
ABSTRACT
Background
Adolescent mental illness is of increasing concern, with prevalence increasing especially in females in the United Kingdom. While service-related barriers can deter help-seeking, the role of family support and engagement in family activities, and attitudes towards seeking help from a doctor has received little attention. Studies exploring help-seeking from family and medical practitioners have done so without incorporating theories of behaviour change. This study aims to develop a model of adolescent help-seeking using the Theory of Planned Behaviour (TPB).
Method
A cross-sectional survey of 1639 male and females aged 13–17 years in Northern Ireland. Structural Equation Modelling determined fit for TBP factors, with the addition of gender, experience of mental health issues, and engagement in family activities.
Results
The Structural Equation Model suggests an adequate description of the relationships between TPB variables [χ2(639) = 8302.36, p < .001; RMSEA = 0.09; SRMR = 0.06; CFI = 0.92; IFI = 0.92], with significant variance (R2) of up to 61% (Intentions to Seek Help from Family) and 24% (Intention to Seek Help from Medical Professionals) explained. Males (compared to females) reported a more supportive family life, fewer mental health problems, more trust in doctors, less prosocial behaviour, more confidence discussing mental health with a doctor, and greater intentions to seek family or medical professional help when having emotional/mental health problems.
Conclusions
When supporting adolescent’s gender, engagement with family and trust in doctors should be considered, especially where they have experienced mental health issues and may be less willing to seek help.
Adolescent mental illness is an issue of public health concern (Nearchou et al., Citation2018), with rates increasing particularly amongst girls (Kessler et al., Citation2005; Lessof et al., Citation2016; Merikangas et al., Citation2010). A recent survey in England showed 14.4% of 11–16 year olds had a mental illness (Department of Health, Citation2018) while the Millennium Cohort Study in the United Kingdom reported 24% of girls and 9% of boys experienced severe symptoms of depression (Lai et al., Citation2019). In Northern Ireland (NI), where the current study was conducted, 23.9% of females recorded a mental health problem, more than twice of that for males (Leavey et al., Citation2020). Findings from adult population surveys indicate limited understanding of mental health help-seeking issues, and paradoxically, individuals will offer help to someone experiencing a mental health problem, but not seek help themselves (Breslin & McCay, Citation2013). While service-related barriers can deter help-seeking, adolescent lack of awareness of available services, and poor understanding of health care rights, may determine a lack of help-seeking. Stigma related to mental illness plays a significant part (Clement et al., Citation2015), manifesting itself in several ways, through: (i) the perception or experience of discrimination by those affected; (ii) negative attitudes towards them; (iii) self- or internalised stigma, and; (iv) discriminatory and stigmatising practices in health services, legislation and media (Van Brakel, Citation2006).
While public health campaigns to reduce stigma have had limited success, few have been tailored to an adolescent population, often risking a misalignment with youth attitudes, beliefs and needs around help-seeking (Howard et al., Citation1999; Jacquez et al., Citation2013; Thackeray & Hunter, Citation2010). Responding to this lack of evidence in relation to young people, the Northern Ireland Schools and Wellbeing Survey (Corry & Leavey, Citation2016: Leavey et al., Citation2020) explored adolescent views of who they would trust when seeking support. While adolescents had a high trust in seeking support from General Practitioners (GPs), those with experience of mental illness were less trusting (36% of the sample), with anxiety about revealing weakness being the main reason (Corry & Leavey, Citation2016; Leavey et al., Citation2020). Adolescent girls were less likely to seek help than their male peers, while confiding in mothers provided comfort when seeking support. Although informative, this research did not interpret or incorporate a framework or detailed theory of behaviour change.
Behaviour change theory
Psychological behaviour change theories that have their origins in social and cognitive sciences explain how and why individuals engage in intentional health behaviours (Hagger & Chatzisarantis, Citation2014). A recognised limitation of the adolescent help-seeking research has been the lack of a unifying behavioural theory. Those available have tended to be descriptive rather than explanatory, or have a macro-level focus on social and economic factors that affect access to services (Pescosolido & Boyer, Citation1999). Given this it is important to explore micro-level psychological factors that facilitate or inhibit motivation to seek help (Breslin & McCay, Citation2013; Rickwood et al., Citation2005) a view in line with National Institute of Health and Care Excellence (NICE, Citation2014) guidance. According to the NICE guidelines incorporating behaviour change theory provides researchers with core structures on motivation, planning and the decision-making process. Although several psychological theories of behaviour change have been applied to mental health help-seeking in adults – for example, the Theory of Reasoned Action (TRA) (Ajzen & Fishbein, Citation1977), and Theory of Planned Behaviour (TPB) (Ajzen, Citation1985; Citation2011; Breslin & McCay, Citation2013; Damghanian & Alijanzadeh, Citation2018; see Rickwood et al., Citation2014 for a review) – they have not yet been applied to adolescent help-seeking from their doctor or family.
The TRA provides an explanation for the motivations surrounding engagement (or not) in health behaviours. It assesses motivational intentions via analysis of attitudes towards a behaviour (A) and associated subjective norm (SN) (Ajzen & Fishbein, Citation1977). In relation to mental health and help-seeking, attitudes comprise the thoughts and feelings a person has towards mental illness and whether they believe it is worth seeking help. Subjective norms relate to how individuals view seeking or giving help and their subsequent behaviours, when considering what significant others would want them to do in that situation. Both views co-exist, and affect an individual’s intention and subsequent help-seeking behaviour (Ajzen, Citation1991; Ajzen & Fishbein, Citation1977; Breslin et al., Citation2019). The TRA was developed into the Theory of Planned Behaviour (TPB) with the inclusion of a third construct – perceived behavioural control (PCB), the perception of being able to competently seek help (Ajzen, Citation1985). Attitudes, subjective norms and perceived behavioural control are correlated, and when statistically modelled they can explain intentions to seek help, explaining up to 24% of variance in health behaviours (McEachan et al., Citation2011).
This study applied the Theory of Planned Behaviour (Ajzen, Citation1985) to the Northern Ireland Schools and Wellbeing Survey (Leavey et al., Citation2020) to examine adolescent help-seeking from both family and General Practitioner (GP). The overall model () integrates attitudes (towards Doctor Help), subjective norms derived from levels of adolescent prosocial behaviour (Prosocial Behaviour), perceived behavioural control (Confidence in Discussing Mental Health with Doctor) with intentions (Intentions to Seek Help from Medical Professionals and Intentions to Seek Help from Family). As adolescent help-seeking is complex, we incorporated a measure of family activity and perceived family life (Harding et al., Citation2015). We included strengths and difficulties experienced by youth as a factor in the model, as mental health has been shown to predict trust in GPs (Leavey et al., Citation2020).
Figure 1. Structural model indicating the predicted relationships between the latent variables.
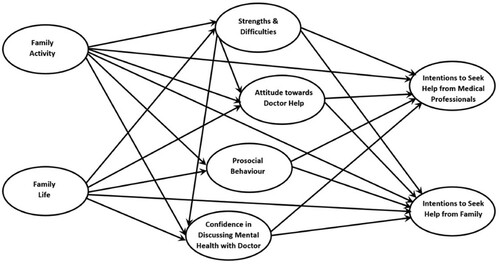
We had four aims in relation to the Structural Equation Model tested (See ). To establish if: (1) TPB variables significantly explain variation in mental health help-seeking intentions; (2) TPB variables have significant positive links to intentions to seek help from medical professions and intentions to seek-help from family; (3) participation in family activities and a supportive family life significantly reduce mental health difficulties (Strengths and Difficulties), and positively influence TPB variables, including intentions to seek help from both medical professionals and family; and finally (4) whether significant model inter-relationship differences exist across gender groupings.
Method
Sample and design
A cross-sectional survey of pupils in Northern Ireland aged 13–17 years (Corry & Leavey, Citation2016) was conducted (N = 1,639; Males = 610; Females = 1029). Schools were purposely chosen from a database of post-primary schools based on Urban/Rural and school type (Grammar/Secondary Modern). Grammar schools are selective i.e. pupils are admitted on the basis of academic ability, Secondary Modern are non-selective. Parents were given a letter explaining the aims of the study, with an opt-out form for non-participation. Pupils provided consent and completed the survey in class groups, across eight schools. The study was approved by Ulster University Research Ethics Committee. A full description of participant recruitment is reported elsewhere (Leavey et al., Citation2020).
Measures
Family activity and life
A 14-item questionnaire from the London-based Determinants of Young Adult Social Well-being and Health (DASH) study – comprising sections on family activity (6 items) and available support from parents (8 items) – was included (Harding et al., Citation2004). After initial testing of the measurement model stage of the Structural Equation Model, the Go for a walk or play sports together item was removed from the family activity component due to its weak factor loading.
Current mental health
The Strengths & Difficulties Questionnaire (SDQ), a validated tool for assessing probable mental health problems in school-age children (Goodman et al., Citation1998) was included. We used the total difficulties score (total score excluding the prosocial scale), which provides a total score between 0 and 40 representing psychological difficulties.
Prosocial behaviour (subjective norm)
The prosocial scale from the Strengths & Difficulties Questionnaire (SDQ) was used to ascertain level of concern for others.
Adolescent attitudes towards seeking help from a general practitioner (attitude)
There are no validated measures of adolescent attitudes towards seeking help from a General Practitioner (GP) as a source of help for mental health problems. Based on previous research (Divin et al., Citation2018; Leavey et al., Citation2020) we developed a 17-item self-report questionnaire on such attitudes, based on a seven-point Likert scale (1 = strongly agree to 7 = strongly disagree). Positively worded items (e.g. “My doctor/GP is very approachable and friendly”) were reverse coded for analysis. Thus, a high score indicates a positive relationship with doctors. This scale demonstrated strong internal consistency (α = .86). Two items (“I usually see the same doctor” and “I am able to see the doctor on my own”) correlated weakly with other factors and were removed for analysis. A single item from this scale – I feel confident discussing an emotional or mental health issue with my family doctor – was separated and used as an indication of confidence in discussing mental health problems with a GP.
Intentions to seek help from family
Help-seeking intentions when having emotional or mental health problems, based on a seven-point Likert self-report scale ranging from (1) not likely to (7) very likely, were examined in relation to family members (father, mother, brother, sister).
Intentions to seek help from a medical professional
Help-seeking intentions when having emotional or mental health problems, based on a seven-point Likert self-report scale ranging from (1) not likely to (7) very likely, were examined in relation to the medical profession (Local family doctor, school nurse).
Analysis
Descriptive statistics (mean average, standard deviations) and independent t-test analyses were conducted to explore the variables within the overall model. The Maximum Likelihood (ML) method estimated the measurement and structural model stages of the full Structural Equation Model (SEM). Normal Theory Weighted Least Squares scaled Chi-square was one of the indices to ascertain how well the model fitted the data, but it is sensitive to sample size so alternative indices were also employed. Consistent with the recommendation of Hu and Bentler (Citation1999) two alternate types of fit indices – residual-based (Standardised Root Mean Residual; SRMR), and comparative fit (Comparative Fit Index, Incremental Fit Index, and Root Mean Square Error of Approximation; CFI, IFI and RMSEA respectively) – were used to minimise Type I and II error rates. Combination rules highlighted by Hu and Bentler (Citation1999) suggest SRMR and RMSEA scores below 0.08, in combination with comparative fit indices above 0.95 significantly reduce the instances of model misspecification and the rates of type I and II errors, although acceptable comparative fit cut-offs can be as low as 0.90 according to some authors. To reduce reliance on correlated errors to improve model fit, while adversely affecting the parsimony of the model, the current study accepts a model that has fit statistics that are within proximity of the recommended levels. A multi-group analysis of the accepted model was also undertaken to assess equivalence across gender groupings.
Results
Descriptive statistics () show moderate Family Activity levels, including watching television, having meals and going out together. The Family Life mean score indicates a moderately high level of support from parents and moderately high levels of intention to seek help from family (father, mother or sibling) where participants reported emotional or mental health problems. A relatively low mean SDQ score (peer, emotional, conduct and hyperactivity problems) suggests low levels of mental health problems within the sample. While attitudes towards seeing a doctor for help with emotional or mental health issues were moderately positive, both confidence in discussing mental health problems with a doctor and intention to seek help from medical professionals (local family doctor, school nurse) were relatively low. Concern for others, measured as Prosocial behaviour levels (Subjective Norm), were relatively high.
Table 1. Descriptive statistics for the latent variables within the model.
Generally, shows that males (when compared with females) reported a more supportive family life, fewer mental health problems (Strengths & Difficulties), more trust in GPs, less prosocial behaviour, more confidence discussing mental health with doctor, and greater intentions to seek family or medical professional help when having emotional/ mental health problems. Family activity was similar for males and females (p > .05).
Table 2. Descriptive statistics split by gender for the latent variables within the model.
The measurement model () indicates that observed item indicators are acceptable representations of their specific latent variables. The measurement model fit indices (Hu & Bentler, Citation1999) suggest an adequate description of the relationships between the variables [χ2(639) = 8611.67, p < .001; RMSEA = 0.09; SRMR = 0.06; CFI = 0.91; IFI = 0.91].
Table 3. The estimated measurement components of the structural equation model.
Aim 1: TPB variables significantly explain variation in mental health help-seeking intentions
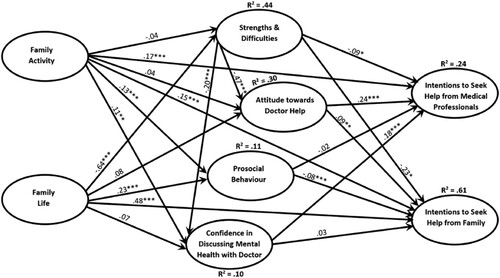
The fit indices for the full Structural Equation Model (See ) suggests an adequate description of the relationships between the variables [χ2(639) = 8302.36, p < .001; RMSEA = 0.09; SRMR = 0.06; CFI = 0.92; IFI = 0.92], with significant variance (R2) of up to 61% (with intention to seek help from family) explained within endogenous variables, including Intention to Seek Help from Medical Professionals and Intention to Seek Help from Family.
Figure 2. Structural model indicating the relationships between the latent variables.
Note: *p < 0.05; **p < 0.01; ***p < 0.001.
Aim 2: TPB variables have significant positive links to intentions
Positive attitudes towards doctor help and greater confidence in discussing mental health with a doctor had significant but weak positive relationships with greater intention to seek help from medical professionals. Although the rest of the TPB variable relationships with intention to seek help from medical professional and family were significant, they were all very weak (less than .1). However, it should be noted that greater levels of mental health problems (Strengths & Difficulties) had a statistically significant negative but minimal impact on intentions to seek help from medical professionals and a stronger significant negative impact on attitude to doctor help.
Aim 3: participation in family activities and a supportive family life significantly reduce mental health difficulties and positively influence TPB variables
Levels of family activity were positively associated with prosocial behaviour and confidence in discussing mental health with doctor. Greater levels of family activity had significant weak positive relationships with greater intention to seek help from medical professionals. A supportive family life significantly and strongly related to lower mental health difficulties (Strengths & Difficulties) and positive help-seeking from family for emotional or mental health problems, while having a significant weak positive impact on prosocial behaviour. In addition, it must be noted that Mental health problems (Strengths & Difficulties) were negatively and significantly associated with intentions to seek help from family.
Aim 4: significant model inter-relationship differences exist across gender groupings
A multi-group comparison between a no restrictions model (Means and path coefficients allowed to vary freely across groups) and a fully restricted model (Means and path coefficients restricted to be equal across groups) indicated a significant difference in model means and path coefficients across gender groupings (χ2(95) = 6413.31, p < .001).
Upon further scrutiny of the model across gender groupings (), significant and sizeable differences between path coefficients are noticeable. For example, involvement in more family activities had a sizeably stronger positive link with greater intentions to seek help from medical professions and prosocial behaviour within the male sample. In addition, a more supportive family life had sizeably stronger links with greater confidence discussing mental health with a doctor and prosocial behaviour within the male sample. A supportive family life links more strongly to greater intentions to seek help from family in the female sample, compared to a weak link in the male sample. Positive attitudes towards a doctor’s help links to lower mental health problems (SDQ) more strongly within the female sample.
Table 4. Multi-group comparison of SEM model path coefficients, by gender.
Discussion
Using Structural Equation Modelling we applied the Theory of Planned Behaviour (Ajzen, Citation1985) to examine adolescent intention to seek help from either a medical professional or a family member. The four aims itemised above were examined. An SEM representing TPB constructs () provided an adequate fit and description of the relationships between the core TPB variables (Attitude to Doctor Help, Prosocial Behaviour, and Confidence Discussing Mental Health with Doctor) whilst confirming the model provided a significant explanation of variation in adolescent help-seeking intentions – 61% from family and 24% from health professionals. Findings were largely consistent with studies across multiple health behaviours (McEachan et al., Citation2011), such that psychological (i.e. attitudes, confidence) and social (i.e. subjective norms) factors exert direct and indirect influences on mental health help-seeking behaviours, development of which seems required to mitigate the high prevalence of adolescent mental illness (WHO, Citation2013).
Consistent with extant evidence in the general population (Schomerus et al., Citation2009), in relation to Aim 2, adolescents’ positive attitudes towards seeking help from a doctor and greater confidence in discussing mental health with a doctor had a positive relationship with intentions to seek help from a medical professional. Given such positive relationships, we suggest that those involved in delivering mental health awareness messages to adolescents promote greater internal control, acknowledgement of benefits, and personal confidence, possibly via role plays, case studies and/or access to help-seeking resources (e.g. helplines, websites; Bohon et al., Citation2016).
With regards to Aim 3, both family activity and having a positive family life contributed to adolescent help-seeking. Interestingly, experiencing mental health problems (SDQ) were negatively associated with help-seeking from family and GPs, while levels of family activity were positively associated with prosocial behaviour and confidence in discussing mental health with a doctor. Also notable was that having a supportive family life significantly and strongly related to fewer mental health difficulties (Strengths and Difficulties), with adolescents scoring higher in family life more likely to seek help from family for emotional or mental health problems. These findings support evidence from the DASH study suggesting that youth mental health help-seeking can be predicted through family activity and comfort with family life (Harding et al., Citation2015).
In terms of Aim 4, for males, family activity had a significantly stronger positive impact on seeking help from medical professionals, while for females, family life had a significantly stronger positive impact on help-seeking from family. On inspection of mean differences, males reported significantly more involvement in family life than females, lower mental health difficulties, more positive attitudes towards GPs, greater confidence in discussing mental health issues with a doctor, and greater intentions to seek family and medical profession help when experiencing mental health problems. Given that in the UK higher proportions of females (compared to males) experience mental and emotional problems (Lai et al., Citation2019; Leavey et al., Citation2020), it is perhaps these factors that provide a protection for males given that, if the results of this study are generalisable, they are more likely to seek help. Any interventions to support adolescent help-seeking should consider the nuances of gender.
Until recently, researchers have highlighted that adolescent perspectives are not typically accounted for in mental health programme support (Howard et al., Citation1999; Jacquez et al., Citation2013; Thackeray & Hunter, Citation2010) – compared with adults they tend to have different views and interpretations of the world, making intervention less effective or aligned to what may actually be required in the form of support (Howard et al., Citation1999). Furthermore, the role of family life and family activities could be explored more as a way of supporting young people. Because mothers are more likely to be asked for help by their children (Leavey et al., Citation2011), their inclusion in the design of help-seeking interventions alongside adolescents and doctors would be advantageous. Additionally, broader socio-cultural change enabling children to engage fathers as a source for emotional support could also be developed. There is therefore a need for future research to explore creative ways to increase help-seeking in young people.
Study limitations and recommendations
The study had several limitations: the survey was cross-sectional, restricting development of cause and effect relationships; it relied on self-report which, given the sensitive nature of the topic and its associated stigma, may have inhibited some participants in their responses; also more females took part than males – although the sample met the criteria for SEM analysis a more gender-balanced sample could have been recruited. Future research could consider the longer-term effects of help-seeking through longitudinal follow-up. Furthermore, clinician reports of mental illness and views of parents would provide more detail on what illness those adolescents are experiencing who did not initially want to seek help. By taking an approach that goes beyond surveying young people alone, but also their family may provide a more comprehensive description of the young people’s mental health.
Finally, the Theory of Planned Behaviour along with family activity and family life variables provide a useful framework on which to assess adolescent mental health help-seeking from family and medical doctors. The attitude towards doctor help, prosocial behaviour (Subjective norms) and confidence in discussing mental health with a doctor (Perceived Behavioural Control) predicted intentions to seek help from both a medical professional and from family. Our findings demonstrate for the first time how the TPB can be integrated with the protective factors of family life and family activities in supporting adolescent mental health. Specifically, public health campaign designers seeking to promote help seeking in adolescents could go through the TPB constructs and produce ideas of how their messages align to encouraging positive attitudes towards help-seeking, showing that other adolescents seek help as it is normal to seek help (subjective norms) and encouraging competence (perceived behavioural control) in asking for support. We recommend that further longitudinal research is conducted into adolescent mental health help seeking. But we are also cautious, as one UK based research study found that, while three quarters of parents seek help on their child’s behalf, only one quarter receive any (Khan, Citation2016), raising systemic issues of concern in service delivery that goes beyond help-seeking. While an estimated 29% of people are affected by a mental disorder in their lifetime (Steel et al., Citation2014), few adolescents with a diagnosable mental illness will ever receive professional help (Meltzer et al., Citation2003). More creative ways of engagement with young people is required to support their confidence in help-seeking, with the provision of adequate follow up services.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Additional information
Funding
Notes on contributors
Gavin Breslin
Dr. Gavin Breslin, is a Senior Lecturer in Psychology researching mental health and wellbeing in young people.
Stephen Shannon
Dr. Stephen Shannon, is a Lecturer in Sport and Exercise with a focus on children's wellbeing and physical activity.
Garry Prentice
Dr. Garry Prentice, is a Lecturer in Psychology and researcher in addiction, health and quantitative research methods.
Michael Rosato
Dr. Michael Rosato, is a Senior Research Fellow and Epidemiologist in mental health.
Gerard Leavey
Professor Gerard Leavey, is the Director of the Bamford Centre for Mental Health and Wellbeing, at Ulster University.
References
- Ajzen, I. (1985). From intentions to actions: A theory of planned behavior. In J. Kuhl & J. Beckman (Eds.), Action-control: From cognition to behavior (pp. 11–39). Springer.
- Ajzen, I. (1991). The theory of planned behavior. Organizational behavior and human decision processes, 50(2), 179–211.
- Ajzen, I. (2011). The theory of planned behaviour: Reactions and reflections. Psychology & Health, 26(9), 1113–1127. https://doi.org/10.1080/08870446.2011.613995
- Ajzen, I., & Fishbein, M. (1977). Attitude-behavior relations: A theoretical analysis and review of empirical research. Psychological Bulletin, 84(5), 888–918. https://doi.org/10.1037/0033-2909.84.5.888
- Bohon, L. M., Cotter, K. A., Kravitz, R. L., Cello, P. C., Jr., & Fernandez y Garcia, E. (2016). The theory of planned behavior as it predicts potential intention to seek mental health services for depression among college students. Journal of American College Health, 64(8), 593–603. https://doi.org/10.1080/07448481.2016.1207646
- Breslin, G., & McCay, N. (2013). Perceived control over physical and mental well-being: The effects of gender, age and social class. Journal of Health Psychology, 18(1), 38–45. https://doi.org/10.1177/1359105312438600
- Breslin, G., Shannon, S., Ferguson, K., Devlin, S., Haughey, T., & Prentice, G. (2019). Predicting athlete mental health stigma using the theory of reasoned action framework. Journal of Clinical Sport Psychology, 13(1), 103–115. https://doi.org/10.1123/jcsp.2017-0055
- Clement, S., Schauman, O., Graham, T., Maggioni, F., Evans-Lacko, S., Bezborodovs, N., Morgan, C., Rüsch, N., Brown, J. S. L., & Thornicroft, G. (2015). What is the impact of mental health-related stigma on help-seeking? A systematic review of quantitative and qualitative studies. Psychological Medicine, 45(1), 11–27. https://doi.org/10.1017/S0033291714000129
- Corry, D., & Leavey, G. (2016). Adolescent trust and primary care: Help-seeking for emotional and psychological difficulties. Journal of Adolescence, 54, 1–8. https://doi.org/10.1016/j.adolescence.2016.11.003
- Damghanian, M., & Alijanzadeh, M. (2018). Theory of planned behavior, self-stigma, and perceived barriers explains the behavior of seeking mental health services for people at risk of affective disorders. Social Health and Behavior, 1(2), 54–61. https://doi.org/10.4103/SHB.SHB_27_18
- Department of Health. (2018). Mental health of children and young people in England. 2017 London NHS Digital.
- Divin, N., Harper, P., Curran, E., Corry, D., & Leavey, G. (2018). Help-seeking measures and their use in adolescents: A systematic review. Adolescent Research Review, 3(1), 113–122. https://doi.org/10.1007/s40894-017-0078-8
- Goodman, R., Meltzer, H., & Bailey, V. (1998). The strengths and difficulties questionnaire: A pilot study on the validity of the self-report version. European Child & Adolescent Psychiatry, 7(3), 125–130. https://doi.org/10.1007/s007870050057
- Hagger, M. S., & Chatzisarantis, N. L. (2014). An integrated behavior change model for physical activity. Exercise and Sport Sciences Reviews, 42(2), 62–69. https://doi.org/10.1249/JES.0000000000000008
- Harding, S., Read, U. M., Molaodi, O. R., Cassidy, A., Maynard, M. J., Lenguerrand, E., Astell-Burt, T., Teyhan, A., Whitrow, M., & Enayat, Z. E. (2015). The determinants of young adult social well-being and health (DASH) study: Diversity, psychosocial determinants and health. Social Psychiatry and Psychiatric Epidemiology, 50(8), 1173–1188. https://doi.org/10.1007/s00127-015-1047-9
- Harding, S., Rosato, M., & Cruickshank, J. K. (2004). Lack of change in birthweights of infants by generational status among Indian, Pakistani, Bangladeshi, Black Caribbean and Black African mothers in a British cohort study. International Journal of Epidemiology, 33(6), 1279–1285. https://doi.org/10.1093/ije/dyh186
- Howard, S., Dryden, J., & Johnson, B. (1999). Childhood resilience: Review and critique of literature. Oxford Review of Education, 25(3), 307–323. https://doi.org/10.1080/030549899104008
- Hu, L. T., & Bentler, P. M. (1999). Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Structural Equation Modeling: A Multidisciplinary Journal, 6(1), 1–55. https://doi.org/10.1080/10705519909540118
- Jacquez, F., Vaughn, L. M., & Wagner, E. (2013). Youth as partners, participants or passive recipients: A review of children and adolescents in community-based participatory research (CBPR). American Journal of Community Psychology, 51(1-2), 176–189. https://doi.org/10.1007/s10464-012-9533-7
- Kessler, R. C., Berglund, P., Demler, O., Jin, R., Merikangas, K. R., & Walters, E. E. (2005). Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the national comorbidity survey replication. Archives of General Psychiatry, 62(6), 593–602. https://doi.org/10.1001/archpsyc.62.6.593
- Khan, L. (2016). Missed opportunities: A review of recent evidence into children and young people’s mental health, centre for mental health 2016 & annual report of the chief medical officer 2012, our children deserve better. Prevention Pays.
- Lai, E. T. C., Wickham, S., Law, C., Whitehead, M., Barr, D., & Taylor-Robinson, D. (2019). Poverty dynamics and health in late childhood in the UK: Evidence from the millennium cohort study. Archives of Disease in Childhood, 104(11), 1049–1055. https://doi.org/10.1136/archdischild-2018-316702
- Leavey, G., Rosato, M., Harding, S., Corry, D., Divin, N., & Breslin, G. (2020). Adolescent mental health problems, suicidality and seeking help from general practice: A cross-sectional study (Northern Ireland Schools and Wellbeing study). Journal of Affective Disorders, 274(1), 535–544. https://doi.org/10.1016/j.jad.2020.05.083
- Leavey, G., Rothi, D., & Paul, R. (2011). Trust, autonomy and relationships: The help-seeking preferences of young people in secondary level schools in London (UK). Journal of Adolescence, 34(4), 685–693. https://doi.org/10.1016/j.adolescence.2010.09.004
- Lessof, C., Ross, A., Brind, R., Bell, E., & Newton, S. (2016). Longitudinal study of young people in England cohort 2: Health and wellbeing at wave 2. Department for Education.
- McEachan, R. R. C., Conner, M., Taylor, N. J., & Lawton, R. J. (2011). Prospective prediction of health-related behaviours with the theory of planned behaviour: A meta-analysis. Health Psychology Review, 5(2), 97–144. https://doi.org/10.1080/17437199.2010.521684
- Meltzer, H., Gatward, R., Goodman, R., & Ford, T. (2003). Mental health of children and adolescents in Great Britain. International Review of Psychiatry, 15(1-2), 185–187. https://doi.org/10.1080/0954026021000046155
- Merikangas, K. R., He, J. P., Burstein, M., Swanson, S. A., Avenevoli, S., Cui, L., Benjet, C., Georgiades, K., & Swendsen, J. (2010). Lifetime prevalence of mental disorders in US adolescents: Results from the national comorbidity survey replication–adolescent supplement (NCS-A). Journal of the American Academy of Child & Adolescent Psychiatry, 49(10), 980–989. https://doi.org/10.1016/j.jaac.2010.05.017
- National Institute for Health and Care Excellence. (2014). Behaviour change: individual approaches Public health guideline. Retrieved September 21, 2020, from www.nice.org.uk/guidance/ph49
- Nearchou, F. A., Bird, N., Costello, A., Duggan, S., Gilroy, J., Long, R., McHugh, L., & Hennessy, E. (2018). Personal and perceived public mental-health stigma as predictors of help-seeking intentions in adolescents. Journal of Adolescence, 66, 83–90. https://doi.org/10.1016/j.adolescence.2018.05.003
- Pescosolido, B. A., & Boyer, C. A. (1999). How do people come to use mental health services? Current knowledge and changing perspectives. In A. V. Horwitz & T. Sheid (Eds.), A handbook for the study of mental health: Social contexts, theories and systems (pp. 392–411). Cambridge University Press.
- Rickwood, D., Deane, F. P., Wilson, C. J., & Ciarrochi, J. (2005). Young people’s help-seeking for mental health problems. Australian E-Journal for the Advancement of Mental Health, 4(3), 218–251. https://doi.org/10.5172/jamh.4.3.218
- Schomerus, G., Matschinger, H., & Angermeyer, M. (2009). Attitudes that determine willingness to seek psychiatric help for depression: A representative population survey applying the theory of planned behaviour. Psychological Medicine, 39(11), 1855–1865. https://doi.org/10.1017/S0033291709005832
- Steel, Z., Marnane, C., Iranpour, C., Chey, T., Jackson, J. W., Patel, V., & Silove, D. (2014). The global prevalence of common mental disorders: A systematic review and meta-analysis 1980–2013. International Journal of Epidemiology, 43(2), 476–493. https://doi.org/10.1093/ije/dyu038
- Thackeray, R., & Hunter, M. (2010). Empowering youth: Use of technology in advocacy to affect social change. Journal of Computer-Mediated Communication, 15(4), 575–591. https://doi.org/10.1111/j.1083-6101.2009.01503.x
- Van Brakel, W. H. (2006). Measuring health-related stigma—A literature review. Psychology, Health & Medicine, 11(3), 307–334. https://doi.org/10.1080/13548500600595160
- World Health Organization. (2013). Mental health action plan 2013–2020.
