
Abstract
Objectives: The aim of this study was to explore if inner strength is independently associated with a reduced prevalence of depression after controlling for other known risk factors associated with depression.
Methods: A population-based cross-sectional study was performed, where all women living in Åland, a Finnish self-govern island community in the Baltic Sea, aged 65 years or older were sent a questionnaire including the Geriatric Depression Scale and the Inner Strength Scale along with several other questions related to depression. Factors associated with depression were analyzed by means of multivariate logistic regression.
Results: The results showed that 11.2% of the studied women (n = 1452) were depressed and that the prevalence increased with age and was as high as 20% in the oldest age group. Non-depressed women were more likely to never or seldom feel lonely, have a strong inner strength, take fewer prescription drugs, feeling needed, being able to engage in meaningful leisure activities, as well as cohabit.
Conclusion: Our results showed an association between stronger inner strength and being non-depressed. This can be interpreted to mean that inner strength might have a protective effect against depression. These findings are interesting from a health-promotion perspective, yet to verify these results, further longitudinal studies are required.
Introduction
Depression is the leading cause of disability worldwide, and it is a major contributor to the global burden of disease (World Health Organization, Citation2012). It is known that late-life depressions are common, underdiagnosed, and inadequately treated (Alexopoulos, Citation2005; Djernes, Citation2006; Petersson et al., Citation2014). Depression can worsen the outcomes of many other medical illnesses and can increase mortality (Alexopoulos, Citation2005) in addition to its negative effects on quality of life (Dingley & Roux, Citation2014).
Female gender and old age are known predictors of depressive disorders and depressive symptoms. So are chronic somatic diseases, functional impairment, institutionalization, lack or loss of social contacts or social support, living alone, history of depression or other psychiatric disorders, low education, smoking, adverse life events, cognitive impairments, pharmaceutical treatments, personality factors, and alcohol consumption (Djernes, Citation2006; Skoog, Citation2011). On the other hand, feeling valued and important, as well as religiousness, have been shown to be associated with fewer and reduced depressive symptoms (Chippendale, Citation2013; Smith, McCullough, & Poll, Citation2003). Furthermore, it appears that there is an inverse relationship between depression and high levels of inner strength. Depressive symptoms are negatively associated with inner strength among women survivors of cancer (Dingley & Roux, Citation2014), among women living with chronic health conditions (Lewis & Roux, Citation2011), and among the oldest old (Lundman et al., Citation2012). In a meta-theoretical study, a model of inner strength was developed (Lundman, Aléx, et al., Citation2010). Further, an instrument to estimate inner strength, Inner Strength Scale (ISS), was developed (Lundman et al, Citation2011). An inverse relationship between depression and high ISS scores has been found (Viglund, Jonsén, Lundman, Strandberg, & Nygren, Citation2013), and the ISS has been used to support the hypothesis that inner strength can partially mediate the relationship between disease and self-rated health (Viglund, Jonsen, Strandberg, Lundman, & Nygren, Citation2014).
Depression is a major threat to older women's health, and there are several known predictors of depressive disorders. From a health-promotion perspective, it is just as important to explore factors that can contribute to well-being as those that contribute to illness. It seems likely that inner strength, as described in a theoretical model and assessed by the ISS, might be associated with a reduced risk of depression, but there is still a knowledge gap within this field. The aim of this study, therefore, was to explore whether inner strength is independently associated with a reduced prevalence of depression after controlling for other factors known to be associated with depression.
Methods
The study was a population-based cross-sectional study carried out as part of a larger project studying inner strength and vulnerability among older women. The study was performed in Åland, a self-governing island community in Finland with about 28,500 inhabitants.
Sampling and participants
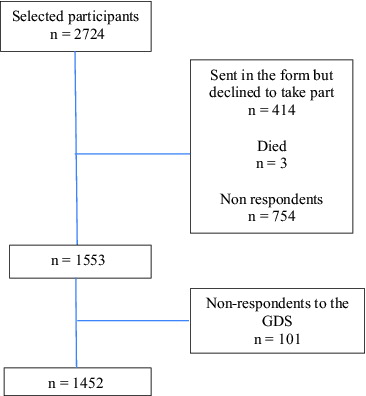
Every woman registered at the Local Register Office in Åland and born in or before 1945 (N = 2724) was sent a questionnaire in May of 2010. The questionnaire was sent by post along with a prepaid response envelope. A letter with general information, information about voluntary participation, as well as confidentiality of the data and presentation of the results was enclosed. A completed questionnaire was considered to be the consent to participate. After one reminder, 1553 women had answered and returned the questionnaire. The main focus of this study was depression, therefore, non-respondents (more than five missing items) on the Geriatric Depression Scale (GDS) part of the questionnaire were excluded from further analysis (n = 101) ending up with a total of 1452 participants (). The non-respondents to the GDS tended to be older (p < 0.001), were more likely to live alone (p < 0.001), and were more likely to have a diagnosed disease (p < 0.05).
Figure 1. Flowchart of participants.
Questionnaire
Geriatric Depression Scale
The GDS (Yesavage et al., Citation1983) was used to estimate depression. In this study, the 15-item version was used with a possible range of scores of 0–15 (Sheikh & Yesavage, Citation1986). According to Sheikh & Yesavage (Citation1986), scores of 5 or higher indicate depression. The 15-item version of the GDS is a well-validated tool for screening depression in older adults (Almeida & Almeida, Citation1999; Nyunt, Fones, Niti, & Ng, Citation2009; Sheikh & Yesavage, Citation1986). The GDS has also been shown to be useful for overall assessment of depressive symptoms even among very old people with impaired cognitive function (those with Mini-Mental State Examination scores of 10–17) (Conradsson et al., Citation2013). One to five missing items on the GDS led to imputation, e.g. if a person answered 12 of the 15 items and reported a score of 3 points, the total score was imputed to be (Aging Clinical Research Center (CitationACRC) website).
Inner Strength Scale
Inner strength was measured with the ISS (Lundman et al., Citation2011). The scale relies on the interaction of the dimensions of connectedness, firmness, flexibility, and creativity and consists of five items in each of the four dimensions. The responses are in the form of a Likert scale with responses ranging from 1 (totally disagree) to 6 (totally agree). All items were phrased positively, and the scores ranged from 20 to 120 with higher scores denoting higher degrees of inner strength. The ISS has been found to be a valid and reliable instrument for capturing a multifaceted understanding of inner strength with a Cronbach's alpha of 0.86 (Lundman et al., Citation2011). Cronbach's alpha in the current study was 0.92. When analyzing the scale, up to three missing values were accepted and were replaced with the mode values for the population.
Background characteristics
The questionnaire included questions about cohabiting and having children, as well as questions about having someone intimate to share both troubles and joy with. The women were also asked about their ability to carry out meaningful leisure activities, if they had been outdoors during the previous week, if they were taking part in volunteer work, and if they felt needed. The answer alternatives to all of these questions were Yes or No. The women were also asked if they believed in God or a higher power, and this was dichotomized into Yes or No (No or Indecisive). They were also asked to specify persons of importance for daily life functioning, including the answer alternative Nobody. The question was reformulated to ask whether they could manage without important others in their everyday life, and this was dichotomized into responses of Yes or No. To explore economic status, the respondents finished the sentence Regarding my finances…, and the three answer alternatives were dichotomized as Yes (I have enough money to cover costs and to save some/I have enough money but there is nothing left) or No (I do not have enough money). Education level was dichotomized into higher education (further studies than elementary school) or not. Two questions were related specifically to the women's health. The first was “How many different kinds of drugs from the pharmacy do you take on a regular basis?” and the second was about having a diagnosed disease (Yes or No) with the possibility to specify what kind of disease with some explicitly mentioned such as stroke, myocardial infarction, cancer, and diabetes.
Statistics
The data were analyzed using SPSS 21.0. Depression was the dependent variable and was dichotomized into non-depressed (GDS < 5) or depressed (GDS ≥ 5). Continuous variables were studied with Student's t-test, and the background characteristics were compared using the χ2 test. A p-value of <0.05 was regarded as statistically significant. Multicollinearity was controlled for by using Pearson's correlation coefficient analysis. None of the variables were excluded due to multicollinearity. Significant variables were entered into logistic regression analysis. Non-significant variables with the highest p-values were removed manually one by one until all variables were significant while still controlling for age. The result was compared with a backward logistic regression model by entering the same variables as the above model, and this led to a similar result.
Ethical considerations
The study was considered and approved by the ethical committee of Åland's Public Health Care Service on 20 November 2008.
Results
Characteristics of the participants are presented in . Of the 1452 participants, the mean age was 73.92 ± 7.16 years and the majority (96.5%) lived in their own homes. Indications of depression (GDS ≥ 5) were found among 11.2% (n = 162) of the participants. For those aged 65–69 years, the prevalence of depression was 5.9%; for those aged 70–74 years, it was 9.8%; for those aged 75–79 years, it was 12.5%; and for those aged 80+ years, it was 20%. Women with depression were significantly older (t = −6.29, 95% confidence interval (CI): −5.35 to −2.80), took a larger number of different drugs (t = −8.58, 95% CI: −3.35 to −2.10), and had significantly lower ISS scores (t = 10.47, 95% CI: 10.51–15.37) than the non-depressed.
Table 1. Characteristics of the participants with or without depression.
Logistic regression was performed to assess how well the associated variables explained depression and the relative importance of each variable. Initially, the model contained 15 independent variables (the significant variables from ). In the next step, the non-significant variables in the regression model were excluded one by one based on the highest p-values while still controlling for age. The final model contained the following six associated variables: never or seldom feeling lonely, inner strength, number of prescribed drugs, feeling needed, and being able to engage in meaningful leisure activities (). The model was significant and χ2 (6, n = 1187) = 245.99 (p < 0.001) indicating that it was able to distinguish between depressed and non-depressed respondents. The model as a whole explained between 18.7% (Cox and Snell R2) and 39.4% (Nagelkerke R2) of the variance in depression and correctly classified 90.1% of all cases. The ISS independently explained variance in depression even when controlling for other factors associated with depression (Odds ratio = 0.963, p < 0.001).
Table 2. Logistic regression predicting likelihood of reporting depression.
Discussion
The result of this study shows that 11.2% of the studied women were depressed and that the prevalence increased with age up to 20% in those 80 years of age or older. We have also shown that inner strength appears to be associated with a reduced risk of depression independent of other protective factors.
The strongest predictor of being non-depressed was never or seldom feeling lonely. Loneliness is a known risk factor (Bergendahl, Allard, Aléx, Lundman, & Gustafson, Citation2007; Cacioppo, Huges, Waite, Hawkley, & Thisted, Citation2006), but the relationship might have dual directions, and loneliness and depressive symptomatology can act synergistically to diminish well-being (Cacioppo et al., Citation2006). Feeling lonely is not the same as being alone (Hawley & Cacioppo, Citation2010), but expressing feelings of loneliness can be an indication of diminished social support. Our results also showed that being able to engage in meaningful leisure activities and feeling needed were independently associated with being non-depressed. This is also in line with previous studies, and reduced investment in leisure activities that include some form of social interaction (Adams, Roberts, & Cole, Citation2011) as well as reduced investment in overall leisure activities (Lee et al., Citation2012) has been shown to increase the risk for depression. Furthermore, given the prevalence of chronic health conditions among the old, it has been suggested that late-life interventions that promote the feeling of being valued have greater potential than changes in health status for preventing or treating depressive symptoms (Chippendale, Citation2013).
Our results further indicate that being non-depressed is related to better health because such people are more likely to be engaged in meaningful leisure activities. Being able to engage in meaningful leisure activities can be regarded as an expression of independence in activities of daily living, and mobility limitations have been associated with depression (Djernes, Citation2006; Lee et al., Citation2012). Furthermore, women with depression took a higher number of different kinds of drugs than the non-depressed, and this could be interpreted that depressed women also have poorer health, which is a well-known contributor to depression (Djernes, Citation2006; Skoog, Citation2011).
When reporting diseases, only myocardial infarction and diabetes showed significant correlations in the univariate analysis, but neither of these were significant in the final model. Stroke, which is a known predictor of depression (Djernes, Citation2006; Petersson et al., Citation2014; Skoog, Citation2011), showed no significance at any level in our study. This might be explained by the low incidence rate in our study population, which in turn might be related to difficulties in participating in this kind of study due to post-stroke complications. Another notable result in our study was that age did not independently explain variation in depression in the final regression model even though old age has also been reported to be a predictor of depression (Djernes, Citation2006; Skoog, Citation2011; von Heideken Wågert et al., Citation2005). Our seemingly contradictory results might be explained by the fact that our population mainly represented the third age, and depression becomes more frequent when reaching the oldest ages (von Heideken Wågert et al., Citation2005).
Finally, we found that women rating their inner strength higher were also more likely to be non-depressed. The theoretical model of inner strength (Lundman, Aléx, et al., Citation2010) has its origin in the five salutogenic concepts of sense of coherence, purpose in life, self-transcendence, resilience, and hardiness. These have been studied in relation to depression in prior studies and have been interpreted to be resources that are related to fewer depressive symptoms (Cataldo, Citation1994; Dezutter, Weismann, Apers, & Luyckx, Citation2013; Hardy, Concato, & Gill, Citation2004; Hedberg, Gustafson, Aléx, & Brulin, Citation2010; Lundman, Forsberg, et al., Citation2010; Solhaug, Romuld, Romild, & Stordal, Citation2012; Stinson & Kirk, Citation2006). It is notable that Hedberg et al. (Citation2010) found that although purpose in life and depression showed a significant inverse relationship in a cross-sectional study, sensing purpose in life did not seem to protect against development of depression over time.
Strengths and limitations
One of the strengths of this study is that the prevalence rates of depression are in line with previous studies (Forsman, Nyqvist, Schierenbeck, Gustafson, & Wahlbeck, Citation2012; Papadopoulos et al., Citation2005; Wild et al., Citation2012) indicating that the results appear reliable. Also, the GDS-15 has been shown to be sensitive for major depression, and a cut-off point of 4 or 5 has been shown to produce robust results in previous studies (Almeida & Almeida, Citation1999; Bijl, van Marwijk, Hermanz, Beekman, & de Haan, Citation2006; Nyunt et al., Citation2009), even though it has been suggested that higher cut-off points might be more accurate for the diagnosis of depressive episodes (Almeida & Almeida, Citation1999). Since GDS is sensitive for major depression, our measurement excludes persons with other kinds of depressive states and this could be considered a weakness in this study. Also, inner strength in some ways is an abstract construct and can be difficult to measure, but still the ISS has shown acceptable psychometric properties (cf. Lundman et al., Citation2011) and the construct is built on a thoroughly performed and presented meta-analysis (Lundman, Aléx et al., Citation2010). Furthermore, our results might have been affected by the low response rate from the oldest old, persons living alone, and those with more diseases, i.e. the frailest old. The relatively high numbers of dropouts in this specific group might negatively affect our ability to transfer our results to older women in general, though they are presumably generalizable to women in the third age. There is also a possibility that respondents may have had help filling in the questionnaire and the answer might have been affected by the presence of the other person (social desirability response bias) (cf. Polit & Beck, Citation2004). Another weakness is the cross-sectional design, which prevents us of from making causal inferences. Thus, there is a need for longitudinal studies exploring the relationship between inner strength and depression.
Conclusions
Our results showed an association between strong inner strength and being non-depressed, and that inner strength independently has an effect on depression. This goes in line with findings that inner strength is associated with mental health (Nygren et al., Citation2005) and is a mediator of the relationship between diseases (among them depression) and self-rated health (Viglund et al., Citation2014). The findings from the present study can be interpreted as inner strength might have a protective effect on depression. These findings are interesting from a health-promotion perspective, but further studies are needed to verify that high inner strength can reduce the incidence of depression.
Acknowledgements
We thank Edvard Johansson for statistical consultations.
Additional information
Funding
References
- Adams, K.B., Roberts, A.R., & Cole, M.B. (2011). Changes in activity and interest in the third and fourth age: Associations with health, functioning and depressive symptoms. Occupational Therapy International, 18(1), 4–17.
- Aging Clinical Research Center (ACRC). Geriatric Depression Scale. Retrieved from http://www.stanford.edu/~yesavage/GDS.html
- Alexopoulos, G. (2005). Depression in the elderly. Lancet, 365, 1961–1970.
- Almeida, O.P., & Almeida, S.A. (1999). Short versions of the geriatric depression scale: A study of their validity for the diagnosis of a major depressive episode according to ICD-10 and DSM-IV. International Journal of Geriatric Psychiatry, 14, 858–865.
- Bergendahl, E., Allard, P., Aléx, L., Lundman, B., & Gustafson Y. (2007). Gender differences in depression among the very old. International Psychogeriatriatrics, 19(6), 1125–1140.
- Bijl, D., van Marwijk, H., Hermanz, J.A., Beekman, A., & de Haan, M. (2006). Test-characteristics of the DGS-15 in screening for major depression in elderly patients in general practice. Clinical Gerontologist, 29(1), 1–9.
- Cacioppo, J.T., Huges, M.E., Waite, L.J., Hawkley, L.C., & Thisted, R.A. (2006). Loneliness as a specific risk factor for depressive symptoms: Cross-sectional and longitudinal analyses. Psychology and Aging, 21(1), 140–151.
- Cataldo, J.K. (1994). Hardiness and death attitudes: Predictors of depression in the institutionalized elderly. Archives of Psychiatric Nursing, 8(5), 326–332.
- Chippendale, T. (2013). Factors associated with depressive symptoms among elders in senior residences: The importance of feeling valued by others. Clinical Gerontology, 36, 162–169.
- Conradsson, M., Rosendahl, E., Littbrand, H., Gustafson, Y., Olofsson, B., & Lövheim, H. (2013). Usefulness of Geriatric Depression Scale 15-item version among very old people with and without cognitive impairment. Aging & Mental Health, 17(5), 638--645.
- Dezutter, J., Weismann, U., Apers, S., & Luyckx, K. (2013). Sense of coherence, depressive feelings and life satisfaction in older persons: A closer look at the role of integrity and despair. Aging & Mental Health, 17(7), 839--843.
- Dingley, C., & Roux, G. (2014). The role of inner strength in quality of life and self-management in women survivors of cancer. Research in Nursing & Health 37, 32–41.
- Djernes, J. (2006). Precalence and predictors of depression in populations of elderly: A review. Acta Psychiatrica Scandinavia, 113, 372–387
- Forsman, A.K., Nyqvist, F., Schierenbeck, I., Gustafson, Y., & Wahlbeck, K. (2012). Structural and cognitive social capital and depression among older adults in two Nordic regions. Aging & Mental Health, 16(6), 771--779.
- Hardy, S., Concato, J., & Gill, T.M. (2004). Resilience of community-dwelling order persons. Journal of American Geriatrics Society, 52, 257–262.
- Hawley, L.C., & Cacioppo, J.T. (2010). Loneliness matter: A theoretical and empirical review of consequences and mechanisms. Annals of Behavioral Medicine, 40, 218–227.
- Hedberg, P., Gustafson, Y., Aléx, L., & Brulin, C. (2010). Depression in relation to purpose in life among very old population: A five-year follow-up study. Aging & Mental Health, 14(6), 757–763.
- Lee, C., Yeh, C., Lee, M., Lin, H., Chen, V., & Lai, T. (2012). Leisure activity, mobility limitation and stress as modifiable risk factors for depressive symptoms in the elderly: Results of a national longitudinal study. Archives of Gerontology and Geriatrics, 54(2), e221–e229.
- Lewis, K.L., & Roux, G. (2011). Psychometric testing of the Inner Strength Questionnaire: Women living with chronic health conditions. Applied Nursing Research, 24, 153–160.
- Lundman, B., Aléx, L., Jonsén, E., Norberg, A., Nygren, B., Santamäki-Fischer, R., & Strandberg, G. (2010). Inner strength – a theoretical analysis of salutogenic concepts. International Journal of Nursing Studies, 47(2), 251–260.
- Lundman, B., Forsberg, K.A., Jonsén, E., Gustafson, Y., Olofsson, K., Strandberg G, & Lövheim, H. (2010). Sense of coherence (SOC) related to health and mortality among the very old: The Umeå 85+ study. Archives of Gerontology and Geriatrics, 51(3), 329–332.
- Lundman, B., Viglund, K., Aléx, L., Jonsén, E., Norberg, A., Santamäki-Fischer, R., … Nygren, B. (2011). Development and psychometric properties of the Inner Strength Scale. International Journal of Nursing Studies, 48(10), 1266–1274.
- Lundman, B., Aléx, L., Jonsén, E., Lövheim, H., Nygren, B., Santamäki Fischer, R., … Norberg, A. (2012). Inner strength in relation to functional status, disease, living arrangements, and social relationships among people aged 85 years and older. Geriatric Nursing, 33(3), 167–176.
- Nygren, B., Aléx, L., Jonsén, E., Gustafson, Y., Norberg, A., & Lundman, B. (2005). Resilience, sense of coherence, purpose in life and self-transcendence in relation to perceived physical and mental health among the oldest old. Aging & Mental Health, 9(4), 354–362.
- Nyunt, M.S., Fones, C., Niti, M., & Ng, T-P. (2009). Criterion-based validity and reliability of the geriatric depression screening scale (GDS-15) in a large validation sample of community-living Asian older adults. Aging & Mental Health, 13(3), 376–382.
- Papadopoulos, F.C., Petridou, E., Argyropoulou, S., Kantaxakis, V., Dessypris, N., Anastasiou, A., … Lyketsos, C. (2005). Prevalence and correlates of depression in late life: A population based study from a rural Greek town. International Journal of Geriatric Psychiatry, 20, 350–357.
- Petersson, S., Mathillas, J., Wallin, K., Olofsson, B., Allard, P., & Gustafson, Y. (2014). Risk factors for depressive disorders in very old age: A population-based cohort study with a 5-year follow-up. Social Psychiatry and Psychiatric Epidemiology, 49(5), 831–839.
- Polit, D.F., & Beck, C.T. (2004). Principles and methods (7th ed.). Philadelphia, PA: Lippincott Williams & Wilkins.
- Sheikh, J.I., & Yesavage, J.A. (1986). Geriatric Depression Scale (GDS): Recent evidence and development of a shorter version. Clinical Gerontologist, 5(1), 165–173.
- Skoog, I. (2011). Psychiatric disorders in the elderly. Canadian Journal of Psychiatry, 56(7), 387–397.
- Smith, T.B., McCullough, M.E., & Poll, J. (2003). Religiousness and depression: Evidence for a mail effect and the moderating influence of stressful life events. Psychological Bulletin, 129, 614–636.
- Solhaug, H.I., Romuld, E.B., Romild, U., & Stordal, E. (2012). Increased prevalence of depression in cohorts of elderly: An 11-year follow-up in the general population – the HUNT study. International Psychogeriatrics, 24(1), 151–158.
- Stinson, C.K., & Kirk, E. (2006). Structured reminiscence: An intervention to decrease depression and increase self-transcendence in older women. Journal of Clinical Nursing, 15, 208–218.
- Viglund, K., Jonsén, E., Lundman, B., Strandberg, G., & Nygren, B. (2013). Inner strength in relation to age, gender and culture among old people – a cross-sectional population study in two Nordic countries. Aging & Mental Health, 17(8), 1016–1022.
- Viglund, K., Jonsen, E., Strandberg, G., Lundman, B., & Nygren, B. (2014). Inner strength as a mediator of the relationship between disease and self-rated health among old people. Journal of Advanced Nursing, 70(1), 144–152.
- von Heideken Wågert, P., Rönnmark, B., Rosendahl, E., Lundin-Olsson, L., Gustavsson, J.M., Nygren, B., … Gustafson, Y. (2005). Morale in the oldest old: The Umeå 85+ study. Age and Ageing, 34, 249–255.
- Wild, B., Herzog, W., Schellberg, D., Lechner, S., Niehoff, D., Brenner, H., … Raum, E. (2012). Association between prevalence of depression and age in large representative German sample of population aged 53 to 80 years. International Journal of Geriatric Psychiatry, 27, 375–381.
- World Health Organization. (2012). Depression. Retrieved from http://www.who.int/mediacentre/factsheets/fs369/en/
- Yesavage, J.A., Brink, T.L., Rose, T.L., Lum, O., Huang, V., Adey, M., & Leirer, V.O. (1983). Development and validation of a geriatric depression screening scale: A preliminary report. Journal of Psychiatric Research, 17(1), 37–49.