
ABSTRACT
To meet the Sustainable Development Goals target of ending poverty “in all its forms”, it is critical to monitor progress towards poverty alleviation, including amongst people with disabilities. This research used data from a population-based nested case control studies (n=667) and compares monetary and multidimensional poverty levels amongst people with and without disabilities in the districts of Cam Le, Vietnam and Tanahun, Nepal. Overall, there were no significant differences in incidence of monetary poverty between people with and without disabilities. However, approximately half of people with disabilities were multidimensionally poor in both settings, twice as frequent as compared to people without disabilities. Amongst people with disabilities, multidimensional poverty was associated with having a functional limitation affecting cognition and self-care, disability severity and younger age. The high incidence of multidimensional poverty amongst people with disabilities even in the absence of monetary poverty indicates a need for social protection and other interventions.
Introduction
Disability and poverty are intimately linked, with the one reinforcing the other (Banks, Kuper, Polack, & Van Wouwe, Citation2017; Groce, Kett, Lang, & Trani, Citation2011; Palmer, Citation2011).Footnote1 The international community is increasingly recognising the importance of disability-inclusive poverty reduction strategies, most notably in the 2030 Sustainable Development Agenda (Palmer, Citation2011; United Nations, Citation2015b). For example, the 2030 Sustainable Development Goals (SDGs), which have been adopted by 193 countries, call for the disaggregation of all targets and indicators by disability so as to ‘leave no one behind’ from advances towards eliminating poverty (SDG 1) and other Goals (United Nations, Citation2015a, Citation2015b).
However, poverty is a complex concept to define, and consequently there is no consensus on a single best measurement approach. In its broadest definition, poverty can be described as ‘a state in which individuals or households show significant deficits in well-being’ (Barrientos, Citation2011).
Historically, monetary measures have been used, such as comparing an individual or household’s income against an absolute threshold or ‘poverty line’, below which they are classified as living in poverty (Laderchi, Saith, & Stewart, Citation2003). In addition to national poverty lines, the World Bank’s international poverty line of $1.90 per person per day (with 2011 purchasing power parity) is used to define and track ‘extreme poverty’ across countries (World Bank, Citation2015). Poverty may also be measured relatively, by comparing an individual or household’s income or expenditures against what is typically commanded by others in that setting (Laderchi et al., Citation2003). The diversity of poverty measurements is highlighted in the range of targets and indicators used to track progress towards the SDGs, particularly SDG 1, which seeks to ‘[e]nd poverty in all its forms’ (United Nations, Citation2017a). For example, the international poverty line and national poverty lines are the focus of SDG indicators 1.1.1 and 1.2.1, respectively, while relative monetary poverty is captured in SDG indicator 10.2.1 (United Nations, Citation2017a, Citation2017b).
While monetary measures are critical for assessing poverty, it is increasingly recognised that these indicators alone do not encompass all forms of deprivation and that poverty should be seen in multidimensional terms (Alkire & Foster, Citation2011; Trani, Bakhshi, Myers Tlapek, Lopez, & Gall, Citation2015). For example, the capability approach advanced by Sen recognises that while income and other financial resources are often necessary to achieving desired functionings, they are insufficient as measures of well-being (Sen, Citation1993). Individuals may face ‘conversion handicaps’ in translating these resources into desired ‘capabilities’ and ‘functionings,’ such as being healthy, employed or having access to healthcare, education and other essential services due to factors such as gender, location and disability. Directly measuring deprivation in these areas may better capture poverty and well-being than using monetary indicators alone (Nussbaum & Sen, Citation1993). Consequently, Multidimensional Poverty Indexes (MPIs), using the Alkire-Foster method, have been used by many governments, as well as the United Nations Development Programme (UNDP), to collate and analyse data on a range of multidimensional indicators of poverty (Alkire et al., Citation2015; UNDP, Citation2016). MPIs are used frequently in monitoring SDG indicator 1.2.2, which addresses ‘poverty in all its dimensions according to national definitions’ (United Nations, Citation2017a).
People with disabilities may face an increased risk of poverty across both monetary and multidimensional measures. Studies have found people with disabilities face high levels of absolute poverty using national or international poverty lines (Braithwaite & Mont, Citation2009; Mitra, Citation2017; Mitra, Posarac, & Vick, Citation2013), as well as relative poverty compared to others without disabilities in the same setting (Filmer, Citation2008; Hosseinpoor et al., Citation2013). Additionally, several studies have used MPIs to assess poverty among people with disabilities, with all finding a link between disability and multidimensional poverty (Mitra, Citation2006; Mitra et al., Citation2013; Trani et al., Citation2015; Trani & Loeb, Citation2012). However, few studies have compared both multidimensional and monetary poverty in a single sample, or explored predictors of different forms of poverty amongst people with disabilities.
Understanding in greater depth the experience of both monetary and multidimensional poverty among people with disabilities is important for informing policy responses. For example, social protection programmes are increasingly being adopted in low- and middle-income countries (LMICs) as a set of strategies for poverty reduction, with many targeted explicitly to people with disabilities (Barrientos, Citation2018; Gentilini & Omamo, Citation2011). More information on the lived experience of people with disabilities – who constitute 15% of the global population – is essential to better tailor programmes to meet their needs (World Health Organization & World Bank, Citation2011). Consequently, this study aimed to compare levels of and contributors to monetary and multidimensional poverty amongst adults with and without disabilities and their households in the districts of Cam Le, Vietnam and Tanahun, Nepal, districts which have implemented disability-targeted poverty reduction programmes.
Study methods
In both settings, data was collected through a population-based survey of disability, with a nested case-control study of adults, aged 18 + . Data collection was undertaken between May-June 2016 in Cam Le, Vietnam and August-October 2016 in Tanahun, Nepal. Ethical approval for this research was granted from the Ethics Committees at the London School of Hygiene & Tropical Medicine, the Nepal Health Research Council and the Hanoi Univeristy of Public Health.
This research was also part of a larger study on disability and social protection (Banks et al., Citation2019, Citation2019). The countries and districts were selected through interviews with in-country stakeholders and a rapid policy review (Walsham, Kuper, Banks, & Blanchet, Citation2018), due to having strong social protection systems in place to address poverty amongst people with disabilities (e.g. disability-targeted cash transfers) (Banks et al., Citation2019). Tanahun is part of Province No. 4 in the Hills region of Nepal and is predominantly rural, while Cam Le is an urban district of the province of Da Nang in the South-Central Coast region of Vietnam.
A two-stage sampling strategy was undertaken for the population-based survey. Each setting had a sample size for the population-based survey of 6,000 people ages five and over, based on an anticipated prevalence of disability of 5% and 80% response rate. For the first stage, population-proportionate-to-size sampling was used to select clusters (30 in Tanahun, 75 in Cam Le), using the most recent national census as the sampling frame. A cluster was the smallest administrative unit (Village Development Committee (VDC) ward in Nepal, Population Group in Vietnam). For the second stage, individuals within each cluster (200 for Tanahun, 80 for Cam Le) were enumerated using compact segment sampling. The household questionnaire contained information on household members (including disability status) and household-level socioeconomic status (e.g. income, assets, housing characteristics).
The population-based household survey measured disability amongst people ages five and over. However, for the purposes of this analysis, the sample is restricted to people ages 18 and older to allow for better comparability across poverty measures. The Washington Group Short Set and an accepted adaptation of the Washington Group Extended Set (Washington Short Set Enhanced) were used in Vietnam and Nepal, respectively, to screen for disability (Washington Group, Citation2017). These question sets have been validated in a range of contexts, including in LMICs, and have been recommended by the United Nations and other stakeholders for providing robust and comparable estimates of disability (Government of New Zealand, Citation2017). These tools focus on the level of difficulty (none, some, a lot or cannot do) an individual experiences in performing everyday activities. For this study, disability was defined using cut-offs recommended by Washington Group protocol (Washington Group on Disability Statistics, Citation2009, Citation2010).
For Nepal this included:
Reported ‘a lot of difficulty’ or ‘cannot do’ in at least one of the following domains: seeing, hearing, walking/climbing, communicating (understanding/being understood), remembering/concentrating, self-care, upper body strength, fine dexterity.
Reported experiencing symptoms of anxiety or depression ‘daily’, at a level described as ‘a lot’.
For Vietnam this included:
Reported ‘a lot of difficulty’ or ‘cannot do’ in at least one of the following domains: seeing, hearing, walking/climbing, communicating, remembering/concentrating, self-care.
Severity of disability was determined based on the level of functional difficulty: people who reported ‘cannot do’ for at least one domain were classified as having a severe disability, while people reporting no more than a ‘a lot of difficulty’ were classified as having a moderate disability (Mitra, Citation2017).
Any person identified during the population-based survey as having a disability was invited to participate in the case-control study. Each case with a disability was matched to a person without a disability (control), by sex, cluster and age (± 5 years). Controls could not be from a household with another member with a disability, to limit intra-household effects of disability. Further, only one control per household was permitted. The case control questionnaire explored in greater depth individual-level indicators of poverty, such as educational attainment, health, work status and social participation, and information from this questionnaire was used to create the multidimensional poverty measure.
Measuring poverty
The following measures were calculated to assess economic poverty, in line with SDG indicators:
Poverty headcount, using the international poverty line of $1.90 per person per day, with 2011 purchasing power parity (PPP) (SDG Indicator 1.1.1) and poverty gap.
Poverty headcount, using national poverty lines (SDG Indicator 1.2.1) and poverty gap.
Proportion of people living below 50% of median income (SDG Indicator 10.2.1).
All of the above measures used income data. Household heads reported average total household monthly income from all sources (including salary, remittances, gifts, social assistance transfers). Household income was equivalised using the OECD equivalence scale (OECD, Citationn.d.).
At the time of data collection, the national poverty line in Vietnam was VND 780,000 per person per month (equivalent to $3.82 per person per day with 2011 PPP) (General Statistics Office of Vietnam, Citation2018), while the poverty line in Nepal is NPR 19,262 per person per year (equivalent to $2.14 per person per day with 2011 PPP) (World Bank, Citation2020).
This study also measured multidimensional poverty. The Alkire-Foster (AF) method has been widely used for designing MPIs that are relevant to different contexts and study purposes (Alkire, Citation2007; Alkire & Foster, Citation2011). Under this approach, an MPI uses a set of dimensions and linked indicators in areas considered critical to the experience of poverty.
The AF method uses a double cut-off approach to assess poverty. First, deprivation cut-offs are set for each indicator as are relative weights, which reflects its relative contribution to poverty. The sum across all indicators in an MPI falls between 0 and 1, with 1 reflecting complete deprivation across all indicators and 0 indicating no deprivation in any indicator. Next, the individual’s weighted sum of deprivations is calculated and compared against a final cut-off k – the multidimensional poverty line – to determine if an individual is considered multidimensionally poor. Choice of indicators and dimensions, their weights and cut-offs, as well as the overall poverty cut-off k are subject to normative judgements and assumptions, such as on what are acceptable levels of deprivation and how important each indicator is to an individual’s experience of poverty. To improve the validity of these choices, participatory and expert-based approaches are recommended (Alkire & Santos, Citation2010). Further, robustness testing – particularly in the rank ordering (i.e. comparison of poverty levels between groups or areas) with different MPI structures and values of k – is also important for strengthening the utility of the MPI in informing policy decisions (Foster, McGillivray, & Seth, Citation2009).
Three measures are calculated when using the AF method. First, the poverty headcount (H), or incidence of multidimensional poverty, indicates the proportion of individuals in a population who are considered multidimensionally poor. Second, the average deprivation share or intensity (A) provides an indication of the intensity of poverty by calculating the average weighted proportion of deprivations that the poor experience (i.e. those below the poverty threshold). Finally, the adjusted headcount (M0), which is the product of H and A, presents a summary measure of both the breadth and depth of multidimensional poverty.
The measure used in this study included five dimensions (livelihoods, social inclusion, access to services, health and well-being and household living conditions) and 13 indicators (). These dimensions and indicators are relevant for adults (ages 18+) across the lifecycle and for people with and without disabilities. The selection of dimensions and indicators was based on a review of the literature of existing MPIs, including ones used in other studies exploring multidimensional poverty amongst people with disabilities (Alkire & Santos, Citation2010; Mitra, Citation2017; Trani et al., Citation2015). In addition, the selected indicators and dimensions are grounded within international and national conceptualisations of poverty, including the SDGs and United Nations Convention on the Rights of Persons with Disabilities (Devandas Aguilar, Citation2015; United Nations, Citation2015c). For example, food security, access to services and adequate living conditions are indicators of an individual and their household’s ability to meet basic needs, while indicators in work and health are important for developing stronger and more resilient livelihoods that can protect against persistent poverty. Further, indicators in social inclusion relate to agency and participation, which have been highlighted as importance in the experience of poverty, particularly amongst people with disabilities (Devandas Aguilar, Citation2015; Eide & Ingstad, Citation2013). Indicators measured at the individual-level were selected as much as possible to capture individual achievements and deprivations.
Table 1. Dimensions, indicators and weights for the multidimensional poverty measure
Indicators measured at the individual-level rather than the household-level were used when possible so as to best capture individual achievements and avoid masking intra-household inequalities. For the 13 indicators, seven are specific to individuals (livelihoods, voting, decision-making, individual access to water and sanitation, violence and health events) and the remainder (living conditions, spending on healthcare and food insecurity) are characteristics of the households in which they live. For each indicator, deprivation cut-offs are based primarily on international or national standards (see Appendix 1). The multidimensional poverty measure uses nested weights, in which dimensions are all given equal weighting, which is then subdivided amongst indicators in that dimension (Salazar, Díaz, & Pinzón, Citation2013). As such, each dimension is considered equally important in the experience of multidimensional poverty, as is each indicator within a poverty dimension. The poverty cut-off was equal to 30% (k = 0.30) – meaning if she/he is deprived in 30% or more of the weighted sum of indicators (equivalent to the weight of more than one dimension), the person is considered multidimensionally poor.
Robustness testing was undertaken to compare the effect of using different MPI structures, with differing indicator cut-offs and weighting structures (see Appendix 2 for details). Pairwise comparisons were then used to explore differences in the MPI rankings between people with and without disabilities in each of the MPI structures over varying values of the poverty cut-off k.
Multivariate logistic regression was used to compare indicators of monetary and multidimensional poverty between people with and without disabilities, and amongst people with disabilities. Regression analyses included adjustments for the individual’s age and gender and for Nepal, location (rural/urban). As Cam Le, Vietnam is all urban and relatively homogenous, a location variable was not included. Data was analysed using Stata 15.
Disability and poverty
Overall, 5,692 people were screened for disability in Nepal (response rate: 94.9%) and 6,705 people in Vietnam (response rate: 95.1%). In Nepal, 214 people were identified as having a disability (prevalence in age 5+: 3.8%, 95%CI: 3.3–4.3%), of whom 188 were ages 18 or older. In Cam Le (Vietnam), 150 people were identified as having a disability (prevalence in age 5+: 2.5%, 95% CI: 2.1–2.9%), of whom 137 were ages 18 or older. In both settings, disability prevalence increased significantly with age (p < 0.001) and in Nepal disability was slightly more prevalent in men after adjusting for age (4.5% vs 3.2%, p = 0.04).
All 137 people with disabilities aged 18 and older in Vietnam (100%) and 186 of 188 people with disabilities in Nepal (99%) agreed to take part in the case-control study and were matched to controls without disabilities (total response rates: 98.0% and 97.7% for Vietnam and Nepal, respectively). Although matching was imperfect when the sample was restricted to the subset of people aged 18+, cases and controls were still similar on key characteristics (no differences were significant) ().
Table 2. Characteristics of study sample (ages 18+)
Few people in either study setting were living in extreme poverty (5.2% in Vietnam and 9.4% in Nepal, amongst all case and control households), according to the international poverty line (). Given the small numbers, there was no significant difference in the poverty headcount or gap at the international poverty line. Similarly, there were no significant differences in monetary poverty headcount or gap using national poverty lines.
Table 3. Monetary poverty between households with and without members with disabilities
However, people with disabilities had significantly lower median incomes in both settings compared to people without disabilities. Median equivalised household income per capita was approximately a third less for people with disabilities in both Vietnam and Nepal.
People with disabilities were more likely to be deprived compared to people without disabilities in most of the indicators used in the MPI (). This difference was significant for nine of 13 indicators (work, voting, decision-making, sanitation and violence food security, health care spending, flooring and assets) in Nepal. In Vietnam, people with disabilities were significantly more likely to be deprived in six of 13 indicators (work, voting, decision-making, water, health event, violence).
Table 4. Deprivation by indicator (uncensored headcounts) amongst people with and without disabilities
Incidence of multidimensional poverty was at least twice as high amongst people with disabilities compared to people without disabilities in both Nepal and Vietnam (58.1% vs 25.8% in Nepal, p < 0.001; 45.3% vs 2.2% in Vietnam, p < 0.001) (). Amongst the multidimensionally poor, people with disabilities were deprived in about 40% of the weighted sum of indicators in each setting, which was significantly higher compared to people without disabilities in Nepal (p = 0.002), but not in Vietnam. Consequently, the adjusted headcount ratio (M0) amongst people with disabilities is much higher compared to people without disabilities in Nepal (0.244 vs 0.097, p < 0.001) and in Vietnam (0.163 vs 0.008, p < 0.001). Robustness testing of different MPI structures and cut-offs of k consistently found people with disabilities had a higher adjusted headcount ratio (M0) compared to people without disabilities (see Appendix 2).
Table 5. Incidence, intensity and multidimensional poverty amongst people with and without disabilities
Percent contribution to MPI amongst people with and without disabilities can be found in Appendix 3.
Comparing income and multidimensional poverty amongst people with disabilities
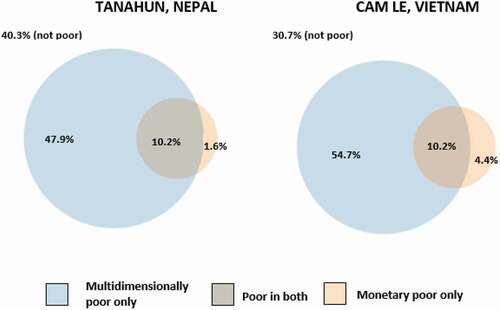
Amongst people with disabilities, 40.3% in Nepal and 30.7% in Vietnam were not poor by either monetary (using national poverty line) or multidimensional measures (). In Nepal, 10.2% were poor by both measures, while 47.9% were only multidimensionally poor. Only a small proportion of people with disabilities in Nepal were monetary poor only (1.6%). In Vietnam, 10.2% were poor by both measures, while 4.4% were monetary poor only and 54.7% were multidimensionally poor only.
Figure 1. Overlap between monetary (national poverty line) and multidimensional poverty headcounts, amongst people with disabilities
Amongst people with disabilities in both settings, multidimensional poverty was significantly more common amongst people with severe compared to moderate disabilities, and amongst people with functional limitations affecting self-care and cognition (). In Nepal, multidimensional poverty was also associated with female gender and negatively associated with old age (65+ years) and having a sensory limitation. In Vietnam, multidimensional poverty was less common amongst middle age adults (36–64 years) and more common amongst people with communication difficulties.
Table 6. Predictors of monetary and multidimensional poverty amongst people with disabilities from multivariate regression
There were few statistically significant predictors of monetary poverty amongst people with disabilities, given the small numbers of people with disabilities living below the national poverty line. However, rural location and receiving social assistance was associated with monetary poverty in Nepal.
Conclusion
This study found high levels of multidimensional poverty amongst people with disabilities, even in the absence of monetary poverty. Overall, approximately half of people with disabilities (45.3% in Vietnam, 58.1% in Nepal) were multidimensionally poor, which was more than double the incidence for people without disabilities. In contrast, there was no significant difference in the monetary poverty headcount or poverty gap using either the international or national poverty lines between people with and without disabilities, although the median household per capita income people with disabilities was significantly less (approximately a third of the income of people without disabilities).
Other studies, using different MPI structures, have similarly found high levels of multidimensional poverty amongst people with disabilities, and significant inequalities in comparison to people without disabilities (Mitra, Citation2017; Mitra et al., Citation2013; Pinilla-Roncancio & Alkire, Citation2017; Trani et al., Citation2015; Trani & Loeb, Citation2012). As with this study, inequalities between people with and without disabilities tend to be more apparent when using individual-level indicators compared to the household-level. For example, Pinilla-Roncancio & Alkire found disabled households were more likely to be multidimensionally poor compared to non-disabled households in only 4 of 11 LMICs when using the UNDP global MPI, in which all indicators are measured at the household-level (Pinilla-Roncancio & Alkire, Citation2017). In contrast, inclusion of individual-level indicators (e.g. employment status, health status, educational attainment) in other MPIs has evinced starker and more consistent differences between people with and without disabilities (Mitra, Citation2017; Mitra et al., Citation2013; Trani et al., Citation2015; Trani & Loeb, Citation2012). This finding underscores the importance of using individual- rather than household-level indicators of poverty and deprivation, as household-indicators may mask intra-household inequalities due to either a lower prioritisation in the division of household resources or additional barriers to meeting an adequate standard of living (Klasen & Lahoti, Citation2016). For example, access to clean water and sanitation is often measured at the household-level in the SDGs and the Global MPI. However, several studies have found people with disabilities may not use the same facility as other household members or in the same way (e.g. hygienically, independently and with dignity) (Banks, White et al., Citation2019; White et al., Citation2016). In this study, people with disabilities were more likely to be deprived compared to people without disabilities in indicators measured at the individual-level, such as those for social inclusion (voting, decision-making), violence, work and old age security, inequalities also found in other studies (Devries et al., Citation2018; Eide, Neupane, & Hem, Citation2016; Hughes et al., Citation2012; Mitra, Citation2017; Mizunoya & Mitra, Citation2013; Palmer, Citation2014).
Levels and contributors to multidimensional poverty differed between Vietnam and Nepal, reflecting differences in development between the two settings. Vietnam is a middle-income country, and Cam Le is an urban and relatively wealthy district, while Nepal is a low-income country and Tanahun is predominantly rural (World Bank, Citation2016). Consequently, most households with and without disabilities in Cam Le, Vietnam had met most basic needs (e.g. adequate housing conditions, minimum asset levels, improved sanitation and water sources, cooking fuel), while in Tanahun, Nepal, many households still do not have these needs fulfilled. As such, multidimensional poverty levels were lower in Vietnam than Nepal. However, inequalities between people with and without disabilities were higher in Vietnam, which may reflect the theory that as countries develop, people with disabilities are more likely to be excluded from progress (Groce et al., Citation2011).
Although this study did not find a significant difference in monetary poverty between people with and without disabilities in either context, it is likely that monetary poverty was underestimated. Notably, people with disabilities and their households frequently contend with additional disability-related expenses (e.g. personal assistance, additional medical or transportation costs, assistive devices) (Braithwaite & Mont, Citation2009; Hanass-Hancock, Nene, Deghaye, & Pillay, Citation2017; Mitra, Palmer, Kim, Mont, & Groce, Citation2017; Palmer et al., Citation2015). Diverting resources towards these costs can lower standard of living for a given level of income, relative to other households without members with disabilities who do not incur these costs (Mitra, Citation2006). As such, there is growing support for adjusting poverty lines to capture these extra disability-related costs (Braithwaite & Mont, Citation2009; Mitra et al., Citation2017). Other studies have found that incorporating these costs significantly increases the proportion of people with disabilities living in poverty. For example, Braithwaite & Mont estimated extra costs of disability at 9% and 14% of household income in Vietnam and Bosnia and Herzegovina, respectively (Braithwaite & Mont, Citation2009), which raised the prevalence of poverty among people with disabilities from 16.4% to 20.1% in Vietnam and 21.1% to 30.8% in Bosnia and Herzegovina. Similarly, in Cambodia, extra costs were estimated at 19% of household income, which nearly doubled poverty from 18% to 37% among households with members with disabilities (Palmer, Williams, & McPake, Citation2018). Finally, in China disability-related extra costs were ranged from 8–43%, which raised the national poverty prevalence amongst all households from 35.8% to 38.8% (Loyalka, Liu, Chen, & Zheng, Citation2014).
The presence of disability-related extra costs, as well as other ‘conversion handicaps’ may explain the high incidence of multidimensional poverty even in the absence of monetary poverty (Sen, Citation1993). Spending on disability-related extra costs reduces disposable income that could go towards achieving functionings (e.g. spending on assistive devices and accommodations instead of schooling), while unmet costs can impact capabilities (e.g. inability to travel to school due to the lack of an assistive device). Additionally, barriers such as inaccessible built environments and discrimination, which cannot be overcome by individual spending alone, may increase the risk of many forms of multidimensional poverty (e.g. exclusion from school and work, violence) amongst people with disabilities, even if their households are not facing monetary poverty.
This study also explored predictors of monetary or multidimensional poverty amongst people with disabilities. Multidimensional poverty was associated with disability severity – mirroring findings from Ethiopia, Malawi, Uganda and Tanzania (Mitra, Citation2017) – as was having functional limitations affecting self-care, cognition and, in Vietnam, communication. Monetary poverty, in contrast, was not significantly associated with disability severity or particular functional limitations. Other factors not explored in this study, such as whether the person with a disability is engaged in paid work and the quality of that work, or caregiving responsibilities of other household members, may better explain monetary poverty amongst people with disabilities. This study found that women with disabilities were more likely to be multidimensionally poor compared to men, although this association was only significant in Nepal. Other studies have also found women with disabilities face a higher risk of both monetary and multidimensional poverty, which may reflect the double disadvantage due to both disability and gender (Mitra, Citation2017; Trani et al., Citation2015).
Interestingly, receipt of social assistance was not protective against monetary or multidimensional poverty in either setting. In Nepal, social assistance was inversely associated with monetary poverty; however, this may reflect the eligibility criteria of some means-tested programmes. Further research is needed to explore how social protection and other poverty-reduction programmes could be improved in order to reduce both monetary and multidimensional forms of poverty amongst recipients with disabilities. In particular, research is needed to explore the magnitude of disability-related extra costs – both actual and needed expenditures (Mont & Cote, Citation2020) – and the extent to which they are covered through existing social protection schemes. Research from other settings indicates that there are likely gaps. For example, social health insurance schemes often do not cover assistive devices or disability-related health services, and so recipients with disabilities may still face impoverishing healthcare spending or (Banks, White et al., Citation2021, Citation2019; Palmer, Citation2014; Soltani, Takian, Sari, Majdzadeh, & Kamali, Citation2019). Similarly, cash transfer amounts are often too low to cover all needed expenses, particularly when eligibility is restricted to people who are also living in poverty (Hanass-Hancock & McKenzie, Citation2017; Mitra, Citation2010).
Several limitations should be considered when interpreting this study’s findings. First, households were the main unit of analysis for all monetary poverty measures and some indicators within the MPI, which assumes deprivations or resources are shared equally among all individuals. This assumption is questionable, particularly for people with disabilities, who may face discrimination within the household or additional barriers to participation. Second, differences in quality may be an issue for certain indicators in the MPI. For example, people with disabilities may be more likely to engage in less stable, lower paid work compared to people without disabilities, which is not captured in this study’s indicator for employment. Third, participatory approaches could strengthen the validity of the MPI, to ensure that the resulting structure is in line with how people with and without disabilities conceptualise poverty in both study settings. Finally, both settings have relatively well-functioning social protection systems, decent availability of disability supports and are wealthier than other areas of the country. Consequently, levels of poverty and inequality may be higher in other areas of Nepal and Vietnam. Exploring how and why poverty levels and inequalities differ in other districts is important for further research and informing policy decisions. For example, research in Vietnam found that the poverty gap between people with and without disabilities was attenuated in districts with better health care and infrastructure (Mont & Nguyen, Citation2018). Finally, the analyses of predictors of poverty, particularly monetary poverty, may have been underpowered to detect some differences amongst people with disabilities.
This study carries several important implications for policy and future research. For example, this study highlights the importance of using disability-sensitive indicators of poverty in tracking the SDGs and other development goals. This includes using indicators measured at the individual-level as much as possible, and capturing deprivations that are important for people with disabilities (e.g. attending school that is inclusive, access to accessible water and sanitation). Further, it is clear from this research that policy responses are needed to fulfil the SDG mandate of ‘no one left behind.’ Both Vietnam and Nepal have put in place social protection and other poverty-reduction programmes to address poverty among its citizens, including people with disabilities. However, as is, available policies and programmes appear insufficient to protect people with disabilities and their households from poverty. Increasing access to available programmes, as well as strengthening their design and delivery, may be required. For example, given the high incidence of multidimensional poverty even in the absence of monetary poverty, interventions addressing non-financial barriers to participation, such as inaccessible environments and discrimination, are needed in addition to cash transfers.
Supplemental Material
Download MS Word (1.4 MB)Disclosure statement
No potential conflict of interest was reported by the author(s).
Supplementary material
Supplemental data for this article can be accessed online.
Additional information
Funding
Notes on contributors
Lena Morgon Banks
Dr Lena Morgon Banks is an Assistant Professor of Disability Research at the London School of Hygiene & Tropical Medicine.
Monica Pinilla-Roncancio
Dr Monica Pinilla-Roncancio is an Assistant Professor at the Universidad de los Andes and the Director of Metrics and Policy at the Oxford Poverty and Human Development Initiative.
Matthew Walsham
Dr Matthew Walsham is a Research Associate at the Global Development Institute at the University of Manchester.
Hoang Van Minh
Dr Hoang Van Minh is a Professor and the Director of the Center for Population Health Sciences at the Hanoi University of Public Health.
Shailes Neupane
Shailes Neupane is the Director of the Valley Research Group
Vu Quynh Mai
Vu Quynh Mai is a Researcher with the Center for Population Health Sciences, Hanoi University of Public Health
Saurav Neupane
Saurav Neupane is a Research Officer with the Valley Research Group.
Karl Blanchet
Dr Karl Blanchet is a Professor in Humanitarian Public Health at the University of Geneva and Director of the Geneva Centre of Humanitarian Studies
Hannah Kuper
Dr Hannah Kuper is a Professor of Epidemiology and co-Director of the International Centre for Evidence in Disability at the London School of Hygiene & Tropical Medicine
Notes
1. Parts of this paper originally appeared in Paper 3, ‘Does disability increase the risk of poverty “in all its forms”?’ In: Investigating disability-inclusion in social protection programmes in low- and middle-income countries, with case studies from Vietnam and Nepal (Doctoral dissertation). London School of Hygiene & Tropical Medicine. Available at: https://researchonline.lshtm.ac.uk/id/eprint/4655981/2/2019_ITD_PhD_BANKS_M-Copy.pdf
References
- Alkire, S. (2007). Choosing dimensions: The capability approach and multidimensional poverty. Chronic Poverty Research Centre.
- Alkire, S., & Foster, J. (2011). Counting and multidimensional poverty measurement. Journal of Public Economics, 95(7), 476–487.
- Alkire, S., Foster, J., Seth, S., Santos, M. E., Roche, J. M., & Ballon, P. (2015). Multidimensional poverty measurement and analysis. Oxford, UK: Oxford University Press.
- Alkire, S., & Santos, M. E. (2010). Acute multidimensional poverty: A new index for developing countries.
- Banks, L. M., Hameed, S., Alghaib, O. A., Nyariki, E., Olenja, J., Kulsum, U., & Shakespeare, T. (2021). “It is too much for us”: Direct and indirect costs of disability amongst working-aged people with disabilities in Dhaka, Bangladesh and Nairobi, Kenya. Journal of Human Development and Capabilities, 1–24. doi:https://doi.org/10.1080/19452829.2021.1932774
- Banks, L. M., Kuper, H., Polack, S., & Van Wouwe, J. P. (2017). Poverty and disability in low-and middle-income countries: A systematic review. PloS One, 12(12), e0189996.
- Banks, L. M., Walsham, M., Minh, H. V., Duong, D. T. T., Ngan, T. T., Mai, V. Q., … Kuper, H. (2019). Access to social protection among people with disabilities: Evidence from Viet Nam. International Social Security Review, 72(1), 59–82.
- Banks, L. M., Walsham, M., Neupane, S., Neupane, S., Pradhananga, Y., Maharjan, M., … Kuper, H. (2019). Access to social protection among people with disabilities: mixed methods research from Tanahun, Nepal. The European Journal of Development Research, 31, 1–28.
- Banks, L. M., White, S., Biran, A., Wilbur, J., Neupane, S., Neupane, S., … Kuper, H. (2019). Are current approaches for measuring access to clean water and sanitation inclusive of people with disabilities? Comparison of individual-and household-level access between people with and without disabilities in the Tanahun district of Nepal. PloS One, 14(10), e0223557.
- Barrientos, A. (2011). Social protection and poverty. International Journal of Social Welfare, 20(3), 240–249.
- Barrientos, A. (2018). The informational basis of emerging social assistance in low and middle-income countries
- Braithwaite, J., & Mont, D. (2009). Disability and poverty: A survey of World Bank poverty assessments and implications. ALTER-European Journal of Disability Research/Revue Européenne De Recherche Sur Le Handicap, 3(3), 219–232.
- Devandas Aguilar, C. (2015). Report of the special rapporteur on the rights of persons with disabilities: United Nations general assembly 70th session. http://www.un.org/en/ga/search/view_doc.asp?symbol=A/70/297
- Devries, K., Kuper, H., Knight, L., Allen, E., Kyegombe, N., Banks, L. M., … Naker, D. (2018). Reducing physical violence toward primary school students with disabilities. Journal of Adolescent Health, 62(3), 303–310.
- Eide, A., & Ingstad, B. (2013). Disability and poverty–Reflections on research experiences in Africa and beyond. African Journal of Disability, 2(1). doi:https://doi.org/10.4102/ajod.v2i1.31
- Eide, A., Neupane, S., & Hem, K. G. (2016). Living conditions among people with disability in Nepal
- Filmer, D. (2008). Disability, poverty, and schooling in developing countries: Results from 14 household surveys. The World Bank Economic Review, 22(1), 141–163.
- Foster, J. E., McGillivray, M., & Seth, S. (2009). Rank robustness of composite indices: Dominance and ambiguity
- General Statistics Office of Vietnam. (2018). General poverty rate by residence and by region: Footnotes. Hanoi, Vietnam: Government of Vietnam.
- Gentilini, U., & Omamo, S. W. (2011). Social protection 2.0: Exploring issues, evidence and debates in a globalizing world. Food Policy, 36(3), 329–340.
- Government of New Zealand. (2017). Information on the Washington Group short set of questions on disability. Auckland, New Zealand: Government of New Zealand.
- Groce, N., Kett, M., Lang, R., & Trani, J.-F. (2011). Disability and poverty: The need for a more nuanced understanding of implications for development policy and practice. Third World Quarterly, 32(8), 1493–1513.
- Hanass-Hancock, J., & McKenzie, T. C. (2017). People with disabilities and income-related social protection measures in South Africa: Where is the gap? African Journal of Disability (Online), 6, 1–11.
- Hanass-Hancock, J., Nene, S., Deghaye, N., & Pillay, S. (2017). ‘These are not luxuries, it is essential for access to life’: Disability related out-of-pocket costs as a driver of economic vulnerability in South Africa. African Journal of Disability, 6(1), 1–10.
- Hosseinpoor, A. R., Stewart Williams, J. A., Gautam, J., Posarac, A., Officer, A., Verdes, E., … Chatterji, S. (2013). Socioeconomic inequality in disability among adults: A multicountry study using the world health survey. American Journal of Public Health, 103(7), 1278–1286.
- Hughes, K., Bellis, M. A., Jones, L., Wood, S., Bates, G., Eckley, L., … Officer, A. (2012). Prevalence and risk of violence against adults with disabilities: A systematic review and meta-analysis of observational studies. The Lancet, 379(9826), 1621–1629.
- Klasen, S., & Lahoti, R. (2016). How serious is the neglect of intra-household inequality in multi-dimensional poverty indices?
- Laderchi, C. R., Saith, R., & Stewart, F. (2003). Does it matter that we do not agree on the definition of poverty? A comparison of four approaches. Oxford Development Studies, 31(3), 243–274.
- Loyalka, P., Liu, L., Chen, G., & Zheng, X. (2014). The cost of disability in China. Demography, 51(1), 97–118.
- Mitra, S. (2006). The capability approach and disability. Journal of Disability Policy Studies, 16(4), 236–247.
- Mitra, S. (2010). Disability cash transfers in the context of poverty and unemployment: The case of South Africa. World Development, 38(12), 1692–1709.
- Mitra, S. (2017). Disability, health and human development. New York, USA: Springer.
- Mitra, S., Palmer, M., Kim, H., Mont, D., & Groce, N. (2017). Extra costs of living with a disability: A review and agenda for future research. Disability and Health Journal, 10(4), 475–484.
- Mitra, S., Posarac, A., & Vick, B. (2013). Disability and poverty in developing countries: A multidimensional study. World Development, 41, 1–18.
- Mizunoya, S., & Mitra, S. (2013). Is there a disability gap in employment rates in developing countries? World Development, 42, 28–43.
- Mont, D., & Cote, A. (2020). Considering the disability related extra costs in social protection
- Mont, D., & Nguyen, C. (2018). Spatial variation in the poverty gap between people with and without disabilities: Evidence from Vietnam. Social Indicators Research, 137(2), 745–763.
- Nussbaum, M., & Sen, A. (1993). The quality of life. Oxford, UK: Oxford University Press.
- OECD. (n.d.). What are equivalence scales?. http://www.oecd.org/els/soc/OECD-Note-EquivalenceScales.pdf
- Palmer, M. (2011). Disability and poverty: A conceptual review. Journal of Disability Policy Studies, 21(4), 210–218.
- Palmer, M. (2014). Inequalities in universal health coverage: Evidence from Vietnam. World Development, 64, 384–394.
- Palmer, M., Groce, N., Mont, D., Nguyen, O. H., Mitra, S., & Federici, S. (2015). The economic lives of people with disabilities in Vietnam. PloS One, 10(7), e0133623.
- Palmer, M., Williams, J., & McPake, B. (2018). Standard of living and disability in Cambodia. The Journal of Development Studies, 55, 1–21.
- Pinilla-Roncancio, M., & Alkire, S. (2017). How poor are people with disabilities around the globe? A multidimensional perspective
- Salazar, R. C. A., Díaz, B. Y., & Pinzón, R. P. (2013). A counting multidimensional poverty index in public policy context: The case of Colombia (No. 1907194495
- Sen, A. (1993). Capability and well-being. In A. Sen & M. Nussbaum (Eds.), The quality of life (Vol. 30). Oxford, UK: Oxford University Press.
- Soltani, S., Takian, A., Sari, A. A., Majdzadeh, R., & Kamali, M. (2019). Financial barriers to access to health services for adult people with disability in Iran: The challenges for universal health coverage. Iranian Journal of Public Health, 48(3), 508.
- Trani, J.-F., Bakhshi, P., Myers Tlapek, S., Lopez, D., & Gall, F. (2015). Disability and poverty in Morocco and Tunisia: A multidimensional approach. Journal of Human Development and Capabilities, 16(4), 518–548.
- Trani, J.-F., & Loeb, M. (2012). Poverty and disability: A vicious circle? Evidence from Afghanistan and Zambia. Journal of International Development, 24(S1), S19–S52.
- UNDP. (2016). Human development report 2016 http://hdr.undp.org/en/content/multidimensional-poverty-index-mpi
- United Nations. (2015a). Sustainable development goals officially adopted by 193 countries. Retrieved November 17 from
- United Nations. (2015b). Transforming our world: The 2030 Agenda for sustainable development
- United Nations. (2015c). Transforming our world: The 2030 agenda for sustainable development. General Assembley 70 session.
- United Nations. (2017a). Sustainable development goal 1: End poverty in all its forms everywhere. https://sustainabledevelopment.un.org/sdg1
- United Nations. (2017b). Sustainable development goal 10: Reduce inequalities within and among countries. United Nations. Retrieved August 27 from https://sustainabledevelopment.un.org/sdg10
- Walsham, M., Kuper, H., Banks, L. M., & Blanchet, K. (2018). Social protection for people with disabilities in Africa and Asia: A review of programmes for low-and middle-income countries. Oxford Development Studies. 1–16.
- Washington Group. (2017). Analytic guidelines: Creating disability identifiers using the Washington Group Extended Set (WG-ES) SPSS syntax. (http://www.washingtongroup-disability.com/wp-content/uploads/2016/12/WG-Document-6-Analytic-Guidelines-for-the-Washington-Group-Extended-Set.pdf
- Washington Group on Disability Statistics. (2009). Understanding and interpreting disability as measured using the Washington Group short set of questions
- Washington Group on Disability Statistics. (2010). The measurement of disability recommendations for the 2010 round of censuses http://www.washingtongroup-disability.com/wp-content/uploads/2016/02/recommendations_for_disability_measurement-1.pdf
- White, S., Kuper, H., Itimu-Phiri, A., Holm, R., Biran, A., & Federici, S. (2016). A qualitative study of barriers to accessing water, sanitation and hygiene for disabled people in Malawi. PloS One, 11(5), e0155043.
- World Bank. (2015). Global poverty line update. Retrieved from http://www.worldbank.org/en/topic/poverty/brief/global-poverty-line-faq
- World Bank. (2016). World bank analytical classifications: Historical classifications. Retrieved from https://datahelpdesk.worldbank.org/knowledgebase/articles/378834-how-does-the-world-bank-classify-countries
- World Bank. (2020). Poverty & equity brief: Nepal. June 1. Retrieved from https://databank.worldbank.org/data/download/poverty/987B9C90-CB9F-4D93-AE8C-750588BF00QA/SM2020/Global_POVEQ_NPL.pdf
- World Health Organization & World Bank. (2011). World report on disability. World Health Organization.