
ABSTRACT
Workers in varied non-clinical settings are often exposed to dying and death in the community. This scoping review aimed to explore the physical and psychosocial Work Health and Safety impacts of exposures to death on workers in non-clinical occupational roles, and their coping strategies. Electronic databases PsycINFO (Ovid), Medline (Ovid), AMED (EBSCO), CINAHL (EBSCO), and ProQuest Social Sciences were searched for peer reviewed research articles published between March 1971 and April 2022. PRISMA-ScR guidelines were followed. Three authors independently assessed articles for inclusion. Fifteen studies with exposure settings in first response, disaster relief, social services, funeral work and teaching were identified. Five main themes were developed and organised using a systems approach: Environment, Workplace, Job Demands, Impacts, and Coping. These findings demonstrate that exposure to the dying, the dead and their families in non-clinical settings impacts workers emotionally, physically, and behaviourally, suggesting the need for mitigation through work redesign.
The impacts on workers’ health and safety (WHS) for those dealing with dying and death have not been widely or comprehensively examined beyond healthcare worker exposures (Barnes et al., Citation2020; Roche, Darzins, Oakman, et al., Citation2022; Zheng et al., Citation2018). A scoping review by Roche, Darzins, Oakman, et al. (Citation2022) focused on workers in clinical contexts, finding they were impacted at a personal and professional level and were required to manage with minimal organisational support or resources to mitigate negative outcomes such as grief, stress, trauma and helplessness.
Non-clinical settings refer to domestic, community or public spaces, in which health care may be provided but has not been designed nor structured to be an actual healthcare setting. Exposure to dying and death is a WHS hazard that workers in non-clinical environments may also experience or may routinely encounter. These work environments are often uncontrolled, referring to work conditions that are not under the direct control of the workers or employer, for example public spaces where an accident or disaster has occurred. In non-clinical environments, workers may also perform their duties in volatile situations where family members are present and encounter extreme distress or even violence among the bereaved (Mainds & Jones, Citation2018; Nelson et al., Citation2020). Job demands will vary depending on the occupation and work context, but non-clinical settings can present a range of hazards to a person’s health and wellbeing that are difficult to predict and manage in uncontrolled and often unpredictable environments (Lawn et al., Citation2020; Terry et al., Citation2015).
Many workers encounter dying and death in the course of their work, but understanding of risks from these exposures, the impacts of dealing with dying and death, and their coping strategies is limited. Previous research has identified that exposure to dying and death at work can significantly impact social, emotional, physical and mental health (Renck et al., Citation2002; Roche, Darzins, Oakman, et al., Citation2022; Ursano et al., Citation1999). However, most research focused on workers in non-clinical settings has examined first or emergency-responders, with limited studies focused on the issues of exposure to dying or death in other occupational groups such as social or welfare services (Douglas, Citation2013; Gustavsson & MacEachron, Citation2002), protective services (Csikai et al., Citation2011), teachers (Hart & Garza, Citation2013) and funeral workers (Roche, Darzins, & Stuckey, Citation2022).
Previous research available into the health and well-being of non-clinical workers quantifies the impacts on those exposed to dying and death in non-clinical environments (Berger et al., Citation2011; Hom et al., Citation2018; Huang et al., Citation2013; Mishra et al., Citation2010). Findings from these quantitative studies suggest that exposure to dying and death may be an important determinant of health and wellbeing of workers in non-clinical settings. However, the methodology of these studies limits the understanding of real-world lived experiences of workers’ exposure to dying and death and impacts on their health and well-being, a gap which may be addressed in qualitative studies. Additionally, most previous quantitative research has focused primarily on the presence or frequency of exposures and the prevalence of clinical outcomes or symptoms rather than the nature of the experience. Qualitative studies which explore the experience of the workers may help with a richer understanding the underlying behaviours, attitudes and perceptions that determine workers’ health outcomes following exposure to dying and death (Tolley et al., Citation2016).
Further, a key finding of the qualitative scoping review by Roche, Darzins, Oakman, et al. (Citation2022) was that workers are embedded within their organisational systems, interconnected and influenced by the broader cultural and socio-political context, which is consistent with approaches to understanding WHS systems (Oakman et al., Citation2018). Utilising a systems framework may assist in understanding any influences of these determinants by examining the individual parts of the workplace environment, job demands (including exposure to dying and death), and workers experiences from the qualitative data (Oakman et al., Citation2018). Findings can then inform development of evidence-based interventions to address impacts on workers’ health and wellbeing.
To identify what is known about non-clinical workers’ experiences of dying and death to address gaps in the research and inform further investigation, a qualitative scoping review was conducted. Unlike a literature review, scoping reviews follow a systematic approach to map evidence on a topic and identify the main concepts, theories, sources, and knowledge gaps (Tricco et al., Citation2018). Scoping reviews are an ideal tool for understanding the extent and breadth of existing literature for a particular subject and rigorously examining emerging evidence when it is still unclear what other, more specific questions can be posed and valuably addressed by a more precise systematic review (Munn et al., Citation2018). The aim of this scoping review was to explore the physical and psychosocial WHS impacts of exposures to dying and death on workers in non-clinical occupational roles, and their coping strategies.
Methods
The scoping review followed a prescribed, rigorous, previously validated process. The five-stage framework Arksey and O’Malley (Citation2005) research methodology was used to conduct a scoping review by systematically mapping current peer reviewed qualitative research and identifying gaps in existing literature. Identification and selection of articles followed the process for Preferred Reporting Items for Systematic Reviews and Meta-Analyses for Scoping Review extension (PRISMA-ScR) guidelines (Tricco et al., Citation2018) (Appendix D).
Search strategy
Stage 1: identifying the research question
This review explored the physical and psychosocial WHS impacts on non-clinical workers of exposure to death within their occupational roles, and their coping strategies. Although workers exposed to death are employed across a range of settings, the focus of this search was on workers exposed in non-clinical environments in the community such as those working in emergency services, education, cemeteries, and disaster relief. The research question for the Scoping Review was ‘What is the worker experience of physical and psychosocial impacts of exposure to dying and death in non-clinical settings and how do they cope with these impacts?’
Stage 2: identifying relevant articles
The electronic databases Medline (Ovid), CINAHL (EBSCO), PsycINFO (Ovid), AMED (EBSCO), and ProQuest Social Sciences were searched on 20 March 2021 for peer reviewed research articles published between 20 March 1971 and 20 March 2021.
A selection of keywords based on the review questions or the main concepts of the research topic with similar terms or phrases that might also be used to describe these concepts were mapped using subject headings and medical subject headings (MeSH) terms from the databases (workers, death, impact, coping). The MeSH terms were broadly applied to encompass a diversity of study populations. The keywords were checked using trial searches to ensure key known articles were identified and were combined with search terms using Boolean operators and truncations, and then the concepts were searched in the databases (Appendix A). The search used the following inclusion criteria: peer-reviewed journal, qualitative or mixed methodology, English language, published between 20 March 1971 and 20 March 2021, and full-text availability. Mixed methods studies were included if they had separate qualitative data collection and analysis. Review articles were included if they contained qualitative research. Articles from 1971 onwards were selected to capture 50 years of data to identify any changes over time and two generations of workers to understand key factors which may have influenced their experiences.
An identical database search was completed on 29 April 2022, that yielded 68 articles published from 2021 to 2022, but no additional articles were identified that met the inclusion criteria.
Stage 3: article selection
A total of 3788 articles were identified in the initial search, and abstracts were entered into Covidence Systematic Review Software (Veritas Health Innovation, Citation2021) for review. Removal of 1278 duplicates left 2510 articles for title and abstract review (). All article abstracts were reviewed by two authors, all by NR with a second independent review of each by either RS or SD against the agreed inclusion and exclusion criteria established between these three authors (Appendix B).
Figure 1. PRISMA-ScR flow diagram of the scoping review process for article selection.
Any disagreements about article inclusion were managed through discussion with the three reviewing authors until consensus was achieved. This process excluded 2214 articles and 267 articles moved to full-text review. The same process was used by these three authors for full-text review with 252 articles excluded. The reasons for full-text article exclusion are detailed in the PRISMA-Scr (). Articles focused on the impacts of exposure to dying and death related to COVID-19 were excluded, due to the multifaceted and unusual nature of these exposures and variability of these study outcomes and data and reducing heterogeneity of included research. Fifteen articles were identified as relevant and included in the scoping review.
Stage 4: charting data
Three reviewers undertook data charting (NR, RS and SD). First, extraction criteria were developed and refined using Covidence Systematic Review Software (Veritas Health Innovation, Citation2021) with headings: Author; Date/Year; Type of literature (journal article, dissertation, literature review, systematic review); Publication/Journal; Title; Aim of the study; Country of study; Industry; Occupation/job title; Participant role and where they work; Location (metropolitan, regional, rural, all, unknown); Who services were provided to; Age of the dead (all ages, adult, children, infants); Participant age range; Years of experience in role; Frequency of exposure to death/type of exposure to death; Number of participants; Participant gender; Research design (qualitative, mixed methods, review); Ethics approval (yes/no/unclear); Methods (study methods, sampling method, data collection, data analysis); Outcomes/findings; Implications and relevance to our study; Author reported limitations; Reflections on article results/themes.
Second, using the data extraction criteria, two authors extracted, synthesised, and interpreted the materials according to the criteria, key outcomes, and relevant results and themes for each article using categories from the systems framework developed in Roche, Darzins, Oakman, et al. (Citation2022) to arrange the extracted data. The authors recorded their thoughts and reflections on emerging themes for each article. Data extraction from all included articles was completed by NR, with a second, independent data extraction for each article by either RS or SD. These three authors then discussed disagreements, key outcomes, and reflections on emerging themes from each article and consensus reached.
Third, reflexive thematic analysis (Braun & Clarke, Citation2019, Citation2022) was used by NR to synthesise themes across the included articles. Independent checking of the developed themes and comparing them back to the original articles were carried out independently by the other three authors – RS, SD, and JO.
Results
Summary of articles included
A total of 15 studies published between 1992 and 2022 were included in the review. The study identification process is summarised in using a PRISMA-ScR flowchart (Tricco et al., Citation2018).
General aspects of the literature
Methodologies for the selected studies included 13 qualitative and 2 mixed-methods studies. Most studies focused on Emergency Service worker populations. summarises the key characteristics and references for each of the included studies. For the purposes of readability within the results section, each of these studies has also been given an identification (ID) number in which is then further used as an identifier in the results text.
Table 1. Article ID, study reference and demographic information of the participants of included Studies/Articles.
The work context for most of the studies (n = 12) was in uncontrolled environments in the wider community, with the others conducted in cemeteries (n = 1), podiatry clinics (n = 1) and schools (n = 1) (). Of these studies, most focused on frontline first response or emergency health workers (n = 12), one on homeless-sector workers, one with teachers, and one with podiatrists. Participant numbers across the studies ranged from n = 9 to n = 700. Some 67% of the participants were male (n = 858) where studies specified gender. Across all studies, workers were exposed to dying/death of people of all ages.
Experiences and impacts on workers
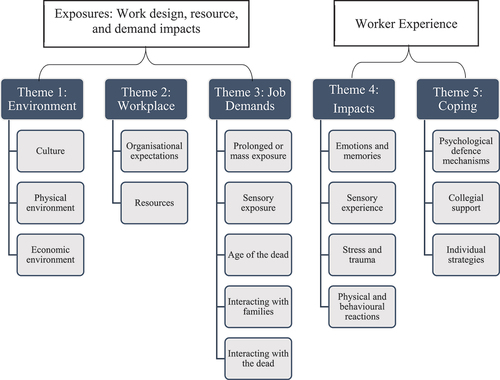
Following the thematic analysis (Braun & Clarke, Citation2022), 17 sub-themes were developed () and were organised into five themed categories (Environment, Workplace, Job Demands, Impacts and Coping) based on Roche, Darzins, Oakman, et al. (Citation2022) system’s framework.
Figure 2. Flowchart of themes.
The worker experience – themes and sub-themes
Workers experiences were impacted by the physical, cultural and economic environment associated with the context in which they were working. The subthemes focused on more specific elements of the general themes (Appendix C).
Theme 1: environment
The environment theme had three sub-themes, culture, and physical and economic environments, describing the influences and impacts of the context of the work exposures.
Culture
The cultural environment comprised the core community beliefs and social practices that lead to rules for workplace interactions, expectations, and practices for workers.
Cultural beliefs, values, and practices were found to influence perceptions of worker roles and informed diverse workplace practices.
Heroism
Workers in emergency services or rescue relief roles were often socially established as ‘heroes’ who risked their lives and health for the benefits of others [1, 2, 7, 15]. This led to the workers wanting to fulfil these expectations for the community such as ‘soldering on’ [2] and performing duties for ‘show’ such as Cardiopulmonary Resuscitation (CPR) when a person is clearly deceased [1]. ‘We perform CPR more for show. He was dead with a crushed face’ [1] and ‘ … doing all this fancy intervention lifesaving stuff and people still died’ [7].
Stigma
Conversely, workers whose duties were focused on the dead, rather than saving the dying, were not recognised within their culture as heroic, and they experienced stigma from the community [3, 4, 12]. Rescue volunteers felt that while they were performing a significant service for the dead and the families of the dead, community reinforcement of the value of their work was essential in addressing stigma [10].
Physical environment
The physical environment posed challenges for disaster relief workers, and was often described as overwhelming to the senses, with no private space or time for workers to process their immediate experiences [4, 5, 6, 10,12]. When working with the deceased, workers were often physically separated or isolated from others, which was felt to further perpetuate stigma and disconnect from colleagues [4, 12]. This separation and disconnect was highlighted in Flynn et al. (Citation2015), ‘The only time they [other workers] really even acknowledge that we’re on the compound is if they have to deal with us. If they don’t have to, we’re not even there’ [4].
Economic environment
Government funding was identified as inadequate to support the needs of different organisations, and their workers [8, 12]. Workers in social services [8] felt that some deaths of service users were preventable if greater capacity was available to ‘do more’ in supporting these people, which led to feelings of frustration and distress and a perception of unnecessary loss of life.
Theme 2: workplace
The workplace theme describes the impacts of the work context, resources, and role expectations that determine the occupational tasks and experiences workers face in their environments.
Organisational expectations
Organisational expectations arose from a workplace culture that centred around a sense of duty to serve the community [1, 3, 4, 6–13, 15]. This sometimes resulted in workers being expected to undertake tasks beyond their professional boundaries yet still perform efficiently and capably [1, 6, 9–13]. Workplaces reacting or responding to emergencies or disasters often had only vague expectations of how workers were expected to help, while many workers felt that their professional role boundaries were unclear, and roles were conflicted [1, 6, 10–13]. For example, firefighters in one study [1] identified that they were expected to attend emergency medical situations; however, medical care is not an extensive part of their training, resulting in unclear professional boundaries. Medically trained workers involved with mass retrieval of dead bodies, expressed confusion over their roles as medical professionals and a lack of direction in what they were meant to do: ‘What am I doing here? I cannot resuscitate anyone’ [6].
Teachers were expected to receive the news about a student's death and then immediately convey this news to their class with little instruction or support in approaching this very challenging task:
I come into the classroom without knowing how to get enough air to breathe …everyone is standing around and crying and screaming … total hysteria… and I have to manage all this now. What should I do?! I have no idea, I have no idea at the moment so I act according to my instincts… . [9]
Resources
Workplace resources included staffing, equipment, training, formal support and time. Social and professional support was seen as essential in all studies. Almost all workplaces experienced a lack of support, time, or training that had negative impacts on workers' ability to undertake tasks and their subsequent health and safety experience [1–14]. For example, firefighters in Abelsson (Citation2019) identified that decision-making was often based on intrinsic resources rather than evidence-based practice or procedures: ‘There is no right way, no template, it is a gut feeling, how to handle people. Some firefighters are better, and some are not so good at it’ [1]. Ambulance staff felt a lack of recognition from their employer and rare opportunities to debrief despite frequent exposure to traumatic death, or where support was available, that it was inappropriate and inadequate with support staff being ‘a bunch of volunteers’ from the same organisation [12]. In reactive and fast paced workplaces, workers were often not able to take any time or space to process emotions or reflect on their experiences [1–6, 8–14]. For example, cemetery workers reported that ‘the amount of work is so great, things overlap, but not for waste of time on our part’ and ‘we are forced to overload ourselves with work … I feel like crying … But what should I do? I keep it [in]!’ [3]. Having resources such as training, team support, situational preparation or debriefing was identified as protective factors in all studies.
Theme 3: job demands
Job demands experienced by the workers were influenced by the environmental conditions, in which they were required to work, and the duties required as part of their occupation. The nature and scale of the exposure to dying and death was a key factor in how their job demands affected their WHS experience.
Prolonged or mass exposure to death
The frequency and nature of exposure to death varied, depending on the work context and role. Six studies identified that the quantity of dying and death a worker was exposed to impacted on their health and safety. Quantity of exposure included prolonged contact or exposure to mass death [3, 4, 5,6, 10, 13]. McCarroll et al. (Citation1993) described this experience: ‘the bodies just kept coming and coming. It felt like you were surrounded’ [10], despite these disaster management workers expecting to be frequently exposed to death. Workers without expectations of dealing with death as part of their role, such as teachers and podiatrists, also reported these exposures as influencing their emotional reactions to death [9, 14], suggesting that impacts persisted despite expectations of this job demand.
Client age
Twelve studies reported that infants and children’s deaths were extremely emotionally challenging [1–3, 5, 7–9, 11–13, 15]. Levkovich and Duvshan’s (Citation2020) study of homeroom teachers reported, ‘I really couldn’t detach myself from it. It was truly like a mother mourning a child’ [9]. This distress was also reported by firefighters in Abelsson (Citation2019), ‘ … I touched something and felt relief – I told myself it was a dog. But then I realised that it was not a dog at all – it was a dead infant’ [5].
Sensory exposure
Job demands that included exposure to traumatic or mass death were described as sensory overload, or overwhelming senses including odours, sounds, and mutilated bodies [4–6, 8, 10, 13]. McCarroll et al. (Citation1993) described the impact of exposure to the smells of decomposing flesh and burned bodies, the sounds of saws cutting bone and the tactile experience of handling the bodies [10].
Interacting with families
Interactions with families included having to notify families of the death of a loved one or attempting to save the life of a person in front of their family. For most studies, these interactions were identified as a challenging and often distressing for workers to manage [1–5, 7, 8, 11, 12, 13, 14]. As identified by Abelsson (Citation2019), this could cause conflict when not knowing how to best manage these situations: ‘Relatives are running into the scene of the accident. You can’t stop a mother in a panic who wants to see her dead family in the car. Maybe it was good that she got to see’ [1].
Identifying with the dead
Identifying with the dead or with their family on a personal level, such as being reminded of a relative, also influenced the emotional impacts of the death [3–6, 8, 10, 12, 13]. ‘You realise that … wow … my son is at the age that this could happen’ [13]. This was relevant for cemetery workers who empathised with parents who had lost a child, ‘Many parents arrive who have lost their children, and for me, as a parent, I feel very bad’ [3]. Likewise, handling the personal effects of the dead frequently led to identification with the deceased or their family, which heightened distressful job demands [4, 6, 10].
Theme 4: impacts
The health and safety impacts on the workers were influenced by the environment, workplace and job demands. Individual impacts included emotional responses such as grief, sensory overload, stress and trauma. Workers also experienced behavioural changes and physical impacts.
Emotions and memories
All studies identified strong emotional reactions such as shock, anger, sadness, and helplessness, both immediately following exposure to death and then over time [1–15]. ‘You accumulate each accident and at the end your backpack is full. Then you need to vent the backpack’ [1]. Reactions included experiencing grief [4, 5, 7–9, 12–15] and guilt [5, 7–9, 12, 13, 15], and memories that still elicited these emotional reactions despite the passing of time since the death [2, 5–7, 9, 13]. ‘I really didn’t think he was going to die … I wasn’t prepared for that … Stuck with me for a while’ [6]. Unexpected or mass exposure to death also elicited very strong emotional reactions [2, 5–10, 12, 13, 15]. A participant in Lakeman (Citation2011) questioned their career choice following an unexpected death: ‘I think something happened inside me when that happened because I really did get affected by that, definitely something kind of … It made me question, Jesus, is this the job for me and is this what I want to do?’ [8]. The inability to maintain control over a person’s experience of dying or death, or their environment, led to feelings of vulnerability including powerlessness and a perception of loss of control [1–15] as highlighted by Fullerton et al. (Citation1992) ‘There was nothing more you could have done to save them … You feel helpless’ [5].
Sensory experience
The experience of exposure to the sensory job demands associated with death (sight, hearing, smell, touch and taste) was often overwhelming for workers, resulting in various immediate symptoms such as anxiety, difficulty focusing, stress and fear, panic or shock [4–8, 10, 12, 13]. One participant in Keller and Bobo (Citation2002) described the experience of the smell as so intense that it ‘burnt his/her lungs’, heightening their sensitivity to rescue noises such as vehicle sirens [6]. Some experienced visceral responses such as disgust or repulsion [5–8. 10] that could linger despite the stimuli no longer being present [4–6, 10]. For example, Fullerton et al. (Citation1992) identified that some workers attempted repeated washing to get rid of the smells [6]. Flynn et al. (Citation2015) described how re-exposure to an odour associated with death could bring memories of the event flooding back: ‘My husband fixed ribs a few months ago and he accidentally burned them on the grill. I was like, ‘You’re gonna have to get it out of the house. I can’t smell it’ [4]. The sounds of people dying and being unable to assist were also re-lived by workers: ‘We heard the screams but could not get to them because the fire was too much. I think about that every Christmas’ [5].
Stress and trauma
Workers experienced high levels of stress associated with their job demands [1, 4, 5, 6, 7, 9, 11, 12, 13, 15]. The volume and workload of dealing with the dead was reported as stressful, as highlighted by cemetery worker: ‘we are forced to overload ourselves with work’ [4] and disaster relief:
You can’t allow yourself to get too wound up early in the shift because you may have to handle more that night. You may not be able to respond effectively to a later emergency if you become exhausted. [5]
Others identified their exposure to dying and death as traumatic, with Nelson et al. (Citation2020) describing impacts related to particular exposures: ‘Our crews went out to [colleague’s suicide] and that, as a group, affected us really badly’ [12]. Others described experiencing symptoms of burnout [2, 3, 9, 12, 13] and PTSD including severe anxiety, flashbacks, and persistent memories of the event [2, 4, 7, 9, 12, 13]. ‘I’d go to bed, I’d close my eyes, and there would be the lady doing a swan dive off the balcony again, as clear as you sitting in front of me’ [13].
Physical and behavioural reactions
Workers described physical and behavioural reactions including substance abuse [2, 7, 13], drinking alcohol [2, 7, 10–13], negative behaviours impacting personal relationships [1, 5–7, 9, 13] and emotional reactivity [6, 7, 9, 11]. Psychophysical reactions included musculoskeletal disorders [3], headaches, sleep difficulties and nightmares [5–10, 12, 13]. A participant in Regehr et al. (Citation2002) discussed the impact on their personal life: ‘I just basically burned out and fell into a pot of booze. Then I quit because it was killing me, killing my family, killing my work’, while for another, the emotional challenges of the work contributed to perpetrating family violence [13].
Theme 5: coping
Workers described how they coped with the impacts of exposure to death, using various considered strategies including environmental and workplace support and individual tactics. Most coping strategies relied on the individual worker to seek support and find ways to cope emotionally, behaviourally and spiritually outside their workplace.
Psychological coping mechanisms
Each of the included studies found that workers applied psychological defence mechanisms to cope with dying and death [1–15]. Avoidant coping strategies of detachment and compartmentalising experiences and emotions associated with exposure to dying and death, were the most common way workers coped [1, 2, 4–15]. Participants avoided discussing their work outside of the workplace, instead focusing on the work tasks to escape facing difficult emotions or mitigate feelings of helplessness and guilt [1, 6–8, 10, 11, 13, 15]. Regehr et al. (Citation2002) described how suppression of emotions impacted life outside work:
The coping mechanisms that I’ve developed for work unfortunately can have a slight negative impact at home because I’m utilising a coping mechanism (avoiding discussing impacts of job demands) that probably shouldn’t be utilised in that setting but I can’t go back and forth and that’s a problem, so that’s certainly the downside. [13]
One positive strategy utilised was to balance negative emotions with a sense of meaning or purpose [4, 6–8, 15]. Participants in Lakeman (Citation2011) discussed positively framing the dying or death as helpful: ‘He got the best service that we could possibly give him here, we kind of went above and beyond a lot of times …he was happy … ’ [8]. These psychological defense mechanisms allowed workers to maintain the professional facade expected of them by the community and other workers, through placing their emotions to one side, so they could focus on the demands of their job [1–15]. As a participant in Keller & Bobo (Citation2002) described: ‘Focusing intently so as to not allow horror to enter’ [6]. Closely associated to this focus was workers feeling like they had done everything they could for that person [1, 6, 7, 8, 10, 11, 13, 15]
Collegial support
Finding informal support from other colleagues was a frequently described coping strategy [1, 2, 4, 5, 7, 8, 10, 13, 15]. Supports included debriefing or sharing experiences with other colleagues or more experienced workers, to share in group processing: ‘The only one who can really understand your attitudes and feelings is the guy next to you’ [5]. Black humour [5, 6, 7, 10, 11] and rituals including attending funerals with colleagues were also helpful in coping [6–8, 9, 13]. ‘I mean like you see people shot in the head and you make jokes about it’ [7]. Many felt that people outside their work environment would not be able to understand and validate their experiences, or they did not want to burden others [1, 2, 4, 5, 7, 8, 10, 13, 15]. Their own families were often not seen or used as a source of support:
I just can’t go home and say ‘Hey honey, this is what happened with my day’. I don’t want to damage my husband. I can’t tell my kids about it because I don’t want to damage them … They don’t need that mental picture; they don’t deserve it. [4]
Many workers found debriefing with peers more helpful than formal professional support or training, and fundamental to coping [1, 2, 4, 5, 7, 8, 10, 13, 15]. ‘Talking about and processing the accident around the coffee table works in most situations. Discussions with colleagues were more relaxed [than with others] and not so contrived’ [1]. With no peer support workers felt disenfranchised and their experiences unnoticed which was a barrier to coping, perpetuating a culture of silence [3–4, 12].
Individual strategies
Most coping strategies relied on the individual worker to seek support and find ways to cope emotionally outside the workplace. Workers utilised self-care strategies such as physical exercise, spending time with family, and reflection to cope with their work demands, and personal health and wellbeing [5, 7, 8,13, 15]. For some, this included avoidant behaviours:
I would just keep riding and riding and riding and wherever I was at the end of 12 hours, I would just stop and either sleep at a gas station or sometimes I’d get a hotel or whatever. I guess it was an escape. [7]
Others also focused on creating positive meaning from their experiences and building individual capacity to increase mental preparedness for their work [1, 3, 4, 6–8, 15]. Training and experience were also identified as coping strategies, although many also felt this was not adequate to prepare for their experiences [5]. ‘There is no training that can prepare you for this’ [5].
Discussion
The aim of this scoping review was to identify how exposure to dying and death impacts workers and how they cope with these impacts. This scoping review identified 15 qualitative articles which addressed how workers in non-clinical settings experienced exposure to dying and death. This limited number of studies may, in part, reflect the difficulties associated with exploring socially challenging issues for both participants and researchers (Komaromy, Citation2020). The overall findings demonstrate that a range of workers in varied occupations are similarly impacted regardless of different exposures to dying and death as part of their work. Despite differences in the setting and nature of the exposure, in all studies, exposure to dying and death consistently impacted workers emotionally, physically, behaviourally, or socially. Issues identified were similar regardless of the time the study was undertaken, suggesting that despite possible changes in culture and job demands over time, workers experience similar impacts. Findings from this review, informed by the systems framework developed by Roche, Darzins, Oakman, et al. (Citation2022), suggest that the nature of the exposure and relationships between the environment, workplace resources and job demands affect how workers are impacted and how they cope. These findings indicated that common coping strategies were at an individual level rather than being initiated or resourced from the workplace.
The physical environments in which workers were exposed to dying and death were largely in uncontrolled and non-clinical settings. Some of these environments were considered high risk, such as post-disaster relief. In these non-clinical environments, dying and death are usually sudden, unexpected and/or traumatic, and linked to both short- and long-term negative health outcomes for workers (Myall et al., Citation2020; Naushad et al., Citation2019; Thormar et al., Citation2010). Despite encountering dying and death as an expected job demand for most workers, this expectation did not mitigate negative impacts and potentially contributed to experiencing anticipation anxiety (Grupe & Nitschke, Citation2013).
The cultural environment influenced the manner and nature of the experience of workers through their job demands. Sixty per cent of studies identified that workers experienced stigma or a misunderstanding of their professional role boundaries, which has implications for worker safety, wellbeing and individual identity (Bickmeier et al., Citation2014). Conversely, workers also experience being viewed as heroic. The concept of heroism implies an acceptance of self-sacrificial work duties and has been discussed in the context of health care workers with physical and psychologically harmful consequences (Halberg et al., Citation2021). The role of a ‘hero’ or ‘rescuer’ has been found to exacerbate posttraumatic reactions and can act as a barrier to seeking formal forms of post-incident support when workers have been placed in situations of extreme trauma, including exposure to death (Hill & Brunsden, Citation2009). This culturally imposed narrative may further contribute to negative health and safety impacts for these workers.
The type of job demands and exposures to dying and death impacted the experiences of workers. The degree of trauma associated with death, such as mass death, prolonged exposure, children or gruesome death, was related to emotional distress, anxiety, depression, substance abuse, risk of Post-Traumatic Stress Disorder (PTSD) and fatigue symptoms, which is consistent with previous research (Brooks et al., Citation2016; Ursano et al., Citation2017). Personal identification with dying or death, was also emotionally challenging and distressing and has been linked to higher rates of PTSD, complicated grief, greater intrusion, self-destructive and avoidant behaviours (Cetin et al., Citation2005; Haddock et al., Citation2017; Ursano et al., Citation1999). Dealing with families or death notification was also a challenge for workers, also associated with negative psychological consequences such as depression, anxiety, and PTSD (Johnson & Panagioti, Citation2018;).
The level of strain experienced by workers as a result of their death-related job demands was also determined by the resources, or lack of, to draw upon. Pressure to constantly save lives combined with inadequate resources is associated with detrimental impacts on workers' physical and emotional health (Pilbeam & Snow, Citation2022). Role ambiguity and having insufficient job-related information are associated with increased anxiety, secondary traumatisation and job burnout (Thormar et al., Citation2013).
Where organisational support and resources were lacking, workers found their own ways to cope with the emotional and mental demands of working with dying and death. This scoping review identified that coping was mostly managed at an individual level. All studies identified coping strategies which focused on avoidance such as compartmentalisation, suppressing emotion, or focusing on the needs of the dying, dead, or the bereaved, which is consistent with previous research in palliative care at a personal and organisational level (Ashby, Citation2017). Avoidance behaviours were experienced by workers in six studies, which is also a symptom of PTSD (Kashdan et al., Citation2010). Research on coping strategies suggests that avoidance and denial were associated with poorer outcomes for workers (Brooks et al., Citation2016). Further, if coping energy and efforts are significantly invested in suppression or avoidance, this may hinder efforts to engage in positive, pleasurable activities that can also mitigate the impacts of job demands (Kashdan et al., Citation2010).
One important protective factor for coping was for workers to feel they had done as much as they could to prevent death, respectfully deal with the body and assist the family of the bereaved. When the workers believed the workplace system could have done more to prevent a death but failed to do so due to limited resources, workers experienced more challenges in accepting the death. Not providing adequate resources that enable staff to know whether or not they have done all they can to prevent death has been identified as a challenge in community services (Csikai et al., Citation2011). Workers may be at risk of interpreting system failures (i.e. not having time to thoroughly assess the situation) as a personal failure.
That peers are important for debriefing is consistent with other studies focusing on coping strategies and interventions for managing workplace grief and stress (Bateman et al., Citation2012; Eng et al., Citation2015; Graham et al., Citation2019). Although workers felt peer debriefing was helpful, Harder et al. (Citation2020) identified a need for organisational support and formal debriefing following exposure to dying or death, but that evidence-based debriefing frameworks are lacking.
Although at the individual-level workers were able to employ their own coping strategies, this strategy does not address the mitigation of the impacts of job demands and work pressures that required emotional and cognitive energy and effort at a systems level regardless of the setting in which workers were employed.
The findings of this qualitative scoping review demonstrate the relationship between inadequate organisational resources such as emotional support, lack of appropriate training or addressing high work pressure demands, can affect workers and their ability to cope with exposure to dying and death at work, and subsequent negative consequences for worker’s health and wellbeing including relationships with their friends, family and others. Regardless of the cultural context of the exposure to dying and death, or the workplace types or settings, all workers experienced health and wellbeing impacts at both personal and professional levels.
Strengths and limitations
The purpose of a scoping review is to map the evidence, not to evaluate the quality of the evidence presented in the articles included in the review (Arksey & O’Malley, Citation2005). This weakness has the potential to limit the conclusions derived from scoping reviews (Grant & Booth, Citation2009). The inclusion of only peer reviewed articles improves the quality of evidence.
Additionally, only including studies published in English may create a potential reporting bias, particularly as the review identified cultural influences as a key influence on workers’ experience and cultures which were not included may have had different impacts. Studies from low resourced countries may have been omitted as a result of the language exclusion. As only three studies in this scoping review were not in an emergency service or frontline response setting, findings in those other settings may have been diluted. However, this finding demonstrates a paucity of literature in settings beyond emergency and first response in non-clinical environments.
This scoping review utilised a rigorous review process which included four reviewers, all experienced both as occupational health practitioners and academics (NR, RS, SD and JO) and auditing of the final thematic analysis. Included studies were from 1992 to 2022 to capture changes over time; however, the same issues emerged from earlier studies, suggesting that little has changed in how these workers are impacted in almost 30 years. Despite some inevitable changes to cultural environments, contexts and work practices over this time, the persistence of these themes enhances their relevance to contemporary practice.
Implications
The scoping review identified that further research is required on the impact of exposure to death for non-clinical or community workplaces and mitigation of impacts associated with death exposures including the efficacy of existing risk management strategies. Impacts on workers were experienced at an individual, familial, community, workplace, and cultural level, and we therefore need to address WHS of workers exposed to dying and death within their work and explore recommendations to reduce these risks. Research into exposure to dying and death as a specific occupational risk is necessary to understand how this affects workers, and to inform recommendations and policies to mitigate the impacts. The global COVID-19 pandemic has also posed additional demands on non-clinical workers, which is not well understood and provides a valuable opportunity to further explore the protective and risk factors for these workers dealing with death.
Conclusion
This scoping review provides a comprehensive summary of the experiences of dying and death for workers working in non-clinical settings and provides insights into the research and practice gaps. Workers experiences were impacted by the demands of their work, which was dependent on the contexts or environment associated with their role. Opportunities exist for the development of policies and resources to support workers in managing death and dying at work, regardless of their work environment or context.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Additional information
Notes on contributors
Natalie Roche
Natalie Roche is an Occupational Therapy academic at Australian Catholic University with more then 12 years experience working as an Occupational Therapist in Australia and the United Kingdom in community palliative care and vocational rehabilitation. She has over 6 years experience as a tertiary educator, leading coordinating and teaching units of study to undergraduate Occupational Therapy students. Natalie received her Master of Ergonomics, Safety and Health at La Trobe University with a research focus on funeral workers health and safety experiences. Natalie is currently completing a PhD at La Trobe University, investigating the impacts of exposure to death on workers.
Susan Darzins
Susan Darzins is an occupational therapy academic with more than 25 years’ experience as a tertiary level educator, leader and researcher. Susan worked for several years in Australia and Canada in the area of work health and safety, vocational assessment and work injury management. Her research in this area has included investigation of factors that influence heavy industry workers to use back protection behaviours, development of normative grip strength data in automotive workers and reliability of manual handling assessments. Her doctoral and post-doctoral research has investigated measurement of participation-related concepts; evaluation of health services aiming to support people’s ability to live in the community; and building evidence to support occupational therapy practice. She has local health sector, national, and international research collaborators. Susan has developed and led tertiary level curricula and programs of study and coordinated and taught units of study at both undergraduate and post-graduate level. She has extensive expertise in use of enquiry-based learning methods to create flexible learning structures that enable students to be engaged as directors of their own learning. Susan was a co-investigator in research attracting $AUS1.2 million in external funding investigating student learning outcomes from a simulated clinical placement when embedded in occupational therapy clinical training, as replacement for traditional clinical placement.
Jodi Oakman
Jodi Oakman is a Professor and head of the Centre for Ergonomics and Human Factors, La Trobe University. Her background is a mix of industry and academia and she has worked extensively in industry across a range of sectors including health, manufacturing and logistics. Her research is focused on the impact of work and organisations on employees’ health. She is focussed on using evidence to inform interventions in organisations. Some examples of current projects are on managing the psychosocial work environment, future of work health and safety and using evidence to guide risk management in organisations. Jodi’s team have developed tool to assist workplaces with a more comprehensive approach to managing work related musculoskeletal disorders.
Rwth Stuckey
Rwth Stuckey is an experienced OHS and ergonomics practitioner who has worked as an OHS, ergonomics consultant and occupational rehabilitation adviser for more than 40 years, in many industries across Australia and internationally. She coordinated and taught subjects in the Department of Epidemiology and Preventive Medicine at Monash University for over 20 years and commenced at La Trobe undertaking teaching and research role in 2009. Her current roles include Associate Professor and Course Coordinator in Ergonomics Safety and Health and Teaching and Learning Coordinator for the Department of Public Health. She has a keen interest in workers’ health, prevention and management of work-related injuries and the implementation of effective systems. Her current research interests are broad and include investigation of the efficacy of worker health and wellbeing programs; risks and exposures for musculoskeletal injuries and OHS risks related to homelessness. She has a long history of community based voluntary work and was awarded a Medal (OAM) of the Order of Australia in 2023 for Services to the Health of the Community.
References
- Abelsson, A. (2019). First response emergency care – Experiences described by firefighters. International Journal of Emergency Services, 8(3), 247–258. https://doi.org/10.1108/IJES-05-2018-0026
- Arksey, H., & O’Malley, L. (2005). Scoping studies: Towards a methodological framework. International Journal of Social Research Methodology, 8(1), 19–32. https://doi.org/10.1080/1364557032000119616
- Ashby, M. (2017). Unconscious dying: The lightly tilled soil of palliative care and psychodynamics. Mortality, 22(3), 209–223. https://doi.org/10.1080/13576275.2016.1255602
- Barbee, A. P., Fallat, M. E., Forest, R., McClure, M. E., Henry, K., & Cunningham, M. R. (2016). EMS perspectives on coping with child death in an out-of-hospital setting. Journal of Loss and Trauma, 21(6), 455–470. https://doi.org/10.1080/15325024.2015.1117929
- Barnes, S., Jordan, Z., & Broom, M. (2020). Health professionals’ experiences of grief associated with the death of pediatric patients: A systematic review. JBI Evidence Synthesis, 18(3), 459–515. https://doi.org/10.11124/JBISRIR-D-19-00156
- Bateman, S. T., Dixon, R., & Trozzi, M. (2012). The wrap-up: A unique forum to support pediatric residents when faced with the death of a child. Journal of Palliative Medicine, 15(12), 1329–1334. https://doi.org/10.1089/jpm.2012.0253
- Berger, W., Coutinho, E. S. F., Figueira, I., Marques-Portella, C., Luz, M. P., Neylan, T. C., Marmar, C. R., & Mendlowicz, M. V. (2011). Rescuers at risk: A systematic review and meta-regression analysis of the worldwide current prevalence and correlates of PTSD in rescue workers. Social Psychiatry & Psychiatric Epidemiology, 47(6), 1001–1011. https://doi.org/10.1007/s00127-011-0408-2
- Bickmeier, R., Lopina, E., & Rogelberg, S. G. (2014). Well-being and performance in the context of dirty work. In Veldhoven, Peccei, Riccardo, & Bickmeier, Robert M (Eds.), Well-being and performance at work: The role of context (pp. 37–52). Taylor and Francis.
- Braun, V., & Clarke, V. (2019). Reflecting on reflexive thematic analysis. Qualitative Research in Sport, Exercise & Health, 11(4), 589–597. https://doi.org/10.1080/2159676X.2019.1628806
- Braun, V., & Clarke, V. (2022). Thematic analysis : A practical guide to understanding and doing (1st ed.). SAGE.
- Brooks, S. K., Dunn, R., Amlôt, R., Greenberg, N., & James Rubin, G. (2016). Social and occupational factors associated with psychological distress and disorder among disaster responders: A systematic review. BMC Psychology, 4(1), 18–18. https://doi.org/10.1186/s40359-016-0120-9
- Cetin, M., Kose, S., Ebrinc, S., Yigit, S., Elhai, J. D., & Basoglu, C. (2005). Identification and posttraumatic stress disorder symptoms in rescue workers in the Marmara, Turkey, earthquake. Journal of Traumatic Stress, 18(5), 485–489. https://doi.org/10.1002/jts.20056
- Colombo, L., Emanuel, F., & Zito, M. (2019). Secondary traumatic stress: Relationship with symptoms, exhaustion, and emotions among cemetery workers. Frontiers in Psychology, 10, 633. https://doi.org/10.3389/fpsyg.2019.00633
- Csikai, E. L., Whalen, M., Otto, J., & Durkin, D. W. (2011). Adult Protective Services Workers’ experiences with serious illness and death. Journal of Elder Abuse & Neglect, 23(2), 169–189. https://doi.org/10.1080/08946566.2011.558788
- Douglas. (2013). Child welfare workers who experience the death of a child client. Administration in Social Work, 37(1), 59–72. https://doi.org/10.1080/03643107.2012.654903
- Eng, J., Schulman, E., Jhanwar, S. M., & Shah, M. K. (2015). Patient death debriefing sessions to support residents’ emotional reactions to patient deaths. Journal of Graduate Medical Education, 7(3), 430–436. https://doi.org/10.4300/JGME-D-14-00544.1
- Fernández-Aedo, I., Pérez-Urdiales, I., Unanue-Arza, S., García-Azpiazu, Z., & Ballesteros-Peña, S. (2017). A qualitative study about experiences and emotions of emergency medical technicians and out-of-hospital emergency nurses after performing cardiopulmonary resuscitation resulting in death. Enfermería Intensiva (English Ed), 28(2), 57–63. https://doi.org/10.1016/j.enfie.2016.10.001
- Flynn, B. W., McCarroll, J. E., & Biggs, Q. M. (2015). Stress and resilience in military mortuary workers: Care of the dead from battlefield to home. Death Studies, 39(2), 92–98. https://doi.org/10.1080/07481187.2014.893463
- Fullerton, C. S., McCarroll, J. E., Ursano, R. J., & Wright, K. M. (1992). Psychological responses of rescue workers: Fire fighters and trauma. American Journal of Orthopsychiatry, 62(3), 371–378. https://doi.org/10.1037/h0079363
- Graham, P., Zerbi, G., Norcross, W., Montross-Thomas, L., Lobbestael, L., & Davidson, J. (2019). Testing of a caregiver support team. Explore, 15(1), 19–26. https://doi.org/10.1016/j.explore.2018.07.004
- Grant, M. J., & Booth, A. (2009). A typology of reviews: An analysis of 14 review types and associated methodologies. Health Information & Libraries Journal, 26(2), 91–108. https://doi.org/10.1111/j.1471-1842.2009.00848.x
- Grupe, D. W., & Nitschke, J. B. (2013). Uncertainty and anticipation in anxiety: An integrated neurobiological and psychological perspective. Nature Reviews Neuroscience, 14(7), 488–501. https://doi.org/10.1038/nrn3524
- Gustavsson, N., & MacEachron, A. E. (2002). Death and the child welfare worker. Children & Youth Services Review, 24(12), 903–915. https://doi.org/10.1016/S0190-7409(02)00251-7
- Haddock, N., Poston, W. S. C., Jahnke, S. A., & Jitnarin, N. (2017). Alcohol Use and Problem Drinking among Women Firefighters. Women’s Health Issues, 27(6), 632–638. https://doi.org/10.1016/j.whi.2017.07.003
- Halberg, N., Jensen, P. S., & Larsen, T. S. (2021). We are not heroes—the flipside of the hero narrative amidst the COVID19‐pandemic: A Danish hospital ethnography. Journal of Advanced Nursing, 77(5), 2429–2436. https://doi.org/10.1111/jan.14811
- Halpern, J., Gurevich, M., Schwartz, B., & Brazeau, P. (2009). What makes an incident critical for ambulance workers? Emotional outcomes and implications for intervention. Work & Stress, 23(2), 173–189. https://doi.org/10.1080/02678370903057317
- Harder, N., Lemoine, J., & Harwood, R. (2020). Psychological outcomes of debriefing healthcare providers who experience expected and unexpected patient death in clinical or simulation experiences: A scoping review. Journal of Clinical Nursing, 29(3–4), 330–346. https://doi.org/10.1111/jocn.15085
- Hart, L., & Garza, Y. (2013). Teachers perceptions of effects of a Student’s death: A phenomenological study. Omega: Journal of Death and Dying, 66(4), 301–311. https://doi.org/10.2190/OM.66.4.b
- Hill, R., & Brunsden, V. (2009). ‘Heroes’ as victims: Role reversal in the fire andRescue service. The Irish Journal of Psychology, 30(1–2), 75–86. https://doi.org/10.1080/03033910.2009.10446299
- Hom, M. A., Stanley, I. H., Spencer‐Thomas, S., & Joiner, T. E. (2018). Exposure to suicide and suicide bereavement among women firefighters: Associated suicidality and psychiatric symptoms. Journal of Clinical Psychology, 74(12), 2219–2237. https://doi.org/10.1002/jclp.22674
- Huang, J., Liu, Q. Y., Li, J. L., Li, X. J., You, J., Zhang, L., Tian, C. F., & Luan, R. S. (2013). Post-traumatic stress disorder status in a rescue group after the Wenchuan earthquake relief. Neural Regeneration Research, 8(20), 1898–1906. https://doi.org/10.3969/j.issn.1673-5374.2013.20.009
- Johnson, J., & Panagioti, M. (2018). Interventions to improve the breaking of bad or difficult news by physicians, medical students, and Interns/Residents: A systematic review and meta-analysis. Academic Medicine, 93(9), 1400–1412. https://doi.org/10.1097/ACM.0000000000002308
- Kashdan, T. B., Breen, W. E., & Julian, T. (2010). Everyday strivings in war veterans with posttraumatic stress disorder: Suffering from a hyper-focus on avoidance and Emotion Regulation. Behaviour Therapy, 41(3), 350–363. https://doi.org/10.1016/j.beth.2009.09.003
- Keller, R. T., & Bobo, W. V. (2002). Handling human remains following the terrorist attack on the Pentagon: Experiences of 10 uniformed health care workers. Military Medicine, 167(9), 8–11. https://doi.org/10.1093/milmed/167.Suppl_4.8
- Komaromy, C. (2020). The performance of researching sensitive issues. Mortality, 25(3), 364–377. https://doi.org/10.1080/13576275.2019.1635104
- Lakeman, R. (2011). How homeless sector workers deal with the death of service users: A grounded theory study. Death Studies, 35(10), 925–948. https://doi.org/10.1080/07481187.2011.553328
- Lawn, S., Roberts, L., Willis, E., Couzner, L., Mohammadi, L., & Goble, E. (2020). The effects of emergency medical service work on the psychological, physical, and social well-being of ambulance personnel: A systematic review of qualitative research. BMC Psychiatry, 20(1), 348–348. https://doi.org/10.1186/s12888-020-02752-4
- Levkovich, I., & Duvshan, R. (2020). “I keep it together at work but fall apart at home”: The experience of Israeli homeroom teachers coping with the death of a student in their class. Omega: Journal of Death and Dying, 84(2), 474–490. https://doi.org/10.1177/0030222819899501
- Mainds, M., & Jones, C. (2018). Breaking bad news and managing family during an out-of-hospital cardiac arrest. Journal of Paramedic Practice: The Clinical Monthly for Emergency Care Professionals, 10(7), 292–299. https://doi.org/10.12968/jpar.2018.10.7.292
- McCarroll, J. E., Ursano, R. J., Wright, K. M., & Fullerton, C. S. (1993). Handling bodies after violent death: strategies for coping. The American Journal of Orthopsychiatry, 63(2), 209–214. https://doi.org/10.1037/h0079438
- Mishra, S., Goebert, D., Char, E., Dukes, P., & Ahmed, I. (2010). Trauma exposure and symptoms of post-traumatic stress disorder in emergency medical services personnel in Hawaii. Emergency Medicine Journal: EMJ, 27(9), 708–711. https://doi.org/10.1136/emj.2009.080622
- Mitchell, M., & Munro, A. (1996). The influence of the occupational culture on how police probationers learn to deal with incidents of sudden death. Issues in Criminological & Legal Psychology (special Issue), 25 , 47–53.
- Munn, Z., Peters, M. D. J., Stern, C., Tufanaru, C., McArthur, A., & Aromataris, E. (2018). Systematic review or scoping review? Guidance for authors when choosing between a systematic or scoping review approach. BMC Medical Research Methodology, 18(1), 143–143. https://doi.org/10.1186/s12874-018-0611-x
- Myall, M., Rowsell, A., Lund, S., Turnbull, J., Arber, M., Crouch, R., Pocock, H., Deakin, C., & Richardson, A. (2020). Death and dying in prehospital care: What are the experiences and issues for prehospital practitioners, families and bystanders? A scoping review. BMJ Open, 10(9), e036925. https://doi.org/10.1136/bmjopen-2020-036925
- Naushad, V. V., Bierens, J. J. L. M., Nishan, K. P., Firjeeth, C. P., Mohammad, O. H., Maliyakkal, A. M., Chalihadan, S., & Schreiber, M. D. (2019). A systematic review of the impact of disaster on the mental health of medical responders. Prehospital and Disaster Medicine, 34(6), 632–643. https://doi.org/10.1017/S1049023X19004874
- Nelson, P. A., Cordingley, L., Kapur, N., Chew-Graham, C. A., Shaw, J., Smith, S., McGale, B., & McDonnell, S. (2020). “We’re the first port of call’ – Perspectives of ambulance staff on responding to deaths by suicide: A qualitative study. Frontiers in Psychology, 11, 722. https://doi.org/10.3389/fpsyg.2020.00722
- Oakman, J., Macdonald, W., Bartram, T., Keegel, T., & Kinsman, N. (2018). Workplace risk management practices to prevent musculoskeletal and mental health disorders: What are the gaps? Safety Science, 101, 220–230. https://doi.org/10.1016/j.ssci.2017.09.004
- Pilbeam, C., & Snow, S. (2022). “Thank you for helping me remember a nightmare I wanted to forget”: Qualitative interviews exploring experiences of death and dying during COVID-19 in the UK for nurses redeployed to ICU. Mortality, 27(4), 459–475. https://doi.org/10.1080/13576275.2022.2144356
- Regehr, C., Goldberg, G., & Hughes, J. (2002). Exposure to human tragedy, empathy, and trauma in ambulance paramedics. American Journal of Orthopsychiatry, 72(4), 505–513. https://doi.org/10.1037/0002-9432.72.4.505
- Renck, B., Weisæth, L., & Skarbö, S. (2002). Stress reactions in police officers after a disaster rescue operation. Nordic Journal of Psychiatry, 56(1), 7–14. https://doi.org/10.1080/08039480252803855
- Robson, K., & Williams, C. M. (2017). Dealing with the death of a long term patient; what is the impact and how do podiatrists cope? Journal of Foot and Ankle Research, 10(1), 36. https://doi.org/10.1186/s13047-017-0219-0
- Roche, N., Darzins, S., Oakman, R., & Stuckey, J. (2022). Worker experiences of the work health and safety impacts of exposure to dying and death in clinical settings: A qualitative scoping review. Omega: Journal of Death and Dying, 003022282211179. https://doi.org/10.1177/00302228221117902
- Roche, N., Darzins, S., & Stuckey, R. (2022). Funeral industry workers’ work health and safety in Australia and Ireland. Omega: Journal of Death and Dying, 302228221075289. https://doi.org/10.1177/00302228221075289
- Terry, D., Lê, Q., Nguyen, U., & Hoang, H. (2015). Workplace health and safety issues among community nurses: A study regarding the impact on providing care to rural consumers. BMJ Open, 5(8), e008306. https://doi.org/10.1136/bmjopen-2015-008306
- Thormar, S. B., Gersons, B. P. R., Juen, B., Djakababa, M. N., Karlsson, T., & Olff, M. (2013). Organisational factors and mental health in community volunteers. The role of exposure, preparation, training, tasks assigned, and support. Anxiety, Stress & Coping, 26(6), 624–642. https://doi.org/10.1080/10615806.2012.743021
- Thormar, S. B., Gersons, B. P., Juen, B., Marschang, A., Djakababa, M. N., & Olff, M. (2010). The mental health impact of volunteering in a disaster setting. Journal of Nervous & Mental Disease, 198(8), 529–538. https://doi.org/10.1097/NMD.0b013e3181ea1fa9
- Tolley, E. (2016). Qualitative Methods in Public Health: A field Guide for applied research (2nd ed.). Jossey-Bass & Pfeiffer Imprints, Wiley.
- Tricco, A. C., Lillie, E., Zarin, W., O’Brien, K. K., Colquhoun, H., Levac, D., Moher, D., Peters, M., Horsley, T., Weeks, L., Hempel, S., Akl, E. A., Chang, C., McGowan, J., Stewart, L., Hartling, L., Aldcroft, A., Wilson, M. G., Garritty, C., … Straus, S. E. (2018). PRISMA extension for scoping reviews (PRISMA-ScR): Checklist and explanation. Annals of Internal Medicine, 169(7), 467–473. https://doi.org/10.7326/M18-0850
- Ursano, R. J., Fullerton, C. S., Vance, K., & Kao, T.-C. (1999). Posttraumatic stress disorder and identification in disaster workers. The American Journal of Psychiatry, 156(3), 353–359. https://doi.org/10.1176/ajp.156.3.353
- Ursano, R. J., Fullerton, C. S., Weisaeth, L., & Raphael, B. (Eds.). (2017). Textbook of disaster psychiatry. Cambridge University Press.
- Veritas Health Innovation. (2021). Covidence systematic review software [computer software]. www.covidence.org
- Zheng, R., Lee, S. F., & Bloomer, M. J. (2018). How nurses cope with patient death: A systematic review and qualitative meta-synthesis. Journal of Clinical Nursing, 27(1–2), e39–e49. https://doi.org/10.1111/jocn.13975
