
ABSTRACT
Objectives:
Existing scholarship has consistently demonstrated disparities in healthcare experience based on sexual identity. However, relatively little research has considered intersections with race/ethnicity, despite that intersection with other characteristics may complicate healthcare experiences and satisfaction among sexual minorities. This study aims to address such a gap by examining healthcare satisfaction across the intersections of sexual and racial/ethnic identity.
Design:
Utilizing data on U.S. adults included in the 2013–2018 Behavioral Risk Factor Surveillance System (BRFSS) (n = 372,766), we investigate levels of satisfaction with care among a range of groups simultaneously embodying two identities.
Results:
Findings from ordered logistic regression models show that among adults who identify as heterosexual, the odds of reporting high satisfaction with care are lower among Blacks, Asians, and Native Americans. Among sexual minority adults, the likelihood of reporting high satisfaction with care is consistently lower among Native American gay and lesbian adults compared to gays and lesbians of other race/ethnicity or Native American and White heterosexuals, indicating heightened vulnerability to poorer healthcare experience among this multiple minority group.
Conclusion:
While levels of satisfaction with care tend to be generally high across groups, future research should endeavor to investigate the driving factors that lower the odds of high healthcare satisfaction among those with intersecting minority identities.
Introduction
As more than 10 million U.S. adults identify as a sexual minority (Conron and Goldberg Citation2020), understanding their healthcare-related needs and experiences is becoming increasingly important. Studies show that assumptions of heteronormativity and discriminatory experiences in healthcare settings operate as entrenched barriers that lead to heightened levels of dissatisfaction with healthcare (Cant Citation2002) as well as delay or avoidance of care (Malebranche et al. Citation2004) among sexual minorities. Considering the serious health challenges that sexual minorities may experience (IOM Citation2011), examining factors associated with healthcare satisfaction is important in order to improve health care utilization and the efficacy of care received among this vulnerable population.
Existing scholarship has consistently demonstrated disparities in healthcare experience based on sexual identity. This work documents lower levels of satisfaction with care among sexual minorities in comparison to heterosexuals, with a lack of provider knowledge and training as they relate to the health needs of the population identified as the main barrier (IOM Citation2011). For example, lesbian, gay and bisexual adults report lower satisfaction with care even after adjusting for sociodemographic factors (Blosnich Citation2017), and lesbians and bisexual women, in particular, are more likely to be dissatisfied (Avery, Hellman, and Sudderth Citation2001). Importantly, however, while intersection with other characteristics may complicate healthcare experiences and satisfaction among sexual minorities, relatively little research has considered this directly, especially intersections with race/ethnicity. Yet considering race/ethnicity is crucial since prior research shows that racial/ethnic minorities demonstrate lower levels of satisfaction compared to Whites. For example, Blacks and other racial/ethnic minorities display lower post-consultation satisfaction than Whites (Bowling, Rowe, and McKee Citation2013). Asian/Pacific Islanders also report worse experiences with healthcare compared to Whites (Weech-Maldonado et al. Citation2004), as do Hispanics (Lurie et al. Citation2003). Similarly, American Indian/Alaska Natives living in poverty rank among the least satisfied among all racial/ethnic groups (Haviland et al. Citation2005). Altogether, different streams of research document variable healthcare experiences by sexual and racial/ethnic identity, with some work suggesting that individuals who hold both sexual and racial/ethnic minority identities report greater barriers to healthcare access and lower satisfaction (Avery, Hellman, and Sudderth Citation2001; Turpin et al. Citation2021). More research is needed that is inclusive of diverse and understudied population groups, as ‘intersecting axes of power and inequality operate to our collective and individual disadvantage’ (Cho, Crenshaw, and McCall Citation2013, 795).
To that end, we apply an intersectional perspective that allows us to assess how multiple and intersecting social identities shape wellbeing (Collins and Bilge Citation2016; McCall Citation2005), including health status and experience (Bowleg Citation2012, Citation2021). Despite its significance, intersectional approaches to the health status of sexual minorities present methodological challenges due to their small population size (IOM Citation2011). With available data that allows us to address such challenges, however, we examine levels of healthcare satisfaction across the specific intersections of sexual orientation (heterosexual, gay/lesbian, bisexual) and racial/ethnic identity (White, Black, Hispanic, Asian, and Native American). In particular, we construct a measure of intersectionality that reflects the joint and simultaneous embodiment (Bowleg Citation2008) of these two identities, instead of examining them in an additive fashion where each identity is construed as independent and separate. Our perspective on intersectionality is based on the notion that social identities interact through mutually constructive processes and that, accordingly, no single characteristic must be prioritized or layered over another in order to investigate the human experience (Hankivsky Citation2012).
Reflecting this perspective, in this study we examine how the various intersections of sexual and racial/ethnic identity are associated with healthcare satisfaction, drawing on probability-based data of U.S. adults included in the 2013–2018 Behavioral Risk Factor Surveillance System (BRFSS). Our primary aim is to provide a more nuanced understanding of healthcare experience among adults with diverse identities. Specifically, we compare across sexual orientation groups within a particular racial/ethnic identity (e.g. between Black heterosexual and Black bisexual adults) as well as across racial/ethnic identity within a particular sexual orientation (e.g. between White gay/lesbian and Asian gay/lesbian adults). Since the use of intersectionality has mostly occurred in qualitative research (Bauer Citation2014), our quantitative research design is expected to advance the study of intersectional identities and their relationship to health at the population level. Considering research that documents significant health disparities (Wilson and Yoshikawa Citation2007) as well as lower engagement in care (Brenick et al. Citation2017) among sexual minorities of color, our analyses will have implications for public health interventions by providing a useful lens to better understand the nuances of healthcare-related experience among U.S. adults, particularly those with multiple minority identities.
Materials and methods
Data
We draw on data from the Behavioral Risk Factor Surveillance System (BRFSS) from years 2013 to 2018. The BRFSS is a collaborative project between all U.S. states including U.S. territories and the Centers for Disease Control and Prevention (CDC) (https://www.cdc.gov/brfss/index.html). Using a disproportionate stratified sampling design, data were collected via telephone from the non-institutionalized U.S. adult population aged 18 and over. The BRFSS questionnaire is composed of a core component, optional modules, and state-added questions. The core component includes a standard set of questions that all states use that inquire about current health-related perceptions, conditions and behaviors, along with demographic questions. Additional questions can be included through two routes: (1) states may opt to include questions from one of a variety of topical modules available through the national BRFSS, and (2) states may ask questions they write themselves.
BRFSS has been asking about healthcare satisfaction since 2013, with the exception of 2015 when the question was not asked. For the present analyses, we merged data from 29 states that included a sexual orientation question on their questionnaire, and also queried about healthcare satisfaction, at any point between 2013 and 2018. Our analytic sample includes 53 state-years of data (see ) and n = 372,766 observations with valid information on racial/ethnic identity, sexual orientation, and healthcare satisfaction.
Table 1. Interview states and years.
Measures
Our dependent variable is healthcare satisfaction. It was originally asked in the questionnaire as ‘In general, how satisfied are you with the healthcare you received?’, inquiring about respondents’ experience in the past 12 months. Respondents could choose 1 ‘very satisfied’ 2 ‘somewhat satisfied’ and 3 ‘not at all satisfied.’ Responses were reverse coded so that higher values indicated greater satisfaction with healthcare.
Our independent variable of interest is a combined measure of race/ethnicity and sexual orientation that reflects our emphasis on the joint and simultaneous nature of intersectional identity (Bowleg Citation2008). First, race/ethnicity measures whether a respondent identifies as White, Black, Hispanic, Asian, or Native American. Respondents were first able to identify as Hispanic to the question that asked ‘Are you Hispanic, Latino/a, or Spanish origin?’ Then to the following question that asked ‘Which one or more of the following would you say is your race?’, respondents could identify as White, Black, Asian, or Native American (American Indian or Alaska Native). Respondents who identified as Pacific Islander, other, did not know, or refused to answer were excluded from the analytic sample because of their small size in our sample or the lack of specificity on their identity. Second, sexual orientation measures whether a respondent identifies as heterosexual, gay or lesbian, or bisexual. Although exact wording varies slightly by state and year, it was most often asked as ‘Do you consider yourself to be: (1) heterosexual/straight, (2) lesbian or gay, (3) bisexual?’ Some respondents identified as other, did not know, or refused to answer, and these cases were excluded from the analytic sample. Based on these two measures, our analytic sample is composed of 298,957 White heterosexuals, 4,601 White gays/lesbians, 3,730 White bisexuals, 25,761 Black heterosexuals, 349 Black gays/lesbians, 394 Black bisexuals, 25,182 Hispanic heterosexuals, 435 Hispanic gays/lesbians, 432 Hispanic bisexuals, 4,777 Asian heterosexuals, 81 Asian gays/lesbians, 90 Asian bisexuals, 7,742 Native American heterosexuals, 102 Native American gays/lesbians, and 133 Native American bisexuals (see ).
Table 2. Weighted sample characteristics, by race/ethnicity and sexual orientation (n = 372,766).
In order to document more accurate patterns of healthcare satisfaction across the intersections of sexual and racial/ethnic identity, we rely on Andersen’s theoretical model of healthcare access and utilization (Andersen Citation1968, Citation1995) to adjust for a variety of factors that may confound the association. Specifically, we organize our control measures into three groups. First, predisposing characteristics include demographic and social structural factors that may influence an individual’s use of health services, such as age, gender, education and occupation. In our models, we account for age at interview, gender (1 = female, 0 = male), marital status (1 = married/unmarried couple, 0 = formerly/never married), number of children in the household (range from 0-5+), education level (1 = high school or less, 2 = some college, 3 = college or more), and employment status (1 = employed for wages or self-employed, 0 = out of work, homemaker, student, retired, or unable to work).
Second, enabling resources refer to a set of means that make available or facilitate the use of health services, such as income, insurance and regular source of care (e.g. personal doctor). To account for enabling resources, we include annual household income (1 = less than $25,000, 0 = $25,000 or more), having ever missed medical care due to cost in the past 12 months (1 = yes, 0 = no), insurance status (1 = insured, 0 = not insured), and whether or not the respondent has a personal doctor (1 = yes, 0 = no).
Finally, perceived need for care relates to an individual’s perception of general health status or specific conditions in need of professional care. Our measures of perceived need for care include current smoking (1 = yes, 0 = no), heavy drinking (1 = heavy drinker [defined as eight or more drinks per week for women and fifteen or more drinks per week for men], 0 = all less), overweight or obesity (1 = overweight or obese, 0 = all less), and number of chronic medical conditions (range from 0-6, among asthma, diabetes, stroke, heart attack, angina or coronary heart disease, and cancer).
Analysis
All analyses were conducted using Stata 15.0. Using ordered logistic regression predicting healthcare satisfaction (where high values = greater satisfaction), we present a series of models starting from the baseline model that includes only the combined measure of race/ethnicity and sexual orientation, as well as age (Model 1). Following, in Model 2 we add the other predisposing characteristics, and in Model 3 we add enabling resources. In the fully adjusted model, we account for all predisposing characteristics, enabling resources, and need-based characteristics (Model 4). All analyses control for state and interview year and are weighted to account for multiple state-years of data, and all missing data have been multiply imputed using chained equations in Stata.Footnote1
Results
Sample characteristics
presents weighted sample characteristics by race/ethnicity and sexual orientation. We first find that while respondents are generally satisfied with the care they received, White heterosexuals exhibit the highest proportion of those who report being very satisfied (67%), followed by White gays and lesbians (64%). This compares to a substantially lower proportion reporting that they are very satisfied with care received among Native American gays and lesbians (26%), and more intermediate rates among Asian bisexuals (45%) and Hispanic bisexuals (47%). Among Whites and Hispanics, we find that heterosexuals display the highest proportion of those who are very satisfied, and that for Blacks and Native Americans, the rates are on par with bisexuals. Among Asians, gays and lesbians report the highest rate of being very satisfied.
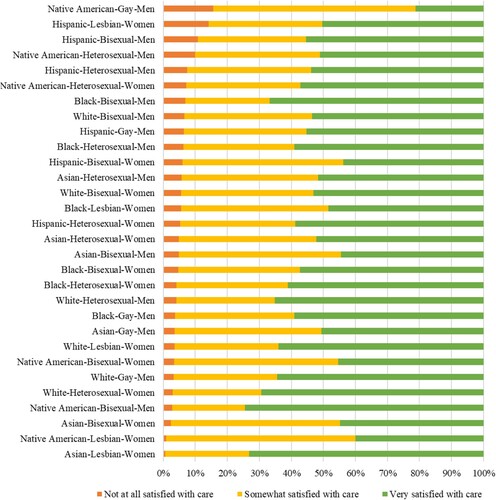
To facilitate more detailed comparison across subgroups by race/ethnicity, sexual orientation and gender, we visualized relative proportions of levels of satisfaction for each subgroup (see ). We find that Native American gay men exhibit the highest rate of being not at all satisfied (15.5%), and that they also display the lowest rate of being very satisfied (21.2%), with a majority being somewhat satisfied. Native American gay men are thus distinctive compared to other subgroups among whom much higher rates of being very satisfied are identified. They are closely followed by Hispanic lesbian women (14.2% not at all satisfied) and Hispanic bisexual men (10.9% not at all satisfied), as well as Native American and Hispanic heterosexual men (10% and 7.4% not at all satisfied, respectively) who also rank among the groups with high rates of being not at all satisfied.
Figure 1. Healthcare satisfaction (percentage) by race/ethnicity, sexual orientation and gender.
Predisposing characteristics reveal that across racial/ethnic groups, bisexuals are the youngest in the group while heterosexuals are the oldest, with gays and lesbians in the middle. On average, White and Black respondents tend to be older than Hispanic and Asian respondents, with Native American respondents in between. Marital status is consistently dependent on sexual orientation within each racial/ethnic group, with heterosexuals reporting the greatest proportion of those who are married or unmarried couple. In terms of education level, Asian heterosexuals display the greatest proportion of those with at least a college degree (51%), whereas a much lower proportion of Black bisexuals and Native Americans report a college degree. Across racial/ethnic groups in general, employment rates are lower among bisexuals; the only exception is among Native Americans, where employment is lowest among heterosexuals.
As for enabling resources, we find that bisexuals in each racial/ethnic group report greater prevalence of poverty compared to heterosexuals and gay/lesbian adults. In terms of having missed care due to cost in the past 12 months, Hispanic bisexuals stand out with 32% reporting such experience. Hispanics, regardless of sexual orientation, also have lowest levels of insurance coverage. As to having a personal doctor, in general, White respondents report higher proportions of having a personal doctor than respondents from other racial/ethnic groups. Within each racial/ethnic group, the proportion of having a personal doctor is lowest among bisexuals (on par with heterosexuals among Native Americans), with the exception of Hispanics and Asians.
Need-based characteristics show that across racial/ethnic groups, current smoking is more frequent among sexual minorities than among heterosexuals. Except for Asians, the proportion of current smoking is greater among gays, lesbians and bisexuals than among heterosexuals within each racial/ethnic group. Similarly, heavy drinking is more frequent among sexual minorities than among heterosexuals, regardless of race/ethnicity. In contrast, overweight or obesity tends to be more prevalent among heterosexuals in each racial/ethnic group, except for Native Americans among whom gays and lesbians actually have the highest prevalence. In terms of chronic conditions, Asians, regardless of sexual orientation, report fewer conditions compared to other racial/ethnic groups.
Ordered logistic regression models predicting healthcare satisfaction
displays odds ratios from ordered logistic regression models predicting healthcare satisfaction. In the baseline model adjusting only for the combined measure of race/ethnicity and sexual orientation and age, we find that various groups across race/ethnicity and sexual orientation report significantly lower odds of higher satisfaction than White heterosexuals. White bisexuals have 32% lower odds of reporting higher satisfaction compared to White heterosexuals (p < .001), and Black heterosexuals have 22% lower odds (p < .001). Hispanics, regardless of sexual orientation, exhibit significantly lower odds of reporting higher satisfaction than White heterosexuals. Asian heterosexuals and bisexuals, likewise, display lower odds of higher satisfaction compared to White heterosexuals. While Native American heterosexuals, gays and lesbians all report lower odds of higher satisfaction than White heterosexuals, it is particularly notable among gays and lesbians. Native American gays and lesbians report specifically 74% lower odds of higher satisfaction compared to White heterosexuals (p < .001).
Table 3. Odds ratios from ordered logistic regression models predicting healthcare satisfaction (n = 372,766).
After adding the other predisposing characteristics in Model 2, we find that the previously significant association for Hispanic gays and lesbians becomes non-significant, and it results in a slight increase in the odds ratios for all groups, except for White bisexuals and Asian heterosexuals and bisexuals. Age remains a significant predictor positively associated with healthcare satisfaction, and women have 16% greater odds of reporting higher satisfaction than men (p < .001). We also find that married or unmarried couples have about 13% greater odds of reporting higher satisfaction compared to those who are formerly or never married (p < .001). While an additional child in the household and being employed are both negatively associated with healthcare satisfaction, higher levels of education are positively associated with healthcare satisfaction. Those with some college-level of education have 9% greater odds of reporting higher satisfaction than their counterparts with high school or less level of education, and those with college or more level of education have 40% greater odds (both differences are significant at p < .001).
Accounting for enabling resources in Model 3, we see that all Hispanic groups and Asian bisexuals no longer exhibit significantly different associations with healthcare satisfaction compared to White heterosexuals. This implies that material resources such as income and insurance may be particularly significant predictors of healthcare satisfaction among these groups, regardless of sexual orientation. While age and gender consistently remain positively associated with healthcare satisfaction, we now find that married or unmarried couples do not differ in their odds of reporting greater satisfaction from those who are formerly or never married. Having an additional child in the household is still significantly associated with healthcare satisfaction, whereas having some college-level of education has lost its significance. However, having college or more level of education is still positively associated with healthcare satisfaction (OR = 1.16, p < .001). Accounting for enabling resources has strengthened the previously negative relationship between employment status and healthcare satisfaction, in a way that those who are employed now have 11% lower odds of reporting higher satisfaction than those who are unemployed or out of the workforce (p < .001). Newly added enabling resources exhibit relationships in expected directions, such that having an annual household income below $25,000 and having missed care due to cost in the past 12 months are associated with reduced odds of reporting higher satisfaction, whereas being insured and having a personal doctor are associated with increased odds (all significant at p < .001).
In our fully adjusted model with the addition of need-based characteristics, we find that White and Asian bisexuals, as well as Native American gays and lesbians, have significantly lower odds of reporting higher satisfaction than White heterosexuals. With the exception of Hispanics, all heterosexuals from racial/ethnic minority groups continue to have significantly lower odds of reporting higher satisfaction compared to White heterosexuals. Black heterosexuals have 11%, Native Americans have 23%, and Asians have 43% lower odds of reporting higher satisfaction than White heterosexuals (all significant at p < .001). As to need-based characteristics, we find that those who currently smoke have 24% lower odds of reporting higher satisfaction than those who do not smoke (p < .001), and that heavy drinkers report significantly lower odds of higher satisfaction than those who drink less. Those who are overweight or obese likewise report significantly lower odds of higher satisfaction than those of healthy weight, and additional number of chronic conditions is associated with 8% lower odds of reporting higher satisfaction (all significant at p < .001).
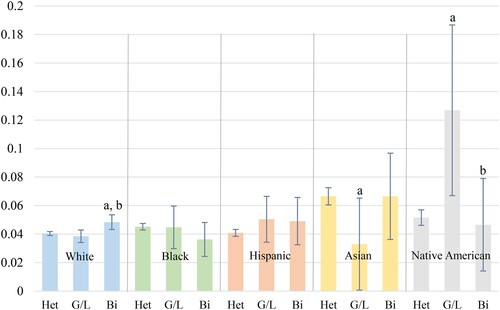
To facilitate comparison across groups, we visualized our regression findings by generating predicted probabilities from the fully adjusted model in . When we first look at differences by sexual orientation within each racial/ethnic group (see ), we see the distinctive status of Native American gay and lesbian adults, who experience a significantly elevated probability of being not at all satisfied with care received. White bisexuals also report greater likelihood of being not at all satisfied compared to both their heterosexual and gay/lesbian counterparts. On the other hand, Asian gays and lesbians are less likely to be not at all satisfied with care received than Asian heterosexuals, as do Native American bisexuals compared to Native American gays and lesbians.
Figure 2. Adjusted Predicted Probabilities and 95% CIs for Lowest Satisfaction by Race/ethnicity.
Note: (1) Letters indicate significant pairwise comparison (all at p<.05) across sexual orientation groups; a = heterosexual, b = gay/lesbian, c = bisexual. (2) Heterosexual, gay and lesbian, and bisexual respondents are abbreviated as ‘Het’, ‘G/L’, and ‘Bi’, respectively, due to spatial limitation.
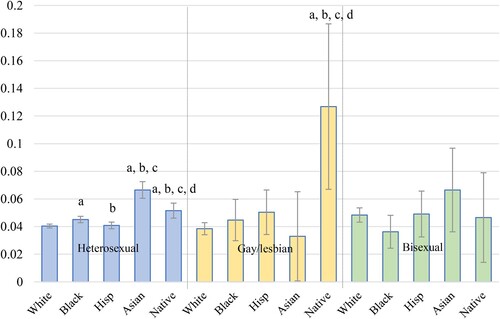
When we then look across racial/ethnic groups by sexual orientation (see ), we find that among heterosexuals, Asian adults report a significantly higher probability of being not at all satisfied compared to heterosexuals in all other racial/ethnic groups. Black heterosexuals similarly show greater likelihood of being not at all satisfied with care received than White heterosexuals. Among gays and lesbians, the status of Native Americans is again distinctive, with higher likelihood of being not at all satisfied than all other racial/ethnic groups. These findings imply that the intersection of marginal identities renders Native Americans who identify as gay or lesbian particularly vulnerable to having a poor healthcare experience, while Asians also experience elevated dissatisfaction with care, but only among heterosexuals.
Figure 3. Adjusted Predicted Probabilities and 95% CIs for Lowest Satisfaction by Sexual Orientation.
Note: (1) Letters indicate significant pairwise comparison (all at p < .05) across racial/ethnic groups; a = white, b = black, c = Hispanic, d = Asian. (2) Hispanic and Native American respondents are abbreviated as ‘Hisp’ and ‘Native’, respectively, due to spatial limitation.
Discussion
The sexual minority population in the U.S. is on the rise. From 3.5% in 2012, the population has steadily increased to a record 4.5% in 2017 (Gallup News, May 22, 2018). This increase is heavily driven by a cohort of millennials born between 1980 and 1999, among whom the proportion of those who identify as LGBT has continuously increased from 5.8% in 2012 to 7.3% in 2016, and 8.1% in 2017 (Gallup News, May 22, 2018). As more young adults are identifying as a sexual minority, investigating the care-related experiences and needs of this population will become increasingly important for public health knowledge. In light of such significance, our study examined healthcare satisfaction from an intersectional perspective that considers both sexual orientation and race/ethnicity.
Findings first revealed that heterosexuals from all racial/ethnic minority groups, Hispanic and Native American gays and lesbians, and White, Hispanic, and Asian bisexuals have lower odds of greater satisfaction than White heterosexuals, adjusting for age. With addition of other predisposing characteristics and enabling resources, however, significant differences for all Hispanic groups relative to White heterosexuals became non-significant. This indicates that acquiring resources such as health insurance or income sufficient enough to facilitate care may be particularly meaningful in predicting healthcare satisfaction among these groups, as existing research has confirmed (Cabrera-Barona, Blaschke, and Kienberger Citation2017; ). Hispanics on average report considerable levels of poverty and employment in unskilled, high-risk work (Velasco-Mondragon et al. Citation2016), as well as greater risk of being uninsured, lacking a regular source of care, or even forgoing care because of cost compared to Whites (Callahan, Gerald, and Cooper Citation2006; Durden and Hummer Citation2006; Gary et al. Citation2003; Weaver et al. Citation2010). As such, the importance of acquiring these material resources that grant initial access to healthcare seems to outweigh finer disparities by sexual orientation, as our models showed that once we adjust for systematic differences across groups based on predisposing characteristics and enabling resources, healthcare experience of Hispanics does not differ significantly from that of White heterosexuals.
In our fully-adjusted model, all groups of heterosexuals (except for Hispanics) reported lower odds of greater satisfaction than White heterosexuals. This implies that racial/ethnic disparities in healthcare satisfaction manifest most clearly among heterosexuals. It may be that other identities become more salient (Stryker Citation1980) for heterosexuals who do not experience negative attitudes or discrimination in healthcare settings based on sexual orientation (Malebranche et al. Citation2004) as do sexual minorities. The fact that Asian heterosexuals stood out as reporting the greatest likelihood of being not at all satisfied among heterosexuals implies that this group may be either holding different evaluation tendencies (Liao et al. Citation2020; Saha and Hickam Citation2003) or experiencing greater barriers to satisfactory healthcare such as heightened levels of discrimination (Harris, Cormack, and Stanley Citation2019) that call for public attention.
As to lower odds of greater satisfaction that surfaced among White and Asian bisexuals, this finding is interesting because they are not particularly disadvantaged in terms of their demographic, socioeconomic or health-specific conditions. In fact, other sexual minorities who fare worse than these two groups do not differ in their levels of healthcare satisfaction from White heterosexuals. Thus, we speculate that other facets of healthcare that we were unable to account for in our analysis may have contributed to such outcome. For instance, when disclosing their sexual identity, bisexuals face unique barriers like monosexism, heightened heteronormative expectations, and assumptions of promiscuity (Scherrer, Kazyak, and Schmitz Citation2015). It may be that these barriers underlie their lower likelihood for outness but higher likelihood for self-presentation in a different sexual identity when compared to gays and lesbians (Mohr, Jackson, and Sheets Citation2017). Such experiences may further result in greater sense of discrepancy and unmet medical needs among bisexuals, particularly among those who are White or Asian for whom sexual minority identity can have greater implications than their other characteristics.
Finally, the status of Native American gays and lesbians calls for attention. This group reported the greatest likelihood of being not at all satisfied with their healthcare when compared either to White and Native American heterosexuals or gays and lesbians from other racial/ethnic groups. This signals that the intersection of sexual and racial/ethnic minority identity relegates Native American gays and lesbians to experience the least satisfactory healthcare settings in comparison to other diverse groups. As shown in , Native American gay men exhibit a greater proportion of those who are not at all satisfied (15.5% vs. 0.8%) but smaller proportion of those very satisfied (21.2% vs. 40.0%) than Native American lesbians, suggesting that gender may be shaping this finding in important ways. In general, gays and lesbians are more likely to disclose their sexual identity than other sexual minorities (Durso and Meyer Citation2013; Mohr, Jackson, and Sheets Citation2017), but at the same time scholarship shows that gay men tend to be less socially accepted than lesbians (Bettinsoli, Suppes, and Napier Citation2020). Unfortunately, being out can be strongly associated with negative evaluations by others (Zaikman, Stimatze, and Zeiber Citation2020) as well as less positive emotional outcomes (Legate, Ryan, and Weinstein Citation2012), particularly under homonegative and oppressive environments.
Findings for Native American gays and lesbians may also be understood as reflecting such sociocultural context. It is important to note that historically, eradication of homosexuality constituted an essential part of European colonization, and that negative attitudes penetrated reservations over time and induced many Native American communities to suppress gender diversity and homosexuality for the sake of acculturation (Balsam et al. Citation2004; Lang Citation2016). Indeed, colonization plays an impactful and nefarious role in the health of gay and lesbian Native Americans, as Evans-Campbell et al. (Citation2012) find among their sample of urban two-spirit elders (note: two-spirit is a broad term for Native Americans who identify as gay, lesbian, bisexual, and/or transgender), those who attended Indian boarding school or were raised by a boarding school attendee had elevated rates of mental health and substance use disorders. Chae and Walters (Citation2009) find that higher levels of discrimination among two-spirit Native American persons are associated with higher levels of physical pain and impairment – but that the likelihood of poorer self-rated health outcomes is mitigated when two-spirit individuals have higher levels of actualizing characteristics (i.e. are ‘proud to be Indian’). These findings underscore the continued health relevance of colonization, suggesting that gay and lesbian Native Americans, and especially gay men, are less satisfied with their health care as they face homophobia within their Native communities (homophobia which is introduced via colonization) and racism among the gender and sexual minority communities (Fieland, Walters, and Simoni Citation2007). Thus, the unique contexts under which Native American sexual minorities find themselves may influence their less satisfactory interactions with the healthcare system, especially among gays and lesbians who tend to be more out and stigmatized for being so.
While we have identified significant disparities in relation to healthcare satisfaction among a range of groups located at the intersections of sexual and racial/ethnic identity, our study has its limitations. Although we relied on a systematic model of health services use to examine the factors that are associated with healthcare satisfaction, the models of our study are not exhaustive and have yet to include other important psychosocial aspects. Indeed, even after adjustment for an array of predisposing, enabling, and need-based characteristics, our models showed significant disparities in healthcare satisfaction across the intersections of sexual and racial/ethnic identity. To further examine the drivers of healthcare-related experience including satisfaction, psychosocial measurements - among others - that make it available to evaluate the sociocultural climate in healthcare settings, especially interpersonal interaction with healthcare providers (Lykens, LeBlanc, and Bockting Citation2018), must be developed and incorporated into data and analysis. This is because perceived relationship with healthcare providers has been verified to affect satisfaction with care the most (Raposo, Alves, and Duarte Citation2009), especially among sexual and racial/ethnic minorities (Mosack, Brouwer, and Petroll Citation2013; Nápoles et al. Citation2009; Weech-Maldonado et al. Citation2004). Thus, from a perspective in which healthcare satisfaction is understood as a multidimensional construct (Naidu Citation2009) that is impacted not only by instrumental but also by psychosocial dimensions, incorporating necessary measurements to reflect such multidimensionality merits considerable attention. Future research with available measurements should consider incorporation of such factors when examining satisfaction with care. In addition, our study relied on a cross-sectional design, which only enabled us to investigate the patterns, or associations, relevant to healthcare satisfaction. In order to examine the successive processes whereby certain factors may or may not continue to have influence on satisfaction with care over time, future research should employ a longitudinal design and track such change.
Nevertheless, our study contributes to existing literature on healthcare satisfaction, most importantly through our emphasis on intersectionality – whereby identities are jointly embodied and experienced – that exposes elaborate patterns of inequality in satisfaction. While we found little difference among Whites, Blacks and Hispanics, our findings for Asians and Native Americans provide important insights that may potentially advance understanding of healthcare satisfaction at the intersections of sexual orientation and race/ethnicity. Public health intervention efforts aimed at enhancing satisfaction with care should endeavor to develop more elaborate measurements of satisfaction as well as invest in promoting a culturally competent healthcare environment, especially for populations who may occupy more than one minority identity. In particular, developing curricula or training courses for healthcare providers tailored to the unique needs of targeted subpopulations may lead to improved ratings of healthcare in the long run. As highlighted in , substantial difference exists in perceptions of the healthcare experience across the intersections of race/ethnicity, sexual orientation and gender. As such, participatory approaches that focus on better understanding the feelings and perceptions among communities reporting the lowest satisfaction (e.g. Native American gay men) may be especially useful for identifying effective intervention efforts.
Acknowledgements
The authors thank the Centers for Disease Control and Prevention (CDC) for Behavioral Risk Factor Surveillance System survey data, Atlanta, Georgia: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, 2013–2018; Alaska BRFSS Program; Tomassilli, J. C. & Morris, J. C. California Behavioral Risk Factor Surveillance System (BRFSS) SAS Dataset Documentation and Technical Report: 1984-2018: Public Health Survey Research Program, California State University, Sacramento, 2018; the Idaho Department of Health and Welfare BRFSS program; BRFSS staff in Massachusetts; the Michigan Department of Health and Human Services; Montana BRFSS 2013–2014 office; New Mexico BRFSS office; North Carolina BRFSS office; Ohio BRFSS office; Oregon BRFSS office; Rhode Island Behavioral Risk Factor Surveillance System, 2013–2014 Center for Health Data and Analysis, Rhode Island Department of Health, and supported in part by the National Center for Chronic Disease Prevention and Health Promotion, Centers for Disease Control and Prevention Cooperative Agreement Number, U58 DP006067; Office of Public Health Assessment, Utah Behavioral Risk Factor Surveillance System Survey Data, Salt Lake City, UT: Utah Department of Health, 2013-2014; the Washington State BRFSS program, and the Wisconsin BRFSS program.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Data availability statement
Behavioral Risk Factor Surveillance System survey data are available from the Centers for Disease Control and Prevention (CDC), Atlanta, Georgia: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention (https://www.cdc.gov/brfss/index.html).
Additional information
Funding
Notes
1 The percentage of missing observations for most variables is low (under 3%), with two exceptions: annual household income (12.46%) and overweight/obesity (4.91%).
References
- Andersen, Ronald M. 1968. “Behavioral Model of Families’ Use of Health Services.” Research Series No.25. Chicago, IL: Center for Health Administration Studies, University of Chicago.
- Andersen, Ronald M. 1995. “Revisiting the Behavioral Model and Access to Medical Care: Does it Matter?” Journal of Health and Social Behavior 36 (March): 1–10.
- Avery, Anna M., Ronald E. Hellman, and Lori K. Sudderth. 2001. “Satisfaction with Mental Health Services among Sexual Minorities with Major Mental Illness.” American Journal of Public Health 91 (6): 990–991.
- Balsam, Kimberly F., Bu Huang, Karen C. Fieland, Jane M. Simoni, and Karina L. Walters. 2004. “Culture, Trauma, and Wellness: A Comparison of Heterosexual and Lesbian, Gay, Bisexual, and Two-Spirit Native Americans.” Cultural Diversity and Ethnic Minority Psychology 10 (3): 287–301.
- Bauer, Greta R. 2014. “Incorporating Intersectionality Theory Into Population Health Research Methodology: Challenges and the Potential to Advance Health Equity.” Social Science & Medicine 110: 10–17.
- Bettinsoli, Maria Laura, Alexandra Suppes, and Jaime L. Napier. 2020. “Predictors of Attitudes Toward Gay Men and Lesbian Women in 23 Countries.” Social Psychological and Personality Science XX (X): 1–12.
- Blosnich, John R. 2017. “Sexual Orientation Differences in Satisfaction with Healthcare: Findings from the Behavioral Risk Factor Surveillance System, 2014.” LGBT Health 4 (3): 227–231.
- Bowleg, Lisa. 2008. “When Black + Lesbian + Woman ≠ Black Lesbian Woman: The Methodological Challenges of Qualitative and Quantitative Intersectionality Research.” Sex Roles 59: 312–325.
- Bowleg, Lisa. 2012. “The Problem with the Phrase Women and Minorities: Intersectionality—An Important Theoretical Framework for Public Health.” American Journal of Public Health 102 (7): 1267–1273.
- Bowleg, Lisa. 2021. “Evolving Intersectionality Within Public Health: From Analysis to Action.” American Journal of Public Health 111 (1): 88–90.
- Bowling, Ann, Gene Rowe, and Martin McKee. 2013. “Patients’ Experiences of Their Healthcare in Relation to Their Expectations and Satisfaction: A Population Survey.” Journal of the Royal Society of Medicine 106: 143–149.
- Brenick, Alaina, Kelly Romano, Christopher Kegler, and Lisa A. Eaton. 2017. “Understanding the Influence of Stigma and Medical Mistrust on Engagement in Routine Healthcare among Black Women Who Have Sex with Women.” LGBT Health 4 (1): 4–10.
- Cabrera-Barona, Pablo, Thomas Blaschke, and Stefan Kienberger. 2017. “Explaining Accessibility and Satisfaction Related to Healthcare: A Mixed-Methods Approach.” Social Indicators Research 133: 719–739.
- Callahan, S. Todd, B. Hickson Gerald, and William O. Cooper. 2006. “Health Care Access of Hispanic Young Adults in the United States.” Journal of Adolescent Health 39: 627–633.
- Cant, Bob. 2002. “An Exploration of the Views of Gay and Bisexual Men in One London Borough of Both Their Primary Care Needs and the Practice of Primary Care Practitioners.” Primary Health Care Research and Development 3: 124–130.
- Chae, David H., and Karina L. Walters. 2009. “Racial Discrimination and Racial Identity Attitudes in Relation to Self-Rated Health and Physical Pain and Impairment among Two-Spirit American Indians/Alaska Natives.” American Journal of Public Health 99 (S1): S144–S151.
- Cho, Sumi, Kimberlé Williams Crenshaw, and Leslie McCall. 2013. “Toward a Field of Intersectionality Studies: Theory, Applications, and Praxis.” Signs: Journal of Women in Culture and Society 38 (4): 785–810.
- Collins, Patricia H., and Sirma Bilge. 2016. Intersectionality. Hoboken, NJ: John Wiley & Sons.
- Conron, Kerith J., and Shoshana K. Goldberg. 2020. Adult LGBT Population in the United States. Los Angeles, CA: The Williams Institute, UCLA.
- Durden, T. Elizabeth, and Robert A. Hummer. 2006. “Access to Healthcare among Working-Aged Hispanic Adults in the United States.” Social Science Quarterly 87 (5): 1319–1343.
- Durso, Laura E., and Ilan H. Meyer. 2013. “Patterns and Predictors of Disclosure of Sexual Orientation to Healthcare Providers among Lesbians, Gay Men, and Bisexuals.” Sexuality Research and Social Policy 10 (1): 35–42.
- Evans-Campbell, Teresa, Karina L. Walters, Cynthia R. Pearson, and Christopher D. Campbell. 2012. “Indian Boarding School Experience, Substance Use, and Mental Health among Urban Two-Spirit American Indian/Alaska Natives.” American Journal of Drug and Alcohol Abuse 38 (5): 421–427.
- Fieland, Karen C., Karina L. Walters, and Jane M. Simoni. 2007. “Determinants of Health AmongTwo-Spirit American Indians and Alaska Natives.” In The Health of Sexual Minorities: Public Health Perspectives on Lesbian, Gay, Bisexual, and Transgender Populations, edited by I. H. Meyer, and M. E. Northridge, 268–300. Boston: Springer.
- Gary, Tiffany L., K. M. Venkat Narayan, Edward W. Gregg, Gloria L. A. Beckles, and Jinan B. Saaddine. 2003. “Racial/Ethnic Differences in the Healthcare Experience (Coverage, Utilization, and Satisfaction) of US Adults with Diabetes.” Ethnicity & Disease 13: 47–54.
- Hankivsky, Olena. 2012. “Women’s Health, Men’s Health, and Gender and Health: Implications of Intersectionality.” Social Science & Medicine 74 (11): 1712–1720.
- Harris, Ricci B., Donna M. Cormack, and James Stanley. 2019. “Experience of Racism and Associations with Unmet Need and Healthcare Satisfaction: The 2011/12 Adult New Zealand Health Survey.” Australian and New Zealand Journal of Public Health 43 (1): 75–80.
- Haviland, Mark G., Leo S. Morales, Thomas H. Dial, and Harold Alan Pincus. 2005. “Race/Ethnicity, Socioeconomic Status, and Satisfaction with Health Care.” American Journal of Medical Quality 20 (4): 195–203.
- Institute of Medicine (IOM). 2011. The Health of Lesbian, Gay, Bisexual, and Transgender People: Building a Foundation for Better Understanding. Washington, DC: National Academies Press.
- Lang, Sabine. 2016. “Native American Men-Women, Lesbians, Two-Spirits: Contemporary and Historical Perspectives.” Journal of Lesbian Studies 20 (3-4): 299–323.
- Legate, Nicole, Richard M. Ryan, and Netta Weinstein. 2012. “Is Coming Out Always a ‘‘Good Thing’’? Exploring the Relations of Autonomy Support, Outness, and Wellness for Lesbian, Gay, and Bisexual Individuals.” Social Psychological and Personality Science 3 (2): 145–152.
- Liao, Lillian, Sukyung Chung, Jonathan Altamirano, Luis Garcia, Magali Fassiotto, Bonnie Maldonado, Paul Heidenreich, and Latha Palaniappan. 2020. “The Association Between Asian Patient Race/Ethnicity and Lower Satisfaction Scores.” BMC Health Services Research 20: 678.
- Lurie, Nicole, Chunliu Zhan, Judith Sangl, Arlene S. Bierman, and Edward S. Sekscenski. 2003. “Variation in Racial and Ethnic Differences in Consumer Assessments of Health Care.” American Journal of Managed Care 9 (7): 502–509.
- Lykens, James E., Allen J. LeBlanc, and Walter O. Bockting. 2018. “Healthcare Experiences among Young Adults Who Identify as Genderqueer or Nonbinary.” LGBT Health 5 (3): 191–196.
- Malebranche, David J., John L. Peterson, Robert E. Fullilove, and Richard W. Stackhouse. 2004. “Race and Sexual Identity: Perceptions About Medical Culture and Healthcare among Black Men Who Have Sex with Men.” Journal of the National Medical Association 96 (1): 97–107.
- McCall, Leslie. 2005. “The Complexity of Intersectionality.” Signs: Journal of Women in Culture and Society 30 (3): 1771–1800.
- Mohr, Jonathan J., Skyler D. Jackson, and Raymond L. Sheets. 2017. “Sexual Orientation Self-Presentation among Bisexual-Identified Women and Men: Patterns and Predictors.” Archives of Sexual Behavior 46: 1465–1479.
- Mosack, Katie E., Amanda M. Brouwer, and Andrew E. Petroll. 2013. “Sexual Identity, Identity Disclosure, and Health Care Experiences: Is There Evidence for Differential Homophobia in Primary Care Practice?” Women’s Health Issues 23 (6): e341–e346.
- Naidu, Aditi. 2009. “Factors Affecting Patient Satisfaction and Healthcare Quality.” International Journal of Health Care Quality Assurance 22 (4): 366–381.
- Nápoles, Anna María, Steven E. Gregorich, Jasmine Santoyo-Olsson, Helen O’Brien, and Anita L. Stewart. 2009. “Interpersonal Processes of Care and Patient Satisfaction: Do Associations Differ by Race, Ethnicity, and Language?” Health Research and Educational Trust 44 (4): 1326–1344.
- Raposo, Mário L., Helena M. Alves, and Paulo A. Duarte. 2009. “Dimensions of Service Quality and Satisfaction in Healthcare: A Patient’s Satisfaction Index.” Service Business 3: 85–100.
- Saha, Somnath, and David H. Hickam. 2003. “Explaining Low Ratings of Patient Satisfaction among Asian-Americans.” American Journal of Medical Quality 18 (6): 256–264.
- Scherrer, Kristin S., Emily Kazyak, and Rachel Schmitz. 2015. “Getting “Bi” in the Family: Bisexual People’s Disclosure Experiences.” Journal of Marriage and Family 77: 680–696.
- Stryker, Sheldon. 1980. Symbolic Interactionism: A Social Structural Version. Menlo Park, CA: Benjamin/Cummings.
- Turpin, Rodman E., Ellesse-Roselee L. Akré, Natasha D. Williams, Bradley O. Boekeloo, and Jessica N. Fish. 2021. “Differences in Health Care Access and Satisfaction Across Intersections of Race/Ethnicity and Sexual Identity.” Academic Medicine 96 (11): 1592–1597.
- Velasco-Mondragon, Eduardo, Angela Jimenez, Anna G. Palladino-Davis, Dawn Davis, and Jose A. Escamilla-Cejudo. 2016. “Hispanic Health in the USA: A Scoping Review of the Literature.” Public Health Reviews 37: 31.
- Weaver, Kathryn E., Julia H. Rowland, Keith M. Bellizzi, and Noreen M. Aziz. 2010. “Forgoing Medical Care Because of Cost.” Cancer 116: 3493–3504.
- Weech-Maldonado, Robert, Marc N. Elliott, Leo S. Morales, Karen Spritzer, Grant N. Marshall, and Ron D. Hays. 2004. “Health Plan Effects on Patient Assessments of Medicaid Managed Care among Racial/Ethnic Minorities.” Journal of General Internal Medicine 19: 136–145.
- Wilson, Patrick A., and Hirokazu Yoshikawa. 2007. “Improving Access to Health Care among African-American, Asian and Pacific Islander, and Latino Lesbian, Gay, and Bisexual Populations.” In The Health of Sexual Minorities: Public Health Perspectives on Lesbian, Gay, Bisexual, and Transgender Populations, edited by I. H. Meyer, and M. E. Northridge, 607–637. Boston: Springer.
- Zaikman, Yuliana, Tamara Stimatze, and Jacqueline A. Zeiber. 2020. “Women’s and Men’s Evaluations of Lesbians and Gay Men and Their Levels of Outness.” Sex Roles 83: 211–225.
