stimuli) and Primed region (between the eyes or on the mouth) as within-subjects repeated measures factors. Group (SAD, Control) was added as a between-subjects factor. Emotion was added as an additional factor in all analyses. For this purpose, emotional stimuli were coded as either threatening (angry) or non-threatening (happy or neutral).
Significant interaction effects were followed up with Bonferroni corrected pairwise comparisons. The alpha level was set to .05. Effect sizes are reported as differences in proportions of first fixations to the left between groups or conditions (Δb). Statistical significance was tested with analyses of variance (ANOVAs).
A multiple regression analysis was used to examine independent relations between dimensional autistic symptoms traits and social anxiety symptoms on the LVF bias. One outlier showed over 80% bias to the right of the vertical midline in three out of four conditions, which was highly unexpected in light of previous studies (e.g. (Butler et al., Citation2005; Guo et al., Citation2009)). This participant was removed from further analysis.
Results
LVF ratio
Results are shown in and . The LVF ratio was significantly higher than 0.5 in all conditions in the control group, confirming the existence of an LVF bias. In the SAD group, an LVF ratio significantly above 0.5 was only observed for upright faces with the mouth as Primed region. As can be seen in , the highest density of first fixations was seen in the left part of the eye region.
Figure 3. Left: Heatmaps showing the density of first fixations in the control and SAD groups overlaid on an example of the stimulus images. A gaussian filter with sigma corresponding to ∼.5 degrees of the visual field was applied to the data. Right: Difference in fixation density between the control and SAD groups scaled to maximum difference (higher values indicate higher fixation density in controls).
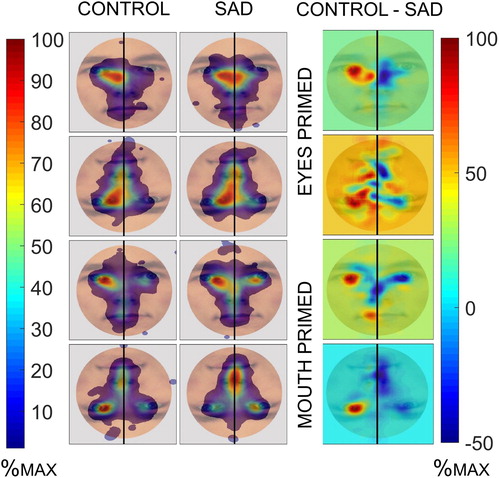
Table 2. Left Visual Field Ratio (% first fixations to the left) by condition in relation to chance level (.50)
Across groups, a main effect of Orientation was found, reflecting a stronger LVF bias for upright than inverted faces, F = 20.32, p = <.001, Δb = −0.08, SE = 0.02. The LVF bias was also higher when the eyes were primed, than when the mouth was primed, F = 5.95, p = 0.015, Δb = −0.04, SE = 0.02. The LVF bias was higher in controls than in the SAD group, but the difference was not significant, F = 3.31, p = 0.070, Δb = 0.13, SE = 0.07. There was no main effect of Emotion, F = 0.01, p = .917, Δb <0.01, SE = 0.02.
No significant two-way interactions were found between Orientation and Group, F = 0.54, p = 0.461, Δb = 0.03, SE = 0.03, Primed region and Group, F = 0.10, p = 0.747, Δb = −0.01, SE = 0.03, Emotion and Group F = 0.16, p = 0.689, Δb = 0.01, SE = 0.03, or Orientation and Primed region, F = 1.71, p = 0.192, Δb = −0.04, SE = 0.03. However, a statistically significant three-way interaction was found between Group, Primed region and Orientation, F = 26.70, p = <.001. The three-way Group x Primed region x Orientation interaction was followed up in two steps. In a first step, separate Group x Primed region analyses were conducted for each orientation. In a second step, separate Primed region x Orientation analyses were conducted for each group separately.
Follow-up analyses: comparison between SAD and control group
Significant interaction effects were found between Group and Primed region in both the upright, F = 8.75, p = 0.003, Δb = 0.18, SE = 0.06, and the inverted conditions, F = 6.97, p = 0.008, Δb = −0.16, SE = 0.06. These interactions were followed up with pairwise Bonferroni-corrected comparisons. The LVF ratio was higher in controls than in the SAD group when the eyes were primed in the upright condition, F = 6.89, p = 0.040, Δ b = 0.20, SE = 0.08, and when the eyes were primed in the inverted condition, F = 6.86, p = 0.040, Δb = 0.22, SE = 0.08. No other pairwise comparisons were significant (p > .25).
Follow-up analyses: SAD group
A main effect of Orientation was found in the SAD group, reflecting a higher proportion of leftwards fixations for upright faces, F = 11.41, p = 0.001, Δb = −0.09, SE = 0.03. The main effect of Primed region was not significant F = 1.97, p = 0.162, Δb = −0.04, SE = 0.03. However, a significant interaction effect between Orientation and Primed region was found, F = 15.79, p = <.001, Δb = −0.20, SE = 0.05. Follow-up tests showed that an inversion effect was found for the eye region, F = 15.90, p = <.001, Δb = −0.19, SE = 0.05, but not the mouth region, F = 0.02, p = 0.884, Δb = 0.01, SE = 0.07. Furthermore, an effect of Primed region was observed for inverted faces, driven by a lower LVF ratio when the eyes were primed F = 7.99, p = 0.024, Δb = −0.14, SE = 0.05. In contrast, no effect of Primed region was found for upright faces, F = 2.31, p = 0.524, Δb = 0.07, SE = 0.04
Follow-up analyses: control group
A significant main effect of Orientation was found in the control group, F = 9.46, p = 0.002, Δb = −0.06, SE = 0.02, reflecting a higher LVF ratio for upright faces. No significant main effect of Primed region was found, F = 3.46, p = 0.065, Δb = −0.05, SE = 0.03. A significant interaction effect was found between Orientation and Primed region, F = 12.60, p = 0.001, Δb = 0.14, SE = 0.04. An effect of Primed region was found in the upright condition, driven by a higher LVF ratio when the eyes were primed, F = 10.37, p = 0.008, Δb = −0.12, SE = 0.04, but not in the inverted condition, F = 0.37, p = 0.547, Δb = 0.02, SE = 0.04. Pairwise comparisons showed no effect of inversion when the mouth was primed, F = 5.30, p = 0.096, Δb = −0.12, SE = 0.05, or when the eyes were primed, F = 0.03, p = 0.857, Δb = 0.01, SE = 0.03.
Dimensional analysis
A multiple regression analysis was used to examine dimensional links between the LVF ratio, social anxiety symptoms (SPAI-C), and autistic traits (SRS). The dependent variable was the average LVF ratio in the two conditions where a group difference between adolescents with SAD and controls was found, i.e. for upright trials where the mouth was primed, and for inverted trials where the eyes were found. Both groups were included in the analysis. The overall model was significant, F (41) = 4.13, p = .023. A reduced LVF ratio was independently predicted by autistic traits (β = -.51, SE = 0.20, p = .018), but not by social anxiety symptoms, (β = .17, SE = 0.21, p = .390)
Summary of the results
First, whereas controls showed a significant LVF bias in all conditions, this was only found in the SAD group when the mouth was primed in the upright conditions. Second, group differences driven by reduced LVF ratios in the SAD group were found when the mouth was primed in the upright condition, or when the eyes were primed in the inverted condition. Third, both groups showed the expected reduction of leftward fixations when faces were inverted. However, this inversion effect was stronger for the eye region than for the mouth region in adolescents with SAD, but was not modulated by Primed region in the control group. Finally, a dimensional analysis suggested that a reduced LVF bias was independently predicted by autistic traits, but not social anxiety symptoms.
Discussion
The aim of this study was to investigate LVF bias for faces on the first fixation in adolescents with SAD and healthy controls. The SAD group was hypothesized to show a less expressed LVF bias for upright faces compared to controls, as well as a reduced effect of face inversion.
The first hypothesis was partly supported. Whereas the control group showed a consistent LVF bias across the experimental conditions, adolescents with SAD showed a reliable bias only when the mouth was primed in the upright condition. Unexpectedly however, significant group differences were found in two conditions only – when either the mouth of upright faces or the eyes of inverted faces were primed. In other words, it seems that a reduced LVF bias in adolescents with SAD was found when stimuli were mainly visible in the lower visual hemifield, but not in the upper hemifield. While the general pattern of these results (e.g. a reduced LVF bias in adolescents with SAD) was expected, the apparent effect of upper vs lower visual hemifield was not hypothesized. Information in the upper visual field is more strongly projected to the ventral visual stream specialised for object recognition than information in the lower hemifield. As a consequence, an upper visual field advantage has been reported for object processing, which is domain-general and applies to both faces and objects (Carlei et al., Citation2017; Fecteau et al., Citation2000). Reduced LVF bias in adolescents with SAD could potentially reflect a higher degree of reliance on domain-general processes that are preferentially activated when information is present in the upper hemifield. However, more research is needed to determine this.
Secondly, we hypothesized that inversion would reduce the LVF bias, but that this effect of inversion would be reduced in SAD. This hypothesis was not supported.
Across conditions, both groups showed the expected reduced LVF bias for inverted as compared to upright faces (Coolican et al., Citation2008; Luh, Citation1998). However, this inversion effect was modulated by primed region in the SAD group, where a stronger inversion effect was found for the eye region than for the mouth region. To the best of our knowledge, no previous study has examined how priming of specific face regions affects the LVF bias in face processing. However, it is known from previous studies that gaze to (upright) eyes leads to enhanced activity in brain structures known to be crucial for the face inversion effect as well as in face processing more generally (Hadjikhani et al., Citation2017; Senju & Johnson, Citation2009). For example, Hadjikhani et al. (Citation2017) demonstrated that the activity in brain regions implicated in the face inversion effect as well as face processing more generally, such as the fusiform face area and amygdala, is enhanced when an individual’s gaze is constrained to the eye region. Atypical activation of these areas has previously been documented in SAD (Frick et al., Citation2013; Gentili et al., Citation2016). As outlined in the introduction, eyes with direct gaze signal a potential social threat, and are therefore a disorder relevant stimulus in SAD. Consequently, it is possible that face processing is particularly disrupted in SAD when the eyes are primed (Kleberg et al., Citation2017; Weeks et al., Citation2013).
Our third aim was to examine the joint influence of social anxiety and autistic traits on the left visual field bias. This analysis was motivated by the known overlap between the two symptom dimensions (Cholemkery et al., Citation2014; Simonoff et al., Citation2008), as well as previous reports of a reduced LVF in autism (Ashwin et al., Citation2005; Dundas et al., Citation2012; Guillon et al., Citation2014). Results from the dimensional analysis suggest that a reduced LVF bias may be best explained by autistic traits rather than by the level of social anxiety. This result adds to a small number of studies suggesting that autistic traits and social anxiety may have different relations to social attention processes (Capriola-Hall et al., Citation2018; Kleberg et al., Citation2017). As noted in the introduction, social anxiety and autism are overlapping symptom dimensions, and a better understanding of their respective relation to atypical social attention may enhance our understanding of both conditions. This is potentially important in clinical settings, since the presence of autistic traits in SAD may be related to both treatment outcome and etiological factors (Maddox & White, Citation2015; Puleo & Kendall, Citation2011; South & Rodgers, Citation2017).
No effect of emotion was found, indicating that the observed effects were not specific for threat-related stimuli. This stands in contrast to previous studies that examined visual scanpaths over several seconds and found a pattern of visual avoidance of threat (J. Chen et al., Citation2020; N. T. M. Chen & Clarke, Citation2017; but see Högström et al., Citation2019).
Taken together, these results indicate that SAD is associated with impaired processing of faces at an early time stage. As noted in the introduction, SAD is associated with a bias to interpret other people as threatening or overly critical, which leads to avoidance of social interaction. Impaired face processing is likely to increase the risk of social misinterpretation, and could therefore be linked to the maintenance of symptoms, or contribute to the etiology of SAD.
The present study has a number of limitations. Sample sizes were small, although similar to most previous eye tracking studies of adolescent SAD. Thus, replication studies with larger samples are needed before firm conclusions can be drawn. In addition, the high proportion of female participants means that more research is needed to determine if the results generalise to males. Stimuli were presented for a relatively short time (1500 MS). While this is sufficient to examine the first fixation bias, longer presentation times would have been needed to examine other aspects of the scanpath such as the accumulated fixation time at different regions of the face. Future studies should also include participants with a diagnosis of autism as an additional comparison group. Another limitation is that handedness was not formally assessed but only self-reported. As noted in the introduction, the typical age of onset of SAD is in late childhood or adolescence. Recent research has suggested that lateralisation of face processing may be affected by pubertal hormones (Beking et al., Citation2018). An interesting venue for future studies is to examine the LVF bias in SAD in relation to hormonal factors.
To conclude, this study is the first to our knowledge to investigate LVF bias for faces in adolescents with clinically diagnosed SAD. The results suggest that the LVF bias for faces is reduced in adolescents with SAD, and also that this reduction is related to coexisting autistic traits. Together, the findings of this study can contribute to a better understanding of subcomponents of typical and atypical social attention and the underlying mechanisms of SAD.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Additional information
Funding
References
- American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (DSM-5). American Psychiatric Pub.
- Ashwin, C., Wheelwright, S., & Baron-Cohen, S. (2005). Laterality biases to chimeric faces in Asperger syndrome: What is “right” about face-processing? Journal of Autism and Developmental Disorders, 35(2), 183–196. https://doi.org/10.1007/s10803-004-1997-3
- Beidel, D. C., Turner, S. M., & Morris, T. L. (1995). A new inventory to assess childhood social anxiety and phobia: The social Phobia and anxiety Inventory for Children. Psychological Assessment, 7(1), 73–79. https://doi.org/10.1037/1040-3590.7.1.73
- Beking, T., Geuze, R. H., Van Faassen, M., Kema, I. P., Kreukels, B. P. C., & Groothuis, T. G. G. (2018). Prenatal and pubertal testosterone affect brain lateralization. Psychoneuroendocrinology, 88, 78–91. https://doi.org/10.1016/j.psyneuen.2017.10.027
- Bölte, S., Poustka, F., & Constantino, J. N. (2008). Assessing autistic traits: Cross-Cultural validation of the social Responsiveness Scale (SRS). Autism Research, 1, 354–363. https://doi.org/10.1002/aur.49
- Bourne, V. J., & Vladeanu, M. (2011). Lateralisation for processing facial emotion and anxiety: Contrasting state, trait and social anxiety. Neuropsychologia, 49(5), 1343–1349. https://doi:10.1016/J.NEUROPSYCHOLOGIA.2011.02.008
- Bourne, V. J., & Vladeanu, M. (2017). Cognition and emotion Depression or anxiety: Which is best able to predict patterns of lateralisation for the processing of emotional faces? Cognition and Emotion, 31(1), 201–208. https://doi.org/10.1080/02699931.2015.1089841
- Butler, S., Gilchrist, I. D., Burt, D. M., Perrett, D. I., Jones, E., & Harvey, M. (2005). Are the perceptual biases found in chimeric face processing reflected in eye-movement patterns? Neuropsychologia, 43(1), 52–59. https://doi:10.1016/j.neuropsychologia.2004.06.005
- Capriola-Hall, N. N., Wieckowski, A. T., Ollendick, T. H., & White, S. W. (2018). The influence of social Communication Impairments on gaze in adolescents with social anxiety disorder. Child Psychiatry & Human Development, 49(4), 672–679. https://doi.org/10.1007/s10578-018-0782-z
- Carlei, C., Framorando, D., Burra, N., & Kerzel, D. (2017). Visual Cognition face processing is enhanced in the left and upper visual hemi-fields. Visual Cognition, 25(7–8), 749–761. https://doi.org/10.1080/13506285.2017.1327466
- Chen, N. T. M., & Clarke, P. J. F. (2017). Gaze-Based Assessments of Vigilance and avoidance in social anxiety: A review. Current Psychiatry Reports, 19(59),1–9. https://doi.org/10.1007/s11920-017-0808-4
- Chen, N. T. M., Thomas, L. M., Joseph, P., Clarke, F., Hickie, I. B., & Guastella, A. J. (2015). Hyperscanning and avoidance in social anxiety disorder: The visual scanpath during public speaking. Psychiatry Research, 225, 667–672. https://doi.org/10.1016/j.psychres.2014.11.025
- Chen, J., van den Bos, E., & Westenberg, P. M. (2020). A systematic review of visual avoidance of faces in socially anxious individuals: Influence of severity, type of social situation, and development. Journal of Anxiety Disorders, 70, 102193. https://doi.org/10.1016/j.janxdis.2020.102193
- Chita-Tegmark, M. (2016). Social attention in ASD: A review and meta-analysis of eye-tracking studies. Research in Developmental Disabilities, 48, 79–93. https://doi.org/10.1016/j.ridd.2015.10.011
- Cholemkery, H., Mojica, L., Rohrmann, S., Gensthaler, A., & Freitag, C. M. (2014). Can autism spectrum disorders and social anxiety disorders be differentiated by the social responsiveness scale in children and adolescents? Journal of Autism and Developmental Disorders, 44(5), 1168–1182. https://doi.org/10.1007/s10803-013-1979-4
- Constantino, J. N., & Gruber, C. P. (2012). Social responsiven Pess scale (SRS). Torrance, CA: Western Psychological Services. Title. Western Psychological Services.
- Coolican, J., Eskes, G. A., McMullen, P. A., & Lecky, E. (2008). Perceptual biases in processing facial identity and emotion. Brain and Cognition, 66(2), 176–187. https://doi.org/10.1016/j.bandc.2007.07.001
- Dundas, E. M., Best, C. A., Minshew, N. J., & Strauss, M. S. (2012). A Lack of left visual field bias when individuals with autism process faces. Journal of Autism and Developmental Disorders, 42, 1104–1111. https://doi.org/10.1007/s10803-011-1354-2
- Fecteau, J. H., Enns, J. T., & Kingstone, A. (2000). Competition-induced visual field differences in search. Psychological Science, 11(5), 386–393. https://doi.org/10.1111/1467-9280.00275
- Flykt, A., Lundqvist, D., Flykt, A., & Öhman, A. (1998). The Karolinska directed emotional faces (KDEF). CD ROM from Department of Clinical Neuroscience, Psychology Section, Karolinska Institutet.
- Frick, A., Howner, K., Fischer, H., Kristiansson, M., & Furmark, T. (2013). Altered fusiform connectivity during processing of fearful faces in social anxiety disorder. Translational Psychiatry, 3(10), e312–e312. https://doi.org/10.1038/tp.2013.85
- Gentili, C., Cristea, I. A., Angstadt, M., Klumpp, H., Tozzi, L., Phan, L., & Pietrini, P. (2016). Beyond emotions: A meta-analysis of neural response within face processing system in social anxiety. Experimental Biology and Medicine, 241, 225–237. https://doi.org/10.1177/1535370215603514
- Gingnell, M., Frick, A., Engman, J., Alaie, I., Björkstrand, J., Faria, V., & Furmark, T. (2016). Combining escitalopram and cognitive-behavioural therapy for social anxiety disorder: Randomized controlled fMRI trial. British Journal of Psychiatry, 209(3), 229–235. https://doi.org/10.1192/bjp.bp.115.175794
- Guillon, Q., Hadjikhani, N., Baduel, S., Kruck, J., Arnaud, M., & Rogé, B. (2014). Both dog and human faces are explored abnormally by young children with autism spectrum disorders. Neuroreport, 25(15), 1237–1241. https://doi.org/10.1097/WNR.0000000000000257
- Guo, K., Meints, K., Hall, C., Hall, S., & Mills, D. (2009). Left gaze bias in humans, rhesus monkeys and domestic dogs. Animal Cognition, 12(3), 409–418. https://doi.org/10.1007/s10071-008-0199-3
- Guo, K., Smith, C., Powell, K., & Nicholls, K. (2012). Consistent left gaze bias in processing different facial cues. Psychological Research, 76(3), 263–269. https://doi.org/10.1007/s00426-011-0340-9.
- Hadjikhani, N., Zurcher, N. R., Lassalle, A., Hippolyte, L., Ward, N., & Johnels, JÅ. (2017). The effect of constraining eye-contact during dynamic emotional face perception—an fMRI study. Social Cognitive and Affective Neuroscience, 12(7), 1197–1207. https://doi.org/10.1093/scan/nsx046
- Hofmann, S. G. (2007). Cognitive factors that maintain social anxiety disorder: A comprehensive model and its treatment implications. Cognitive Behaviour Therapy, 36(4), 193–209. https://doi.org/10.1080/16506070701421313
- Högström, J., Nordh, M., Larson Lindal, M., Taylor, E., Serlachius, E., & Kleberg, J. L. (2019). Visual attention to emotional faces in adolescents with social anxiety disorder receiving cognitive behavioral therapy. PloS One, 14(11), e0225603. https://doi.org/10.1371/journal.pone.0225603
- Keil, V., Hepach, R., Vierrath, S., Caffier, D., Tuschen-Caffier, B., Klein, C., & Schmitz, J. (2018). Children with social anxiety disorder show blunted pupillary reactivity and altered eye contact processing in response to emotional faces: Insights from pupillometry and eye movements. Journal of Anxiety Disorders, 58, 61–69. https://doi.org/10.1016/j.janxdis.2018.07.001
- Kleberg, J. L., Hanqvist, C., Serlachius, E., & Högström, J. (2019). Pupil dilation to emotional expressions in adolescent social anxiety disorder is related to treatment outcome. Journal of Anxiety Disorders, 65, 26–33. https://doi.org/10.1016/J.JANXDIS.2019.04.006
- Kleberg, J. L., Högström, J., Nord, M., Bölte, S., Serlachius, E., & Falck-Ytter, T. (2017). Autistic traits and symptoms of social anxiety are Differentially related to attention to others’ eyes in social anxiety disorder. Journal of Autism and Developmental Disorders, 47(12), 3814–3821. https://doi.org/10.1007/s10803-016-2978-z
- Lau, J. Y. F., & Waters, A. M. (2017). Annual Research review: An expanded account of information-processing mechanisms in risk for child and adolescent anxiety and depression. Journal of Child Psychology and Psychiatry and Allied Disciplines, 58(4), 387–407. https://doi.org/10.1111/jcpp.12653
- Leonards, U., & Scott-Samuel, N. E. (2005). Idiosyncratic initiation of saccadic face exploration in humans. Vision Research, 45, 2677–2684. https://doi.org/10.1016/j.visres.2005.03.009
- Luh, K. (1998). Effect of inversion on perceptual biases for chimeric faces. Brain and Cognition, 37(1), 105–108.
- Maddox, B. B., & White, S. W. (2015). Comorbid social anxiety disorder in Adults with autism spectrum disorder. Journal of Autism and Developmental Disorders, 45(12), 3949–3960. https://doi.org/10.1007/s10803-015-2531-5
- Nordh, M., Vigerland, S., Öst, L.-G., Ljótsson, B., Mataix-Cols, D., Serlachius, E., & Högström, J. (2017). Therapist-guided internet-delivered cognitive–behavioural therapy supplemented with group exposure sessions for adolescents with social anxiety disorder: A feasibility trial. BMJ Open, 7(12), e018345. https://doi.org/10.1136/bmjopen-2017-018345
- Puleo, C. M., & Kendall, P. C. (2011). Anxiety disorders in typically developing youth: Autism spectrum symptoms as a predictor of cognitive-behavioral treatment. Journal of Autism and Developmental Disorders, 41(3), 275–286. https://doi.org/10.1007/s10803-010-1047-2
- Rapee, R. M., & Heimberg, R. G. (1997). A cognitive-behavioral model of anxiety in social Phobia. Behaviour Research and Therapy, 35(8), 741–756. https://doi.org/10.1016/s0005-7967(97)00022-3
- Rapee, R. M., & Spence, S. H. (2004). The etiology of social phobia: Empirical evidence and an initial model. Clinical Psychology Review, 24(7), 737–767. https://doi.org/10.1016/j.cpr.2004.06.004
- Rossion, B. (2009). Distinguishing the cause and consequence of face inversion: The perceptual field hypothesis. Acta Psychologica, 132, 300–312. https://doi.org/10.1016/j.actpsy.2009.08.002
- Schneier, F. R., Rodebaugh, T. L., Blanco, C., Lewin, H., & Liebowitz, M. R. (2011). Fear and avoidance of eye contact in social anxiety disorder. Comprehensive Psychiatry, 52, 81–87. https://doi.org/10.1016/j.comppsych.2010.04.006
- Senju, A., & Johnson, M. H. (2009). The eye contact effect: Mechanisms and development. Trends in Cognitive Sciences, 13(3), 127–134. https://doi.org/10.1016/j.tics.2008.11.009
- Sheehan, D. V., Sheehan, K. H., Shytle, R. D., Janavs, J., Bannon, Y., Rogers, J. E., … Wilkinson, B. (2010). Reliability and validity of the mini International Neuropsychiatric Interview for Children and adolescents (MINI-KID). The Journal of Clinical Psychiatry, 71(3), 313–326. https://doi.org/10.4088/JCP.09m05305whi
- Simonoff, E., Pickles, A., Charman, T., Chandler, S., Loucas, T., & Baird, G. (2008). Psychiatric disorders in children with autism spectrum disorders: Prevalence, comorbidity, and associated factors in a population-derived sample. Journal of the American Academy of Child and Adolescent Psychiatry, 47(8), 921–929. https://doi.org/10.1097/CHI.0b013e318179964f
- South, M., & Rodgers, J. (2017). Sensory, emotional and cognitive Contributions to anxiety in autism spectrum Disorders. Frontiers in Human Neuroscience, 11, 20. https://doi.org/10.3389/fnhum.2017.00020
- Stein, M. B., Chen, C. Y., Jain, S., Jensen, K. P., He, F., Heeringa, S. G., & Zaslavsky, A. M. (2017). Genetic risk variants for social anxiety. American Journal of Medical Genetics, Part B: Neuropsychiatric Genetics, 174(2), 120–131. https://doi.org/10.1002/ajmg.b.32520
- Van Steensel, F., Bögels, S. M., & Perrin, S.. (2011). Anxiety disorders in children and adolescents with autistic spectrum disorders: A meta-analysis. Clinical Child and Family Psychology Review, 14(3), 302.
- Wechsler, D. (2003). Wechsler intelligence scale for children–fourth edition. The Psychological Corporation
- Wechsler, D. (2008). Wechsler adult intelligence scale–fourth edition. The Psychological Corporation.
- Weeks, J. W., Heimberg, R. G., Rodebaugh, T. L., & Norton, P. J. (2008). Exploring the relationship between fear of positive evaluation and social anxiety. Journal of Anxiety Disorders, 22(3), 386–400. https://doi.org/10.1016/j.janxdis.2007.04.009
- Weeks, J. W., Howell, A. N., & Goldin, P. R. (2013). Gaze avoidance in social anxiety disorder. Depression and Anxiety, 30(8), 749–756. https://doi.org/10.1002/da.22146
- Yoon, K. L., & Zinbarg, R. E. (2008). Interpreting neutral faces as threatening Is a Default Mode for Socially Anxious individuals. Journal of Abnormal Psychology (1965), 117(3), 680–685. https://doi.org/10.1037/0021-843X.117.3.680
- Yovel, G., & Kanwisher, N. (2005). The Neural Basis of the Behavioral Face-Inversion Effect. Current Biology (Vol. 15). https://doi.org/10.1016/j.cub.2005.10.072
- Yovel, G., Tambini, A., & Brandman, T. (2008). The asymmetry of the fusiform face area is a stable individual characteristic that underlies the left-visual-field superiority for faces. Neuropsychologia, 46, 3061–3068. https://doi.org/10.1016/j.neuropsychologia.2008.06.017