
Abstract
Objective
Given the lack of information on the psychological impact of COVID-19 on people aged ≥60, we aimed to describe their psychological responses to this pandemic and lockdown situation and compare them with those under 60 years of age.
Methods
Secondary analysis of a larger online cross-sectional study designed to determine the psychological impact of the COVID-19 pandemic and lockdown across Spain. We analyzed a total of 1690 respondents aged ≥60 years and compared them with 13,363 respondents under 60 years of age. We employed the Depression, Anxiety, and Stress Scale and the Impact of Event Scale to evaluate psychological responses.
Results
In all, 52.6% of women and 34.3% of men were found to be probable cases of any emotional distress (p < 0.001). In both sexes, the most common psychological response was avoidance behavior (34.7% and 23.8%, respectively), followed by depression (28.5 and 14.2%). Older women and men were considered probable cases of any emotional distress less often than younger ones (women: 52.6% vs. 72.3%, p < 0.001; men: 34.3% vs. 50.6%, p < 0.001). Finally, the results of the binary logistic regression showed that only depressive and stress responses are psychological factors associated with age group [age ≥ 60 years, O.R. = 0.617 (95% CI = 0.501 − 0.759) and 0.437 (95% CI = 0.334 − 0.573), respectively].
Conclusion
Contrary to our hypothesis and despite the high percentage of emotional distress we found in older adults, especially women, they are actually at lower risk of developing depressive and stress consequences from COVID-19 and lockdown than those under 60 years of age. That said, we believe our results highlight the need for expert guidance in this age group, especially older women living alone.
Introduction
Although a previous virus epidemic occurred in 2003, the current official declaration of emergency and lockdown is a new situation for the Spanish population and those of other European. Along with worry and even fear of becoming infected, citizens have to cope with the distressing experience of quarantine. To be confined at home implies the loss of freedom and separation from friends and family members (Brooks et al., Citation2020), as well as significant changes in daily routines, especially work or study activities. For Spaniards, who are culturally used to spending time with friends and families outside the home, it would require extra effort to adapt to this new situation. All these environmental factors may take a higher psychological toll on older people, as they also have to adapt to the biological, socioeconomic, and psychosocial risk factors of aging.
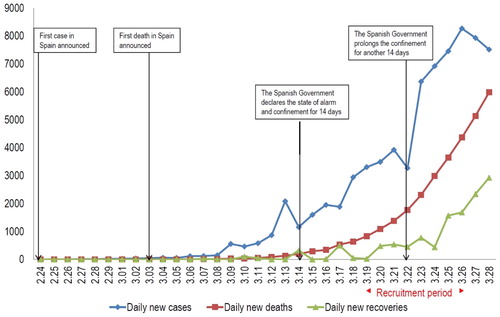
It is a well-known fact that older people have a higher risk of dying from a coronavirus infection (Applegate & Ouslander, Citation2020), yet there is no information concerning their psychological risk. In Spain, at the time we conducted the survey, people aged 60 or more accounted for 95% of deaths and 48.3% of the infected population according to the official statistics (Equipo COVID-19, Citation2020) (). Furthermore, social media and traditional media, including radio, TV, and newspapers, broadcast daily information on dramatic deaths in geriatric facilities, and the public debate on the dilemma of allocating scarce resources (such as mechanical ventilators) had started by that time. Thus, the psychological atmosphere surrounding COVID-19 was already more unfavorable for the older than for the younger population. On the other hand, the social distancing and isolation imposed by the crisis puts older adults at higher risk of developing or worsening mental health problems (Armitage & Nellums, Citation2020; Gerst-Emerson & Jayawardhana, Citation2015), including increased rates of depression, anxiety (Santini et al., Citation2020), post-traumatic stress disorder (Li et al., Citation2020), and suicide (Chan, Chiu, Lam, Leung, & Conwell, Citation2006; Yip, Cheung, Chau, & Law, Citation2010). However, it is necessary to point out that some studies show that older adults demonstrate resilience mechanisms that allow them to cope with adverse situations in a more positive way (Fontes & Neri, Citation2015; Silva Júnior et al., Citation2019). Furthermore, depression often affects the elderly, but it seems to be less severe and prolonged than in young people (Santos Lima et al., Citation2019).
Figure 1. The national epidemic trend of the outbreak of the coronavirus disease 2019 (COVID-19) and socio-psychological milestones in Spain from February 24 to March 28, 2020.
Given the lack of information on the psychological impact of COVID-19 in people aged 60 and over, we decided to carry out this sub-analysis to describe the psychological responses to the COVID-19 pandemic and the lockdown situation in this population and compare them with those of the respondents under 60 years of age. We hypothesized that older adults would experience a greater psychological impact due to both knowledge of their high risk of mortality if they become infected and the psychosocial consequences of lockdown, mainly isolation.
Methods
Design
This study is a secondary analysis of a larger cross-sectional study designed to determine the psychological impact of the COVID-19 pandemic and lockdown across Spain (for more details see García Álvarez et al., 2020). Between March 19 and 26, we administered an anonymous questionnaire through social networks and email using a snowball sampling method. To improve the external validity of the study, we used the researchers' interpersonal connections through social networks to encourage participation and maximum dissemination of the survey. In addition, academic and health institutions encouraged participation through their social networks, and email was used to ask different population profiles and organizations to participate and disseminate it as much as possible among their members and contacts.
The questionnaire was launched five days after the official declaration of emergency and 14-day lockdown order. Until then, the attitude toward COVID-19 in Spain was one of relative unconcern. However, on March 22, the Spanish President announced an extension of the lockdown due to the uncontrolled spread of the infection and the number of deaths.
The study followed the ethical principles of the Declaration of Helsinki (World Medical Association, Citation2013) and the Ethics Committee of Hospital Universitario Central de Asturias approved it (ref. 2020.162). All respondents had to sign the informed consent before they could answer the questionnaire.
Subjects
In this paper, we analyzed a total of 1690 respondents aged 60 years or over who reported not having/never having had any mental disorder. They represent 8% of the total respondents (n = 21.207). As a comparator group, we used all respondents under 60 years of age without a past or current mental disorder (n = 13,363). We decided to exclude subjects with self-reported past or current mental disorders because these two conditions were significantly less prevalent in the older than in the younger group (men: 16.5% vs. 20.8%, Chi-square = 12.170, p = 0.002; women: 28.3% vs. 33.3%, Chi-square = 21.487, p < 0.001). Furthermore, we had previously shown that these two conditions are risk factors for developing symptoms of emotional distress (García Álvarez et al., 2020).
The inclusion criteria of the study were: 1) being over 17 years or age and 2) giving informed consent by clicking ‘I am of legal age and wish to participate in this project,’ placed at the end of the information of the study and before the beginning of the questionnaire. There were no exclusion criteria.
Assessments
The questionnaire recorded self-reported sociodemographic information (age, sex, province of residence, education, marital status, living arrangement, work status, monthly income, changes in work status due to COVID-19, changes in monthly income due to COVID-19, number and age of dependent children, and dependent older adults) as well as information on physical health (no health conditions, hypertension, diabetes, cardiovascular and respiratory diseases, and cancer). COVID-19 variables included coronavirus testing (none, positive, negative, and results pending), coronavirus retesting, number of days with COVID-19 symptoms, COVID-19 symptoms (none, fever, dry cough, tiredness, congestion, muscle aches, headache, diarrhea, other), hospitalization due to COVID-19, number of family members infected with coronavirus and relationship to them, and number of household members infected with coronavirus. In addition, information on past and current psychiatric history was recorded (type of disorder, pharmacological and psychological treatment). Finally, respondents answered the Spanish versions of the two self-report questionnaires used to assess psychological impact: the Depression, Anxiety, and Stress scale (DASS-21) (Bados, Solanas, & Andrés, Citation2005) and the Impact of Event Scale (IES) (Báguena et al., Citation2001). The DASS-21 demonstrated internal reliability as well as convergent, divergent, and discriminant validity, while the IES scale demonstrated acceptable internal consistency.
These two questionnaires provide information on symptoms of emotional distress in reaction to a specific event or situation, in our case, the COVID-19 pandemic and lockdown situation, over the past week (see ).
Figure 2. Images of the beginning of the self-reported questionnaires that appeared to the subjects when they answered.
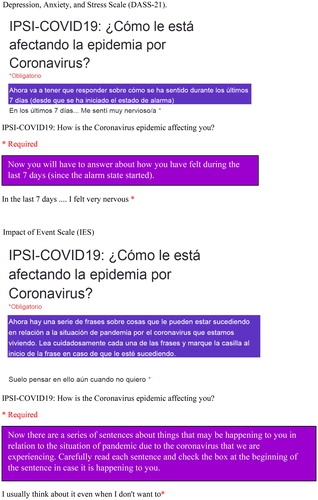
The DASS-21 evaluates depressive, anxious, and stress responses while the IES assesses intrusive thoughts and avoidant behaviors. On each of these five subscales, subjects can score between 0 and 7, except for on intrusive thoughts, which ranges between 0 and 8. In all cases, the higher the score, the greater the severity of the maladaptive response. Subscale scores between 0 and 3 were considered ‘not a case’ and >3 ‘a probable case.’ (For more details see García Álvarez et al., 2020 under review.)
Statistical analysis
We used IBM SPSS Statistics for Windows, version 24.0 (IBM Corp, Citation2016). The significance level was set at p < 0.05. For the descriptive analysis, we used means and standard deviations or frequencies and percentages, as appropriate. To identify differences between sex or age groups, we employed the Chi-square test or Student’s t-test depending on the type of variables.As there were statistically significant differences according to sex in all psychological variables, we decided to perform the analysis separately according to sex.
Finally, we conducted a binary logistic regression to determine the impact of psychological responses and a number of independent variables on the likelihood that respondents would be classified as having under 60 years or 60 years or over. The independent variables were identified in the univariate analyses (see of Supplementary material) and were introduced into the regression using a backward stepwise method.
Table 1. Sociodemographic characteristics and psychological impact of COVID-19 and lockdown according to sex.
Results
The mean age of the older sample was 65.9 (5.1) years, 50.8% were women, 72.3% were married or living as married, and only 17.8% were living alone. Concerning socioeconomic status, 72.3% had a university degree, 53.7% were retired, and 66.5% had monthly income > €1,499.
Sociodemographic data, physical diseases, COVID-19 variables, and psychological impact of the COVID-19 pandemic and lockdown in the older sample according to sex
As can be seen in , women were significantly younger than men [65.4 (4.8) vs. 66.5 (5.4), Student’s t-test = 4.451, p < 0.001), were less often married (61.0% vs. 84.0%, Chi-square = 112.955, p < 0.001), and they were more frequently living alone (24.9% vs. 10.5%, Chi-square = 67.817, p < 0.001). Regarding income, fewer earned more than €1,499 (58.4% vs. 70.0%, Chi-square = 91.229, p < 0.001), but more had not experienced changes in income due to COVID-19 (86.8% vs. 80.9%, Chi-square = 13.850, p = 0.008).
Fewer women reported having physical diseases than men (46.2% vs. 52.4%, Chi-square = 5.363, p = 0.022). However, no statistically significant differences were found in any of the COVID-19 variables studied according to sex.
Finally, compared with men, women scored significantly worse in the five psychological domains evaluated, and they were more often classified as a probable case, except in the anxious dimension (see ). In both sexes, the most common psychological response was avoidance behavior (women: 34.7%, men: 23.8%), followed by depression (28.5 and 14.2%, respectively) (see ). Furthermore, women were considered a probable case of any emotional distress response more frequently than men (52.6% vs. 34.3%, Chi-square = 57.667, p < 0.001).
Differences in psychological impact according to age
There were statistically significant differences between respondents of both sexes <60 years and ≥60 years of age in the majority of demographic, social, and physical variables (see of Supplementary material).
Results on the DASS-21 scale demonstrated that females and males aged ≥60 years scored significantly lower on the three subscales, and they were less often considered probably a case than those aged <60 years (see ). In almost all items, the older group chose the symptomatic answer less often than the younger group. The exceptions were on the depression subscale, where there were no statistically significant differences between the two age groups in items 3 and 2 in women and men, respectively (see ).
Table 2. Psychological impact according to age, for women and men separately.
Concerning the IES, in both sexes, those ≥60 years scored significantly lower on the two subscales and fewer were classified as a probable case than respondents aged <60 years. The analyses of specific questions identified similar answers between the two age groups in males for the majority of items on the avoidant behavior subscale (see ). Furthermore, older women and men were considered a probable case of any emotional distress less frequently than younger women and men (women: 52.6% vs. 72.3%, Chi-square = 146.631, p < 0.001; men: 34.3% vs. 50.6%, Chi-square = 146.631, p < 0.001).
Table 3. Factors associated with being classified as having under 60 years or 60 years or over.
Finally, the results of the binary logistic regression showed that only depressive and stress responses are psychological factors associated with age group [age ≥ 60 years, O.R. = 0.617 (95% CI = 0.501 − 0.759) and 0.437 (95% CI = 0.334 − 0.573), respectively] (see ).
Discussion
To our knowledge, this is the first study reporting on the psychological consequences of COVID-19 in older adults. We found that one in two women and one in three men self-reported symptoms of emotional distress that they attributed to the COVID-19 pandemic and lockdown, at least in one of the five psychological domains evaluated. The most common reactions in both sexes were avoidant behaviors, followed by depression, while the anxious response was the less common. Contrary to our hypothesis, older women and men reacted less frequently with depressive and stress responses than younger ones. It can be argued that our older group had a more comfortable socioeconomic status and a more benign COVID-19 profile, which may have softened the psychological impact derived from these factors, while younger people may have concerns about their future, regarding employment, children, financial problems, etc. due to the instability of their living conditions. However, on the other hand, they were separated/divorced/widowed, living alone, had dependent children, and had physical illnesses more often than respondents aged <60 years, factors that may work in the opposite direction.
Better capacity for resilience in the older adults would at least partially explain our findings. Resilience is ‘the process of adapting well in the face of adversity, trauma, tragedy, threats, or significant sources of stress’ (APA, Citation2020). It is an individual trait susceptible to improvement by practice (Southwick, Bonanno, Masten, Panter-Brick, & Yehuda, Citation2014); thus, it could be expected that older subjects have greater resilience as, in general, they have faced more stressful events than younger subjects. Furthermore, Spanish older adults were children and adolescents during the post-Civil War period and the Franco regime, which may have contributed to their resilience and, consequently, may now be softening the psychological impact of COVID-19. Although all these are speculations, results reported by Silva Júnior et al. (Citation2019) partially support them, since they found a high capacity for resilience in the elderly. Furthermore, one study showed that older adults are more psychologically resilient, especially with regard to emotional regulation and problem-solving, than the younger ones (Gooding, Hurst, Johnson, & Tarrier, Citation2012). In that sense, resilience in the elderly has been associated with positive outcomes, including adaptive coping, optimism, and lower symptoms of depression. (MacLeod, Musich, Hawkins, Alsgaard, & Wicker, Citation2016). Resilience could be the explanation for why older adults adapt better than other groups. This highlights the importance of designing interventions to enhance resilience in the general population, specifically to cope with future pandemics. Nevertheless, it is a pity that we did not ask about spiritual beliefs, a resource essential for coping with adversities of life that were significantly associated with resilience in the aforementioned study. Data on the Spanish population in 2018 revealed greater religiosity among older than younger adults (9.5% agnostic among those ≥65 years vs. almost 50% of those between 18 and 24 years) (Centro de Investigaciones Sociológicas, Citation2018), adding more support to that factor as a resilience contribution. Another possible explanation is that older people are more likely to adopt comprehensive precautionary measures as demonstrated in previous epidemic scenarios (Leung et al., Citation2003). These data are not consistent with previous studies the where the elderly had an increased risk of completed suicide after the 2003 SARS outbreak (Chan et al., Citation2006; Lau et al., Citation2008), as well as higher rates of depression and anxiety after the 2013 earthquake in China (Liang, Citation2017).
Social distancing is a risk factor for developing depression and anxiety in older Americans (Santini et al., Citation2020); however, our anxiety rate does not support this previous finding. Although American and Spanish societies have vast differences that may contribute to the discrepancies, we believe that other factors are mainly responsible. Among them, the content differences between the instruments employed to measure anxiety (DASS-21 vs. HADS), our study-specific relationship between psychopathological reactions to COVID-19 and lockdown, and short period of social distancing in our study are the principal factors. Furthermore, Armitage and Nellums (Citation2020) pointed out that the disproportionate effect of COVID-19 and isolation on the elderly would be primarily on those without social contacts at home. We found that only one in four women and one in ten men lived alone; thus, it may help to understand why our psychopathological reactions were lower than expected and why women experienced a more negative impact. This is in line with previous studies on COVID-19 and the SARS outbreak (Mihashi et al., Citation2009; Wang et al., Citation2020), which have shown that being female is associated with an increased likelihood of developing emotional distress symptoms. Furthermore, women were more frequently single or divorced and unemployed or homemakers, factors associated with a greater psychological impact (Esteban-Gonzalo, Aparicio, Estaban-Gonzalo, Citation2018).
It has been reported that post-traumatic stress disorder is the most common mental disorder after natural disasters (Neria, Nandi, & Galea, Citation2008), and being older has been identified as one of its risk factors (Li et al., Citation2020). In keeping with this, we demonstrated that avoidant behaviors were the most common psychological response in older subjects, while depression was more prevalent among younger subjects. It could be that avoidant behavior (i.e. not talking about the event, remove it from memory, trying not to think about it, etc.) may act as a psychological defense against worries and physical anxiety symptoms. Thus, this would explain the lower rates of anxious responses found in the elderly, but also the younger age group.
Readers should carefully consider the data we present here due to the main limitation of the study, i.e. the high socioeconomic profile of our sample. It was educated and, in general, had a good income for Spain, probably related to the need to have access to digital resources and be digitally literate and the snowball recruitment strategy. On the contrary, the large sample size and its national characteristics are a significant strength. Another important limitation is the cross-sectional design of the study and the lack of previous psychological status information.
Contrary to our hypothesis, our results show that despite the considerable proportion of symptoms of emotional distress we found in older adults, especially women, they are at a lower risk of developing psychological depressive and stress consequences from COVID-19 and lockdown than those under 60 years of age. This said, we believe our results support the urgent call by Lloyd-Sherlock et al. (Citation2020) to the WHO for expert guidance in this age group, especially older women living alone.
Supplemental Material
Download MS Word (57.1 KB)Acknowledgements
The authors wish to thank Sharon Grevet for her English assistance.
Disclosure statement
Paz Garcia-Portilla has been a consultant to and/or has received honoraria/grants from Angelini, Alianza Otsuka-Lundbeck, Instituto de Salud Carlos III, Janssen-Cilag, Lundbeck, Otsuka, Pfizer, and SAGE Therapeutics.
The rest of the authors report no conflicts of interest.
Additional information
Funding
References
- American Psychological Association. (2020, February 1). Building Your Resilience. Retrieved April 17, 2020, from https://www.apa.org/topics/resilience
- Applegate, W. B., & Ouslander, J. G. (2020). COVID-19 presents high risk to older persons. Journal of American Geriatric Society, 68(4), 681. doi:10.1111/jgs.16426
- Armitage, R., & Nellums, L. B. (2020). COVID-19 and the consequences of isolating the elderly. Lancet Public Health, 5(5), e256. doi:10.1016/S2468-2667(20)30061-X
- Bados, A., Solanas, A., & Andrés, A. (2005). Psychometric properties of the Spanish version of Depression, Anxiety and Stress Scale (DASS). Psicothema, 17, 679–683.
- Báguena, M. J., Villarroya, E., Beleña, A., Díaz, A., Roldán, C., & Reig, R. (2001). Propiedades Psicométricas de la Versión Española de la escala Revisada de Impacto del Estresor. Anales de Modificación de Conducta, 27, 581–604.
- Brooks, S. K., Webster, R. K., Smith, L. E., Woodland, L., Wessely, S., Greenberg, N., & Rubin, G. J. (2020). The psychological impact of quarantine and how to reduce it: Rapid review of the evidence. Lancet (London, England), 395(10227), 912–920. doi:10.1016/S0140-6736(20)30460-8
- Centro de Investigaciones Sociológicas. (2018). Media de Barómetros de 2018. Elaboración: Europa Laica Religiosidad por edad %. Año 2018. España. Retrieved April 17, 2020, from https://laicismo.org/grafica-religiosidad-por-edad-2018/
- Chan, S. M., Chiu, F. K., Lam, C. W., Leung, P. Y., & Conwell, Y. (2006). Elderly suicide and the 2003 SARS epidemic in Hong Kong. International Journal of Geriatric Psychiatry, 21(2), 113–118. doi:10.1002/gps.1432
- Equipo COVID-19. CSiViES. CNE. CNM (ISCIII). (2020). Informe sobre la situación de COVID-19 en España (Informe COVID-19 n° 17. 27.03.20). National Epidemiology Report. Madrid: ISCIII (Instituto de Salud Carlos III); CNE (National Center of Epidemiology).
- Esteban-Gonzalo, S., Aparicio, M., & Estaban-Gonzalo, L. (2018). Employment status, gender and health in Spanish women. Women Health,58(7), 744–758. https://doi.org/10.1080/03630242.2017.1353574
- Fontes, A. P., & Neri, A. L. (2015). Resilience in aging: Literature review. Ciencia & Saude Coletiva, 20(5), 1475–1495. doi:10.1590/1413-81232015205.00502014
- García Álvarez, L., de la Fuente Tomás, L., García-Portilla, M. P., Sáiz Martínez, P. A., Moya Lacasa, C., Dal Santo, F., … Bobes, J. (2020). Early psychological impact of the 2019 coranavirus disease (COVID-19) pandemic and lockdown in a large Spanish sample. Journal of Global Health.
- Gerst-Emerson, K., & Jayawardhana, J. (2015). Loneliness as a public health issue: The impact of loneliness on health care utilization among older adults. American Journal of Public Health, 105(5), 1013–1019. doi:10.2105/AJPH.2014.302427
- Gooding, P. A., Hurst, A., Johnson, J., & Tarrier, N. (2012). Psychological resilience in young and older adults. International Journal of Geriatric Psychiatry, 27(3), 262–270. doi:10.1002/gps.2712
- IBM Corp. (2016). IBM SPSS Statistics for Windows, Version 24.0. Armonk, NY: IBM Corp.
- Lau, A. L., Chi, I., Cummins, R. A., Lee, T. M., Chou, K. L., & Chung, L. W. (2008). The SARS (Severe Acute Respiratory Syndrome) pandemic in Hong Kong: Effects on the subjective wellbeing of elderly and younger people. Aging & Mental Health, 12(6), 746–760. doi:10.1080/13607860802380607
- Leung, G. M., Lam, T. H., Ho, L. M., Ho, S. Y., Chan, B. H., Wong, I. O., & Hedley, A. J. (2003). The impact of community psychological responses on outbreak control for severe acute respiratory syndrome in Hong Kong. Journal of Epidemiology & Community Health, 57(11), 857–863. doi:10.1136/jech.57.11.857
- Li, L., Reinhardt, J. D., Van Dyke, C., Wang, H., Liu, M., Yamamoto, A., … Hu, X. (2020). Prevalence and risk factors of post-traumatic stress disorder among elderly survivors six months after the 2008 Wenchuan earthquake in China. BMC Psychiatry, 20(1), 78. doi:10.1186/s12888-020-2474-z
- Liang, Y. (2017). Depression and anxiety among elderly earthquake survivors in China. Journal of Health Psychology, 22(14), 1869–1879. doi:10.1177/1359105316639437
- Lloyd-Sherlock, P. G., Kalache, A., McKee, M., Derbyshire, J., Geffen, L., Gomez, O., & Casas, F. (2020). WHO must prioritise the needs of older people in its response to the covid-19 pandemic. BMJ, 368, m1164.
- MacLeod, S., Musich, S., Hawkins, K., Alsgaard, K., & Wicker, E. R. (2016). The impact of resilience among older adults. Geriatric Nursing, 37(4), 266–272. doi:10.1016/j.gerinurse.2016.02.014
- Mihashi, M., Otsubo, Y., Yinjuan, X., Nagatomi, K., Hoshiko, M., & Ishitake, T. (2009). Predictive factors of psychological disorder development during recovery following SARS outbreak. Health Psychology: Official Journal of the Division of Health Psychology, American Psychological Association, 28(1), 91–100. doi:10.1037/a0013674
- Neria, Y., Nandi, A., & Galea, S. (2008). Post-traumatic stress disorder following disasters: A systematic review. Psychological Medicine, 38(4), 467–480. doi:10.1017/S0033291707001353
- Santini, Z., Jose, P., Cornwell, E., Koyanagi, A., Nielsen, L., Hinrichsen, C., … Koushede, V. (2020). Social disconnectedness, perceived isolation, and symptoms of depression and anxiety among older Americans (NSHAP): A longitudinal mediation analysis. The Lancet Public Health, 5(1), e62–70–e70. doi:10.1016/S2468-2667(19)30230-0
- Santos Lima, G., Oliveira Souza, I. M., Baldin Storti, L., Silva, M. M. J., Kusumota, L., & Marques, S. (2019). Resilience, quality of life and symptoms of depression among elderlies receiving outpactient care. Revista Latino-Americana de Enfermagem, 27, e3212. doi:10.1590/1518-8345.3133.3212
- Silva Júnior, E. G. D., Eulálio, M. D C., Souto, R. Q., Santos, K. D L., Melo, R. L. P. D., & Lacerda, A. R. (2019). The capacity for resilience and social support in the urban elderly. Ciencia & Saude Coletiva, 24(1), 7–16. doi:10.1590/1413-81232018241.32722016
- Southwick, S. M., Bonanno, G. A., Masten, A. S., Panter-Brick, C., & Yehuda, R. (2014). Resilience definitions, theory, and challenges: Interdisciplinary perspectives. European Journal of Psychotraumatology, 5(1), 25338. doi:10.3402/ejpt.v5.25338
- Wang, C., Pan, R., Wan, X., Tan, Y., Xu, L., Ho, C., & Ho, R. C. (2020). Immediate psychological responses and associated factors during the initial stage of the 2019 Coronavirus Disease (COVID-19): Epidemic among the General Population in China. International Journal of Environmental Research and Public Health, 17(5), 1729. doi:10.3390/ijerph17051729
- World Medical Association. (2013). World Medical Association declaration of Helsinki: Ethical principles for medical research involving human subjects. JAMA, 310, 2191–2194.
- Yip, P. S., Cheung, Y. T., Chau, P. H., & Law, Y. W. (2010). The impact of epidemic outbreak: The case of severe acute respiratory syndrome (SARS) and suicide among older adults in Hong Kong. Crisis, 31(2), 86–92. doi:10.1027/0227-5910/a000015