
Abstract
Perceived loneliness has implications in both cognitive and affective domains. High loneliness is considered to be a major risk factor for major depressive disorder. Loneliness is also associated with impaired executive control functioning (ECF) including multiple cognitive subdomains, such as working memory, planning, response inhibition, and attention control. However, little knowledge exists as to whether perceived loneliness is associated with impaired functioning of specific ECF components. The relationship between perceived loneliness and the latent dimensions capturing multiple measures across different ECF paradigms has not been established. In this study, we first investigated the latent dimensions of ECF processes across a comprehensive range of paradigms using exploratory factor analysis. We then examined the association of perceived loneliness and the resulted ECF components in older adults while simultaneously controlling for other demographic and affective measures. Four components emerged from the factor analysis: social cognition and processing speed, planning and working memory, selective, divided attention and inhibition control, and sustained attention and motor inhibition. We observed that the second ECF component, planning and working memory, was a significant predictor of perceived loneliness even after controlling for depressive characteristics measured by the Geriatric Depression Scale. Our findings have potential clinical significance in the older population, by showing that planning and working memory functions may predict perceived loneliness, which is also associated with higher risk for major depression. Thus, older individuals who have lower planning and working memory functions may be specifically targeted for possible early prevention of chronic loneliness and depression.
Perceived loneliness refers to the perception of being socially isolated resulting from a discrepancy between one’s social needs or expectation and real-life social relationships (Cacioppo, Norris, Decety, Monteleone, & Nusbaum, Citation2009). Perceived loneliness has both affective and cognitive implications. On the affective side, perceived loneliness is a major risk factor for depression, especially in older adults (Cacioppo & Hawkley, Citation2009), and is generally associated with higher levels of negative mood, anxiety, anger, and depressive symptomatology (Santini et al., Citation2020). On the cognitive side, perceived loneliness has been associated with greater risk for developing Alzheimer’s disease and potential impairment in various cognitive domains, such as working memory and processing speed (Boss, Kang, & Branson, Citation2015). Cacioppo and Patrick (Citation2008) suggested that lonely individuals typically display negative affective bias that affects their emotions, thoughts, and behaviors. Specifically, perceived loneliness activates implicit hypervigilance for social threat in one’s environment; in chronic form, this could exhaust the cognitive resources for executive control of the affective system (Cacioppo & Hawkley, Citation2009). Reduction in cognitive and affective control could lead to further enhanced negative bias constituting a growing cycle (Gotlib & Joorman, Citation2010). Precise characterization of the cognitive control function of lonely older adults is key to understanding the mechanisms through which perceived loneliness affects emotional and cognitive health.
Critical in the context of emotional and cognitive control, ECF consists of several cognitive subdomains such as response inhibition, planning, problem-solving, attention, working memory, set shifting (mental flexibility), abstract thinking, and judgement (Zheng et al., Citation2012). In a daily context, these executive processes are routinely employed in a goal-directed manner aimed at maintaining adequate top-down control of lower level affective processes and are essential for self-regulation (Lewis & Miller, Citation2007). Poor self-regulation is a strong risk factor for mental health issues such as major depressive disorder and addiction (Nigg, Citation2017), especially among older adults. Considering the high prevalence of late-life depression (Blazer, Citation2003), efficient self-regulation could be an important protective factor in preventing older adults from developing depression. An array of neuropsychological and laboratory tasks (Lewis & Miller, Citation2007) exist that assess different ECF processes. For example, The Tower of London Task (ToL), Stroop Colour Word Task (Colour-Stroop), Colour Trails Test (CTT), and Continuous Performance Test (CPT) are widely used cognitive tasks that measure planning and working memory, as well as inhibition and attention control functions, respectively (Burton et al., Citation2010; Epp, Dobson, Dozois, & Frewen, Citation2012; Köstering et al., Citation2015; Lee, Yuen, & Chan, Citation2002). These ECF processes, along with social cognitive processes such as theory of mind (ToM), empathy, and perspective taking, might determine the lonely individual’s emotional and cognitive health (Cacioppo et al., Citation2009).
Existing evidence indicates an association between perceived loneliness and ECF. Among the older adult population, perceived loneliness was negatively correlated with cognitive processes such as processing speed and verbal fluency at baseline and was a predictor of subsequent cognitive impairments (Boss et al., Citation2015; Cacioppo & Hawkley, Citation2009; Donovan et al., Citation2017). Lonely people were found to have difficulty inhibiting the prepotent response (Cacioppo & Hawkley, Citation2009) and performed worse than non-lonely individuals on a battery of cognitive measures including memory tests, attention tasks, and processing speed (Wilson et al., Citation2007). However, some evidence suggested that the association between loneliness and ECF disappeared after controlling for demographic or psychosocial factors but not after controlling for depressive symptoms (Boss et al., Citation2015; Wilson et al., Citation2007).
As described above, different cognitive paradigms have been developed to measure different ECF domains. However, most of the existing paradigms are not a pure measure of a single ECF process. For example, ToL can measure planning, inhibitory control, and working memory capacities (Luciana et al., Citation2009), and the Colour-Stroop task can measure both inhibition and attention control, as was previously found in the Chinese population (Lee et al., Citation2002). As such, it is difficult to interpret any observed association between loneliness and cognitive task performance in terms of the precise cognitive processes implicated. Moreover, different measures from the same task might reflect partially non-overlapping executive functions. For example, one study examining genetic contribution to ToL performance suggested that the speed for completing the task, as reflected by the time spent in problem-solving, represented a separate, albeit correlated, factor from the efficiency of task performance as reflected by the number of moves (Kremen et al., Citation2009). Another study showed that while both ToL time and number of move indices correlated with backward digit span, suggesting a potential working memory determinant, only the number of moves correlated with target detection performance, indicating a potential, sustained attention determinant (Luciana et al., 2009). Therefore, it might be more useful to consider cognitive “components” rather than individual cognitive processes or task measures with one component possibly reflecting shared processes of multiple tasks and measures. In other words, the cognitive components are latent constructs that can capture the overlap across different paradigms and indices. Existing studies on cognitive components have been limited and inconsistent. Lewis and Miller (Citation2007) suggested there are four important components that underlie ECF, including working memory, planning, cognitive fluency, and cognitive flexibility. Another study suggested that only three cognitive components underlie the ECF, including inhibition of prepotent response (response inhibition), updating and monitoring of working memory representations (working memory), and shifting between tasks and mental sets (task switching) (Miyake et al., Citation2000).
As outlined above, there is currently a gap in knowledge on the association of perceived loneliness and ECF components after accounting for various demographic, psychometric, and psychosocial factors. In particular, loneliness is closely associated with elevated depressive symptoms (Cacioppo et al., Citation2015) that could impact ECF (e.g. Chantiluke et al., Citation2012). It is important to control for objective social isolation when investigating the effect of perceived loneliness or subjective social isolation (Layden et al., Citation2017). In the current study, we used exploratory factor analysis to capture the latent dimensions of executive control processes across ECF tasks and measures and examined the association of loneliness and those ECF components in older adults. Based on the limited existing research, we hypothesized that perceived loneliness would be predicted by altered functions of one or several ECF components encompassing the various processes such as attention, working memory, planning and processing speed, even after controlling for key demographic, psychometric, and psychosocial variables.
Methods
Participants and data collection
The Institutional Review Board in the University of Hong Kong approved this study. The study was carried out in The Institute of Clinical Neuropsychology of The University of Hong Kong. The participants were residents throughout the 18 city districts of Hong Kong. They were recruited from the community via words of mouth and with the help of various nongovernmental organizations. Demographic information including age, sex, education years, marital status, housing ownership, housing type and social participation was collected by self-reporting. Age and sex were additionally verified by the participant’s Hong Kong identity card. Participants were included only if they did not have any histories of major psychiatric or physical illness. Those with a score of < 22 on the Montreal Cognitive Assessment (MoCA), score of > 7 on the Geriatric Depression Scale (GDS), or a history of neurological diseases were excluded to ensure no confounding effect of cognitive impairment or neurological changes.
Participants signed the fully informed written consent form after they were briefed of the study objectives and procedures. Participants did not receive any financial incentive, but they received a neuropsychological consultation by our in-house clinical psychologists. The whole data collection process was carried out by various fully-trained research personnel, including research assistants and postgraduate students.
Psychological measures
Executive control functioning tests
Tower of London task (ToL)
ToL was developed to measure the planning ability and working memory of an individual (Rainville, Lepage, Gauthier, Kergoat, & Belleville, Citation2012). The ToL apparatus consists of two kits, each with a wooden base. On the base, three wooden pegs with different lengths are mounted. In each kit, there is a green, blue, and red ball, each with a hollow core that can be moved easily from one peg to another. One of the kits serves to display the goal arrangement. This is the examiner’s kit. The other is for participants to reproduce the arrangement. This is the participant’s kit. There are 10 problems in total. The total number of moves, the total number of correct answers, and the total time of completion are recorded.
Stroop color word task (stroop)
The Stroop was developed to measure cognitive inhibitory and attention control (Lee et al., Citation2002). The Dot subtask displays items consisting of colored dots, the Word subtask displays items consisting of common words unrelated to color, and the Color-Word subtask displays items consisted of words that are color names. Each subtask is made up of six rows of four items. The four color names used are blue, green, red, and yellow. Participants are required to name the colors in which the items are printed while disregarding their verbal content. The test–retest reliability of the Chinese version of the Dot, Word, and Color-Word subtasks was 0.89, 0.91 and 0.90, respectively (Lee et al., Citation2002). Interference scores for both accuracy and reaction time were generated by subtracting the performance on the Color-Word subtask from that of the Dot subtask.
Colour trails test (CTT)
The CTT was used to measure the divided attention of an individual (Lee et al., Citation2002). The test contains two parts: part A and part B. In part A, participants are required to connect 25 circled numbers randomly arranged on the test sheet in ascending numerical order. In part B, participants connect the 25 circled numbers sequentially, this time alternating between pink and yellow numbers. The time required to complete each part of the task is recorded. The interference index was calculated using the formula [Time (B) – Time (A)]/Time (A).
Continuous performance test (CPT)
The CPT was used to measure the sustained attention and motor inhibition of an individual (Egeland & Kovalik-Gran, Citation2010; Wright, Lipszyc, Dupuis, Thayapararajah, & Schachar, Citation2014). It is a computer-administered task that requires the participants to press the space bar when any letter other than X is flashed on the screen. The participants have to inhibit responses when the stimulus is not the target and maintain attention or vigilance continuously. The commission errors and omission errors made by the participants are recorded.
Halstead category test (HCT)
The Halstead Category Test (HCT) was designed to measure the mental flexibility of an individual (Nici & Hom, Citation2013). In the test, participants are shown a series of shape designs. For each series of designs, there is a single hidden rule that the participants must discern through hypothesis testing and trial-and-error learning. For each design, participants press a key on an answer panel to indicate their response. Immediate feedback is given in the form of a bell ring for a correct answer or a buzzer sound for an incorrect answer. There are seven subtests in total. The total number of errors made is recorded.
Symbols digit modality test (SDMT)
The Symbols Digit Modality Test (SDMT) is used for assessing the processing speed of an individual (Bird, Papadopoulou, Ricciardelli, Rossor, & Cipolotti, Citation2004). In this test, participants need to complete 50 blank squares, each indexed with an abstract symbol. Each symbol is paired with a single digit number (1–9), as indicated by a row of keys displayed in the upper section of the worksheet. During the test, participants need to fill in the squares with the digits that are correctly linked with the symbols as quickly as possible. The total number of correct answer is recorded.
Social cognitive tests
Frith-Happe animations (FHA)
The Frith-Happe Animations (FHA) is a test used for assessing social cognition, especially the ToM (Ladegaard, Larsen, Videbech, & Lysaker, Citation2014). This test consists of short video sequences of animated shapes, specifically a red and a blue triangle in a contained space. Half of the clips, each of which is associated with a unique story (e.g.the small triangle is told off as it tries to mimic the big triangle), can deploy their kinetic properties or ToM animations to elicit a mental state attribution. The other half of the clips consists of random motions with no storyline. After viewing each clip, participants answer twelve categorization questions and eight emotion-related questions. A high number of questions answered correctly reflect greater ToM ability.
Reading the mind in the eyes test (eye test)
The eye test was designed to measure the ability of an individual to perceive the mental states of others through eye gaze (Olderbak et al., Citation2015). The test includes 36 items. For each item, participants view the eyes, but not other parts of the face, of a person and select among four mental state terms to describe the state of the person. The number of correct answers is recorded.
Questionnaires
UCLA loneliness scale (LS)
The UCLA Loneliness Scale (LS) measures participants’ perceived loneliness level (Russell, Citation1996). It has proven sensitivity to perceived loneliness with high internal consistency (coefficient alpha ranging from 0.89 to 0.94), test–retest reliability (r = 0.73), suitability for use in older adults (Cacioppo, Hawkley, & Thisted, Citation2010; Hawkley, Thisted, & Cacioppo, Citation2009). The Chinese version of the LS has good internal consistency with an alpha coefficient of 0.88 (Wu et al., Citation2010). The test–retest reliability over 2 weeks is 0.85 for the Chinese version (Chen & Chung, Citation2007).
Geriatric depression scale (GDS)
The Chinese version of the GDS is used to measure the severity of participants’ depression. The GDS consists of fifteen items and is a widely used scale for assessing the severity of depressive symptoms in older adults (Kurlowicz & Greenberg, Citation2007). It has good internal consistency (Cronbach alpha = 0.89) (Chan, Citation1996). The score ranges from 0–15, with a higher score indicating more severe depressive symptoms.
Participants were asked how frequently they engaged in social activities. The tool that we used to measure social engagement was referred to and adapted from previous studies on older adults (Glass, de Leon, Marottoli, & Berkman, Citation1999; Gonzales, Matz-Costa, & Morrow-Howell, Citation2015), which found that higher social engagement was associated with lower mortality rate and better life quality. Three sets of questions were asked which assess both job- and leisure-related social activities (please refer to supplementary Table S1 for more details). The employment status question asked whether the participant was employed or unemployed. For the second and third parts, the scales ranged from 0 to 4, with 0 representing no participation at all and 4 representing the highest level of participation. The total mark ranged from 0–68, with higher scores indicating greater social participation levels.
Statistical analysis
Factor analysis
Exploratory factor analysis with varimax rotation was performed on the outcome measures of the eight cognitive tests, which assess cognitive functions in various domains including social cognition, processing speed, planning, working memory, selective attention, divided attention, inhibition control, sustained attention and motor inhibition, in order to detect the underlying common cognitive constructs being captured by those measures. All the outcome measures were converted into z scores before the factor analysis.
Linear regression
Linear regression was performed with the LS scores as the dependent variable. We included the components that were yielded from the factor analysis, along with age, marital status, years of education, sex, GDS scores, and social participation scores, as the predictors. For each component, the z scores of all the individual measures were summed to compute the composite score for the component. The measures were inverse-scored where appropriate such that higher scores always reflected greater performance. All other continuous variables were also converted into z scores. When constructing the model, we entered the predictors in a stepwise fashion where the demographic variables and the GDS scores were entered first, followed by the component variables.
Some previous literature suggests that ‘older adults’ may be divided into heterogeneous age-defined subgroups, including young old (60–69 years), middle old (70–79 years), and old old (≥ 80 years). Existing evidence suggests that loneliness levels may be higher in the combined group of middle old and old old groups (i.e.age ≥ 70 years) compared to the young old group (Andersson, Citation1998; Luanaigh & Lawlor, Citation2008; Luhmann & Hawkley, Citation2016). Unfortunately, our participants all fell in the young old and middle old age groups. Thus, it was not possible for us to assess the loneliness level in the old old age group. In a supplementary analysis, we added an age group variable (young old vs. middle old) into our existing regression model to assess whether loneliness levels may be different between the young old and middle old participants.
Results
Two hundred and twenty-five older participants aged more than 60 years (53 males and 172 females, age 65.29 ± 10.93 years) were recruited from the community and participated in the study. Demographical and psychometric scores of the participants are presented in .
Table 1. Demographics of the participants.
Among the participants, around two thirds were married, while the rest reported to be single, divorced, separated or widow. We may assume those who were not married were living alone. Regarding the housing situation, we asked participants about their housing ownership, including the options of self-owned or rental, and housing type, which assessed whether the participant was living in public housing, home ownership scheme flat, quarter, private housing, temporary housing or others. The question did not specifically include the option of senior living community, which was generically covered in the ‘others’ option. Around three fourths of the participants owned their flat while the remaining rented it. For the housing type, the majority of the participants (around 65%) lived in private housing, while similar proportions stayed in either public housing or home ownership scheme flat (13% and 16% respectively). The rest were in quarter (1 participant) or under the option ‘others’.
Factor analysis
Exploratory factor analysis generated four factors among the thirteen outcome measures from the eight cognitive tests (). The model accounted for 56% of the total variance of the cognitive measures. This four-factor model generated relatively distinct factors, each composed of 2–5 items, with the items loading relatively heavily on one factor (≥0.6) but minimally on the other factors.
Table 2. The exploratory factor analysis results of the cognitive measures.
The first factor, composed of five outcome measures, appeared to reflect social cognition, processing speed, and mental flexibility. The second factor appeared to reflect the planning and working memory abilities as indexed by the three outcome measures of the ToL task. The third factor appeared to reflect the divided and selective attention and cognitive inhibitory control abilities. It consisted of the three outcome measures of the CTT and Colour-Word Stroop task. The last factor comprised of two outcome measures from the CPT. It appeared to reflect the sustained attention and motor inhibition functions.
Linear regression
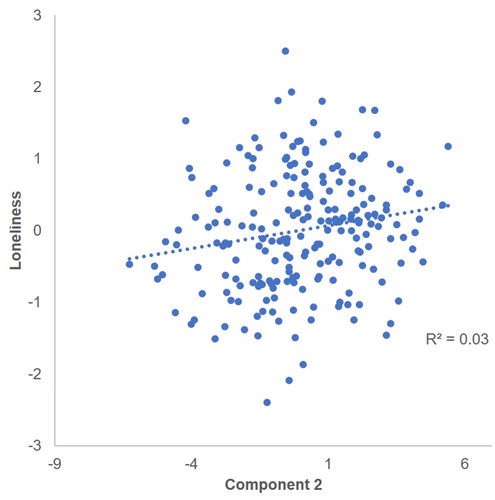
In the linear regression analysis, we only included the demographic information including age, sex, education years, marital status and social participation into the model. We did not include the housing ownership and housing type in our model as we found that the two housing variables were not related to loneliness score (Supplementary Table S2). Our result showed that the GDS score (beta = 0.573, t = 9.434, p < 0.01) was the best predictor of LS score in older adults (). Among the cognitive components, only component 2, ToL Planning and Working Memory, showed additional significant association with the LS scores (beta = 0.146, t = 2.361, p = 0.019) (). The r2 value demonstrated a reasonably good accuracy of the prediction (r2= 0.336) (see Supplementary Table S3 for the full regression analysis results). Finally, we found that the age group variable (young old vs. middle old) had no significant effect on loneliness level (beta = 0.019; t = 0.285, p = 0.776).
Figure 1. The partial correlation between perceived loneliness and GDS score. Both x and y axis display variables that are residuals, i.e.after regressing out the covariance with other predictors for the GDS score, and after regressing out the effects of other predictors for the loneliness score.
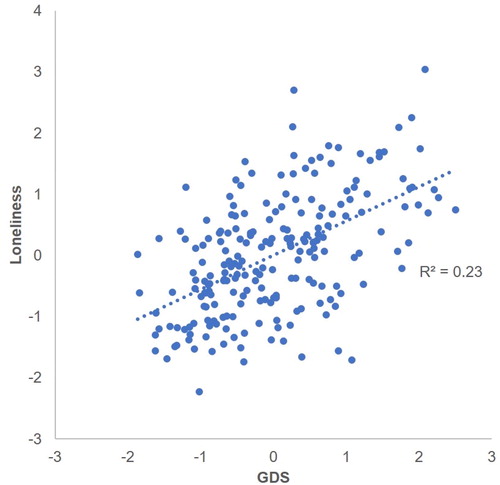
Figure 2. The partial correlation between perceived loneliness and component 2. Both x and y axis display variables that are residuals, i.e.after regressing out the covariance with other predictors for the component 2 value, and after regressing out the effects of other predictors for loneliness score.
Discussion
Our study showed that executive control processes may be classified into four components: social cognition and processing speed, planning and working memory, selective, divided attention and inhibition control, and sustained attention and motor inhibition. Most importantly, we showed that the GDS score and ECF component 2 were significant predictors for perceived loneliness in the older population. While the GDS was the strongest predictor quantitatively, the predictive strength of the ECF component 2 was significant even after controlling for the GDS score and other demographic, psychometric, and cognitive measures.
Our factor analysis results were consistent with those of previous studies. The first component consisted of the outcome measures of tasks that assessed social cognition and processing speed. Previous studies suggested that processing speed would reduce with age, and that this change would affect the speed of older adults’ reactions across different situations (Kerchner et al., Citation2012). Social environment is highly complex with many embedding cues. Thus, an individual needs to perceive and process those cues quickly and accurately in order to give a suitable response or to understand the implication of those social behaviors. Older adults with lower processing speed may show impaired ability to process social cues, due to reduced cognitive reserve and capacity. (Kerchner et al., Citation2012). This may explain the relatively high correlations between social cognition and processing speed measures. Component 2 contains solely the outcome measures of ToL to form the factor that represents planning and working memory. Previous evidence suggests that different ToL measures might be more or less reflective of different ECF processes. For example, the time of task completion might reflect working memory, whereas the number of moves might reflect both working memory and sustained attention (Luciana et al., 2009). However, evidence also indicates that the different ToL measures are highly correlated (Kreman et al., 2009), and this is consistent with our current findings.
Components 3 and 4 represented attention and cognitive inhibition, as well as attention and motor inhibition, respectively. The two components captured different types of attention, with selective/divided attention in component 3 and sustained attention in component 4. Previous studies showed that inhibition declined with age, which would reduce the functional capacity of working memory and result in poorer encoding, retrieval, and comprehension in older adults (McDowd, Citation1997). With less efficient inhibition function, the individual would have difficulty in preventing irrelevant information from entering their attention span. Attention also plays an essential role at the stimulus-encoding phase. Effective selective attention is the fundamental ECF basis for goal-directed volitional actions. It is of no surprise that the measures of selective attention and inhibitory control are highly correlated. However, the measures of sustained attention tended to correlate with component 4, motor inhibition, rather than component 3, selective attention and inhibitory control. We speculate that cognitive inhibition demands more selective attentional control compared to motor inhibition, as measured by the CPT, which may depend more on the ability to maintain attention and vigilance throughout the task. The association between sustained attention and motor inhibition during CPT performance was also previously noted (Burton et al., Citation2010).
Our results aligned with those of previous studies suggesting that the GDS score is a predictor for perceived loneliness. A wide range of studies have shown that there is a strong correlation between depression and perceived loneliness, especially in older populations (Aziz & Steffens, Citation2013; Djukanović, Sorjonen, & Peterson, Citation2015; Singh & Misra, Citation2009). Depressed individuals typically exhibit negative perceptual and cognitive biases (Beck, Citation2008; Disner, Beevers, Haigh, & Beck, Citation2011). Similarly, lonely individuals are postulated to be hypervigilant to negative social stimuli and to show negative bias in social interactions (Cacioppo & Hawkley, Citation2009). There is a known association between aging and a high rate of developing major depression (Aziz & Steffens, Citation2013; Beekman et al., Citation1995; Blazer, Citation2003), and this would likely impede the development and maintenance of social connections, resulting in a higher incidence of loneliness (Singh & Misra, Citation2009). Moreover, avolition, or a severe lack of initiative to accomplish purposeful tasks, is a core characteristic of depressed people (Singh & Misra, Citation2009). This would hinder them from engaging in social activities, with the consequence of gradually reduced social support and social connectedness resulting in the perception of loneliness (Cornwell & Waite, Citation2009). Our findings highlight the important association between loneliness and emotional health and the clinical implication of loneliness in the older population.
The second predictor found in our study was component 2, planning and working memory, which included the 3 outcome measures of ToL. ToL is commonly used to measure the planning function of an individual, but some studies suggest that ToL also measures other ECF processes such as working memory and inhibition. To successfully perform ToL, the individual needs to engage in a range of cognitive processes, including goal identification, by assessing the current situation based on comparing between the initial stage and the final stage, defining a series of subgoals, mental rehearsal of the sequence of moves in order to attain the sub goals, revising the sequence, and executing the sequence correctly (Phillips, Wynn, McPherson, & Gilhooly, Citation2001). Similarly, researchers suggested that planning was not to be a single process but should involve mental generation, evaluation, and selection of action sequences in relation to goal achievement (Gilhooly, Phillips, Wynn, Logie, & Sala, Citation1999), which overlap with the processes involved in ToL. Planning is an important survival skill for successful aging (Kremen et al., Citation2009), for several important reasons. First, it was found that at older age, there is a large reduction in the prefrontal region (Raz & Rodrigue, Citation2006), which is important for the planning skill. Thus, it is particularly important to preserve planning function as older individuals experience neural declines. Second, at older age, there are many changes to people’s lives such as loss of friends and retirement. These changes may create stress with negative health implications, while stress could be reduced with better planning functions especially in the older age (Williams, Suchy, & Rau, Citation2009). Third, it was also found that lower planning skills were associated with late life depression, as individuals with planning deficits may have difficulty anticipating and preparing for future changes (Alexopoulos, Citation2003).
Planning encompasses working memory and inhibition processes, both of which show a reduction in normal aging (Rainville et al., Citation2012). Existing evidence suggests that impairments in inhibition and working memory are in turn associated with failure in self-monitoring and self-control (Schmeichel, Volokhov, & Demaree, Citation2008). Self-monitoring is an important process linked with self-regulation of emotions, impulsivity control, and anticipation of behavioral consequences (Black, Semple, Pokhrel, & Grenard, Citation2011). Impairment in self-monitoring is a prominent characteristic of people suffering from major depression, who may also have difficulty in affect management, which reduces their coping efficacy and eventually contributes to the development of perceived loneliness (Cacioppo & Hawkley, Citation2009). It is interesting to note that social cognition was not found to be a predictor of perceived loneliness in our study, and this suggests that planning and working memory contributed more to the development of perceived loneliness through the self-monitoring mechanism as mentioned before (Schmeichel et al., Citation2008).
Our findings should be considered with awareness of a number of limitations to our study. First, the sex ratio of our sample was biased toward female participants, although it may reflect the actual gender distribution in people self-labeled as lonely (Borys & Perlman, Citation1985). Notwithstanding, our findings may not generalize to populations with equal sex distribution or a higher proportion of males. This needs to be validated in future research. Also, our study only included older adults aged between 60–79 years old, and thus no data from individuals in the old old age group (≥ 80 years) was available. Further study should include the full spectrum of older adults. The third limitation of our study was that we did not include tasks that specifically measure mnemonic functions other than working memory processes. In future studies, it may be worth expanding our research to other memory processes, such as long-term, short-term, and episodic memories, to obtain a more comprehensive picture of the relationship between memory and loneliness. Fourthly, future studies may wish to include participants with clinical depression to further investigate the cognitive profiles of perceived loneliness in healthy and depressed populations, respectively. Moreover, our study was cross-sectional, meaning the causal direction of any association between cognitive, affective measures, and loneliness could not be established. Future studies should employ the longitudinal approach to establish the temporal trajectory of the loneliness profiles. Although our participants were all free of major physical, neurological or psychological diseases, we could not completely rule out the potential impact of relatively minor medical comorbidities on social engagement, objective social isolation and/or perceived social isolation. Further studies should include more comprehensive assessments of participants’ medical conditions. Lastly, since we did not explicitly ask participants detailed information about their social status of living (e.g.by one’s own, cohabiting with 1 or 2 people, etc), we had to partly infer this information based on participants’ self-reported marital status. This inference could be inaccurate. Future studies should include more extensive measures in this aspect.
In summary, our study provided important evidence on the underlying cognitive component that may contribute to the development of perceived loneliness. We established that the latent cognitive component of planning and working memory, as reflected by scores on the ToL measures, predicted loneliness even after accounting for depressive characteristics and other demographic and cognitive variables. Thus, our findings contribute to our understanding of the cognitive–affective mechanism of loneliness and may inform clinical interventions targeted to reduce late-life loneliness and depression.
Supplemental Material
Download MS Word (17.8 KB)Disclosure statement
No potential conflict of interest was reported by the author(s).
Additional information
Funding
References
- Alexopoulos, G. S. (2003). Role of executive function in late-life depression. Journal of Clinical Psychiatry, 64 (Suppl 14), 18–23.
- Andersson, L. (1998). Loneliness research and interventions: A review of the literature. Journal Aging & Mental Health, 2(4), 264–274. doi:10.1080/13607869856506
- Aziz, R., & Steffens, D. C. (2013). What are the causes of late-life depression? Psychiatric Clinics of North America, 36(4), 497–516. doi:10.1016/j.psc.2013.08.001
- Beekman, A. T., Deeg, D. J., van Tilburg, T., Smit, J. H., Hooijer, C., & van Tilburg, W. (1995). Major and minor depression in later life: A study of prevalence and risk factors. Journal of Affective Disorders, 36(1–2), 65–75. doi:10.1016/0165-0327(95)00061-5
- Beck, A. T. (2008). The evolution of the cognitive model of depression and its neurobiological correlates. The American Journal of Psychiatry, 165(8), 969–977. doi:10.1176/appi.ajp.2008.08050721
- Bird, C. M., Papadopoulou, K., Ricciardelli, P., Rossor, M. N., & Cipolotti, L. (2004). Monitoring cognitive changes: Psychometric properties of six cognitive tests. The British Journal of Clinical Psychology, 43(Pt 2), 197–210. https://doi.org/https://doi.org/10.1348/014466504323088051 doi:10.1348/014466504323088051
- Black, D. S., Semple, R. J., Pokhrel, P., & Grenard, J. L. (2011). Component processes of executive function—mindfulness, self-control, and working memory—and their relationships with mental and behavioral health. Mindfulness, 2(3), 179–185. doi:10.1007/s12671-011-0057-2
- Blazer, D. G. (2003). Depression in late life: Review and commentary. The Journals of Gerontology: Series A, 58(3), M249–M265. doi:10.1093/gerona/58.3.M249
- Borys, S., & Perlman, D. (1985). Gender differences in loneliness. Personality and Social Psychology Bulletin, 11(1), 63–74. doi:10.1177/0146167285111006
- Boss, L., Kang, D.-H., & Branson, S. (2015). Loneliness and cognitive function in the older adult: A systematic review. International Psychogeriatrics, 27(4), 541–553. doi:10.1017/S1041610214002749
- Burton, L., Pfaff, D., Bolt, N., Hadjikyriacou, D., Silton, N., Kilgallen, C., … Allimant, J. (2010). Effects of gender and personality on the Conners Continuous Performance Test. Journal of Clinical and Experimental Neuropsychology, 32(1), 66–70. doi:10.1080/13803390902806568
- Cacioppo, S., Grippo, A. J., London, S., Goossens, L., & Cacioppo, J. T. (2015). Loneliness: Clinical import and interventions. Perspectives on Psychological Science: A Journal of the Association for Psychological Science, 10(2), 238–249. doi:10.1177/1745691615570616
- Cacioppo, J. T., & Hawkley, L. C. (2009). Perceived social isolation and cognition. Trends in Cognitive Sciences, 13(10), 447–454. doi:10.1016/j.tics.2009.06.005
- Cacioppo, J. T., Hawkley, L. C., & Thisted, R. A. (2010). Perceived social isolation makes me sad: 5-year cross-lagged analyses of loneliness and depressive symptomatology in the Chicago Health, Aging, and Social Relations Study. Psychology and Aging, 25(2), 453–463. doi:10.1037/a0017216
- Cacioppo, J. T., Norris, C. J., Decety, J., Monteleone, G., & Nusbaum, H. (2009). In the eye of the beholder: Individual differences in perceived social isolation predict regional brain activation to social stimuli. Journal of Cognitive Neuroscience, 21(1), 83–92. doi:10.1162/jocn.2009.21007
- Cacioppo, J. T., & Patrick, W. (2008). Loneliness: Human Nature and the Need for Social Connection. W. W. Norton & Company.
- Chan, A. C. (1996). Clinical validation of the Geriatric Depression Scale (GDS): Chinese version. Journal of Aging and Health, 8(2), 238–253. doi:10.1177/089826439600800205
- Chantiluke, K., Halari, R., Simic, M., Pariante, C. M., Papadopoulos, A., Giampietro, V., & Rubia, K. (2012). Fronto-striato-cerebellar dysregulation in adolescents with depression during motivated attention. Biological Psychiatry, 71(1), 59–67. doi:10.1016/j.biopsych.2011.09.005
- Chen, L.-J., & Chung, S.-K. (2007). Loneliness, social connectedness, and family income among undergraduate females and males in Taiwan. doi:10.2224/sbp.2007.35.10.1353
- Cornwell, E. Y., & Waite, L. J. (2009). Social disconnectedness, perceived isolation, and health among older adults. Journal of Health and Social Behavior, 50(1), 31–48. doi:10.1177/002214650905000103
- Disner, S. G., Beevers, C. G., Haigh, E. A. P., & Beck, A. T. (2011). Neural mechanisms of the cognitive model of depression. Nature Reviews. Neuroscience, 12(8), 467–477. doi:10.1038/nrn3027
- Djukanović, I., Sorjonen, K., & Peterson, U. (2015). Association between depressive symptoms and age, sex, loneliness and treatment among older people in Sweden. Aging & Mental Health, 19(6), 560–568. doi:10.1080/13607863.2014.962001
- Donovan, N. J., Wu, Q., Rentz, D. M., Sperling, R. A., Marshall, G. A., & Glymour, M. M. (2017). Loneliness, depression and cognitive function in older U.S. adults. International Journal of Geriatric Psychiatry, 32(5), 564–573. doi:10.1002/gps.4495
- Egeland, J., & Kovalik-Gran, I. (2010). Validity of the factor structure of Conners’ CPT. Journal of Attention Disorders, 13(4), 347–357. doi:10.1177/1087054709332477
- Epp, A. M., Dobson, K. S., Dozois, D. J. A., & Frewen, P. A. (2012). A systematic meta-analysis of the Stroop task in depression. Clinical Psychology Review, 32(4), 316–328. doi:10.1016/j.cpr.2012.02.005
- Glass, T. A., de Leon, C. M., Marottoli, R. A., & Berkman, L. F. (1999). Population based study of social and productive activities as predictors of survival among elderly Americans. BMJ, 319(7208), 478–483. doi:10.1136/bmj.319.7208.478
- Gilhooly, K. J., Phillips, L. H., Wynn, V., Logie, R. H., & Sala, S. D. (1999). Planning processes and age in the five-disc Tower of London task. Thinking & Reasoning, 5(4), 339–361. doi:10.1080/135467899393977
- Gonzales, E., Matz-Costa, C., & Morrow-Howell, N. (2015). Increasing opportunities for the productive engagement of older adults: A response to population aging. The Gerontologist, 55(2), 252–261. doi:10.1093/geront/gnu176
- Gotlib, I. H., & Joormann, J. (2010). Cognition and Depression: Current Status and Future Directions. Annual Review of Clinical Psychology, 6, 285–312. doi:10.1146/annurev.clinpsy.121208.131305
- Hawkley, L. C., Thisted, R. A., & Cacioppo, J. T. (2009). Loneliness predicts reduced physical activity: Cross-sectional & longitudinal analyses. Health Psychology, 28(3), 354–363. doi:10.1037/a0014400
- Kerchner, G. A., Racine, C. A., Hale, S., Wilheim, R., Laluz, V., Miller, B. L., & Kramer, J. H. (2012). Cognitive processing speed in older adults: Relationship with white matter integrity. PLOS One., 7(11), e50425. doi:10.1371/journal.pone.0050425
- Köstering, L., Schmidt, C. S. M., Egger, K., Amtage, F., Peter, J., Klöppel, S., … Kaller, C. P. (2015). Assessment of planning performance in clinical samples: Reliability and validity of the Tower of London task (TOL-F). Neuropsychologia, 75, 646–655. doi:10.1016/j.neuropsychologia.2015.07.017
- Kremen, W. S., Jacobson, K. C., Panizzon, M. S., Xian, H., Eaves, L. J., Eisen, S. A., … Lyons, M. J. (2009). Factor structure of planning and problem-solving: A behavioral genetic analysis of the Tower of London task in middle-aged twins. Behavior Genetics, 39(2), 133–144. doi:10.1007/s10519-008-9242-z
- Kurlowicz, L., & Greenberg, S. A. (2007). The Geriatric Depression Scale (GDS). AJN the American Journal of Nursing, 107(10), 67. 10.1097/01.NAJ.0000292207.37066.2f
- Lee, T., Yuen, K., & Chan, C. (2002). Normative data for neuropsychological measures of fluency, attention, and memory measures for Hong Kong Chinese. Journal of Clinical and Experimental Neuropsychology, 24(5), 615–632. doi:10.1076/jcen.24.5.615.1001
- Ladegaard, N., Larsen, E. R., Videbech, P., & Lysaker, P. H. (2014). Higher-order social cognition in first-episode major depression. Psychiatry Research, 216(1), 37–43. doi:10.1016/j.psychres.2013.12.010
- Layden, E. A., Cacioppo, J. T., Cacioppo, S., Cappa, S. F., Dodich, A., Falini, A., & Canessa, N. (2017). Perceived social isolation is associated with altered functional connectivity in neural networks associated with tonic alertness and executive control. NeuroImage, 145(Pt A), 58–73. doi:10.1016/j.neuroimage.2016.09.050
- Lewis, M. S., & Miller, L. S. (2007). Executive control functioning and functional ability in older adults. The Clinical Neuropsychologist, 21(2), 274–285. doi:10.1080/13854040500519752
- Luanaigh, C. Ó., & Lawlor, B. A. (2008). Loneliness and the health of older people. International Journal of Geriatric Psychiatry, 23(12), 1213–1221. doi:10.1002/gps.2054
- Luciana, M., Collins, P. F., Olson, E. A., & Schissel, A. M. (2009). Tower of London Performance in Healthy Adolescents: The Development of Planning Skills and Associations With Self-Reported Inattention and Impulsivity. Developmental Neuropsychology, 34(4), 461–475. doi:10.1080/87565640902964540
- Luhmann, M., & Hawkley, L. C. (2016). Age differences in loneliness from late adolescence to oldest old age. Developmental Psychology, 52(6), 943–959. doi:10.1037/dev0000117
- McDowd, J. M. (1997). Inhibition in attention and aging. The Journals of Gerontology Series B: Psychological Sciences and Social Sciences, 52B(6), P265–P273. doi:10.1093/geronb/52B.6.P265
- Miyake, A., Friedman, N. P., Emerson, M. J., Witzki, A. H., Howerter, A., & Wager, T. D. (2000). The unity and diversity of executive functions and their contributions to complex “Frontal Lobe” tasks: A latent variable analysis. Cognitive Psychology, 41(1), 49–100. doi:10.1006/cogp.1999.0734
- Nici, J., & Hom, J. (2013). Comparability of the computerized Halstead Category Test with the original version. Archives of Clinical Neuropsychology, 28(8), 824–828. doi:10.1093/arclin/act075
- Nigg, J. T. (2017). Annual Research Review: On the relations among self-regulation, self-control, executive functioning, effortful control, cognitive control, impulsivity, risk-taking, and inhibition for developmental psychopathology. Journal of Child Psychology and Psychiatry, 58(4), 361–383. doi:10.1111/jcpp.12675
- Olderbak, S., Wilhelm, O., Olaru, G., Geiger, M., Brenneman, M. W., & Roberts, R. D. (2015). A psychometric analysis of the reading the mind in the eyes test: Toward a brief form for research and applied settings. Frontiers in Psychology, 6, 1503. doi:10.3389/fpsyg.2015.01503
- Phillips, L. H., Wynn, V. E., McPherson, S., & Gilhooly, K. J. (2001). Mental planning and the Tower of London task. The Quarterly Journal of Experimental Psychology Section A, 54(2), 579–597. doi:10.1080/713755977
- Rainville, C., Lepage, E., Gauthier, S., Kergoat, M.-J., & Belleville, S. (2012). Executive function deficits in persons with mild cognitive impairment: A study with a Tower of London task. Journal of Clinical and Experimental Neuropsychology, 34(3), 306–324. doi:10.1080/13803395.2011.639298
- Raz, N., & Rodrigue, K. M. (2006). Differential aging of the brain: Patterns, cognitive correlates and modifiers. Neuroscience and Biobehavioral Reviews, 30(6), 730–748. doi:10.1016/j.neubiorev.2006.07.001
- Russell, D. W. (1996). UCLA Loneliness Scale (Version 3): Reliability, validity, and factor structure. Journal of Personality Assessment, 66(1), 20–40. doi:10.1207/s15327752jpa6601_2
- Santini, Z. I., Jose, P. E., York Cornwell, E., Koyanagi, A., Nielsen, L., Hinrichsen, C., Meilstrup, C., Madsen, K. R., & Koushede, V. (2020). Social disconnectedness, perceived isolation, and symptoms of depression and anxiety among older Americans (NSHAP): A longitudinal mediation analysis. The Lancet. Public Health, 5(1), e62–e70. doi:10.1016/S2468-2667(19)30230-0
- Schmeichel, B. J., Volokhov, R. N., & Demaree, H. A. (2008). Working memory capacity and the self-regulation of emotional expression and experience. Journal of Personality and Social Psychology; Washington , 95(6), 1526–1540. http://dx.doi.org.eproxy.lib.hku.hk/10.1037/a0013345 doi:10.1037/a0013345
- Singh, A., & Misra, N. (2009). Loneliness, depression and sociability in old age. Industrial Psychiatry Journal, 18(1), 51–55. http://dx.doi.org.eproxy.lib.hku.hk/10.4103/0972-6748.57861 doi:10.4103/0972-6748.57861
- Williams, P. G., Suchy, Y., & Rau, H. K. (2009). Individual differences in executive functioning: Implications for stress regulation. Annals of Behavioral Medicine, 37(2), 126–140. http://dx.doi.org.eproxy.lib.hku.hk/10.1007/s12160-009-9100-0 doi:10.1007/s12160-009-9100-0
- Wilson, R. S., Krueger, K. R., Arnold, S. E., Schneider, J. A., Kelly, J. F., Barnes, L. L., … Bennett, D. A. (2007). Loneliness and risk of Alzheimer disease. Archives of General Psychiatry, 64(2), 234–240. doi:10.1001/archpsyc.64.2.234
- Wright, L., Lipszyc, J., Dupuis, A., Thayapararajah, S. W., & Schachar, R. (2014). Response inhibition and psychopathology: A meta-analysis of go/no-go task performance. Journal of Abnormal Psychology, 123(2), 429–439. doi:10.1037/a0036295
- Wu, Z.-Q., Sun, L., Sun, Y.-H., Zhang, X.-J., Tao, F.-B., & Cui, G.-H. (2010). Correlation between loneliness and social relationship among empty nest elderly in Anhui rural area, China. Aging & Mental Health, 14(1), 108–112. doi:10.1080/13607860903228796
- Zheng, D., Dong, X., Sun, H., Xu, Y., Ma, Y., & Wang, X. (2012). The overall impairment of core executive function components in patients with amnestic mild cognitive impairment: A cross-sectional study. BMC Neurology, 12(1), 138. doi:10.1186/1471-2377-12-138