
 ?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.
?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.Abstract
Objectives
Multimorbidity poses various challenges, and previous research has indicated a causal relation with depression. As multimorbidity is not curable, the underlying mechanisms are of great interest. Positive affect is a major resource for coping with chronic conditions and for the prevention of depression. Long-term multimorbidity, however, may deplete positive affect. The purpose of this paper is to investigate the role of positive affect in the association between multimorbidity and depressive symptoms.
Method
We used four consecutive waves (2008, 2011, 2014, 2017) of the nationally representative German Ageing Survey (DEAS) with a total of 1,558 older adults aged 40 and over. To account for time-varying confounding, exposure-induced mediator-outcome confounding, and reciprocities, we applied the mediational g-formula with inverse-probability weighting techniques. We also tested for exposure-mediator interaction to adjust for differences in mediation across the duration of multimorbidity.
Results
We confirmed a positive longitudinal relation between multimorbidity and depressive symptoms, both of which were negatively associated with while positive affect. The model without interaction indicated a share mediated of ca. 18.3% on the total effect of multimorbidity on depressive symptoms. Addition of interaction led to substantial differences for multimorbidity duration and levels of positive affect. Associations for long-term multimorbidity (at least two survey waves) were more substantial, and the share mediated doubled (>40%). Additionally, the direct effect of multimorbidity on depressive symptoms diminished for short-term multimorbidity.
Conclusion
Strengthening positive affect could reduce depressive symptoms in those facing multimorbidity. This study also discusses methodological challenges in performing longitudinal mediation analysis. We advise researchers to consider the mediational g-formula and exposure-mediator interaction.
Introduction
Multimorbidity is the condition of having at least two chronic and incurable diseases (van den Akker, Buntinx, Roos, & Knottnerus, Citation2001). Interest in multimorbidity has considerably increased over the past two decades, as population ageing has led to higher rates of overall morbidity and multimorbidity (Tetzlaff, Muschik, Epping, Eberhard, & Geyer, Citation2017). For instance, in Germany, more than half of people aged 50 years and over are considered multimorbid, with increasing prevalence in older age groups (Puth, Weckbecker, Schmid, & Münster, Citation2017). The increase in multimorbidity poses challenges for healthcare systems, in terms of higher costs (Glynn et al., Citation2011), multi-professional treatments, polypharmacy and coordination demands (Moffat & Mercer, Citation2015). Furthermore, multimorbid patients suffer from various physical and psychological conditions that may mutually reinforce one another and increase the risk of depression (for a meta-analysis, see: Read, Sharpe, Modini, & Dear, Citation2017).
In general, multimorbidity imposes stressors on the individual. Additionally, the incurability of multimorbidity fosters the accumulation of stressors over time. Persistent exposure to stress increases the likelihood of depression (Folkman, Citation2012). In the ‘transactional model’ of Lazarus and Folkman (Citation1984), the impact of stress is determined by the perception, appraisal and reaction of it. Primary and secondary appraisal (appraisal-phase) of the stressor determine the resource allocation, which then determines the reaction or coping strategy (coping-phase). Under this lens, multimorbidity is a stressor that negatively affects (mental) health through increased symptoms, loss of physical functioning (Katon, Citation2003), and increased levels of anxiety, resulting in decreased quality of life (Gould, O'Hara, Goldstein, & Beaudreau, Citation2016).
The critical determinant for the prevention of stress and depressive symptoms is positive affect, which is the ability to experience positive emotions despite being exposed to stressful situations (Ashby, Isen, & Turken, Citation1999). Applied to the ‘transactional model’ of Lazarus and Folkman (Citation1984), positive affect reduces the perception of stress in the appraisal-phase. Among older adults, it is especially important for coping with stress (Ong, Bergeman, Bisconti, & Wallace, Citation2006), and for problem-solving (Paterson, Yeung, & Thornton, Citation2016). More precisely, it is involved in ‘positive reappraisal’, ‘problem-focused coping’ and ‘creation of positive events’ (Folkman & Moskowitz, Citation2000, pp. 650–651). The ‘broaden-and-build theory’ also supports the importance of positive affect in successful coping (Fredrickson, Citation2001; Fredrickson, Mancuso, Branigan, & Tugade, Citation2000). According to this theory, positive affect not only increases the repertoire of actions, but also helps in acquiring and maintaining resources required for coping (Fredrickson & Cohn, Citation2008). Positive affect is the resource and mechanism of the coping process (Lyubomirsky, King, & Diener, Citation2005; Pressman, Jenkins, & Moskowitz, Citation2019).
According to the ‘tripartite model of anxiety and depression’ proposed by Clark and Watson (Citation1991), depression and anxiety share negative affect, whereas low positive affect has a discriminatory attribute towards depression. Hofmann, Sawyer, Fang, and Asnaani (Citation2012) elaborated on the association of depression and affect with the ‘emotion dysregulation model’. In this model, dysregulations of affective styles are antecedents of disorders. In this model, dysregulations in affect (e.g. low positive affect) are not equivalent to depression, but rather intermediate mechanisms in the development of depression. Similarly, the transdiagnostic approaches also emphasise the differentiation of anxiety disorders and depression from affect (Nolen-Hoeksema, Wisco, & Lyubomirsky, Citation2008; Wilamowska et al., Citation2010).
Numerous studies have documented positive affect as a buffering resource for stress (e.g. Sewart et al., Citation2019; Tugade & Fredrickson, Citation2007), which reduces the likelihood of developing depression (Bos et al., Citation2013; Garland et al., Citation2010; Lindahl & Archer, Citation2013; Xu et al., Citation2015) and improves the treatment of chronic disease (Hart, Vella, & Mohr, Citation2008; Schiavon, Marchetti, Gurgel, Busnello, & Reppold, Citation2016). As positive affect is an intermediate tangible factor, the distinction between positive affect and depression is also of practical relevance when planning interventions to reduce depression (Boumparis, Karyotaki, Kleiboer, Hofmann, & Cuijpers, Citation2016; Sin, Della Porta, & Lyubomirsky, Citation2011; Taylor, Lyubomirsky, & Stein, Citation2017; Vazquez, Citation2017).
Positive affect is depletable, however. In a longitudinal study of older adults (aged 75 to 94), Wahl, Drapaniotis, and Heyl (Citation2014) showed, that loss of functional status decreases positive affect, even after adjustment for potential reverse-causality. Similarly, Gana et al. (Citation2016) showed in a longitudinal analysis that health status predicts subsequent levels of positive affect in older adults. Also, extensive research has been conducted on the negative impacts of chronic diseases on personality traits (e.g. Jokela, Hakulinen, Singh-Manoux, & Kivimäki, Citation2014; Stanton, Revenson, & Tennen, Citation2007). Especially in settings where stressors persist regardless of the coping-result, a depletion of positive affect seems plausible (Moskowitz, Shmueli-Blumberg, Acree, & Folkman, Citation2012). Reduction of stress is nevertheless essential for the prevention of progredient deterioration of chronic conditions and even mortality (Prior et al., Citation2016).
The combination of persistent shortages of coping resources, inadequate coping and exposure to stress increases the vulnerability to inflammatory processes and diseases (Crestani, Citation2017; Seeman & McEwen, Citation1996). This connection helps to explain the bidirectional relation between multimorbidity and depressive symptoms. One example is the onset of cardiovascular diseases and depression. Not only does, depression increase the risk of cardiovascular diseases (Nicholson, Kuper, & Hemingway, Citation2006), but depression is also more likely after the onset of cardiovascular diseases (Williams, Citation2011). Additionally, there is also some evidence that positive affect mediates the association between depression and biological correlates, such as heart rate (Bhattacharyya, Whitehead, Rakhit, & Steptoe, Citation2008; Steptoe, Dockray, & Wardle, Citation2009), blood pressure and cortisol levels (Bostock, Hamer, Wawrzyniak, Mitchell, & Steptoe, Citation2011).
To summarise, we argue that positive affect mediates the association of multimorbidity and depressive symptoms for three reasons. First, according to the ‘transactional model’ by Lazarus and Folkman (Citation1984) and the ‘broaden-built-theory’ by Fredrickson (Citation2001), positive affect is the most important mechanism for coping with stress. Second, as demonstrated by Wahl et al. (Citation2014) and Gana et al. (Citation2016), multimorbidity is accompanied by reductions in physical health, which deplete positive affect over time. Third, depletion of positive affect increases adverse outcomes of the coping process and emotion dysregulations, thus facilitating depressive symptoms. We evaluate this process as unidirectional in the cross-section, although we also acknowledge that longitudinal-wise it is reciprocal. Reduced positive affect and increased depressive symptoms could worsen or even cause multimorbidity. We will consider the reciprocity further in the method section.
We also test for moderations between multimorbidity and positive affect (XM-interaction). XM-interaction implies that the effect of multimorbidity on depressive symptoms varies (interacts) with the level of positive affect and vice-versa. In the context of multimorbidity and positive affect, testing for XM-interaction is especially important, because the assumption that the mediational process is equal across all multimorbidity durations is unlikely to be true. The longer the exposure to multimorbidity, the greater the depletion of positive affect and thus the degree of mediation. We state the following hypotheses:
H1: Multimorbidity increases depressive symptoms.
H2: Positive affect is a longitudinal mediator of the relation between multimorbidity and depressive symptoms.
H3: Duration of multimorbidity increases the strength of mediation by positive affect.
However, the association between multimorbidity, positive affect and depressive symptoms may be ameliorated by additional factors. These confounding factors affect at least two variables of interest simultaneously (Pearl, Citation2009). The reciprocal relations between multimorbidity, positive affect and depressive symptoms can be considered as confounding factors. Another confounder of multimorbidity and positive affect is age. Ageing increases the likelihood of multimorbidity and reduces positive affect (Charles, Reynolds, & Gatz, Citation2001). Additionally, stress-buffering factors such as social relations may confound the multimorbidity depression association through health-behavioural, psychological or biological pathways (Berkman, Glass, Brissette, & Seeman, Citation2000). The underlying conditions of multimorbidity are also stratified by sex. For instance, men face an increased risk of cardiometabolic diseases, and women face an increased risk of mechanical limitations (Schäfer et al., Citation2012). Women are also more likely than men to experience depressive symptoms throughout their lives (Nolen-Hoeksema, Citation2001). Socio-economic-status (SES) shapes the social environment and subjective wellbeing (Pinquart & Sörensen, Citation2000). More recent research suggests that SES, in lifetime perspectives, can even contribute to the development of multimorbidity (Singer, Green, Rowe, Ben-Shlomo, & Morrissey, Citation2019). There are other confounding factors at the health-behavioural level. For instance, regular physical activity, even for the chronically ill, is a protective factor against the development of depression, and it increases self-rated health in general (Faß, Pyun, & Schlesinger, Citation2020).
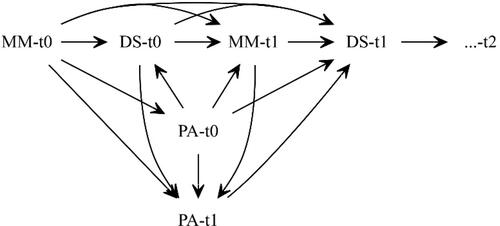
The depicted directed acyclic graph (DAG) provides a further illustration of the theoretical implications (Pearl, Citation1995).
Methods
Data
We used data from the German Ageing Survey (DEAS), which is a cross-sectional and longitudinal nationally representative study of people aged 40 and older (Klaus et al., Citation2017). Funded by the German Federal Ministry of Family Affairs, Senior Citizens, Women and Youth (BMFSFJ), the DEAS is an ongoing survey, started in 1996. Overall the DEAS consists of six survey time-points (1996, 2002, 2008, 2011, 2014, 2017), each with different samples. For the survey waves in 1996, 2002, 2008 and 2014, nationally representative samples (cross-sections) were drawn. The survey method consists of computer-assisted personal interviews (CAPIs) and self-completed questionnaires (drop-off). The main research areas of the survey are employment and retirement; health and health behaviour; quality of life; and subjective wellbeing. The longitudinal design and the main research areas make the dataset well suited for the aim of analysis.
To maximise the number of cases and time-points, we used data from panel participants within four time-points, spanning nearly a decade (2008, 2011, 2014, 2017). We excluded the earlier waves (1996 and 2002) from analysis due to the longer gaps between surveys (6 years) and the high number of drop-outs. Additionally, in 2008 a new starting cohort joined the panel. The panel participation rate of the starting sample in 2008 (N = 6,205) is about 46% in 2011 (N = 2,858), about 41% (N = 2,569) in 2014 and about 34% (N = 2,109) between 2014 and 2017. The eligible birth cohorts were 1923 to 1968. Furthermore, the drop-off questionnaire had lower participation than the CAPI.
illustrates the sample selection process. The data restriction criteria were continuous observation since 2008 and uninterrupted participation in the CAPI and the drop-off questionnaire. As we wanted to inspect changes of multimorbidity, positive affect and depressive symptoms within individuals over four points in time, we required valid values for the primary analysis variables. In total, 125 respondents were removed from the analysis due to missing or incomplete values for the analysis variables (case-wise deletion). From the initial 6,089 respondents in 2008, only 1,558 remained in the final analysis sample in 2017. Missing panel-participation consent caused the highest amount of respondent loss.
Measurements: Positive affect, depressive symptoms and multimorbidity
Since its start, the DEAS has surveyed positive affect with the PANAS-Scale developed by Watson, Clark, and Tellegen (Citation1988). The scale ranges from 1 to 5 with pseudo-metric values. Moreover, the DEAS has continuously surveyed depressive symptoms based on the 15-item German ADS-K (Allgemeine Depressions Skala–Kurzform; Hautzinger & Bailer, Citation1993), which is an adaptation of the CES-D (Radloff, Citation1977). On the ADS-K, respondents score from 0 to 42, with higher values indicating greater depressive symptoms.
In the CAPI, respondents tick on a list the diseases with which they have been diagnosed. Applicable conditions are coded as 1, non-applicable ones as 0. Applicable conditions are summed to a morbidity sum-score. As multimorbidity can be defined as ‘the co-occurrence of multiple diseases and medical conditions within one person’ (van den Akker, Buntinx, & Knottnerus, Citation1996, p. 69), multimorbidity was operationalised as a binary measurement, which means that only individuals with a morbidity sum-score greater than two are counted as multimorbid. Using a binary measurement for multimorbidity is common practice in epidemiology (e.g. Barnett et al., Citation2012; Fortin, Stewart, Poitras, Almirall, & Maddocks, Citation2012; Pefoyo et al., Citation2015) and psychology (e.g. Kristensen, König, & Hajek, Citation2019; Palladino, Tayu Lee, Ashworth, Triassi, & Millett, Citation2016). We set a somewhat restrictive definition of multimorbidity of more than two conditions (for reviews on definitions, see Diederichs, Berger, & Bartels, Citation2011; Yarnall et al., Citation2017). Our definition allows us to distinguish multimorbidity from co-morbidity (van den Bussche et al., Citation2011). provides a more detailed description of the diseases counted in the morbidity sum-score.
Table 1. Overview of measurements used for data analysis.
Measurements: Confounding factors
We selected covariates based on their assumed confounding effect on the longitudinal process. We divided them into time-varying and time-constant confounders. The time-constant confounders were sex (binary), age (metric) and education (ISCED-classification) as a sub-dimension of SES. The time-varying confounders were social relations, for which we used the proxy measure of family status (binary), and health behaviours, measured by smoking status (binary) and physical activity (categorical). also lists the categories and values of all measurements.
Longitudinal mediation analyses
Our investigation focuses on the mediation of the effect of multimorbidity on depressive symptoms
by positive affect
Although empirical studies of mediation have a long tradition (Baron & Kenny, Citation1986; Hayes, Citation2009), the conditions under which these analyses can identify direct and indirect effects have been detailed only recently. These are often captured under the term ‘sequential ignorability’ (Imai, Keele, & Tingley, Citation2010) or ‘unconfoundedness assumptions’ (Pearl, Citation2014; Shpitser & VanderWeele, Citation2011) and require the researcher to measure and adjust for common causes of the exposure, the mediator and the outcome. The first three assumptions (A to C) all address the confounding between exposure, mediator and outcome. The last assumption (D) states that there must be no mediator-outcome confounder that is affected by the exposure, regardless of the observability of such confounders, which means that even adjusting for this type of confounding is insufficient. In longitudinal mediational settings, however, this type of confounding (D-confounding) is very likely to occur (VanderWeele, Vansteelandt, & Robins, Citation2014).
Especially in the setting of multimorbidity, positive affect and depressive symptoms, D-confounding is inherent due to the reciprocal process. illustrates D-confounding. Depressive symptoms at t0 (DS-t0) confound the path between positive affect at t1 (PA-t1) and depressive symptoms at t1 (DS-t1) while also being influenced by multimorbidity at t0 (MM-t0), which renders the depressive symptoms at t0 as a D-confounder. Our analysis, therefore, requires sophisticated methods that specifically account for D-confounding.
Figure 1. Simplified DAG.
Note: MM = Multimorbidity; PA = Positive affect; DS = Depressive symptoms. Depicted time-points t0 and t1. Confounding factors and time-points t2 and t3 omitted for illustration purposes.
Mediational g-formula
As a solution to D-confounding, VanderWeele and Tchetgen Tchetgen (Citation2017) proposed the mediational g-formula. This formula cancels the exposure-induced mediator outcome confounding by simultaneously intervening on the mediator and fixing its distribution (for a detailed proof, see: VanderWeele & Tchetgen Tchetgen, Citation2017, pp. 921–922).
The practical application of this method follows three steps: (1) adjustment for D- confounding by inverse probability weighting (IPW); (2) the estimation of two marginal structural models (MSM), an outcome model and a mediator model, each weighted by its IPW of step 1; and (3) multiplication and bootstrapping of the coefficients derived from step 2.
For the calculation of the IPWs in step 1, we used logistic regressions to estimate the probability of being multimorbid at each time-period. We used least-square regressions for the estimated probability of the level of positive affect at each time-point, using the previous values of multimorbidity, positive affect and depressive symptoms as time-varying confounders. The addition of these previous values adjusts the weights for the reciprocity. We further stabilised the weights as suggested by Robins, Hernán, and Brumback (Citation2000). Additionally, we truncated the 1st and the 99th percentiles to improve stability. In settings where the occurrences of certain combinations of
are implausible to occur, truncation has become a standard practice for applying IPWs (Cole & Hernán, Citation2008). This especially holds for multimorbidity, as multiple changes are unlikely during the observation period.
We used these weights for the MSMs of step 2 and applied generalised linear models with maximum likelihood optimisation and clustered standard errors at the individual level. The first MSM is the outcome model (EquationEq. (1)(1)
(1) ). This model estimates the cumulative effect of the multimorbidity
and positive affect
trajectories on depressive symptoms; where
is the sum of multimorbidity exposures after t0 and
is the sum of the positive affect scores after t0. EquationEquation (1)
(1)
(1) tests for H1, the direct effect of multimorbidity on depressive symptoms.
(1)
(1)
The second MSM is the mediator model, which evaluates the effect of the average multimorbidity trajectory on positive affect. EquationEquation (2)(2)
(2) tests the assumption that multimorbidity decreases positive affect. We use the identity link function because positive affect is continuously measured.
(2)
(2)
In step 3, as shown by VanderWeele and Tchetgen Tchetgen (Citation2017, pp. 927–928), the interventional direct effect (IDE) and interventional indirect effect (IIE) can be calculated using EquationEq. (3)(3)
(3) .
(3)
(3)
The IDE equals the coefficient for multimorbidity () of EquationEq. (1)
(1)
(1) multiplied over all time-points
which is the cumulative direct effect of multimorbidity on depressive symptoms. The IIE is the product of multimorbidity’s effect on positive affect
and positive affect effect on depressive symptoms (
on all time-periods (
Therefore, the IIE captures the quantity of multimorbidity’s effect on depressive symptoms that proceeds through positive affect.
H3 assumed that longer durations of multimorbidity would deplete positive affect more strongly; thus, the mediation would be different. The mediational g-formula is flexible towards XM-interactions, which allows for testing moderated mediation. EquationEquation (4)(4)
(4) extends EquationEq. (1)
(1)
(1) with an interaction term, allowing the mediation by positive affect to be different for the duration of multimorbidity.
(4)
(4)
The interventional effects can be calculated through Eq. (5), as demonstrated by VanderWeele and Tchetgen Tchetgen (Citation2017, pp. 934–936).
(5)
Generally, the interventional effects (EquationEqs. (3)(3)
(3) and (5)) provide an intuitive interpretation. They express the difference in depressive symptoms if positive affect’s distribution would have been the same (intervened), irrespective of multimorbidity status. In some cases, interventional effects are even of primary interest. This especially holds in the context of multimorbidity, as positive affect is more tangible than multimorbidity. In this setting, interventional effects are of practical relevance, because they could potentially be realised through interventions on positive affect (VanderWeele & Tchetgen Tchetgen, Citation2017, p. 921). In the online supplementary material, we provide step-by-step Stata code for the estimation of the IPWs and the interventional effects. The Appendix includes the formulas used to obtain the set of IPWs (EquationEqs. (6)
(6)
(6) and Equation(7)
(7)
(7) ).
Results
Descriptive statistics
displays the distribution of the main variables and age between different nested samples. The starting sample of is the parent sample, which consists of all individuals who participated in 2008 (t0). The remained at t3 sample consists of all individuals who were observable in 2008 and in 2017 (t3). The final analysis sample consists of all the individuals who were consistently observed between 2008 and 2017 with valid entries at each measurement occasion. We calculated selectivity effects according to Lindenberger, Singer, and Baltes (Citation2002). The total selectivity (TS) compares the parent sample with the analysis sample. The TS decomposes into mortality-associated selectivity (MAS), which is the selectivity between the remain at t3 sample and the parent sample, and the experimental selectivity (ES), which is the selectivity between the remain at t3 sample and the analysis sample. The selectivity effect sizes can be interpreted according to Cohen (Citation1977).
Figure 2. Flow chart for the analysis data selection of the German Ageing Survey (DEAS). Note: Survey time-points are: t0 = 2008, t1 = 2011, t2 = 2014, t3 = 2017.
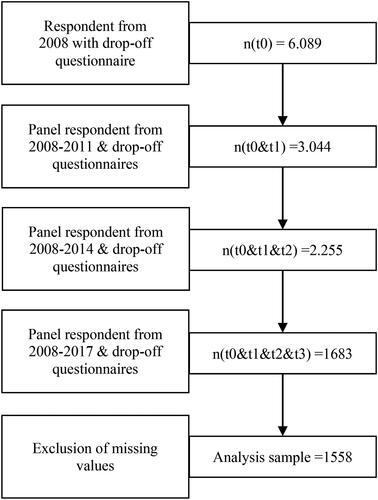
Table 2. Distributional properties of analysis variables and sample selectivity.
In total, multimorbidity increased in the parent sample from 37.5% in t0 to 47.5% in t3. The total selectivity at t0 is −0.110, indicating a low selectivity effect towards less morbid individuals. Similarly, there is a low selectivity of age at t0 (TS = −0.199). The TS of depressive symptoms is < −0.1, indicating only a weak selection towards less depressed individuals. The TS for positive affect is slightly higher (0.128 at t0), showing a low selectivity towards individuals with higher positive affect. In summary, we found a low selectivity caused by the MAS towards younger, less morbid individuals with higher positive affect.
lists the reliability measure Cronbach’s alpha for the sum scores of positive affect and depressive symptoms for all measurement occasions. Overall, the reliabilities of the sum scores were similar and acceptable, with a Cronbach’s alpha ranging from 0.830 to 0.850.
Table 3. Reliability measure for positive affect and depressive symptoms.
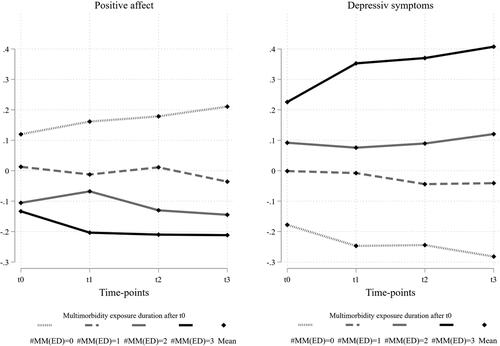
To illustrate the difference in mean changes between the multimorbidity exposure durations, we Z-standardised the measures of positive affect and depressive symptoms to a mean of 0 and a SD of 1.
indicates coherent changes for positive affect and depressive symptoms. Increased exposure duration to multimorbidity results in decreased positive affect and increased depressive symptoms over time. The comparison of the mean differences between those ‘never’ observed as multimorbid and ‘always’ observed as multimorbid after t0 indicate larger differences in depressive symptoms. Together both groups represent the majority (63.41%) of observations in the analysis sample. The differences in mean at t3 between these groups are 0.7 (0.4 to −0.3) for depressive symptoms and 0.4 (0.2 to −0.2) for positive affect.
Figure 3. Mean changes of Z-standardised positive affect and depressive symptoms over time and multimorbidity exposure duration.
Note: Changes in Z-standardised positive affect (left side) and depressive symptoms (right side) for the different multimorbidity exposure durations (MM(ED)) over the observation periods (t). MM(ED) = multimorbidity exposure duration after t0. Bold-black lines represent individuals continuously observed as multimorbid after t0 (#MM(ED) = 3). Dotted lines represent individuals never observed as multimorbid after t0 (#MM(ED) = 0).
Main results
displays the distributional properties of the stabilised weights before and after truncation. A high SD and mean value much larger than 1 indicates an unstable weight. Unstable weights are often present when the underlying models are not correctly specified (Cole & Hernán, Citation2008). In , all weights have mean values around 1.1, which indicates sufficient stability. Truncation increased stability further by reducing the SD. No case received a weight below 0.330 or above 5.26.
Table 4. Properties of calculated weights.
All models used the truncated weights. shows the respective coefficients. The estimated coefficients of the mediator and outcome model are highly significant (p < 0.001). The outcome model with interaction (M2) has a significant interaction (p < 0.01) with an appropriate effect size. The correlation of error terms between the mediator and outcome model provides information on the violation of confounding assumptions and ranges between −1 and 1 (Imai et al., Citation2010). Values of
can indicate the presence of unobserved confounding. shows that
Table 5. Effect size of MSM estimates.
contains the cumulative interventional effects with and without XM-interaction. In the model without XM-interaction (M1), all interventional effects are highly significant with an overall effect of 2.934, an indirect effect of 0.537 and a direct effect of 2.397. Thus, the share mediated amounts to 18.3%. After adding the interaction term in M2, the indirect effect becomes 0.759 and is highly significant, but the direct and overall effects are insignificant.
Table 6. Cumulative interventional effects without and with interaction.
To gain clearer insights into the effects changed by the XM-interaction we inserted the mean value of cumulative positive affect () into Eq. (5) for the different multimorbidity exposure durations. Practically, this would equal an intervention on positive affect to the mean value. We then calculated the share mediated relative to the effect sizes. The results reveal that the indirect and direct effects increase as exposure durations to multimorbidity increase (MM(ED) ≥ 2). At two exposure durations (MM(ED) = 2), the indirect effect is 4.365 (p < 0.01) with a share of the overall effect of 45.4%. At three exposure durations to multimorbidity (MM(ED) = 3), the indirect effect doubles in size to 8.732 (p < 0.01). The overall effect is 21.643 (p < 0.001), and the share mediated by positive affect is about 40.3%. For the ‘once’ or ‘never’ multimorbidity exposure durations, we omitted the percentage mediated due to the missing direct and total effects. The comparison of M1 and M2 in reveals that the mediation differs vastly after the addition of an interaction.
illustrates the difference in the level of mediation between the multimorbidity exposure durations (MM(ED) ≤ 1 vs. MM(ED) ≥ 2); see also, Fritz and MacKinnon (Citation2008). It contrasts the linear predictions of the outcome models from and M2) for the multimorbidity exposure duration groups MM(ED) ≤ 1 and MM(ED) ≥ 2.
Figure 4. Difference in mediation between M1 and M2 for different multimorbidity exposure durations.
Note: Presented differences are between the multimorbidity exposure duration groups: MM(ED) ≤ 1 & MM(ED) ≥ 2. M1: mediation model without interaction; M2: mediation model with interaction. Predictions obtained from .
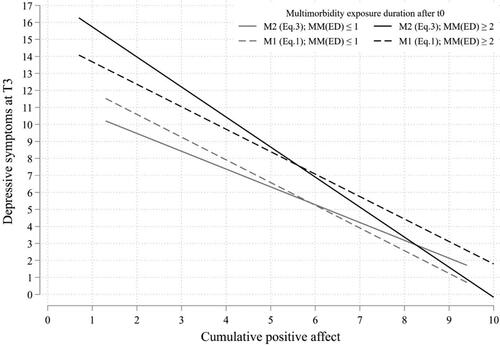
also illustrates that equality of mediation for all exposure durations of multimorbidity is not true. M1, however, assumes equal mediation for the exposure durations of multimorbidity, as shown by the parallel linear predictions (dashed lines) at different levels. After inclusion of the XM-interaction (M2), the predictions are not parallel, as shown by the difference between the bold lines. In comparison to M1, M2 shows a much steeper prediction for individuals with prolonged exposure to multimorbidity (bold black line vs. dashed black line). The prediction is less steep for individuals with short or recent exposure to multimorbidity (bold grey line vs. dashed grey line).
Discussion
Our investigation focused on the longitudinal relation between multimorbidity, positive affect and depressive symptoms in older adults (aged 40 and older) living in Germany. We hypothesised (H1) that exposure to multimorbidity increases the risk of depressive symptoms due to expanded stressor exposure. We argued that positive affect is the primary mechanism in coping with stress but that it is also depleted by chronic exposure to stress. Consequently, we hypothesised (H2) that the stressors of multimorbidity lead to changes in positive affect. We further argued that the depletion of positive affect increases as the duration of multimorbidity increases. Thus, we hypothesised (H3) that the degree of mediation is relative to the exposure duration of multimorbidity.
The major methodological challenge was exposure-induced mediator-outcome confounding (D-confounding). We responded to this challenge by using the mediational g-formula proposed by VanderWeele and Tchetgen Tchetgen (Citation2017). Additionally, we expanded the mediational g-formula with an XM-interaction to test H3. We used representative data from the German Ageing Survey (DEAS). Moreover, we observed our analysis population for nearly a decade within four distinct survey-points. This enabled us to note individual changes of multimorbidity, positive affect and depressive symptoms.
The results support all our hypotheses. M1 (EquationEq. (1)(1)
(1) ) indicated that the multimorbidity duration had a highly significant effect on depressive symptoms, and therefore supports H1 (multimorbidity increases depressive symptoms). M1 also indicated that positive affect had a highly significant negative effect on depressive symptoms. The mediator model (EquationEq. (2)
(2)
(2) ) showed that multimorbidity had a significant negative effect on positive affect. Positive affect reduces depressive symptoms and multimorbidity reduces positive affect. The product of these effects is the indirect effect (IIE); that is, the effect of multimorbidity on depressive symptoms that is transmitted by positive affect. This effect is highly significant and amounts to 18.3% of the overall effect (IOE), and thus supports H2.
However, and M2 revealed that the level of mediation is relative to the duration of exposure to multimorbidity. We found no direct effect on depressive symptoms for individuals that were never or only once observed as multimorbid, thus implying no mediation by positive affect. In contrast to M1, M2 shows that longer exposure to multimorbidity has greater significant direct effects on depressive symptoms and greater significant indirect effects by positive affect. Likewise, the share mediated by positive affect more than doubled for individuals with at least two durations of exposure to multimorbidity. Consequently, the results confirm H3: The degree of mediation is relative to the duration of exposure to multimorbidity. We strongly recommend that mediation analysts test for exposure-mediator interaction, because the assumption that the level of mediation is equal across all exposure groups is hazardous (MacKinnon, Valente, & Gonzalez, Citation2020). In the following paragraphs, we will discuss these results based on data (self-)selection, measurements, alternative empirical strategies, and theoretical explanations.
The selectivity effects in revealed a low selection towards less morbid and younger older adults with less positive affect. The selectivity towards less depressed individuals was relatively low (TS < −0.1). Overall, the selectivity was mostly caused by attrition in participation at T3 (MAS). Concerning the probability of a type-II error and the statistical validity of our findings, we evaluate the effect of this selection on the estimator as conservative.
Theoretical and methodological considerations shaped the decision on the selection of confounding variables. One shortcoming is our measure for SES. Education does not capture all confounding effects of SES. For instance, old-age poverty might persist irrespective of educational degree. We added health behaviour and partnership status as time-varying confounders, but partnership status captures stress-buffering social dynamics in only a limited way. Additionally, these factors are especially relevant for ageing and multimorbidity (e.g. Ellwardt, van Tilburg, Aartsen, Wittek, & Steverink, Citation2015; Kristensen et al., Citation2019). Empirically, we interpret the correlation of the error terms from the mediator and outcome model () as small; yet, we cannot entirely cancel unobserved confounding out.
The multimorbidity measurement requires more reflection because of the underlying heterogeneity. To reduce heterogeneity, we distinguished between co-morbidity and multimorbidity. Yet, different disease profiles impose different stressors and coping demands on the individual (Hopman et al., Citation2016) and thus have a different impact on positive affect and depressive symptoms.
Regarding alternative, more conventional methods, structural equation modelling (SEM) might seem favourable. For instance, MacKinnon (Citation2008, pp. 204–206) also investigated on the longitudinal relation between
and
in his ‘autoregressive model III’. Although SEM is a flexible tool, there are some crucial drawbacks, such as increased complexity and computability issues in longitudinal settings. More importantly, the SEM approach does not identify direct and indirect effects if D-confounding is present (VanderWeele et al., Citation2014; VanderWeele & Tchetgen Tchetgen, Citation2017). Moreover, when dealing with XM-interactions, conventional methods, such as SEM, are less efficient than counterfactual methods (MacKinnon et al., Citation2020). The additional comparison between naïve and covariate adjusted models, provided in in the Appendix, shows that the covariate adjusted model yields biased, overcontrolled, estimates due to the violation of D-confounding; the naïve model ignores confounding, resulting in upwardly biased estimates. These comparisons illustrate the necessity of adequate methods when dealing with longitudinal mediations.
Table A1. Model comparison naïve vs. adjusted.
Concerning the causal implications of our results, we want to emphasise that ‘(…) no statistical test can ever identify the true causal model from the entire set of all logically possible models’ (Fiedler, Harris, & Schott, Citation2018, p. 100). However, Fiedler et al. (Citation2018) recommended at least the inspection of alternative mediators and causal models when conducting mediation analysis. We tested for two alternatives, as shown in in the Appendix.
An alternative mediator could be health behaviours, such as sports participation (e.g. Diegelmann et al., Citation2018). We performed the same mediation analysis as in M1, but with weekly sport participation as a mediator and positive affect as a confounder. We found no indirect effect of sports participation but there was still a direct effect of multimorbidity on depressive symptoms.
Another alternative model could be the bidirectional association between multimorbidity and depressive symptoms. We tested this by inverting the temporal order between multimorbidity and depressive symptoms while retaining positive affect as the intermediate. Although this model shows a significant direct effect of depressive symptoms on multimorbidity, the model also indicates a lower overall mediation in terms of significance and effect size. Additionally, the IPWs are less stable. We cannot entirely rule out inverse causality; however, we interpret these results as supportive of reciprocity and thus D-confounding. Prior depressive symptoms confound the current causal paths of our initial model. Yet, more investigation on the bidirectional association is required, especially about the confounding variables and the involved intermediate processes.
If we view our causal model and results as valid, the interpretation for health policy is straightforward. A potential intervention to promote positive affect in older adults with multimorbidity could reduce their depressive symptoms substantially (in the context of HIV, see Moskowitz et al., Citation2017). Although the mediation was greater for longer durations of multimorbidity, we do not explicitly advocate for interventions for these individuals only. It is crucial to block the negative impact of multimorbidity on positive affect before the emergence of depressive symptoms. Increasing positive affect and reducing depressive symptoms are also adequate for the prevention of chronic diseases.
Our analysis revealed that the longer the exposure to multimorbidity, the stronger the association with depressive symptoms. Positive affect mediated a substantial proportion of this association when the duration of multimorbidity was high. Since late-life depression predicts mortality through various pathways (e.g. van den Berg et al., Citation2019), we recommend promoting positive affect in the early stages of multimorbidity to prevent the development of depressive symptoms.
Supplemental Material
Download PDF (23 KB)References
- Ashby, F. G., Isen, A. M., & Turken, A. U. (1999). A neuropsychological theory of positive affect and its influence on cognition. Psychological Review, 106(3), 529–550. doi:https://doi.org/10.1037/0033-295x.106.3.529
- Barnett, K., Mercer, S. W., Norbury, M., Watt, G., Wyke, S., & Guthrie, B. (2012). Epidemiology of multimorbidity and implications for health care, research, and medical education: A cross-sectional study. The Lancet, 380(9836), 37–43. doi:https://doi.org/10.1016/S0140-6736(12)60240-2
- Baron, R. M., & Kenny, D. A. (1986). The moderator–mediator variable distinction in social psychological research: Conceptual, strategic, and statistical considerations. Journal of Personality and Social Psychology, 51(6), 1173–1182. doi:https://doi.org/10.1037//0022-3514.51.6.1173
- Berkman, L. F., Glass, T., Brissette, I., & Seeman, T. E. (2000). From social integration to health: Durkheim in the new millennium. Social Science & Medicine (1982), 51(6), 843–857. doi:https://doi.org/10.1016/S0277-9536(00)00065-4
- Bhattacharyya, M. R., Whitehead, D. L., Rakhit, R., & Steptoe, A. (2008). Depressed mood, positive affect, and heart rate variability in patients with suspected coronary artery disease. Psychosomatic Medicine, 70(9), 1020–1027. doi:https://doi.org/10.1097/PSY.0b013e318189afcc
- Bos, S. C., Macedo, A., Marques, M., Pereira, A. T., Maia, B. R., Soares, M. J., … Azevedo, M. H. (2013). Is positive affect in pregnancy protective of postpartum depression? Revista Brasileira de Psiquiatria, 35(1), 5–12. doi:https://doi.org/10.1016/j.rbp.2011.11.002
- Bostock, S., Hamer, M., Wawrzyniak, A. J., Mitchell, E. S., & Steptoe, A. (2011). Positive emotional style and subjective, cardiovascular and cortisol responses to acute laboratory stress. Psychoneuroendocrinology, 36(8), 1175–1183. doi:https://doi.org/10.1016/j.psyneuen.2011.02.009
- Boumparis, N., Karyotaki, E., Kleiboer, A., Hofmann, S. G., & Cuijpers, P. (2016). The effect of psychotherapeutic interventions on positive and negative affect in depression: A systematic review and meta-analysis. Journal of Affective Disorders, 202, 153–162. doi:https://doi.org/10.1016/j.jad.2016.05.019
- Charles, S. T., Reynolds, C. A., & Gatz, M. (2001). Age-related differences and change in positive and negative affect over 23 years. Journal of Personality and Social Psychology, 80(1), 136–151. doi:https://doi.org/10.1037/0022-3514.80.1.136
- Clark, L. A., & Watson, D. (1991). Tripartite model of anxiety and depression: Psychometric evidence and taxonomic implications. Journal of Abnormal Psychology, 100(3), 316–336. doi:https://doi.org/10.1037/0021-843X.100.3.316
- Cohen, J. (1977). Statistical power analysis for the behavioral sciences (Rev. ed.). New York: Academic Press.
- Cole, S. R., & Hernán, M. A. (2008). Constructing inverse probability weights for marginal structural models. American Journal of Epidemiology, 168(6), 656–664. doi:https://doi.org/10.1093/aje/kwn164
- Crestani, C. C. (2017). Adolescent vulnerability to cardiovascular consequences of chronic emotional stress: Review and perspectives for future research. Neuroscience and Biobehavioral Reviews, 74(Pt B), 466–475. doi:https://doi.org/10.1016/j.neubiorev.2016.03.027
- Diederichs, C., Berger, K., & Bartels, D. B. (2011). The measurement of multiple chronic diseases-a systematic review on existing multimorbidity indices. The Journals of Gerontology, Series A, 66(3), 301–311. doi:https://doi.org/10.1093/gerona/glq208
- Diegelmann, M., Jansen, C. P., Wahl, H. W., Schilling, O. K., Schnabel, E. L., & Hauer, K. (2018). Does a physical activity program in the nursing home impact on depressive symptoms? A generalized linear mixed-model approach. Aging & Mental Health, 22(6), 784–793. doi:https://doi.org/10.1080/13607863.2017.1310804
- Ellwardt, L., van Tilburg, T., Aartsen, M., Wittek, R., & Steverink, N. (2015). Personal networks and mortality risk in older adults: A twenty-year longitudinal study. PloS One, 10(3), e0116731. doi:https://doi.org/10.1371/journal.pone.0116731
- Faß, E., Pyun, H., & Schlesinger, T. (2020). Perception of aging in the relation between sport activity and self-rated health in middle and older age - A longitudinal analysis. SSM - Population Health, 11, 100610. doi:https://doi.org/10.1016/j.ssmph.2020.100610
- Fiedler, K., Harris, C., & Schott, M. (2018). Unwarranted inferences from statistical mediation tests–An analysis of articles published in 2015. Journal of Experimental Social Psychology, 75, 95–102. doi:https://doi.org/10.1016/j.jesp.2017.11.008
- Folkman, S. (2012). The Oxford handbook of stress, health, and coping. New York: Oxford University Press. https://doi.org/10.1093/oxfordhb/9780195375343.001.0001
- Folkman, S., & Moskowitz, J. T. (2000). Positive affect and the other side of coping. American Psychologist, 55(6), 647–654. doi:https://doi.org/10.1037/0003-066X.55.6.647
- Fortin, M., Stewart, M., Poitras, M. E., Almirall, J., & Maddocks, H. (2012). A systematic review of prevalence studies on multimorbidity: Toward a more uniform methodology. Annals of Family Medicine, 10(2), 142–151. doi:https://doi.org/10.1370/afm.1337
- Fredrickson, B. L. (2001). The role of positive emotions in positive psychology: The broaden-and-build theory of positive emotions. American Psychologist, 56(3), 218–226. doi:https://doi.org/10.1037/0003-066X.56.3.218
- Fredrickson, B. L., & Cohn, M. A. (2008). Positive emotions. In M. Lewis, J. M. Haviland-Jones, & L. F. Barrett (Eds.), Handbook of emotions (pp. 777–796). New York: The Guilford Press.
- Fredrickson, B. L., Mancuso, R. A., Branigan, C., & Tugade, M. M. (2000). The undoing effect of positive emotions. Motivation and Emotion, 24(4), 237–258. doi:https://doi.org/10.1023/A:1010796329158
- Fritz, M. S., & MacKinnon, D. P. (2008). A graphical representation of the mediated effect. Behavior Research Methods, 40(1), 55–60. doi:https://doi.org/10.3758/brm.40.1.55
- Gana, K., Saada, Y., Broc, G., Quintard, B., Amieva, H., & Dartigues, J.-F. (2016). As long as you've got your health: Longitudinal relationships between positive affect and functional health in old age. Social Science & Medicine, 150, 231–238. doi:https://doi.org/10.1016/j.socscimed.2015.11.038
- Garland, E. L., Fredrickson, B., Kring, A. M., Johnson, D. P., Meyer, P. S., & Penn, D. L. (2010). Upward spirals of positive emotions counter downward spirals of negativity: Insights from the broaden-and-build theory and affective neuroscience on the treatment of emotion dysfunctions and deficits in psychopathology. Clinical Psychology Review, 30(7), 849–864. doi:https://doi.org/10.1016/j.cpr.2010.03.002
- Glynn, L. G., Valderas, J. M., Healy, P., Burke, E., Newell, J., Gillespie, P., & Murphy, A. W. (2011). The prevalence of multimorbidity in primary care and its effect on health care utilization and cost. Family Practice, 28(5), 516–523. doi:https://doi.org/10.1093/fampra/cmr013
- Gould, C. E., O'Hara, R., Goldstein, M. K., & Beaudreau, S. A. (2016). Multimorbidity is associated with anxiety in older adults in the health and retirement study. International Journal of Geriatric Psychiatry, 31(10), 1105–1115. doi:https://doi.org/10.1002/gps.4532
- Hart, S. L., Vella, L., & Mohr, D. C. (2008). Relationships among depressive symptoms, benefit-finding, optimism, and positive affect in multiple sclerosis patients after psychotherapy for depression. Health Psychology, 27(2), 230–238. doi:https://doi.org/10.1037/0278-6133.27.2.230
- Hautzinger, M., & Bailer, M. (1993). ADS, Allgemeine Depressions Skala. Manual. Weinheim: Beltz Test.
- Hayes, A. F. (2009). Beyond Baron and Kenny: Statistical mediation analysis in the new millennium. Communication Monographs, 76(4), 408–420. doi:https://doi.org/10.1080/03637750903310360
- Hofmann, S. G., Sawyer, A. T., Fang, A., & Asnaani, A. (2012). Emotion dysregulation model of mood and anxiety disorders. Depression and Anxiety, 29(5), 409–416. doi:https://doi.org/10.1002/da.21888
- Hopman, P., Bruin, S. R. D., Forjaz, M. J., Rodriguez-Blazquez, C., Tonnara, G., Lemmens, L. C., … Rijken, M. (2016). Effectiveness of comprehensive care programs for patients with multiple chronic conditions or frailty: A systematic literature review. Health Policy (Amsterdam, Netherlands)), 120(7), 818–832. doi:https://doi.org/10.1016/j.healthpol.2016.04.002
- Imai, K., Keele, L., & Tingley, D. (2010). A general approach to causal mediation analysis. Psychological Methods, 15(4), 309–334. doi:https://doi.org/10.1037/a0020761
- Jokela, M., Hakulinen, C., Singh-Manoux, A., & Kivimäki, M. (2014). Personality change associated with chronic diseases: Pooled analysis of four prospective cohort studies. Psychological Medicine, 44(12), 2629–2640. doi:https://doi.org/10.1017/S0033291714000257
- Katon, W. J. (2003). Clinical and health services relationships between major depression, depressive symptoms, and general medical illness. Biological Psychiatry, 54(3), 216–226. doi:https://doi.org/10.1016/S0006-3223(03)00273-7
- Klaus, D., Engstler, H., Mahne, K., Wolff, J. K., Simonson, J., Wurm, S., & Tesch-Römer, C. (2017). Cohort profile: The German ageing survey (DEAS). International Journal of Epidemiology, 46(4), 1105–1105g. doi:https://doi.org/10.1093/ije/dyw326
- Kristensen, K., König, H. H., & Hajek, A. (2019). The longitudinal association of multimorbidity on loneliness and network size: Findings from a population‐based study. International Journal of Geriatric Psychiatry, 34(10), 1490–1497. doi:https://doi.org/10.1002/gps.5158
- Lazarus, R. S., & Folkman, S. (1984). Stress, appraisal, and coping. New York: Springer.
- Lindahl, M., & Archer, T. (2013). Depressive expression and anti-depressive protection in adolescence: Stress, positive affect, motivation and self-efficacy. Psychology, 04 (06), 495–505. doi:https://doi.org/10.4236/psych.2013.46070
- Lindenberger, U., Singer, T., & Baltes, P. B. (2002). Longitudinal selectivity in aging populations: Separating mortality-associated versus experimental components in the Berlin Aging Study (BASE). The Journals of Gerontology Series B: Psychological Sciences and Social Sciences, 57(6), P474–P482. doi:https://doi.org/10.1093/geronb/57.6.P474
- Lyubomirsky, S., King, L., & Diener, E. (2005). The benefits of frequent positive affect: Does happiness lead to success? Psychological Bulletin, 131(6), 803–855. doi:https://doi.org/10.1037/0033-2909.131.6.803
- MacKinnon, D. (2008). Introduction to statistical mediation analysis. New York: Routledge. doi:https://doi.org/10.4324/9780203809556
- MacKinnon, D., Valente, M. J., & Gonzalez, O. (2020). The correspondence between causal and traditional mediation analysis: The link is the mediator by treatment interaction. Prevention Science : The Official Journal of the Society for Prevention Research, 21(2), 147–157. doi:https://doi.org/10.1007/s11121-019-01076-4
- Moffat, K., & Mercer, S. W. (2015). Challenges of managing people with multimorbidity in today's healthcare systems. BMC Family Practice, 16(1), 129. doi:https://doi.org/10.1186/s12875-015-0344-4
- Moskowitz, J. T., Carrico, A. W., Duncan, L. G., Cohn, M. A., Cheung, E. O., Batchelder, A., … Folkman, S. (2017). Randomized controlled trial of a positive affect intervention for people newly diagnosed with HIV. Journal of Consulting and Clinical Psychology, 85(5), 409–423. doi:https://doi.org/10.1037/ccp0000188
- Moskowitz, J. T., Shmueli-Blumberg, D., Acree, M., & Folkman, S. (2012). Positive affect in the midst of distress: Implications for role functioning. Journal of Community & Applied Social Psychology, 22(6), 502–518. doi:https://doi.org/10.1002/casp.1133
- Nicholson, A., Kuper, H., & Hemingway, H. (2006). Depression as an aetiologic and prognostic factor in coronary heart disease: A meta-analysis of 6362 events among 146 538 participants in 54 observational studies. European Heart Journal, 27(23), 2763–2774. doi:https://doi.org/10.1093/eurheartj/ehl338
- Nolen-Hoeksema, S. (2001). Gender differences in depression. Current Directions in Psychological Science, 10(5), 173–176. doi:https://doi.org/10.1111/1467-8721.00142
- Nolen-Hoeksema, S., Wisco, B. E., & Lyubomirsky, S. (2008). Rethinking rumination. Perspectives on Psychological Science, 3(5), 400–424. doi:https://doi.org/10.1111/j.1745-6924.2008.00088.x
- Ong, A. D., Bergeman, C. S., Bisconti, T. L., & Wallace, K. A. (2006). Psychological resilience, positive emotions, and successful adaptation to stress in later life. Journal of Personality and Social Psychology, 91(4), 730–749. doi:https://doi.org/10.1037/0022-3514.91.4.730
- Palladino, R., Tayu Lee, J., Ashworth, M., Triassi, M., & Millett, C. (2016). Associations between multimorbidity, healthcare utilisation and health status: Evidence from 16 European countries. Age and Ageing, 45(3), 431–435. doi:https://doi.org/10.1093/ageing/afw044
- Paterson, T. S. E., Yeung, S. E., & Thornton, W. L. (2016). Positive affect predicts everyday problem-solving ability in older adults. Aging & Mental Health, 20(8), 871–879. doi:https://doi.org/10.1080/13607863.2015.1043619
- Pearl, J. (1995). Causal diagrams for empirical research. Biometrika, 82(4), 669–688. doi:https://doi.org/10.1093/biomet/82.4.669
- Pearl, J. (2009). Causal inference in statistics: An overview. Statistics Surveys, 3(0), 96–146. doi:https://doi.org/10.1214/09-SS057
- Pearl, J. (2014). Interpretation and identification of causal mediation. Psychological Methods, 19(4), 459–481. doi:https://doi.org/10.1037/a0036434
- Pefoyo, A. J. K., Bronskill, S. E., Gruneir, A., Calzavara, A., Thavorn, K., Petrosyan, Y., … Wodchis, W. P. (2015). The increasing burden and complexity of multimorbidity. BMC Public Health, 15(1), 415 doi:https://doi.org/10.1186/s12889-015-1733-2
- Pinquart, M., & Sörensen, S. (2000). Influences of socioeconomic status, social network, and competence on subjective well-being in later life: A meta-analysis. Psychology and Aging, 15(2), 187–224. doi:https://doi.org/10.1037/0882-7974.15.2.187
- Pressman, S. D., Jenkins, B. N., & Moskowitz, J. T. (2019). Positive affect and health: What do we know and where next should we go? Annual Review of Psychology, 70, 627–650. doi:https://doi.org/10.1146/annurev-psych-010418-102955
- Prior, A., Fenger-Grøn, M., Larsen, K. K., Larsen, F. B., Robinson, K. M., Nielsen, M. G., … Vestergaard, M. (2016). The association between perceived stress and mortality among people with multimorbidity: A prospective population-based cohort study. American Journal of Epidemiology, 184(3), 199–210. doi:https://doi.org/10.1093/aje/kwv324
- Puth, M.-T., Weckbecker, K., Schmid, M., & Münster, E. (2017). Prevalence of multimorbidity in Germany: Impact of age and educational level in a cross-sectional study on 19,294 adults. BMC Public Health, 17(1), 826. doi:https://doi.org/10.1186/s12889-017-4833-3
- Radloff, L. S. (1977). The CES-D scale. Applied Psychological Measurement, 1(3), 385–401. doi:https://doi.org/10.1177/014662167700100306
- Read, J. R., Sharpe, L., Modini, M., & Dear, B. F. (2017). Multimorbidity and depression: A systematic review and meta-analysis. Journal of Affective Disorders, 221, 36–46. doi:https://doi.org/10.1016/j.jad.2017.06.009
- Robins, J. M., Hernán, M. Á., & Brumback, B. (2000). Marginal structural models and causal inference in epidemiology. Epidemiology (Cambridge, MA), 11(5), 550–560. https://journals.lww.com/epidem/Fulltext/2000/09000/Marginal_Structural_Models_and_Causal_Inference_in.11.aspx
- Schäfer, I., Hansen, H., Schön, G., Höfels, S., Altiner, A., Dahlhaus, A., … Wiese, B. (2012). The influence of age, gender and socio-economic status on multimorbidity patterns in primary care. First results from the multicare cohort study. BMC Health Services Research, 12, 89. doi:https://doi.org/10.1186/1472-6963-12-89
- Schiavon, C. C., Marchetti, E., Gurgel, L. G., Busnello, F. M., & Reppold, C. T. (2016). Optimism and hope in chronic disease: A systematic Review. Frontiers in Psychology, 7, 2022. doi:https://doi.org/10.3389/fpsyg.2016.02022
- Seeman, T. E., & McEwen, B. S. (1996). Impact of social environment characteristics on neuroendocrine regulation. Psychosomatic Medicine, 58(5), 459–471. doi:https://doi.org/10.1097/00006842-199609000-00008
- Sewart, A. R., Zbozinek, T. D., Hammen, C., Zinbarg, R. E., Mineka, S., & Craske, M. G. (2019). Positive affect as a buffer between chronic stress and symptom severity of emotional disorders. Clinical Psychological Science, 7(5), 914–927. doi:https://doi.org/10.1177/2167702619834576
- Shpitser, I., & VanderWeele, T. J. (2011). A complete graphical criterion for the adjustment formula in mediation analysis. The International Journal of Biostatistics, 7(1), 16. doi:https://doi.org/10.2202/1557-4679.1297
- Sin, N. L., Della Porta, M. D., & Lyubomirsky, S. (2011). Tailoring positive psychology interventions to treat depressed individuals. In S. I. Donaldson, M. Csikszentmihalyi, & J. Nakamura (Eds.), Series in applied psychology. Applied positive psychology: Improving everyday life, health, schools, work, and society (pp. 79–96). New York: Routledge/Taylor & Francis Group.
- Singer, L., Green, M., Rowe, F., Ben-Shlomo, Y., & Morrissey, K. (2019). Social determinants of multimorbidity and multiple functional limitations among the ageing population of England, 2002-2015. SSM - Population Health, 8, 100413. doi:https://doi.org/10.1016/j.ssmph.2019.100413
- Stanton, A. L., Revenson, T. A., & Tennen, H. (2007). Health psychology: Psychological adjustment to chronic disease. Annual Review of Psychology, 58, 565–592. doi:https://doi.org/10.1146/annurev.psych.58.110405.085615
- Steptoe, A., Dockray, S., & Wardle, J. (2009). Positive affect and psychobiological processes relevant to health. Journal of Personality, 77(6), 1747–1775. doi:https://doi.org/10.1111/j.1467-6494.2009.00599.x
- Taylor, C. T., Lyubomirsky, S., & Stein, M. B. (2017). Upregulating the positive affect system in anxiety and depression: Outcomes of a positive activity intervention. Depression and Anxiety, 34(3), 267–280. doi:https://doi.org/10.1002/da.22593
- Tetzlaff, J., Muschik, D., Epping, J., Eberhard, S., & Geyer, S. (2017). Expansion or compression of multimorbidity? 10-year development of life years spent in multimorbidity based on health insurance claims data of Lower Saxony, Germany. International Journal of Public Health, 62(6), 679–686. doi:https://doi.org/10.1007/s00038-017-0962-9
- Tugade, M. M., & Fredrickson, B. L. (2007). Regulation of positive emotions: Emotion regulation strategies that promote resilience. Journal of Happiness Studies, 8(3), 311–333. doi:https://doi.org/10.1007/s10902-006-9015-4
- van den Akker, M., Buntinx, F., & Knottnerus, J. A. (1996). Comorbidity or multimorbidity: What's in a name? A review of literature. European Journal of General Practice, 2(2), 65–70. doi:https://doi.org/10.3109/13814789609162146
- van den Akker, M., Buntinx, F., Roos, S., & Knottnerus, J. A. (2001). Problems in determining occurrence rates of multimorbidity. Journal of Clinical Epidemiology, 54(7), 675–679. doi:https://doi.org/10.1016/S0895-4356(00)00358-9
- van den Berg, K. S., Wiersema, C., Hegeman, J. M., van den Brink, R. H. S., Rhebergen, D., Marijnissen, R. M., & Oude Voshaar, R. C. (2019). Clinical characteristics of late-life depression predicting mortality. Aging & Mental Health, 1–8. Advance online publication. doi:https://doi.org/10.1080/13607863.2019.1699900
- van den Bussche, H., Koller, D., Kolonko, T., Hansen, H., Wegscheider, K., Glaeske, G., … Schön, G. (2011). Which chronic diseases and disease combinations are specific to multimorbidity in the elderly? Results of a claims data based cross-sectional study in Germany. BMC Public Health, 11, 101. doi:https://doi.org/10.1186/1471-2458-11-101
- VanderWeele, T. J., & Tchetgen Tchetgen, E. J. (2017). Mediation analysis with time varying exposures and mediators. Journal of the Royal Statistical Society, Series B, 79(3), 917–938. doi:https://doi.org/10.1111/rssb.12194
- VanderWeele, T. J., Vansteelandt, S., & Robins, J. M. (2014). Effect decomposition in the presence of an exposure-induced mediator-outcome confounder. Epidemiology (Cambridge, MA), 25(2), 300–306. https://doi.org/10.1097/EDE.0000000000000034
- Vazquez, C. (2017). What does positivity add to psychopathology? An introduction to the special issue on 'positive emotions and cognitions in clinical psychology. Cognitive Therapy and Research, 41(3), 325–334. doi:https://doi.org/10.1007/s10608-017-9847-8
- Wahl, H. W., Drapaniotis, P. M., & Heyl, V. (2014). Functional ability loss in sensory impaired and sensory unimpaired very old adults: Analyzing causal relations with positive affect across four years. Experimental Gerontology, 59, 65–73. doi:https://doi.org/10.1016/j.exger.2014.06.008
- Watson, D., Clark, L. A., & Tellegen, A. (1988). Development and validation of brief measures of positive and negative affect: The PANAS scales. Journal of Personality and Social Psychology, 54(6), 1063–1070. doi:https://doi.org/10.1037//0022-3514.54.6.1063
- Wilamowska, Z. A., Thompson‐Hollands, J., Fairholme, C. P., Ellard, K. K., Farchione, T. J., & Barlow, D. H. (2010). Conceptual background, development, and preliminary data from the unified protocol for transdiagnostic treatment of emotional disorders. Depression and Anxiety, 27(10), 882–890. doi:https://doi.org/10.1002/da.20735
- Williams, R. B. (2011). Cardiology patient page. Depression after heart attack: Why should I be concerned about depression after a heart attack? Circulation, 123(25), e639–e640. doi:https://doi.org/10.1161/CIRCULATIONAHA.110.017285
- Xu, Y., Yu, Y., Xie, Y., Peng, L., Liu, B., Xie, J., … Li, M. (2015). Positive affect promotes well-being and alleviates depression: The mediating effect of attentional bias. Psychiatry Research, 228(3), 482–487. doi:https://doi.org/10.1016/j.psychres.2015.06.011
- Yarnall, A. J., Sayer, A. A., Clegg, A., Rockwood, K., Parker, S., & Hindle, J. V. (2017). New horizons in multimorbidity in older adults. Age and Ageing, 46(6), 882–888. doi:https://doi.org/10.1093/ageing/afx150
Appendix
Formulas for IPW calculation
Calculation of inverse probability weight for outcome model:(6)
(6)
Calculation of inverse probability weight for mediator model:(7)
(7)