
ABSTRACT
Research has shown that childhood physical activity participation has a positive relationship with markers of wellbeing, such as self-esteem and quality of life, and physical activity participation may serve as protective mechanism against some mental illnesses including depression. The aim of the current study was to examine the relationship between gender, physical activity, screen time, body mass index and wellbeing in Irish school children (N = 705; mean age: 8.74 ± 0.52 years) from social disadvantage. In Northern Ireland, schools included in the 2010 Multiple Deprivation Measure (NIMDM) were invited to participate. Schools included for participation in the Republic of Ireland were from the Delivering Equality of Opportunity in Schools (DEIS) index. Data gathered included accelerometry (physical activity), self-report (screen time and wellbeing), and anthropometric measurements. Physical activity was objectively measured during eight consecutive days using Actigraph GT1M and GT3X devices, using stringent accelerometer protocol. Screen time activities were derived using questions adapted from the Health Promotion Agencies National Children’s Survey in Northern Ireland. The KIDSCREEN-27 is a health-related quality of life measurement, and this tool was used by participants to self-report their health and wellbeing. Results suggest that boys accumulated more minutes of daily screen time than girls, however, boys were more physically active when compared to girls. Wellbeing scores for gender showed inverse associations with daily screen time. Standard multiple regression revealed that gender, physical activity, screen time and body mass index (combined) explained little variance in the prediction of wellbeing. Results indicate the importance of gender-based considerations for physical activity and screen time with children from social disadvantage. The inverse relationship found between overall screen time and wellbeing will help guide future healthy lifestyle interventions for Irish children of low-income communities.
Recent evidence from the World Health Organization's (Citation2016) “Commission Report on Ending Childhood Obesity”, recommends that the implementation of comprehensive programmes for physical activity (PA) promotion and the reduction of sedentary behaviour are warranted for reducing children’s weight status. It is now well-established across many studies from the last decade that children are continuing to lead insufficiently active lifestyles (Eaton et al., Citation2012; Harrington et al., Citation2014, Citation2016; O’ Brien, Belton, & Issartel, Citation2016; O’Brien, Issartel, & Belton, Citation2018; Tremblay et al., Citation2015).
Insufficient PA has been linked with the increasing occurrence of obesity, overweight and health-related diseases into adulthood, such as diabetes and coronary heart disease (Lee et al., Citation2012), with an estimated economic cost of €80.4 billion per year to the EU-28 (International Sport and Culture Association, Centre for Economics and Business Research, Citation2015). Previous research in Ireland undertaken by The National Taskforce on Obesity (Department of Health and Children, Citation2005) outlined that over 300,000 children were estimated to be overweight or obese. More updated data suggest that one in four Irish children (N = 1215; 13.4 ± 2.1 yrs) are physically unfit, overweight, obese or have high blood pressure (Woods, Tannehill, Quinlan, Moyna, & Walsh, Citation2010). Data from the “Health Behaviour in School-Aged Children”(HBSC) study (Inchley et al., Citation2016) has found family affluence to be an important predictor of young people’s health, with an increased prevalence of childhood obesity for those in lower socio-economic regions.
This HBSC study (Inchley et al., Citation2016) highlights that inequalities related to family affluence exist across a range of health outcomes, most notably PA participation. While it is widely endorsed in Ireland and the United Kingdom that children should participate in a minimum of 60 min of moderate-to-vigorous physical activity (MVPA) every day for health (British Heart Foundation National Centre for Physical Activity and Health, Citation2013; Department of Health, Citation2016), researchers have shown that a low proportion of children from social disadvantage are meeting the recommended PA guidelines (Breslin, Brennan, Rafferty, Gallagher, & Hanna, Citation2012; Sutherland et al., Citation2016). For example, previous research within Northern Ireland highlights only 24% of children (aged 8–9 years old) from low socio-economic status (SES) achieve 60 min of MVPA each day (Breslin & Brennan, Citation2012). Furthermore, lower affluence relates to less bouts of childhood PA participation, and higher time spent in sedentary behaviour, specifically in Western Europe (Inchley et al., Citation2016).
Findings from the past decade indicate that higher levels of sedentary behaviours are positively associated with cardio-metabolic risk factors (Biddle et al., Citation2010; Carter, Hartman, Holder, Thijssen, & Hopkins, Citation2017; Young et al., Citation2016). Updated evidence has defined sedentary behaviour as any waking behaviour (independent of sleep), characterised by an energy expenditure ≤1.5 METs, while in a sitting, reclining or lying posture (Tremblay et al., Citation2017). The Canadian Sedentary Behaviour Guidelines for Children (5–11 years of age) and Youth (12–17 years of age) published recommendations (Tremblay et al., Citation2011) stating that for health benefits, screen time should be limited to no more than 2 h per day. Data reported by Inchley et al. (Citation2016) found that between 42% to 46% of Irish boys and girls aged 11 years old watch television for more than two hours per day on weekdays; children from low-affluence families watched more television.
Wellbeing is considered a multifaceted psychosocial construct underpinned by hedonic and eudaimonic theories (Ryan & Deci, Citation2001). Wellbeing incorporates both a subjective “hedonic” component where children can self-report on affective and cognitive aspects of their physical, social and mental health. Wellbeing also comprises a dynamic “eudaimonic” component which is concerned with a child’s sense of autonomy, environmental mastery, ability to develop potential and cultivate strong and positive relationships with others (Beddington et al., Citation2008; Ryan & Deci, Citation2001; The Children's Society, Citation2016). Therefore, wellbeing conceptually reflects how one’s way of living (i.e. dynamic eudaimonic perspective) may influence one’s subjective evaluation of their wellbeing (i.e. evaluative hedonic perspective) (Ryan & Deci, Citation2001). Much cross-sectional research has shown that childhood PA participation has a positive relationship with wellbeing markers, such as self-esteem and quality of life (Biddle & Asare, Citation2011; Breslin et al., Citation2012), and PA participation may protect against some mental illnesses including depression (Edmunds, Biggs, & Goldie, Citation2013).
The present study investigates the possible differences in both PA participation and screen time according to gender and weight status amongst primary-school children, specifically those from disadvantaged areas in Ireland. In line with the literature, the aim of the current study was to examine the relationship between gender, physical activity, screen time, body mass index and wellbeing in Irish school children from social disadvantage. The novelty of this study does not view the wellbeing of primary-school children from social disadvantage in Ireland in isolation, and accounts for the predictive associations of PA and screen time in this evolving dialogue. Findings will have implications for those promoting PA and reducing sedentary behaviour to improve wellbeing in an Irish primary school-aged population. Understanding the factors associated with the above health-related variables in Irish children is considered critical to effective prevention efforts (Economic and Social Research Institute & Department of Children and Youth Affairs, Citation2012).
Materials and methods
Overview
This cross-sectional study is part of a longitudinal programme of research entitled: the Sport for Life: All Island (SFL:AI) childhood physical activity intervention (Breslin et al., Citation2012, Citation2019; Breslin & Brennan, Citation2012). Data for the present study across the island of Ireland were gathered between September and October 2014, which specifically included accelerometry (PA), self-report (screen time and wellbeing), and anthropometric measurements (height and weight). Ethical approval was obtained from the associated Research Ethics Committee. Approval from each of the participating schools was granted by the school principals. Across the 27 schools recruited to the study, the pupil population was 1100. Seven hundred and five participants provided parental consent and assent when baseline measurements were taken (64% opt-in).
Following ethical approval, selected Irish primary schools across the island from areas of social and economic deprivation were identified using statistical databases. In Northern Ireland, schools included in the 2010 Multiple Deprivation Measure (NIMDM) were invited to participate. This database consists of seven domains of deprivation including: income, employment, health, education, proximity to services, living environment and crime. Schools included for participation in the Republic of Ireland were from the Delivering Equality of Opportunity in Schools (DEIS) index. Socio-economic variables in the DEIS database include: local authority accommodation, lone parenthood, Travellers’, large families (5 or more children) and pupils eligible for free books (Department of Education and Science, Citation2005).
Participants
Of the original seven hundred and five participants, 46, 15 and 158 were subsequently omitted from the screen time, BMI and wellbeing data sets, respectively as a result of missing data. Furthermore, due to the feasibility and the stringent accelerometer inclusion protocol for habitual PA measurement, 224 participants provided fully available objective PA data.
Field training Procedure and protocol
Undergraduate students from selected higher education institutions, in each of the four regions of Munster, Connaught, Leinster and Ulster were trained to conduct the research in their locality; all trained field staff were third and final-year undergraduate students enrolled in sports science, physical education and health-related degrees. To ensure consistency in data collection methods, researcher training was provided by the Principal Investigators from the SFL:AI project’s leading institute, across all sites. Training consisted of familiarity with the accelerometer (PA), self-report questionnaire (screen time and wellbeing), and understanding the correct measures for gathering participant height and weight data. To collect data in each region, and to ensure consistency, the trained researchers were accompanied by a senior member from the lead institute, who visited the schools participating in the study. Study participants were organised into groups of 5–6 children, with a member of the research team assigned to each group to assist with numeracy and literacy. Data was coded using a system to protect participant anonymity.
Measures
Physical activity. PA was objectively measured during eight consecutive days using Actigraph GT1M and GT3X devices, using stringent accelerometer protocol. PA was recorded in 5 s epochs to capture the intermittent and sporadic behaviour of youth (Esliger, Copeland, Barnes, & Tremblay, Citation2005). The first (to account for subject reactivity to wearing the device) (Dössegger et al., Citation2014) day from the recorded data were omitted from the analysis. In line with other studies, a day was deemed valid (and thereby included in analysis) if there was a minimum of 600 min recorded wear time per day (Nyberg, Ekelund, & Marcus, Citation2009; O’ Brien et al., Citation2016). The minimum number of valid days required for inclusion in the analysis were 3 weekdays and 1 weekend day (Gorely, Nevill, Morris, Stensel, & Nevill, Citation2009). Strings of “0” counts in bouts of ≥20 min were considered non-wear periods and activity count values of <0 and ≥ 15,000 counts per minute were excluded as these values were deemed biologically implausible (Esliger et al., Citation2005).
Minute-by-minute activity counts were uploaded to determine the amount of time spent in moderate-to-vigorous physical activity (MVPA). The average time spent in MVPA daily was calculated by applying movement thresholds to the Actilife 5.10 software. To standardise the data in line with Breslin & Brennan’s previous work (Citation2012) minutes spent in light, moderate and vigorous PA were estimated using Mattock et al.’s (Citation2007) physical activity cut-off points.
Screen Time. Screen time activities were derived using questions adapted from the Health Promotion Agencies National Children’s Survey in Northern Ireland (Health Promotion Agency, Citation2006). The three types of screen time activities analysed in the present study included (1) television viewing, (2) watching DVD’S and (3) using the computer. Participants were requested to self-report the frequency and duration of each screen time activity for school days (i.e. Monday to Friday), Saturdays and Sundays (i.e. weekend days) over the previous seven days. Overall screen time was calculated by summing the average number of minutes per day for each of the 3 variables (Anderson, Economos, & Must, Citation2008). Self-report screen time data was collected on participants in their class groups (maximum n = 30) during a 1-hour school visit.
Wellbeing. KIDSCREEN-27 (Ravens-Sieberer et al., Citation2014) is a health-related quality of life (HRQoL) measure that assesses physical, psychological, social and behavioural components of children’s self-reported health and wellbeing. This instrument has been previously used to assess wellbeing in studies of 8–9 year old children in Ireland (Breslin et al., Citation2012, Citation2019) and those studies have yielded satisfactory confirmatory fit indices and internal consistency scores. KIDSCREEN-27 aligns with the hedonic perspective of wellbeing and examines five dimensions of HRQoL, (1) Physical wellbeing (2) Psychological wellbeing (3) Parents and autonomy (4) Peer acceptance (5) School and Learning. A 5 point Likert scale was used to answer each item, with possible responses including “never”, “seldom”, “sometimes”, “often” and “always” (scoring 1–5). The Cronbachs Alpha reliability score for each dimension of the KIDSCREEN-27 questionnaire was calculated to assess for internal consistency (Loewenthal, Citation2001), as presented in . In line with previous research (Breslin et al., Citation2017), the KIDSCREEN-27 dimensions were shown to have satisfactory internal reliability in this study (Cronbach’s alpha > 0.6 for each scale Loewenthal, Citation2001). With the intention of assessing wellbeing as a multivariate construct, a total wellbeing score was calculated by adding the five wellbeing dimensions together. Higher scores indicated a more positive wellbeing.
Table 1. Cronbachs alpha reliability scores for the KIDSCREEN-27 questionnaire based on results from the SFL:AI sample.
Body mass index (BMI). Weight was measured to the nearest 0.1 kg using the Seca 761 dual platform weighing scales. Height was measured to the nearest millimetre using a portable Leicester stadiometer. Adhering to ethical gender protocol when measuring childhood height and weight, two field staff were trained by the principal investigator prior to data collection. BMI was calculated using the equation; weight (kg) /height (m)2. BMI scores were then categorised into underweight, healthy weight, overweight and obese using standardised methods (Cole, Flegal, Nicholls, & Jackson, Citation2007)
Data analysis
Data were analysed using SPSS version 22.0 for Windows. Descriptive statistics and frequencies were calculated for the physical characteristics, the types of screen time activities and objectively measured MVPA participation according to gender. Gender differences in PA, types of screen time and BMI mean scores were analysed using independent sample t-tests. Chi-square tests for independence were used to identify whether the percentage of participants meeting the MVPA time categories (30, 45, and 60 min) (O’Brien et al., Citation2018), differed according to gender and weight status (healthy, overweight or obese). Using the normalised data, Pearson product-moment correlations examined the strength of relationship among screen time and PA, screen time and wellbeing, and screen time and BMI scores. Standard multiple linear regression was performed to examine the overall relationship between the measurement of gender, minute-by-minute activity counts of MVPA, screen time and BMI scores in the association with childhood levels of wellbeing. Statistical significance was set at p < 0.05.
Results
The descriptive data of the physical characteristics, the types of screen time activities and objectively measured MVPA participation according to gender are presented in . In terms of weight status, 24% of boys, and 32% of girls are classified as overweight or obese. There were no significant gender differences between the percentages of overweight or obese children (χ2 = 6.362, ϕ = 0.095). In relation to the types of screen time activities, independent sample t-tests confirmed that there were significant gender differences, with boys accumulating more minutes (M = 86.38, SD = 81.17) of daily computer usage compared to girls (M = 44.30, SD = 62.11; t(657) = 7.412, p ≤ 0.01). Furthermore, boys accumulated more minutes (M = 38.07, SD = 16.41) of daily MVPA participation compared to girls (M = 31.80, SD = 11.71; t(222) = 3.258, p ≤ 0.01).
Table 2. Descriptive data for the physical characteristics, the types of screen time activities and objectively measured MVPA participation according to gender.
The overall mean daily screen time for participants was 160.01 ± 132.69 min per day (min per day). outlines the overall daily screen time according to gender and weight status. Boys accumulated significantly more minutes (181.45 min per day) of daily screen time than girls (136.24 min per day; t(657) = 4.425, p ≤ 0.01). When broken down by weight status, overweight and obese weight participants accumulated 160.80 min per day screen time, compared to 157.95 min per day screen time for healthy or underweight participants; yet, no statistically significant differences were observed between overweight and obese participants.
Table 3. Overall daily screen time according to gender and weight status.
and illustrate the prevalence of those accumulating at least 30 min per day, 45 min per day and 60 min per day of MVPA, for both gender and weight status. Chi-square tests for independence indicated that significant gender differences were again observed in those who accumulated at least 45 min per day (χ2 = 7.909, p ≤ 0.01) and 60 min of MVPA per day (χ2 = 8.028, p ≤ 0.01); a statistically higher proportion of boys accumulated at least 45 and 60 min of MVPA per day.
Figure 1. Percentage of boys and girls meeting 30–60 min MVPA per day.
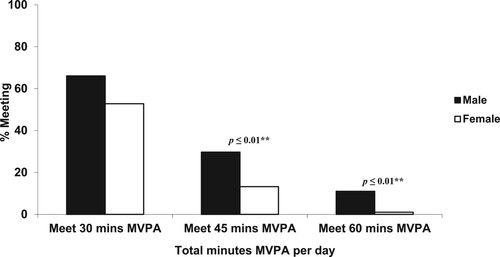
Figure 2. Percentage of healthy weight, overweight and obese participants meeting 30–60 min MVPA per day.
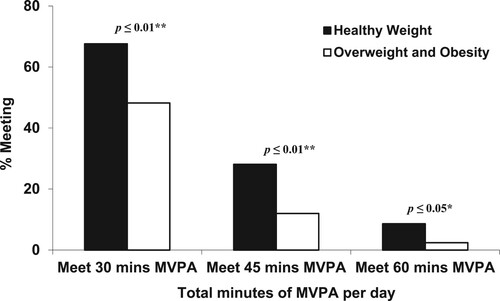
When analysed by weight status, the mean min of MVPA per day, as measured by accelerometry, was higher for healthy weight and underweight participants (37.17 ± 15.33 min per day), than those in the overweight and obese category (28.81 ± 10.72 min per day). Chi-square tests for independence indicated that weight status had a significant effect on those accumulating at least 30 min per day (χ2 = 13.09, p ≤ 0.01), 45 min per day (χ2 = 7.092, p ≤ 0.01), and 60 min per day (χ2 = 4.029, p ≤ 0.05), of MVPA; a higher proportion of healthy weight or under accumulated at least 30, 45 and 60 min per d MVPA.
shows the correlations among types of screen time activities, overall screen time, wellbeing, MVPA and BMI by gender. Wellbeing scores for boys showed weak negative correlations with all three types of screen time activities (r = −.131 to r = −.178), and overall screen time (r = −.214).
Table 4. Coefficients for correlations among types of screen time activities, total wellbeing, PA and BMI scores according to gender.
Wellbeing scores for girls showed weak negative correlations with daily television viewing (r = −.140), and overall screen time (r = −.140). Furthermore, time spent in MVPA for girls showed significant weak negative correlations with daily television viewing only (r = −.225), daily computer usage (r = −.202), and overall screen time (r = −.224).
Finally, standard multiple linear regression was used to assess the ability of gender, PA, screen time and BMI in the association with childhood levels of wellbeing. After the entry of these variables, the model as a whole revealed that gender, PA, screen time and BMI explained 4.6% of the variance in the prediction of childhood levels of wellbeing, but failed to reach statistical significance (F(4, 171) = 3.093).
Discussion
This article examined if possible differences in objectively measured PA participation and self-reported screen time varied according to gender and weight status among 8 and 9 year old Irish youth from social disadvantage. It further investigated if an overall relationship between gender, PA, screen time and BMI exists in the prediction of wellbeing amongst the sample. Boys were found to have higher levels of daily MVPA when compared to girls, a finding consistent with previous studies that have examined associations between gender and objectively measured daily MVPA (Tappe, Glanz, Sallis, Zhou, & Saelens, Citation2013; Vissers et al., Citation2013; D'Haese, Van Dyck, De Bourdeaudhuij, Deforche, & Cardon, Citation2014; Lee & Li, Citation2014). Furthermore, boys were found to be more likely to achieve 45 min of MVPA per day and 60 min of MVPA per day. Again this finding is consistent with previous research on gender specific associations (Kunin-Batson et al., Citation2015). This current study with Irish children of lower SES suggests that a positive relationship may exist between MVPA participation and boys.
Screen time is the most extensively researched form of sedentary behaviour in youth populations (Biddle & Asare, Citation2011). This study found that 8–9 year old boys from low SES backgrounds accumulate more overall screen time than girls. This finding is consistent with those of a large (n = 5844) international study from children from a range of SES across 12 countries (Leblanc et al., Citation2015), indicating this trend is not exclusive to children of low SES backgrounds. Most recent evidence from O’Brien et al. (Citation2018) supports this, as they also found a higher prevalence of screen time for boys, when compared to girls, in an adolescent population. However, both Leblanc et al. (Citation2015) and de Jong et al. (Citation2013) found that common correlates of high levels of screen time were levels of adiposity and having a TV or computer in the bedroom, which according to Tandon et al. (Citation2014) is a more common feature in low SES households. Specifically, the current study found that more daily computer usage was reported by boys than girls, which is in keeping with the findings of a large international survey (Cheema, Citation2015), albeit in 15 year old students. This large (n = 284,717), 43 country (including ROI) survey reported that boys spent more time on a computer using entertainment programmes than girls. Although the age of the children in the Cheema (Citation2015) study are 5–6 years older, it is speculated that perhaps the trend is likely to continue as the children age.
This study found that healthy weight participants were more likely to meet the WHO 60 min MVPA guidelines than their overweight and obese peers. Inchley et al. (Citation2016) found that family affluence impacted the prevalence of childhood obesity with those from lower SES regions, which concurred with the Seabra et al. (Citation2013) assertions. In their large (n = 683) study, Seabra and colleagues also observed a significant negative relationship between body composition and MVPA participation in obese 8–10 year old schoolchildren, in addition to those from lower SES. This recurring finding is concerning as articulated by Vale, Trost, Rêgo, Abreu, and Mota (Citation2015), who found similar results in 733 preschool-aged children, but they also observed significantly more cardiovascular risk factors (blood pressure) in obese children than those who were within the healthy weight category.
This study found an inverse relationship between total screen time and self-reported wellbeing. This finding is consistent with a previous systematic review (Hoare, Milton, Foster, & Allender, Citation2016), where the authors included 32 studies, and concluded a small negative association with sedentary behaviour and wellbeing amongst youth. That said, of the three specific screen time behaviours measured in this study, television viewing was the only variable to be significantly and negatively associated with wellbeing, independent of gender, with computer use and DVD viewing having a negative association with wellbeing for boys only. As this study is cross-sectional, reverse causality is conceivable, as children with poorer wellbeing may choose sedentary pursuits (Biddle, Mutrie, & Gorely, Citation2015). However, recent preliminary intervention studies and research (Hoare et al., Citation2016; Lubans et al., Citation2016) provide moderate evidence for screen time having a small negative influence on children’s wellbeing.
Given the cross-sectional research design of the current study, a true cause-and-effect relationship between participants MVPA and screen time cannot be determined. For these reasons, interpreting the finding that observed a negative association between girls’ MVPA and screen time (see ) has proven difficult. Previous evidence from the United States has observed that there is no relationship between MVPA and screen time in children between the ages of 6- to 11- years old; however, both variables were determined to be independently related to body composition (Fakhouri, Hughes, Brody, Kit, & Ogden, Citation2013). The current finding for girls aligns with recent Irish research (n = 169; 12.87 ± 0.61 years; O’Brien et al., Citation2018), which found that daily television viewing was negatively associated (r = −0.4, p ≤ 0.05) with MVPA levels in young adolescent girls. While the association found in the present study was slight weaker than the O’Brien et al. (Citation2018) data, the result is more difficult to interpret, as all study participants were from areas of social and economic deprivation. It is possible that the currently observed effects for screen time are more salient on girls’ MVPA, given that their PA levels are globally accepted as being significantly lower than boys. Future research is required with children across the island of Ireland to investigate if PA and sedentary behaviour are related, or not (Pearson, Braithwaite, Biddle, van Sluijs, & Atkin, Citation2014).
Finally, no overall relationship was found between gender, daily MVPA participation, screen time and BMI in the association with childhood levels of wellbeing in this study. The interaction of gender, MVPA participation, screen time and BMI within this investigation explained only 4.6% of the variance in the association with childhood levels of wellbeing, specifically with those from socially disadvantaged backgrounds. It is, however, important to note that results from this regression model are correlational, therefore, causation variable analysis is warranted for future longitudinal research. Perhaps, the observed cross-sectional correlational findings for gender between wellbeing and screen time lend support to further examinations of these variables amongst Irish children in low-income or disadvantaged communities (Breslin & Brennan, Citation2012).
While there are several strengths to the current study, including the broad national, all-island geographic spread of Irish participants, the use of objective accelerometry for collection of physical activity data, and the use of previously validated questionnaire items, there are also some limitations which must be acknowledged. Firstly, of note is that different metrics were used for defining low socioeconomic status in Northern Ireland and the Republic of Ireland, which may have some implications for variation in schools that were included in the study. The exclusion of data analysis comparisons for weekday versus weekend time periods for both physical activity and screen time variables could be perceived as a potential limitation for the population sample in question. Also, there was a low compliance with objective PA measurement, as a smaller number of participants provided sufficient data that met the stringent accelerometer inclusion criteria (227 out of 705). Finally, the assessment measure of screen time with participants did not account for contemporary mobile devices and electronic games, which children and youth are reported to use on a regular basis (e.g. tablets, smart phones, electronic games consoles).
Findings from the current study suggest that Irish boys from social disadvantage appear to be significantly more active than girls; conversely, boys do accumulate more minutes of overall screen time, when compared to girls though. Data findings are consistent with some cross-sectional studies in that an increased body composition may have an important association with PA participation, specifically the accumulation of increased minutes of MVPA per day respectively. The inverse relationship found between overall screen time and wellbeing across both gender types provides important information for children of social disadvantage in Ireland. With the extension of this study in a longitudinal capacity, future multi-component school-based interventions (O'Brien, Belton, & Issartel, Citation2015; Sutherland et al., Citation2015), designed to reduce levels of screen time, alongside targeting the increase of overall PA and wellbeing amongst primary-school Irish children in low-income or disadvantaged communities may be of importance.
Acknowledgements
We wish to acknowledge the undergraduate research assistants during data collection and analysis. We express our sincere gratitude to the participants, parents, teachers and principals from each of the Irish primary schools who took part. Research for the study was funded by a grant awarded by the Coca Cola Charitable Foundation. The funder had no input in study design, in the collection, analysis and interpretation of data; in the writing of the report; or in the decision to submit the article for publication.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Additional information
Funding
Notes on contributors
Wesley O’Brien
Dr. Wesley O’Brien, is a Lecturer in Physical Education and Coaching Science on the B.Ed Sports Studies and Physical Education Programme, in the School of Education, at University College Cork.
Sarahjane Belton
Dr. Sarahjane Belton, is current Head of School for Health and Human Performance at Dublin City University.
Ben Fitzpatrick
Dr. Ben Fitzpatrick, is the current Head of the School of Sport at Ulster University, Magee Campus.
Stephen Shannon
Dr. Stephen Shannon is a Lecturer in the School of Sport within the Faculty of Life and Health Sciences at Ulster University.
Deirdre Brennan
Deirdre Brennan, is Professor of Physical Education and Sport at Ulster University. Dr. Karol O'Donovan works at Cork University Hospital in the Department of Emergency Medicine.
Fiona Chambers
Dr. Fiona Chambers, is the Head of the School of Education at University College Cork, a Senior Lecturer in Physical Education and Sport Pedagogy and a Hasso-Plattner Institute-certified Design Thinking Coach.
Gavin Breslin
Dr. Gavin Breslin, is a Senior Lecturer in Psychology in the School of Psychology, Ulster University, and a member of the Sport and Exercise Sciences Research Institute.
References
- Anderson, S. E., Economos, C. D., & Must, A. (2008). Active play and screen time in US children aged 4 to 11 years in relation to sociodemographic and weight status characteristics: A nationally representative cross-sectional analysis. BMC Public Health, 8(366), doi:10.1186/1471-2458-8-366
- Beddington, J., Cooper, C. L., Field, J., Goswami, U., Huppert, F. A., Jenkins, R., … Thomas, S. M. (2008). The mental wealth of nations. Nature, 455(7216), 1057–1060. doi:10.1038/4551057a
- Biddle, S., Cavill, N., Ekelund, U., Gorely, T., Griffiths, M., Jago, R., … Richardson, D. (2010). Sedentary Behaviour and Obesity: Review of the Current Scientific Evidence.
- Biddle, S. J., & Asare, M. (2011). Physical activity and mental health in children and adolescents: A review of reviews. British Journal of Sports Medicine, bjsports90185.
- Biddle, S., Mutrie, N., & Gorely, T. (2015). Psychology of physical activity: Determinants, well-being and interventions (3rd ed.). Milton Park, Abingdon, Oxon; New York, NY: Routledge.
- Breslin, G., & Brennan, D. (2012). A healthy lifestyle intervention delivered by aspiring physical education teachers to children from social disadvantage. Child Care in Practice, 18(3), 207–225.
- Breslin, G., Brennan, D., Rafferty, R., Gallagher, A. M., & Hanna, D. (2012). The effect of a healthy lifestyle programme on 8-9 year olds from social disadvantage. Archives of Disease in Childhood, 97(7), 618–624. doi:10.1136/archdischild-2011-301108
- Breslin, G., Fitzpatrick, B., Brennan, D., Shannon, S., Rafferty, R., O’Brien, W., … Hanna, D. (2017). Physical activity and wellbeing of 8–9 year old children from social disadvantage: An all-Ireland approach to health. Mental Health and Physical Activity, 13, 9–14. doi:10.1016/j.mhpa.2017.06.001
- Breslin, G., Shannon, S., Rafferty, R., Fitzpatrick, B., Belton, S., O’Brien, W., … Brennan, D. (2019). The effect of sport for LIFE: All island in children from low socio-economic status: A clustered randomized controlled trial. Health and Quality of Life Outcomes, 17(1), 1–12. doi:10.1186/s12955-019-1133-x
- British Heart Foundation National Centre for Physical Activity and Health. (2013). Interpreting the UK physical activity guidelines for children and young people (5-18): Guidance for those who work with children and young people. Loughborough University.
- Carter, S., Hartman, Y., Holder, S., Thijssen, D. H., & Hopkins, N. D. (2017). Sedentary behavior and cardiovascular disease risk: Mediating mechanisms. Exercise and Sport Sciences Reviews, 45(2), 80–86. doi:10.1249/JES.0000000000000106
- Cheema, J. R. (2015). Differences in computer use for entertainment between boys and girls: Evidence from a global survey. Entertainment Computing, 9-10, 1–10. doi:10.1016/j.entcom.2015.06.001
- Cole, T. J., Flegal, K. M., Nicholls, D., & Jackson, A. A. (2007). Body mass index cut offs to define thinness in children and adolescents: International survey. BMJ, 335(7612), 194.
- D'Haese, S., Van Dyck, D., De Bourdeaudhuij, I., Deforche, B., & Cardon, G. (2014). The association between objective walkability, neighborhood socio-economic status, and physical activity in Belgian children. International Journal of Behavioral Nutrition and Physical Activity, 11, 104.
- de Jong, E., Visscher, T. L. S., HiraSing, R. A., Heymans, M. W., Seidell, J. C., & Renders, C. M. (2013). Association between TV viewing, computer use and overweight, determinants and competing activities of screen time in 4-to 13-year-old children. International Journal of Obesity, 37(1), 47–53.
- Department of Education and Science. (2005). DEIS - Delivering equality of opportunity in schools: An action plan for educational inclusion summary. Dublin, Designed by Total PD and Printed by New Oceans.
- Department of Health and Department of Transport, Tourism and Sport. (2016). Healthy Ireland: Get Ireland active - National physical activity plan for Ireland. Dublin, Ireland.
- Department of Health and Children. (2005). Obesity: The policy challenges: The report of the national taskforce on obesity 2005. Dublin.
- Dössegger, A., Ruch, N., Jimmy, G., Braun-Fahrländer, C., Mäder, U., Hänggi, J., … Bringolf-Isler, B. (2014). Reactivity to accelerometer measurement of children and adolescents. Medicine and Science in Sports and Exercise, 46(6), 1140–1146. doi:10.1249/MSS.0000000000000215
- Eaton, D. K., Kann, L., Kinchen, S., Shanklin, S., Flint, K. H., Hawkins, J., … Wechsler, H. (2012). Youth risk behavior surveillance - United States, 2011. Morbidity and Mortality Weekly Report, 61(4), 1–162. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/22673000
- Economic and Social Research Institute & Department of Children and Youth Affairs. (2012). Growing Up in Ireland National longitudinal study of children. Dublin, Ireland: Department of Children and Youth Affairs.
- Edmunds, S., Biggs, H., & Goldie, I. (2013). Let’s get physical: The impact of physical activity on wellbeing. Mental Health Foundation (Vol. 38).
- Esliger, D., Copeland, J., Barnes, J., & Tremblay, M. (2005). Standardizing and optimizing the use of accelerometer data for free-living physical activity monitoring. Journal of Physical Activity & Health, 3, 366–383.
- Fakhouri, T. H. I., Hughes, J. P., Brody, D. J., Kit, B. K., & Ogden, C. L. (2013). Physical activity and screen-time viewing Among Elementary School-aged children in the United States from 2009 to 2010. JAMA Pediatrics, 167(3), 223–229. doi:10.1001/2013.jamapediatrics.122
- Gorely, T., Nevill, M. E., Morris, J. G., Stensel, D. J., & Nevill, A. (2009). Effect of a school-based intervention to promote healthy lifestyles in 7-11 year old children. International Journal of Behavioral Nutrition and Physical Activity, 6, 5. doi:10.1186/1479-5868-6-5
- Harrington, D. M., Belton, S., Coppinger, T., Cullen, M., Donnelly, A., Dowd, K., … Woods, C. (2014). Results from Ireland’s 2014 report Card on physical activity in children and youth. Journal of Physical Activity and Health, 11(Supp 1), S63–S68.
- Harrington, D. M., Murphy, M., Carlin, A., Coppinger, T., Donnelly, A., Dowd, K. P., … Belton, S. (2016). Results from Ireland North and South’s 2016 report Card on physical activity for children and youth. Journal of Physical Activity and Health, 13(Suppl 2), S183–S188. doi:10.1123/jpah.2016-0334
- Health Promotion Agency. (2006). Child Health Survey: A study of eating habits, physical activity and obesity levels in primary school children. Health Promotion Agency Northern Ireland. Unpublished Report.
- Hoare, E., Milton, K., Foster, C., & Allender, S. (2016). The associations between sedentary behaviour and mental health among adolescents: A systematic review. International Journal of Behavioral Nutrition and Physical Activity, 13(1), 108.
- Inchley, J., Currie, D., Young, T., Samdal, O., Torsheim, T., Augustson, L., … Barnekow, V. (2016). Growing up unequal: Gender and socioeconomic differences in young people’s health and well-being. Health behaviour in school-aged children study: International report from the 2013/14 survey. Copenhagen.
- International Sport and Culture Association., & Centre for Economics and Business Research. (2015). The economic cost of physical inactivity in Europe.
- Kunin-Batson, A. S., Seburg, E. M., Crain, A. L., Jaka, M. M., Langer, S. L., Levy, R. L., & Sherwood, N. E. (2015). Household factors, family behavior patterns, and adherence to dietary and physical activity guidelines among children at risk for obesity. Journal of Nutrition Education and Behavior, 47(3), 206–215.e1.
- Leblanc, A. G., Katzmarzyk, P. T., Barreira, T. V., Broyles, S. T., Chaput, J. P., Church, T. S., … Kurpad, A. (2015). Correlates of total sedentary time and screen time in 9–11 year-old children around the world: The international study of childhood obesity, lifestyle and the environment. PloS one, 10(6), e0129622.
- Lee, C., & Li, L. (2014). Demographic, physical activity, and route characteristics related to school transportation: An exploratory study. American Journal of Health Promotion, 28(3, Suppl), S77–S88.
- Lee, I.-M., Shiroma, E. J., Lobelo, F., Puska, P., Blair, S. N., & Katzmarzyk, P. T. (2012). Effect of physical inactivity on major non-communicable diseases worldwide: An analysis of burden of disease and life expectancy. Lancet, 380(9838), 219–229. doi:10.1016/S0140-6736(12)61031-9
- Loewenthal, K. M. (2001). An introduction to psychological tests and scales (2nd ed). Hove: Psychology Press.
- Lubans, D. R., Smith, J. J., Morgan, P. J., Beauchamp, M. R., Miller, A., Lonsdale, C., … Dally, K. (2016). Mediators of psychological well-being in adolescent boys. Journal of Adolescent Health, 58(2), 230–236.
- Mattocks, C., Leary, S., Ness, A., Deere, K., Saunders, J., Tilling, K., Kirkby, J., Blair, S. N., & Riddoch, C. (2007). Calibration of an accelerometer during free-living activities in children. International Journal of Pediatric Obesity, 2(4), 218–226. https://doi.org/10.1080/17477160701408809
- Nyberg, G., Ekelund, U., & Marcus, C. (2009). Physical activity in children measured by accelerometry: Stability over time. Scandinavian Journal of Medicine & Science in Sports, 19(1), 30–35. doi:10.1111/j.1600-0838.2007.00756.x
- O'Brien, W., Belton, S., & Issartel, J. (2015). Promoting physical literacy in Irish adolescent youth: The youth-physical activity towards health (Y-PATH) intervention. MOJ Public Health, 2(6), 1–6. doi:10.15406/mojph.2015.02.00041
- O’ Brien, W., Belton, S., & Issartel, J. (2016). The relationship between adolescents’ physical activity, fundamental movement skills and weight status. Journal of Sports Sciences, 34(12), 1159–1167. doi:10.1080/02640414.2015.1096017
- O’Brien, W., Issartel, J., & Belton, S. (2018). Relationship between physical activity, screen time and weight status among young adolescents. Sports, 6(57), 1–11. doi:10.3390/sports6030057
- Pearson, N., Braithwaite, R. E., Biddle, S. J. H., van Sluijs, E. M. F., & Atkin, A. J. (2014). Associations between sedentary behaviour and physical activity in children and adolescents: A meta-analysis. Obesity Reviews, 15(8), 666–675. doi:10.1111/obr.12188
- Ravens-Sieberer, U., Herdman, M., Devine, J., Otto, C., Bullinger, M., Rose, M., & Klasen, F. (2014). The European KIDSCREEN approach to measure quality of life and well-being in children: Development, current application, and future advances. Quality of Life Research, 23(3), 791–803. doi:10.1007/s11136-013-0428-3
- Ryan, R. M., & Deci, E. L. (2001). On happiness and human potentials: A review of research on hedonic and eudaimonic well-being. Annual Review of Psychology, 52(1), 141–166.
- Seabra, A., Mendonça, D., Maia, J., Welk, G., Brustad, R., Fonseca, A. M., & Seabra, A. F. (2013). Gender, weight status and socioeconomic differences in psychosocial correlates of physical activity in schoolchildren. Journal of Science and Medicine in Sport, 16(4), 320–326.
- Sutherland, R., Campbell, E., Lubans, D. R., Morgan, P. J., Okely, A. D., Nathan, N., … Wiggers, J. (2015). Physical activity 4 Everyone ‘ school-based intervention to prevent decline in adolescent physical activity levels : 12 month (mid- intervention) report on a cluster randomised trial. British Journal of Sports Medicine, 0, 1–10. doi:10.1136/bjsports-2014-094523
- Sutherland, R. L., Campbell, E. M., Lubans, D. R., Morgan, P. J., Nathan, N. K., Wolfenden, L., … Wiggers, J. H. (2016). The physical activity 4 Everyone cluster randomized trial: 2-year outcomes of a school physical activity intervention among adolescents. American Journal of Preventive Medicine, In Press, 1–11. doi:10.1016/j.amepre.2016.02.020
- Tandon, P., Grow, H. M., Couch, S., Glanz, K., Sallis, J. F., Frank, L. D., & Saelens, B. E. (2014). Physical and social home environment in relation to children's overall and home-based physical activity and sedentary time. Preventive Medicine, 66, 39–44.
- Tappe, K. A., Glanz, K., Sallis, J. F., Zhou, C., & Saelens, B. E. (2013). Children's physical activity and parents’ perception of the neighborhood environment: Neighborhood impact on kids study. International Journal of Behavioral Nutrition and Physical Activity, 10, 39.
- The Children's Society. (2016). The good childhood report 2016. Retrived from http://cdn.basw.co.uk/upload/basw_94045-10.pdf
- Tremblay, M. S., Aubert, S., Barnes, J. D., Saunders, T. J., Carson, V., Latimer-Cheung, A. E., … SBRN Terminology Consensus Project Participants. (2017). Sedentary behavior research Network (SBRN) - Terminology consensus project process and outcome. International Journal of Behavioral Nutrition and Physical Activity, 14(75), 1–17. doi:10.1186/s12966-017-0525-8
- Tremblay, M. S., Gonzalez, S. A., Katzmarzyk, P. T., Onywera, V. O., Reilly, J. J., & Tomkinson, G. (2015). Physical activity report cards: Active healthy kids global alliance and the Lancet physical activity observatory. Journal of Physical Activity and Health, 12, 297–298. doi:10.1123/jpah.2015-0184
- Tremblay, M. S., Leblanc, A. G., Janssen, I., Kho, M. E., Hicks, A., Murumets, K., … Duggan, M. (2011). Canadian sedentary behaviour guidelines for children and youth. Applied Physiology, Nutrition, and Metabolism, 36(1), 59–64. doi:10.1139/H11-012
- Vale, S., Trost, S. G., Rêgo, C., Abreu, S., & Mota, J. (2015). Physical activity, obesity status, and blood pressure in preschool children. The Journal of Pediatrics, 167(1), 98–102.
- Vissers, P. A. J., Jones, A. P., van Sluijs, E. M. F., Jennings, A., Welch, A., Cassidy, A., & Griffin, S. J. (2013). Association between diet and physical activity and sedentary behaviours in 9–10-year-old British White children. Public Health, 127(3), 231–240.
- Woods, C. B., Tannehill, D., Quinlan, A., Moyna, N., & Walsh, J. (2010). The children’s sport participation and physical activity study (CSPPA). Research Report No 1. Dublin, Ireland.
- World Health Organization. (2016). Report of the commission on ending childhood obesity. Geneva. Retrieved from www.who.int/end-childhood-obesity/en
- Young, D. R., Hivert, M.-F., Alhassan, S., Camhi, S. M., Ferguson, J. F., Katzmarzyk, P. T., … Yong, C. M. (2016). Sedentary behavior and cardiovascular morbidity and mortality: A science advisory from the American heart association. Circulation, 134(13), e262–e279. doi:10.1161/CIR.0000000000000440